Back to Journals » Clinical Interventions in Aging » Volume 18
Three-Dimensional Hounsfield Units Measurement of Pedicle Screw Trajectory for Predicating Screw Loosening in Lumbar Fusion Surgery
Authors Zhao H, Wang Y, Wang R, Liu D, Duan Y, Liu Y, Zeng Y, Zhao Q, Zhang Z
Received 22 October 2022
Accepted for publication 22 March 2023
Published 27 March 2023 Volume 2023:18 Pages 485—493
DOI https://doi.org/10.2147/CIA.S389059
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
He Zhao,1,* Yan-jun Wang,1,* Rui-guo Wang,2 Da Liu,3 Ya-qing Duan,4 Yang-jin Liu,1 Yu-hong Zeng,5 Qin-peng Zhao,2 Zheng-ping Zhang2
1Department of Emergency Medicine, Honghui Hospital, Xi’an Jiaotong University, Xi’an, Shaanxi, 710054, People’s Republic of China; 2Department of Spine Surgery, Honghui Hospital, Xi’an Jiaotong University, Xi’an, Shaanxi, 710054, People’s Republic of China; 3Department of Orthopaedics, General Hospital of Western Theatre Command of PLA, Chengdu, Sichuan, 610083, People’s Republic of China; 4Department of Imaging, Honghui Hospital, Xi’an Jiaotong University, Xi’an, Shaanxi, 710054, People’s Republic of China; 5Department of Osteoporosis, Honghui Hospital, Xi’an Jiaotong University, Xi’an, Shaanxi, 710054, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zheng-ping Zhang, Department of Spine Surgery, Honghui Hospital, Xi’an Jiaotong University, No. 76 Nanguo Road, Xi’an, Shaanxi, 710054, People’s Republic of China, Tel +86 17791674069, Email [email protected]
Purpose: Dual-energy X-ray absorptiometry (DXA) is commonly used for evaluation of bone mineral density before spinal surgery, but frequently leads to overestimation in degenerative spinal diseases due to osteoproliferation factors. We introduce a novel method to compare the predictive ability of Hounsfield Units (HU) and DXA methods to predict screw loosening after lumbar interbody fusion surgery in degenerative spinal diseases by measuring HU of pedicle screw trajectory on computed tomography (CT) images preoperatively.
Patients and Methods: This retrospective study was conducted on patients who underwent posterior lumbar fusion surgery for degenerative diseases. CT HUs measurement was performed using medical imaging software, including the cancellous region on cross-sections of the vertebral body and three-dimensional pedicle screw trajectory. Receiver operating characteristic (ROC) curve analyses were performed for the risk of pedicle screw loosening in association with the Hounsfield scale and preoperative BMD, and the area under the curve (AUC) and the cutoff values were calculated.
Results: A total of 90 patients were enrolled and were divided into loosening (n = 33, 36.7%) and non-loosening groups (n = 57, 63.3%). No significant differences in age, gender, length of fixation and preoperative BMD were found between both groups. The loosening group showed lower CT HU values in the vertebral body and screw trajectory than the non-loosening group. Screw trajectory HU (ST-HU) exhibited a higher AUC value than vertebral body HU (B-HU). The cutoff values of B-HU and ST-HU were 160 and 110 HUs, respectively.
Conclusion: Three-dimensional pedicle screw trajectory HU values yields a stronger predictive value than vertebral body HU values and BMD and may provide more guidance for surgery. The risk of screw loosening is significantly increased at ST-HU < 110 or B-HU < 160 at L5 segment.
Keywords: osteoporosis, degenerative spinal disease, fixation failure, imaging observation
Introduction
Osteoporosis is widely acknowledged as a significant risk factor for screw loosening after spinal surgery,1–3 closely related to gender, age and fixation length. Dual-energy X-ray absorptiometry (DXA) is the gold standard for preoperatively evaluating the degree of osteoporosis via bone mineral density (BMD) scores.3 Preventive techniques against osteoporosis are nowadays available, such as pedicle screw bone cement augmentation.2 However, BMD is frequently overestimated in degenerative spinal diseases due to osteoproliferation factors, causing false negatives.3–5
Computed tomography (CT) assessment of bone quality has been reported in recent years, including Hounsfield units (HU) measurement and quantitative-CT (QCT).3,6,7 HU measures the attenuation of tissue and can focus on evaluating cancellous bone by region of interest (ROI) and thus avoid the interference of degenerative bone cortex,3 while QCT exhibits high precision but poor clinical feasibility.8 Previous studies have reported a fine correlation between HU and BMD values,3,5,7 while several have demonstrated the ability of the Hounsfield scale to predict screw loosening after spine surgery.5,9
Most studies that have assessed the Hounsfield scale in spine CT have focused on the measurement of cross-sectional cancellous bone within the vertebral bodies and pedicles,3–5,9 with no studies conducted from a three-dimensional perspective. In this study, we introduce a novel method using MIMICS software to compare the predictive ability of CT HUs and DXA methods to predict screw loosening after lumbar interbody fusion surgery in degenerative spinal diseases based on reconstruction computed tomography imaging. We hypothesized that three-dimensional pedicle screw trajectory HUs has greater predictive ability for postoperative screw loosening.
Materials and Methods
Demographic Data
This retrospective study was conducted on patients who underwent posterior lumbar fusion surgery for degenerative diseases between July 2018 and August 2019. Informed consent was obtained from the patients, and this study was performed in accordance with the Code of Ethics of the World Medical Association (Declaration of Helsinki) and was reviewed and approved by the Ethics Committee of Honghui Hospital Affiliated with Xi’an Jiaotong University (20220102).
All patients enrolled in this study met the following criteria: (1) degenerative lumbar diseases including lumbar disc herniation, degenerative lumbar spinal stenosis, degenerative lumbar spondylolisthesis and scoliosis; (2) age ≥45 years; (3) adequate imaging data, including CT within 3 months preoperatively in archiving database; (4) complete medical information available. (5) follow-up for at least 6 months. The exclusion criteria were as follows: (1) wrong screw path or screw cement augmentation in surgery; (2) previous history of lumbar surgery; (3) activity limitation before or after the surgery; (4) presence of systemic metabolic disease, long-term glucocorticoid use and malignancies of the osteoarticular system; (5) incomplete medical information. All surgeries were planned and performed by spine specialist team. Demographic characteristics, including age, gender, diagnosis, surgical segment and preoperative BMD scores, were obtained from the Hospital Information System for further analyses.
Screw Assessment
The patients were followed up postoperatively; imaging examinations were conducted, and clinical outcomes were assessed. X-ray and CT scans were used to evaluate the presence of screw loosening, defined as a radiolucent area (≥1mm in this study) around any screw.9–11 A senior spine surgeon and a radiologist evaluated the images independently. At the end of the follow-up, patients were categorized into loosening and non-loosening groups.
Bone Quality Evaluation
DXA examination (Hologic Discovery model A densitometers, Hologic, Inc., Bedford, MA, USA) before the surgery was conducted with standard flow including lumbar spine (L1 to L4 vertebrae), BMD values were recorded as T-scores.
L5 vertebrae were selected for HUs measurement in every patient. Data in DICOM (Digital Imaging and Communications in Medicine) standard from preoperative lumbar CT (SOMATOM Sensation 64 slice scanner, Siemens Medical Solutions, Forchheim, Germany) were reconstructed using MIMICS (version 21.0, Materialise Medical Co, Leuven, Belgium). An axial image at the mid-height level of the L5 vertebra was chosen for the vertebral body measurement, and the ROI was delineated by an oval, including more trabecular bone, while cortical bone and basivertebral foramen were avoided (Figure 1). The ROI of tridimensional pedicle screw trajectory was delineated as a cylinder adapted to screw trajectory (including articular processes, pedicle and vertebral body) and to avoid cortical bone (Figure 1). A senior spine surgeon and a radiology physician evaluated the parameters independently. The vertebral body HU values were recorded as B-HU, while the average of both sides screw trajectory HU values were recorded as ST-HU. Pathological changes like hemangioma or dysosteogenesis were excluded. The intraclass correlation coefficient (ICC) was performed using a two-way random effects model with an absolute agreement and an average measure (κ = 2), in order to ensure consistency.
 |
Figure 1 The methods of selecting ROIs and measuring HU values of vertebral body and screw trajectory. (A-C) Cylinder ROI of screw trajectory in sagittal, axial position; (D) Oral ROI of vertebral body which excluded the basivertebral foramen. |
Statistical Analysis
All statistical analyses were performed using SPSS (version 21.0, IBM Corp., Armonk, NY, USA). HU values were calculated automatically as mean ± standard deviation. The Shapiro–Wilk test was used to evaluate the distribution of quantitative variables; normally distributed variables were described as mean ± standard deviation and analyzed using the t-test. Spearman correlation analyses were performed between B-HU, ST-HU and preoperative BMD. Receiver operating characteristic (ROC) curve analyses were performed for potential pedicle screw loosening risk in association with HU measurements and preoperative BMD, and the area under the curve (AUC) was calculated. The Youden Index was used to obtain the optimal cutoff value. Statistical significance was set at P < 0.05.
Results
Demographics
A total of 90 patients were enrolled in this study (Figure 2) and were divided into loosening (n = 33) and non-loosening (n = 57) groups. The loosening rate was 36.7% (33/90) in degenerative lumbar disease patients with posterior fusion surgery. There were no significant differences between the two groups (P > 0.05) in age, gender, length of fixation, and preoperative BMD (Table 1). Among patients with postoperative screw loosening, S1 was the most common site (n=23/33, 63.9%), followed by L5 (n=9/36, 25%) and L1 and L4 vertebrae (n=2/36, 5.6%).
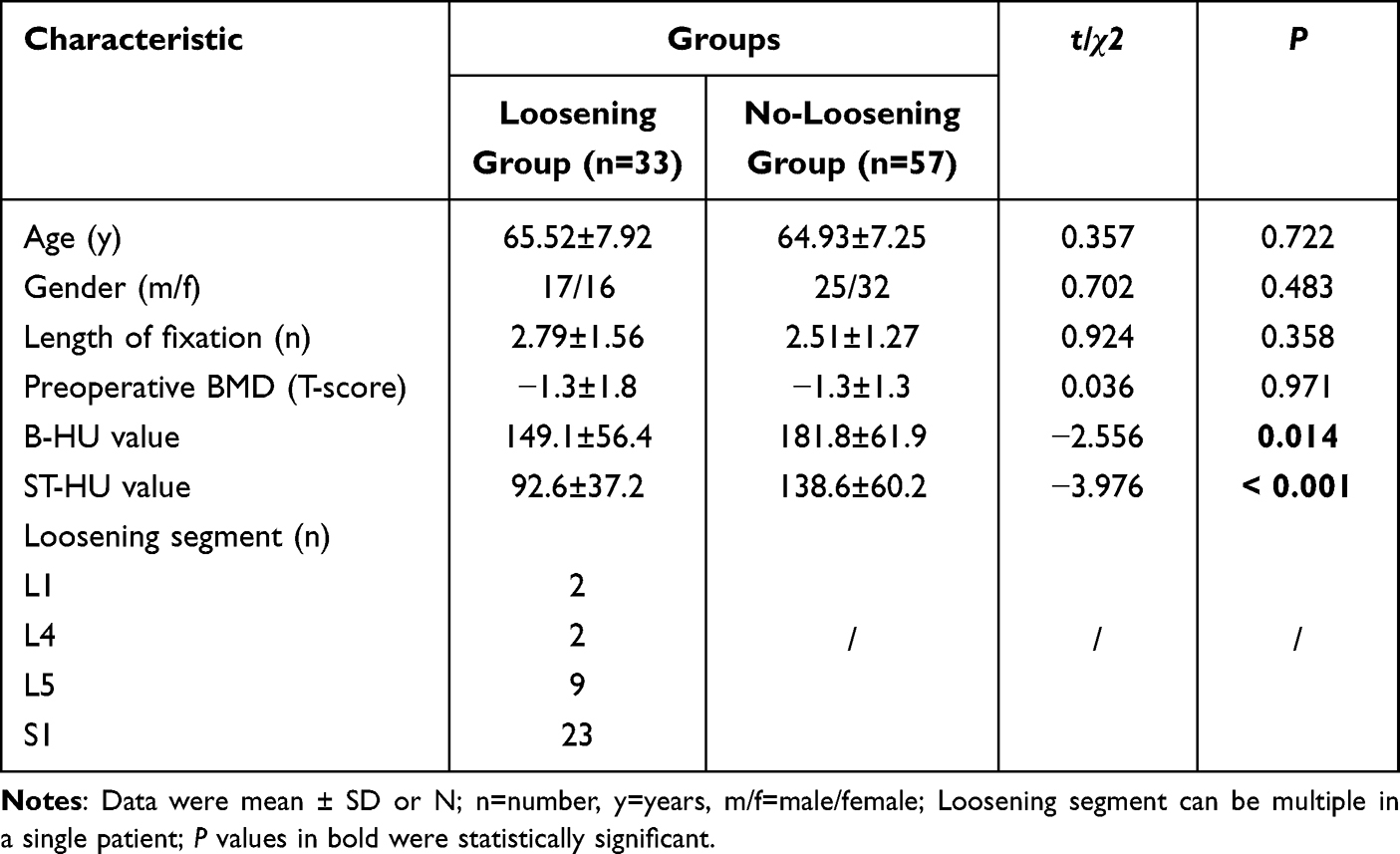 |
Table 1 Demographic Characteristics |
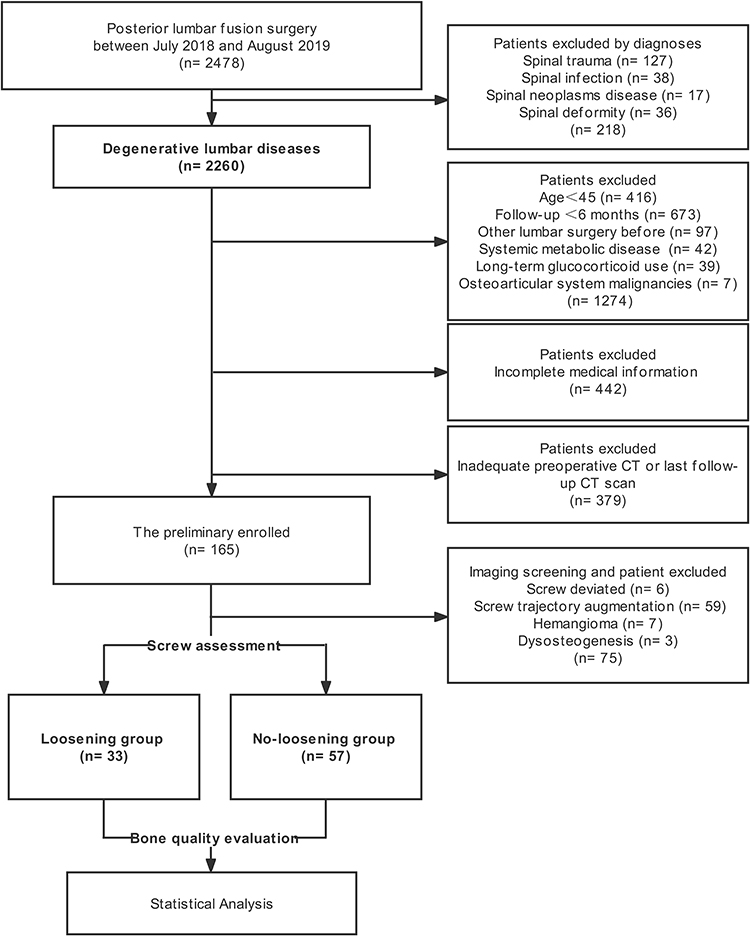 |
Figure 2 Flow diagram of participant screening, exclusion, grouping and measurement. |
HU Values Measurement
Excellent interobserver agreements were demonstrated for all measurements, substantiating the accuracy of our method (Figure 1). ICCs ranged from 0.878 to 0.923, including B-HUs (0.878; 95% CI 0.781, 0.913), Right-ST-HU (0.908; 95% CI 0.792, 0.954) and Left-ST-HU (0.923; 95% CI 0.826, 0.972). The B-HUs were 149.1±56.4 in the loosening group and 181.8±61.9 in the non-loosening group, while the average of ST-HUs were 92.6±37.2 and 138.6±60.2, respectively. The loosening group yielded significantly lower CT HU values in the vertebral body and screw trajectory than the non-loosening group (P < 0.05).
Additionally, correlation analyses among preoperative BMD, B-HU and ST-HU were performed, and all analyses showed significant correlations (P < 0.05) (Figure 3). Preoperative BMD exhibited a weak correlation with B-HU (r = 0.396) and ST-HU (r = 0.465), respectively, while B-HU and ST-HU yielded a satisfactory correlation (r = 0.796).
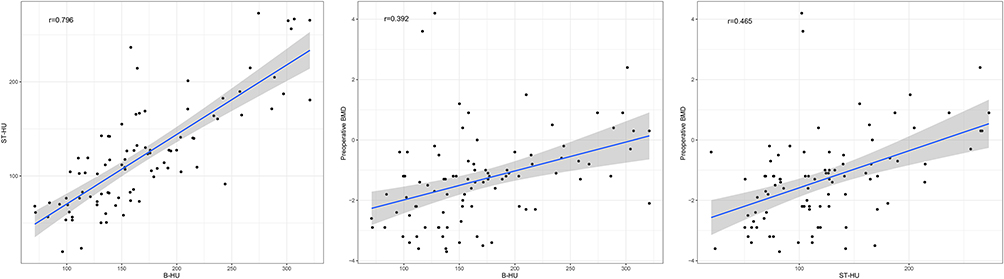 |
Figure 3 Correlation analyses among preoperative BMD, B-HU and ST-HU. |
ROC Curve Analyses
We performed ROC analyses to evaluate the predictive performance of CT HU values and preoperative BMD measurement for potential pedicle screw loosening risk (Table 2). ST-HU yielded a higher AUC value than B-HU, suggesting a better predictive yield (Figure 4), and both showed significant values in predicting screw loosening (P < 0.05). In contrast, preoperative BMD was not statistically significant during ROC analysis (P > 0.05).
 |
Table 2 ROC Analysis of CT HU Values of Vertebral Body and Screw Trajectory and Preoperative BMD in Predicting Screw Loosening |
 |
Figure 4 Receiver operating characteristic curve analyses among preoperative BMD, B-HU and ST-HU. |
To identify the risk of screw loosening, we calculated the cutoff values of B-HU and ST-HU (Table 2). At B-HU values of 160, the sensitivity and specificity rates were 72.7% and 56.1%, respectively. Meanwhile, at a cutoff value of 110 HU for ST-HU, a sensitivity of 78.8% and a specificity of 75.4% were obtained. Lower preoperative CT HU values indicated a high likelihood of postoperative screw loosening in this study.
Discussion
This study documents a novel approach for predicting osteoporotic screw loosening risk before spinal surgery by assessment of the radiodensity of three-dimensional screw trajectory using the Hounsfield scale on computed tomography reconstruction imaging. The results demonstrated that screw trajectory HUs (ST-HU), vertebral body HUs (B-HU) and preoperative BMD (T-scores value) were significantly correlated, and screw trajectory HUs showed good predictive performance for screw loosening compared to vertebral body HUs and preoperative BMD.
DXA is the basic evaluation for bone mineral density before orthopedic surgery and is the gold standard for diagnosing osteoporosis. However, its working principle leads to non-negligible biases for degenerative spinal diseases, including aortic calcification, degeneration of the facet joint, osteophyte formation, and sclerosis of the intervertebral disc.3–5 The QCT technique is widely acknowledged for its good performance in diagnosing osteoporosis, but its high costs limit extensive clinical use. During quantification of the Hounsfield unit, the margin of cortical bone and any bony interference can be excluded. Besides, it has the advantages of easy access and low costs. Most studies on vertebral HUs evaluation were based on two-dimensional target measurements using the picture archiving and communication system (PACS). Zaidi et al3 reviewed the utility of HU assessment of bone quality and reported a threshold value of 110 HUs of L1 for osteoporosis. Zou et al5,12 selected an oval ROI in the vertebral body in spinal degeneration patients over 50 years and compared L1-L4 HU values to the BMD score. They found that preoperative lumbar HUs measurement had an advantage over BMD in osteoporosis prediction and was an independent factor in predicting screw loosening.
Several studies have focused on pedicle HUs evaluation. Xu9 et al estimated the pedicle and vertebrae HUs of L3 in multilevel fusion surgeries. The ROIs were measured as circles in the narrowest part of the pedicle, including and excluding the cortical bone. The advantages of pedicle HUs for predicting screw stability were supported by AUC values ranging from 0.6 to 0.7, and the optimal cutoff value was 180 HUs. Sakai13 et al suggested that low HUs of the screw trajectory represented a risk factor for screw loosening in single-level interbody fusion. The authors enrolled multiple loosening screws and included a rectangle ROI of screw trajectory (from articular processes forward into the vertebral body) in their measurements to reflect the peri-screw bone quality. Patients with screw loosening exhibited lower preoperative HUs in the rectangle ROI, and the cutoff value was 153.5 in women. To our knowledge, morphological studies have substantiated that pedicle isthmus quality could not be predicted by mineral density from the vertebral body.14 In addition, the distribution of bone mass within the vertebral bodies was different, with similar density at all axial levels of the vertebral body, while pedicles exhibited different bone strength in various locations.15 Therefore, measurement of the vertebral body alone is insufficient to assess the risk of loosening.9 This study harnessed CT reconstruction images to evaluate the cancellous bone quality by 3D-ROI of screw trajectory, which yielded higher predictive ability than 2D measurements. Patients after lumbar fusion surgery were retrospectively assessed and separated into the non-loosening and loosening groups. We corroborated that a significant correlation was found between ST-HU, B-HU and preoperative BMD, and ST-HU had significant value for predicting screw stability preoperatively.
Overall, the screw loosening rate in the present study was 36.7%, higher than reported in the past literature (1–30%).9,12,16–18 Indeed, the risk of screw loosening can be affected by many factors, including the degree of osteoporosis, length of fixation, rigid material, sagittal imbalance, distal fixation segment, and so on.19,20 Preoperative DXA evaluations were conducted routinely in patients with osteoporosis risk in our medical department, and the risk of screw loosening was assessed. No significant difference in preoperative BMD was observed between the two groups, which may be attributed to the non-inclusion of cases with screw augmentation. Therefore, there remains an indistinguishable risk of osteoporotic fixation failure in patients with normal preoperative BMD, which highlights the significance of this study.
Indeed, it should be borne in mind that PACS can only delineate bidimensional ROIs, while MIMICS measures three-dimensional ROIs in stereoscopic space. Investigators can manually select the appropriate cancellous bone and avoid cortical structures, thus reducing the interference due to degeneration factors. Interestingly, we found that ST-HU values were lower than B-HU values, although the pedicle is known to be the strongest part of the vertebrae. This finding may be attributed to the ROI definition, which included parts of the vertebral body, pedicle, and superior articular processes, and avoided the cortical bone area (Figure 1). The HU values of cancellous bone in the lumbar spine exhibited a decreasing trend and measurement of multiple segments was not conducive to inter-individual comparison. Therefore, our study focused on single L5 vertebrae instead of multiple fixation segments to obtain more data. Indeed, further studies with more samples are required.
Methods to predict postoperative screw loosening by CT HUs have been reported in recent years, with AUC values ranging from 0.6 to 0.8,9,21,22 which may be influenced by risk factors, including the length of fixation and distal fixation segments.19,20 To achieve optimal sensitivity and specificity, B-HU and ST-HU cutoff values were determined as 160 HUs and 110 HUs separately in the L5 segment, suggesting the loosening risk was significant when HUs were less than the thresholds regardless of the T-scores. In addition to DXA and QCT, CT HUs provides another approach for preoperative assessment with significant implications for preoperative planning and screw failure assessment. We recommend preoperative evaluation of target screw trajectories before long-segment fusion and revision surgery; precautionary measures may be required even when the BMD scores are normal.
The present study has certain limitations. First, screw loosening can be affected by many factors, especially with long-segment fixation. To obtain adequate samples, different lengths of fusion surgeries were enrolled (ranging from 1 to 8), and further studies with controlled variables might improve the specificity of results. Moreover, 3D-ROI measurements using MIMICS software requiring available preoperative CT DICOM data, leading to inconveniences and learning curve difficulties. Indeed, more clinical imaging studies are warranted to facilitate the application of CT measurement techniques. Besides, clinical symptoms and fusion ratios at the final follow-up were not recorded completely. Accordingly, the correlation between screw loosening on imaging and daily symptom could not be demonstrated. Prospective multifactorial studies are warranted to enhance the assessment of osteoporotic spinal diseases.
Conclusion
Hounsfield unit measurement represents a reproducible and reliable method for predicting screw loosening before lumbar degenerative surgeries. The HU values for pedicle screw trajectory yield stronger predictive performance than vertebral body HU values and BMD and may provide more guidance value for surgery. At ST-HU <110 or B-HU <160 at L5, the risk of screw loosening is more significant.
Acknowledgments
The authors thank all patients enrolled in this study for their consent and contribution.
Funding
This work was supported by Leading Innovative Talent Projects of Xi’an Talent Program (XARC210135), General Projects of Xi’an Health Commission (2021ms06) and Key Research and Development Program of Shaanxi Province (2021SF-238).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Gazzeri R, Panagiotopoulos K, Galarza M, Bolognini A, Callovini G. Minimally invasive spinal fixation in an aging population with osteoporosis: clinical and radiological outcomes and safety of expandable screws versus fenestrated screws augmented with polymethylmethacrylate. Neurosurg Focus. 2020;49(2):E14.
2. Hoppe S, Keel MJB. Pedicle screw augmentation in osteoporotic spine: indications, limitations and technical aspects. Eur J Trauma Em Surg. 2017;43(1):3–8.
3. Zaidi Q, Danisa OA, Cheng W. Measurement techniques and utility of Hounsfield unit values for assessment of bone quality prior to spinal instrumentation: a review of current literature. Spine. 2019;44(4):E239–e244.
4. Choi MK, Kim SM, Lim JK. Diagnostic efficacy of Hounsfield units in spine CT for the assessment of real bone mineral density of degenerative spine: correlation study between T-scores determined by DEXA scan and Hounsfield units from CT. Acta neurochirurgica. 2016;158(7):1421–1427.
5. Zou D, Sun Z, Zhou S, Zhong W, Li W. Hounsfield units value is a better predictor of pedicle screw loosening than the T-score of DXA in patients with lumbar degenerative diseases. Eur Spine J. 2020;29(5):1105–1111.
6. Wichmann JL, Booz C, Wesarg S, et al. Quantitative dual-energy CT for phantomless evaluation of cancellous bone mineral density of the vertebral pedicle: correlation with pedicle screw pull-out strength. Eur Radiol. 2015;25(6):1714–1720.
7. Ahern DP, McDonnell JM, Riffault M, et al. A meta-analysis of the diagnostic accuracy of Hounsfield units on computed topography relative to dual-energy X-ray absorptiometry for the diagnosis of osteoporosis in the spine surgery population. Spine J. 2021;21(10):1738–1749.
8. Löffler MT, Jacob A, Valentinitsch A, et al. Improved prediction of incident vertebral fractures using opportunistic QCT compared to DXA. Eur Radiol. 2019;29(9):4980–4989.
9. Xu F, Zou D, Li W, et al. Hounsfield units of the vertebral body and pedicle as predictors of pedicle screw loosening after degenerative lumbar spine surgery. Neurosurg Focus. 2020;49(2):E10.
10. Spirig JM, Sutter R, Götschi T, Farshad-Amacker NA, Farshad M. Value of standard radiographs, computed tomography, and magnetic resonance imaging of the lumbar spine in detection of intraoperatively confirmed pedicle screw loosening-a prospective clinical trial. Spine J. 2019;19(3):461–468.
11. Wu X, Shi J, Wu J, et al. Pedicle screw loosening: the value of radiological imagings and the identification of risk factors assessed by extraction torque during screw removal surgery. J Orthop Surg Res. 2019;14(1):6.
12. Zou D, Muheremu A, Sun Z, Zhong W, Jiang S, Li W. Computed tomography Hounsfield unit-based prediction of pedicle screw loosening after surgery for degenerative lumbar spine disease. J Neurosurg Spine. 2020;1:1–6.
13. Sakai Y, Takenaka S, Matsuo Y, et al. Hounsfield unit of screw trajectory as a predictor of pedicle screw loosening after single level lumbar interbody fusion. J Orthop Sci. 2018;23(5):734–738.
14. Inceoglu S, Burghardt A, Akbay A, Majumdar S, McLain RF. Trabecular architecture of lumbar vertebral pedicle. Spine. 2005;30(13):1485–1490.
15. Odeh K, Rosinski A, Leasure J, Kondrashov D. Pedicle screws challenged: lumbar cortical density and thickness are greater in the posterior elements than in the pedicles. Global Spine j. 2021;11(1):34–43.
16. Galbusera F, Volkheimer D, Reitmaier S, Berger-Roscher N, Kienle A, Wilke HJ. Pedicle screw loosening: a clinically relevant complication? Eur Spine J. 2015;24(5):1005–1016.
17. Uehara M, Takahashi J, Ikegami S, et al. Pedicle screw loosening after posterior spinal fusion for adolescent idiopathic scoliosis in upper and lower instrumented vertebrae having major perforation. Spine. 2017;42(24):1895–1900.
18. Kim DH, Hwang RW, Lee GH, et al. Comparing rates of early pedicle screw loosening in posterolateral lumbar fusion with and without transforaminal lumbar interbody fusion. Spine J. 2020;20(9):1438–1445.
19. Marie-Hardy L, Pascal-Moussellard H, Barnaba A, Bonaccorsi R, Scemama C. Screw loosening in posterior spine fusion: prevalence and risk factors. Global Spine j. 2020;10(5):598–602.
20. Yuan L, Zhang X, Zeng Y, Chen Z. Incidence, risk, and outcome of pedicle screw loosening in degenerative lumbar scoliosis patients undergoing long-segment fusion. J Neurosurg Spine. 2021;21925682211017477.
21. Pickhardt PJ, Pooler BD, Lauder T, Del Rio AM, Bruce RJ, Binkley N. Opportunistic screening for osteoporosis using abdominal computed tomography scans obtained for other indications. Ann Intern Med. 2013;158(8):588–595.
22. Schwaiger BJ, Gersing AS, Baum T, Noël PB, Zimmer C, Bauer JS. Bone mineral density values derived from routine lumbar spine multidetector row CT predict osteoporotic vertebral fractures and screw loosening. AJNR Am J Neuroradiol. 2014;35(8):1628–1633.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.