Back to Journals » Clinical Interventions in Aging » Volume 21
The Systemic Immune-Inflammation Index and High-Sensitivity C-Reactive Protein to High-Density Lipoprotein Cholesterol Ratio Predict Moderate and Severe Coronary Artery Stenosis in Older Patients with Coronary Heart Disease
Authors Liu F, Zhang G ![]() , Luo R, Liu M, Yuan M
, Luo R, Liu M, Yuan M
Received 15 January 2026
Accepted for publication 17 May 2026
Published 23 June 2026 Volume 2026:21 591749
DOI https://doi.org/10.2147/CIA.S591749
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zhi-Ying Wu
Fang Liu,1 Guowu Zhang,2 Rong Luo,1 Mingke Liu,1 Mingjing Yuan1
1Department of Radiology, Yongchuan Hospital of Chongqing Medical University, Chongqing, 402160, People’s Republic of China; 2Department of General Surgery, Yongchuan Hospital of Chongqing Medical University, Chongqing, 402160, People’s Republic of China
Correspondence: Guowu Zhang, Department of General Surgery, Yongchuan Hospital of Chongqing Medical University, 439 Xuanhua Road, Yongchuan Area, Chongqing, 402160, People’s Republic of China, Tel + 86 023-85381572, Email [email protected]
Objective: Coronary heart disease (CHD) stems from functional and organic coronary artery stenosis (CAS). This study explored associations of the systemic immune-inflammation index (SII) and high-sensitivity C-reactive protein to high-density lipoprotein cholesterol ratio (hsCRP/HDL-C) with CAS severity in older patients with CHD.
Methods: This retrospective analysis recruited 786 older patients with CHD, with their clinical data and laboratory parameters collected. Patients were allocated into training and validation sets (7:3, randomization) or into mild, moderate, and severe stenosis groups according to Gensini scores (GS). Correlations of SII and hsCRP/HDL-C with GS, influencing factors for moderate-to-severe CAS, and their diagnostic value in older patients with CHD or complicated with hypertension and/or diabetes were assessed using Spearman’s, univariate/multivariate logistic regression, and receiver operating characteristic curve analyses, respectively.
Results: Elevated SII and hsCRP/HDL-C were observed in patients with moderate-to-severe stenosis, which demonstrated certain correlations with GS, and were independent risk factors (IRFs) for moderate-to-severe CAS in older patients with CHD in both sets. The comparable regression coefficients between the two sets suggested good model consistency and no significant multicollinearity. The area under the curve of the combination of SII and hsCRP/HDL-C for predicting CAS severity was outperforming either marker alone. Hypertension significantly affected the discriminating performance of SII. SII remained stable in the hypertensive population, but its efficacy decreased evidently in the non-hypertensive population.
Conclusion: SII and hsCRP/HDL-C are IRFs for moderate-to-severe CAS in older patients with CHD, and their combination yields good predictive performance. Regression coefficients were well consistent between the two datasets. A study of 786 elderly CAD patients from January 2023 to June 2025 excluded those with incomplete records, severe dysfunctions, complications, autoimmune diseases, recent cerebrovascular disease and previous interventions. Patients were split into training (N=550) and validation (N=236) groups at a 7:3 ratio. Based on Gensini scores, they were categorized into mild (≤ 20 score, N=214/85), moderate (21-45 score, N=196/82) and severe stenosis (> 45 score, N=140/69). Data collected included demographics, medical history and lab results. Analyses involved baseline comparisons, Spearman correlation, logistic regression and ROC curve analysis. SII and hsCRP/HDL-C values emerged as key predictors of coronary artery stenosis in elderly CAD patients.Flowchart on elderly CAD patient study: classification, data collection and analysis methods.
Keywords: elderly coronary heart disease, coronary artery stenosis, systemic immune-inflammation index, high-sensitivity c-reactive protein to high-density lipoprotein cholesterol ratio, correlation
Introduction
Coronary heart disease (CHD), a chronic and complex condition marked by high morbidity and mortality, primarily results from atherosclerotic lesions in the coronary arteries, which can progress to stroke and myocardial infarction.1 Cardiovascular incidents such as heart failure, myocardial infarction, stroke, and cerebral thrombosis are common causes of morbidity and mortality among CHD patients.2 In mainland China, the economic burden imposed by CHD, particularly the direct costs, is more substantial compared to developed nations.3 Although remarkable progress has been made in CHD management, predicting adverse coronary events remains difficult.4 Moreover, elderly patients often exhibit variations in drug response and metabolism due to age-related physiological decline and comorbidities; therefore, they are prone to adverse drug complications and reactions.5 Thus, early and precise identification of older CHD patients at high risk of severe coronary artery stenosis (CAS) is clinically essential for optimizing therapeutic approaches and enhancing outcomes.
Preoperative coronary angiography (CAG) is a well-established standard for evaluating significant CAS.6,7 Despite being relatively safe, CAG remains an invasive procedure and has potential risks, particularly in patients with CHD and other comorbidities.8 Additionally, current imaging techniques have limitations. CAG images often suffer from low resolution, poor contrast, and considerable noise or artifacts, which complicate the segmentation of blood vessels.9 These challenges are especially relevant in elderly patients, who frequently present with complications such as renal insufficiency, coagulation disorders, or general intolerance to CAG.10 Such factors underscore the need for more suitable alternative diagnostic approaches.
The systemic immune-inflammation index (SII), a recently developed inflammatory biomarker, is calculated from peripheral neutrophil count (NEUT), lymphocyte count (LYM), and platelet count (PLT).11,12 As one of the innovative inflammatory indicators compared to traditional peripheral blood cell markers, it can predict the occurrence and prognosis of CHD.13 A myriad of evidence indicates that SII can rapidly and accurately identify CHD in young adults with chest pain,14,15 predict CAS severity in CHD patients,16 and serve as an independent risk factor (IRF) for coronary atherosclerotic heart disease and CAS severity.17,18 Owing to its clinical accessibility and low cost, SII represents a convenient and cost-effective tool for CHD detection.15 Emerging evidence has validated that the SII serves as a powerful prognostic biomarker in patients diagnosed with acute coronary syndrome.19 Furthermore, inflammation and lipid metabolism have been shown to be closely interrelated.20 For instance, the ratio of monocyte or white blood cell count to high-density lipoprotein cholesterol (HDL-C) has been identified as a predictor of long-term adverse outcomes in patients following percutaneous coronary intervention.21,22 Further supporting this link, the high-sensitivity C-reactive protein to HDL-C ratio (hsCRP/HDL-C) has been identified as a significant risk factor for cardiovascular disease in US adults.23 However, the relevance of the SII and hsCRP/HDL-C ratio to CAS severity in older patients with CHD remains unexplored. The objective of this study was to systematically evaluate correlations of both SII and the hsCRP/HDL-C ratio with CAS severity in older individuals with CHD. This study is expected to offer clinicians a simple, low-cost method to more accurately identify high-risk older CHD patients for intensified intervention and improved clinical management.
Materials and Methods
Participants
A total of 1,092 patients with suspected CHD from the Department of Cardiology of Yongchuan Hospital of Chongqing Medical University between January 2023 and June 2025 were retrospectively selected. Based on the inclusion and exclusion criteria, 786 older patients with CHD were ultimately enrolled as the study subjects. Following a ratio of 7:3,24 all participants were randomly assigned to the training set (n = 550) and the validation set (n = 236). The training set data were utilized to identify influencing factors for the severity of CAS in older CHD patients and to establish a predictive model. The validation set data were employed to assess the validity of the model. Subsequently, based on their Gensini scores (GS), older patients with CHD within both the training and validation sets were further classified into the mild stenosis group (≤ 20 points, n = 214/85), the moderate stenosis group (21–45 points, n = 196/82), and the severe stenosis group (> 45 points, n = 140/69). This study complied with the Declaration of Helsinki and was approved by the Ethics Committee of Yongchuan Hospital of Chongqing Medical University (No. 2025EC0249).
Inclusion and Exclusion Criteria
Inclusion criteria were as follows: (1) aged ≥ 60 years and < 80 years; (2) diagnosed with CHD by CAG.
Exclusion criteria were as follows: (1) incomplete clinical data; (2) severe hepatic or renal dysfunction; (3) complication of malignant arrhythmia, heart failure, valvular heart disease, or myocarditis; (4) autoimmune diseases, hematological system diseases, or active malignancy; (5) recent acute cerebrovascular disease; (6) a history of percutaneous coronary intervention or coronary artery bypass grafting surgery.
Diagnostic Criteria for CHD
Diagnostic criteria for CHD included clinical manifestations of myocardial ischemia (chest pain or chest tightness, etc.) and a degree of stenosis ≥ 50% in any of the following four major branches: the left main coronary artery, left anterior descending artery, left circumflex artery, or right coronary artery, as revealed by percutaneous CAG results.
Assessment of CAS Severity Using GS
Based on the angiographic results, each coronary artery segment was evaluated for the location and degree of stenosis. GS was calculated as the sum of the baseline score for the most severe stenosis at each lesion multiplied by the corresponding coefficient (Table 1). According to GS, a score ≤ 20 was defined as mild stenosis, a score between 21 and 45 (inclusive) as moderate stenosis, and a score > 45 as severe stenosis.
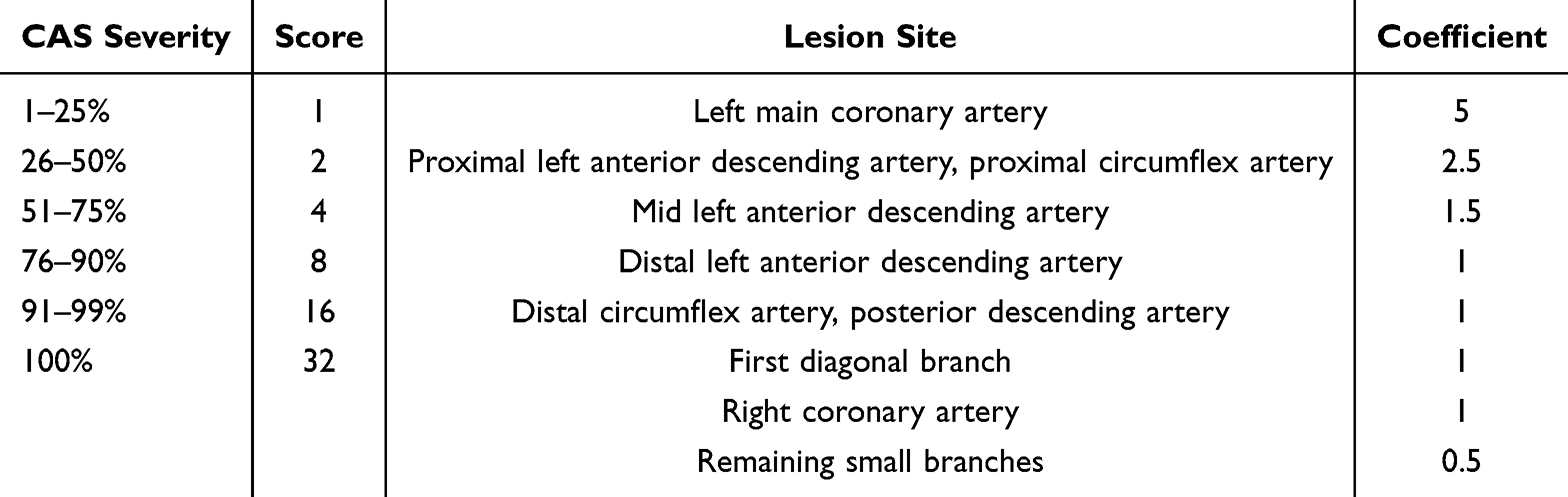 |
Table 1 Weighting Coefficients of Different Coronary Artery Lesion Sites |
Collection of Medical Record Data
General clinical data were gathered for all patients, including age, sex, body mass index (BMI), diabetes, hypertension, smoking history, and drinking history. A smoking history was defined as smoking one or more cigarettes per day for a minimum of six months prior to hospitalization.25 A drinking history was defined as an average weekly intake of at least 100 grams of alcohol for over one year prior to hospitalization.26
Additional laboratory parameters were acquired at the time of admission, including PLT, white blood cell count (WBC), total cholesterol (TC), triacylglycerol (TG), low-density lipoprotein cholesterol (LDL-C), HDL-C, creatinine (Cr), GS, hsCRP, NEUT, LYM, and glycosylated hemoglobin A1c (HbA1c). SII = PLT × NEUT/LYMPH. hsCRP/HDL-C was calculated as below: hsCRP/HDL-C = hsCRP (mg/L)/ [HDL-C (mmol/L) * 386.65].27
Statistical Analysis
Data analysis and graph generation were conducted utilizing SPSS 27.0 (IBM, Armonk, NY, USA) and GraphPad Prism 9.5 (GraphPad, San Diego, CA, USA) software. Data normality was assessed using the Kolmogorov–Smirnov test. Normally distributed measurement data were presented as mean ± standard deviation (SD) and were compared between groups using the independent sample t-test. Non-normally distributed measurement data were expressed as the median (minimum, maximum). Inter-group comparisons were conducted utilizing the Mann–Whitney U-test. Categorical variables were depicted as counts and percentages. The Spearman correlation analysis was employed to evaluate correlations of SII and hsCRP/HDL-C with GS in CHD patients.
Additionally, the variables with p < 0.05 in the univariate analysis were incorporated into the multivariate logistic regression analysis to identify IRFs for severe CAS or coronary occlusion. The Enter method was employed for variable inclusion. Odds ratios (OR) and their corresponding 95% confidence intervals (CI) were calculated. Multicollinearity was assessed by examining the variance inflation factor (VIF); a VIF < 5 indicates no significant multicollinearity among the explanatory variables, whereas a VIF ≥ 5 suggests the presence of multicollinearity. Interaction terms were constructed, and stratified regression analysis was performed. The Chow test was used to compare differences in regression coefficients between the two groups. The predictive value of SII and hsCRP/HDL-C, both individually and in combination, was evaluated using the receiver operating characteristic (ROC) curve analysis. Comparisons of multiple areas under ROC curves (AUCs) were carried out using MedCalc 20.0.15 software (MedCalc Software, Ostend, Belgium). p < 0.05 was considered statistically significant.
Results
Comparisons of Clinical Baseline Data Between Training and Validation Sets in Older Patients with CHD
The two sets showed no statistically significant differences in terms of age, sex, BMI, diabetes, hypertension, smoking history, drinking history, PLT, WBC, TC, TG, LDL-C, HDL-C, GS, Cr, NEUT, LYM, hsCRP, HbA1c, SII, and hsCRP/HDL-C (all p > 0.05) (Table 2).
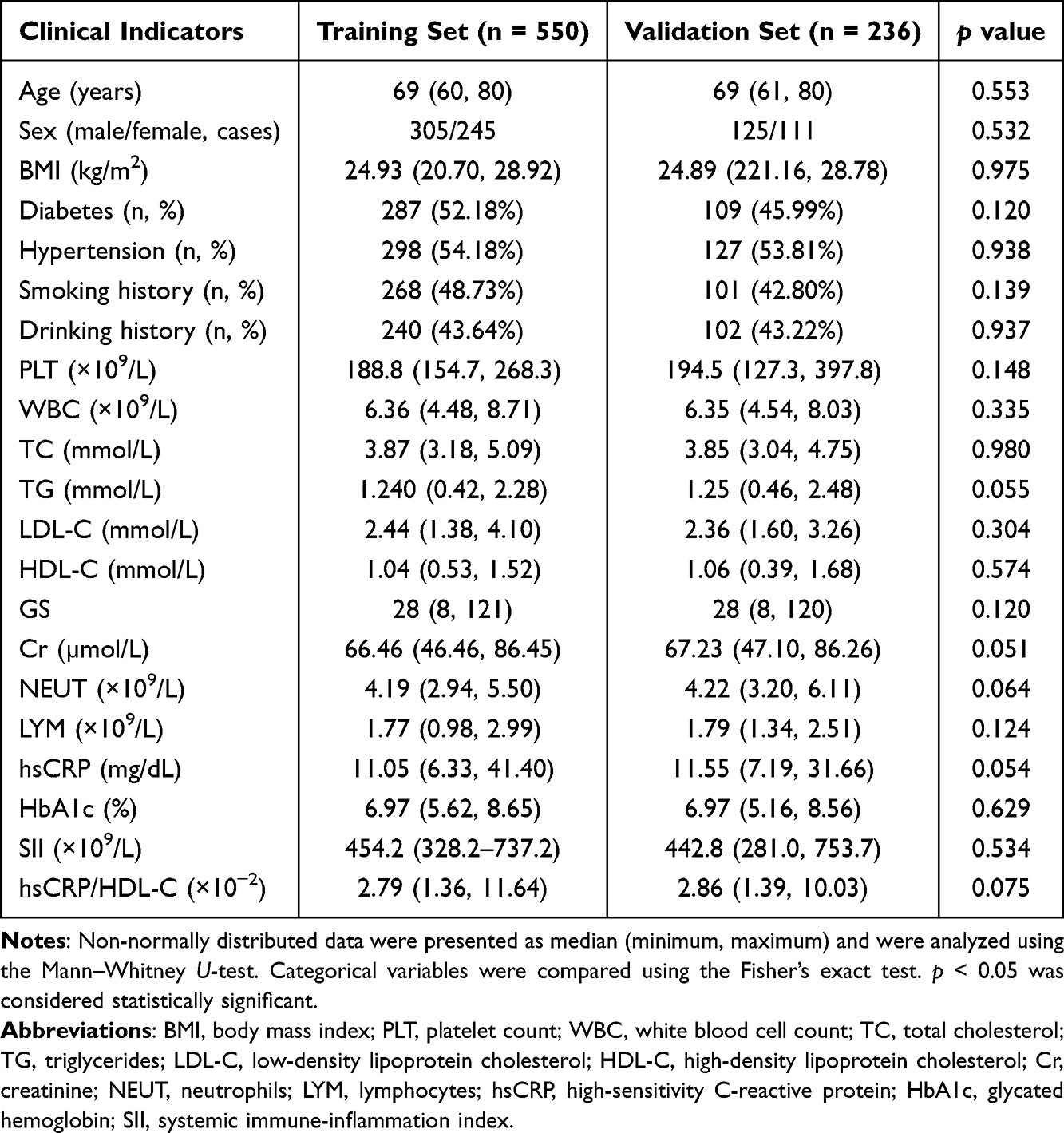 |
Table 2 Comparisons of Clinical Baseline Data of Older Patients with CHD Between Training and Validation Sets |
Comparisons of Clinical Baseline Data Among Older Patients with CHD with Varying Degrees of CAS
Patients in the training and validation sets were subsequently stratified by GS into mild stenosis, moderate stenosis, and severe stenosis groups. Patients in the training set exhibited significant differences in BMI, hypertension, PLT, TG, LDL-C, HDL-C, GS, Cr, NEUT, LYM, hsCRP, and HbA1c (all p < 0.05), whereas no statistically significant differences were observed for age, sex, diabetes, smoking history, drinking history, WBC, and TC (all p > 0.05). In the validation set, significant differences were observed for BMI, hypertension, PLT, TG, LDL-C, HDL-C, GS, Cr, NEUT, hsCRP, and HbA1c (all p < 0.05), while no statistically significant differences were found for age, sex, diabetes, smoking history, drinking history, WBC, TC, and LYM (all p > 0.05) (Table 3).
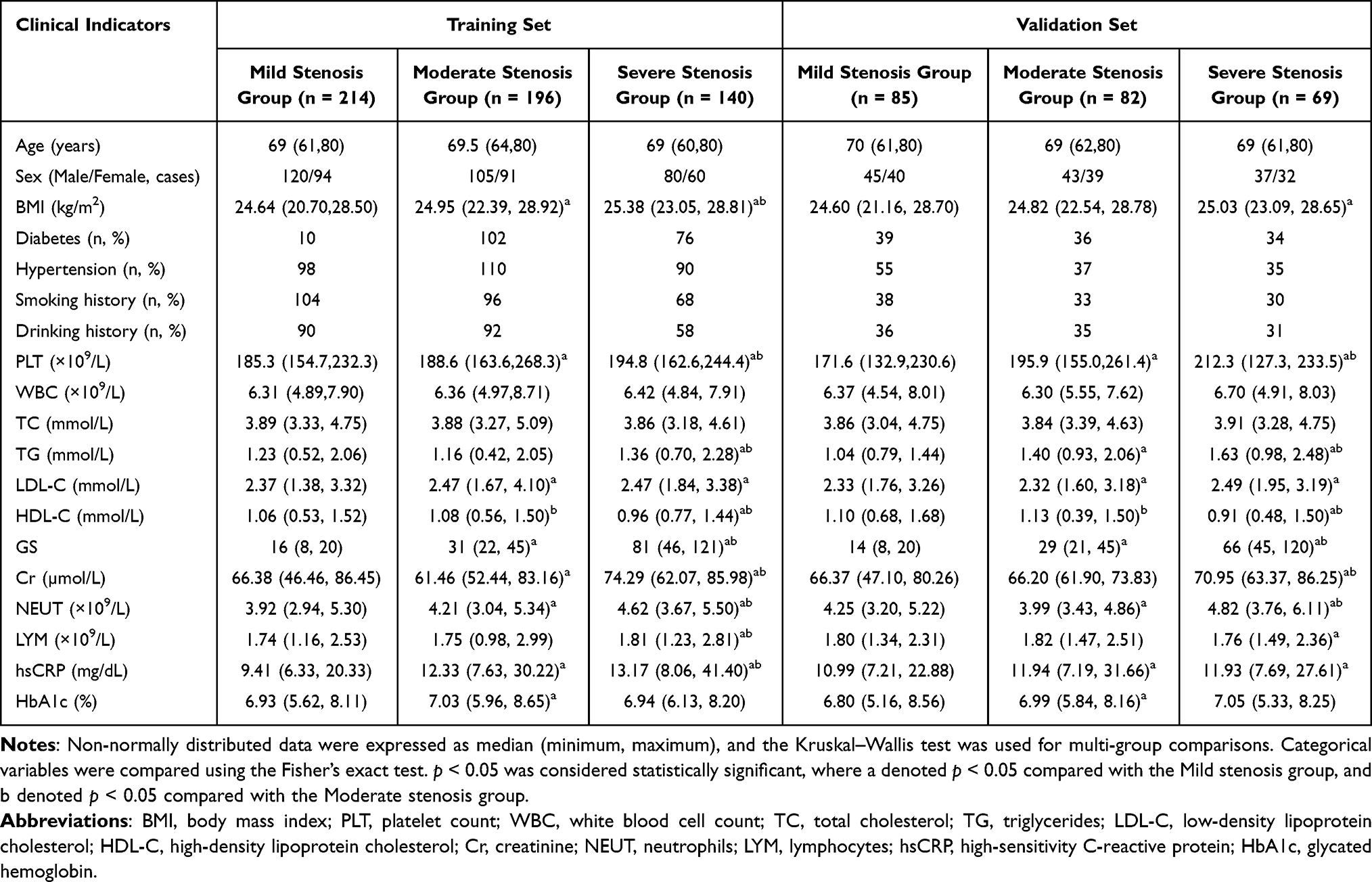 |
Table 3 Comparisons of Clinical Baseline Data Among Patients with Different Degrees of CAS in Training and Validation Sets |
Associations of SII and hsCRP/HDL-C with CAS Severity in Older Patients with CHD
A comparative analysis among groups revealed that SII and hsCRP/HDL-C values were elevated in patients in the moderate or severe stenosis group relative to those in the mild stenosis group (all p < 0.05) (Table 4).
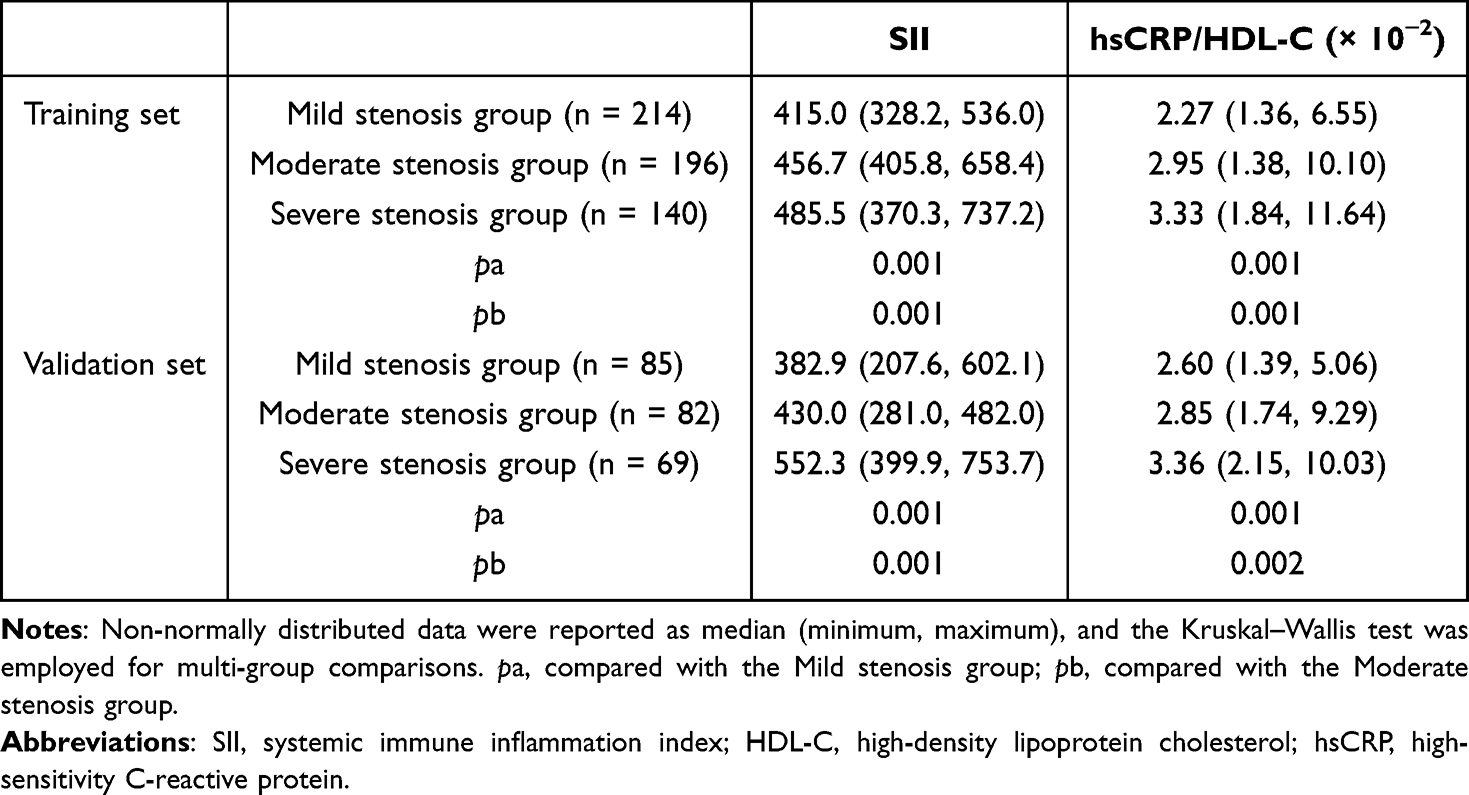 |
Table 4 Comparisons of SII and hsCRP/HDL-C Among Patients with Different Degrees of CAS |
Correlation Analyses of SII and hsCRP/HDL-C with GS in Older Patients with CHD
The Spearman correlation analysis was performed to assess the correlations of SII and hsCRP/HDL-C with GS. In the training set, positive correlations were observed between SII and GS (r = 0.6874, p < 0.01), as well as between hsCRP/HDL-C and GS (r = 0.4524, p < 0.01). In the validation set, both SII (r = 0.6404, p< 0.01) and hsCRP/HDL-C (r = 0.3534, p < 0.01) showed positive correlations with GS (Table 5). Overall, the severity of CAS progressively increased in older patients with CHD as SII and hsCRP/HDL-C levels elevated.
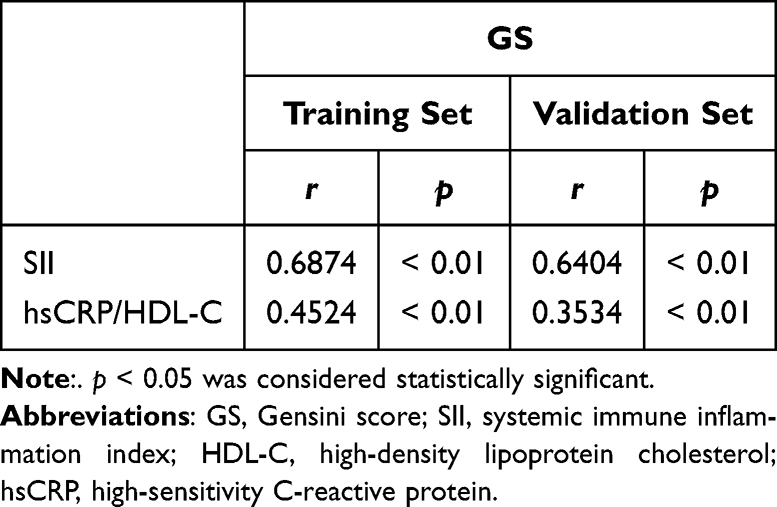 |
Table 5 Correlation Analysis of SII and hsCRP/HDL-C with GS in Older Patients with CHD |
SII and hsCRP/HDL-C Were IRFs for Moderate and Severe CAS in Older Patients with CHD
CAS severity (mild stenosis group = 0, moderate and severe stenosis group = 1) was used as the dependent variable, and potential influencing factors for moderate-to-severe CAS in older patients with CHD (age, sex, BMI, diabetes, hypertension, smoking history, drinking history, PLT, WBC, TC, TG, LDL-C, HDL-C, Cr, NEUT, LYM, hsCRP, HbA1c, SII, hsCRP/HDL-C) were first subjected to the univariate logistic regression analysis. The results showed that age, BMI, hypertension, PLT, WBC, HDL-C, Cr, NEU, hsCRP, HbA1c, SII and hsCRP/HDL-C were potential risk factors for moderate-to-severe CAS in elderly CHD patients. The VIF was further used to evaluate multicollinearity, and variables with a VIF ≥ 5 were excluded to ensure model stability.
Furthermore, the variables with p < 0.05 and VIF < 5 in the univariate analysis were then included as independent variables for the multivariate logistic regression analysis. After adjusting for NEUT (p = 0.001, OR = 4.563) in the training set, elevated SII (p = 0.001, OR = 1.055) and hsCRP/HDL-C (p = 0.001, OR = 2.785) were IRFs for the development of moderate and severe CAS in older patients with CHD (Table 6).
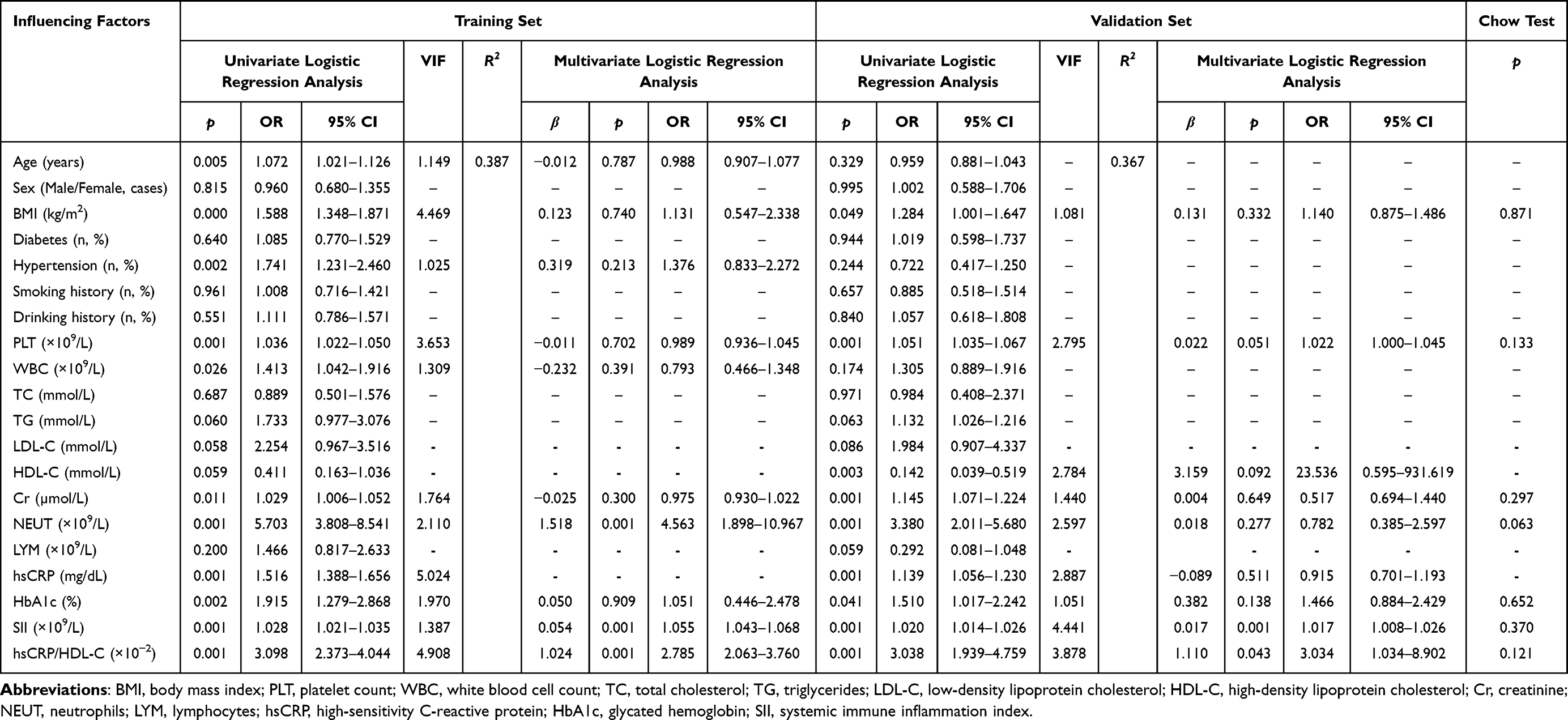 |
Table 6 Logistic Regression Analysis of Factors Influencing the Development of Moderate-to-Severe CAS in Ageing CHD Patients |
Further, increased SII (p = 0.001, OR = 1.017) and hsCRP/HDL-C (p = 0.043, OR = 3.034) in the validation set were identified as IRFs for moderate-to-severe CAS in older patients with CHD. Furthermore, interaction terms were constructed for a stratified regression analysis on the training set (R2 = 0.387) and the validation set (R2 = 0.367). The Chow test was adopted to compare the regression coefficients of common variables in these two sets, including BMI, PLT, Cr, NEU, HbA1c, SII, and hsCRP/HDL-C. All interaction terms showed p > 0.05, indicating good model consistency and absence of substantial multicollinearity (Table 6).
ROC Curve Analysis of Predictive Value of SII and hsCRP/HDL-C for CAS Severity in Older Patients with CHD
The ROC curve analysis was conducted to evaluate the predictive value of SII and hsCRP/HDL-C for CAS severity. In the training set, the AUC of SII for predicting CAS severity in older patients with CHD was 0.865 (444.02 cut-off value, 83.33% sensitivity, 92.99% specificity), that of hsCRP/HDL-C was 0.766 (2.31 cut-off value, 88.99% sensitivity, 52.80% specificity) (Figure 1A and B). In the validation set, the AUC of SII for predicting CAS severity was 0.846 (cut-off value = 450.31, sensitivity = 64.24%, specificity = 90.59%), that of hsCRP/HDL-C was 0.711 (cut-off value = 2.71, sensitivity = 73.51%, specificity = 63.53%) (Figure 1D and E). The findings suggested that both SII and hsCRP/HDL-C demonstrated certain predictive value for the development of severe stenosis or occlusion in older patients with CHD.
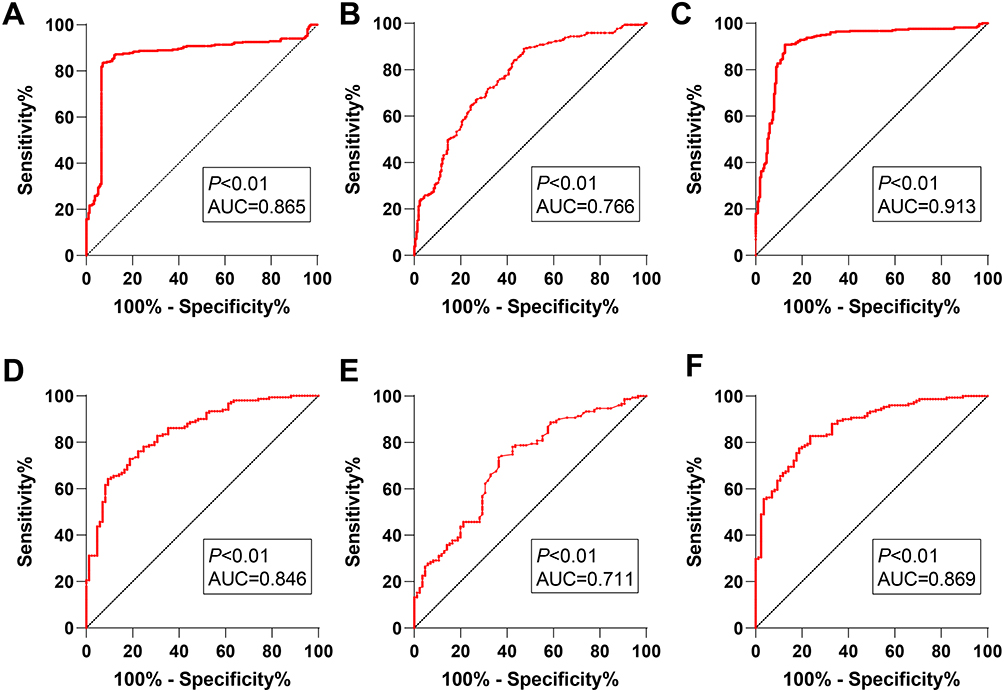 |
Figure 1 ROC curve analysis of SII, hsCRP/HDL-C, and their combination for predicting CAS severity in older patients with CHD. The ROC curve analysis was used to evaluate the predictive value of SII (A and D), hsCRP/HDL-C (B and E), and their combination (C and F) for CAS severity in older patients with CHD in the training set and the validation set. |
To further improve predictive efficacy, a diagnostic model based on SII combined with hsCRP/HDL-C was established. In the training set, the combined model yielded an AUC of 0.913 at a cut-off value of 0.56, with a sensitivity of 90.77%, and a specificity of 87.38% (Figure 1C). In the validation set, the AUC was 0.869 at the same cut-off value of 0.56, with a sensitivity of 82.78%, and a specificity of 76.47% (Figure 1F). The combined model yielded notably higher diagnostic value than either marker alone (p < 0.05) (Table 7), suggesting superior predictive performance of the combined ROC model. Additionally, no statistically significant difference was observed in the AUC of the combined detection of SII and hsCRP/HDL-C between the training set (AUC = 0.913) and the validation set (AUC = 0.869) (p = 0.109).
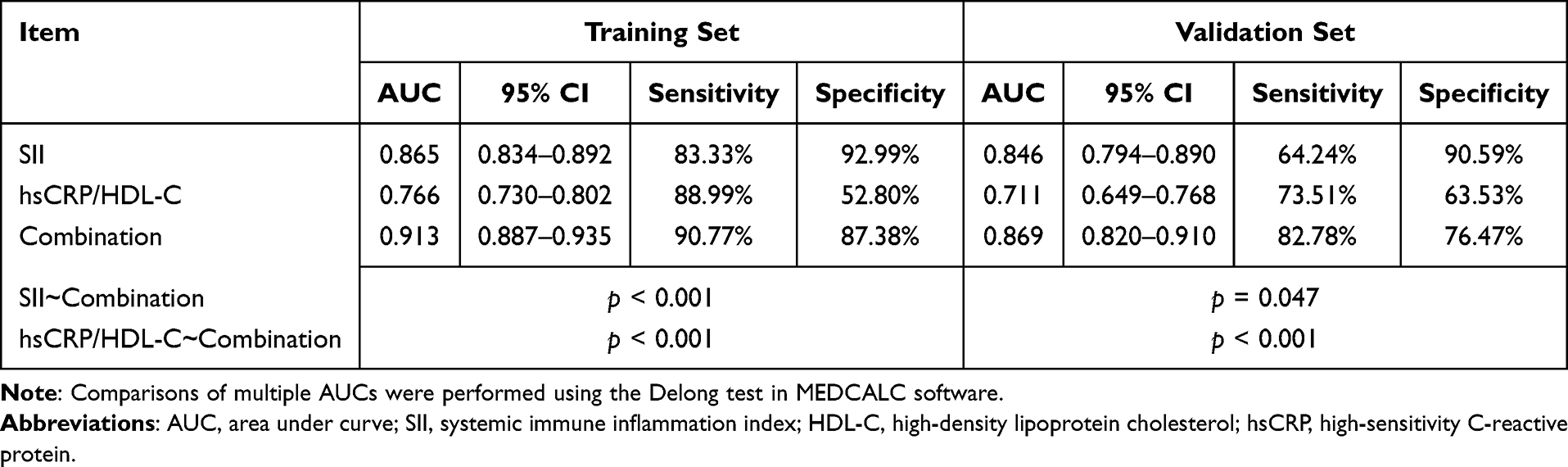 |
Table 7 DeLong Test-Based Comparisons of AUC Values |
ROC Curve Analysis of the Predictive Value of SII and hsCRP/HDL-C Values for CAS Severity in Older Patients with CHD Complicated by Underlying Chronic Diseases
Subgroup ROC analyses of SII and hsCRP/HDL-C in the training and validation sets were performed based on hypertension and diabetes status (Figure 2). The DeLong test was utilized to compare the AUC values among different subgroups. In the validation set, the AUC of SII reached 0.903 in the hypertensive group, which decreased to 0.759 in the non-hypertensive group, showing a significant intergroup difference (p = 0.011) (Table 8). These findings indicated that the discriminating performance of SII was weakened in inflammatory conditions in the absence of hypertension, and hypertension could affect its discriminating ability. Thus, the cut-off value should be adjusted according to hypertensive status in clinical practice.
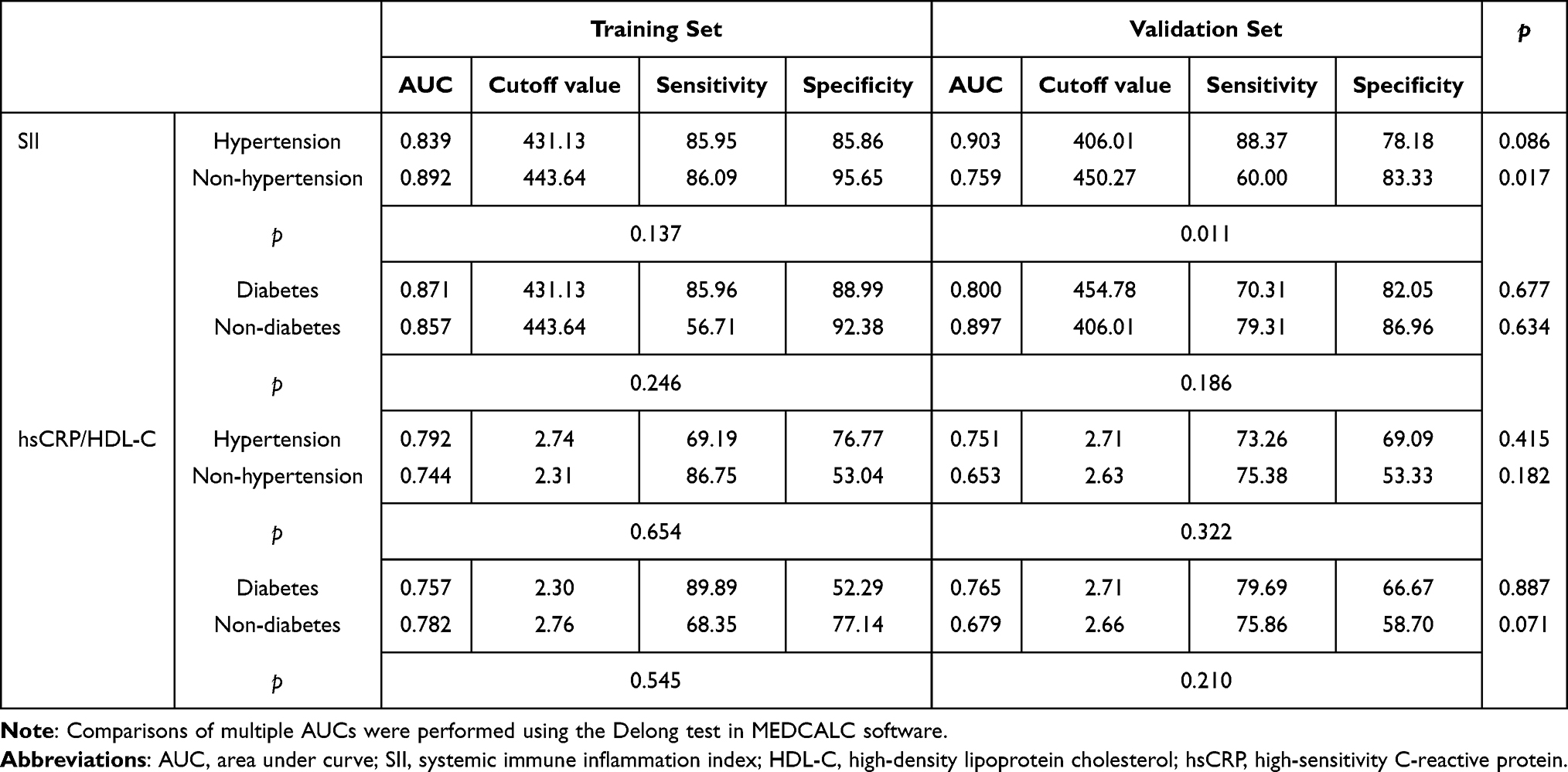 |
Table 8 DeLong Test-Based Comparisons of AUC Values Between Different Subgroups |
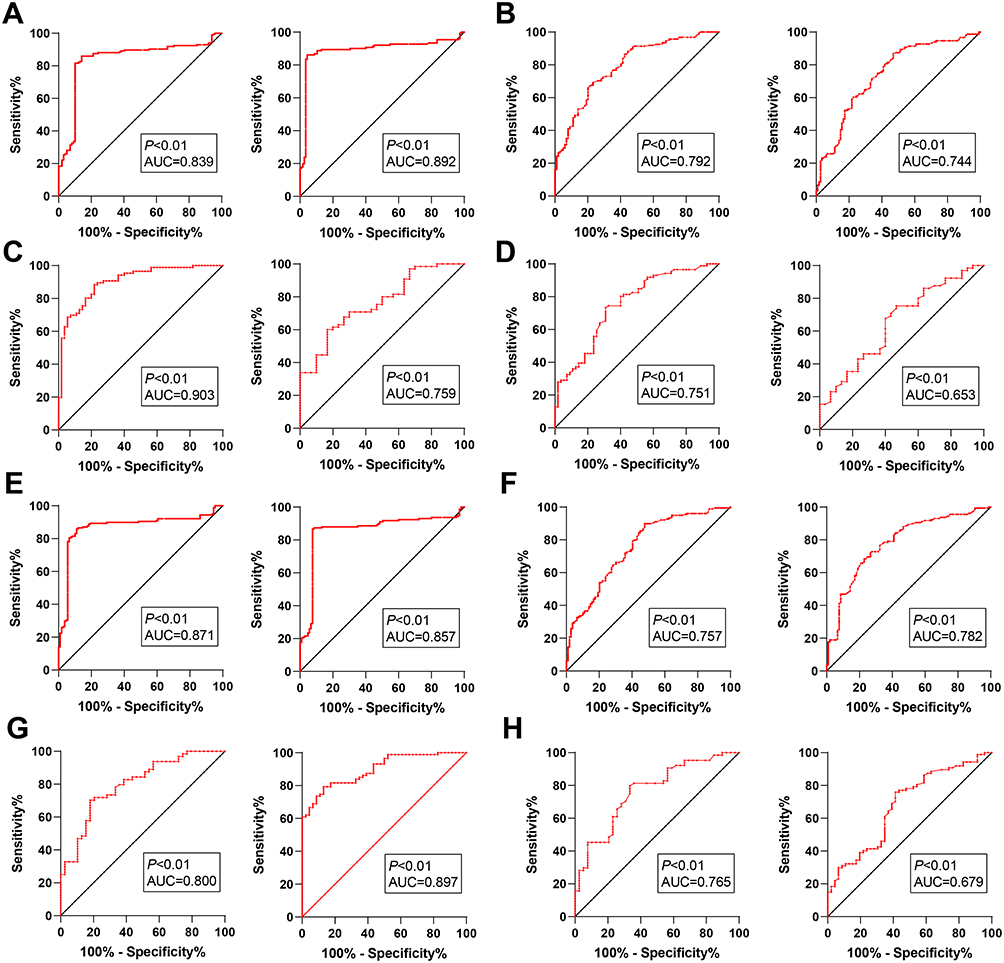 |
Figure 2 ROC curve analysis of SII and hsCRP/HDL-C values for predicting CAS severity in older patients with CHD complicated by underlying chronic diseases. ROC analysis of SII (A and C) and hsCRP/HDL-C (B and D) for predicting CAS severity in CHD population complicated with hypertension in the training and validation sets; ROC analysis of SII (E and G) and hsCRP/HDL-C (F and H) for predicting CAS severity in CHD population complicated with diabetes in the training and validation sets. |
Notably, diabetes exerted no significant stratified effect on the diagnostic performance of the two indicators (p > 0.05) (Table 8), which was not completely consistent with general clinical expectations. Diabetes is commonly recognized as a strong pro-inflammatory state that may amplify the signals of inflammatory biomarkers. However, our data suggested that diabetes might alter the baseline inflammatory levels in both cases and controls, thereby narrowing the discriminatory capacity of the model.
Among elderly CHD patients with or without hypertension and diabetes, no notable differences were found in the AUC values of hsCRP/HDL-C in the training and validation sets (p > 0.05). Although the results were comparable between the two sets, the predictive values remained at a moderate level, suggesting acceptable subgroup stability but limited clinical applicability. For SII, favorable internal consistency was observed in the hypertensive subgroup (training set AUC: 0.839 vs. validation set AUC: 0.903). By contrast, a notable decline was seen in the non-hypertensive group (0.892 vs. 0.759, p = 0.017), indicating poor stability of SII in this subgroup. For the screening of non-hypertensive populations, insufficient sensitivity (declining from 86.09% to 60.00%) may increase the risk of missed diagnosis (Table 8).
Discussion
Monocytes/HDL-C ratio can serve as an independent predictor for CHD and long-term adverse cardiovascular events in elderly patients, and it is positively related to the degree of coronary artery lesions.28 Moreover, an observational study has proposed that SII is an independent predictor for functionally significant CAS in patients with chronic coronary syndrome.29 This study further demonstrates that both SII and hsCRP/HDL-C are independently associated with CAS severity (assessed by the GS) in older patients with CHD. Their combination exhibits favorable predictive performance for CAS severity in older patients with CHD. These findings, including group differences, correlation with severity, independent predictive value, and strong predictive performance, were consistently confirmed in both training and validation sets, which supported the reliability of our results.
SII, which integrates NEUT, LYM, and PLT, provides more comprehensive information on systemic inflammation than many other biomarkers.16,30,31 SII is closely associated with cardiovascular-cause and all-cause mortality in a long-term (20-year) follow-up cohort investigation on 42,875 US adults.32 A strong association exists between SII levels and coronary plaque burden severity as observed by CAG, particularly in patients suffering from CHD.19 Prior studies have also documented an independent association between SII and cardiovascular events after percutaneous coronary intervention30 and a similar link between SII and GS in patients with non-alcoholic fatty liver disease and CHD comorbidity.18 Notably, a study conducted by H Kitano et al has revealed that SII is positively interrelated with CAS severity and has an excellent predictive value in determining the occurrence of CHD and severe CAS.16 Evidence also indicates that elevated SII levels and elevated plaque thickness are associated with atherosclerotic plaque vulnerability in patients with CAS and may signal aggravated CAS.33 In our investigation, SII was elevated in CHD patients with moderate-to-severe CAS. Our study data consistently revealed a positive correlation between SII and CAS severity (assessed by GS) in older patients with CHD. As SII levels increased, CAS severity progressively worsened in older patients with CHD. Intriguingly, our study emphasized that, based on the logistics regression analyses, SII served as an IRF for moderate-to-severe CAS in older patients with CHD. This may be similar to the finding that SII is a key risk factor for coronary artery lesions at admission in either unadjusted or confounder-adjusted models.34 SII remained stable in the hypertensive population, but its efficacy decreased evidently in the non-hypertensive population. Although hypertension may limit the predictive performance of SII, diabetes did not induce such a stratified effect, which is slightly different from the clinical expectation. The reason may be explained by the fact that diabetes affects baseline inflammation in both cases and controls, narrowing its discriminatory capacity.
Owing to the limited diagnostic performance of a single marker, previous studies have paid attention to the combined effects of lipid and inflammatory indicators. hsCRP is a validated inflammatory marker associated with cardiovascular events.35–37 Unlike most lipids, HDL-C can facilitate reverse cholesterol transport and regulate inflammation, exhibiting an adverse correlation with cardiovascular event risk.38 hsCRP/HDL-C also provides enhanced value for predicting cardiovascular risk.39 Observably, our study found that hsCRP/HDL-C was elevated in older patients with CHD with moderate-to-severe stenosis. The epidemiological meta-analysis has shown that hsCRP levels > 3.0 mg/dL increase CAD risk 1.6-fold and correlate with greater lesion count and CHD severity,40 while each 1 mg/dL increment in HDL-C reduces cardiovascular risk by 2–3%.41,42 Furthermore, high-risk hsCRP is independently linked with CAS progression.43 Bilhorn et al have suggested that elevated hsCRP (> 3 mg/L) negates the protective association of HDL-C with CHD.44 Moreover, hsCRP/HDL-C has been reported to be positively interrelated with GS and is an independent predictor of CAD.45 A recent study has proposed hsCRP/HDL-C as a risk factor for cardiometabolic multimorbidity in the middle-aged and elderly population.46 Consistent with this finding, our study also identified hsCRP/HDL-C elevation to be an IRF for moderate-to-severe CAS in older patients with CHD. While each marker alone demonstrated a good predictive ability (AUCs of 0.865 and 0.846 for SII and 0.766 and 0.711 for hsCRP/HDL-C), their combination yielded significantly higher AUCs of 0.913 and 0.869 in the training and validation sets, respectively. This indicates a superior predictive performance of this combination for CAS severity in older patients with CHD.
However, several limitations of this study should be acknowledged. First, the single-center retrospective design may reduce the generalizability of the results. Given the retrospective design, there is a lack of complete data on medication types, dosages, treatment courses, and compliance. Second, not all potential confounders were fully included in this research. In this study, patients aged over 80 years were excluded because the super-aged population usually has multiple comorbidities and medications that may interfere with inflammatory and immune biomarkers.47 In addition, hypertension influences the diagnostic performance and subgroup stability of SII. Owing to the effects of age, underlying diseases, and treatment history; thus, a unified cut-off value is not suitable for populations with different pathological states. The detection results should be interpreted based on individualized patient characteristics, and if necessary, combining with other clinical indicators and imaging examinations. It is worth noting that acute infection and other stress states, such as chronic obstructive pulmonary disease, can trigger systemic inflammatory responses and elevate neutrophils, hsCRP, and SII levels, causing bias in the evaluation of CAS.48–51 Metabolic disorders such as insulin resistance and obesity can reduce HDL-C levels, further interfering with inflammatory biomarkers.52,53 Although patients with obvious inflammatory confounders were excluded, and chronic comorbidities were adjusted during the analysis, whether other chronic inflammation and metabolic disorders (chronic obstructive pulmonary disease, chronic kidney disease, obesity) may still affect these two indicators is undefined. Also, the absence of stratified correction for drug-related confounders might cause bias. Furthermore, smoking status was only defined in this study as a binary variable without quantitative data on smoking intensity and duration, and detailed medications, such as statins, were not finely controlled,54 restricting accurate assessment as well.
Conclusion
Taken together, our study highlighted that elevated SII and hsCRP/HDL-C were IRFs for moderate-to-severe CAS and had predictive value for assessing CAS severity in older patients with CHD. A pivotal finding of our study was the superior predictive performance of their combination over either marker alone. Furthermore, the statistical rigor of our multivariate regression analysis is underscored by the absence of significant multicollinearity. Despite certain limitations in this study, our findings lay a foundation for in-depth research on risk stratification tools. The combined detection of SII and hsCRP/HDL-C is expected to become an effective, auxiliary risk stratification method for optimizing the clinical management of older patients with CHD. In future studies, we will adopt multi-center, prospective designs, expand the sample size, and combine individualized characteristics to better interpret test results. Additionally, we would like to conduct subgroup analyses based on different diseases to clarify the effect size of different interfering factors and dynamically monitor the association between these indicators and the progression of CAS in the following studies.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
This study complied with the Declaration of Helsinki and was approved by the Ethics Committee of Yongchuan Hospital of Chongqing Medical University (No. 2025EC0249). The requirement for informed consent was waived due to the retrospective nature of the study and the use of de-identified data.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report there are no competing interests to declare.
References
1. Wu H, Chiou J. Potential benefits of probiotics and prebiotics for coronary heart disease and stroke. Nutrients. 13(8). doi:10.3390/nu13082878
2. Ma R, Gao J, Mao S, Wang Z. Association between heart rate and cardiovascular death in patients with coronary heart disease: a NHANES-based cohort study. Clin Cardiol. 2022;45(5):574–15. doi:10.1002/clc.23818
3. Mi Y, Xue Z, Qu S, et al. The economic burden of coronary heart disease in mainland China. Public Health. 2023;224:140–151. doi:10.1016/j.puhe.2023.08.034
4. Kwiecinski J, Tzolos E, Williams MC, et al. Noninvasive coronary atherosclerotic plaque imaging. JACC Cardiovasc Imaging. 2023;16(12):1608–1622. doi:10.1016/j.jcmg.2023.08.021
5. Galiuto L, Barchetta S, Fedele E, et al. Effects of late reopening of coronary total occlusion on micRovascular perfusion and myocarDial function: the RECORD study. Eur Heart J Cardiovasc Imaging. 2013;14(5):487–494. doi:10.1093/ehjci/jes188
6. Nishimura RA, Otto CM, Bonow RO, et al. AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Thorac Cardiovasc Surg. 2014;148(1):e1–e132. doi:10.1016/j.jtcvs.2014.05.014
7. Nishimura RA, Otto CM, Bonow RO, et al. AHA/ACC Focused Update of the 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/american Heart Association task force on clinical practice guidelines. J Am Coll Cardiol. 2017;70(2):252–289. doi:10.1016/j.jacc.2017.03.011
8. Elagha A, Khaled W, Gamal S, Helmy M, Kaddah A. Coronary computed tomography versus coronary angiography for preoperative coronary assessment before valve surgery. Egypt Heart J. 2021;73(1):63. doi:10.1186/s43044-021-00180-7
9. Shen Y, Chen Z, Tong J, Jiang N, Ning Y. DBCU-Net: deep learning approach for segmentation of coronary angiography images. Int J Cardiovasc Imaging. 2023;39(8):1571–1579. doi:10.1007/s10554-023-02849-3
10. Knuuti J, Wijns W, Saraste A, et al. ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J. 2019;41(3):407–477. doi:10.1093/eurheartj/ehz425
11. Dolu AK, Karayigit O, Ozkan C, Celik MC, Kalcik M. Relationship between intracoronary thrombus burden and systemic immune-inflammation index in patients with ST-segment elevation myocardial infarction. Acta Cardiol. 2023;78(1):72–79. doi:10.1080/00015385.2022.2035082
12. Bagci A, Aksoy F. Systemic immune-inflammation index predicts new-onset atrial fibrillation after ST elevation myocardial infarction. Biomarker Med. 2021;15(10):731–739. doi:10.2217/bmm-2020-0838
13. Wu X, Zhang H, Liu H. Systemic immune-inflammation index and systemic inflammation response index levels are associated with coronary heart disease prevalence in the asthmatic population: a cross-sectional analysis of the NHANES 2011-2018. Front Public Health. 2025;13:1514016. doi:10.3389/fpubh.2025.1514016
14. Wang C, Yan W, Ren M, Zhong L. Screening significance of systemic immune-inflammation index (SII) and systemic inflammation response index (SIRI) in coronary heart disease of symptomatic youth. Immun Inflamm Dis. 2024;12(8):e1369. doi:10.1002/iid3.1369
15. Ma J, Li K. Systemic immune-inflammation index is associated with coronary heart disease: a cross-sectional study of NHANES 2009-2018. Front Cardiovasc Med. 2023;10:1199433. doi:10.3389/fcvm.2023.1199433
16. Liu Y, Ye T, Chen L, et al. Systemic immune-inflammation index predicts the severity of coronary stenosis in patients with coronary heart disease. Coron Artery Dis. 32(8):715–720. doi:10.1097/MCA.0000000000001037
17. Yilu Z, Zhanglong W, Fanke H, et al. The progression of non-culprit coronary lesion is related to higher SII, SIRI, and PIV in patients with ACS. Medicine. 2024;103(52):e41094. doi:10.1097/MD.0000000000041094
18. Dong W, Gong Y, Zhao J, Wang Y, Li B, Yang Y. A combined analysis of TyG index, SII index, and SIRI index: positive association with CHD risk and coronary atherosclerosis severity in patients with NAFLD. Front Endocrinol. 2023;14:1281839. doi:10.3389/fendo.2023.1281839
19. Wang H, Huang Z, Wang J, et al. Predictive value of system immune-inflammation index for the severity of coronary stenosis in patients with coronary heart disease and diabetes mellitus. Sci Rep. 2024;14(1):31370. doi:10.1038/s41598-024-82826-5
20. Secen O, Uslu MF. Role of nutritional status in acute coronary syndrome patients with diabetes. Medicina. 2025;61(4). doi:10.3390/medicina61040740
21. Zhang DP, Baituola G, Wu TT, et al. An elevated monocyte-to-high-density lipoprotein-cholesterol ratio is associated with mortality in patients with coronary artery disease who have undergone PCI. Biosci Rep. 2020;40(8). doi:10.1042/BSR20201108
22. Wu TT, Zheng YY, Xiu WJ, et al. White blood cell counts to high-density lipoprotein cholesterol ratio, as a novel predictor of long-term adverse outcomes in patients after percutaneous coronary intervention: a retrospective cohort study. Front Cardiovasc Med. 2021;8:616896. doi:10.3389/fcvm.2021.616896
23. Li J, Ma H. Associations of the hs-CRP/HDL-C ratio with cardiovascular disease among US adults: evidence from NHANES 2015-2018. Nutr, Metab Cardiovasc Dis. 2025;35(4):103814. doi:10.1016/j.numecd.2024.103814
24. Ding W, Li T, Fang C, Zhang W XX, Wang E. Association of non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio with coronary heart disease: establishment and validation of a clinical nomogram model. Medicine. 2025;104(11):e41896. doi:10.1097/MD.0000000000041896
25. Ma M, Wu Y, He X, et al. Associations between smoking and coronary heart disease: mediating role of RDW. Front Public Health. 2024;12:1447303. doi:10.3389/fpubh.2024.1447303
26. Wood AM, Kaptoge S, Butterworth AS, et al. Risk thresholds for alcohol consumption: combined analysis of individual-participant data for 599 912 current drinkers in 83 prospective studies. Lancet. 2018;391(10129):1513–1523. doi:10.1016/S0140-6736(18)30134-X
27. Bagenda CN, Nantongo C, Tumusiime J, et al. Association of atherogenic combined index, hs-crp/hdl-c ratio, and tc/hdl-c-bmi index with low vitamin d levels among plwh on antiretroviral therapy: a cross-sectional study in southwestern Uganda. J Int Assoc Provid AIDS Care. 2026;25:23259582261432395. doi:10.1177/23259582261432395
28. He L, Chen S, Zhu X, He F. The change of inflammatory markers may predict long-term major adverse cardiovascular events in elderly patients with coronary heart disease: a retrospective cohort study. Front Med Lausanne. 2024;11:1523581. doi:10.3389/fmed.2024.1523581
29. Erdogan M, Erdol MA, Ozturk S, Durmaz T. Systemic immune-inflammation index is a novel marker to predict functionally significant coronary artery stenosis. Biomarker Med. 2020;14(16):1553–1561. doi:10.2217/bmm-2020-0274
30. Yang YL, Wu CH, Hsu PF, et al. Systemic immune-inflammation index (SII) predicted clinical outcome in patients with coronary artery disease. Eur J Clin Invest. 2020;50(5):e13230. doi:10.1111/eci.13230
31. Hu B, Yang XR, Xu Y, et al. Systemic immune-inflammation index predicts prognosis of patients after curative resection for hepatocellular carcinoma. Clin Cancer Res. 2014;20(23):6212–6222. doi:10.1158/1078-0432.CCR-14-0442
32. Xia Y, Xia C, Wu L, Li Z, Li H, Zhang J. Systemic Immune inflammation index (sii), system inflammation response index (SIRI) and risk of all-cause mortality and cardiovascular mortality: a 20-year follow-up cohort study of 42,875 us adults. J Clin Med. 12(3). doi:10.3390/jcm12031128
33. Wang Y, Chen J, Li X, Tang X, Zhang Y, Yang X. Relationship between carotid intraplaque neovascularization and immune-inflammatory biomarkers with coronary stenosis. Rev Cardiovasc Med. 2025;26(5):28171. doi:10.31083/RCM28171
34. Huang T, Peng Q, Zhang Y, Zhu Z, Fan X. The systemic immune-inflammation index (sii) and coronary artery lesions in kawasaki disease. Clin Exp Med. 2024;24(1):4. doi:10.1007/s10238-023-01265-0
35. Ridker PM, Lei L, Louie MJ, et al. Inflammation and cholesterol as predictors of cardiovascular events among 13 970 contemporary high-risk patients with statin intolerance. Circulation. 2024;149(1):28–35. doi:10.1161/CIRCULATIONAHA.123.066213
36. Denegri A, Boriani G. High sensitivity c-reactive protein (hscrp) and its implications in cardiovascular outcomes. Curr Pharm Des. 2021;27(2):263–275. doi:10.2174/1381612826666200717090334
37. Bassuk SS, Rifai N, Ridker PM. High-sensitivity C-reactive protein: clinical importance. Curr Probl Cardiol. 2004;29(8):439–493.
38. Navab M, Reddy ST, Van Lenten BJ, Fogelman AM. HDL and cardiovascular disease: atherogenic and atheroprotective mechanisms. Nat Rev Cardiol. 2011;8(4):222–232. doi:10.1038/nrcardio.2010.222
39. Gao Y, Wang M, Wang R, et al. The predictive value of the hs-CRP/HDL-C ratio, an inflammation-lipid composite marker, for cardiovascular disease in middle-aged and elderly people: evidence from a large national cohort study. Lipids Health Dis. 2024;23(1):66. doi:10.1186/s12944-024-02055-7
40. Li S, Pan G, Chen H, Niu X. Determination of serum homocysteine and hypersensitive c-reactive protein and their correlation with premature coronary heart disease. Heart Surg Forum. 2019;22(3):E215–E217. doi:10.1532/hsf.2223
41. Kosmas CE, Martinez I, Sourlas A, et al. High-density lipoprotein (HDL) functionality and its relevance to atherosclerotic cardiovascular disease. Drugs Context. 2018;7:212525. doi:10.7573/dic.212525
42. Asztalos BF, Batista M, Horvath KV, et al. Change in α 1 HDL concentration predicts progression in coronary artery stenosis. Arterioscler Thromb Vasc Biol. 2003;23(5):847–852. doi:10.1161/01.ATV.0000066133.32063.BB
43. Liu M, Zhang Z, Zhao Y, et al. Combining ultrasound with bio-indicators reveals progression of carotid stenosis. Ann Palliat Med. 2021;10(11):11539–11547. doi:10.21037/apm-21-2666
44. Bilhorn KR, Luo Y, Lee BT, Wong ND. High-density lipoprotein cholesterol, high-sensitivity C-reactive protein, and cardiovascular disease in United States adults. Am J Cardiol. 2012;110(10):1464–1467. doi:10.1016/j.amjcard.2012.06.056
45. Luo H, Kou T, Yin L. High-sensitivity c-reactive protein to hdl-c ratio. Int Heart J. 2021;62(6):1221–1229. doi:10.1536/ihj.21-246
46. Li S, Liu Y, Sun G, et al. The predictive value of hsCRP/HDL-C ratio for cardiometabolic multimorbidity in middle-aged and elderly people: evidence from a large national cohort study. Front Nutr. 2025;12:1580904. doi:10.3389/fnut.2025.1580904
47. Ramos KA, Boing AC, Andrade JM, Bof de Andrade F. Polypharmacy among older adults in Brazil: association with sociodemographic factors and access to health services. Dialogues Health. 2022;1:100078. doi:10.1016/j.dialog.2022.100078
48. Wang Y, Guan QN, Zhang ZJ, Zhang YM. Interaction between endothelial injury and immune response in septic shock: from basic research to clinical applications. Front Physiol. 2025;16:1627008. doi:10.3389/fphys.2025.1627008
49. Shaukat W, Baig AM, Ali Z, et al. Prognostic value of c-reactive protein and neutrophil-to-lymphocyte ratio in predicting postoperative infections after gastrointestinal surgery: a meta-analysis. Cureus. 2025;17(8):e91123. doi:10.7759/cureus.91123
50. Li Z, Lu Q. The role of neutrophils in autoimmune diseases. Clin Immunol. 2024;266:110334. doi:10.1016/j.clim.2024.110334
51. Feng X, Xiao H, Duan Y, Li Q, Ou X. Prognostic value of neutrophil to lymphocyte ratio for predicting 90-day poor outcomes in hospitalized patients with acute exacerbation of chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2023;18:1219–1230. doi:10.2147/COPD.S399671
52. Stadler JT, Marsche G. Obesity-related changes in high-density lipoprotein metabolism and function. Int J Mol Sci. 2020;21(23). doi:10.3390/ijms21238985
53. Souza DR, Pieri B, Comim VH, et al. Fish oil reduces subclinical inflammation, insulin resistance, and atherogenic factors in overweight/obese type 2 diabetes mellitus patients: a pre-post pilot study. J Diabetes Complications. 2020;34(5):107553. doi:10.1016/j.jdiacomp.2020.107553
54. Koushki K, Shahbaz SK, Mashayekhi K, et al. Anti-inflammatory action of statins in cardiovascular disease: the role of inflammasome and toll-like receptor pathways. Clin Rev Allergy Immunol. 2021;60(2):175–199. doi:10.1007/s12016-020-08791-9
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.