Back to Journals » International Journal of Women's Health » Volume 17
The Surface Electromyography of the Pelvic Floor Muscles in the Early Postpartum Period in Twin Pregnancies of Different Conception Modes: A Single-Centre Retrospective Study in China
Authors Yu S, Chi X, Su X, Ying X, Lv S, Ma J, Wang Y
Received 18 June 2025
Accepted for publication 7 September 2025
Published 19 September 2025 Volume 2025:17 Pages 3087—3095
DOI https://doi.org/10.2147/IJWH.S543734
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Shushu Yu,1,2,* Xiaolei Chi,1,2,* Xiaohan Su,1,2,* Xiang Ying,1,2 Shuping Lv,1,2 Jue Ma,1,2 Yanlin Wang1,2
1Department of Obstetrics and Gynecology, International Peace Maternity and Child Health Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai, 200030, People’s Republic of China; 2Shanghai Key Laboratory of Embryo Original Disease, Shanghai, 200030, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yanlin Wang, Email [email protected]
Purpose: To assess the early postpartum pelvic floor function in twin pregnancies of different conception modalities by measuring surface electromyography of the pelvic floor muscles with the Glazer protocol.
Methods: This retrospective study analyzed 241 twin pregnancies delivered via cesarean section at the International Peace Maternity and Child Health Hospital (IPMCHH), affiliated with Shanghai Jiao Tong University School of Medicine, between March 2019 and December 2023. Participants underwent pelvic floor function assessments 42– 60 days postpartum. Pelvic floor muscle activity was evaluated using surface electromyography (sEMG) following the Glazer protocol. Univariate and multivariable logistic regression analyses were performed to assess the impact of conception modes (natural vs ART) on early postpartum pelvic floor function in twin pregnancies.
Results: The mean anterior resting phase amplitude was 4.80 ± 5.23 μV in the ART group versus 6.38 ± 6.30 μV in the naturally conceived group. Similarly, the posterior resting phase amplitude measured 5.15 ± 5.28 μV (ART) and 6.78 ± 7.67 μV (natural conception). The total Glazer score differed significantly between groups, with ART pregnancies scoring 74.80 ± 14.82 and natural conception pregnancies scoring 67.57 ± 21.57 (P < 0.05). Univariate and multivariable logistic regression analyses confirmed that the total Glazer score during the early postpartum period was independently associated with conception mode (P < 0.05).
Conclusion: Women with twin pregnancies conceived via ART may exhibit marginally improved pelvic floor function during the early postpartum period (6– 8 weeks) compared to naturally conceived counterparts, potentially attributable to elevated estrogen levels associated with ART.
Keywords: twin pregnancies, assisted reproductive technology, ART, Glazer protocol, surface electromyography, sEMG
Introduction
Pelvic floor dysfunction (PFD), often termed a “hidden epidemic”, encompasses pelvic organ prolapse, urinary incontinence, fecal incontinence, and sexual dysfunction, etc.1,2 Epidemiological data indicate that at least 50% of women experience PFD-related symptoms. Risk factors for PFD include advanced age, obesity, parity, the mode of delivery (eg, vaginal vs cesarean), prolonged second stage of labor, instrumental vaginal delivery, perineal trauma, and hormonal fluctuations.3–5 Notably, PFD significantly impacts sexual health and psychological well-being.6
With rising global infertility rates, assisted reproductive technology (ART) has become increasingly prevalent. Twin pregnancies are disproportionately common in ART populations. While ART addresses infertility, it raises concerns about maternal risks, including complications from twin gestation (eg, preterm birth, gestational hypertension) and potential long-term effects of ovarian hyperstimulation. Twin pregnancies may exert additional pressure on the pelvic floor structures due to greater overall fetal weight and more significant uterine enlargement, with greater changes in pelvic structural support during pregnancy in twin pregnancies.7 However, altered hormonal profiles in ART-conceived pregnancies may influence pelvic floor biomechanics postpartum.
Yang X et al found that the Glazer assessment method was more reliable than the manual muscle strength test in evaluating the pelvic floor function of postpartum women.8 This study evaluated early postpartum pelvic floor function in twin pregnancies by comparing ART-conceived and naturally conceived cohorts. Surface electromyography (sEMG) of pelvic floor muscles was performed using the Glazer assessment protocol.8 Univariate and multivariable analyses were employed to assess correlations between conception mode (ART vs natural) and sEMG-derived metrics, including resting tone, phasic contraction amplitudes, and composite Glazer scores.
Materials and Methods
Study Population
This study enrolled 241 primigravid women with twin pregnancies delivered via cesarean section at Shanghai Jiao Tong University Affiliated International Peace Maternity and Children’s Hospital between September 2019 and December 2023. Inclusion criteria were: (1) age ≥20 years; (2) no pre-pregnancy symptoms of pelvic organ prolapse (POP); (3) voluntary participation in standardized pelvic floor function assessments 42–60 days postpartum. Participants were stratified into two cohorts: 153 women who conceived via assisted reproductive technology (ART group) and 88 naturally conceived controls. Written and verbal informed consent was obtained from all participants, with ethical approval granted by the Institutional Review Board of the International Peace Maternity and Child Health Hospital, Shanghai Jiao Tong University School of Medicine (Approval No. GKLW-A- 2024-023-01).
Data Collection
Data were prospectively collected from mothers who returned to the Postpartum Pelvic Floor Rehabilitation Centre for standardized pelvic floor assessments 42–60 days after delivery. This included: (1) general demographic information, (2) clinical identifiers, (3) Glazer protocol-derived sEMG metrics. Trained clinicians at the centre performed sEMG measurements using the Glazer protocol, adhering to a standardized operating procedure. Maternal covariates—age, gestational age, parity, conception mode (ART vs natural), education level, pre-pregnancy BMI, delivery BMI, gestational age at delivery, neonatal birth weight, and pregnancy complications—were extracted from the Obstetric Electronic Medical Record (OEMR) system. Data integration was achieved by linking sEMG results with OEMR entries via the VLOOKUP function (Microsoft Excel 2019), using maternal clinic numbers as unique identifiers.
Outcome Assessment
The evaluation index was the sEMG value of the pelvic floor muscles, which was measured by a modified Glazer protocol. The electromyographic signal acquisition device was a customised vaginal metal probe (CACB04, MLD V1, Med lander Medical Instruments Ltd., Nanjing, China), the processing device was a neuromuscular stimulation instrument (SA9800, MLD B4, Med lander Medical Instruments Ltd.), and the software analysis was performed using the MYOTRAC Infiniti system (The final results were expressed in microvolts (µV)).
As per the Glazer Protocol, we divided the test into two phases: a fast-twitch muscle (Type II fiber) phase and a slow-twitch muscle (Type I fiber) phase. During the fast-twitch muscle evaluation phase, after short-term pelvic floor muscle contractions, the maximum (peak) values were recorded, and the fast-twitch muscle function was evaluated. During the slow-twitch muscle evaluation phase, five slow and gentle PFM contractions and a sustained maximum contraction for 10 seconds were performed with the reported values being the average of five measurements.9 A composite Glazer score ≥80 was classified as normal pelvic floor function.
Covariates
Based on the existing literature, the covariates in this study included the general condition of the mother (age, pre-pregnancy BMI, educational qualification, weight change during pregnancy, number of pregnancies, mode of conception), obstetric clinical conditions (hypertensive disorders of pregnancy, diabetes mellitus of pregnancy, anaemia in pregnancy, thyroid dysfunction in pregnancy, etc.), gestational week of delivery of newborn, and neonatal birth weight.
Statistical Analyses
Applying R 4.3.3 software, categorical variables were expressed as frequencies and percentages, normally distributed variables in continuous variables were expressed as mean ± standard deviation, and non-normally distributed variables were expressed as median ± interquartile spacing. Differences between groups of categorical variables were compared using the X2 test or Fisher’s exact test, and differences between groups of continuous variables were compared using the t test (for normally distributed variables) or the Mann–Whitney rank sum test (for non-normally distributed variables). Glazer scores at different stages of pelvic floor function in the early postpartum period were compared between the two groups using multifactorial logistic regression to correct for confounders, and the difference was considered statistically significant at a two-sided P < 0.05.
Results
The basic characteristics of the study population are shown in Table 1. No statistically significant differences were observed between the assisted reproductive technology (ART) and naturally conceived groups in pre-pregnancy BMI, delivery BMI, educational attainment, or prevalence of gestational hypertension and gestational diabetes mellitus (P > 0.05). However, the ART group exhibited significantly higher proportions of advanced maternal age (≥35 years: 37.25% [57/153] vs 11.36% [10/88]), gestational weight gain <20 kg (81.05% [124/153] vs 65.91% [58/88]), and dichorionic diamniotic (DCDA) twins (89.54% [137/153] vs 54.55% [48/88]) compared to the naturally conceived group. Additionally, the ART group had higher mean neonatal birth weight (5100 ± 935 g vs 4655 ± 774 g), later gestational age at delivery (36.6 ± 1.0 vs 36.2 ± 1.9 weeks), and a greater prevalence of gestational thyroid dysfunction (28.76% [44/153] vs 12.50% [11/88]). All these differences were statistically significant (P < 0.05).
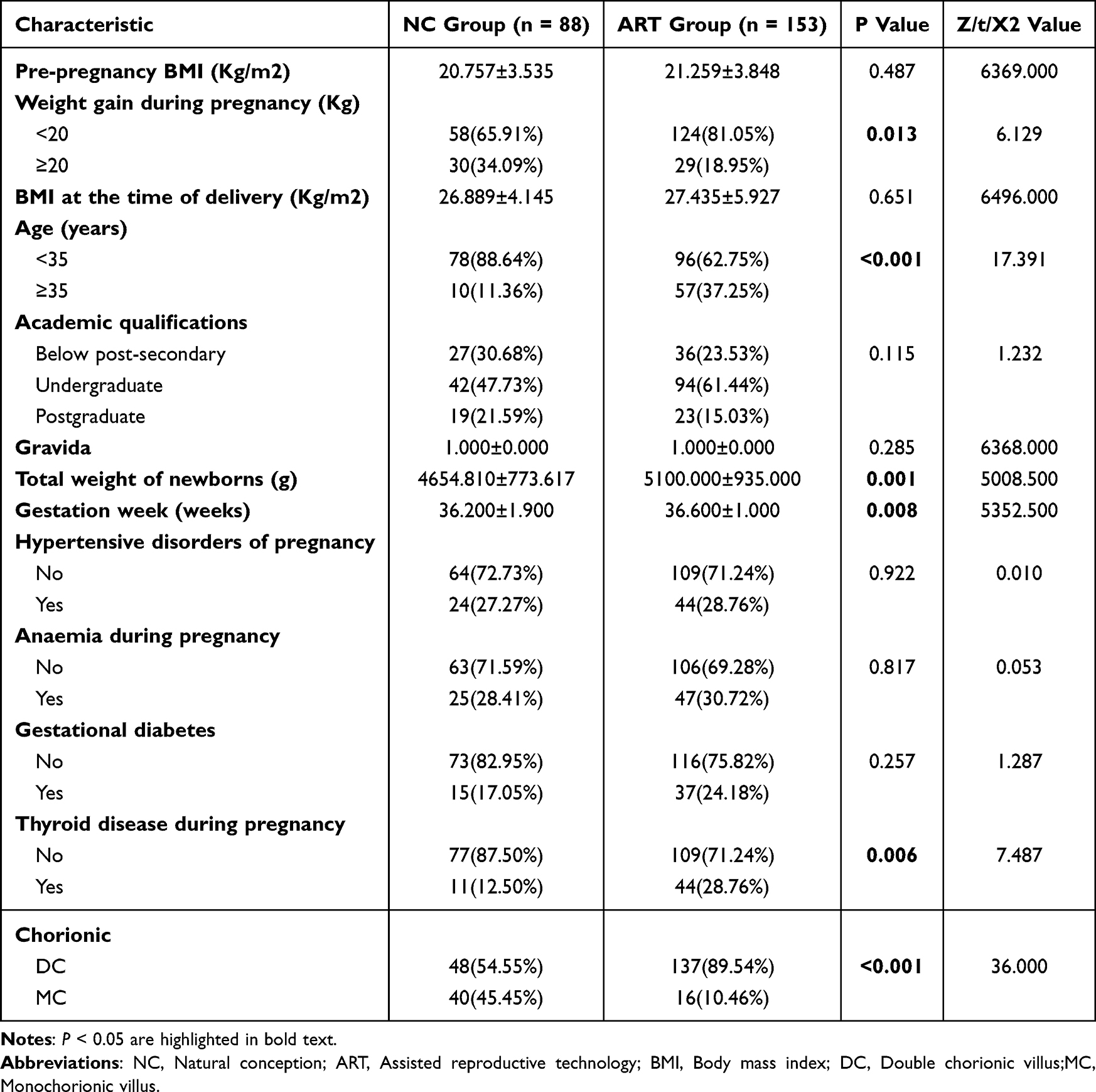 |
Table 1 Basic and Clinical Characteristics of Two Groups (NC Group vs ART Group) |
Glazer scores were used to assess pelvic floor function in the early postpartum period in both groups. Mean values of the anterior resting phase were 4.800 ± 5.230 μV in the ART group and 6.380 ± 6.300 μV in the naturally conceived group; mean values of the posterior resting phase were 5.150 ± 5.280 μV in the ART group and 6.780 ± 7.670 μV in the naturally conceived group; maximal values of the fast muscle (class II fibres) phase in the ART group were 44.070 ± 20.990 μV in the ART group and 42.320 ± 26.960 μV in the naturally conceived group; the maximum value of the slow muscle (class I fibre) phase was 31.350 ± 16.160 μV in the ART group and 28.670 ± 18.450 μV in the naturally conceived group. The total score was 74.800 ± 14.820 in the ART group and 67.570 ± 21.570 in the naturally conceived group. There was a statistically significant difference (p < 0.05) in the total Glazer score between the two groups as shown in Table 2.
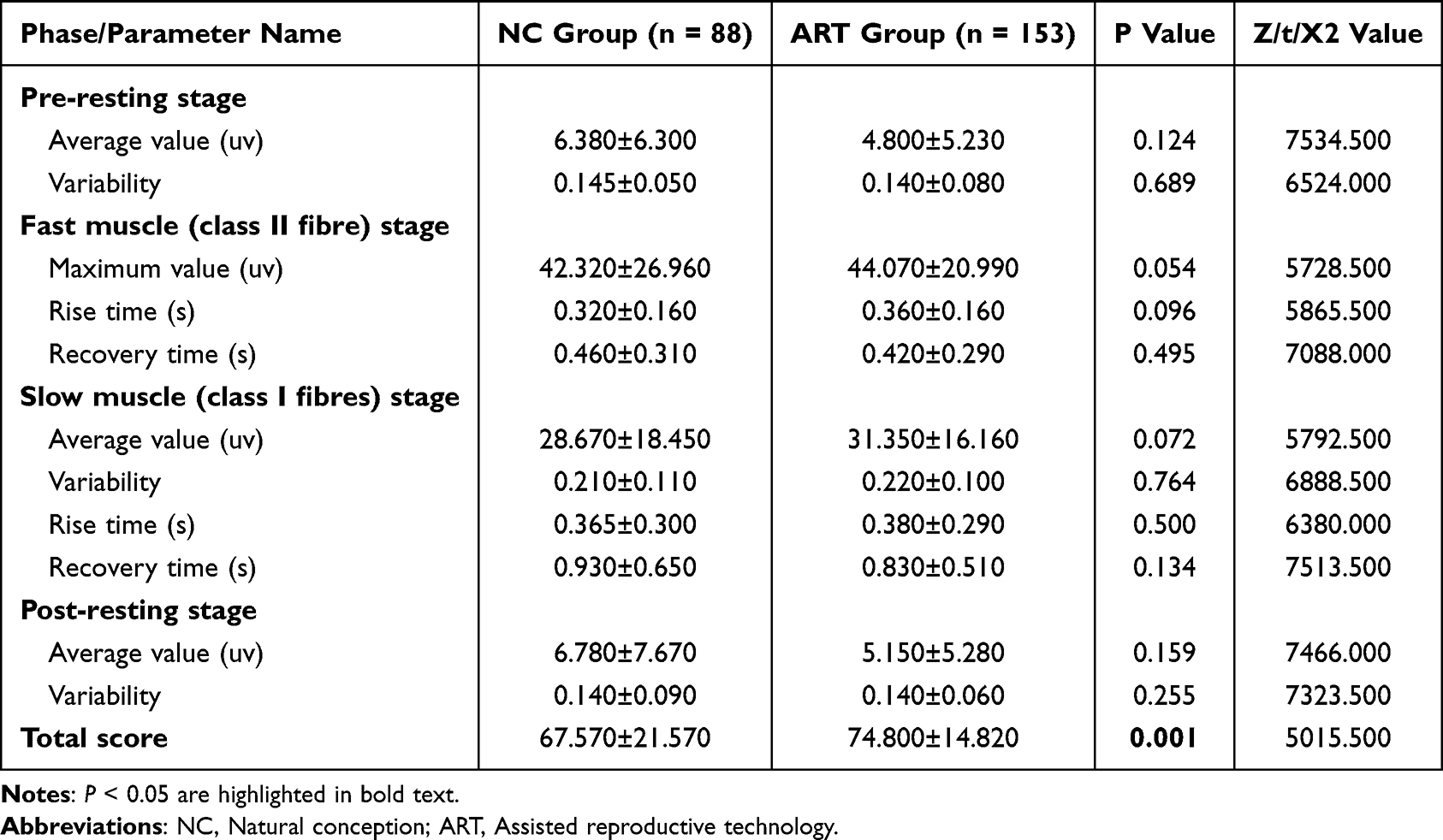 |
Table 2 Comparison of Pelvic Floor Electromyography Data (Median ± standard Deviation) Between Two Groups (NC Group vs ART Group) |
The total Galzer score ≥80 was considered essentially normal, and they were divided into two groups, and univariate logistic regression analysis revealed that the two groups were only associated with the mode of conception (OR = 0.508, 95% CI: 0.271–0.953, P < 0.05), and there were no statistical differences (P > 0.05) with maternal age, pre-pregnancy BMI, BMI at delivery, total newborn body weight, prevalence of anaemia in pregnancy, prevalence of hypertensive disorders in pregnancy, prevalence of diabetes in pregnancy, prevalence of thyroid disorders in pregnancy, frequency of pregnancy, week of delivery, chorionicity, and change in body weight during pregnancy. Prevalence of hypertensive disorders, prevalence of gestational diabetes mellitus, prevalence of thyroid disorders in pregnancy, number of pregnancies, gestational week of delivery, chorionicity, and change in body weight during pregnancy were not statistically different (P > 0.05) see Table 3. Factors with P < 0.20 for univariate analyses were included in the multivariate analysis, and multivariate logistic regression analyses showed that the two groups were still associated with the mode of conception (OR = 0.520, 95% CI: 0.270–1.000,P < 0.05) and not associated with the presence of thyroid disease during pregnancy (P > 0.05) see Table 4.
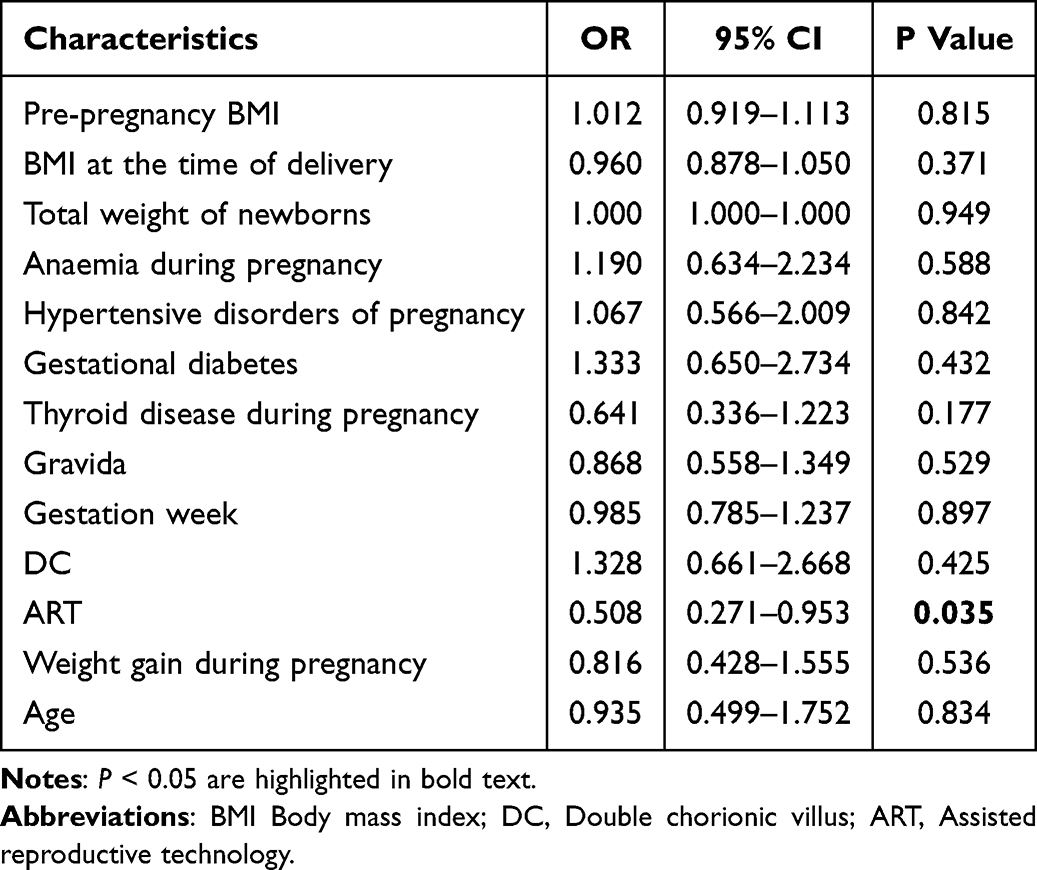 |
Table 3 One-Way Regression Analysis of Total Glazer Assessment Score ≥80 |
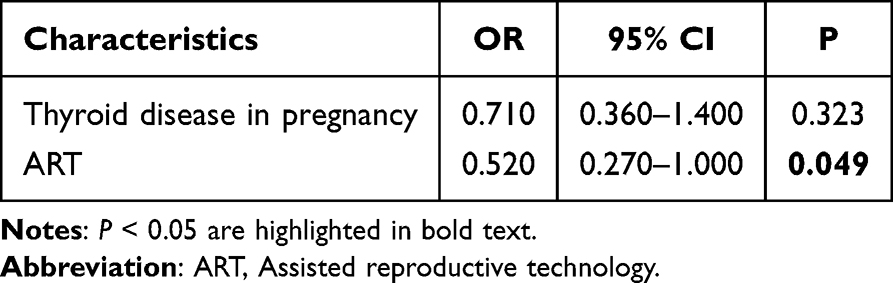 |
Table 4 Multifactorial Regression Analysis of Total Glazer Assessment Scores ≥80 |
Discussion
Pelvic floor dysfunction disorders (PFDD), encompassing pelvic organ prolapse, stress urinary incontinence, and sexual dysfunction, represent a spectrum of conditions affecting women across various life stages. The pathophysiology of PFDD is multifactorial, involving obstetric factors (eg, parity, delivery mode, neonatal birth weight), anthropometric indices (pre-pregnancy body mass index [BMI], gestational weight gain), biochemical influences (vitamin D deficiency, hypoestrogenism), and genetic predisposition.10–14 Currently recognised risk factors include age, number of births, gestation, delivery, mode of delivery, and body mass index. With the development of assisted reproductive technology, the incidence of twin pregnancies is also on the rise. The rate of multiple pregnancies in ART pregnancies reaches 30% to 50%, while the rate of multiple pregnancies in natural pregnancies is only 3.0%. Both twin pregnancies and assisted reproductive conception are high risk factors for adverse pregnancy outcomes.15 The Glazer protocol was studied to measure surface electromyography of the pelvic floor muscles to assess pelvic floor function in the early postpartum period in twin pregnancies with different modes of conception. The Glazer assessment was carried out using sEMG, which is a non-invasive technique that captures the muscle motor potentials by means of electrodes on the surface of the skin, whereby numerous sequences of action potentials generated within the motor unit during neuromuscular excitation are superimposed on the surface of the skin to form an electrical signal. The electrical signal is generated by the superimposition of numerous action potential sequences within the motor unit on the surface skin during neuromuscular excitation. Previous studies have shown that the Glazer method is more reliable than manual muscle testing in assessing the function of the pelvic floor muscles in parturient women.7,8
In the present study, the mean values of the anterior resting phase and posterior resting phase of the ART group were slightly lower than those of the naturally conceived group, and the maximal values of the fast muscle (class II fibre) phase and the maximal values of the slow muscle (class I fibre) phase of the ART group were slightly higher than those of the naturally conceived group. Although there was no statistically significant difference between the above, it still indicates that the naturally conceived group is prone to hypertonicity in the early postpartum period of twin pregnancies and is prone to spasm of the pelvic floor muscles, painful sexual intercourse, constipation, and other symptoms. In addition to this, the total score of 74.800 ± 14.820 in ART group in this study was significantly higher than that of 67.570 ± 21.570 in natural conception group. Previous studies suggested that the total score of Glazer’s score of 80 or more was basically normal, 2–3 sessions of physiotherapy were recommended for less than 60 points, 1–2 sessions of physiotherapy were recommended for 60–80 points, and 80–85 points of subjective willingness of the patient or the use of pelvic floor rehabilitator. In this study, the Glazer score of 80 points was used as the cut-off point, and the patients were divided into the group with basically normal pelvic floor function in the early postpartum period and the group with non-normal pelvic floor function. Unifactorial and multifactorial logistic regression analyses of their influencing factors suggested that they were related to the mode of conception and had no significant correlation with other factors. The multifactorial logistic regression analysis OR = 0.520, 95% CI: 0.270–1.000, P < 0.05, showed that ART was to some extent a protective factor for pelvic floor function in the early postpartum period of twin pregnancies.
For patients undergoing assisted reproduction, especially those with ovulation disorders such as PCOS, who have poor oocyte quality due to disorders in their hormonal regulation, more E2 is needed than in the non-PCOS population to promote follicular development and improve oocyte quality, thus increasing the success rate of assisted reproduction treatment in the PCOS population. Superovulation has been a routine strategy for ART, and serum oestradiol levels are higher in women undergoing ART due to ovarian stimulation.16 Higher follicular oestradiol levels improve the success rate of fertilisation after assisted reproductive therapy to some extent.17 It has been noted that maintaining a higher rate of estradiol increase during the follicular stimulation phase improves the clinical pregnancy rate.18 Decreased oestradiol levels during controlled ovarian stimulation reduce ART clinical pregnancy rates to some extent.19 During early pregnancy, steroidal sex hormone concentrations were significantly higher in the ART group compared to natural conception after controlled ovarian stimulation-embryo transfer.20 Previously there was controversy regarding the role of estrogen and selective estrogen receptor modulators on the development of POP.21,22 The present study also supports to some extent that oestrogen levels in women may affect female pelvic floor function. Estrogen receptors are widely distributed in the female uterus, bladder, vagina, urethra, pelvic floor muscles and ligamentous tissues, and the reproductive system and pelvic floor supportive tissues are target organs for estrogen. Previous studies have suggested that exogenous oestrogens can activate the immune system, limit extracellular matrix degradation and induce tissue regeneration in the genitourinary tract.23 Low estrogen levels in the body lead to loss of collagen and elastin, among others, which causes the pelvic floor muscles to become flaccid and ligaments to lose elasticity, further weakening the ligaments that support the pelvis and pelvic floor muscles, thus leading to PPFD.13,24,25 For postmenopausal women who tend to be in a hypoestrogenic state, postmenopausal treatment with hormone therapy results in thicker anorectal muscle thickness and greater pelvic floor functional strength with 3D ultrasound compared to no hormone therapy.26 To some extent, this study explores the efficacy of topical estrogen in enhancing wound healing for perineal lacerations following vaginal delivery.
In addition, Lukasz et al examined 96 non-pregnant women aged 22–27 years, height: 168.6 ± 5.1 cm, weight: 57.1 ± 11.8 kg, and the results showed that the fast muscle contraction phase: 49.76 ± 26.44 μV, and slow muscle contraction phase: 37.05 ± 25.99 μV.27 In the present study, the maximal values of the fast muscle (class II fibres) phase and the maximal values of the slow muscle (class I fibres) phase in both groups were significantly lower than those in the above study, which also suggests to some extent that twin pregnancy affects pelvic floor function in the early postpartum period in women.
Conclusion
Twin pregnancies treated with ART have higher oestrogen levels than naturally conceived pregnancies due to follicular stimulation and hormone supplementation during implantation. The present study showed that high estrogen levels in the twin pregnancy group receiving ART may have protected maternal pelvic floor function to some extent. However, the effects of high oestrogen status on maternal and neonatal outcomes are still controversial, and the variability of hormone levels in pregnant women with different follicular stimulation regimens, how different hormone levels affect pelvic floor function, and how to administer hormone supplementation, and what is a safe hormone supplementation dosage and route, need to be further explored. In subsequent clinical investigations, it is warranted to examine whether longitudinal monitoring of estrogen levels throughout gestation can elucidate their association with postpartum pelvic floor dysfunction. Such research may ultimately inform evidence-based strategies for improving postpartum recovery and pelvic health management.
Abbreviations
ART, Assisted reproductive technology; BMI, Body mass index; DC, Double chorionic villus; MC, Monochorionic villus; NC, Natural conception; PFDD, Pelvic floor dysfunction disorders; sEMG, Surface electromyography.
Date Sharing Statement
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study has obtained consent from all participants. Participants gave verbal and written consent to participate in the study, which was approved by the Ethics Committee of the International Peace Maternity and Child Health Hospital, Shanghai Jiao Tong University School of Medicine (No. GKLW-A- 2024-023-01). This study adheres to the Declaration of Helsinki.
Acknowledgments
We recognize the Pelvic Floor Rehabilitation Center of the International Peace Maternal and Child Health Hospital for its contribution to this study and the staff who supported the data collection process of this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This project is supported by the Key Research and Development Program of the Ministry of Science and Technology (2023YFC2705901).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Verbeek M, Hayward L. Pelvic floor dysfunction and its effect on quality of sexual life. Sexual Medicine Reviews. 2019;7(4):559–564. doi:10.1016/j.sxmr.2019.05.007
2. Palmieri S, De Bastiani SS, Degliuomini R, et al. Prevalence and severity of pelvic floor disorders in pregnant and postpartum women. International Journal of Gynaecology and Obstetrics. 2022;158(2):346–351. doi:10.1002/ijgo.14019
3. Caudwell-Hall J, Kamisan Atan I, Martin A, et al. Intrapartum predictors of maternal levator ani injury. Acta obstetricia et gynecologica Scandinavica. 2017;96(4):426–431. doi:10.1111/aogs.13103
4. Chi X, Yu S, Zhu K, et al. Influence of different obstetric factors on early postpartum pelvic floor function in Primiparas after vaginal delivery. International Journal of Women’s Health. 2023;15:81–90. doi:10.2147/IJWH.S390626
5. Pelvic Organ Prolapse: ACOG Practice Bulletin, Number 214. Obstet Gynecol. 2019 Nov;134(5):e126–e142. doi:10.1097/AOG.0000000000003519
6. Li J, Zhao X, Li T, et al. Pelvic organ prolapse after delivery: effects on sexual function, quality of life, and psychological health. The Journal of Sexual Medicine. 2023;20(12):1384–1390. doi:10.1093/jsxmed/qdad120
7. Kubotani JS, Araujo Júnior E, Zanetti MR, et al. Assessing the impact of twin pregnancies on the pelvic floor using 3-dimensional sonography: a pilot study. J Ultrasound Med. 2014;33(7):1179–1183. doi:10.7863/ultra.33.7.1179
8. Yang X, Zhu L, Li W, et al. Comparisons of electromyography and digital palpation measurement of pelvic floor muscle strength in postpartum women with stress urinary incontinence and asymptomatic parturients: a Cross-Sectional Study. Gynecol Obstet Invest. 2019;84(6):599–605. doi:10.1159/000501825
9. Oleksy Ł, Mika A, Stolarczyk A, et al. The reliability of pelvic floor muscle bioelectrical activity (sEMG) assessment using a multi-activity measurement protocol in young women. International Journal of Environmental Research and Public Health. 2021;18(2):765. doi:10.3390/ijerph18020765
10. Yang F, Liao H. The influence of obstetric factors on the occurrence of pelvic floor dysfunction in women in the early postpartum period. Int J Gen Med. 2022;15:3353–3361. doi:10.2147/IJGM.S355913
11. Tian Z, Wang X, Hu X, et al. Effect of surgically induced weight loss on pelvic organ prolapse: a meta-analysis. Obes Surg. 2023;33(11):3402–3410. doi:10.1007/s11695-023-06867-x
12. Romero-Franco N, Molina-Mula J, Casado A, et al. Therapeutic exercise to improve pelvic floor muscle function in a female sporting population: a systematic review and meta-analysis. Physiotherapy. 2021;113:44–52. doi:10.1016/j.physio.2021.04.006
13. Zhuo Z, Wang C, Li J, et al. The relationship between pelvic floor function and sexual function in perimenopausal women. Sex Med. 2021;9(6):100441. doi:10.1016/j.esxm.2021.100441
14. Jiang J. Relationship between abnormal pelvic floor electromyography and obstetric factors in postpartum women: a cross-sectional study. BMC Women’s Health. 2024;24(1):239. doi:10.1186/s12905-024-03045-8
15. Qin J, Liu X, Gao S, et al. Assisted reproductive technology and the risk of pregnancy-related complications and adverse pregnancy outcomes in singleton pregnancies: a meta-analysis of cohort studies. Fertil Steril. 2016;105(1):73–85.e71–76. doi:10.1016/j.fertnstert.2015.09.007
16. Zhou CL, Xu GF, Sheng JZ, et al. Diminished verbal ability among children conceived through ART with exposure to high serum estradiol in utero. J Assist Reprod Genet. 2020;37(8):1931–1938. doi:10.1007/s10815-020-01835-1
17. Sreerangaraja Urs DB, Wu WH, Kao SH, et al. Mitochondrial function in modulating human granulosa cell steroidogenesis and female fertility. Int J Mol Sci. 2020;21(10):3592. doi:10.3390/ijms21103592
18. Wei CX, Zhang L, Zhang JW, et al. Effect of the ratios of estradiol increase on the outcome of in vitro fertilization-embryo transfer with antagonist regimens: a single center retrospective cohort study. BMC Pregnancy Childbirth. 2023;23(1):134. doi:10.1186/s12884-023-05438-3
19. Cheng J, Yang S, Zhao J, et al. Estradiol (E (2)) reduction adversely affect the embryo quality and clinical outcomes of in vitro fertilization and embryo transfer (IVF-ET). J Healthc Eng. 2022;2022:2473876. doi:10.1155/2022/2473876
20. Parisi F, Fenizia C, Savasi V, et al. The pathophysiological role of estrogens in the initial stages of pregnancy: molecular mechanisms and clinical implications for pregnancy outcome from the periconceptional period to end of the first trimester. Hum Reprod Update. 2023;29(6):699–720. doi:10.1093/humupd/dmad016
21. Weintraub AY, Glinter H, Marcus-Braun N. Narrative review of the epidemiology, diagnosis and pathophysiology of pelvic organ prolapse. Int Braz J Urol. 2020;46(1):5–14. doi:10.1590/s1677-5538.ibju.2018.0581
22. Taithongchai A, Johnson EE, Thakar R, et al. Oestrogen therapy for treating pelvic organ prolapse in postmenopausal women. Cochrane Database Syst Rev. 2023;7(7):Cd014592. doi:10.1002/14651858.CD014592.pub2
23. Tyagi T, Alarab M, Shynlova O, et al. Local oestrogen therapy modulates extracellular matrix and immune response in the vaginal tissue of post-menopausal women with severe pelvic organ prolapse. J Cell Mol Med. 2019;23(4):2907–2919. doi:10.1111/jcmm.14199
24. Harada BS, De Bortolli TT, Marini G, et al. Diastasis recti abdominis and pelvic floor dysfunction in peri- and postmenopausal women: a cross-sectional study. Physiother Theory Pract. 2022;38(10):1538–1544. doi:10.1080/09593985.2020.1849476
25. Johnston SL. Pelvic floor dysfunction in midlife women. Climacteric. 2019;22(3):270–276. doi:10.1080/13697137.2019.1568402
26. Marques Gomes Delmanto LR, Omodei MS, Nahas EAP, et al. Three-dimensional ultrasound evaluation of the pelvic floor in postmenopausal women using hormone therapy. Maturitas. 2021;143:65–71. doi:10.1016/j.maturitas.2020.08.009
27. Oleksy Ł, Wojciechowska M, Stolarczyk A, et al. Normative values for Glazer Protocol in the evaluation of pelvic floor muscle bioelectrical activity. Medicine. 2020;99(5):e19060. doi:10.1097/MD.0000000000019060
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.