Back to Journals » Clinical Ophthalmology » Volume 20
Three-Dimensional Reconstruction for Localizing Retinal Tears in Treatment of Rhegmatogenous Retinal Detachment by Foldable Capsular Buckle
Received 20 November 2025
Accepted for publication 5 March 2026
Published 21 March 2026 Volume 2026:20 583192
DOI https://doi.org/10.2147/OPTH.S583192
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yousef Fouad
Xuemin Tian,1 Qianying Gao2
1Department of Ophthalmology, The 988th Hospital of Joint Logistics Support Forces of the People’s Liberation Army, Zhengzhou, Henan, 450000, People’s Republic of China; 2Research and Development Department, Vesber Vitreous Institute, Guangzhou, Guangdong, 510060, People’s Republic of China
Correspondence: Qianying Gao, Research and Development Department, Vesber Vitreous Institute, Nanjiang Second Road No. 6, Zhujiang Street, Nansha District, Guangzhou, Guangdong, 510060, People’s Republic of China, Tel +86-20-28687088, Email [email protected]
Purpose: This study aimed to accurately localize retinal tears using computer three-dimensional (3D) reconstruction technology and to validate this method in combination with Foldable Capsular Buckle (FCB) implantation for treating rhegmatogenous retinal detachment (RRD).
Methods: Assuming a circle passing through the tear, macula, and anterior corneal vertex, computer-aided design (CAD) software calculated half circumferences for varying axial lengths. The distance from the tear’s anterior edge to the posterior corneoscleral limbus was derived as the half circumference minus the corneal radius, further subtracting the arc length from the tear to the macula. The chord length from the tear to the macula was converted from the arc length, and breaks were localized by scaling chord lengths using the optic disc’s horizontal diameter.
Results: For axial lengths of 23.5– 30 mm, half circumferences ranged from 36.5– 45.5 mm. For arc lengths of 11.5– 23.5 mm, corresponding chord lengths were 10– 20 mm, with no significant correlation with axial length. Clinically, retinal reattachment was achieved in 42/43 patients (97.7%), with postoperative fundoscopy confirming effective FCB indentation. Visual acuity improved significantly from a preoperative median of 0.10 (range: hand motion to 0.8) to a postoperative median of 0.40 (range: counting fingers to 1.0) (Z = 5.43, p < 0.001), with 88.4% of patients showing improvement. Intraocular pressure (IOP) increased mildly from 12.6 ± 2.7 mmHg preoperatively to 14.7 ± 1.6 mmHg postoperatively (mean increase: 2.1 mmHg; 95% CI: 1.4– 2.8 mmHg; t = 5.12, p < 0.001), with all values remaining within the normal range.
Conclusion: This simple ruler-based method enables accurate preoperative tear localization and FCB fixation point calculation, providing a practical and effective solution for surgeons performing extraocular buckling procedures.
Keywords: rhegmatogenous retinal detachment, RRD, retinal tear, tear localization, foldable capsular buckle, FCB
Introduction
Rhegmatogenous retinal detachment (RRD) is a common vitreoretinal disease characterized by separation of the neuroepithelial layer from the pigment epithelial layer, leading to photoreceptor apoptosis and severe visual impairment.1 Its annual incidence is approximately 1 per 10,000 individuals.2 Treatment requires surgical identification and closure of all retinal tears while relieving vitreoretinal traction. Surgical approaches include extraocular methods—traditional scleral buckling (SB) and foldable capsular buckle (FCB) implantation—and intraocular methods such as pars plana vitrectomy (PPV) and pneumatic retinopexy (PR).3,4
The key to successful RRD repair lies in the accurate localization and closure of the retinal break—a principle unchanged since Gonin first established the role of the break in RRD pathogenesis in 1929.5 Over the past 80 years, surgical techniques have evolved from extensive diathermy and scleral resection to segmental buckling, cerclage, pneumatic retinopexy, and vitrectomy; however, the fundamental requirement remains the same: to find and adequately seal the causative break.5
During extraocular surgery,6–9 accurate localization of retinal tears, appropriate application of cryotherapy, and confirmation that the tear is positioned on the buckle ridge are critical steps.10,11 Nevertheless, current methods—including direct and indirect ophthalmoscopy, slit-lamp biomicroscopy, and ultra-widefield imaging—rely heavily on surgeon experience, lack quantitative accuracy, and provide no standardized preoperative protocol.12,13 These limitations are particularly problematic in myopic eyes, cases with variable optic disc anatomy, or minimally invasive procedures.12,13
The foldable capsular buckle (FCB) is a novel, minimally invasive device for scleral indentation without intraocular intervention.14,15 The application of FCB in scleral buckling surgery for RRD represents a technique that is straightforward, safe, effective, minimally invasive, and associated with fewer complications.14,15 Critically, the success of FCB implantation depends on accurate preoperative break localization to ensure the buckle ridge effectively tamponades the tear.14
To address this need, we developed a 3D reconstruction method using CAD to quantitatively calculate tear positions based on axial length, optic disc metrics, and geometric modeling. By integrating this approach with FCB implantation, we aimed to establish a simple, ruler-based protocol for preoperative tear localization and FCB fixation point determination, ultimately improving surgical precision and success rates in RRD repair. This method directly addresses the limitations of existing qualitative techniques by providing a quantitative, standardized, and easily implementable solution for preoperative tear mapping.
Methods
Localization of Retinal Break
Assuming a circle passing through the retinal break, macula, and anterior corneal vertex (Figure 1A), half circumferences for different axial lengths were calculated using CAD software (Figure 1B–D). The human eye was approximated as a sphere for computational simplicity, consistent with prior studies on ocular biometry. While the eye’s true pear-shaped anatomy introduces minor deviations, this assumption allows standardized calculations across axial lengths (23.5–30 mm) and facilitates integration with clinical databases.16
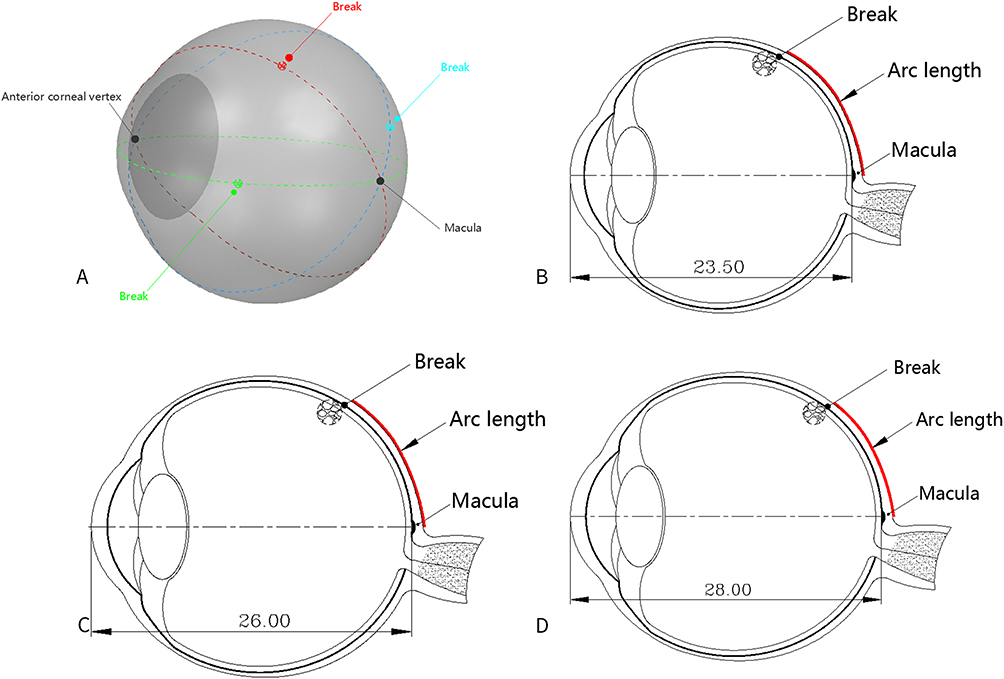 |
Figure 1 Localization of retinal break under different axial lengths. (A) Circle passing through retinal break, macula, and anterior corneal vertex. (B) Axial length 23.5 mm. (C) Axial length 26 mm. (D) Axial length 28 mm. |
The distance from the break front edge to the corneoscleral limbus was derived as:
Arc Length = Half Circumference − Corneal Radius − Arc Length from Break Anterior Edge to Macula
Relationship Between Arc Length and Chord Length Based on Different Axial Length
To standardize calculations, chord length (CL)—the straight-line distance between two points on a curved surface—was introduced. Two-dimensional sectional models of axial lengths (23.5–30 mm) were generated in CAD (Figure 2). Within the 23.5–27 mm range, eight models were generated at 0.5 mm intervals; for 27–30 mm, three models were generated at 1 mm intervals.
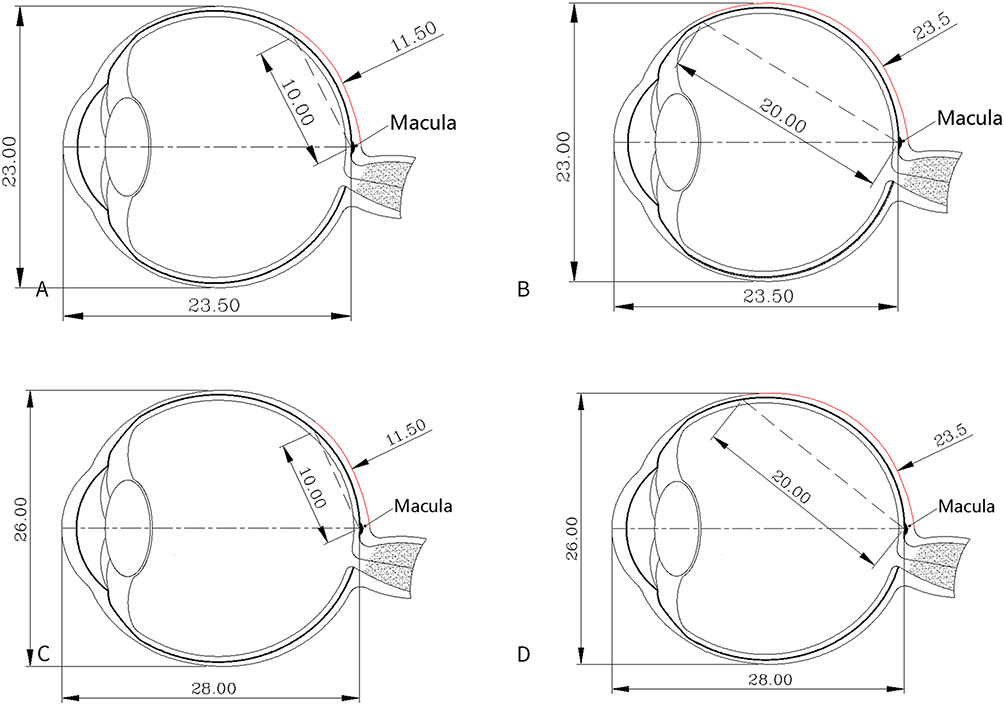 |
Figure 2 Correspondence between chord length and arc length in two-dimensional sectional models for axial lengths of 23.5 mm and 28 mm. (A) AL 23.5 mm: arc 11.5 mm → chord 10 mm. (B) AL 23.5 mm: arc 23.5 mm → chord 20 mm. (C) AL 28 mm: arc 11.5 mm → chord 10 mm. (D) AL 28 mm: arc 23.5 mm → chord 20 mm. |
Calculation of the FCB Capsule Fixation Point Posterior to the Corneoscleral Limbus Based on FCB Physical Parameters
The FCB consists of a capsule integrated with a drainage tube and valve system, forming a single-piece structure. Saline is injected into the capsule through the drainage valve, creating internal pressure. The horizontal and vertical diameters of the capsule increase with the volume of injected saline, and the pressure increases accordingly (Figure 3).
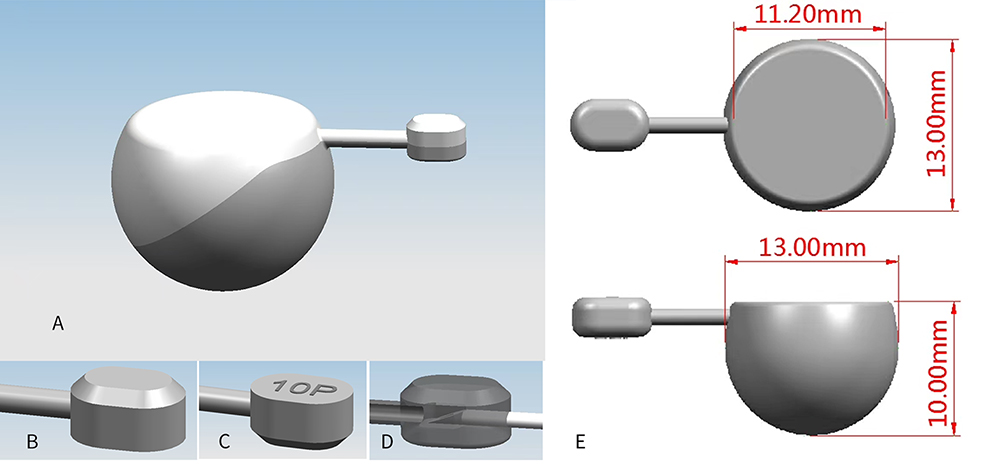 |
Figure 3 FCB physical parameters. (A) Capsule lens surface and parting line. (B) Drainage valve close to optical zone (front view). (C) Drainage valve close to capsule (back view). (D) Drainage cup puncture. (E) Optical zone diameter, capsule diameter, and anteroposterior diameter. |
The FCB’s spherical diameter is 13 mm, with a peripheral 4 mm ring deducted, yielding a 5×5 mm effective indentation area. Accordingly, the formula for calculating the fixation point of the FCB capsule posterior to the corneoscleral limbus is: half circumference − arc length from break anterior edge to macula fovea − corneal radius − 4 mm (Figure 4). The calculated FCB fixation point serves as a preoperative guide.
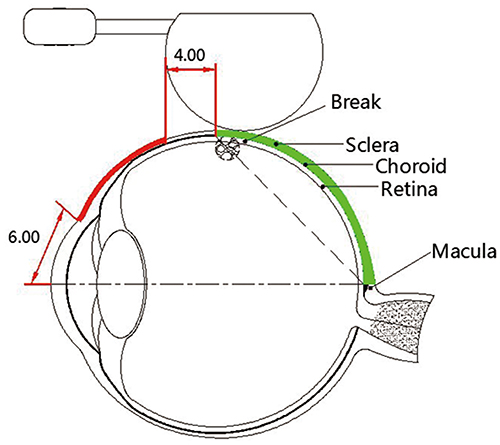 |
Figure 4 Schematic diagram of FCB fixation point on scleral surface and extraocular indentation. |
Clinical Workflow
To facilitate clinical application, the complete preoperative workflow is summarized in Figure 5. Surgeons can use a smartphone and a ruler to measure chord lengths directly from fundus images, enabling rapid calculation of arc lengths. This step-by-step protocol guides the surgeon from initial data collection through final determination of the FCB fixation point, clock-hour position, and recommended saline injection volume. The workflow integrates the formulas, tables, and measurement techniques detailed in the preceding sections into a practical clinical tool.
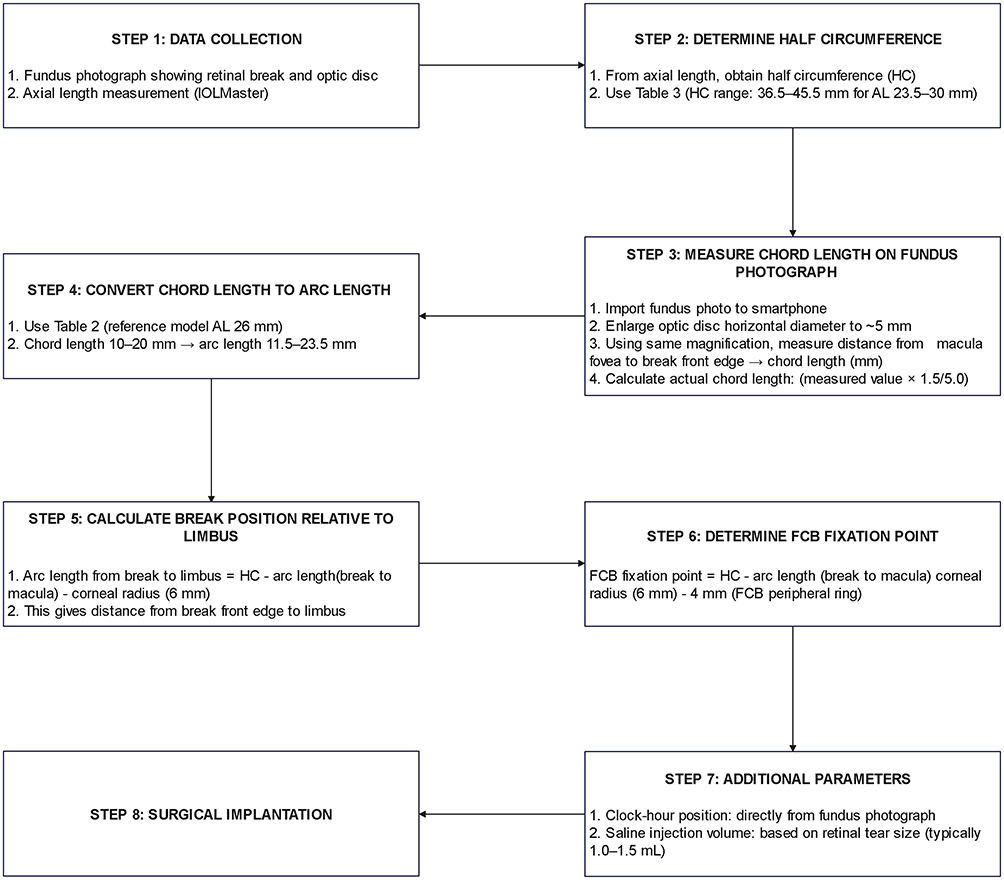 |
Figure 5 Clinical workflow for preoperative tear localization and FCB fixation point determination. |
Case Collection and Verification After FCB Implantation
Fundus photographs and axial length data were collected from patients’ eyes, and 3D reconstruction was performed to locate retinal tears and determine the FCB fixation point, recommended saline injection volume, and implantation orientation. The study protocol was approved by the Medical Ethics Committee of The 988th Hospital of Joint Logistics Support Forces of the People’s Liberation Army (No. 988YY2019048LLSP) and was conducted in accordance with the Declaration of Helsinki, the International Conference on Harmonisation of Good Clinical Practice guidelines, and applicable Chinese law. Written informed consent was obtained from all patients prior to inclusion. All patient data were anonymized and handled confidentially.
The main steps of FCB implantation were: 1) anesthesia; 2) traction suture along the limbus toward the retinal break; 3) incision; 4) fixation suture placement and suturing; 5) product preparation; 6) implantation; 7) subretinal fluid release to lower IOP; 8) saline injection; 9) ligation of the drainage tube and fixation loops; and 10) suture closure of the incision.
Statistical Analysis
To objectively evaluate surgical outcomes, we compared preoperative and postoperative visual acuity using the Wilcoxon signed-rank test and IOP using the paired t-test after confirming normality with the Shapiro–Wilk test.
Results
Localization of Retinal Break
The formula for retinal break localization is: arc length from the break’s anterior edge to the corneoscleral limbus = half circumference − arc length from break anterior edge to macula fovea − corneal radius. Based on this formula, the position of the break’s anterior edge can be precisely determined.
Relationship Between Arc Length and Axial Length Under Different Axial Lengths and Fixed Chord Length
According to computer simulation calculations (Table 1), under a fixed chord length of 15.0 mm and varying axial lengths, the arc length was approximately 17 mm, with minimal differences (≤0.2 mm). Importantly, these arc length values were not derived from a simple spherical approximation; rather, they were generated using CAD models that incorporate individual axial lengths and corresponding ocular dimensions (anteroposterior, horizontal, and vertical diameters), accurately reflecting the true geometry of eyes with varying axial lengths. Furthermore, this finding has direct clinical relevance: the minimal variation in arc length across different axial lengths demonstrates that axial length has a negligible impact on the chord-to-arc length relationship.
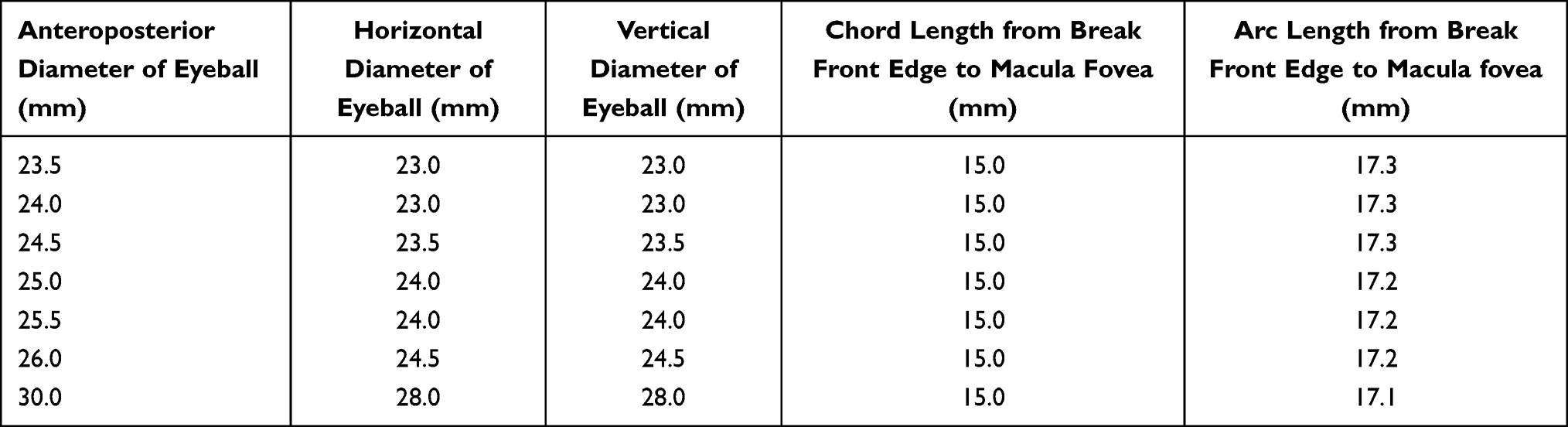 |
Table 1 Relationship Between Arc Length and Axial Length Under Fixed Chord Length |
Relationship Between Chord Length and Arc Length Under 26.0 mm Axial Length
As shown in Table 2, based on the reference ocular model with an axial length of 26.0 mm, computer simulation calculations reveal that with a chord length interval gradient of 1.0 mm, the arc length increases incrementally with chord length. In summary, when chord length ranges from 10.0–20.0 mm, arc length ranges from 11.5–23.5 mm, with no apparent correlation with axial length.
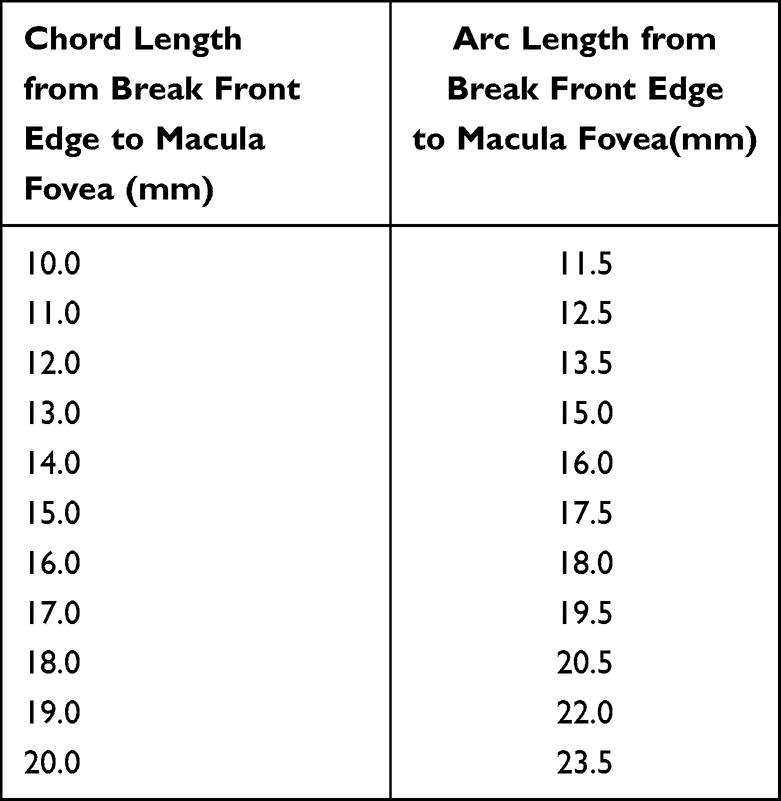 |
Table 2 Relationship Between Arc Length and Chord Length Under 26.0 mm Axial Length |
Relationship Between Half Circumference and Axial Length
As shown in Table 3, the axial length range of 23.5–30.0 mm corresponds to a half circumference range of 36.5–45.5 mm. Axial length increases with the severity of myopia, and half circumference increases correspondingly.
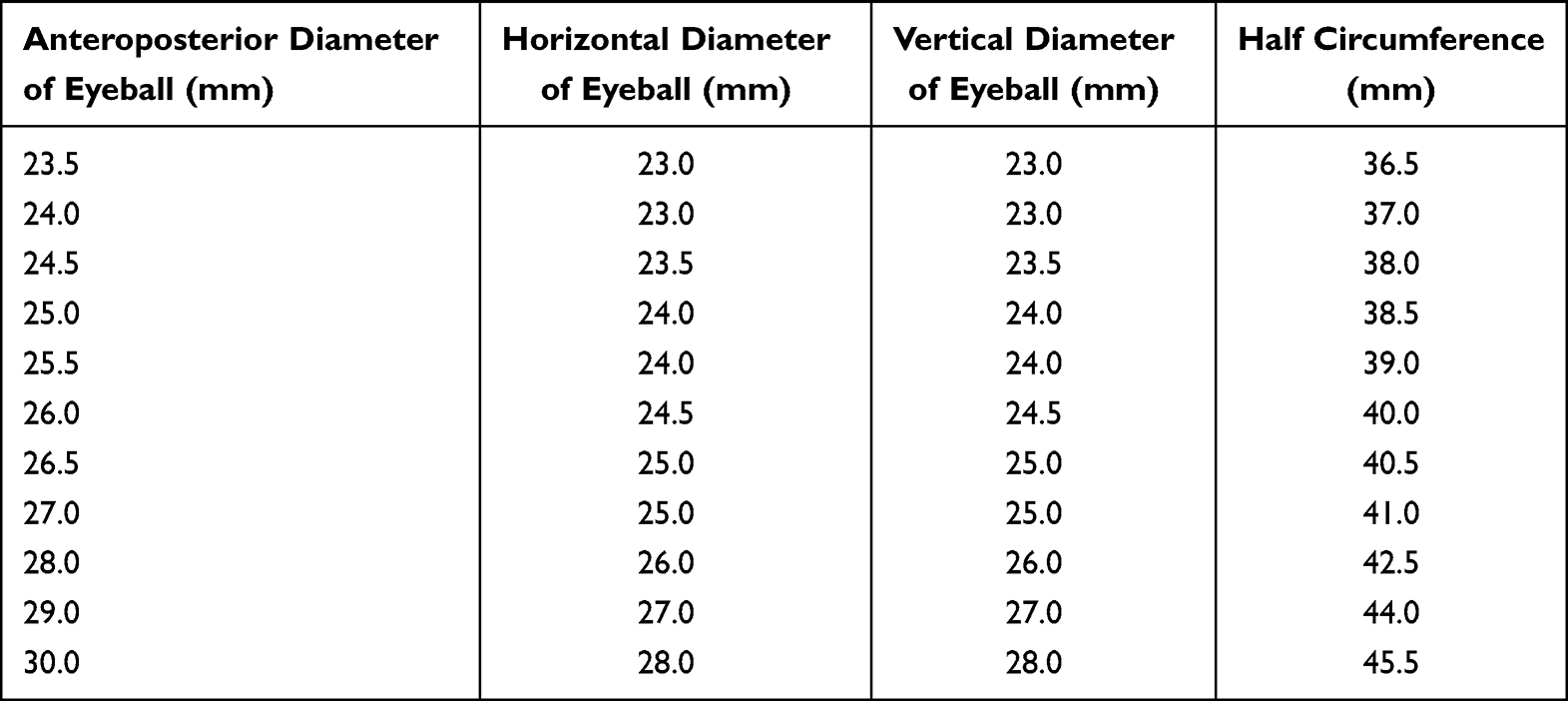 |
Table 3 Relationship Between Half Circumference and Axial Length |
Application Example of Computer Simulation Calculation for FCB Extraocular Indentation Position
In clinical practice, axial length is measured using IOLMaster, and optic disc horizontal diameter is measured using OCT. Fundus photographs are imported into a smartphone, and the optic disc is enlarged to approximately 5 mm. Using a ruler, the distance from the break’s anterior edge to the foveal center is measured at the same magnification. This allows calculation of the arc length from the break’s anterior edge to the corneoscleral limbus and the clock-hour position of the break relative to the macula. Additionally, the FCB’s spherical diameter is 13 mm, with a peripheral 4 mm ring deducted, resulting in an effective indentation area of 5×5 mm. Therefore, the formula for the FCB fixation point (scleral arc length from the FCB capsule–drain tube junction to the corneoscleral limbus) is: half circumference − arc length from break anterior edge to macula fovea − corneal radius − 4 mm.
As shown in Figure 6, for example, with an axial length of 26.5 mm, Table 3 gives a half circumference of 40.5 mm. Using the optic disc horizontal diameter as a scale, chord length is calculated as 18.0 mm, and Table 2 gives a corresponding arc length of 20.5 mm; corneal radius is 6.0 mm. According to the formula, the FCB fixation point (red arrow) is: 40.5 mm − 20.5 mm − 6.0 mm − 4.0 mm = 10.0 mm posterior to the corneoscleral limbus.
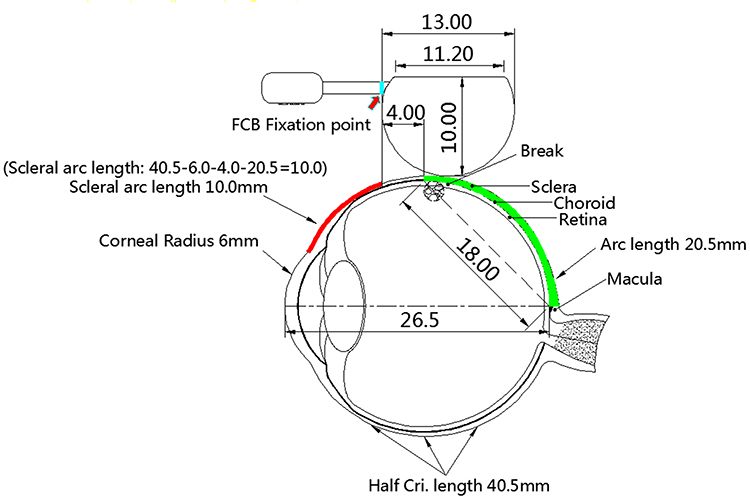 |
Figure 6 Diagram of FCB fixation point (red arrow) calculation. Using the formula from the method section (half circumference - arc length - corneal radius - 4.0 mm), the fixation point is located 10.0 mm posterior to the corneoscleral limbus in this case (axial length: 26.5 mm). |
Comparison of Preoperative and Postoperative Localization in RRD Cases
From November 2023 to December 2024, data were collected from 43 patients (26 males, 17 females; mean age 49 years) at The 988th Hospital. Retinal reattachment was achieved in 42 patients (97.7%), with one requiring repositioning. Break locations varied: superior temporal (15), inferior temporal (8), temporal (7), superior nasal (5), superior central (2), inferior central (2), superior temporal (1), inferior temporal (1), inferior nasal (1), and one undetected. Postoperative fundus examination confirmed appropriate FCB ridge positioning in all cases. In 41 patients (95.3%), the break was located directly on the buckle ridge apex; in the remaining 2 patients (4.7%), the break was on the anterior slope—a minor deviation from intended placement.
Analysis of these two cases revealed axial lengths exceeding 28.0 mm (28.3 mm and 29.1 mm, respectively), suggesting that extreme axial elongation may introduce slight inaccuracies in the spherical model. Despite this deviation, both cases achieved successful reattachment, as the 5×5 mm effective indentation area sufficiently covered and tamponaded the break. The overall anatomical success rate of 97.7% demonstrates that even with minor variations in break positioning, the FCB’s indentation range provides a clinically acceptable margin of error.
Visual acuity improved significantly following FCB implantation. Preoperative visual acuity ranged from hand motion to 0.8 (median: 0.10); postoperatively, it improved to a median of 0.40 (range: counting fingers to 1.0). The Wilcoxon signed-rank test confirmed a highly significant improvement (Z = 5.43, p < 0.001). Among 43 patients, 38 (88.4%) demonstrated improved vision, 5 (11.6%) showed no change, and none deteriorated.
IOP showed a statistically significant but clinically mild increase postoperatively. Mean preoperative IOP was 12.6 ± 2.7 mmHg (range: 8–18 mmHg); mean postoperative IOP was 14.7 ± 1.6 mmHg (range: 11–18 mmHg). The mean increase was 2.1 mmHg (95% CI: 1.4–2.8 mmHg). The paired t-test revealed statistical significance (t = 5.12, df = 42, p < 0.001). All postoperative IOP values remained within the normal range (10–21 mmHg), indicating that the mild elevation is clinically acceptable and likely related to the scleral indentation effect of the FCB rather than any pathological process.
Two representative cases were selected to verify the calculation results:
Case 1: As illustrated in Figure 7A, a 53-year-old male presented with a large superior temporal retinal tear in the left eye (white arrow). Preoperative axial length was 23.93 mm, and optic disc horizontal diameter was 1.5 mm. The fundus photograph was imported into a smartphone, and the optic disc was enlarged to approximately 5 mm (Figure 7B). The chord length from the break’s anterior edge to the macula fovea was measured as 40.0 mm (Figure 7C). The actual chord length was calculated as 40.0 mm × (1.5/5.0) = 12.0 mm. From Table 2, a chord length of 12.0 mm corresponds to an arc length of 13.5 mm. With an axial length of 24.0 mm, Table 3 gives a half circumference of 37.0 mm. The FCB fixation point was calculated as: 37.0 mm − 13.5 mm − 6.0 mm − 4.0 mm = 13.5 mm posterior to the corneoscleral limbus. Postoperative fundus photography (Figure 7D) confirmed a dome-shaped elevation at the site, indicating successful FCB compression.
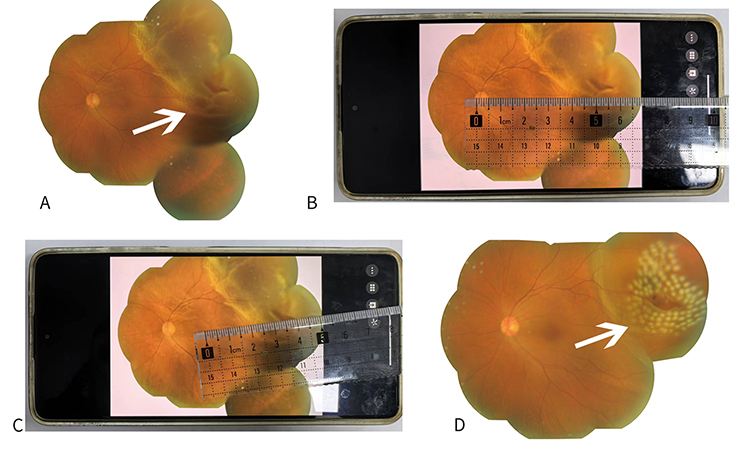 |
Figure 7 Typical Case 1. (A) Preoperative fundus photograph of left eye showing large superior temporal retinal tear (white arrow). (B) Fundus photograph imported into smartphone with optic disc enlarged to approximately 5 mm. (C) Chord length measurement from break anterior edge to macula fovea (40.0 mm). (D) Postoperative fundus photograph showing rounded bulge at site (white arrow), confirming FCB compression. |
Case 2: As shown in Figure 8A, a 50-year-old male presented with two large superior temporal retinal tears in the left eye (white arrows). Preoperative axial length was 26.35 mm. The optic disc was enlarged to 5 mm (Figure 8B). The chord length from the break’s anterior edge to the macula fovea was measured as 55.0 mm (Figure 8C). The actual chord length was 16.5 mm, corresponding to an arc length of 19.5 mm. The FCB fixation point was calculated as: 40.5 mm − 19.5 mm − 6.0 mm − 4.0 mm = 11.0 mm posterior to the corneoscleral limbus. Postoperative fundus photography (Figure 8D) showed a rounded bulge at the site, confirming successful FCB compression.
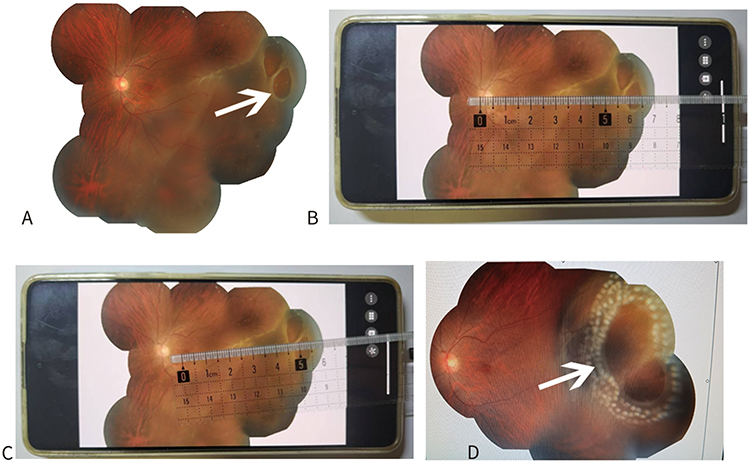 |
Figure 8 Typical Case 2. (A) Preoperative fundus photograph of left eye showing two large superior temporal retinal tears (white arrows). (B) Fundus photograph imported into smartphone with optic disc enlarged to approximately 5 mm. (C) Chord length measurement from break anterior edge to macula fovea (55.0 mm). (D) Postoperative fundus photograph showing rounded bulge at site (white arrow), confirming FCB compression. |
Discussion
Accurate retinal tear localization is fundamental to successful RRD repair. Our 3D reconstruction method addresses the limitations of traditional qualitative techniques by providing a quantitative, standardized protocol. Moreover, our method achieved favorable outcomes in a single-center cohort, laying a solid foundation for broader clinical application of FCB.
Sealing retinal breaks is the cornerstone of RRD treatment; therefore, accurate localization is both crucial and technically challenging. Ishikawa et al13 used ultra-widefield images to calculate the distance between the scleral buckle’s trailing edge and the limbus postoperatively, comparing it with intraoperative measurements. While a regression equation was derived, postoperative calculations cannot accurately estimate changes in ocular shape, and wide-angle image changes are unpredictable Li et al12 addressed this issue, but single imaging cannot cover the entire retina, and the chord length from the ora serrata to the limbus used in their study is based on estimates that may vary individually. Moreover, their data are insufficient for nasal position analysis. Consequently, most commonly used preoperative localization methods—direct and indirect ophthalmoscopy, slit-lamp biomicroscopy with a contact lens, and three-mirror examination15,17–19—remain prevalent. In recent years, ultra-widefield (UWF) cameras20 and Zeiss Clarus 700 imaging21 have been applied clinically to detect tears and estimate their position relative to the limbus. However, these methods lack quantitation, rely on personal experience, and have a steep learning curve. Sun et al22 used preoperative wide-angle fundus photography to locate the clock-hour direction of tears based on the equatorial vortex vein. In their series of 11 eyes undergoing minimally invasive extraocular scleral buckling with FCB, 7 eyes had unsatisfactory retinal attachment postoperatively, with tears failing to adhere to the buckle ridge. In contrast, our 3D reconstruction technique integrates axial length, optic disc metrics, and geometric modeling, reducing interoperator variability and enabling precise preoperative planning for tear localization and FCB implantation. Specifically, we directly measured the distance from the macula fovea to the tear’s anterior edge using a ruler, calculated chord length, and applied 3D reconstruction—a simple, economical, and widely applicable approach.
The significant visual improvement observed in our cohort further validates the clinical effectiveness of our approach. Median visual acuity increased from 0.10 preoperatively to 0.40 postoperatively, with 88.4% of patients improving and none deteriorating. This functional outcome aligns with the high anatomical success rate (97.7%), confirming that accurate preoperative tear localization translates into meaningful visual recovery. The mild but statistically significant IOP increase (mean 2.1 mmHg) is consistent with the expected mechanical effect of scleral indentation created by FCB. Crucially, all postoperative IOP values remained within the normal range, and no patient required intervention for elevated IOP, underscoring the procedure’s safety profile and suggesting that FCB indentation does not induce pathological ocular hypertension.
Because the FCB provides a 5×5 mm indentation area, it creates a smoother, broader, and more effective indentation ridge. Compared with conventional buckling materials such as silicone tires and sponges, FCB can manage cases relatively challenging for standard episcleral procedures. In some patients who would otherwise meet the indications for PPV, this technique allows conversion back to traditional external surgery without disrupting the intraocular microenvironment. Given its minimal intraoperative trauma, absence of extraocular muscle traction, and no requirement for retrobulbar anesthesia, it is particularly suitable for: (1) children, young adults, and pregnant women; (2) high myopia; (3) inferior tears; (4) nasal tears; and (5) horseshoe tears. Postoperative results showed that the FCB indentation area was correctly positioned, the retina reattached, and vision well restored, indicating the feasibility of our localization approach.
Tear drift and individual differences in optic disc horizontal diameter are key concerns. When a retinal tear occurs, liquefied vitreous may pass into the subretinal space, and the tear position may shift due to factors such as eye movements, vitreous traction, or IOP changes. Therefore, although preoperative calculations provide a reliable reference, surgeons should anticipate potential intraoperative positional changes.
Studies have shown that optic disc morphology varies greatly and is influenced by race, gender, age, and refractive status.23–25 The horizontal diameter of the optic disc can serve as an important reference scale for break localization, but individual differences may affect accuracy. Specifically, differences in optic disc diameter can affect judgment of the relative position of retinal lesions and assessment of the peripheral retinal area; a larger diameter may make peripheral retina observation difficult, while a smaller diameter may make it more visible, both of which can influence localization accuracy.
The accuracy of any preoperative localization method must be evaluated in the context of its clinical tolerance for error. In our series, 95.3% achieved precise break placement on the buckle ridge apex, while 4.7% had minor deviations (anterior slope placement). These deviations did not compromise surgical success, as both affected eyes achieved reattachment. This underscores that the FCB’s 5×5 mm indentation area provides a clinically acceptable margin of error.
This study has several limitations. First, many RRD patients have axial lengths exceeding 30 mm or present with posterior staphylomas, and some are pseudophakic, all of which may deviate from the spherical model. Second, the method relies on direct ruler measurement, which lacks precision and may be affected by image distortion when enlarging fundus photographs. Third, the study did not dynamically account for intraoperative tear drift due to scleral depression or vitreous traction; surgeons should anticipate such changes. Finally, the sample size was relatively small, and larger prospective studies are needed to validate the method. Future studies may integrate multimodal imaging and artificial intelligence–assisted analysis to further improve localization accuracy and dynamically account for anatomical variability.
Conclusion
A simple, ruler-based method enables accurate preoperative tear localization and FCB fixation point calculation, providing a practical and effective solution for surgeons performing extraocular buckling procedures.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by The 988th Hospital of Joint Logistics Support Forces of the People’s Liberation Army, the Natural Science Foundation of Henan Province (No. 202300420066), the Scheme of Guangzhou for Leading Talents in Innovation and Entrepreneurship (No. 2020004), Science and Technology Projects in Key Areas of Nansha District (No. 2022ZD009), and Research on Timely Assessment and Treatment of Traumatic Optic Neuropathy (No. YNZX2024008).
Disclosure
Qianying Gao is affiliated with the Vesber Vitreous Institute, it is the inventor of both the three-dimensional reconstruction method and the FCB product. The authors report no other conflicts of interest in this work.
References
1. García-Arumí J, Martínez-Castillo V, Boixadera A, et al. Rhegmatogenous retinal detachment treatment guidelines. Arch Soc Esp Oftalmol. 2013;88(1):11–12. doi:10.1016/j.oftal.2011.10.013
2. Feltgen N, Walter P. Rhegmatogenous retinal detachment—an ophthalmologic emergency. Dtsch Arztebl Int. 2014;111(1–2):12–21. doi:10.3238/arztebl.2014.0012
3. Schick T, Heimann H, Schaub F. Netzhautablösung—Teil 1 [Retinal detachment part 1: epidemiology, risk factors, clinical characteristics, diagnostic approach]. Klin Monbl Augenheilkd. 2020;237(12):1479–1491. doi:10.1055/a-1243-1363
4. Li C, Zhang B, Tan X, et al. A pilot clinical study of complex rhegmatogenous retinal detachment treatment via foldable capsular buckle scleral buckling. BMC Ophthalmol. 2023;23(1):196. doi:10.1186/s12886-023-02913-5
5. Kreissig I. Primary retinal detachment: a review of the development of techniques for repair in the past 80 years. Taiwan J Ophthalmol. 2016;6(4):161–169. doi:10.1016/j.tjo.2016.04.006
6. Neuhaus C, Valmaggia C. Postoperative results in the treatment of retinal detachment with scleral buckling surgery. Klin Monbl Augenheilkd. 2023;240(4):481–485. doi:10.1055/a-2040-3598
7. Bishop PN, Holmes DF, Kadler KE, McLeod D, Bos KJ. Age-related changes on the surface of vitreous collagen fibrils. Invest Ophthalmol Vis Sci. 2004;45(4):1041–1046. doi:10.1167/iovs.03-1017
8. Lincoff H, Kreissig I. Extraocular repeat surgery of retinal detachment: a minimal approach. Ophthalmology. 1996;103(10):1586–1592. doi:10.1016/S0161-6420(96)30459-4
9. Tillery WV, Lucier AC. Round atrophic holes in lattice degeneration—an important cause of phakic retinal detachment. Trans Sect Ophthalmol Am Acad Ophthalmol Otolaryngol. 1976;81(3 Pt 1):509–518.
10. Wang A, Snead MP. Scleral buckling—a brief historical overview and current indications. Graefes Arch Clin Exp Ophthalmol. 2020;258(3):467–478. doi:10.1007/s00417-019-04562-1
11. Nichani PAH, Dhoot AS, Popovic MM, et al. Scleral buckling alone or in combination with pars plana vitrectomy for rhegmatogenous retinal detachment repair: a meta-analysis of 7212 eyes. Ophthalmologica. 2022;245(4):296–314. doi:10.1159/000524888
12. Li D, Zhou N, Gao R, Duan J, Shang Q. Preoperative estimation of retinal hole location using ultra-wide-field imaging. Ann Med. 2023;55(2):2258790. doi:10.1080/07853890.2023.2258790
13. Ishikawa K, Kohno RI, Hasegawa E, et al. Preoperative estimation of distance between retinal break and limbus with wide-field fundus imaging: potential clinical utility for conventional scleral buckling. PLoS One. 2019;14(2):e0212284. doi:10.1371/journal.pone.0212284
14. Zhang B, Li C, Jia Y, et al. A pilot clinical study of treating rhegmatogenous retinal detachment by silicone rubber balloon scleral buckling. Retina. 2020;40(10):1918–1928. doi:10.1097/IAE.0000000000002685
15. Fan FF, Xiao C, Wang L, et al. Efficacy of scleral buckling for the treatment of rhegmatogenous retinal detachment using a novel foldable capsular buckle. Int J Ophthalmol. 2024;17(3):558–563. doi:10.18240/ijo.2024.03.19
16. Long C, Gao Q, Liu S, et al. Precise prediction of size of a foldable capsular vitreous body via computerized three-dimensional ocular reconstruction in severe retinal detachment. BMC Ophthalmol. 2024;24(1):412. doi:10.1186/s12886-024-03646-9
17. Zhong LX, Du Y, Liu W, Huang SY, Zhang SC. Using surgical microscope for sclera buckling and transscleral cryopexy: an alternative procedure of treatment for rhegmatogenous retinal detachment. Biomed Res Int. 2014;2014:364961. doi:10.1155/2014/364961
18. Tomita Y, Kurihara T, Uchida A, et al. Wide-angle viewing system versus conventional indirect ophthalmoscopy for scleral buckling. Sci Rep. 2015;5:13256. doi:10.1038/srep13256
19. Chalam KV, Brar VS, Agarwal S. Direct image-creating aspheric lens for indirect ophthalmoscopy. Ophthalmic Res. 2008;40(2):94–97. doi:10.1159/000113887
20. Ludwig CA, Moon J, Garg I, Miller JB. Ultrawidefield imaging for evaluation of the myopic eye. Semin Ophthalmol. 2021;36:185–190. doi:10.1080/08820538.2021.1887904
21. Karatepe Hashas AS, Popovic Z, Abu-Ishkheidem E, et al. A new diagnostic method for retinal breaks in patients with posterior vitreous detachment: ultra-wide-field imaging with the Zeiss Clarus 700. Acta Ophthalmol. 2023;101:627–635. doi:10.1111/aos.15652
22. Sun XY, Chen TX, Li R, Sun W, Dong FT. Clinical study of rhegmatogenous retinal detachment treatment with minimally invasive foldable capsular buckle scleral buckling. Guoji Yanke Zazhi. 2024;24(2):277–283.
23. Marsh BC, Cantor LB, Wudunn D, et al. Optic nerve head topographic analysis by Stratus OCT in normal subjects: correlation to disc size, age, and ethnicity. J Glaucoma. 2010;19(5):310–318. doi:10.1097/IJG.0b013e3181b6e5cd
24. Addis V, Chen M, Zorger R, et al. A precise method to evaluate 360-degree measures of optic cup and disc morphology in an African American cohort and its genetic applications. Genes. 2021;12:1961. doi:10.3390/genes12121961
25. Lin Q, Jia Y, Li T, et al. Optic disc morphology and peripapillary atrophic changes in diabetic children and adults without diabetic retinopathy or visual impairment. Acta Ophthalmol. 2022;100:e157–e166. doi:10.1111/aos.14885
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.