Back to Journals » International Journal of Women's Health » Volume 17
Three Separate Cases of Polypoid Endometriosis Coincided with Abscess, Angioleiomyoma or Stromal Sarcoma
Authors Wu Z, Xu Q, Sun Y, Ruan F
Received 25 November 2024
Accepted for publication 3 April 2025
Published 13 April 2025 Volume 2025:17 Pages 1049—1054
DOI https://doi.org/10.2147/IJWH.S508521
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Zaigui Wu,1,2 Qiong Xu,3 Yao Sun,4 Fei Ruan1,2
1Department of General Gynecology, Women’s Hospital, School of Medicine, Zhejiang University, Hangzhou, People’s Republic of China; 2Zhejiang Provincial Clinical Research Center for Obstetrics and Gynecology, Hangzhou, People’s Republic of China; 3Department of Radiology, Women’s Hospital, School of Medicine, Zhejiang University, Hangzhou, People’s Republic of China; 4Department of Pathology, Women’s Hospital, School of Medicine, Zhejiang University, Hangzhou, People’s Republic of China
Correspondence: Fei Ruan, Department of General gynecology, Women’s Hospital, School of Medicine, Zhejiang University, Xueshi Road 1, Hangzhou, Zhejiang, People’s Republic of China, Email [email protected]
Background: Polypoid endometriosis is rare and differs from classic endometriosis. It has been primarily documented in case reports and often misdiagnosed as malignancy. The aim of this study is to report three separate cases of polypoid endometriosis coincided with multiple abscess, angioleiomyoma or stromal sarcoma, respectively.
Case Presentation: The first case was 36 years old and presented with six months of dysmenorrhea and menstrual fever. Two cervical masses, one located in vaginal and one in pelvic, were detected by ultrasound. After a total hysterectomy, she was diagnosed with cervical polypoid endometriosis with multiple abscess. The second case aged 36-years too and had menstrual bleeding prolonged to 10– 15 days for four months. Ultrasound showed a 6cm mass like leiomyomas but with rich vascularity, while MRI tested signal intensity similar to that of endometrium. A diagnosis of polypoid endometriosis coincided with angioleiomyoma was made after surgery. The third patient was 40 and experienced lower abdominal pain for eight months. The ultrasound and MRI tested multiple solid-cystic masses in the left ovary and pelvic. The subsequent pathology revealed extensive stromal nodules in various areas such as bilateral ovaries, posterior uterine wall, intestinal tract and left ureter, indicating the diagnosis of low malignant potential stromal sarcoma.
Conclusion: Polypoid endometriosis coincided with multiple abscess, angioleiomyoma or stromal sarcoma are rather rare and require aggressive surgical treatment.
Keywords: polypoid endometriosis, abscess, angioleiomyoma, stromal nodules, case series
Introduction
Endometriosis (EMs) is defined as the ectopic growth of endometrial glands and stroma outside the uterus, while polypoid endometriosis (PEM) is a rare type of EMs, which is characterized by its histological resemblance to endometrial polyps.1,2 It has been revealed mostly by case reports for rare presentations. Unlike classic EMs, it occurs more in peri- or postmenopausal women and involves multiple sites, including the ovary, colon, uterine serosa, and vaginal mucosa.3 So far, fewer than 16 cases under 40 years old and five cases with cervix affected have been reported.3
PEM usually presents as a cystic mass with solid components or mural nodules. These solid nodules shall be differentiated with malignant cancers, endometrial stromal tumors, angioleiomyoma, fibroma and so on. Though each one of these entities has their typical histologic characteristics, immunohistochemical (IHC) staining deserves to establish the correct diagnosis.4 In fact, endometriosis-associated stromal sarcoma is uncommon.5 Herein, we carried out a retrospective case analysis to present three separate cases of PEM coincided with particularly rare histopathology and investigate their clinical and imaging features as well.
Case Presentation
Case 1
The first case was a 36-year-old woman (G4P2) with six months of dysmenorrhea and menstrual high fever up to 39.5°C. She visited our hospital in Oct. 2022. The gynecological examination found a purulent cervical discharge and a 2 cm fresh granuloma at the posterior apex (Figure 1A and B). Contrast-enhanced ultrasound (CEUS) and magnetic resonance imaging (MRI) revealed a benign inflammatory pelvic mass measuring 6 cm in the greatest diameter, along with a posterior granuloma (Figure 1C). Her CA-125 level was 480IU/mL, and she had no significant medical history. The preoperative diagnosis was cervical cancer with pelvic dissemination.
 |
Figure 1 Cervical posterior isthmus penetrating pyogenic PEM. (A and B) Gross appearance of cervix purulent secretion and a fresh granuloma in the posterior apex, (C) MRI imaging showing the pelvic mass and a posterior granuloma, and (D) microphotograph showing endometrial glands, stroma and abscess. |
A diagnostic cervical mass excision was first performed, and the diagnosis of PEM with multiple abscess was made by histopathology. Treatment with ZOLADEX was recommended, but symptoms persisted, and the cervical polypoid masses reappeared, while the pelvic mass did not decrease during the third injection. Thus, a hysterectomy was conducted in Jan. 2023, and the diagnosis of cervical penetrating pyogenic PEM was confirmed by histopathology (Figure 1D). Her CA-125 level normalized quickly after the operation, and no recurrence happened so far.
Case 2
The second case was a 36-year-old female (G1P1) and presented with four months of menstrual bleeding prolonging to 10–15 days. She was diagnosed with submucous myoma in Dec. 2018 and underwent the transcervical resection of myoma in our hospital. A 4 cm hydatidiform mass was resect and immunohistochemical (IHC) staining showed positive smooth muscle actin (SMA) and negativity for HMB-45 and Ki-67. A diagnosis of angioleiomyoma with proliferative endometrium was offered. After operation, her menstrual pattern returned normally for one year.
In Dec.2019, her menstrual period prolonged again to 20 days and ultrasound test detected a 1.5 cm myoma in last site. The myoma grew rapidly to 6cm within nine months, causing menstrual bleeding increased significantly. She referred to our hospital for second surgery in Sep.2020. Preoperative ultrasound test showed leiomyomas exhibiting rich vascularity (Figure 2A) and MRI image showed its signal intensity similar to that of the endometrium (Figure 2B). A laparoscopic removal of the mass revealed a 6 cm brittle mass with no clear myomatoid structure. IHC results showed positivity for Desmin, SMA, ER and CD10 in stromal cells, while the Ki-67 labeling index was 20%. These confirmed the diagnosis of PEM and angioleiomyoma (Figure 2C and D).
 |
Figure 2 PEM coexisting with angioleiomyomas. (A) Ultrasound image showing leiomyomas exhibiting rich vascularity, (B) MRI image showing its signal intensity similar to that of the endometrium, (C and D) microphotograph showing ectopic endometrial and angioleiomyomas. |
Case 3
The third case was a 40-year-old woman (G3P2), and she had underwent abdominal bilateral ovarian cystectomy and myomectomy in 2000. The ovarian cyst recurred with no symptoms in 2012. Until Nov. 2013, she referred to our outpatient clinic for eight months of lower abdominal pain. Ultrasound examination identified a 6 cm hypoechoic mass in posterior uterus with chaotic internal echoes, along with a 8 cm mass behind the uterus which separated unclearly from uterine wall. Further MRI test revealed left ovarian and pelvic multiple solid-cystic masses, while solid components were moderately hyperintense on FS-T2WI and markedly hyperintense on DWI (Figure 3A and B).
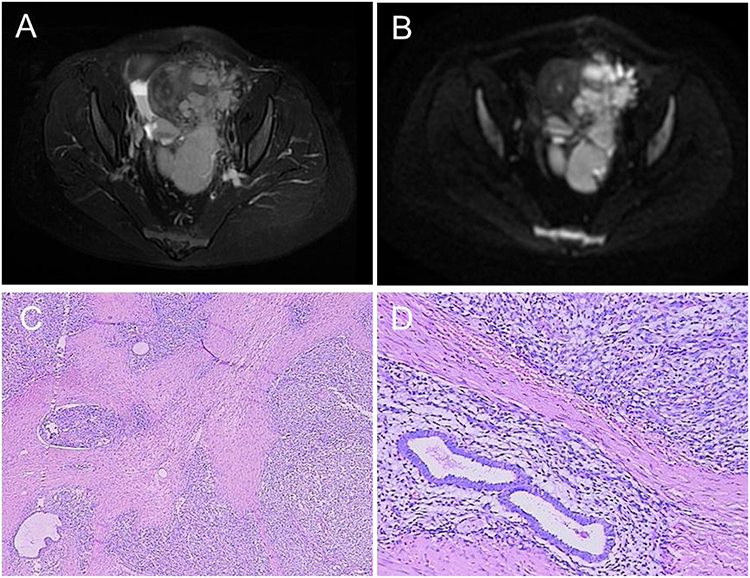 |
Figure 3 PEM with endometrial stromal nodules and disseminated growth. (A) FS-T2WI shows multiple left ovarian and pelvic solid cystic masses, while solid components are moderately hyperintense; (B) solid components are markedly hyperintense on DWI (high b-value), (C) ectopic endometrial and stromal nodules, and (D) endometriosis and abundant stroma. |
During laparoscopy, a solid cystic mass in the left ovary led to a provisional diagnosis of PEM, and abdominal bilateral ovarian and total hysterectomy were eventually done due to dense adhesion. Multiple EM lesions were discovered on the uterus, sigmoid colon, rectum and left ureter extending to the kidney. The histopathological analysis revealed the widespread dissemination of endometrial stromal nodules in both ovaries, right fallopian tube, ovarian blood vessels, intestine and intestinal mesentery. IHC study of these samples revealed positive SMA, CD10, ER and PR, and the Ki-67 labeling index was 30%, supporting the clinical diagnosis of low-grade malignant potential stromal sarcoma (Figure 3C and D).
Discussion
This paper, to the best of our knowledge, is the first case series reported in the literature of PEM coexisting with cervical multiple abscesses, uterine angioleiomyomas, or multi-organ disseminated endometrial stromal nodules, respectively.
EM patients, even virginal young women, are at higher risk for developing ovarian abscess and tends to be more severe, frequently requiring surgical intervention.6,7 The main symptoms are acute fever and abdominal pain, which might not be related to menstrual cycle. To date, there are no reports of PEM presented with abscesses, and cases with cervix involved are documented only in five patients.3 The case 1 was cervical PEM with multiple abscess and exhibited cyclic high fever during menstruation. As imaging features, the black rim sign on MRI and CEUS showing a global hyper-enhancement pattern with fast forward and reverse compared to normal myometrium suggested the diagnosis of PEM with abscess.8–10 Due to multiple abscess, she did not respond to treatment with ZOLADEX, and a radical hysterectomy should be deserved.
There has been one report about intestinal PEM with abundant leiomyoma-like smooth muscle components, but PEM with uterine angioleiomyoma has not been documented before.11 Angioleiomyomas in female urogenital tract is rare, accounting for 0.4% of uterine leiomyomas, and the intracavitary lesions are extremely unusual.4,12 Case 2 is the second report of intracavitary angioleiomyomas and is also the first report of angioleiomyomas coexisted with PEM. It is important to distinguish this condition from atypical polypoid adenomyomas through IHC. PEM with angioleiomyomas showed diffuse and strong positivity for SMA, desmin and CD10 in stromal cells, while CD10 expression in atypical polypoid adenomyomas was negative.4,13
Ovarian PEM often appears as papillary masses in endometriotic cysts, but cysts with solid components or nodules may indicate malignancy. Benign nodules will not be enhanced, while malignant nodules are enhanced by MRI test as shown in case 3.5 Endometrial stromal sarcoma from endometriotic lesions is rare but can spread aggressively in the abdomen.14 The widespread distribution of endometrial stromal nodules in multiple organs along with the IHC results provides evidence for the diagnosis of low-grade malignant potential stromal sarcoma in case 3. The patient’s survival during an almost 11-year follow-up period further validates the favorable influence of endometriosis on the patient’s prognosis.15
Conclusion
In summary, we present three separate and unique cases of PEM with multiple cervical abscesses, uterine angioleiomyomas, and widely disseminated stromal nodules, respectively. Although PEM, endometrial stromal nodules and angioleiomyomas are rare and morphologic mimickers, immunohistochemical staining can play a role in their differential diagnosis.
Abbreviations
Ems, endometriosis; PEM, polypoid endometriosis; CA-125, carbohydrate antigen 125; IHC, immunohistochemical.
Ethics Approval and Informed Consent
This study was approved by the Ethics Committees of Women’s Hospital, School of Medicine, Zhejiang University (IRB-20230272-R). Written informed consent had been provided by these three patients to have the case details and accompanying images published.
Funding
This study was supported by 4+X Clinical Research Project of Women’s Hospital, School of Medicine, Zhejiang University (no. ZDF2022-4X206) and the Zhejiang Province Natural Science Funds Grant (no. LGF22H040002).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Horne AW, Missmer SA. Pathophysiology, diagnosis, and management of endometriosis. BMJ. 2022;379:e70750.
2. Stewart CJ, Bharat C. Clinicopathological and immunohistological features of polypoid endometriosis. Histopathology. 2016;68(3):398–404. doi:10.1111/his.12755
3. Parker RL, Dadmanesh F, Young RH, Clement PB. Polypoid endometriosis: a clinicopathologic analysis of 24 cases and a review of the literature. AM J Surg Pathol. 2004;28(3):285–297. doi:10.1097/00000478-200403000-00001
4. Sanchez-Iglesias J, Capote S, Cubo-Abert M, et al. A giant superinfected uterine angioleiomyoma with distant septic metastases: an extremely rare presentation of a benign process and a systematic review of the literature. Arch Gynecol Obstet. 2019;300(4):841–847. doi:10.1007/s00404-019-05267-w
5. Ohya A, Fujinaga Y. Magnetic resonance imaging findings of cystic ovarian tumors: major differential diagnoses in five types frequently encountered in daily clinical practice. Jpn J Radiol. 2022;40(12):1213–1234. doi:10.1007/s11604-022-01321-x
6. Li H, Zhao Y, Chang X, Wang Y, Zhu H. Clinical characteristics, treatment status and complications in women with tube ovarian abscess and endometriosis: a retrospective study. BMC Womens Health. 2021;21(1):109. doi:10.1186/s12905-020-01119-x
7. Villette C, Bourret A, Santulli P, Gayet V, Chapron C, de Ziegler D. Risks of tubo-ovarian abscess in cases of endometrioma and assisted reproductive technologies are both under- and overreported. Fertil Steril. 2016;106(2):410–415. doi:10.1016/j.fertnstert.2016.04.014
8. Yajima R, Kido A, Minamiguchi S, et al. MR findings of polypoid endometriosis of female genital organs: report of three cases. Abdom Radiol. 2022;47(6):1968–1974. doi:10.1007/s00261-022-03530-4
9. Takeuchi M, Matsuzaki K, Bando Y, Harada M. Magnetic resonance imaging characteristics of polypoid endometriosis and review of the literature. J Obstet Gynaecol Res. 2022;48(10):2583–2593. doi:10.1111/jog.15367
10. Green RW, Epstein E. Dynamic contrast-enhanced ultrasound improves diagnostic performance in endometrial cancer staging. Ultrasound Obst Gyn. 2020;56(1):96–105. doi:10.1002/uog.21885
11. Zimmer V, Emrich K. Polypoid colorectal endometriosis with abundant leiomyoma-like smooth muscle cell proliferation treated by endoscopic resection. Digest Liver Dis. 2023;55(4):557–558. doi:10.1016/j.dld.2023.01.163
12. Gorginzadeh M, Tahermanesh K, Hanjani S, et al. Uterine intracavitary angioleiomyoma. J Obstet Gynaecol. 2020;40(8):1186–1188. doi:10.1080/01443615.2019.1705775
13. Sun Y, Tian L, Liu G. A clinicopathological review of 203 cases of atypical polypoid adenomyoma of the uterus. J Clin Med. 2023;12(4):1511. doi:10.3390/jcm12041511
14. Yang C, Oh HK, Kim D. Mullerian adenosarcoma arising from rectal endometriosis. Ann Coloproctol. 2014;30(5):232–236. doi:10.3393/ac.2014.30.5.232
15. Stern RC, Dash R, Bentley RC, Snyder MJ, Haney AF, Robboy SJ. Malignancy in endometriosis: frequency and comparison of ovarian and extraovarian types. Int J Gynecol Pathol. 2001;20(2):133–139. doi:10.1097/00004347-200104000-00004
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.