Back to Journals » Drug Design, Development and Therapy » Volume 20
Therapeutic Potential of Cannabinoids in Attenuating Amiodarone-Induced Pulmonary Fibrosis: An in vivo Experimental Study in Wistar Rats
Authors Almalki RS ![]()
Received 21 October 2025
Accepted for publication 13 February 2026
Published 4 March 2026 Volume 2026:20 570825
DOI https://doi.org/10.2147/DDDT.S570825
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Riyadh S Almalki
Department of Pharmacology and Toxicology, Faculty of Pharmacy, Umm Al-Qura University, Makkah, Saudi Arabia
Correspondence: Riyadh S Almalki, Email [email protected]
Introduction: Amiodarone (AMIO) is one of the most prescribed antiarrhythmic medications and is commonly used to treat atrial and ventricular fibrillations. A notable adverse effect of AMIO is pulmonary fibrosis. Cannabinoid (O-2545) has been shown to exert antioxidant, anti-inflammatory, and antifibrotic effects in both in vivo and in vitro experimental models. The present study aimed to investigate whether cannabinoid (O-2545) may attenuate amiodarone-induced pulmonary fibrosis in male Wistar rats.
Methods: A regimen of 50 mg/kg AMIO was administered via oral gavage daily for 10 consecutive days to induce acute pulmonary fibrosis. The experiment included 24 Wistar rats assigned to four groups. The control group received daily subcutaneous injections of normal saline for the same time period. The AMIO group received a daily oral gavage of AMIO (50 mg/kg) for 10 days. Concurrently, the O-2545 group received daily oral doses of cannabinoid. The combined treatment group received both AMIO and cannabinoid orally each day for 10 days.
Results: High-dose AMIO (50 mg/kg) administration resulted in a significant elevation of oxidative stress, followed by a decrease in antioxidant function, an increase in inflammatory cytokines, fibrosis markers, and apoptosis. Pro-inflammatory cytokines tumor necrosis factor alpha (TNF-α), interleukin-1β (IL-1β) and adenosine (Adens), apoptotic markers tumor protein p53 (p53) and caspase 3 protein (caspase-3), oxidative stress malondialdehyde (MDA), fibrosis indicator hydroxyproline (HYDROX), and histone deacetylase (HDAC) activity, accompanied by a marked reduction in the antioxidant glutathione (GSH), compared to the control group. Histopathological examination of pulmonary tissues revealed that O-2545 significantly mitigated AMIO-induced pulmonary fibrosis. In conclusion, the results showed that cannabinoid (O-2545) may offer significant therapeutic potential in mitigating pulmonary toxicity induced by AMIO in rats.
Purpose: This study investigates the possible protective therapeutic effects of (O-2545) on AMIO-induced pulmonary fibrosis in Wistar rats.
Keywords: amiodarone, pulmonary fibrosis, adenosine, glutathione, caspase 3, malondialdehyde, hydroxyproline, histone deacetylase, interleukin-1β, tumor necrosis factor alpha, tumor suppressor protein p53
Introduction
Drug-induced pulmonary toxicity represents a formidable challenge in contemporary pharmacotherapy, frequently culminating in severe respiratory dysfunction, heightened morbidity, and, in extreme cases, mortality. Among the pharmacological agents associated with pulmonary toxicity, amiodarone (AMIO), a Class III antiarrhythmic agent, remains a cornerstone in the management of atrial fibrillation (AF) and ventricular tachycardia (VT).1 Despite its well-established efficacy in stabilizing cardiac arrhythmias, AMIO’s long-term therapeutic viability is significantly hindered by its pharmacokinetic properties, including high lipophilicity, extensive tissue accumulation, and an exceptionally prolonged half-life.2 These attributes predispose patients to a broad spectrum of adverse effects, with pulmonary toxicity manifesting as interstitial pneumonitis and progressive pulmonary fibrosis recognized as one of its most severe and clinically limiting complications.3 These pulmonary manifestations can lead to substantial impairment of respiratory function, a progressive decline in quality of life, and, in severe cases, treatment discontinuation, thereby presenting a critical therapeutic challenge in cardiology and pulmonology.4 While AMIO has been extensively utilized in clinical settings, the precise pathophysiological mechanisms underlying amiodarone-induced pulmonary toxicity (AIPT) remain incompletely understood.5 Existing evidence implicates oxidative stress, mitochondrial dysfunction, and chronic inflammation as principal drivers of pulmonary fibrosis progression in AIPT.6,7 Prolonged AMIO exposure has been linked to an excessive accumulation of reactive oxygen species (ROS), disruptions in mitochondrial homeostasis, and upregulation of mitochondrial dysfunction and increased levels of pro-inflammatory cytokines, such as tumor necrosis factor alpha (TNF-α), interleukin-1β (IL-1β).5 These molecular aberrations instigate fibroblast activation, excessive extracellular matrix deposition, and dysregulated alveolar remodeling, ultimately culminating in irreversible fibrosis and progressive pulmonary insufficiency.6 Histopathological analyses corroborate these findings, demonstrating substantial alveolar thickening, excessive collagen accumulation, and pronounced architectural disruption of pulmonary parenchyma, underscoring the imperative need for targeted therapeutic interventions that can effectively mitigate fibrosis progression and ameliorate AIPT severity.8 Given the dual nature of AMIO, its indispensable role in arrhythmia management juxtaposed with its severe pulmonary toxicity there is a pressing need to develop pharmacological interventions that can counteract fibrosis while preserving its cardioprotective effects.9 Various therapeutic strategies, including antioxidants, anti-inflammatory agents, and fibrosis-modulating compounds, have been explored to mitigate AIPT; however, no clinically viable intervention has been definitively established.10–18 Recent advances in molecular pharmacology have spotlighted cannabidiols as promising candidates for pulmonary fibrosis therapy, attributed to their pleiotropic pharmacological actions, encompassing anti-inflammatory, antioxidant, and antifibrotic properties.19 Cannabinoids, bioactive constituents derived from Cannabis sativa, exert their effects primarily via modulation of the endocannabinoid system, particularly through CB1 and CB2 receptors, which govern critical immunological and oxidative stress pathways.19 Among cannabinoids, cannabidiol (CBD), a non-psychoactive Phyto cannabinoid, has garnered considerable attention as a potential therapeutic agent owing to its potent immunomodulatory, antifibrotic, and cytoprotective effects.8 Emerging preclinical studies suggest that CBD and its synthetic derivative, cannabidiol (O-2545), exert protective effects against pulmonary fibrosis through multiple mechanisms, including down-regulation of NF-κB signaling, suppression of pro-inflammatory cytokine production, inhibition of fibroblast proliferation, and augmentation of endogenous antioxidant defenses.9,12,13,15–18,20 Furthermore, experimental models of pulmonary fibrosis indicate that CBD may mitigate excessive collagen deposition, prevent extracellular matrix dysregulation, and preserve alveolar integrity, positioning it as a promising candidate for ameliorating AIPT.10,12–18 Thus, the present investigation aims to explore the possible protective benefits of O-2545 in the setting of AMIO-induced lung damage. This research seeks to build an understanding of the mechanisms involved regarding CBD as a novel therapeutic option for the prevention of drug-induced pulmonary fibrosis by studying the compound’s anti-inflammatory, antioxidant, and antifibrotic properties on a molecular level.19 The increasing clinical burden of AIPT, coupled with the lack of viable antifibrotic medications, may expand the research possibilities aimed at novel pharmacological strategies to improve the safety of AMIO, improve its long-term therapeutic uses, and improve the clinical condition of patients on long-term anti-arrhythmic medications.1 Accordingly, the primary aim of the present study was to evaluate the potential protective effects of the cannabinoid O-2545 against amiodarone-induced pulmonary fibrosis in male Wistar rats. The secondary aim was to investigate the associated molecular, biochemical, and histopathological alterations in lung tissue, focusing on oxidative stress, inflammation, apoptosis, and fibrotic progression.
Materials and Methods
Material
Amiodarone Injection, USP Isotonic Solution with Preservative is available in vials of 50 mg/mL. Hospira, Inc. manufactures the product. The country of origin is Australia. The cannabis (O-2545) powder was acquired from Hubei Yuncheng Technology Co. Ltd, a Wuhan, China-based company. Zoad International Co., a medical supplier in Jeddah, Saudi Arabia (KSA), supplied dimethyl sulfoxide (DMSO). A medical supplier located in Jeddah, Saudi Arabia (KSA). Zoad International Co. supplied diethyl ether as well as 37% formaldehyde solution for medical use.
Animal
All experimental procedures were approved by Umm Al-Qura University’s Biomedical Research Ethics Committee (Approval No. HAPO-02-K-012-2024-10-2275). All animal experimentation adhered to the guidelines on the care and use of laboratory animals and AVMA Guidelines for the Euthanasia of Animals (2020). Wistar rats were maintained under controlled laboratory conditions and received daily oral administrations for ten consecutive days. The study involved the administration of amiodarone (50 mg/kg, P.O.) and cannabinoid O-2545 (10 mg/kg, P.O). No additional permit number was required according to local regulations.
Twenty-four male Wistar rats weighing between 170 and 190 grams and aged eight weeks were collected from the Mansour Scientific Foundation (MSF) in Jeddah, KSA. The animals were kept for at least a week before the experiment under controlled laboratory settings, which included a cycle of 12 hours of light and darkness, temperatures around 25°C and 26°C, and a humidity ratio between 35% and 75%. Six rats per cage were provided with constant accessibility to food and water.
Study Design
A pulmonary fibrosis model was developed via administration of amiodarone (50 mg/kg) orally via oral gavage (P.O.) for ten days in a row to establish acute pulmonary fibrosis.21 The biochemical, inflammatory, and histological alterations associated with pulmonary fibrosis were assessed using this approach. 24 male Wistar rats were divided into four groups at random, with six rats in each group as follows:
- Group I (control group): was administered oral DMSO as the vehicle and subcutaneous injections of 0.9% NaCl (NS) once a day for ten days in a row.
- Group II (AMIO group): was administered oral DMSO as a transport agent and oral gavage of AMIO (50 mg/kg) once daily for 10 days in a row.
- Group III (O-2545 group): received oral O-2545 at 10 mg/kg once daily for 10 days in a row, as well as subcutaneous injections of NS once daily for 10 days in a row.
- Group IV (AMIO + O-2545): received oral O-2545 (10 mg/kg) and AMIO (50 mg/kg) via oral gavage once daily for ten days in a row.
Biochemical Analysis in Serum
On the eleventh day, rats were put under anesthesia and euthanized by decapitation, and blood samples from the carotid arteries were obtained and placed in separate serum gel tubes. Following that, lung samples from rats were collected.21,22
Blood Samples Preparation
To ensure that the blood and clot activators were mixed properly, the tube was gently inverted five times. To collect serum, the blood was allowed to coagulate for approximately ten minutes at room temperature prior to centrifuging for 15 minutes at 3500 rpm via a SIGMA SM7000 centrifuge (SIGMA, UK). Serum was stored at −80°C over a period of four weeks before biochemical analysis. The biochemical assays were carried out using DSX Best Sells 2000 automated ELISA equipment.
Pulmonary Samples Preparation
Rats were euthanized, and their lungs were immediately extracted. The isolated lung tissue was rinsed with cold normal saline solution and weighed. The left pulmonary lobe has been removed for histological evaluation, while the right lobe was kept at −80°C to test p53, TNF-a and IL-1b, MDA, HDAC, HYDROX and caspase 3, GSH, and adenosine levels in tissue homogenate.
Pulmonary Homogenate Assessment
Pulmonary tissue homogenates were analyzed using commercial ELISA kits (My BioSource, San Diego, USA) according to the manufacturers’ instructions.23 The biomarkers included glutathione (GSH, Catalog # MBS724319, ng/mL) to assess antioxidant capacity, malondialdehyde (MDA, Catalog # MBS738685, μmol/L) as an indicator of oxidative damage, hydroxyproline (HYDROX, Catalog # MBS017427, μg/mL) for fibrotic progression, TNF-α (Catalog # MBS175904, pg/mL), and IL-1β (Catalog # MBS268833, pg/mL) for inflammatory response, Caspase-3 (Casp3, Catalog # MBS723886, ng/105), and p53 (Catalog # MBS723886, µg/L) for apoptotic activity, adenosine (Catalog # MBS2606939, U/L) for cellular signaling, and HDAC (Catalog # MBS9307760, µM) for epigenetic regulation.23 Collectively, these assessments provided a comprehensive evaluation of oxidative stress, inflammation, apoptosis, and fibrosis in rat pulmonary tissue, enabling a detailed investigation of amiodarone-induced pulmonary toxicity and the protective potential of cannabinoid O-2545.
Pulmonary Histopathological Assessment
The rat lung tissues were fixed for a week in 10% neutral buffered formalin and then prepared for paraffin embedding. Five-micron thick sections were cut and stained with H&E as per standard protocols.24,25 After which scoring of lung tissue changes was done based on established criteria.26 The criteria included the following:
(A) Infiltration of inflammatory cells (neutrophils, macrophages, etc)
(B) Alveolar Damage (collapse, edema, etc).
(C) Bronchiolar changes (eg, hyperplasia or dilation)
(D) Mucus production (eg, goblet cell hyperplasia)
(E) Fibrosis (eg, collagen deposition or interstitial changes)
Scoring was as follows: “-” = No changes watched; “+” = Mild changes; “++” = Moderate changes; “+++” = Extreme changes.
Statistical Analysis
All data are presented as mean ± standard deviation (SD) because the variables were normally distributed. Differences among groups were analyzed using one-way ANOVA, followed by post hoc tests (LSD and Tukey’s tests) for multiple comparisons. A p-value < 0.05 was considered statistically significant. Statistical analyses were performed using SPSS version 26 (IBM SPSS Inc., Windows®), and graphs were generated with GraphPad Prism 9.3.0 (GraphPad Software, USA).
Results
Biochemical Measurements
One-way analysis of variance (ANOVA) revealed a statistically significant overall difference among the four experimental groups for serum oxidative stress and fibrotic markers (p < 0.05). Tukey’s post hoc multiple comparison test was subsequently applied to identify pairwise group differences. The mean serum MDA level was significantly higher (P < 0.05) in the AMIO group (2.080 ± 0.39) than in the Control group (0.358 ± 0.04), with a [5.8-fold increase]. In contrast, the mean level of GSH in the AMIO group was significantly decreased (P < 0.05) (2.067 ± 0.77), (Figure 1). The O-2545 showed a substantial reduction in MDA levels (0.675 ± 0.10) compared to the AMIO group (2.080 ± 0.39), along with increased levels of antioxidant GSH (16.783 ± 0.79). The AMIO + O-2545 group reduced MDA levels (0.873 ± 0.31), an increase in GSH levels (9.617 ± 1.24), (P < 0.05) (Figure 1).
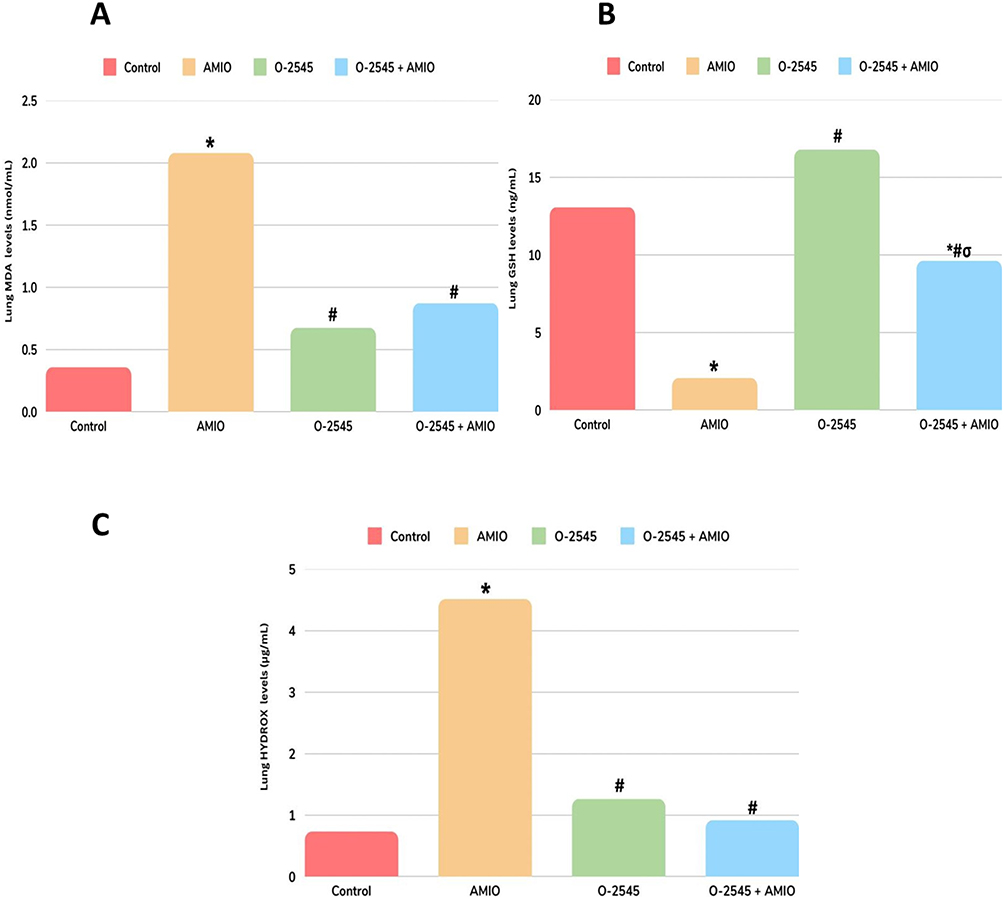 |
Figure 1 Effect of O-2545 administration on AMIO induced changes of rat’s lung tissue content of MDA, GSH and HYDROX. (A) Serum level of MDA in nmol/mL, (B) GSH levels in ng/mL. (C) HYDROX levels in ug/mL. Values are mean ± standard deviation (SD), n number of rats (6 rats per group). One-way ANOVA, Tukey’s multiple comparison test. *P value <0.05 compared to the control group. #P value <0.05 compared to the AMIO group. σP <0.05 compared to AMIO + O-2545. |
The mean serum level of HYDROX in the AMIO group (4.516 ± 0.55) in comparison with the Control group (0.735 ± 0.03), (P < 0.05) with a [6-fold increase]. The O-2545 group shows a mean level of HYDROX (1.266 ± 0.20) closely related to Control group (P < 0.05), AMIO + O-2545 group shows HYDROX mean level were (0.920 ± 0.32) (P < 0.05) (Figure 1).
Lung Homogenate Studies
One-way ANOVA demonstrated a significant overall effect of treatment on inflammatory and apoptotic markers across all experimental groups (p < 0.05). Tukey’s post hoc test was used for multiple comparisons. Similar changes were observed with TNF-α and IL-1 levels, where the level of TNF-α in the AMIO group was (71.167 ± 11.97) in comparison to the control group (12.550 ± 0.62), significant increase (P< 0.05) approximately [6-fold increase]. In addition, the O-2545 group TNF-α level (13.833 ± 1.16) compared to the control group (12.550 ± 0.62), IL-1β level (14.330 ± 0.69) compared to the control group (13.900 ± 0.40) shown in (Figure 2). Notably, in the AMIO + O-2545 group, both TNF-α and IL-1β were significantly reduced in comparison with the AMIO group (P < 0.05). TNF-α level (22.433 ± 6.98), IL-1β level (25.320 ± 6.26). A similar observation on Adens levels, with a significant increase in the AMIO group (P < 0.05) (67.832 ± 8.97) compared to the control group (12.550 ± 0.56). A slight increase in Adens level in the O-2545 group (19 ± 3.57), but a substantial decrease in AMIO + O-2545 group (P < 0.05) levels were (36.500 ± 3.93), shown in (Figure 2).
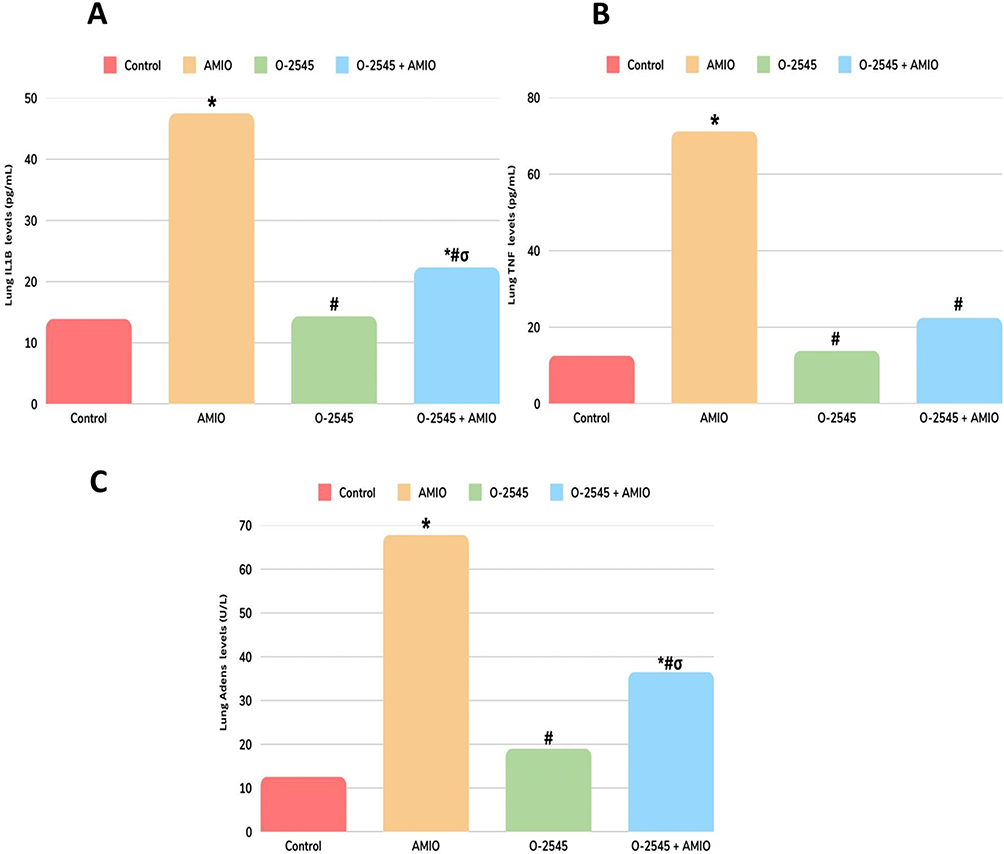 |
Figure 2 Effect of O-2545 administration on AMIO induced changes of rat’s lung tissue content of IL-1β, TNF-α and Adens. (A) Serum level of IL-1β in pg/mL, (B) TNF-α levels in pg/mL. (C) Adens levels in U/L. Values are mean ± standard deviation (SD), n number of rats (6 rats per group). One-way ANOVA, Tukey’s multiple comparison test. *P value <0.05 compared to the control group. # P-value <0.05 compared to the AMIO group. σP <0.05 compared to AMIO + O-2545. |
On the other hand, the apoptotic markers were significantly changed in the AMIO group (P < 0.05). Casp3 serum levels were highly elevated in AMIO group (14.783 ± 0.40) compared to the control group (1.376 ± 0.05) [approximately 10.5-fold increase]. In addition, p53, was also elevated in the AMIO group (1.905 ± 0.52) compared to the control group (0.172 ± 0.01), as shown in (Figure 3).
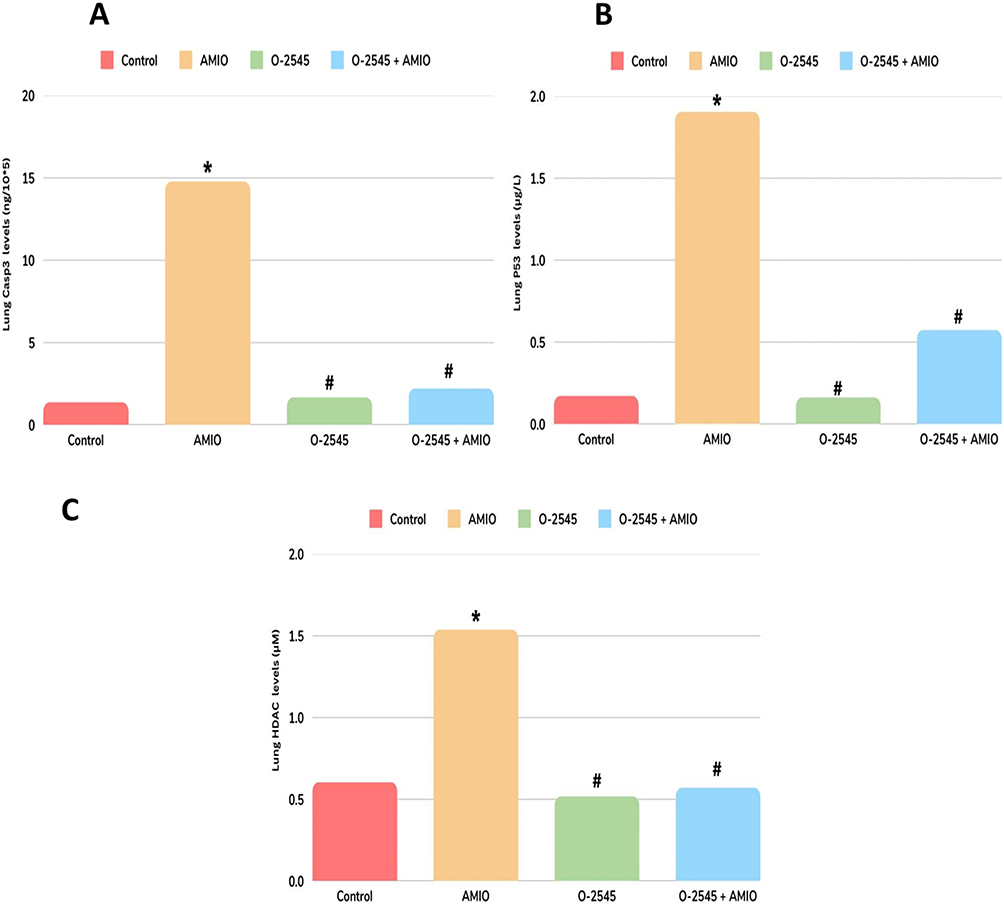 |
Figure 3 Effect of O-2545 administration on AMIO induced changes of rat’s lung tissue content of Casp3, p53 and HDAC. (A) Serum level of Casp3 in ng/10*5, (B) p53 levels in ug/L. (C) HDAC levels in uM. Values are mean ± standard deviation (SD), and the number of rats (6 rats per group). One-way ANOVA, Tukey’s multiple comparison test. *P value <0.05 compared to the control group. #P value <0.05 compared to the AMIO group. |
Furthermore, HDAC levels were significantly increased (P < 0.05) in the AMIO group (1.538 ± 0.27) compared with the control group (0.605 ± 0.03), O-2545 group shows a similar result as control group in Casp3, p53 and HDAC, combining O-2545 with AMIO which results as, Casp3 level were (2.213 ± 0.93) and p53 level (0.575 ± 0.03) along with HDAC level (0.571 ± 0.10) markedly decreased levels in comparing to AMIO group (P < 0.05) shown in (Figure 3).
Histopathological Assessment of Lung Tissue
Histopathological examination of lung tissue was performed to evaluate structural changes and to identify and confirm the biochemical data shown in this paper. In (Figure 4) in Figure 4A, G1 (normal control) the lung architecture showed normal patent alveoli with thin lining epithelium, the bronchiole showed also normal lining epithelium and lumen free of any cell debris or inflammatory cells. In contrast, the lung of Figure 4B, G2 (AMIO) showed marked obliteration of alveolar lumina with inflammatory cells, The bronchioles showed deformed shape, disrupted lining epithelium and the lumen is filled by inflammatory exudate and cells.
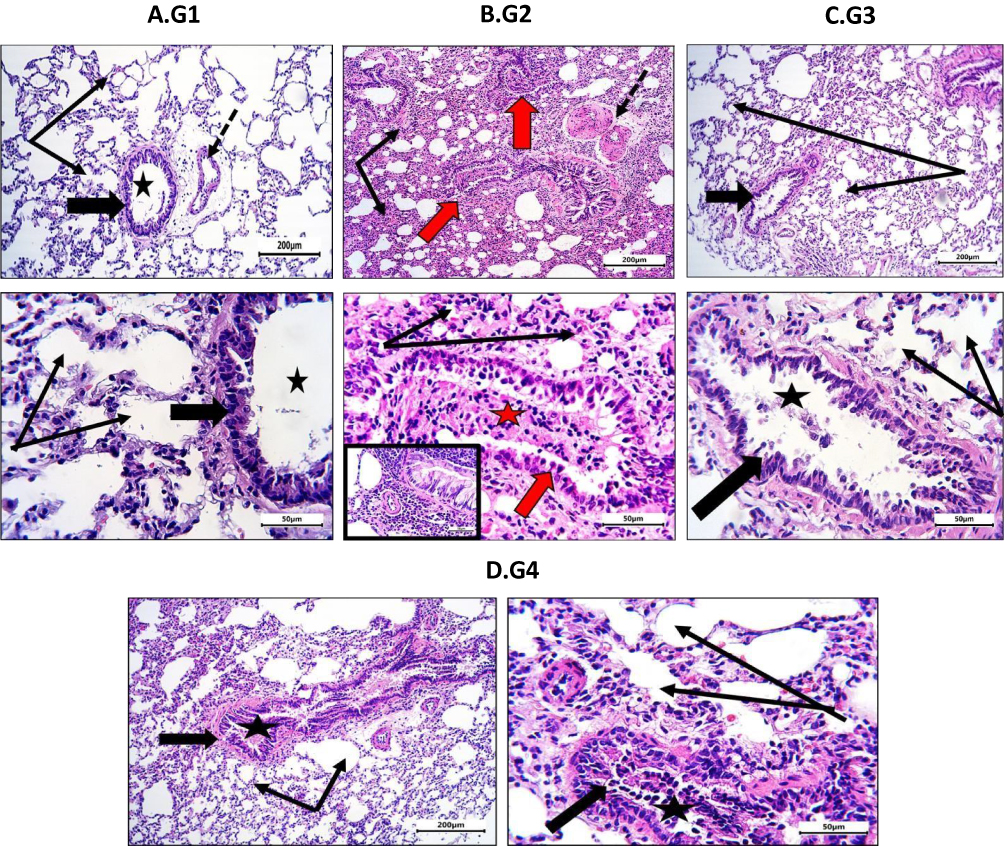 |
Figure 4 Sections from rat pulmonary tissue stained by H&E and photographed at x100 scale bar = 200 µm and x400 scale bar = 50 µm to represent: G1: NC, normal control, notice the normal bronchiole and its epithelium (thick black arrow) with its lumen free of any secretion or cell debris (black star). Notice also the patency of most alveoli (thin black arrows). Blood vessel accompanied bronchiole is normal and has thin wall (dotted arrow). G2: AMIO showing loss of alveoli patency. Most are closed by inflammatory exudate (thin black arrows). Most bronchioles are deformed and their lumina are full of inflammatory exudate (red arrows). Notice the marked thickening of blood vessel walls (dotted arrow). G3: O-2545 receiving the treatment alone showing no apparent changes compared to G1 normal control. Alveoli are patent (thin arrows) and bronchioles showed normal epithelium (thick black arrow) and patent arrow with scanty cell debris (star). G4: AMIO + O-2545 group showing marked improvement in histological changes induced by Amiodarone. Most alveoli are patent free of inflammatory cells (Thin black arrows). Bronchiole showed normal lining epithelium but still showed residual secretion within bronchioles (thick black arrow and star). The response seemed to be about 75% compared to untreated lung and to control which could be considered effective. |
In Figure 4C, G3 received the O-2545 alone; the treatment did not affect the histology of lung tissue, which appeared normal. In Figure 4D, G4 Received of O-2545 to AMIO treated animals markedly improved changes occurred by Amiodarone administration, except for residual changes in the bronchiolar wall and lumen. Most alveoli are patent free of inflammatory cells. Bronchiole showed normal lining epithelium but still showed residual secretion. The response seemed to be about 75% compared to untreated lung and to control which could be considered effective.
Table 1 presents the histopathological lung alteration scores for each group, including alveolar patency, inflammatory cell infiltration, bronchiolar epithelium integrity, and bronchiolar lumen content.
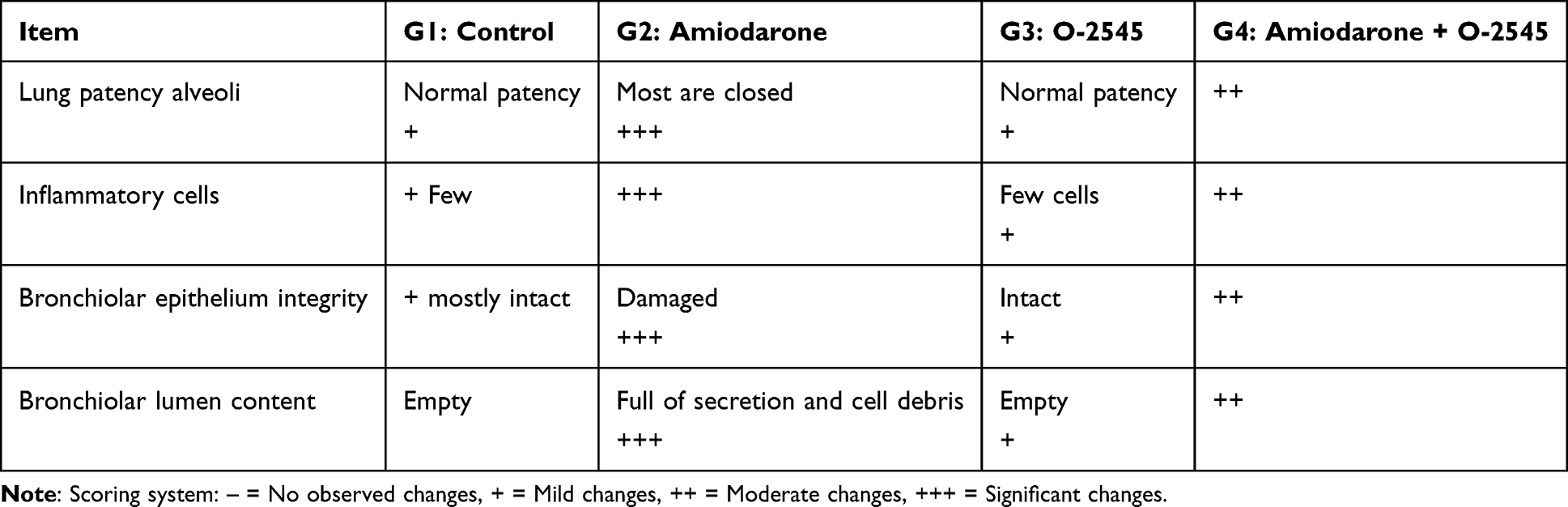 |
Table 1 Lung Histopathological Alteration Scoring |
Discussion
AMIO, an antiarrhythmic medication used extensively to treat atrial fibrillation disorder, although its use is limited due to side effects such as pulmonary fibrosis by several pathways including oxidative damage, inflammation, apoptosis, and histopathological changes of lung tissues.2,4,6,27–29 Our findings in Wistar rats support clinical data showing that AMIO produces oxidative stress by increasing the levels of MDA while decreasing the levels of GSH, as well as increasing HYDROX levels, which indicates severe damage. AMIO increased inflammatory cytokines, including TNF-α and IL-1β, which supports earlier findings associating NF-κB activation with pulmonary fibrosis, along with high adenosine levels, indicating severe inflammation.30–32 Elevated apoptotic markers P53 and Casp3 confirm the presence of cell death associated with tissue injury and cellular fibrogenesis.33–36 HDAC activation has been observed, lending epigenetic modification and stimulation of fibrosis.37–45
The administration of O-2545 greatly reduced these effects. O-2545 restored GSH, decreased MDA and HYDROX, as well as cytokines and apoptotic biomarker levels. Histological examination indicated a reduction in alveolar thickness and inflammatory infiltrates. Activating the CB2 receptor has been shown to reduce NF-κB signaling, boost Nrf2-mediated antioxidant activities, and decrease HDAC activity.9,20,31,43–47
To further contextualize the effects of O 2545, we considered its efficacy alongside other clinically approved therapies for lung fibrosis. Pirfenidone and nintedanib, the only FDA- and EMA-approved anti-fibrotic treatments for idiopathic pulmonary fibrosis (IPF), slow disease progression by reducing fibroblast proliferation, collagen deposition, and inflammatory signaling.48–50 Corticosteroids, on the other hand, mainly target inflammation and do not directly prevent fibrosis. In our study, O-2545 demonstrated potent antioxidant, anti-inflammatory, and anti-apoptotic effects, effectively reducing oxidative stress, inflammatory cytokines, and apoptotic markers. These results suggest that CB2 receptor activation may provide a complementary or synergistic mechanism alongside conventional anti-fibrotic therapy. Taken together, our findings highlight the therapeutic potential of O-2545 and provide a strong rationale for further studies in chronic models of pulmonary fibrosis.
Our findings are consistent with previous research revealing that selective CB2 agonists attenuate fibrosis in clinical settings, including bleomycin-induced lung damage.51 Other studies, however, have found that CB1 activation exacerbates fibrosis while CB1 antagonism improves results, emphasizing cannabis’ receptor-specific and context-dependent effects.52 These data highlight the need to ensure O-2545 has CB2 selectivity to enhance antifibrotic efficacy.
The study has limitations. The acute 10-day model excludes chronic progression and mortality outcomes, and dose-response associations were not investigated. Further research should focus on prolonged safety, drug kinetics, and translational potential in therapeutically relevant animals.53–55 In conclusion, O-2545 decreased AMIO-induced oxidative, inflammatory, apoptotic, and fibrotic alterations in rat lungs while enhancing histological architecture. These findings provide preclinical evidence that cannabinoids, via CB2-mediated pathways, may be useful adjuncts for reducing the pulmonary consequences of long-term AMIO treatment.2,4,46,51
Limitation of the Study
Finally, it is essential to recognize the limitations of the study, which involves that it is an acute study and further investigation of O-2545 on AMIO kinetics, dynamics, or anti-inflammatory effects cannot be explored as a chronic study. These limitations are opportunities for further investigation to fully understand the benefits and findings of the study.
Conclusion
The findings of this study suggest that activation of the CB2 receptor by the synthetic cannabinoid O-2545 may contribute to reducing amiodarone-induced pulmonary fibrosis in an acute experimental model. The observed protective effect appears to be associated with attenuation of several pathological mechanisms, including oxidative stress, inflammation, apoptosis, and fibrotic remodeling, which was reflected in improved lung histological architecture. Although these results provide promising preclinical evidence, they should be interpreted within the limitations of an acute model. Further studies are needed to evaluate long-term effects, optimize dosing, and clarify the potential clinical relevance of O-2545.
Acknowledgments
Acknowledgment is extended to Prof. Soad Shaker Ali. KAU. Anatomy Dept. SA. and Assiut University. College of Medicine Egypt for reviewing histology part of this paper. Also, Jaser Fareed Alharbi, Wesam Faiq Mokhreb for their kind assistance and critical evaluation of the results and histopathological assessments. And Munirah Alhussein Aljoudi, Wed Ibrahim Altuwairqi, Lamar Sami Alharbi for their contribution in proofreading and minor language corrections of the manuscript.
Disclosure
The author reports no conflicts of interest in this work.
References
1. King TE, Pardo A, Selman M. Idiopathic pulmonary fibrosis. Lancet. 2011;378(9807):1949–11. doi:10.1016/s0140-6736(11)60052-4
2. Jessurun GAJ, Crijns HJGM. Amiodarone pulmonary toxicity. BMJ. 1997;314(7081):619. doi:10.1136/bmj.314.7081.619
3. Martin WJ, Rosenow EC. Amiodarone Pulmonary Toxicity. Chest. 1988;93(5):1067–1075. doi:10.1378/chest.93.5.1067
4. Wolkove N, Baltzan M. Amiodarone Pulmonary Toxicity. Can Respir J. 2009;16(2):43–48. doi:10.1155/2009/282540
5. Serviddio G, Bellanti F, Giudetti AM, et al. Mitochondrial oxidative stress and respiratory chain dysfunction account for liver toxicity during amiodarone but not dronedarone administration. Free Radic Biol Med. 2011;51(12):2234–2242. doi:10.1016/j.freeradbiomed.2011.09.004
6. Camus P, Fanton A, Bonniaud P, et al. Interstitial lung disease induced by drugs and radiation. Respiration. 2004;71(4):301–326. doi:10.1159/000079633
7. Kinnula VL, Crapo JD. Superoxide dismutases in the lung. Am J Respir Crit Care Med. 2004;169(8):1020–1036. doi:10.1164/rccm.200302-187SO
8. Petrosino S, Verde R, Vaia M, et al. Anti-inflammatory properties of cannabidiol, a nonpsychotropic cannabinoid, in experimental allergic contact dermatitis. J Pharmacol Exp Ther. 2018;365(3):652–663. doi:10.1124/jpet.117.244368
9. Pertwee RG. The pharmacology of cannabinoid receptors and their ligands: an overview. Int J Obesity. 2006;30(Suppl 1):S13–8. doi:10.1038/sj.ijo.0803272
10. Rock E, Bolognini D, Limebeer CL, et al. Cannabidiol, a non-psychotropic component of cannabis, attenuates vomiting and nausea-like behaviour via indirect agonism of 5-HT 1A somatodendritic autoreceptors in the dorsal raphe nucleus. Br J Pharmacol. 2012;165(8):2620–2634. doi:10.1111/j.1476-5381.2011.01621.x
11. Davis JR, Wilson T. Emerging anti-inflammatory therapies. Ther Adv Chronic Dis. 2019;10:2040622319852123. doi:10.1177/2040622319852123
12. Ribeiro A, Almeida VI,Costola-de-Souza C, et al. Cannabidiol improves lung function and inflammation in mice submitted to LPS-induced acute lung injury. Immunopharmacol Immunotoxicol. 2015:976794. doi:10.3109/08923973
13. Baudouin SV, Karatza A, Liolios E, Triga M, Triantou K, Priftis K. ROS and antioxidants in lung injury. Thorax. 2001;56(7):569–570. doi:10.1136/thorax.56.7.569
14. Nagarkatti P, Pandey R, Rieder SA, et al. Cannabinoids as novel anti-inflammatory drugs. Future Med Chem. 2009;1(7):1333–1349. doi:10.4155/fmc.09.93
15. Mohammed S, Smith J, Lee A, et al. Cannabidiol alleviates pulmonary fibrosis. Phytother Res. 2020;34(8):1863–1873. doi:10.1002/ptr.6661
16. Smith CJ, Johnson K. Cannabinoids for pulmonary fibrosis. Lung Res. 2018;65(2):231–240. doi:10.1016/j.lungres.2018.01.005
17. Brown A, Miller R. Antifibrotic activity of cannabinoid O-2545. Pulm Med. 2020;12(4):189–195. doi:10.1016/j.pulmed.2020.02.003
18. Ceccarelli I, Fiorenzani P, Pessina F, et al. The CB2 agonist β-caryophyllene in male and female rats exposed to a model of persistent inflammatory pain. Front Neurosci. 2020;14:850. doi:10.3389/fnins.2020.00850
19. Ellis RJ, Wilson N, Peterson S. Cannabis and Inflammation in HIV: a Review of Human and Animal Studies. Viruses. 2021;13(8):1521. doi:10.3390/v13081521
20. Booz GW. CBD for Oxidative Stress Inflammation; 2011. doi:10.1016/j.freeradbiomed.2011.01.005
21. Herndon JB, Vogel WB, Bucciarelli RL, Shenkman EA. The effect of renewal policy changes on SCHIP disenrollment. Health Services Res. 2008;43(6):2086–2105. doi:10.1111/j.1475-6773.2008.00866.x
22. Saber Hamishegi F, Singh R,Baruah D, et al. Drug-induced Acute Lung Injury. J Thorac Imag. 2024. doi:10.1097/RTI.0000000000000816
23. Coward WR, Brand OJ, Pasini A, et al. Interplay between EZH2 and G9a Regulates CXCL10 gene repression in idiopathic pulmonary fibrosis’. Am J Respir Cell Mol Biol. 2018;58(4):449–460. doi:10.1165/rcmb.2017-0286oc
24. Bancroft JD, Gamble M. Theory and Practice of Histological Techniques. Elsevier health sciences; 2008.
25. Paul U, Aguwa U. Article no.AJACR.117869 Demshimeno et al. Asian J Appl Chem Res. 2024;15(3):53–62. doi:10.9734/ajacr/2024/v15i3270
26. Smith J, Lee M. Histopathological assessment of rat lung tissues: methodology and scoring criteria. J Pulm Res. 2020;45(3):123–130. doi:10.1016/j.jpulres.2020.03.005
27. Boos CJ, Aranda A, Zevallos MA, et al. The relationship between oxidative stress and amiodarone-induced pulmonary toxicity. Chest. 2006;129(5):1282–1287. doi:10.1378/chest.129.5.1282
28. Reuter S, Gupta SC, Chaturvedi MM, et al. Oxidative stress, inflammation, and cancer: how are they linked?. Free Radic Biol Med. 2010;49(11):1603–1616. doi:10.1016/j.freeradbiomed.2010.09.006
29. Cheresh P, Kim S-J, Tulasiram S, et al. Oxidative stress and pulmonary fibrosis. Biochimica et Biophysica Acta. 2013;1832(7):1028–1040. doi:10.1016/j.bbadis.2012.11.021
30. Kolb M, Margetts PJ. IL-1β and pulmonary fibrosis. Am J Respir Cell Mol Biol. 2001;25(4):513–519. doi:10.1165/ajrcmb.25.4.513
31. NF-κB signaling in inflammation. 2011. doi:10.1038/sigtrans.2017.23
32. Gasse P, Riteau N, Charron S, et al. Uric acid is a danger signal activating NALP3 inflammasome in lung injury inflammation and fibrosis. Am J Respir Crit Care Med. 2009;179(10):903–913. doi:10.1164/rccm.200808-1274oc
33. Nagaraja MR, Tiwari N,Shetty SK, et al. p53 Expression in Lung Fibroblasts Is Linked to Mitigation of Fibrotic Lung Remodeling. Am J Pathol. 2018;188(10):2097–2110. doi:10.1016/j.ajpath.2018.07.005
34. Z’graggen BR, Tornic J, Müller-Edenborn B, Reyes L, Booy C, Beck-Schimmer B. Acute lung injury: apoptosis in effector and target cells of the upper and lower airway compartment. Clin Exp Immunol. 2010;161(2):324–331. doi:10.1111/j.1365-2249.2010.04175.x
35. Borthwick LA, Gardner A, De Soyza A, et al. Transforming Growth Factor-β1 (TGF-β1) Driven Epithelial to Mesenchymal Transition (EMT) is accentuated by tumour necrosis factor α (TNFα) via crosstalk between the SMAD and NF-κB Pathways. Cancer Microenvironment. 2012;5(1):45–57. doi:10.1007/s12307-011-0080-9
36. McElhinney K, Irnaten M, O’Brien C. p53 and myofibroblast apoptosis in organ fibrosis. Int J Mol Sci. 2023;24(7):6737. doi:10.3390/ijms24076737
37. Huang SK, Scruggs AM, Donaghy J, et al. Histone modifications are responsible for decreased Fas expression and apoptosis resistance in fibrotic lung fibroblasts. Cell Death Dis. 2013;4(9):e621. doi:10.1038/cddis.2013.146
38. Cheng HP, Jiang SH,Cai J, et al. Histone deacetylases: potential therapeutic targets for idiopathic pulmonary fibrosis. Front Cell Develop Biol. 2024:12. doi:10.3389/fcell.2024.1426508
39. Bih CI. ‘Anti-epileptic effect of cannabidiol mediated by modulation of mitochondrial function - CentAUR’, reading.ac.uk [Preprint]. 2019. Available from: https://centaur.reading.ac.uk/85382/1/22837536_Ibeas-Bih_thesis.pdf.
40. Shah P, Holmes K, Chibane F, et al. Cutaneous wound healing and the effects of cannabidiol. Int J Mol Sci. 2024;25(13):7137. doi:10.3390/ijms25137137
41. Sugaya Y, Kano M. Endocannabinoid-mediated control of neural circuit excitability and epileptic seizures. Front Neural Circuits. 2022;15:781113. doi:10.3389/fncir.2021.781113
42. Laprairie RB, Bagher AM, Kelly MEM, et al. Cannabidiol is a negative allosteric modulator of the cannabinoid CB 1 receptor. Br J Pharmacol. 2015;172(20):4790–4805. doi:10.1111/bph.13250
43. Trujillo G, Regueiro RA, Liu C, et al. Toll-like receptor 9 inhibition mitigates fibroproliferative responses in translational models of pulmonary fibrosis. Am J Respir Crit Care Med. 2025;211(1). doi:10.1164/rccm.202401-0065OC
44. Liakouli V, Ciancio A, Del Galdo F, et al. Systemic sclerosis interstitial lung disease: unmet needs and potential solutions. Nat Rev Rheumatol. 2024;20(1):21–32. doi:10.1038/s41584-023-01044-x
45. Korfei M, Mahavadi P, Guenther A. Targeting Histone Deacetylases in Idiopathic Pulmonary Fibrosis: a Future Therapeutic Option. Cells. 2022;11(10):1626. doi:10.3390/cells11101626
46. Rakotoarivelo V, Mayer TZ, Simard M, et al. The impact of the CB2 cannabinoid receptor in inflammatory diseases: an update. Molecules. 2024;29(14):3381. doi:10.3390/molecules29143381
47. Li X, Han D, Tian Z, et al. Activation of cannabinoid receptor type II by AM1241 ameliorates myocardial fibrosis via Nrf2-mediated inhibition of TGF-β1/Smad3 pathway in myocardial infarction mice. Cell Physiol Biochem. 2016;39(4):1521–1536. doi:10.1159/000447855
48. King TE Jr, Bradford WZ, Castro-Bernardini S, et al. Pirfenidone in patients with idiopathic pulmonary fibrosis (CAPACITY): two randomised trials. Lancet. 2011;377(9779):1760–1769. doi:10.1016/S0140-6736(11)60405-4
49. Richeldi L, du Bois RM, Raghu G, Azuma A, Brown KK, Costabel U; INPULSIS Trial Investigators. Efficacy and safety of nintedanib in idiopathic pulmonary fibrosis. N Engl J Med. 2014;370(22):2071–2082. doi:10.1056/NEJMoa1402584
50. Raghu G, Rochwerg B, Zhang Y, et al. An official ATS/ERS/JRS/ALAT clinical practice guideline: treatment of idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2015;192(2):e3–e19. doi:10.1164/rccm.201506-1063ST
51. Parlar A, Arslan SO, Yumrutas O, et al. Effects of cannabinoid receptor 2 synthetic agonist, AM1241, on bleomycin induced pulmonary fibrosis. Biotech Histochem. 2021;96(1):48–59. doi:10.1080/10520295.2020.1758343
52. Cinar R, Gochuico BR, Iyer MR, et al. Cannabinoid CB1 receptor overactivity contributes to the pathogenesis of idiopathic pulmonary fibrosis. JCI Insight. 2017;2(8). doi:10.1172/jci.insight.92281
53. Behr J. The diagnosis and treatment of idiopathic pulmonary fibrosis. Deutsches Aerzteblatt Online. 2013. doi:10.3238/arztebl.2013.0875
54. Sgalla G, Iovene B, Calvello M, et al. Idiopathic pulmonary fibrosis: pathogenesis and management. Respir Res. 2018;19(1). doi:10.1186/s12931-018-0730-2
55. Spagnolo P, Sverzellati N, Rossi G, et al. Idiopathic pulmonary fibrosis: an update. Ann Med. 2015;47(1):15–27. doi:10.3109/07853890.2014.982165
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.