Back to Journals » Journal of Asthma and Allergy » Volume 18
Three Biologic-Naïve Patients with Allergic Bronchopulmonary Aspergillosis Showing Significant Clinical Improvement with Tezepelumab
Authors Yamaguchi M ![]() , Yamazaki A, Nakagawa H
, Yamazaki A, Nakagawa H ![]() , Kinose D
, Kinose D ![]() , Nakano Y
, Nakano Y ![]()
Received 27 May 2025
Accepted for publication 21 August 2025
Published 28 August 2025 Volume 2025:18 Pages 1221—1227
DOI https://doi.org/10.2147/JAA.S541770
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Amrita Dosanjh
Masafumi Yamaguchi, Akio Yamazaki, Hiroaki Nakagawa, Daisuke Kinose, Yasutaka Nakano
Division of Respiratory Medicine, Department of Internal Medicine, Shiga University of Medical Science, Otsu, Japan
Correspondence: Masafumi Yamaguchi, Division of Respiratory Medicine, Department of Internal Medicine, Shiga University of Medical Science, Seta Tsukinowa-cho, Otsu, Shiga, 520-2192, Japan, Email [email protected]
Abstract: Allergic bronchopulmonary aspergillosis is characterized by hypersensitivity to Aspergillus spp. and often causes intractable asthma. Studies have been conducted on biologics administered to patients with allergic bronchopulmonary aspergillosis; however, treatment may not always be successful. This may be due to the limitations of the current biologics that selectively target a single cytokine. Tezepelumab, a human monoclonal antibody that blocks the activity of thymic stromal lymphopoietin, broadly suppresses type 2 inflammation by regulating the upstream cascade of airway inflammation. Therefore, it is expected to have favorable effects in patients with allergic bronchopulmonary aspergillosis. We report three cases of allergic bronchopulmonary aspergillosis with uncontrolled symptoms despite the maximal use of conventional anti-asthmatic drugs such as inhalative agents, anti-leukotriene receptor antagonists, and antifungal drugs. None of the patients had previously received biologics. The addition of tezepelumab produced a marked clinical response in all three patients, which included fewer exacerbations and a reduced dosage of oral systemic corticosteroids and/or reduced as-needed short-acting beta-2 agonists. The patients’ pulmonary symptoms were better controlled, peripheral blood eosinophil counts and immunoglobulin E levels decreased, and quality of life scores and respiratory function parameters improved. Mucous plugs accompanied by atelectasis and infiltrative shadows observed on chest computed tomography also improved. Tezepelumab may be a promising treatment option for allergic bronchopulmonary aspergillosis in patients with severe asthma, offering effective symptom control and enabling reduction in systemic corticosteroid use.
Keywords: mucous plug, peripheral blood eosinophilia, severe asthma, type 2 inflammatory biomarker
Introduction
Allergic bronchopulmonary aspergillosis (ABPA) is an allergy-related disease caused by an immune response to Aspergillus spp. It is commonly associated with refractory asthma and pathologically characterized by an increased type 2 immune response.1,2 Chest imaging often reveals bronchiectasis and mucous plugs in the airways, which are sometimes migratory. Systemic corticosteroids, which may be used in conjunction with antifungal agents, are the primary treatment for ABPA. However, owing to concerns regarding the side effects of systemic corticosteroids, biologics have recently been used more aggressively for the treatment of ABPA. Tezepelumab is a monoclonal antibody against thymic stromal lymphopoietin (TSLP), which plays an essential role in the activation of type 2 inflammation through an upstream cascade of innate and acquired immunity. Therefore, tezepelumab is expected to have strong clinical efficacy in controlling a broad spectrum of inflammation in severe asthma, including inflammation related to ABPA.3 Herein, we present three patients with ABPA who had no prior treatment with biologic agents and showed favorable clinical courses, including findings from imaging studies, after undergoing treatment with tezepelumab.
Case Series
Herein, we report three cases of severe asthma complicated by ABPA, which were treated with tezepelumab. All patients demonstrated marked clinical improvement 16 weeks after treatment initiation. All patients were treated consistently at the Division of Respiratory Medicine, Department of Internal Medicine, Shiga University of Medical Science during the study period. As this is a case series consisting of a small number of patients, in accordance with the policy of our institution, approval from the ethics committee was not required for the publication of case details. Written informed consent for the disclosure and publication of details was obtained from all patients. A definite diagnosis of ABPA was made according to a previous report based on the presence of six or more of the following ten criteria:1 (1) Current or previous history of asthma or asthmatic symptoms; (2) peripheral blood eosinophilia (≥500 cells/μL); (3) elevated total serum immunoglobulin E (IgE) levels (≥417 IU/mL); (4) immediate cutaneous hypersensitivity or specific IgE for Aspergillus spp.; (5) presence of precipitins or specific immunoglobulin G (IgG) for Aspergillus spp.; (6) Aspergillus spp. growth in sputum cultures or bronchial lavage fluid; (7) presence of fungal hyphae in the bronchial mucous plugs; (8) central bronchiectasis on computed tomography (CT); (9) presence of mucous plugs in the central bronchi based on CT/bronchoscopy or mucous plug expectoration history; and (10) high-attenuation mucus in the bronchi on CT. None of the patients were smokers or had chronic obstructive pulmonary disease. Adherence to asthma medications and good inhalation techniques was confirmed, and patients with uncontrolled asthma, despite intensive anti-asthmatic therapy, were enrolled. Evaluations to rule out other differential diagnoses included serum anti-neutrophil cytoplasmic antibody (ANCA). Tezepelumab was administered under the supervision of our outpatient clinic, with perfect adherence ensured, as approved by the FDA and the Japanese Ministry of Health, Labour and Welfare for the treatment of severe asthma at the time of administration. Mucous plugs were evaluated by an experienced radiologist. Patients were evaluated every 4 weeks, and improvements in symptoms, quality of life scores, lung function, and peripheral blood eosinophil counts were observed 16 weeks after initiation. Additionally, improvements in findings such as mucous plugs on chest CT were noted 24 weeks after initiation.
Case 1
A 55-year-old Japanese woman with severe bronchial asthma who had been receiving high doses of budesonide/formoterol and montelukast sodium for many years but had no history of biologic agent prescription was referred to our hospital. Tiotropium had been discontinued because the patient experienced dry mouth. Short-acting beta-2 agonists (SABAs) had been frequently used, and short-term systemic corticosteroids were required several times per year for managing symptom exacerbation. The patient’s chief symptoms included viscous sputum, coughing during the Japanese cedar pollen season, and cold air-induced wheezing. A definitive diagnosis of ABPA was determined owing to the existence of bronchial asthma, increased peripheral blood eosinophil counts, elevated total serum IgE levels, positivity for Aspergillus-specific IgE, positivity for precipitin IgG for Aspergillus spp., and the presence of mucous plugs in the central airways on chest CT. Aspergillus spp. was not detected in sputum cultures (Table 1). Itraconazole was discontinued after a short period owing to gastrointestinal symptoms such as nausea and diarrhea. The symptoms improved promptly after tezepelumab treatment initiation. In particular, after 16 weeks of treatment, the amount of sputum decreased, and cold-air-induced wheezing nearly disappeared, leading to no need for SABA, achievement of a full score on the asthma control test (ACT), and improvement of peripheral blood parameters (Figure 1A). Spirometry parameters, including maximal mid-expiratory flow (MMEF), which is thought to reflect peripheral airway lesions, and forced expiratory volume in 1 second (FEV1), also improved (Table 2). After 24 weeks of treatment, CT indicated that the mucous plugs had nearly disappeared and that the associated atelectasis was ameliorated (Figure 2A).
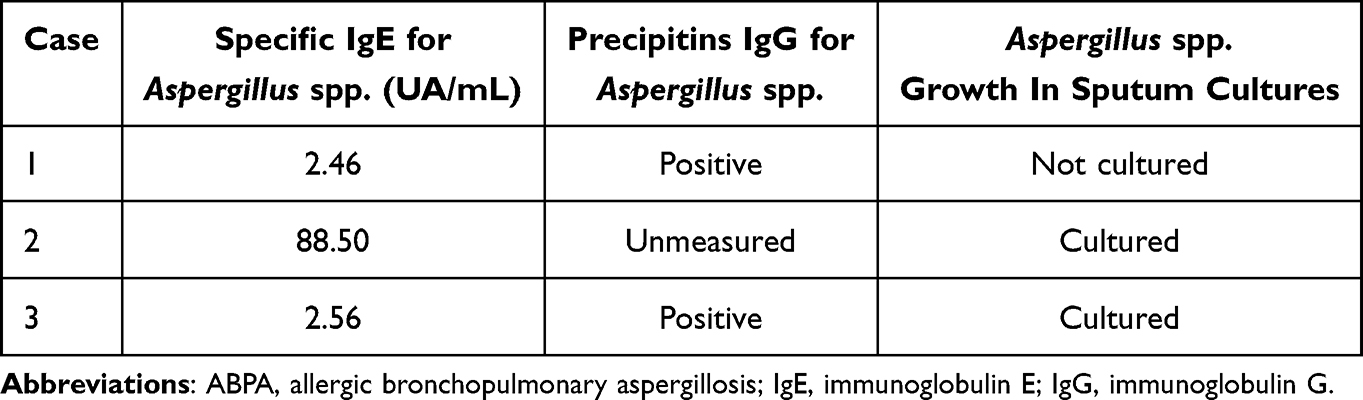 |
Table 1 Serum Markers and Culture Results Related to ABPA Diagnosis Prior to Tezepelumab Treatment in Each Case |
 |
Table 2 Changes in Laboratory and Spirometry Results and ACT Scores Before/16 weeks After Tezepelumab Administration |
 |
Figure 1 Course of asthma control test (ACT) score and peripheral blood eosinophil counts. (A) Case 1: Clinical course of a 55-year-old woman before and 4, 8, 12, and 16 weeks after tezepelumab administration. (B) Case 2: Clinical course of a 63-year-old man before and 4, 8, 12, and 16 weeks after tezepelumab administration. (C) Case 3: Clinical course of a 69-year-old woman before and 4, 8, 12, and 16 weeks after tezepelumab administration. Solid lines represent peripheral blood eosinophil counts, and dashed lines represent ACT scores. |
 |
Figure 2 Computed tomography (CT) of three patients with allergic bronchopulmonary aspergillosis before and after tezepelumab administration. (A) Case 1: Chest CT images of a 55-year-old woman before and 24 weeks after tezepelumab administration. (B) Case 2: Chest CT images of a 63-year-old man before and 24 weeks after tezepelumab administration. (C) Case 3: Chest CT images of a 69-year-old woman before and 24 weeks after tezepelumab administration. Left panel: pre-tezepelumab; right panel: post-tezepelumab. Arrowheads indicate mucous plugs, pulmonary infiltration, or atelectasis. |
Case 2
A 63-year-old Japanese man presented to our hospital with a chief complaint of cough induced by conversation or dust, with associated viscous sputum and wheezing. The patient had been diagnosed with asthma approximately 15 years prior to admission but stopped treatment when he relocated. A definitive diagnosis of ABPA was determined based on the presence of bronchial asthma, peripheral blood eosinophilia, elevated total serum IgE levels, positivity for Aspergillus-specific IgE, positivity for Aspergillus spp. in sputum culture, and central bronchiectasis and mucous plugs in the central airways on CT. No precipitin IgG against Aspergillus spp. was detected (Table 1). High-dose fluticasone furoate/umeclidinium/vilanterol, montelukast sodium, and desloratadine were initiated; however, they were only partially effective. The patient refused itraconazole. Therefore, tezepelumab was added as the first-line biologic agent. Within a few days of the first administration of tezepelumab, the patient showed considerable improvement in symptoms. Viscous sputum was markedly reduced, and coughing and wheezing did not occur even after exposure to triggering agents. The ACT score, various pulmonary function parameters (FEV1 and MMEF), and the fractional concentration of exhaled nitric oxide (FeNO) also improved after 16 weeks of treatment (Table 2 and Figure 1B). Mucous plugs and infiltrative shadows observed on chest CT considerably reduced after 24 weeks of treatment (Figure 2B).
Case 3
A 69-year-old Japanese woman with severe bronchial asthma and a 3-year history of high-dose mometasone furoate/glycopyrronium/indacaterol treatment was referred to our clinic. Another clinic had advised treatment with biologics; however, the patient refused it for financial reasons. The chief complaints were a wet cough induced by cold air or strong odors and nocturnal wheezing. These symptoms were followed by difficulty staying asleep. In addition, short bursts of systemic corticosteroids for asthma exacerbation were required approximately four times per year. The presence of asthma, increased peripheral blood eosinophil count, elevated total serum IgE levels, positivity for Aspergillus-specific IgE, positivity for Aspergillus spp. in sputum culture, positivity for precipitin IgG for Aspergillus spp., and high attenuation mucous plugs in the central airways on CT led to a confirmed diagnosis of ABPA (Table 1). The frequency of exacerbations did not decrease despite the addition of montelukast and itraconazole, and the need for systemic corticosteroids did not change. Therefore, tezepelumab was initiated after communicating with the patient regarding their current respiratory status and the benefits of the recommended treatment. After 16 weeks of treatment, the cough, sputum production, and wheezing improved. The ACT score and pulmonary function test indices also markedly improved (Table 2 and Figure 1C). Chest CT revealed the disappearance of the mucous plugs and corresponding central bronchiectasis after 24 weeks of treatment (Figure 2C).
Discussion
Although systemic corticosteroids have long been the mainstay of ABPA treatment, their side effects often cause significant problems. Biologics are increasingly being administered to enable patients to reduce or discontinue the use of systemic corticosteroids. However, treatment with biologics targeting a single type 2 inflammatory cytokine may not be successful, which sometimes necessitates a change between biologics. For example, reports exist of cases in which omalizumab was ineffective but mepolizumab was effective,4 those in which mepolizumab was ineffective but dupilumab was effective,5 and those in which benralizumab was ineffective but dupilumab was effective;6 however, to the best of our knowledge, no resistance to dupilumab has been reported. There are few reports on tezepelumab, a monoclonal antibody against TSLP, which is secreted primarily from airway epithelial cells and plays an important role in activating type 2 inflammation through the upstream cascade of innate and acquired immunity. This leads to broad and potent inhibition of inflammation in the pathophysiology of ABPA. The efficacy of treatment with this biologic is clear in that the three patients in our study had favorable clinical responses.7
In recent years, mucous plugs have received increasing attention in the pathogenesis of severe asthma and are thought to mainly involve two type 2 cytokines: interleukin (IL)-13 and IL-5.8 Pham et al reported that tezepelumab normalizes serum IL-5 and IL-13 levels in patients with uncontrolled severe asthma.9 Other studies have shown that treatment with anti-IL-5 antibodies does not improve mucous plugs in patients with ABPA, and an alternative biologic must be used.5,6 Tezepelumab significantly reduced the mucous plug size in all three patients in the current study. This is likely due to its biological activity as an antibody against TSLP, which is located upstream of the airway inflammatory cascade and regulates a wide range of type 2 airway inflammatory cytokines, including IL-13 and IL-5.
In addition, spirometry parameters, including FEV1 and MMEF, thought to reflect small airway dysfunction, significantly improved in all patients in this study, which may be due to the improvement of mucous plugs along with the direct anti-inflammatory effects of tezepelumab. Furthermore, all three patients showed improvement in symptoms such as cold-air-induced wheezing/coughing or wheezing/coughing associated with strong odors or conversation. The decrease in these symptoms suggests a clinical improvement in airway hyperresponsiveness. Several mechanisms may explain these findings. First, previous reports have suggested that both peripheral blood eosinophil counts and FeNO levels should be controlled to improve airway hyperresponsiveness.10 In the cases included in this study, improvements in both parameters were observed, consistent with the findings of a clinical trial.11 Second, TSLP loading has been shown to impair airway epithelial integrity and barrier function, and tezepelumab administration may restore these functions.12 Third, human airway smooth muscle cells loaded with TSLP have been reported to exhibit an enhanced Ca2+ response to histamine, which is inhibited by anti-TSLP antibodies.13
In contrast, type 2 inflammatory biomarkers, specifically FeNO, peripheral blood, and eosinophil count, improved in all three patients after 16 weeks of tezepelumab administration. Total IgE levels improved in two cases; in Case 1, the total IgE levels were lower than expected, likely because the patient had taken oral systemic prednisolone 20 mg daily for several days owing to symptom deterioration immediately prior to tezepelumab administration. In fact, the data from several months before showed that the patient’s total IgE level was over 700 IU/mL, and the peripheral blood eosinophil count was also over 1000 cells/μL. Therefore, we believe that the total IgE levels improved in a manner similar to that observed in other patients. These results are generally consistent with the findings of a clinical trial on tezepelumab in patients with severe asthma.11 A previous report suggested that the targeted improvement in total IgE levels in ABPA is a 25–50% reduction;14 however, another report indicated that a reduction in total IgE levels does not necessarily correlate with clinical improvement,15 leaving room for further discussion. However, in the three cases presented herein, clinical improvement was evident. Therefore, we consider tezepelumab to have significant clinical value.
In this study, we presented three cases in which tezepelumab demonstrated favorable efficacy. However, further clinical trials involving a larger number of patients are required before these results can be generalized.
Conclusion
In conclusion, tezepelumab can be considered as an effective treatment option for ABPA. The successful treatment of three patients with ABPA using tezepelumab demonstrates the importance of broadly controlling type 2 airway inflammation, particularly in the pathology of ABPA involving mucous plug formation.
Abbreviations
ABPA, allergic bronchopulmonary aspergillosis; ACT, asthma control test; ANCA, anti-neutrophil cytoplasmic antibody, CT, computed tomography; IgE, immunoglobulin E; IgG, immunoglobulin G; IL, interleukin; FeNO, fractional concentration of exhaled nitric oxide; FEV1, forced expiratory volume in 1 second; MMEF, maximal mid-expiratory flow; SABA, short-acting beta-2 agonists; TSLP, thymic stromal lymphopoietin.
Acknowledgment
We would like to thank Editage (www.editage.jp) for English language editing.
Disclosure
M.Y. receives lecture fees from AstraZeneca, GlaxoSmithKline, Sanofi, and Kyorin. H.N. receives lecture fees from Boehringer Ingelheim. Y.N. receives lecture fees from AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, and Teijin Pharma. The authors declare no other conflicts of interest in this work.
References
1. Asano K, Hebisawa A, Ishiguro T, et al. New clinical diagnostic criteria for allergic bronchopulmonary aspergillosis/mycosis and its validation. J Allergy Clin Immunol. 2021;147(4):1261–1268.e5. doi:10.1016/j.jaci.2020.08.029
2. Roboubi A, Audousset C, Fréalle É, et al. Allergic bronchopulmonary aspergillosis: a multidisciplinary review. J Mycol Med. 2023;33(3):101392. doi:10.1016/j.mycmed.2023.101392
3. Parnes JR, Molfino NA, Colice G, Martin U, Corren J, Menzies-Gow A. Targeting TSLP in asthma. J Asthma Allergy. 2022;15:749–765. doi:10.2147/JAA.S275039
4. Hirota S, Kobayashi Y, Ishiguro T, et al. Allergic bronchopulmonary aspergillosis successfully treated with mepolizumab: case report and review of the literature. Respir Med Case Rep. 2018;26:59–62. doi:10.1016/j.rmcr.2018.11.013
5. Kawasaki Y, Nishiki K, Ishizaki T. Successful treatment with dupilumab in mepolizumab-resistant allergic bronchopulmonary aspergillosis. Respir Med Case Rep. 2024;47:101964. doi:10.1016/j.rmcr.2023.101964
6. Kotetsu Y, Ogata H, Sha K, Moriwaki A, Yoshida M. A case of allergic bronchopulmonary aspergillosis with failure of benralizumab and response to dupilumab. Cureus. 2023;15(7):e42464. doi:10.7759/cureus.42464
7. Matsuno O. Allergic bronchopulmonary aspergillosis successfully treated with tezepelumab. J Allergy Clin Immunol Pract. 2023;11(8):2589–2591. doi:10.1016/j.jaip.2023.05.026
8. Dunican EM, Watchorn DC, Fahy JV. Autopsy and imaging studies of mucus in asthma. Lessons learned about disease mechanisms and the role of mucus in airflow obstruction. Ann Am Thorac Soc. 2018;15(Suppl 3):S184–S191. doi:10.1513/AnnalsATS.201807-485AW
9. Pham TH, Chen C, Colice G, Parnes JR, Griffiths JM, Cook B. Tezepelumab normalizes serum interleukin-5 and −13 levels in patients with severe, uncontrolled asthma. Ann Allergy Asthma Immunol. 2021;127(6):689–691. doi:10.1016/j.anai.2021.08.008
10. Malinovschi A, Janson C, Borres M, Alving K. Simultaneously increased fraction of exhaled nitric oxide levels and blood eosinophil counts relate to increased asthma morbidity. J Allergy Clin Immunol. 2016;138(5):1301–1308.e2. doi:10.1016/j.jaci.2016.01.044
11. Menzies-Gow A, Corren J, Bourdin A, et al. Tezepelumab in adults and adolescents with severe, uncontrolled asthma. N Engl J Med. 2021;384(19):1800–1809. doi:10.1056/NEJMoa2034975
12. Dong H, Hu Y, Liu L, et al. Distinct roles of short and long thymic stromal lymphopoietin isoforms in house dust mite-induced asthmatic airway epithelial barrier disruption. Sci Rep. 2016;6:39559. doi:10.1038/srep39559
13. Smelter DF, Sathish V, Thompson MA, Pabelick CM, Vassallo R, Prakash YS. Thymic stromal lymphopoietin in cigarette smoke-exposed human airway smooth muscle. J Immunol. 2010;185(5):3035–3040. doi:10.4049/jimmunol.1000252
14. Agarwal R, Gupta D, Aggarwal AN, et al. Clinical significance of decline in serum IgE levels in allergic bronchopulmonary aspergillosis. Respir Med. 2010;104(2):204–210. doi:10.1016/j.rmed.2009.09.005
15. Tolebeyan A, Mohammadi O, Vaezi Z, Amini A. Mepolizumab as possible treatment for allergic bronchopulmonary aspergillosis: a review of eight cases. Cureus. 2020;12(8):e9684. doi:10.7759/cureus.9684
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.