Back to Journals » Clinical Ophthalmology » Volume 19
The Value of Patient-Reported Questionnaires in Detecting Ocular Surface Manifestations in Dupilumab Therapy: A Case-Control Study
Authors Teixeira-Martins R ![]() , Araújo C, Faria Pereira A
, Araújo C, Faria Pereira A ![]() , Coelho-Costa I
, Coelho-Costa I ![]() , Rocha-Sousa A
, Rocha-Sousa A ![]() , Plácido JL, Pinheiro-Costa J
, Plácido JL, Pinheiro-Costa J ![]() , Lima-Fontes M
, Lima-Fontes M ![]()
Received 7 July 2025
Accepted for publication 11 September 2025
Published 22 October 2025 Volume 2025:19 Pages 3869—3880
DOI https://doi.org/10.2147/OPTH.S552197
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Rita Teixeira-Martins,1 Célia Araújo,1,2 Ana Faria Pereira,1 Inês Coelho-Costa,1 Amândio Rocha-Sousa,1,3 Jose Luís Plácido,4 João Pinheiro-Costa,5 Mário Lima-Fontes1,3
1Department of Ophthalmology; São João Local Health Unit, Porto, Portugal; 2Faculty of Medicine; University of Porto, Porto, Portugal; 3Department of Surgery and Physiology, Faculty of Medicine; University of Porto, Porto, Portugal; 4Department of Immunoallergology, São João Local Health Unit, Porto, Portugal; 5Department of Biomedicine, Faculty of Medicine, University of Porto, Porto, Portugal
Correspondence: Rita Teixeira-Martins, São João Local Health Unit, Porto, 4202-451, Portugal, Email rita.teixeira.martins@[email protected]
Purpose: Dupilumab-associated ocular surface disease (DAOSD) is a reported side effect with several manifestations and uncertain risk factors. This study uses objective assessments and a patient-reported questionnaire to evaluate ocular surface disease (OSD) in Dupilumab-treated patients.
Methods: A case-control study at São João Local Health Unit (ULS São João), Porto, Portugal, included 58 Dupilumab-treated adults categorized by the DAOSD Questionnaire. Cases (Group A, n=40) had ≥ 3 symptoms or ≥ 1 severe symptom, while controls (Group B, n=18) had < 3 symptoms without daily impact. Ocular surface parameters were assessed, including eye redness score, non-invasive break-up time (NIBUT), tear meniscus thickness, tear film stability evaluation (TFSE®), and tear osmolarity. The Ocular Surface Disease Index (OSDI) classified symptom severity.
Results: Group A had significantly higher tear osmolarity (303.43± 7.61 vs 293.31± 5.11 mOsm/L, p< 0.001) and eye redness (2.00 (1.00) vs 1.00 (1.00) points, p= 0.036). TFSE values were higher (252.76± 3.30 vs 138.74± 3.43 points, p=0.094), while NIBUT was lower (1.00 (4.00) vs 6.50 (10.00) s, p=0.078). Conjunctivitis was more frequent in Group A (57.50% vs 33.33%, p= 0.089), followed by posterior blepharitis (40.00% vs 5.56%, p= 0.008). OSDI scores had significantly different mean in Group A (27.32± 20.24 vs 2.11± 3.24 points, p< 0.001), with 37.5% exhibiting severe disease classification.
Conclusion: DAOSD is associated with increased symptom burden. The DAOSD questionnaire correlated with OSDI scores and ocular surface changes, supporting its role in early detection and referral for ophthalmological management.
Keywords: dupilumab, ocular surface disease, atopic dermatitis, tear osmolarity, conjunctivitis
Introduction
Dupilumab (Dupixent®) is a human monoclonal IgG4-based antibody that acts as an antagonist of the interleukin-4 (IL-4) receptor alpha chain (IL-4Rα), thereby inhibiting IL-4 and IL-13 signaling-key drivers of type 2 inflammation.1,2 It is approved for treating moderate-to-severe atopic dermatitis (AD), severe asthma (SA) with type 2 inflammation, chronic rhinosinusitis with nasal polyps (CRSwNP), nodular prurigo (NP), and eosinophilic esophagitis (EoE) in different age groups.3
Ocular symptoms such as redness, pruritus, tearing, dryness, irritation, discharge, photosensitivity, blurred vision, a foreign body sensation, and pain are commonly reported in patients treated with Dupilumab. These symptoms are now collectively recognized as Dupilumab-Associated Ocular Surface Disease (DAOSD).1,4 This condition includes different inflammatory ocular manifestations, such as severe follicular conjunctivitis, limbal nodules, cicatricial ectropion, keratitis, dry eye disease, and blepharoconjunctivitis.5
Each Dupilumab indication may influence the risk of DAOSD among users. Notably, DAOSD has been predominantly reported in clinical trials involving AD patients, with little to no cases documented in non-AD trials. Its incidence appears to be higher in this population, reaching 25.1% in prospective studies and 20.6% in real-life retrospective studies.6,7
The pathophysiology of DAOSD remains unclear, with several hypotheses proposed.8 The blocking effect of Dupilumab on IL-4 and IL-13 leads to impaired function of conjunctival goblet cells (GCs) in Mucin 5AC (MUC5AC) production, further increasing the risk of ocular surface inflammation.9 Supporting this, a study showed that tear production, assessed by the Schirmer test, remained stable or even increased in AD patients treated with Dupilumab. Specifically, the median Schirmer value increased from 15 mm (interquartile range (IQR):12–21) at baseline to 18 mm (IQR: 11–27) after 28 weeks of Dupilumab treatment. In contrast, tear break-up time (TBUT) slightly decreased during treatment, with median TBUT reducing from 8 seconds (IQR: 5–10) at baseline to 7 seconds (IQR: 4–10) after 28 weeks. Therefore, it is hypothesized that the dry eye sensation, a hallmark symptom of DAOSD, is not due to insufficient tear production but rather to reduced mucus secretion by GCs and/or Meibomian gland dysfunction.10
DAOSD can trigger a vicious cycle in which chronic inflammation accelerates severe ocular complications, including corneal scarring, corneal neovascularization, and recurrent corneal erosion syndrome. In those cases, corneal transplantation may be necessary to prevent irreversible vision loss.6 Approximately 4.5% of patients with DAOSD discontinued Dupilumab treatment.7 Despite its significance in enhancing patients’ quality of life by controlling the primary disease, Dupilumab’s association with DAOSD underscores the importance of early recognition and management of these ocular manifestations. In this context, the use of a patient-reported questionnaire is particularly relevant, as there remains a gap in simple, validated tools for early detection. Incorporating patient perspectives supports a multidisciplinary approach to care.
This case-control study aims to characterize the affected population based on clinical presentation and to assess its impact on noninvasive ocular surface parameters. Additionally, it explores the feasibility and relevance of implementing specific guidelines at São João Local Health Unit (ULS São João) and potentially in other health units to mitigate DAOSD’s impact and minimize disruptions associated with Dupilumab therapy.
Materials and Methods
A case-control study was conducted at the Ophthalmology Department of ULS São João, Porto, Portugal.
Adult patients (aged ≥18 years) who were receiving or had previously received Dupilumab were identified through pharmacy records at ULS São João. A questionnaire (Appendix 1), adapted from the DAOSD Activity Assessment Questionnaire, was administered via telephone to select patients for a noninvasive ocular surface evaluation based on predefined inclusion and exclusion criteria. Patients who had discontinued Dupilumab treatment or declined ophthalmology assessment were excluded. Based on the questionnaire’s scoring system, patients were then categorized into case and control groups (Figure 1). Cases (Group A) included patients reporting three or more ocular symptoms, regardless of their impact on daily life, or at least one symptom with a severity score of five or higher. Controls (Group B) comprised patients reporting fewer than three ocular symptoms and no impact on daily life (severity score of zero).
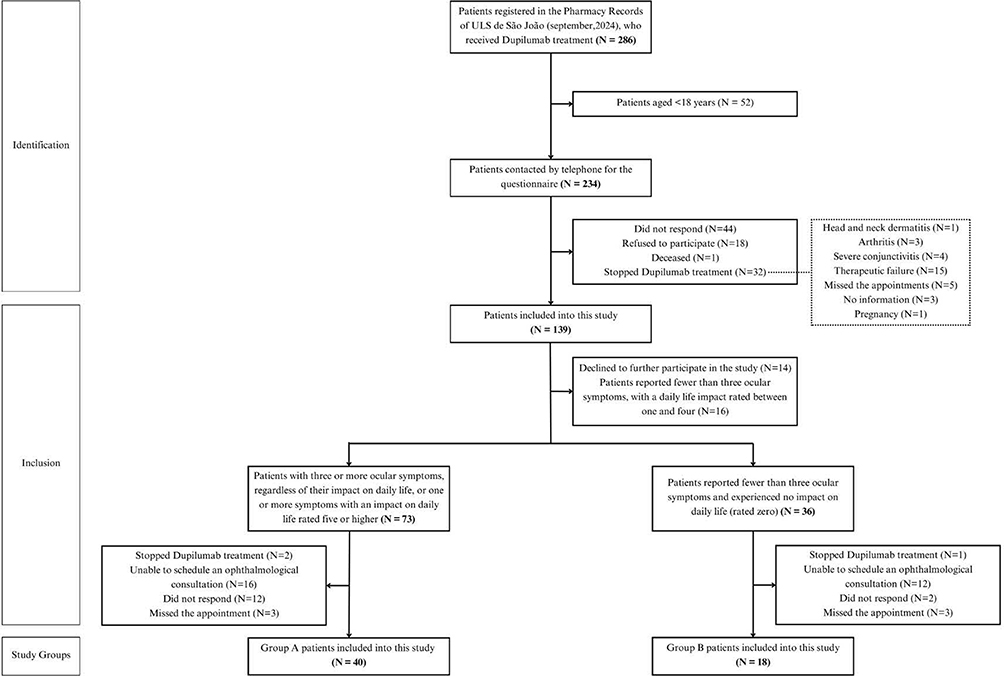 |
Figure 1 Flowchart of the study design. |
The ophthalmological examination included best-corrected visual acuity (BCVA), tear osmolarity using the ScoutPro®, biomicroscopy, and the use of the TearCheck® device (ESW Vision, Linz, Austria), for assessment of the eye redness score, non-invasive break-up time (NIBUT), tear meniscus thickness (TMT) and tear film stability evaluation (TFSE®). BCVA was measured using Snellen charts and converted to decimal notation for analysis. The most symptomatic eye was selected for assessment. In cases where both eyes exhibit identical symptomatology, the right eye is systematically chosen as the default for examination. Investigators were blinded to the participant’s group allocation to ensure unbiased classification. Additionally, patients were instructed to discontinue the use of contact lenses and ocular topical medications at least one week before the examination.
Eye redness was classified using a scale from 1 to 4 based on reference images provided by the device. NIBUT was measured on a scale ranging from 2 to 10 seconds. Investigators predefined that values below this range would be recorded as 1 second, while values above 10 seconds would be classified as 11 seconds. The device measures both the thickest point and the thickness below the iris center. For this study, only the thickest point was considered since the thickness below the iris was not always available. The tear film instability, assessed by TFSE, reflects the micro-deformations occurring on the ocular surface over a 10-second interval, with higher scores indicating greater instability. Cases in which dots were detected outside the ocular surface were excluded from the analysis.11
In addition, all patients completed a second questionnaire (Appendix 2) covering Dupilumab treatment, past or current ophthalmological conditions, use of ophthalmic medication, and the presence or absence of symptoms, assessed using the Portuguese-validated Ocular Surface Disease Index (OSDI).12 The OSDI questionnaire consists of 12 items divided into three subscales: ocular symptoms, vision-related function, and environmental triggers. Each item is rated on a five-point scale, ranging from “none of the time” (0 points) to “all the time” (4 points). If a question does not apply to the patient, the “N/A” option can be selected. The global score is calculated by summing the points for all responses, multiplying the total by 25, and dividing by the number of valid answers. This results in a score ranging from 0 to 100 points, which is then used to classify patients as having a normal ocular surface (0–12 points), mild disease (13–22 points), moderate disease (23–32 points), or severe disease (33–100 points).13
Clinical characteristics were collected from the questionnaire and electronic health records. We also collected demographic data, including gender, age, indication, the average duration of treatment with Dupilumab, and the use of ophthalmologic treatment. No a priori sample size calculation was conducted, as the study cohort was defined by the availability and consecutive inclusion of all eligible individuals seen during the study period.
The study was approved by the Ethics Committee of ULS São João (project no. 325/2024) and was conducted under the principles of the Helsinki Declaration. All patients provided informed consent for the analysis and publication of the collected data.
Statistical analysis was performed using IBM SPSS Statistics software, version 29 (IBM®, Chicago, IL). Different statistical tests were performed to compare differences between groups: Chi-square tests for categorical variables, Student’s t-test for parametric continuous variables, and Mann–Whitney U-tests for non-parametric continuous variables. When chi-square tests involved multiple comparisons, p-values were adjusted using the Bonferroni correction. Frequencies and percentages were used to describe qualitative variables. In contrast, quantitative variables were presented as mean (standard deviation) when normally distributed or median with IQR for non-normally distributed continuous variables. A p-value < 0.05 was considered statistically significant.
Results
Patients were divided into case (Group A) and control (Group B) groups based on a score sheet adapted from the DAOSD Activity Assessment Questionnaire. The questionnaire results, detailed in Table 1, showed a statistically significant difference between the groups across all answers.
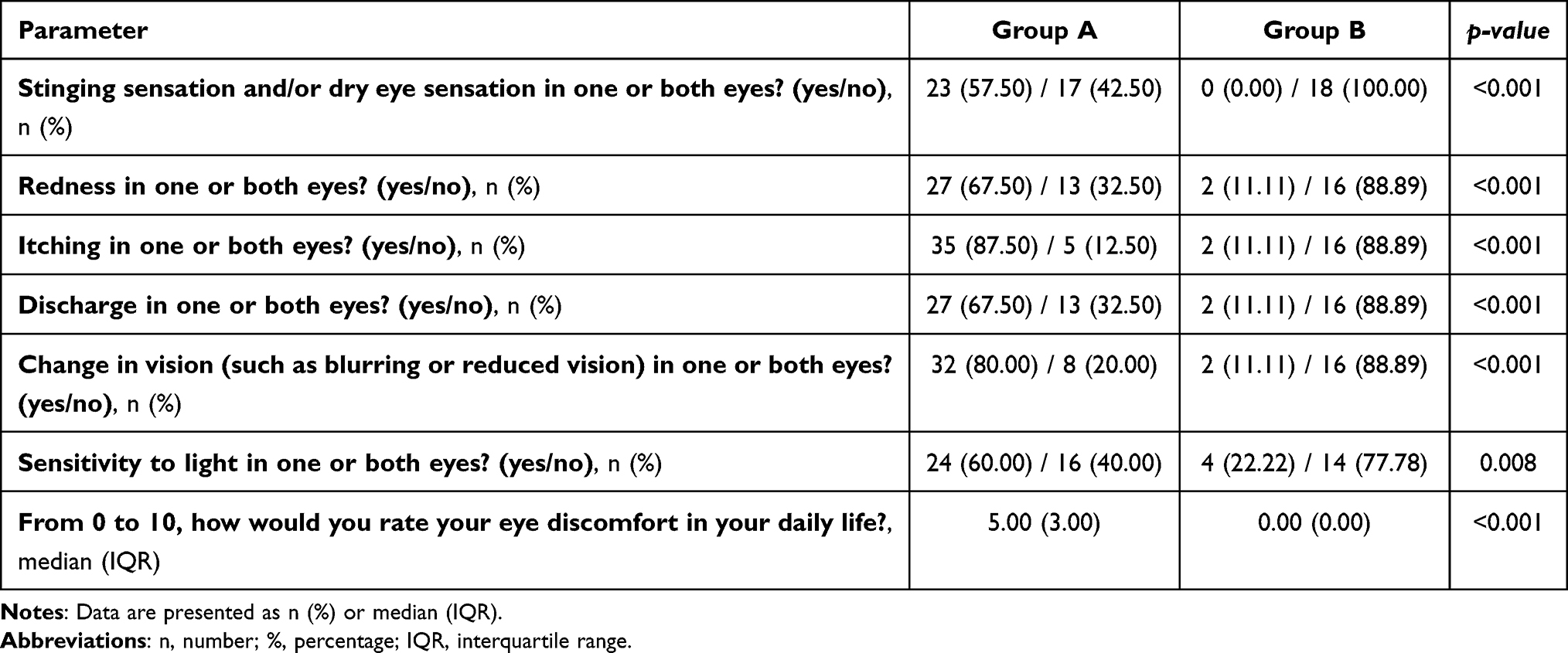 |
Table 1 Comparison of Ocular Symptoms Prevalence and Their Impact on Daily Life Between Group A and Group B |
A total of 58 patients were included: 40 in Group A and 18 in Group B. The mean age was 45.3 ± 14.8 years in Group A and 49.6 ± 16.7 years in Group B. Group A included 21 males and 19 females, while Group B had 11 males and 7 females. The primary indication for Dupilumab was moderate-to-severe AD in 55.0% of Group A and 27.8% of Group B. SA accounted for 20.0% of Group A and 11.1% in Group B, while CRSwNP accounted for 20.0% in Group A and 50.0% in Group B. NP was the indication in 5.0% of Group A and 5.6% of Group B, whereas EoE was reported in 5.6% of Group B. The mean treatment duration was 777.4 ± 1.6 days in Group A and 659.6 ± 1.7 days in Group B. No significant differences were observed between the groups regarding age, gender, treatment indication, or mean Dupilumab treatment duration. No chronic ocular diseases were reported in either group, and most patients only mentioned the use of glasses. However, regarding recent ophthalmic treatments, self-reported use of artificial tears during the week preceding the ophthalmological examination was 35.0% in Group A, while the use of topical corticosteroids was reported by 17.5% of Group A and 5.6% of Group B. These differences were statistically significant (p = 0.011), as shown in Table 2.
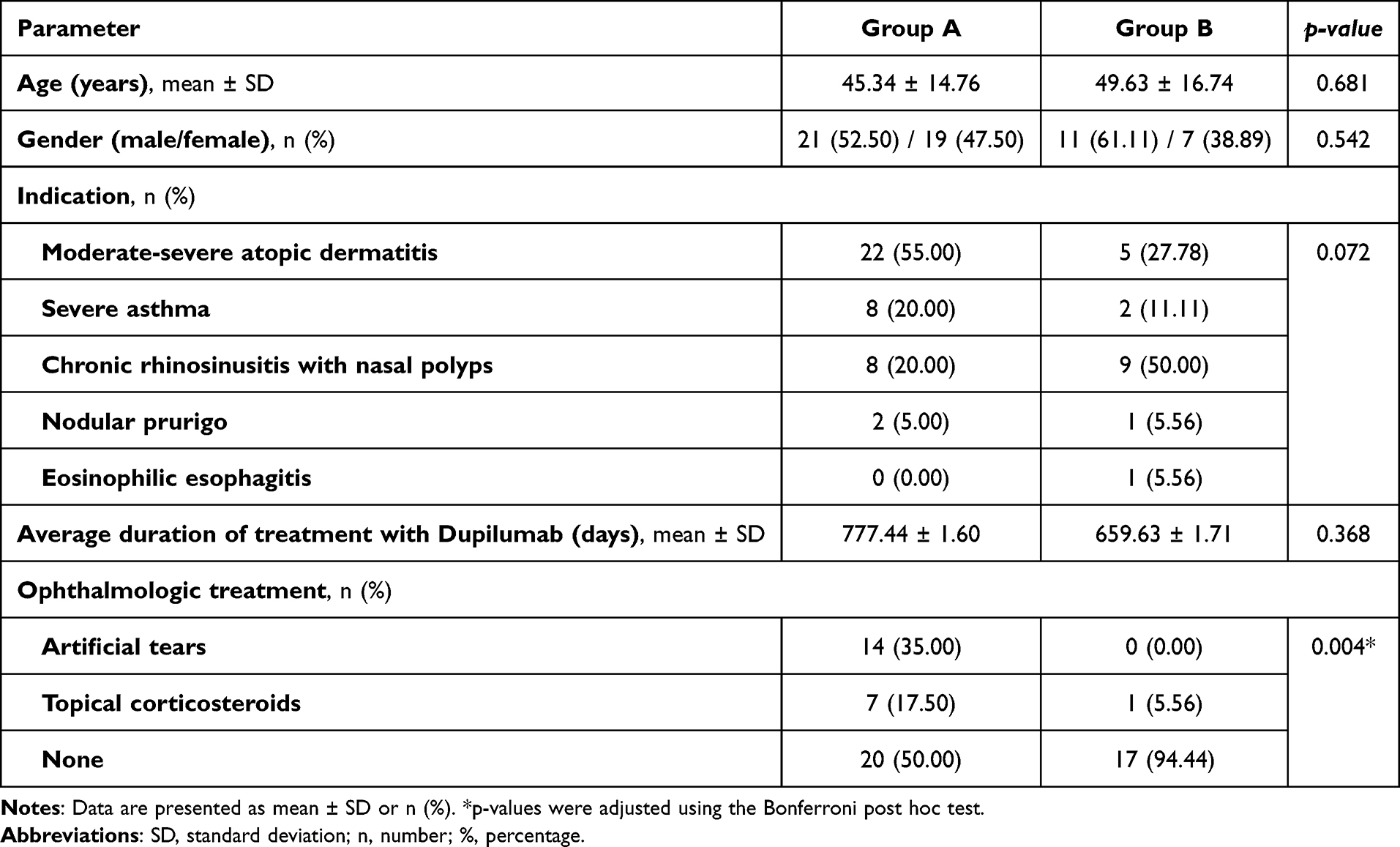 |
Table 2 Comparison of Age (Years), Gender, Indication, Average Duration of Treatment with Dupilumab and Ophthalmologic Treatment Between Group A and Group B |
Regarding ocular surface parameters (Table 3), tear osmolarity (p < 0.001) and eye redness (p = 0.036) were significantly different in Group A than in Group B. The mean tear osmolarity was higher in Group A (303.43 ± 7.61 mOsm/L) compared to Group B (293.31 ± 5.11 mOsm/L). Similarly, the median eye redness score was higher in Group A (2.00 (1.00) points) than in Group B (1.00 (1.00) points). TMT showed no significant difference between groups, with mean values of 0.74 ± 0.24 mm in Group A and 0.78 ± 0.22 mm in Group B (p = 0.538). NIBUT was lower in Group A, with a median of 1.00 (4.00) seconds, compared to 6.50 (10.00) seconds in Group B; however, this difference was not statistically significant (p = 0.078). Similarly, TFSE was higher in Group A, with a mean of 252.8 ± 3.3 points compared to 138.7 ± 3.4 points in Group B; however, this difference did not reach statistical significance (p = 0.094). Figures 2, 3 and 4 show examples of the eye redness scale, TMT, NIBUT, and TFSE measurements.
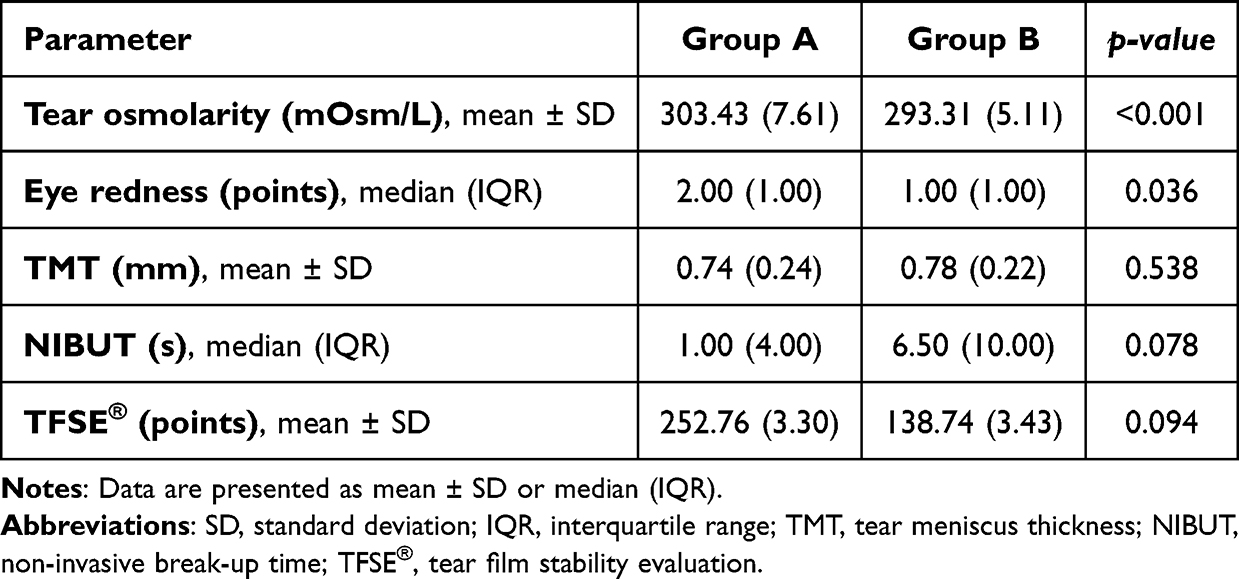 |
Table 3 Comparison of the Various Parameters Evaluated During the Ophthalmological Examination Between Groups A and B |
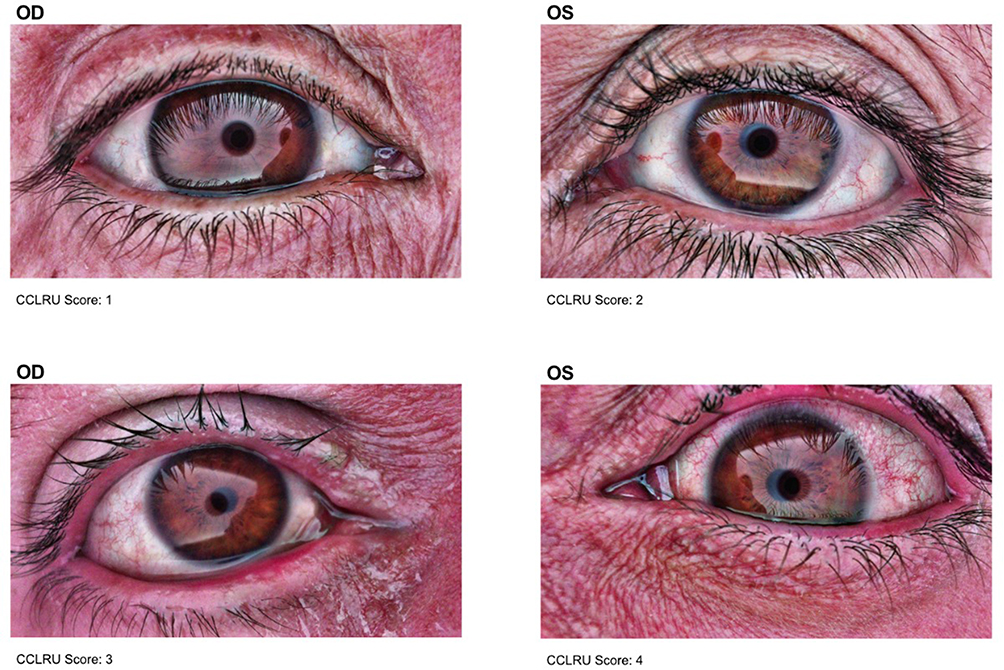 |
Figure 2 The degree of redness is determined by evaluating the visibility of small blood vessels on the ocular surface. Eyes were classified into four grades (1 to 4) based on increasing vessel prominence, respectively. |
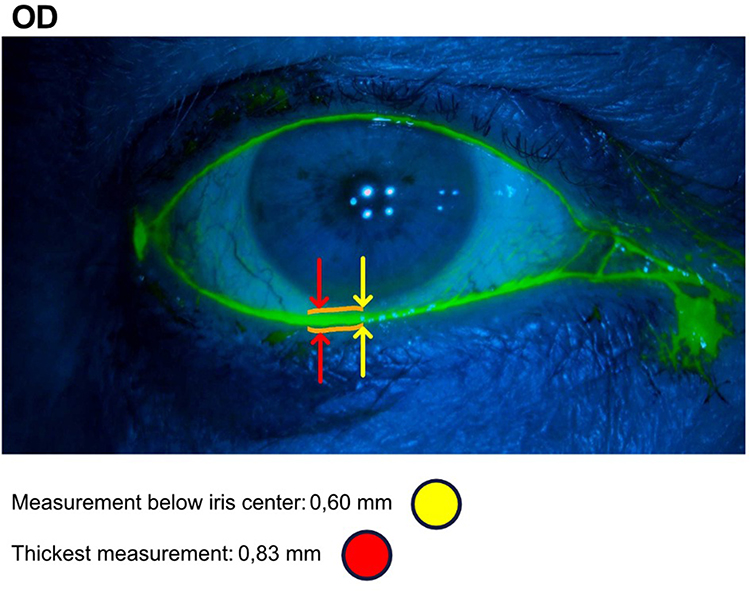 |
Figure 3 Example of tear meniscus thickness assessment: Defined as the height of the tear film at the midpoint of the lower eyelid. For analysis, only the thickest measurement was considered, as values below the iris center were not always available. |
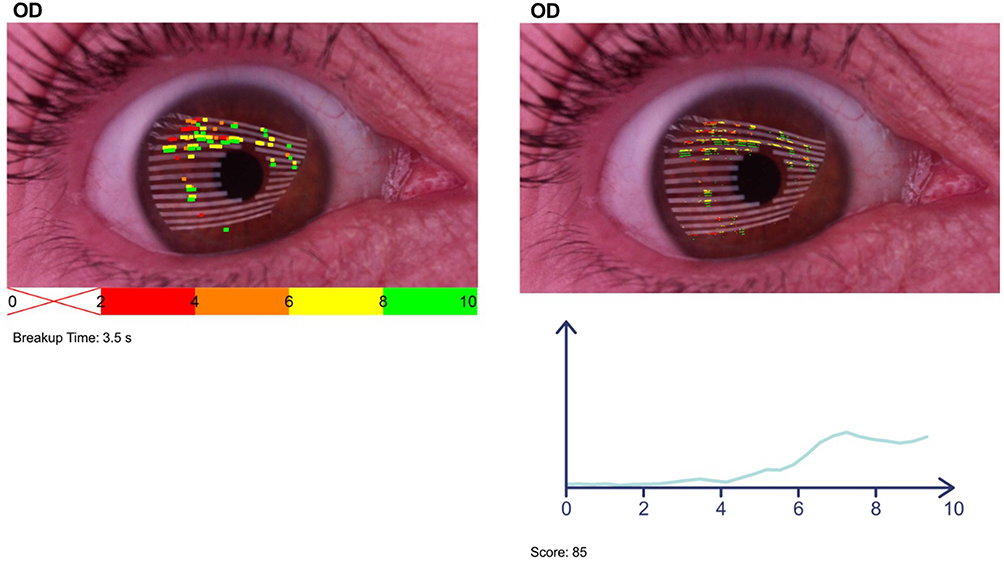 |
Figure 4 Examples of non-invasive breakup time (NIBUT) and tear film stability (TFSE®) assessment (left and right pictures, respectively). NIBUT identifies the location and timing of tear film rupture, while TFSE® evaluates micro-deformations on the tear film surface, indicating instability. Based on these parameters, patients are classified into four groups. This example represents the second group, characterized by a notable presence of micro-deformations, primarily occurring towards the end of the 10-second acquisition period. |
Concerning the ocular surface biomicroscopy findings observed during ophthalmological examination (Table 4), posterior blepharitis and bulbar conjunctivitis were identified in 40.0% and 57.5% of patients in Group A, respectively, compared to 5.56% and 33.3%, respectively, in Group B. Additionally, chalazion was identified in 2.5% in Group A and 5.56% in Group B. In Group A, limbal neovascularization was present in 10.0% of cases, while ectropion and madarosis were observed in 5.0% and temporal episcleritis in 2.5%; none of these conditions were reported in Group B. Only posterior blepharitis showed a significant difference between groups (p = 0.008). The median BCVA in the most symptomatic eye was 0.9 (0.1) in Group A and 0.95 (0.1) in Group B, with no statistically significant difference (p = 0.315).
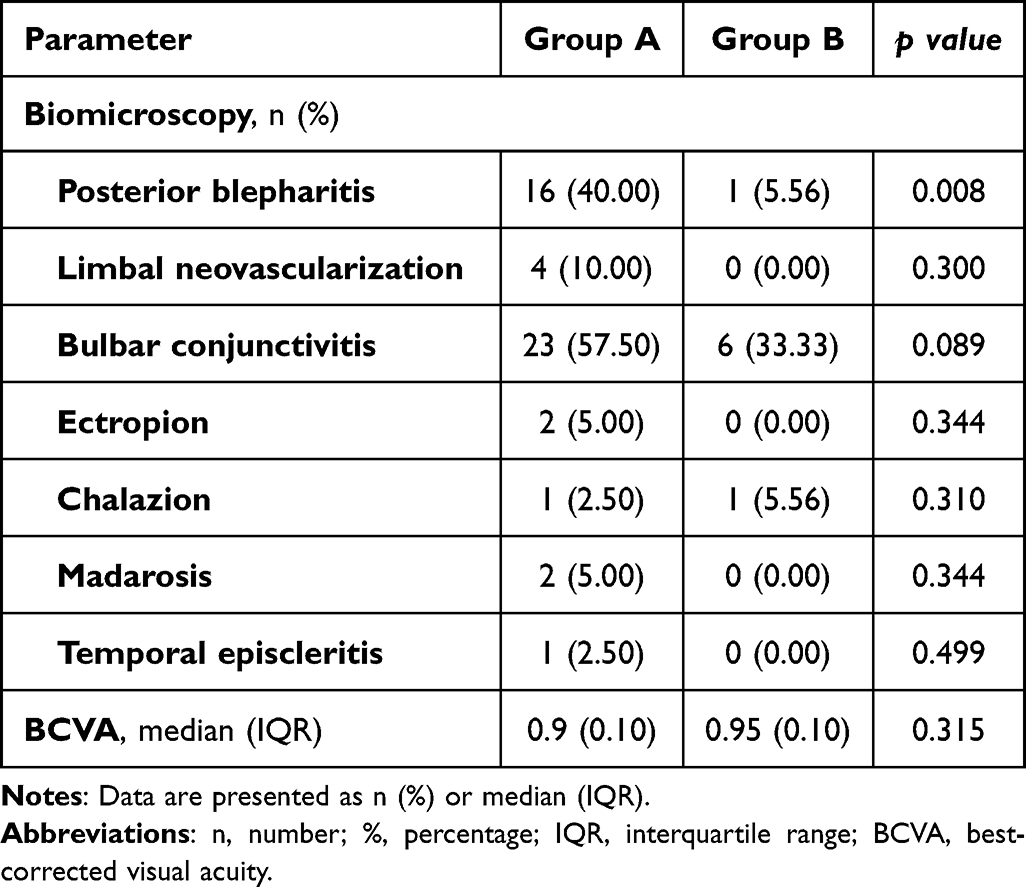 |
Table 4 Comparison of Ocular Surface Biomicroscopy Findings Observed During Ophthalmological Examination Between Groups A and B |
In assessing ocular symptoms, Group A had a significantly higher mean OSDI score than Group B (27.32 ± 20.24 vs 2.11 ± 3.24 points, p < 0.001). The severity of ocular symptoms in both groups, as determined by the OSDI score, is detailed in Table 5. A significantly higher proportion (100%) of patients in Group B had a normal ocular surface classification, whereas in Group A, 37.5% of patients exhibited severe ocular surface classification (p < 0.001).
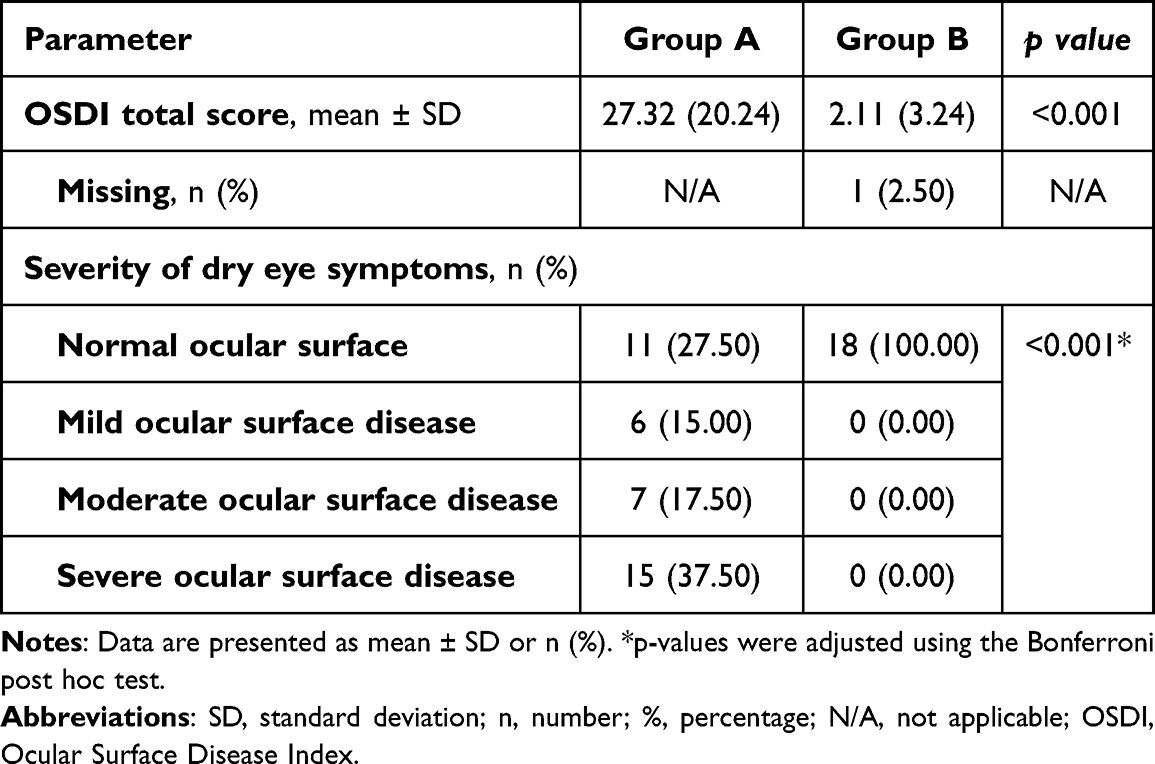 |
Table 5 Comparison of the OSDI Score and the Severity of Dry Eye Symptoms Between Groups |
After initiating Dupilumab treatment, 45.0% of patients in Group A sought emergency care for ocular symptoms, whereas none in Group B did (p < 0.001). Among Group A patients, the time from treatment initiation to symptom onset varied: 2.5% within 2–4 weeks, 10.0% within 1–3 months, 5% within 3–6 months, 17.5% within 6–12 months, and 10.0% within 1–3 years. Furthermore, as indicated in Table 6, all symptomatic patients (45.0%) in Group A needed ophthalmological care for ocular surface complaints; however, half of them reported that their symptoms persisted after the recommended treatment.
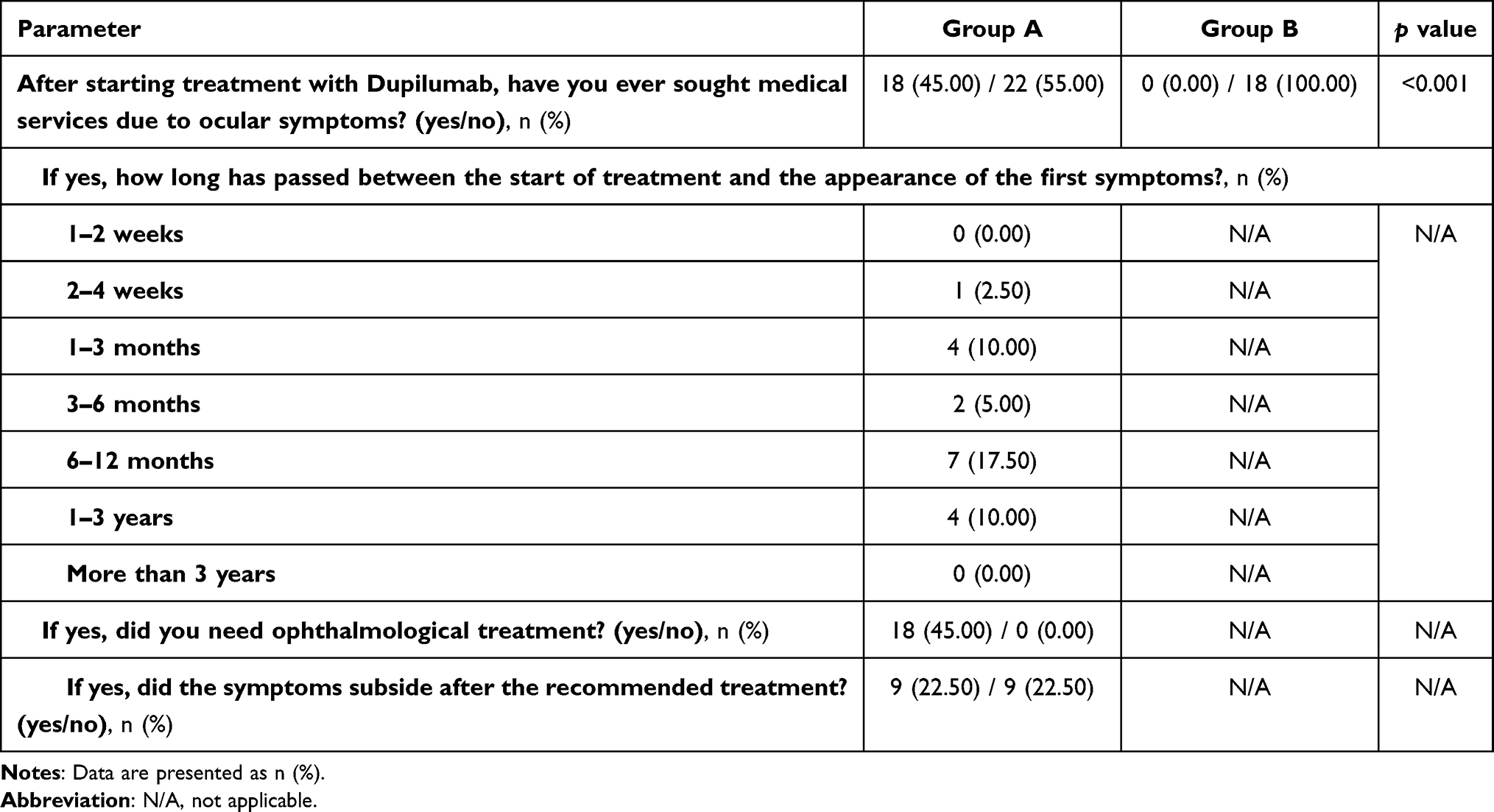 |
Table 6 Comparison of Medical Visits Related to Ocular Symptoms Between Group A and Group B Following Dupilumab Treatment |
Additionally, the reasons for discontinuing Dupilumab treatment during the identification phase of the study included side effects in 25% of patients, with 12.5% reporting severe conjunctivitis, 9.4% having arthritis, and 3.1% having head and neck dermatitis (Table 7).
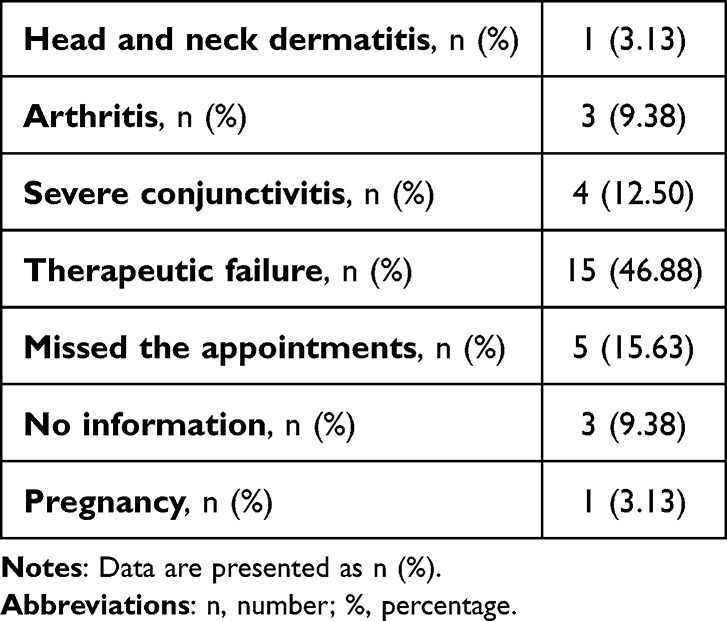 |
Table 7 Reasons for Discontinuation of Dupilumab Treatment During the Identification Phase |
Discussion
Dupilumab is a valuable treatment option for moderate-to-severe AD when topical treatments are insufficient or unsuitable, as well as for SA with type 2 inflammation that remains uncontrolled despite high-dose inhaled corticosteroids and another controller medication. Additionally, adults with CRSwNP who have not achieved adequate relief with systemic corticosteroids and/or surgery may also benefit from Dupilumab.14 Phase 3 clinical trials have demonstrated that Dupilumab improved pruritus, feelings of anxiety and depression, and quality of life compared to placebo. These benefits were not short-lived, as longer-term studies have shown that Dupilumab’s benefits are sustained over time.15
The DAOSD Activity Assessment Questionnaire & Scoring Sheet was adapted to assess DAOSD and successfully identified prevalent ocular symptoms. In agreement with the results of similar studies, the most common symptoms were itching (87.50%) and blurry vision (80.00%).10 The tool’s effectiveness in assessing DAOSD was manifested by statistically significant differences between the case and control groups when all responses were compared. Appropriate demographic and treatment-related variables, such as gender distribution, age, nature of indications for treatment, and duration of Dupilumab therapy, did not significantly differ between groups. This suggests that variations in questionnaire responses are primarily due to the presence and severity of DAOSD, rather than confounding demographic or clinical factors.
Ocular adverse effects were reported in up to 22.1% of AD clinical trials, whereas incidence rates were lower in asthma, CRSwNP, and EoE trials (1.7%).16 Consistent with our findings, AD patients in Group A had a higher incidence of ocular symptoms (55.0%) compared to other conditions treated with Dupilumab. In contrast, CRSwNP was the most prevalent condition in the control group (50.0%). Although the difference was not statistically significant, this trend warrants further investigation into the potential risk of ocular adverse events in AD patients receiving Dupilumab. Future studies with larger cohorts should also include subgroup analyses by underlying disease to determine whether specific conditions confer a higher risk of DAOSD.
Group A exhibited significantly higher tear osmolarity, ocular redness scores, and TFSE. In contrast, Group B showed a trend toward higher tear meniscus thickness and NIBUT, though the differences were not statistically significant. These findings align with the proposed pathophysiology of DAOSD. Tear osmolarity reflects the concentration of solutes in the tear film and is an important biomarker for ocular surface damage, inflammation, and instability of the tear film in dry eye disease (DED).17 In our study, tear osmolarity was significantly elevated in Group A (303.43 mOsm/L vs 293.31 mOsm/L, p < 0.001), supporting the presence of tear film instability and ocular surface dysfunction in patients with DAOSD.
Three layers comprise the tear film: the GCs produce the mucus layer, the lacrimal gland produces the aqueous layer, and the Meibomian glands provide the lipid layer.18 Although not statistically significant, the trend toward higher TMT and NIBUT in Group B suggests that DAOSD is more likely related to meibomian gland dysfunction or decreased mucus secretion by GC rather than insufficient aqueous tear production. Atchen et al10 reported that in patients who developed DAOSD, the number of GCs remained stable compared to their baseline levels. However, flow cytometry analysis revealed a significant reduction in CK19-CD45-MUC5AC+ cells after 4 and 28 weeks of Dupilumab treatment, indicating a decline in functional GCs. Since CK19-CD45-MUC5AC+ cells are a marker of GC activity, these findings suggest that Dupilumab impairs GC function rather than reducing their overall number. Serino et al19 observed reduced NIBUT with preserved tear volume measured by the Schirmer test and TMT, reinforcing that DAOSD primarily reflects ocular surface inflammation and tear film instability rather than aqueous deficiency. Elevated osmolarity and ocular redness, both hallmarks of ocular surface inflammation, further support the model in which DAOSD primarily results from GC dysfunction and meibomian gland involvement. Since tear film stabilization with artificial tears or lipid-based formulations may be insufficient, treatment should focus on reducing ocular inflammation with topical corticosteroids or cyclosporine in severe cases.10
Injection site responses, head and neck dermatitis, hypereosinophilia, arthritis, and ocular complications — specifically, DAOSD, which includes blepharitis, conjunctivitis, keratoconjunctivitis, keratitis, or dry eye syndrome — are typical side effects of Dupilumab treatment.20 Severe ocular adverse events are rare, but they have been reported, especially in long-term Dupilumab users. For instance, after receiving Dupilumab for AD for 57 months, a healthy 56-year-old man developed bilateral limbal stem cell deficiency and widespread diffuse symblepharon that affected his extraocular movements.21 In our study, the most prevalent surface alterations observed in Groups A and B were posterior blepharitis in 40.0% and 5.56% and bulbar conjunctivitis in 57.5% and 33.3%, respectively. Clinical trials have reported conjunctivitis in 6–15% of adults treated with Dupilumab, compared to 0.9–10.9% in placebo groups. Real-world data from 14 studies indicate a significantly higher incidence, with conjunctivitis occurring in 26.1% of 908 AD patients, along with an increased prevalence of dry eye symptoms.22 While most studies did not specify conjunctivitis subtypes, they generally described it as manageable and not requiring treatment discontinuation; however, 4.2% of patients discontinued Dupilumab due to noninfectious ocular disease.23 In our study, 25% of patients discontinued treatment due to adverse effects, with severe conjunctivitis accounting for half of these cases (12.5%). Despite its high prevalence, predicting which patients will develop conjunctivitis during Dupilumab treatment remains challenging. A history of allergic conjunctivitis appears to increase the risk.24 There were also reports of other ocular adverse effects. Keratitis was reported in 6.2%, and blepharitis was reported in 9.6%.23
Regarding OSDI score, Group A patients had a significantly higher mean OSDI score than Group B patients (27.32 vs 2.11 points, p < 0.001), indicating more frequent and severe ocular discomfort, dryness, and visual disturbances. The strong association between Dupilumab use and ocular surface disease (OSD) is evident, as 37.50% of Group A patients had severe OSD. Furthermore, the presence of more severe symptoms correlates with a higher OSDI score and alterations in ocular surface parameters. This suggests that validated questionnaires, such as the DAOSD Activity Assessment Questionnaire & Scoring Sheet, are valuable screening tools for colleagues in other specialties who manage these patients. Performing these assessments before starting Dupilumab treatment and during follow-ups can help identify those who should be promptly referred to Ophthalmology. These results also reinforce that ocular surface disease in DAOSD can progress to clinically relevant degrees if not managed earlier.
In our study, ocular symptoms led 45% of Group A patients to seek emergency care. Although severe ocular complications often lead to Dupilumab discontinuation, many affected patients are not promptly referred to an ophthalmologist for evaluation and treatment. A study found that only 65% of the 20% of AD patients and none of the 17.6% of SA patients who discontinued Dupilumab due to ocular complications were referred for ophthalmologic evaluation. Among AD patients who experienced adverse events but continued Dupilumab, 31% were referred to an ophthalmologist, and 86.3% of these received one or more ophthalmic treatments. Similarly, 82.4% of SA patients with ocular adverse events continued Dupilumab, with 64.3% receiving ophthalmic treatment and only 28.6% being referred to an ophthalmologist.8 Given these findings, a multidisciplinary collaboration with ophthalmologists is crucial to improving DAOSD management. A coordinated approach may help patients achieve better control of their primary systemic disease while ensuring appropriate ocular care.
Although we report some interesting findings, it is essential to acknowledge that our study has limitations that should be noted. Firstly, the limited sample size might have reduced the statistical power to detect significant differences for some parameters and could limit the generalizability of our findings. Secondly, the composition of the control group, which included dupilumab-treated patients with fewer than three ocular symptoms and no impact on daily life, rather than patients with AD, SA, CRSwNP, NP, or EoE who were not receiving dupilumab therapy, limits causal conclusions. This choice was made due to the high prevalence of these conditions and the availability of multiple treatment options. Our results would be further strengthened by a prospective design with a control group and standardized, repeatable techniques. Given the retrospective nature of the study, it is not possible to determine whether some patients had pre-existing undiagnosed ocular surface disease or if dupilumab contributed to increased susceptibility to chronic inflammation. Thirdly, the exclusion criteria could have been more exhaustive. Even after controlling significant systemic and ocular disorders, the study sample may have been further refined by excluding other factors such as the use of contact lenses, topical lubricants, or other ocular treatments like prior corneal or refractive laser surgery. To minimize this limitation and potential biases, we employed a randomized selection process and instructed patients to stop using contact lenses or ocular topical medications at least one week before the examination. This measure reduces, though may not fully eliminate, the possibility of residual effects on the ocular surface. Fourthly, additional investigative methods, such as meibography, could have provided further insight into the structural changes of the meibomian glands. However, the subjective nature of interpretation, the need for operator expertise, and the possibility of image quality variations limit its application. Despite these challenges, meibography could be a valuable tool for identifying glandular alterations in various ocular surface diseases, ultimately aiding in their management.
In conclusion, this case-control study shows that patients with a higher burden of symptoms present corresponding ocular surface alterations during Dupilumab therapy, not only among those with AD but also in patients treated for other indications. DAOSD can reduce quality of life and, in some cases, may necessitate treatment discontinuation. These findings highlight the value of patient-reported questionnaires in complementing objective measures for the early detection of DAOSD. Importantly, such questionnaires may also have applicability in non-ophthalmic settings, such as dermatology and allergy clinics, where early symptom screening could facilitate timely referral for ophthalmologic assessment. This approach may enable earlier diagnosis and intervention, thereby reducing the risk of treatment interruption.
Moreover, these results support the development of a practical algorithm based on ocular findings, which could represent a major step forward in establishing a multidisciplinary approach, particularly involving ophthalmologists, to ensure adequate ocular care while maintaining the systemic benefits of Dupilumab therapy.
Future prospective studies with larger cohorts are warranted to validate these findings and better characterize long-term ocular outcomes in dupilumab-treated patients.
Acknowledgments
The authors would like to express their gratitude to Goldfarma, Odivelas, Portugal, for sharing their TearCheck® device and ScoutPro® and to all of the volunteers who took part in this study.
Funding
This research received no specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Foley P, Kerdraon YA, Hogden JP, et al. Dupilumab-associated ocular surface disease: an interdisciplinary decision framework for prescribers in the Australian setting. Australas J Dermatol. 2022;63:421–436. doi:10.1111/ajd.13924
2. Le Floc’h A, Allinne J, Nagashima K, et al. Dual blockade of IL-4 and IL-13 with dupilumab, an IL-4Rα antibody, is required to broadly inhibit type 2 inflammation. Allergy. 2020;75:1188–1204. doi:10.1111/all.14151
3. European Medicines Agency. Dupixent EPAR – product Information. Available from: https://www.ema.europa.eu/en/documents/product-information/dupixent-epar-product-information_en.pdf.
4. Bohner A, Topham C, Strunck J, et al. Dupilumab-associated ocular surface disease: clinical characteristics, treatment, and follow-up. Cornea. 2021;40:584–589. doi:10.1097/ICO.0000000000002461
5. Popiela MZ, Barbara R, Turnbull AMJ, et al. Dupilumab-associated ocular surface disease: presentation, management and long-term sequelae. Eye. 2021;35:3277–3284. doi:10.1038/s41433-020-01379-9
6. Lin TY, Wang CY, Wang FY, Kang EYC, Hwang YS. Association between dupilumab and conjunctivitis: a systematic review and meta-analysis of randomized controlled trials. Pharmaceutics. 2023;16:15. doi:10.3390/pharmaceutics15041031
7. Fachler T, Shreberk-Hassidim R, Molho-Pessach V. Dupilumab-induced ocular surface disease: a systematic review. J Am Dermatol. 2022;86:486–487. doi:10.1016/j.jaad.2021.09.029
8. Schlösser AR, Bult L, Thelen JC, et al. Higher prevalence of dupilumab-induced ocular adverse events in atopic dermatitis compared to asthma: a daily practice analysis. Clin Transl Allergy. 2024:14. doi:10.1002/clt2.12386
9. Achten R, Thijs J, van der Wal M, et al. Ocular surface disease in moderate-to-severe atopic dermatitis patients and the effect of biological therapy. Clin Exp Immunol. 2024;54:241–252. doi:10.1111/cea.14461
10. Achten R, Thijs J, van der Wal M, et al. Dupilumab-associated ocular surface disease in atopic dermatitis patients: clinical characteristics, ophthalmic treatment response and conjunctival goblet cell analysis. Allergy. 2023;78:2266–2276. doi:10.1111/all.15717
11. ESW Vision. User Manual - TearCheck. Available from: https://www.esw-vision.com/wp-content/uploads/2022/08/M040GB000D___-DOC00-User-Manual-tearcheck.pdf.
12. Prigol AM, Tenório MB, Matschinske R, Gehlen ML, Skare T. Tradução e validação do índice da doença da superfície ocular para a língua portuguesa [Translation and validation of ocular surface disease index to Portuguese]. Arq Bras Oftalmol. 2012;75(1):24–28. doi:10.1590/s0004-27492012000100005
13. Schiffman RM, Christianson MD, Jacobsen G, Hirsch JD, Reis BL. Reliability and validity of the ocular surface disease index. Arch Ophthalmol. 2000;118(5):615–621. doi:10.1001/archopht.118.5.615
14. Muñoz-Bellido FJ, Moreno E, Dávila I. Dupilumab: a review of present indications and off-label uses. J Investig Allergol Clin Immunol. 2022;32:97–115. doi:10.18176/jiaci.0682
15. Simpson EL, Bieber T, Guttman-Yassky E, et al. Two phase 3 trials of dupilumab versus placebo in atopic dermatitis. N Engl J Med. 2016;375:2335–2348. doi:10.1056/nejmoa1610020
16. Akinlade B, Guttman-Yassky E, de Bruin-Weller M, et al. Conjunctivitis in dupilumab clinical trials. Br J Dermatol. 2019;181:459–473. doi:10.1111/bjd.17869
17. Potvin R, Makari S, Rapuano CJ. Tear film osmolarity and dry eye disease: a review of the literature. Clin Ophthalmol. 2015;9:2039–2047. doi:10.2147/OPTH.S95242
18. Chang AY, Purt B. Biochemistry, Tear Film. [Updated June 5, 2023]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025. Available from: https://www.ncbi.nlm.nih.gov/books/NBK572136/.
19. Serino F, Dattilo V, Cennamo M, et al. Dupilumab-associated blepharoconjunctivitis: clinical and morphological aspects. Biomedicines. 2023;12:11. doi:10.3390/biomedicines11123104
20. Kychygina A, Cassagne M, Tauber M, et al. Dupilumab-associated adverse events during treatment of allergic diseases. Clin Rev Allergy Immunol. 2022;62:519–533. doi:10.1007/s12016-022-08934-0
21. Mehta U, Farid M. Dupilumab induced limbal stem cell deficiency. Int Med Case Rep J. 2021;14:275–278. doi:10.2147/IMCRJ.S308583
22. Ardern-Jones MR, Brown SJ, Flohr C, et al. An expert consensus on managing dupilumab-related ocular surface disorders in people with atopic dermatitis 2024. Br J Dermatol. 2024;191:865–885. doi:10.1093/bjd/ljae344
23. Halling AS, Loft N, Silverberg JI, Guttman-Yassky E, Thyssen JP. Real-world evidence of dupilumab efficacy and risk of adverse events: a systematic review and meta-analysis. J Am Acad Dermatol. 2021;84:139–147. doi:10.1016/j.jaad.2020.08.051
24. Treister AD, Kraff-Cooper C, Lio PA. Risk factors for dupilumab-associated conjunctivitis in patients with atopic dermatitis. JAMA Dermatol. 2018;154:1208–1211. doi:10.1001/jamadermatol.2018.2690
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.