Back to Journals » Patient Preference and Adherence » Volume 16
The Ward Round: Patients’ Perceptions of a Patient-Centered Approach and Their Suggestions for Improved Participation
Authors Aronsson L, Frithiof A, Röstedal A, Rudberg C, Ekström W
Received 29 November 2021
Accepted for publication 4 July 2022
Published 18 August 2022 Volume 2022:16 Pages 2203—2211
DOI https://doi.org/10.2147/PPA.S343955
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Linda Aronsson,1 Angelica Frithiof,1 Annie Röstedal,1 Charlotte Rudberg,2 Wilhelmina Ekström3
1Department of Orthopedics, Karolinska University Hospital, Stockholm, Sweden; 2Karolinska Institutet, Women’s Health and Allied Health Professionals Theme, Department of Occupational Therapy and Physiotherapy, Karolinska University Hospital, Stockholm, Sweden; 3Karolinska Institutet, Department of Molecular Medicine and Surgery, Department of Trauma, Acute Surgery and Orthopedics, Karolinska University Hospital, Stockholm, Sweden
Correspondence: Wilhelmina Ekström, Karolinska Institutet, Department of Molecular Medicine and Surgery, Department of Trauma, Acute Surgery and Orthopedics, Karolinska University Hospital, Stockholm, Sweden, Tel +46 7254 23 78, Fax +46 8 517 72695, Email [email protected]
Purpose: To explore, through a learning activity for healthcare students, how patients perceived the ward round and its patient-centered approach.
Patients and Methods: Patients admitted for elective orthopedic surgery were invited to participate in the study, which involved answering a survey comprising seven intersectional questions and eight free text questions. In addition, medical and nursing students did semi-structured interviews with the patients, covering the same free text questions. Twenty-three patients answered the survey, of whom fifteen also completed the interviews. The results from the interviews were explored using a thematic content analysis.
Results: Forty-three percent (10/23) of the patients strongly agreed or agreed that their knowledge of patient-centered ward round was sufficient to be able to participate actively, and thirty percent (7/23) indicated they had good knowledge of the laws and regulations governing the care of patients. Most of the patients felt satisfied with how their own and their relatives’ experiences were taken into account. The categories information and to be listened to were mentioned repeatedly by patients as priorities for patient-centered ward rounds. The interview analysis revealed four main categories: preparation, communication, organization, and safety as important and in need of improvement.
Conclusion: Less than half of the patients surveyed felt they could participate in the ward round, which indicates that there is an opportunity for improvement and development. Better information and communication about legal rights, as well as about the structure and content of the ward round, could be valuable to patients before admission. It is also important to find a way for patients’ individual wishes to be more fully and easily conveyed to medical staff. Creating a more tailor-made ward round for each patient and fulfilling a patient-centered approach will likely entail a substantial organizational and mental shift.
Keywords: patient-centered, ward round, patient perception, patient representative, learning activity
Introduction
Patient-centered care has been introduced worldwide with the aim of making patients more involved in decision-making and in their own care.1–4 However, patients’ knowledge about the link between patient-centeredness and ward rounds still seems to be abstract and unclear.5,6 According to the International Alliance of Patients’ Organizations, to be able to take part in their own care and treatment, patients need relevant, accurate and understandable information.4
Perfect conditions for carrying out the ward round are not always possible to achieve. In many respects, the ward round is still stuck in a traditional context, with limited and one-way communication. Research shows that few ward rounds (18%) involve patient participation in decisions about their care.7 Several factors influence patients’ ability to participate in the ward round in an adequate and relevant manner. External factors can also reduce patients’ ability to participate in decision-making according to previous studies, including the staff’s approach to patient involvement, the staff’s assessment of the need for patient information, role expectations, high workload, lack of experienced staff and continuity.8–10 Other patient-related factors such as the ability to negotiate, language comprehension, trust and input, and support from relatives and friends may also play a major role in creating opportunities to participate in decision-making.5
The combination of effective care processes and a patient-centered approach in the ward round can be difficult to achieve – especially if there is a lack of, or different views on, relevant and good communication. According to previous research, patients score the communication and information they receive poorly13 and desire more two-way communication.11–13 Multidisciplinary staff also consider good communication as crucial to ward round quality.14 Variable levels of care and a lack of standardization in patient assessment during ward rounds also have a negative impact on the ward round.15 Other authors emphasize the ward round as an opportunity for patient involvement in their own care.6,13 In their study, Brown et al report that a surgical communication check sheet increased awareness of patients’ concerns and empowered them to ask questions and thus improve ward round communication.16 The use of a special ward round checklist or surgical taxonomy showing good and poor examples of ward round skills also supports staff in improving their ward round and patient-perceived quality of care.17,18
In the present study, the interdisciplinary ward round at the orthopedic department includes a premeeting with the doctor, the nurse, and the physiotherapist in the morning. The care team discuss each patient’s situation using a ward round checklist. The patients are then visited in their individual rooms for exchange of information about current examinations, surgical procedures, and plans for the day. The patients are given an opportunity to ask questions and provide input concerning their discharge plan, which is then is resolved with the patient.
The current study was initiated by the staff of the department, whose ambition it was to evolve the ward round to become more patient-centered as part of a developmental project. It was also inspired by the results of the National Patient Survey, which made the clinic want to improve its outcome in information provision, patient participation19 and its understanding of patients’ perceptions of the ward round. Lastly, the study was intended to highlight issues that are important to patients and how patient-centered ward rounds could increase understanding, both for staff and especially for students, of patients’ situations.
The overall aims of this study were, through a learning activity for healthcare students, to explore patients’ perceptions of the ward round and aspects of the patient-centered approach.
Materials and Methods
Study Design
This study used both a survey and semi-structured interviews to obtain data from as many patients as possible, while also achieving a more in-depth understanding of their opinions regarding one phenomenon, ie, patient-centered ward rounds. The interviews used both predetermined and open-ended questions (Box 1).
 |
Box 1 Semi-Structured and Open-Ended Questions in the Interview Guide |
Ethics
The study was conducted according to the provisions of the Helsinki Declaration. Ethical approval for the study was obtained from The Regional Ethical Review Board in Stockholm (Dnr: 2019-00257, 2019-03325). Oral and written information about the purpose of the study was given to all participants, and it was made clear that participation was voluntary and that the participants could, at any time, withdraw from the study. Written informed consent was obtained from all participants prior to the study for the publication of anonymized responses and quotes. Each patient was shown and approved the transcript of their interview.
Participants
Patients scheduled to receive elective orthopedic surgery during a 12-week period (n=49) were informed about the study. Of these patients, 23 chose to participate. The exclusion criteria were patients with dementia and/or difficulty in understanding and writing in Swedish.
The patients who wanted to participate filled out a consent form and then filled out the survey individually. Each interview took place in the patient’s own room in the clinic at a time of their choosing. If the patient’s first choice of time was not possible, another convenient time was found.
Data Collection
The study was conducted at Karolinska University Hospital in Stockholm in collaboration with the Karolinska Institute during the spring semester of 2019. The data collection was done at a clinical education department where students have their interprofessional work-based training. The data were collected by medical, physiotherapy and nursing students who were on placement in the department for a two-week period.
The purpose specific survey papers were handed to the participating patients by the physiotherapy students. The first part of the questionnaire consisted of seven intersectional questions related to the patients’ knowledge and perception of the ward round, which were evaluated on a five-point Likert scale. The second part contained eight free text questions originating in the National Patient Survey.19
The medical and nursing students conducted the interviews using the same eight questions that were in the second part of the survey. The students used standard texts to start the interviews, to get the patients to expand on issues raised, and to close the interviews. These texts were developed with the local patient representative. The interviews were tape recorded and later transcribed verbatim.
The patient representative (AF) at the Department of Orthopedics at Karolinska University Hospital, whose main purpose was to involve patients on a structural level to increase the quality of care, had been in place since 2017. Her qualifications included specific training in medical ethics, psychology, and methods of narrative therapy. AF gave a lecture in interview technique and supported the medical students before the interviews. The lecture covered many topics, including body language and presence, tone of voice, emphasis, rephrasing of questions, creative questioning, respectful and ethical approaches, and validation of conversations during the final phase of the interview. The students also received a checklist with advice for the interviews.
Data Analysis
According to the explorative character of the study, thematic content analyses of the interviews and written comments were done through iterative readings.20 The analyses were compared and discussed in meetings with the research team, who then extracted meaning units consisting of one or more words, sentences, or paragraphs containing common themes. A theme was created that covered the text links and categories that emerged from the text. The results are presented below with direct quotes from the interviews.
The findings from the written survey comments were compared with the findings from the individual interviews, but no major contrasts were identified.
Statistical Analysis
All the items were summarized using standard descriptive statistics such as means, standard deviation (SD), and frequency. Pearson’s χ2 test was applied to the frequency of agreements (ie, agrees and totally agrees). The option neither-nor was collapsed with disagreements, ie, does not agree and does not agree at all. If a cell frequency was below 5, the crosstable was rearranged and a Fisher’s exact test was conducted. The significance level in all analyses was five percent (two-tailed).
Results
Patient Survey
Surveys were distributed to 49 patients during the study period, of whom 23 fully answered and returned the survey. There were 15 patients who could not fill out the survey due to surgery, discharge from hospital, or relocation to another care facility. Others declined due to pain or fatigue after surgery (n=8). One patient thought the questions were too complicated, another declined because of difficulties in reading, and one patient did not give a reason for declining participation. Ten patients (43%) strongly agreed or agreed that their knowledge of patient-centered ward rounds was sufficient to be able to participate, and seven (30%) thought they had good knowledge of the laws and regulations governing the care of patients. Most of the patients believed that healthcare professionals considered patients’ own experiences of their illnesses (21/23 or 91%) and the views of patients’ relatives (20/23 or 86%). The majority of patients (19/23 or 83%) thought that they and their relatives were involved in the decisions that were made regarding their treatment and planned care (Figure 1).
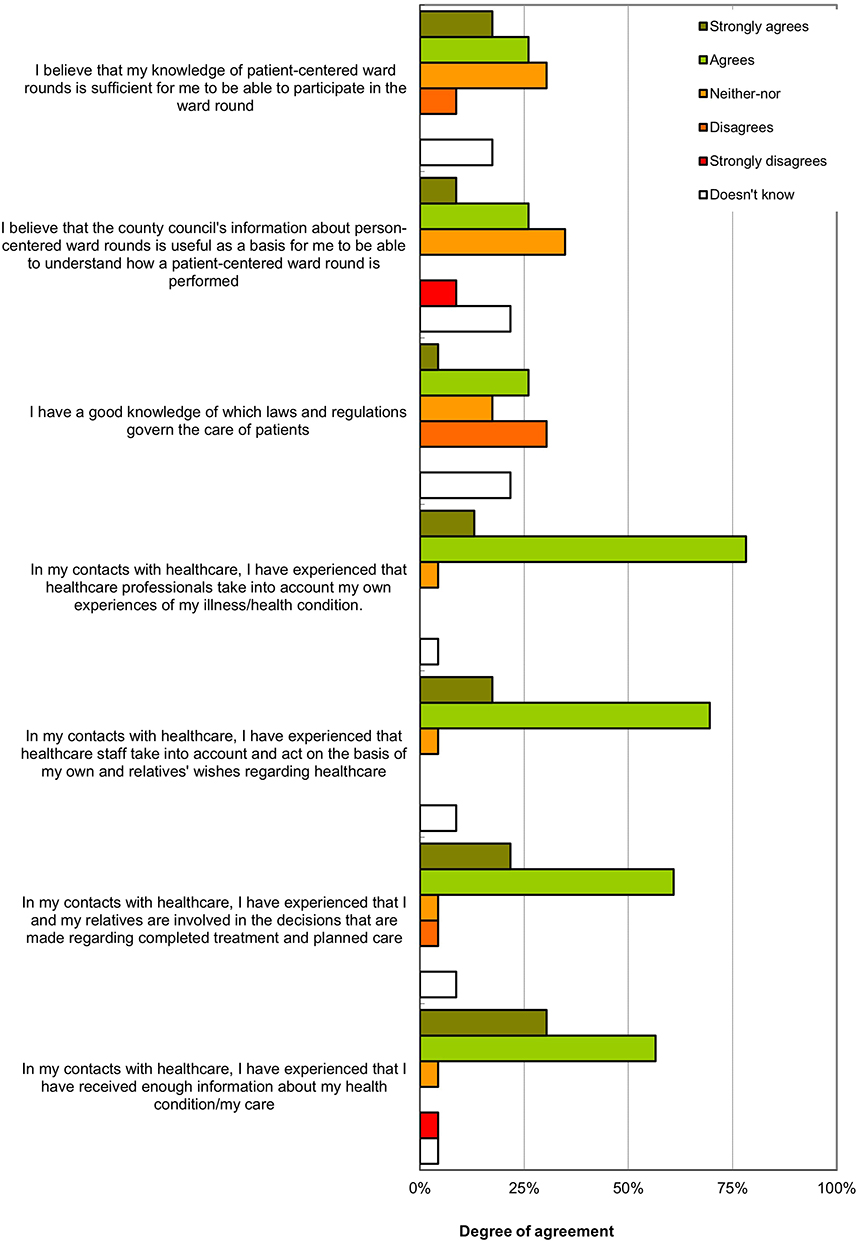 |
Figure 1 Survey on patients’ perceptions of patient-centeredness during the ward round (n=23). |
Only eight patients submitted answers to the free text questions, with information emerging as a recurrent theme of what patients wanted most as a part of a patient-centered ward round (patients 1, 2, 5, 6, 7 and 8). The information they wanted included what was planned and when, pre-prepared patient information, and, if all went according to plan, specific information for relatives and about future measures. To fully utilize the patients’ experiences, opportunity and time should be provided for the patients to be listened to (patients 1, 3, 4, 5 and 7).
Patient Interviews
Twenty-seven patients were asked to participate in the interviews, of whom twelve patients were prevented from participating for the following reasons: discharge before the interview (n=6), insufficient strength after surgery (n=2), change of mind (n=1), and finding the questions too complicated (n=1). Two interviews could not be completed due to the interviewer being ill. In total, 15 patients gave an interview. When studying the patients’ suggestions for improvements to the ward round, the suggestions could be divided into the following four categories: preparation, organization, communication, and safety. These themes are detailed below.
Preparation
The category of preparation reflects the patients’ wish to be well prepared before participating in a ward round. The name and the concept of a patient-centered ward round was described as “unknown” and “difficult to understand”. Patients described the importance of having information to prepare for the ward round, suggested having prepared questions to consider in advance, and wanted a schedule including the purpose of each round and the intended activities. For some patients, written information was essential, while for others oral information was sufficient:
“If I myself would be more prepared before they come [the ward round], then maybe it would be an even better conversation or dialogue.” [Patient 5]
“If you know that you have five minutes with a doctor, then you can prepare some questions about your prognosis, further treatment, what to do at home, etc.” [Patient 2]
“Yes … you could have a small questionnaire or some paper with examples of questions I could prepare … and explain what the ward round really means … what to ask, what they cannot answer, for example? I do not know that as a patient.” [Patient 13]
The quote below indicates that the patient noticed there were legal aspects that patients should be aware of to fully present their views during their care period.
“Not all hospitals tell me what rights I have as a patient – the patient does not know about their rights. And I think they are important to know so you know what you can wish for, for example, if the situation is sustainable at home or if you need more help.” [Patient 1]
Organization of the Ward Round
The category of organization reflects the patients’ opinions about how the care unit should prepare them for patient-centered ward rounds. The patients wished to see a clear plan for their stay in the ward, with a description of what was planned for their treatment. They wanted to be able to prepare well in advance. The patients found the ward rounds stressful, and they desired more time for conversations – especially with the treating surgeon.
“Hmm … that you introduce the goal early, the purpose to be here [at the hospital] … because then you have the whole concept … not at the end, but at the start … then you understand why.” [Patient 6]
“Explain the ‘schedule’, everything that will happen in which order and with easy-to-understand language.” [Patient 1]
“But it is precisely this that I would like to have documented … because I know that afterwards I will wonder … what was it he said about that … how long was it I was not allowed to sit and when … was I allowed to sit 15 minutes a day, no more, or 15 minutes at a time … ?” [Patient 12]
Communication
Many patients wanted more time for discussions during the ward round. A recurring point of view was the desire to be listened to. Another common desire among patients was for individual visits by clinicians to avoid the presence of too many people at the same time, while others wanted a larger group of professionals for the ward round.
“Mmm … that you listen. Because it is important that there is a space for me to say what I think and feel and that you listen to it.” [Patient 2]
“That the staff has my history and knows what to do and who I am … the information is passed on from staff to staff about what happened last time. Then, I will get treated like a person not just a number.” [Patient 7]
“As a patient, it can be difficult to ask the ‘right’ questions when you are ‘blocked’ … for example, I received a note that I should write down how much I drink. I was not clearly informed about this and thus I forgot to record my drinking.” [Patient 1]
Safety
The patients described their appreciation when staff showed knowledge of their patient history and stressed the importance of the medical staff having access to updated information for maintaining patient safety. Being able to recognize the people who were part of the care team was also described as important for the feeling of security.
“I think time is of the essence. I feel here that all staff categories have time for me.” [Patient 15]
“You lie there pitifully and look up at them [the ward round] and it’s almost … a little yes … you feel a little worried.” [Patient 5]
“The only thing I could think of was that there were so many of them when they came in, that … I’m a person who can be stressed by such a thing … but since everyone is different, some think it’s good when there are six people, I myself become like this ‘Ohhh ohhh’.” [Patient 4]
Strengths and Limitations
A limitation of this study is the patient dropout rate. The reduced number of responses means the results should be treated with caution. For the same reason, there is a risk of bias as patients who did not have the strength or felt ill declined to participate. Another limitation on getting patients to participate may have been the rapid rotation of patients at the ward and their personal difficulties after surgery. Moreover, the patients were interviewed by healthcare students participating in a learning activity, not professional interviewers, so there is of course a risk of coercion and response bias, and a neutral data collector and interviewer may have reduced this risk. Alternatives to handing out physical survey sheets to patients could have been to offer a digital survey or performing the survey and interviews outside of the care period. A later evaluation could also have minimized the possible impact of care dependency after surgery, but this would have hindered the learning activity for the students. A strength of this study is the collaboration with an experienced patient representative, AF, who gave a valuable overview of the patient perspective. Another strength is the interprofessional collaboration within the research group, which made it possible to take full account of the different professional aspects.
Discussion
The aim of this study was, through a learning activity for healthcare students, to explore patients’ perceptions of the ward round and its patient-centered approach.
This study has highlighted a deficit of knowledge among patients concerning the structure, organization, and content of ward rounds. Only a third of the patients in the study was acquainted with the laws and regulations governing patient care, which may explain why the patients felt it was difficult to be fully involved in their own care.
In order to strengthen patients’ legal security, the Swedish Patient Law was created in 2015.2
The law states that healthcare must, as far as possible, be designed and implemented in consultation with the patient, and certain care or treatment measures must be based on the patient’s wishes and individual conditions. Despite this law, patients’ experiences of care according to The Swedish Agency for Health and Care Services Analysis show several shortcomings and few signs of improvement in legal compliance over time.21 If patients are not sufficiently aware of their rights, it is difficult for them to be sufficiently involved in their own care. This is in accordance with a study by Redley et al, in which 31% of patients report an active control preference for participation in decision-making during ward rounds.7
Walton et al also report that the term “ward round” was largely unknown to the patients in their study.6 This can be explained by the fact that the ward round is still carried out in a more or less traditional way, which makes it difficult for patients to participate in it according to their own wishes.
Many patients mentioned the importance of being prepared for the ward round, both in terms of its timing and also by writing down their questions and thoughts to bring up during the ward round. The patients offered some ideas for improvement, including a ward round schedule, activity plan, prepared questions to consider in advance, and an opportunity to convey their own expectations and wishes for the care period. Other studies support these findings as a prerequisite for patients to be able to play an active role in the planning of their care.10 In order to achieve this, it is essential that patients be properly listened to when expressing their views.5,10
In this study, patients called for more time for communication and clear signs that they were being listened to. This is also in line with other studies, where both patients and staff scored communication poorly when assessing quality of care and patient participation.7,12,15 Caregivers may often falsely believe that patients have a clear understanding of the intended aim and content of the ward round, which are not always achieved. Patients may also be prevented from participating in the round due to time constraints and have no opportunity to ask questions or receive explanations of technical information and jargon.7,12 A possible aggravating circumstance is that the responsible surgeon is present in the care ward to a lesser extent during the day due to placement in the operating room or reception, which can reduce the time for communication with patients.
Patients may also be influenced by prevailing traditions and respect for medical staff, in addition to a more general uncertainty about what to wish for.7 By giving examples of what patients may wish for and varying questioning frameworks, the answers may become different and more elaborate. Brown et al report that the use of a surgical check sheet improved ward round communication and was welcomed by a majority of patients (85%)16 because the surgeon was immediately aware of their questions and concerns and could address them. The patients could also formulate questions before the ward round, which bolstered their confidence to ask them.
This study has highlighted differences among the patients regarding how much information they wanted and when. Some patients wanted full information about their case and to be involved in all aspects of their treatment, while others preferred to rely entirely on the staff and did not want to be involved at all. A common request was that information should be given to patients in a clear and understandable form and that they should have enough time to express their questions and concerns. Swenne et al assert that patients’ communication with healthcare professionals is influenced by several interactions such as each patient’s own communication goals, how the patients and physicians address those goals, the ability to put their message across, and the environment in which the communication occurs – all of which can help create a more patient-centered ward round.11
According to the NHS, shared decision-making will become the norm and will be expressed as: “no decision about me, without me”.3 Patients should have access to the information they want, make choices about their own care, and have increased control over their own care records.3 This means that the care process should be tailor-made for each patient. To achieve this and fulfill a patient-centered approach, there must be an organizational and mental shift in the healthcare system and its staff. In the current study, the patients offered several suggestions for the improvement of ward rounds that are valuable to consider.
Conclusion
In this study, less than half the patients felt they could participate in the ward round, which suggests there may be an opportunity for improvement and development in how it is conducted. Better information and communication about legal rights and the structure and content of the ward round could be valuable to patients before admission to help them understand how their individual wishes can be conveyed. To enable a tailor-made ward round for each patient and fulfill a patient-centered approach, both an organizational and mental shift are likely to be necessary.
Acknowledgments
We would like to thank Gunnar Edman for his support with the statistical analysis. We would also like to thank all the patients for taking part in the study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. WHO global strategy on people-centred and integrated health services: interim report; 2015. Available from: https://apps.who.int/iris/handle/10665/155002. Accessed August 12, 2022.
2. Ministry of Social Affairs. The Patient Law (SFS 2014:821), Chapter 5, §§ 1–3. Stockholm, Sweden: Ministry of Social Affairs; 2014.
3. Department of Health. Equity and excellence: liberating the NHS. Cm 7881. DH. 2010.
4. IAPO’s policy statement. Available from: www.iapo.org.uk/patient-information-and-health-literacy.
5. Smith SK, Dixon A, Trevena L, Nutbeam D, McCaffery KJ. Exploring patient involvement in healthcare decision making across different education and functional health literacy groups. Soc Sci Med. 2009;69(12):1805–1812. doi:10.1016/j.socscimed.2009.09.056
6. Walton V, Hogden A, Long JC, Johnson JK, Greenfield D. Patients, health professionals, and the health system: influencers on patients’ participation in ward rounds. Patient Prefer Adherence. 2019;13:1415–1429. doi:10.2147/PPA.S211073
7. Redley B, McTeer L, Botti M, et al. Patient participation in inpatient ward rounds on acute inpatient medical wards: a descriptive study. BMJ Qual Saf. 2019;28:15–23. doi:10.1136/bmjqs-2017-007292
8. Edwards M, Davies M, Edwards A. What are the external influences on information exchange and shared decision-making in healthcare consultations: a meta-synthesis of the literature. Patient Educ Couns. 2009;75(1):37–52. doi:10.1016/j.pec.2008.09.025
9. Tobiano G, Bucknall T, Marshall A, Guinane J, Chaboyer W. Nurses’ views of patient participation in nursing care. J Adv Nurs. 2015;71(12):2741–2752. doi:10.1111/jan.12740
10. Moore L, Britten N, Lydahl D, Naldemirci Ö, Elam M, Wolf A. Axel Wolf Barriers and facilitators to the implementation of person-centered care in different healthcare contexts. Scand J Caring Sci. 2017;31(4):662–673. doi:10.1111/scs.12376
11. Swenne CL, Skytt B. The ward round–patient experiences and barriers to participation. Scand J Caring Sci. 2014;28(2):297–304. doi:10.1111/scs.12059
12. Stalenhag S, Sterner E. Factors that create obstacles and opportunity for patient participation in orthopedic nursing care. J Eur Wound Manag Assoc. 2019;20(1). doi:10.35279/jewma201905.06
13. Reddin G, Davis NF, Donald KM. Ward stories: lessons learned from patient perception of the ward round. Ir J Med Sci. 2019;188(4):1119–1128. doi:10.1007/s11845-019-01975-z
14. Pucher PH, Aggarwal R, Singh P, Tahir M, Darzi A. Identifying quality markers and improvement measures for ward-based surgical care: a semi structured interview study. Am J Surg. 2015;210(2):211–8. 27. doi:10.1016/j.amjsurg.2014.11.013
15. Pucher PH, Aggarwal R, Darzi A. Surgical ward round quality and impact on variable patient outcomes. Ann Surg. 2014;259(2):222–226. doi:10.1097/SLA.0000000000000376
16. Brown O, Toi TH, Barbosa PR, Pookarnjanamorakot P, Trompeter A. A patient-centered check sheet improves communication on the trauma ward round. Br J Hosp Med. 2019;80(8):472–475. doi:10.12968/hmed.2019.80.8.472.
17. Schuur K, Murray K, Maran N, Flin R, Paterson-Brown S. A Ward-Round Non-Technical Skills for Surgery (WANTSS) taxonomy review. J Surg Educ. 2020;77(2):369–379. doi:10.1016/j.jsurg.2019.09.011
18. Read J, Perry W, Rossaak JI. Ward round checklist improves patient perception of care. Randomized controlled trial. ANZ J Surg. 2021;91(5):854–859. doi:10.1111/ans.16543
19. Swedish national patient survey. Available from: https://resultat.patientenkat.se/Specialiserad%20sjukhusv%C3%A5rd%20sluten/2021.
20. Graneheim UH, Lundman B. Qualitative content analysis in nursing research: concepts, procedures, and measures to achieve trustworthiness. Nurse Educ Today. 2004;24:105–112. doi:10.1016/j.nedt.2003.10.001
21. Assessment of the Swedish Patient Act. 2014–2017. Available from: https://www.vardanalys.se/in-english/reports/act-without-impact/.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.