Back to Journals » Clinical Interventions in Aging » Volume 20
The Validation of a Nomogram for Predicting Recurrence in Patients with Non-Valvular Atrial Fibrillation Post-Ablation
Authors Yu Y, Chen JL, Li GY, Huang SS, Wang T, Li XK, Li YG
Received 30 July 2025
Accepted for publication 6 November 2025
Published 20 November 2025 Volume 2025:20 Pages 2091—2104
DOI https://doi.org/10.2147/CIA.S557166
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Yi Yu,1 Jin-Lan Chen,2 Guang-Yin Li,2 Shen-Shen Huang,2 Ting Wang,3 Xiao-Kai Li,2 Yi-Gang Li3
1Department of Ultrasound, Shanghai Chest Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China; 2Medical Imaging Technology, Shanghai University of Sport, Shanghai, People’s Republic of China; 3Department of Cardiology, Xinhua Hospital Affiliated to School of Medicine, Shanghai JiaoTong University, Shanghai, People’s Republic of China
Correspondence: Yi Yu, Email [email protected] Yi-Gang Li, Email [email protected]
Purpose: To utilize the developed nomogram for evaluating the risk of recurrence in non-valvular atrial fibrillation (NVAF) patients after radiofrequency catheter ablation (RFCA) and compare the model’s performance with the APPLE, ATLAS, and Antwerp scores.
Patients and Methods: 242 patients with NVAF requiring RFCA were enrolled. These patients were randomly divided into a training cohort (n=169) and a validation cohort (n=73) according to 7:3. A nomogram was developed based on LAVI, RAVI, SII, NYHA classification, CHA2DS2-VASc score to estimate the risk of AF recurrence after RFCA. The APPLE, ATLAS, and Antwerp scores were calculated using the “pROC” package in R software. The AUC value of the nomogram compared with each of the three scores was evaluated using the DeLong test. The integrated discrimination improvement and net reclassification index were calculated to compare the predictive performance of the nomogram against the scores in R software.
Results: The nomogram achieved significantly higher values with an AUC of 0.837 (95% CI: 0.774– 0.899) in the training cohort and 0.895 (95% CI: 0.823– 0.968) in the validation cohort (all P < 0.05) than the three scores. It also achieved better positive and negative predictive values, indicating enhanced discriminatory power. By integrating multidimensional parameters and optimizing risk stratification, it significantly reduced misjudgment rates. Furthermore, the model demonstrated a more balanced sensitivity-specificity profile and greater predictive stability than single-dimensional scores. It also provides more robust clinical decision support for predicting post-RFCA recurrence across diverse datasets.
Conclusion: The APPLE, ATLAS, and Antwerp scores all demonstrated effectiveness in predicting AF recurrence after RFCA in patients with NVAF. Among these established scoring systems, the APPLE score showed better performance compared to the other two. More importantly, our newly developed nomogram exhibited superior performance compared to all three existing scores, demonstrating a marked improvement in predicting the risk of AF recurrence. While our model represents a promising tool, it is still in the preliminary stage and requires further validation in larger, multi-center, prospective cohorts to confirm its generalizability.
Keywords: nomogram, recurrence risk scores, validation, non-valvular atrial fibrillation, radiofrequency catheter ablation
Introduction
Atrial fibrillation (AF) is a common arrhythmia, and its global prevalence is increasing annually, particularly among the elderly.1 AF significantly increases the risk of severe complications such as stroke and heart failure, which not only reduces patients’ quality of life but also imposes a substantial economic burden on families and society. Although radiofrequency catheter ablation (RFCA) can effectively improve patients’ symptoms and quality of life, post-procedural recurrence remains a significant challenge requiring urgent solutions. The predominant mechanism underlying AF recurrence after RFCA is pulmonary vein (PV) reconnection, due to the transient and non-transmural nature of the ablation lesions. This allows for the re-establishment of electrical conduction from previously isolated PVs. Additional factors include the presence of non-PV triggers and progressive atrial substrate.2 2023 ACC/AHA/ACCP/HRS Guideline highlighted the progressive emphasis on patient selection, the central role of pulmonary vein isolation (PVI) as the cornerstone, and the conditional recommendation for more extensive ablation strategies in persistent AF.3
Studies report widely varying recurrence rates after AF ablation, typically ranging from 20% to 40%.4 This high recurrence rate not only compromises the effectiveness of the procedure but may also increase the psychological and economic burden on patients. Therefore, accurately predicting the risk of recurrence after AF ablation has become a major research focus in the cardiovascular field. However, existing prediction models still have limitations and remain to be improved.5 Therefore, more precise, and readily applicable models are particularly crucial and urgent.
The aim of our study was to utilize the developed nomogram for evaluating the risk of recurrence in non-valvular atrial fibrillation (NVAF) patients after RFCA and compare its performance with the APPLE, ATLAS and Antwerp scores.
Materials and Methods
Study Population
This retrospective study developed and internally validated an AF recurrence risk model by collecting clinical characteristics, laboratory values and echocardiographic data from 242 patients with NVAF who underwent successful RFCA at our hospital between September 2022 and November 2023. Additionally, an interactive web-based dynamic nomogram was constructed.
Definition and Follow Up
AF was classified as paroxysmal or non-paroxysmal (persistent, long-standing persistent, or permanent). New York Heart Association (NYHA) functional classification was categorized according to the 2022 AHA/ACC/HFSA Heart Failure Guidelines.6 Patients were followed per a standardized protocol, with outpatient clinic visits at 3, 6, and 12 months. A 12-lead ECG was obtained at each visit. Additionally, all patients received a handheld single-lead ECG monitor and were instructed to record twice daily and upon symptom occurrence. All transmitted recordings were reviewed by two independent cardiologists. AF recurrence was defined as any atrial arrhythmia (AF, atrial flutter, or atrial tachycardia) lasting >30 seconds after the 3-month blanking period.6 Systemic immune-inflammatory index (SII) was calculated as: [neutrophil count (×109/L) × platelet count (×109/L)] / lymphocyte count (×109/L).7–9 Recurrence risk scores were evaluated as follows: APPLE score10 (range: 0–5 points; 1 point each for): Age >65 years, persistent AF, impaired eGFR (<60 mL/min/1.73m²), left atrial diameter ≥43 mm, left ventricular ejection fraction (LVEF) <50%; ATLAS score:11 age >60 years (1 point), female sex (4 points), non-paroxysmal AF (2 points), current smoking (7 points), left atrial volume index (LAVI) (1 point per 10 mL/m²); Antwerp score:12 LAVI >50 mL/m² (1 point), history of paroxysmal AF (1 point), QRS duration >120ms (any morphology; 2 points), heart failure etiology (2 points). Baseline characteristics were retrospectively collected from medical records by physicians blinded to study objectives.
Statistical Analysis
Statistical analyses were performed using SPSS 24.0 (SPSS Inc., Chicago, IL, USA) for descriptive statistics and hypothesis testing. Nomogram development and internal validation were conducted in R version 4.3.3 (R foundation for statistical computing). Continuous variables with normal distribution are presented as mean ± standard deviation (SD), while quantitative data with a skewed distribution are expressed as the median [M (Q25, Q75)]. Categorical variables were expressed as percentages (%). For normally distributed continuous variables, independent samples t-tests were employed for comparison; for non-normally distributed continuous variables, the Mann–Whitney U-test was used for analysis. Comparisons of categorical variables were performed using the χ²-test or Fisher’s exact test, based on the data distribution. Independent predictors for the multivariable model were identified by first screening baseline variables via univariate analysis (p < 0.1), followed by backward elimination in a logistic regression model (retained at p < 0.05). The final nomogram was derived from the coefficients of this model. This dynamic nomogram was deployed as an interactive web application using the DNbuilder function (DynNom R package), enabling real-time clinical implementation. Model performance metrics, including AUC, sensitivity, specificity, accuracy, PPV, NPV, were calculated using the “pROC” package in R software. The DeLong test compared nomogram AUC against each of the three scores. Predictive value assessment included 95% confidence intervals for all scores. Additionally, the IDI using the “PredictABEL” package and the NRI using the “nricens” package were calculated to compare the predictive performance of the nomogram against the scores in R software. The lrm function from the “rms” package was used to fit a logistic regression model. The calibrate function from the “rms” and decision curve function from the “rmda” package were used. A p-value < 0.05 was considered to indicate statistically significant.
Results
1. Baseline characteristic of the patients with NVAF were summarized in Table 1. Comparative analysis of the non-recurrent and recurrent patients with NVAF in the two cohorts were summarized in Table 2. The predictive model was developed by five variables including LAVI: OR 1.055 (95% CI: 1.021–1.090), P = 0.001; RAVI: OR 1.040 (95% CI: 1.008–1.073), P = 0.014; SII: OR 1.015 (95% CI: 1.001–1.030), P = 0.036; NYHA functional classification: OR 2.861 (95% CI: 1.282–6.383), P = 0.010; CHA2DS2-VASc score: OR 1.417 (95% CI: 1.077–1.864), P = 0.013. Examples of an online (Dynamic Nomogram) application via the shinyapps.io platform (Figure 1a and b). Baseline features of the recurrence risk scores (Table 3): The differences between non-recurrent and recurrent patients were statistically significant for the three scores in the two cohorts (all P < 0.01). The receiver operating characteristic (ROC) curve and area under curve (AUC) analysis for predicting NVAF post-RFCA recurrence risk with the three scores were revealed in Table 4. The results of the DeLong test showed that there were no statistically significant differences in the AUC values between any pairwise comparisons of the three scores in the two cohorts (all P > 0.05).
 |
Table 1 Training Cohort and Validation Cohort of the Patients with Non-Valvular Atrial Fibrillation |
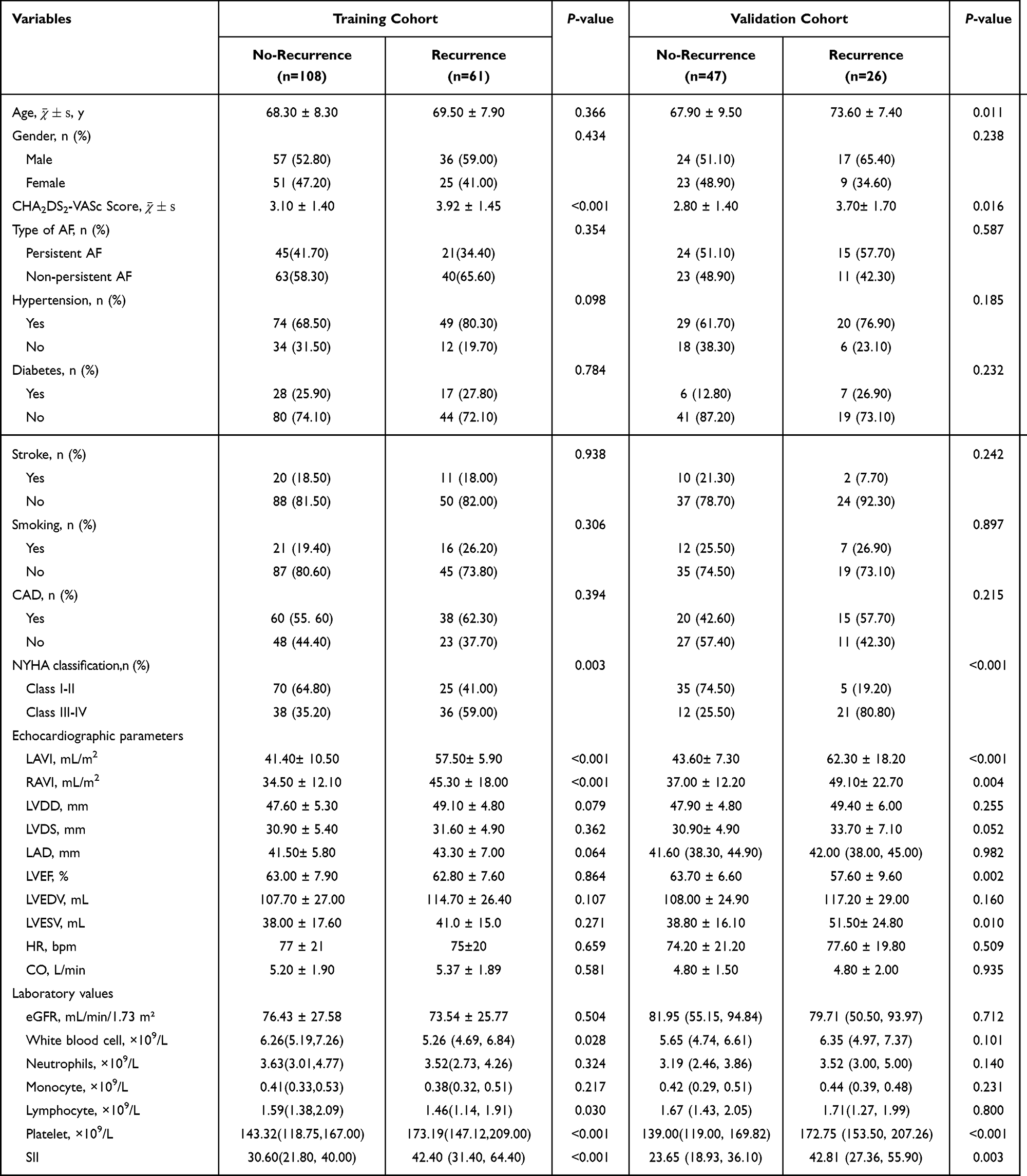 |
Table 2 Comparative Analysis of the Training and Validation Cohort Patients with Non-Valvular Atrial Fibrillation |
 |
Table 3 Comparative Analysis of Recurrence Risk Scores Between Recurrent and Non-Recurrent Patients in the Both Groups |
 |
Table 4 ROC Analysis of the Three Scores in Predicting Post-Procedural Recurrence Risk of the NVAF Patients |
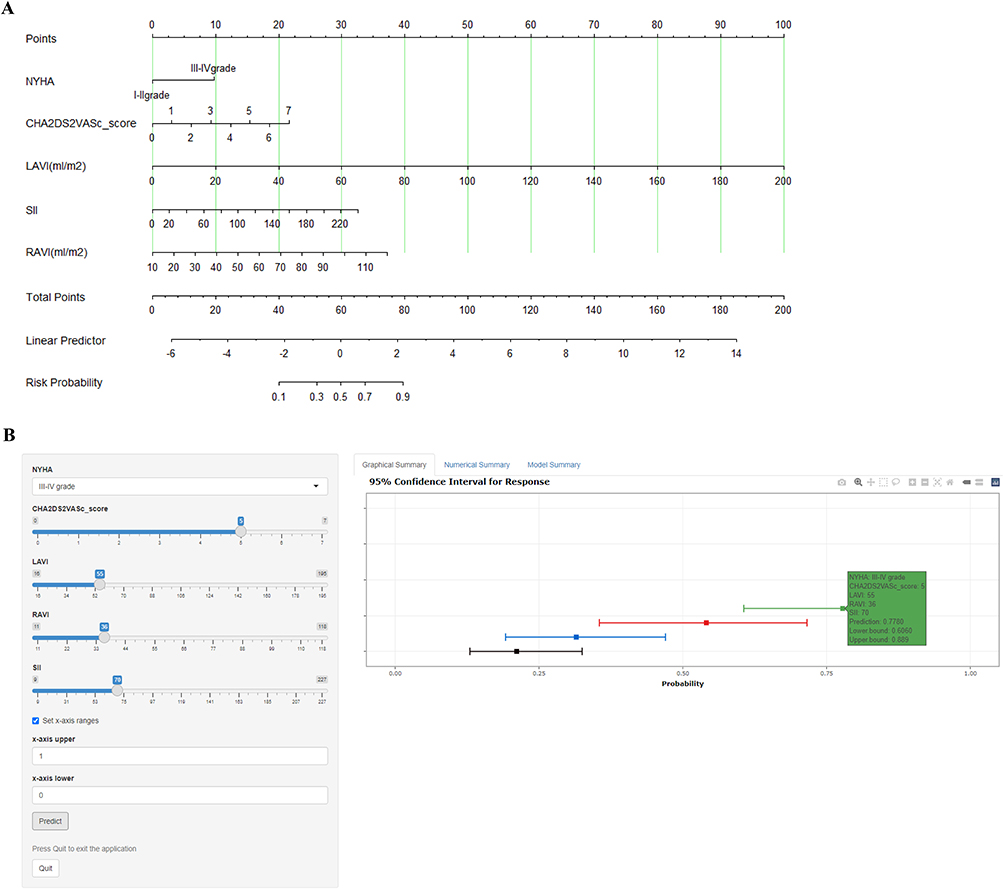 |
Figure 1 The risk prediction nomogram and an example.(A) For the NVAF patient with the following pre-ablation characteristics: NYHA class: I–IV, CHA2DS2-VASc score, LAVI, RAVI, SII. The dynamic nomogram predicted a probability of 1-year AF recurrence. (B) For a NVAF patient with the following pre-ablation characteristics: NYHA class: III–IV, CHA2DS2-VASc score: 5, LAVI: 55 mL/m², RAVI: 36 mL/m², SII: 70 (values presented as SII/10). The dynamic nomogram predicted a 77.8% (95% CI: 60.6%-88.9%) probability of 1-year AF recurrence. Abbreviations: NVAF, non-valvular atrial fibrillation; NYHA, New York Heart Association; LAVI, left atrial volume index; RAVI, right atrial volume index; SII, systemic immune-inflammation index; CI, confidence interval; AF, atrial fibrillation. |
2. Comparison of ROC and AUC curves for predicting NVAF post-RFCA recurrence risk: nomogram vs recurrence risk scores (Figure 2a and b and Table 5).
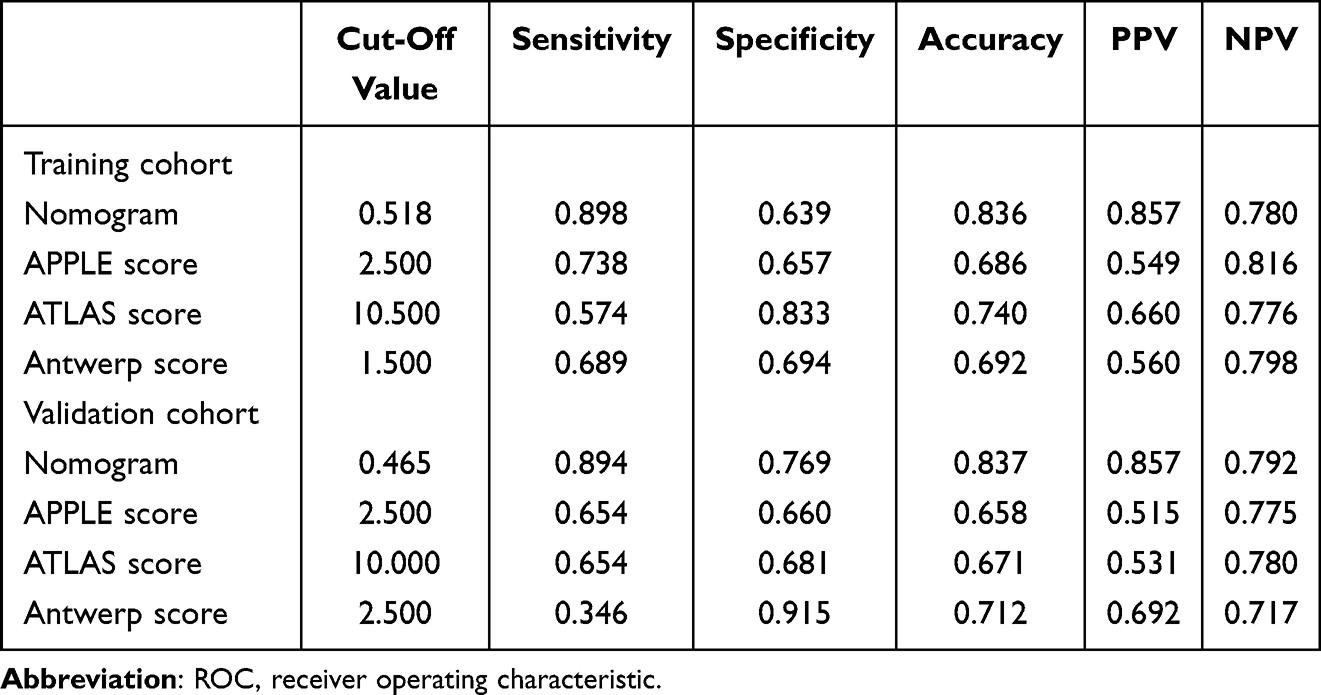 |
Table 5 ROC Analysis of the Nomogram and Recurrence Risk Scores |
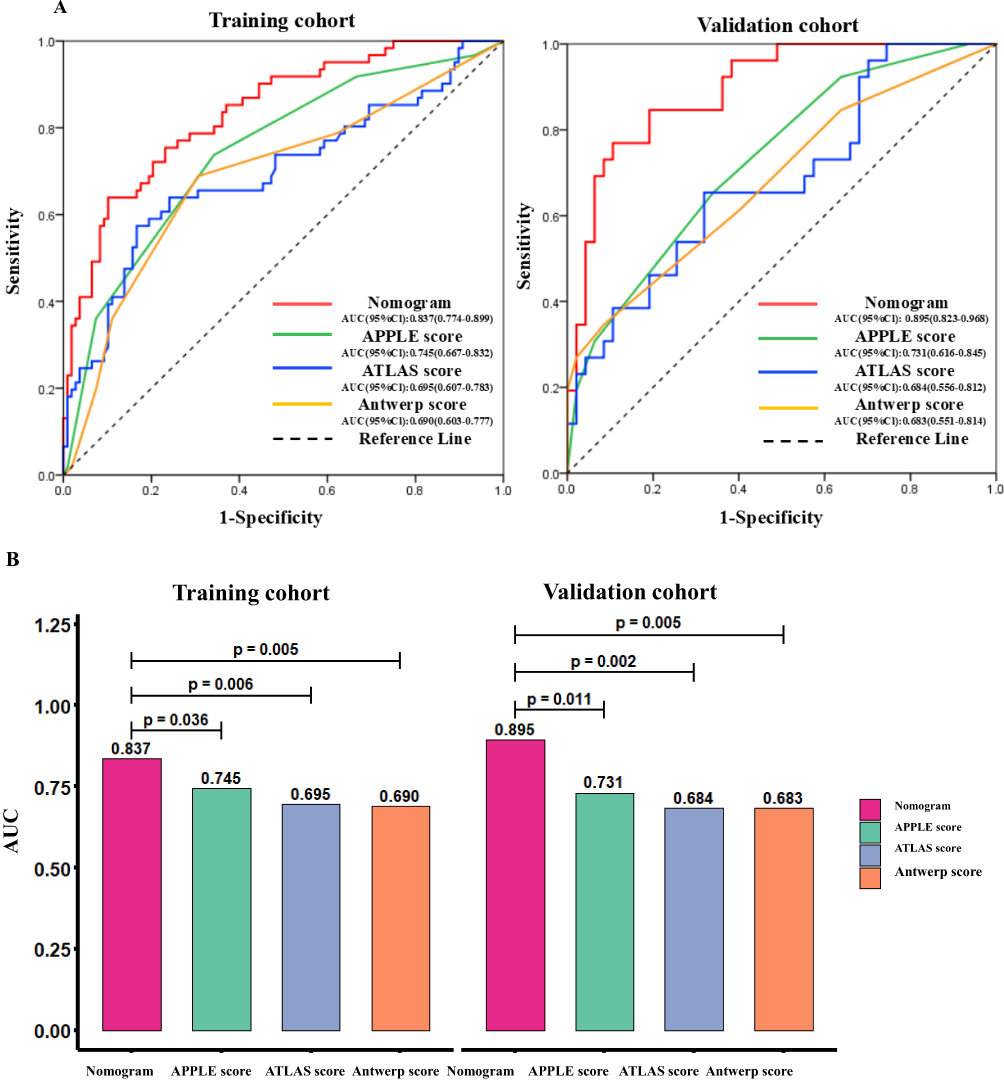 |
Figure 2 Comparison of ROC curves and AUC analysis for predicting NVAF post-RFCA recurrence risk: nomogram vs recurrence risk scores (A) The nomogram showed the performance metrics with a sensitivity of 63.9%, specificity of 89.8% and accuracy of 83.6% in the training cohort and sensitivity of 89.4%, specificity of 76.9% and accuracy of 83.7% in the validation cohort. (B) The model achieved significantly higher values with an AUC of 0.837 (95% CI: 0.774–0.899) in the training cohort and 0.895 (95% CI: 0.823–0.968) in the validation cohort (P < 0.05) than those of the APPLE score (0.745/0.731), ATLAS score (0.695/0.684), and Antwerp score (0.690/0.683) in both cohorts, respectively. Abbreviations: ROC, receiver operating characteristic; AUC, area under the curve. |
The risk of postoperative recurrence increased when values exceeded these thresholds in the validation cohort, that is, nomogram (0.465), APPLE score (2.5), ATLAS score (10.0), Antwerp score (2.5). The sensitivity and accuracy of the nomogram were higher than the three scores in the two cohorts. The nomogram’s positive predictive value (PPV) and negative predictive value (NPV) were also superior to the three scores. This indicated the nomogram had higher discriminatory power for predicting AF recurrence post-RFCA. The limitations of the individual scores were with a consistently low specificity (65.7%/66.0%) of the APPLE score, low PPV (54.9%/51.5%) and might lead to a risk of excessive intervention in non-recurrent patients. The characteristic of the ATLAS score was including inadequate sensitivity in the training cohort (57.4%), imbalance between sensitivity (65.4%) and specificity (68.1%) in the validation cohort, which led to 34.6% recurrence cases missed diagnosis in the validation cohort. The feature of the Antwerp score was including high specificity (91.5%), but drastically reduced sensitivity (34.6%) and finally led to missed diagnosis rate as high as 65.4% in the validation cohort.
By integrating multi-dimensional parameters and optimizing risk stratification, the nomogram significantly reduced the misjudgment rate of 16.5%-53.6% and 24.0%-34.2%, which compared with the APPLE and ATLAS scores, respectively. The nomogram demonstrated significantly better balance between sensitivity and specificity and superior predictive stability compared to the single-dimension scores.
The model achieved significantly higher values with an AUC of 0.837 in the training cohort and 0.895 in the validation cohort than those of the APPLE, ATLAS and Antwerp scores (vs 0.745/0.731, 0.695/0.684, 0.690/0.683) (all P < 0.05). This demonstrated the superior predictive capability and stability of the nomogram for AF recurrence post-RFCA. DeLong test pairwise comparisons revealed that the AUC of the nomogram was significantly different from the AUCs of the three scores in the two cohorts. In the training cohort vs validation cohort, DeLong test pairwise comparisons revealed that the AUC of the nomogram was significantly different from the AUCs of the APPLE score (Z=2.103, P=0.036 vs Z=2.530, P=0.011), ATLAS score (Z=2.741, P=0.006 vs Z=3.155, P=0.002), and Antwerp score (Z=2.800, P=0.005 vs Z=2.778, P=0.005), respectively.
3. Comparison of calibration and decision curves for predicting NVAF post-RFCA recurrence risk: nomogram vs recurrence risk scores (Figure 3a and b).
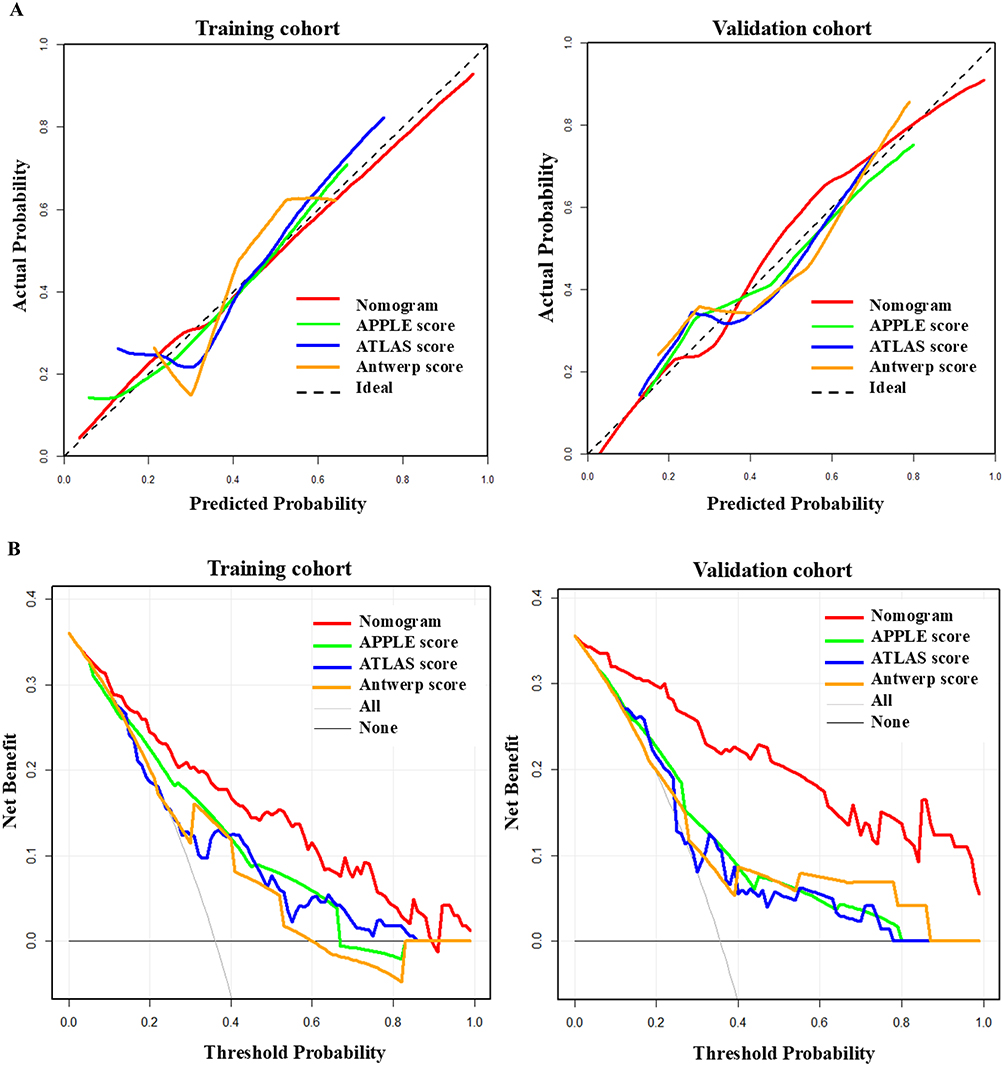 |
Figure 3 Comparison of calibration curves and decision curves for predicting NVAF post-RFCA recurrence risk: nomogram vs recurrence risk scores. (A) The model’s calibration curve demonstrated high agreement with the ideal line (diagonal) in the training and validation cohorts. In contrast, the calibration curves of the APPLE, ATLAS score and Antwerp scores showed varying degrees of deviation from the ideal line. This deviation was particularly noticeable in the medium-to-high recurrence probability range for the three scores, indicating reduced prediction accuracy within this risk range. (B) In the training and validation cohorts, the decision curve of the nomogram lay above those of the APPLE, ATLAS, and Antwerp scores across a broad range of threshold probabilities (0.1–1.0). In the validation cohort, the net benefit value of the nomogram (approximately 0.22) was also higher than those of the APPLE score (0.09), ATLAS score (0.06), Antwerp score (0.08). These results indicated that the nomogram provided superior comprehensive net benefit at different clinical decision thresholds. It offered more valuable decision support for clinically predicting recurrence after RFCA across different datasets. |
The model’s calibration curve demonstrated high agreement with the ideal line (diagonal) in the two cohorts, while the three scores showed varying degrees of deviation from the ideal line. This deviation was particularly noticeable in the medium-to-high recurrence probability range for the three scores, indicating reduced prediction accuracy within this risk range.
In the two cohorts, the decision curve of the nomogram lay above those of the three scores across a broad range of threshold probabilities (0.1–1.0). These results indicated that the nomogram provided superior comprehensive net benefit at different clinical decision thresholds. It offered more valuable decision support for clinically predicting recurrence after RFCA across different datasets.
4. Comparative analysis of the integrated discrimination improvement (IDI) and net reclassification index (NRI) between the nomogram and recurrence risk scores. (Table 6).
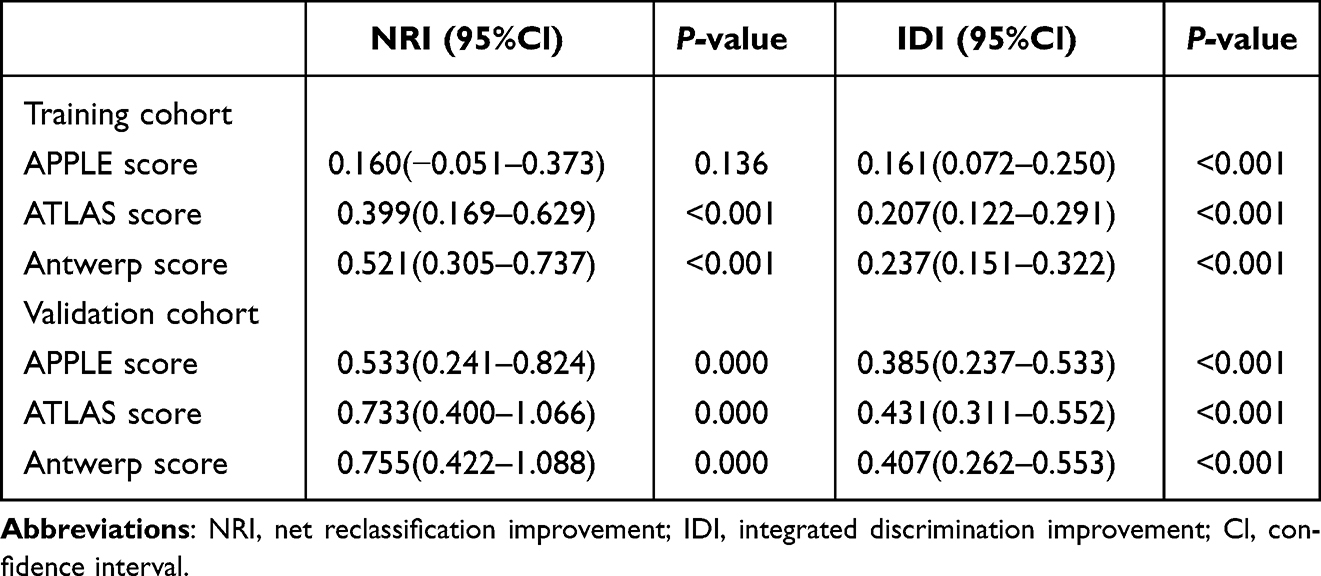 |
Table 6 Comparative Analysis of NRI and IDI Between the Nomogram and Recurrence Risk Scores |
The nomogram demonstrated superior NRI and IDI across the cohorts. Although the improvement in NRI compared to the APPLE score in the training cohort did not reach statistical significance, the nomogram significantly outperformed the three scores on all metrics in the validation cohort (all P < 0.001). Compared to the ATLAS and Antwerp scores in the training cohort, the nomogram showed significant advantages in NRI and IDI (P < 0.001). Compared to the APPLE score, the NRI was not statistically significant (P = 0.136). However, the IDI was still significantly better than the APPLE score (P < 0.001). In the validation cohort, the nomogram comprehensively outperformed the three scores.
Discussion
This study developed a predictive model integrating LAVI, right atrial volume index (RAVI), SII, NYHA classification, and the CHA2DS2-VASc score. Compared to the APPLE, ATLAS and Antwerp scores, the nomogram demonstrated superior predictive capability and stability for post-RFCA AF recurrence, evidenced by its higher AUC, improved PPV and NPV. By incorporating multi-dimensional parameters and optimizing risk stratification, it significantly reduced misclassification rates while achieving a more balanced sensitivity-specificity profile than single-dimensional scores. Furthermore, the nomogram maintained robust predictive stability across diverse datasets, offering enhanced clinical decision support for post-RFCA recurrence risk assessment.
Unlike early prediction scores7,13,14 and subsequent models,10,11 most traditional scoring systems inadequately incorporated inflammatory biomarkers or lacked standardized criteria. These limitations hindered their application in precision medicine.6,15–22 In contrast, the present nomogram integrating atrial structure, SII, and clinical factors, enables more precise individualized assessment of AF recurrence risk. This is supported by established evidence, including the dose-dependent relationship between LAVI and recurrence risk (3.2% increase per 1 mL/m²),23 the independent prognostic value of RAVI >30 mL/m²,24,25 and the role of SII in reflecting inflammation-driven atrial remodeling that directly fuels AF recurrence.7,26,27 The inclusion of NYHA class was motivated by the well-established pathophysiological link between heart failure and AF recurrence risk, as these conditions frequently coexist and mutually exacerbate each other. This rationale is supported by a multicenter study,28 which found a significantly higher AF recurrence rate in patients with versus without advanced heart failure (40% vs 29.6%; P=0.011). Similarly, the CHA2DS2-VASc score was incorporated as a clinically relevant comorbidity marker to enhance the model’s predictive value. The APPLE score demonstrated superior overall predictive value for post-ablation recurrence in NVAF patients compared to the ATLAS and Antwerp scores, consistent with prior studies.8,29,30 This advantage was particularly evidenced by its significantly higher AUC on ROC analysis. In both datasets, the APPLE score achieved moderate discrimination for predicting post-procedure AF recurrence, indicating reasonable reliability and stability. All three scores exhibited stronger predictive performance for negative outcomes (absence of recurrence) than for positive outcomes (recurrence). This discrepancy likely stems from the complex clinical profiles and heterogeneous complications among recurrence patients, resulting in higher negative predictive rates, which aligning with existing literatures.8,29,30
Our nomogram, constructed from multi-dimensional parameters, demonstrated superior discrimination for predicting AF recurrence compared to existing models. This contrasts with Jud et al’s SUCCESS score approach.31 While the APPLE score showed some efficacy in early studies,6 its parameter selection inadequately incorporated key pathological factors, limiting predictive power. Tang et al32 analyzed 11 prediction models and found the ATLAS score relatively superior, yet it still demonstrated suboptimal overall performance and clinical utility. The Antwerp score exhibited markedly elevated specificity (0.915) but critically low sensitivity (0.346), reflecting an “overly conservative” screening tendency that risks missing high-recurrence patients. This limitation aligns with reports showing insufficient sensitivity in high-risk populations for scores relying solely on QRS duration and heart failure etiology.33,34 Crucially, our inclusion of SII directly supports Korantzopoulos et al’s “inflammation-structural remodeling-electrical remodeling” theory of AF recurrence.35 The nomogram maintained strong generalizability, with AUC rising to 0.895 in validation. In contrast, all three comparator scores showed performance degradation during external validation (eg, Antwerp AUC: from 0.690 to 0.683), suggesting over-reliance on paroxysmal AF population characteristics.
Significantly, the nomogram achieved higher predictive accuracy and reliability for recurrence compared to all three scores. Their suboptimal calibration likely stems from differences in parameter selection. Huang et al36 demonstrated that the inflammatory marker platelet-to-lymphocyte ratio (PLR) emerged as an independent predictor of post-RFCA recurrence in AF patients. Notably, supplementing the APPLE score with PLR significantly improved its calibration. Furthermore, the ATLAS score consistently underestimated recurrence probability in moderate-to-high-risk AF patients. Although incorporating LAVI, its broad scoring intervals likely compromised model fit for this parameter. While the Antwerp score effectively predicts left ventricular functional recovery post-ablation in heart failure patients (AUC: 0.86–0.93),10,12 its association with AF recurrence requires further validation.33,34
Nevertheless, our nomogram’s holistic integration of multi-dimensional parameters enabled more precise identification of high-risk patients. Decision curve analysis (DCA)37 confirmed its superior clinical utility: across the 0.1–1.0 threshold probability range in the validation cohort, the nomogram yielded significantly higher net benefit than comparator scores. This advantage is particularly relevant given the CHA2DS2-VASc score’s documented decision uncertainty for intermediate-risk patients in current guidelines.38 By quantifying atrial remodeling and inflammatory status, the nomogram provides a more robust foundation for individualized anticoagulation strategies while demonstrating superior reclassification ability and comprehensive predictive improvement. These findings align with Ma et al,39 whose model outperformed the APPLE score in predicting AF recurrence after RFCA (n=500) using IDI and NRI metrics.40,41 The nomogram’s stable discriminative enhancement suggests that synthesizing multi-dimensional variables with optimized weighting effectively mitigates prediction errors inherent in the three scores, which may arise from variable selection bias or linear modeling constraints.
Although the nomogram’s NRI compared to the APPLE score did not reach statistical significance in the training cohort, its significant IDI confirmed meaningful enhancement in overall risk discrimination. This differential performance between discrimination and reclassification metrics may reflect the model’s enhanced precision in identifying high-risk subgroups, which consistent with Pencina et al’s42 study wherein IDI demonstrates greater sensitivity to improvements within high-risk populations.
We thus demonstrate that the nomogram effectively integrates multiple variables to predict recurrence risk in patients with NVAF following RFCA. These findings underscore its potential for clinical application in recurrence risk assessment. Critically, our nomogram enables the consolidation of diverse parameters including clinical features, laboratory values, and echocardiographic data into a unified model, establishing a comprehensive evaluation system.
Therefore, our study demonstrates that the nomogram effectively integrates multivariable predictors to assess recurrence risk in NVAF patients post-RFCA. These findings highlight its clinical applicability for recurrence risk stratification. Crucially, the model synthesizes diverse parameters including clinical features, laboratory values, and echocardiographic data into a unified model, establishing a comprehensive risk stratification system.
Limitations
There are several limitations in this study. First, this study is a single-center retrospective investigation with a limited sample size, and there may be a risk of over fitting the performance boundary of the model. The clinical applicability of the nomogram requires further validation through multicenter prospective data, particularly for external validation across diverse populations. Second, the measurement of the SII could be affected by laboratory testing methodologies; establishing standardized detection protocols in the future is necessary to minimize this potential bias. Third, the three scoring systems (APPLE, ATLAS, and Antwerp scores) exhibit lower predictive efficacy, largely attributed to their relatively simplistic parameter selection. This limitation hinders their ability to adequately capture the complex pathophysiological mechanisms underlying AF recurrence. Future research should focus on optimizing model parameters, validating external performance, and exploring individualized treatment strategies.
Conclusions
In summary, the APPLE, ATLAS, and Antwerp scores all demonstrated effectiveness in predicting AF recurrence after RFCA in patients with NVAF. Among these established scoring systems, the APPLE score showed better performance compared to the other two. More importantly, our newly developed nomogram exhibited superior performance compared to all three existing scores, demonstrating a marked improvement in predicting the risk of AF recurrence. While our model represents a promising tool, it is still in the preliminary stage and requires further validation in larger, multi-center, prospective cohorts to confirm its generalizability.
Ethics Statement
The study was conducted in accordance with the Declaration of Helsinki and has been approved by Shanghai Chest Hospital, Shanghai Jiao Tong University School of Medicine. Due to the study being a retrospective analysis, the review committee waived the requirement for written informed consent. Confidential patient information was removed from the entire data set prior to analysis.
Funding
Shanghai Health and Family Planning Commission (grant number 202240110); and Shanghai Chest Hospital affiliated with Shanghai Jiao Tong University School of Medicine (grant number yuyi2024); Xuhui District Campus Local Cooperation Project (grant number 23XHYD-22).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chugh SS, Havmoeller R, Narayanan K, et al. Worldwide epidemiology of atrial fibrillation: a global burden of disease 2010 Study. Circulation. 2014;129(8):837–847. doi:10.1161/CIRCULATIONAHA.113.005119
2. Cho S, Kim D, Park H, et al. Mapping and ablation outcomes of extra-pulmonary vein triggers in atrial fibrillation: single-centre retrospective study with consistent provocation protocol. Europace. 2025;27(10):euaf225. doi:10.1093/europace/euaf225
3. Joglar JA, Chung MK, Armbruster AL, et al. Peer Review Committee Members. 2023 ACC/AHA/ACCP/HRS Guideline for the Diagnosis and Management of Atrial Fibrillation: a Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2024;149(1):e1–e156. doi:10.1161/CIR.0000000000001193
4. Calkins H, Hindricks G. Cappato R, et al. 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation. Heart Rhythm. 2017;14(10):e275–e444. doi:10.1016/j.hrthm.2017.05.012
5. Kornej J, Hindricks G, Shoemaker MB, et al. The APPLE score: a novel and simple score for the prediction of rhythm outcomes after catheter ablation of atrial fibrillation. Clin Res Cardiol. 2015;104(10):871–876. doi:10.1007/s00392-015-0856-x
6. Hindricks G, Potpara T, Dagres N, et al. ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): the task force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J. 2021;42(5):373–498. doi:10.1093/eurheartj/ehaa612
7. Wang RH, Wen WX, Jiang ZP, et al. The clinical value of neutrophil-to-lymphocyte ratio (NLR), systemic immune-inflammation index (SII), platelet-to-lymphocyte ratio (PLR) and systemic inflammation response index (SIRI) for predicting the occurrence and severity of pneumonia in patients with intracerebral hemorrhage. Front Immunol. 2023;14:
8. Kornej J, Büttner P, Sommer P, et al. Prediction of electro-anatomical substrate using APPLE score and biomarkers. Europace. 2019;21(1):54–59. doi:10.1093/europace/euy120
9. Dong W, Gong Y, J Z, et al. A combined analysis of TyG index, SII index, and SIRI index: positive association with CHD risk and coronary atherosclerosis severity in patients with NAFLD. Front Endocrinol. 2024;14:1281839. doi:10.3389/fendo.2023.1281839
10. Bergonti M, Spera F, Tijskens M. Tijskens M, et al. A new prediction model for left ventricular systolic function recovery after catheter ablation of atrial fibrillation in patients with heart failure: the ANTWOORD Study. Int J Cardiol. 2022;358:45–50. doi:10.1016/j.ijcard.2022.04.040
11. Mesquita J, Ferreira AM, Cavaco D, Adragão P. Development and validation of a risk score for predicting atrial fibrillation recurrence after a first catheter ablation procedure: ATLAS score-Author’s reply. Europace. 2018;20(FI_3):f460–f462. doi:10.1093/europace/euy043
12. Bergonti M, Ascione C, Marcon L, et al. Left ventricular functional recovery after atrial fibrillation catheter ablation in heart failure: a prediction model. Eur Heart J. 2023;44(35):3327–3335. doi:10.1093/eurheartj/ehad428
13. Zheng JY, Li DT, Qıu YG, et al. CHA2DS2-VASc score as a prognostic indicator in patients with atrial fibrillation undergoing coronary stenting. Turk J Med Sci. 2022;52(4):1103–1110. doi:10.55730/1300-0144.5413
14. Chen K, Bai R, Deng W, et al. HATCH score in the prediction of new-onset atrial fibrillation after catheter ablation of typical atrial flutter. Heart Rhythm. 2015;12(7):1483–1489. doi:10.1016/j.hrthm.2015.04.008
15. Zhao X, Huang L, Hu J, et al. The association between systemic inflammation markers and paroxysmal atrial fibrillation. BMC Cardiovasc Disord. 2024;24(1):334. DOI:10.1186/s12872-024-04004-9
16. Ruan ZB, Liang HX, Wang F. Wang F, et al. Influencing factors of recurrence of nonvalvular atrial fibrillation after radiofrequency catheter ablation and construction of clinical nomogram prediction model. Int J Clin Pract. 2022;15:8521735. doi:10.1155/2022/8521735
17. Aydın SŞ, Aksakal E. The role of HATCH score in the prediction of ischemic cerebrovascular events in patients with heart failure and atrial fibrillation. Clin Appl Thromb Hemost. 2024;30:10760296241227935. doi:10.1177/10760296241227935
18. Mujović N, Marinković M, Marković N, et al. Prediction of very late arrhythmia recurrence after radiofrequency catheter ablation of atrial fibrillation: the MB-LATER clinical score. Sci Rep. 2017;7:40828. doi:10.1038/srep40828
19. Winkle RA, Jarman JW, Mead RH, et al. Predicting atrial fibrillation ablation outcome: the CAAP-AF score. Heart Rhythm. 2016;13(11):2119–2125. doi:10.1016/j.hrthm.2016.07.018
20. Mulder MJ, Kemme MJB, Hopman LHGA, et al. Comparison of the predictive value of ten risk scores for outcomes of atrial fibrillation patients undergoing radiofrequency pulmonary vein isolation. Int. J Cardiol. 2021;344:103–110. doi:10.1016/j.ijcard.2021.09.029
21. Chao TF, Ambrose K, Tsao HM, et al. Relationship between the CHADS(2) score and risk of very late recurrences after catheter ablation of paroxysmal atrial fibrillation. Heart Rhythm. 2012;9(8):1185–1191. doi:10.1016/j.hrthm.2012.03.007
22. Ziegler A. Clinical prediction models: a practical approach to development, validation, and updating. Biometrical J. 2020;62(4):1122–1123. doi:10.1002/bimj.202000088
23. Njoku A, Kannabhiran M, Arora R, et al. Left atrial volume predicts atrial fibrillation recurrence after radiofrequency ablation: a meta-analysis. Europace. 2018;20(1):33–42. doi:10.1093/europace/eux013
24. Ko KY, Jang JH, Choi SH, et al. Impact of right atrial enlargement on clinical outcome in patients with atrial fibrillation. Front Cardiovasc Med. 2022;23(9):989012. doi:10.3389/fcvm.2022.989012
25. Hopman LHGA, Visch JE, Bhagirath P. et al. Right atrial function and fibrosis in relation to successful atrial fibrillation ablation. Eur Heart J Cardiovasc Imaging. 2023;24(3):336–345. doi:10.1093/ehjci/jeac152
26. Harada M, Nattel S. Implications of inflammation and fibrosis in atrial fibrillation pathophysiology. Card Electrophysiol Clin. 2021;13(1):25–35. doi:10.1016/j.ccep.2020.11.002
27. Wu N, Yu B, Xiang Y, et al. Association of inflammatory factors with occurrence and recurrence of atrial fibrillation: a meta-analysis. Int J Cardiol. 2013;169(1):62–72. doi:10.1016/j.ijcard.2013.08.078
28. Sultan A, Lüker J, Andresen D, et al. Predictors of atrial fibrillation recurrence after catheter ablation: data from the german ablation registry. Sci Rep. 2017;7:16678. doi:10.1038/s41598-017-16938-6
29. Huang W, Sun H, Luo Y, et al. Better performance of the APPLE score for the prediction of very early atrial fibrillation recurrence post-ablation. Hellenic J Cardiol. 2024;13:S1109–9666(24)00176–3. doi:10.1016/j.hjc.2024.08.008
30. Parameswaran R, Kalman JM, Savelieva I. Savelieva I. et al. APPLE score in atrial fibrillation: a simple solution to predict a complex process? Europace. 2019;21(1):1–2. doi:10.1093/europace/euy157
31. Jud FN, Obeid S, Duru F, et al. A novel score in the prediction of rhythm outcome after ablation of atrial fibrillation: the SUCCESS score. Anatol J Cardiol. 2019;21(3):142–149. doi:10.14744/AnatolJCardiol.2018.76570
32. Tang LYW, Hawkins NM, Macle L, et al. Predicting atrial fibrillation recurrence after catheter ablation: a comparative evaluation in the CIRCA-DOSE trial. Circ Arrhythm Electrophysiol. 2021;14(12):e010443. doi:10.1161/CIRCEP.121.010443
33. Serban T, du Fay du Lavallaz J, Barker DC, et al. Validation of a novel score to predict which patients with atrial fibrillation and depressed left ventricular ejection fraction will respond to catheter ablation. Rev Esp Cardiol. 2023;76(9):745–748. doi:10.1016/j.rec.2023.03.014
34. Mohanty S, La Fazia VM, Natale A. The Antwerp score: is this the ‘new hope on the horizon’? Eur Heart J. 2023;44(35):3336–3338. doi:10.1093/eurheartj/ehad420
35. Korantzopoulos P, Letsas KP, Tse G, et al. Inflammation and atrial fibrillation: a comprehensive review. J Arrhythm. 2018;34(4):394–401. doi:10.1002/joa3.12077
36. Huang W, Sun H, Tang Y, et al. Platelet-to-lymphocyte ratio improves the predictive ability of the risk score for atrial fibrillation recurrence after radiofrequency ablation. J Inflamm Res. 2023;11(16):6023–6038. doi:10.2147/JIR.S440722
37. Van Calster B, Wynants L, Verbeek JFM, et al. Reporting and interpreting decision curve analysis: a guide for investigators. Eur Urol. 2018;74(6):796–804. doi:10.1016/j.euuro.2018.08.038
38. January CT, Wann LS, Calkins H, et al. AHA/ACC/HRS focused update of the 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines and the Heart Rhythm Society. J Am Coll Cardiol. 2019;74(1):104–132. doi:10.1016/j.jacc.2019.01.011
39. Ma G, Zou C, Zhang Z, et al. A novel nomogram for predicting the recurrence of atrial fibrillation in patients treated with first-time radiofrequency catheter ablation for atrial fibrillation. Front Cardiovasc Med. 2024;21(11):1397287. DOI:10.3389/fcvm.2024.1397287
40. Kerr KF, Wang Z, Janes H, et al. Net reclassification indices for evaluating risk prediction instruments: a critical review. Epidemiology. 2014;25(1):114–121. doi:10.1097/EDE.0000000000000018
41. Van Calster B, Van Huffel S. Integrated discrimination improvement and probability-sensitive AUC variants. Stat Med. 2010;29(2):318–319. doi:10.1002/sim.3761
42. Pencina MJ, D’Agostino RB, D’Agostino RB, et al. Evaluating the added predictive ability of a new marker: from area under the ROC curve to reclassification and beyond. Stat in Med. 2008;27(2):157–172. doi:10.1002/sim.2929
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.