Back to Journals » Clinical Ophthalmology » Volume 20
The Science of Pseudoaccommodation and Its Therapeutic Potential
Authors Poliński J ![]() , Walasik-Szemplińska D, Skrzypecki J
, Walasik-Szemplińska D, Skrzypecki J ![]()
Received 11 July 2025
Accepted for publication 5 November 2025
Published 8 January 2026 Volume 2026:20 553059
DOI https://doi.org/10.2147/OPTH.S553059
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr John Miller
Jakub Poliński,1,2 Dorota Walasik-Szemplińska,2 Janusz Skrzypecki2– 4
1Department of Ophthalmology, National Medical Institute of the Ministry of the Interior and Administration, Warsaw, Poland; 2Sensor Cliniq, Warsaw, Poland; 3Mediq Cliniq, Legionowo, Poland; 4Department of Experimental Physiology and Pathophysiology, Medical University of Warsaw, Warsaw, Poland
Correspondence: Janusz Skrzypecki, Department of Experimental Physiology and Pathophysiology, Medical University of Warsaw, Banacha 1B, Warsaw, 02-097, Poland, Tel +48 22 116 6195, Fax +48 22 57 20 734, Email [email protected]
Abstract: Pseudoaccommodation is a critical yet often underappreciated factor influencing visual outcomes after cataract surgery. Despite the irreversible loss of true accommodation due to presbyopia or intraocular lens (IOL) implantation, many patients retain meaningful near and intermediate vision—a phenomenon driven by optical and anatomical contributors such as pupil size, astigmatism, and higher-order aberrations. This functional benefit, known as pseudoaccommodation, can be further enhanced pharmacologically through miotic agents like pilocarpine or surgically via multifocal and extended depth-of-field (EDOF) IOLs. However, these strategies may come with trade-offs, including dysphotopsia and reduced contrast sensitivity. Understanding the mechanisms and limitations of pseudoaccommodation is essential for optimizing IOL selection, managing patient expectations, and improving satisfaction. This comprehensive review synthesizes the current evidence on the anatomical, optical, pharmacologic, and technological factors that contribute to pseudoaccommodation, offering practical guidance for counseling both phakic and pseudophakic presbyopic patients.
Keywords: presbyopia, optical system, pseudoaccommodation
Introduction
Presbyopia remains one of the most prevalent causes of near-vision impairment worldwide, affecting virtually all individuals over the age of 40. As the crystalline lens loses its elasticity and the ciliary muscle–zonular complex becomes less effective, true accommodation diminishes, leading to dependence on reading glasses or other corrective strategies. However, many presbyopic and pseudophakic patients still demonstrate a degree of functional near vision that exceeds what would be expected from complete loss of accommodation. This phenomenon—termed pseudoaccommodation—is driven by static optical and anatomical factors such as pupil size, astigmatism, and higher-order aberrations, as well as by newer intraocular lens (IOL) and corneal technologies that extend depth-of-field.
Because pseudoaccommodation blurs the traditional distinction between “accommodating” and “non-accommodating” eyes, it has become a central concept in modern presbyopia management. Multifocal and extended-depth-of-field (EDOF) IOLs, miotic eye drops, and advanced corneal laser procedures all exploit aspects of pseudoaccommodation to reduce spectacle dependence, but the mechanisms, outcomes, and patient suitability vary widely (Figure 1). Understanding these factors is crucial for clinicians selecting the most appropriate intervention and for researchers developing next-generation solutions.
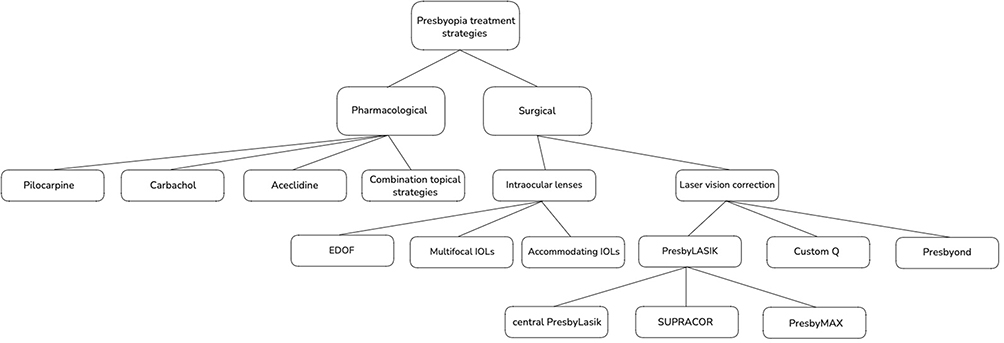 |
Figure 1 Overview of presbyopia treatment strategies. |
The purpose of this review is to critically examine the evidence on factors influencing pseudoaccommodation in both phakic and pseudophakic presbyopes—including astigmatism, pupil diameter, higher-order aberrations, pharmacological modulation, and modern IOL and corneal designs—and to place these findings within the context of a new functional classification of intraocular lenses based on defocus curves.
What Was Known
Pseudoaccommodation explains residual near vision in presbyopic and pseudophakic eyes; it’s influenced by astigmatism, pupil size, and higher-order aberrations.
Multifocal and EDOF IOLs, as well as miotic drops, can enhance near vision but often at the cost of reduced contrast sensitivity or dysphotopsias.
What This Paper Adds
Presents a critical appraisal of current strategies to enhance pseudoaccommodation (IOL design, pharmacological and corneal approaches) in light of emerging evidence.
Frames these findings within the new functional classification of intraocular lenses based on defocus curves, offering a structured perspective for future lens selection and innovation.
Search Strategy and Scope
To identify relevant studies, we searched PubMed/MEDLINE, Embase, and the Cochrane Library from January 1990 through June 2024 using combinations of the terms “pseudoaccommodation,” “presbyopia,” “intraocular lenses,” “pupil size,” “higher-order aberrations,” and “depth of field/focus.” We included English-language original articles, clinical trials, and systematic reviews addressing factors influencing pseudoaccommodation in either phakic or pseudophakic eyes. Reference lists of key papers were hand-searched to identify additional studies. This approach was designed to capture both foundational and the most recent evidence, but it is not intended as a fully systematic review.
(Pseudo)accommodation vs Depth-of-Field vs Depth-of Focus
Accommodation (true accommodation) refers to the dynamic change in the eye’s optical power—driven by ciliary muscle contraction—that allows clear vision at different distances.1 Pseudoaccommodation describes static optical factors such as pupil size, astigmatism, and higher-order aberrations that enhance near vision without active ciliary muscle involvement.2 Pseudophakic accommodation denotes a dynamic refractive change produced by anterior movement of the intraocular lens–capsular bag complex in response to ciliary muscle contraction.3 The functional near vision achieved with multifocal intraocular lenses or multifocal corneal procedures is therefore considered pseudoaccommodation. Depth of field (DOFi) refers to the range in object space over which images appear acceptably sharp, whereas depth of focus (DOFo) denotes the tolerance to defocus at the retinal image plane.4 Although related, these concepts are distinct and are often used interchangeably in the literature, contributing to ongoing confusion.
Accommodation Mechanism
Accommodation is the process by which the eye’s optical power adjusts to facilitate near vision. The most widely accepted theory of accommodation, proposed by Helmholtz, describes this process as involving contraction of the ciliary muscle, relaxation of the zonular fibers, and an increase in the curvature of the crystalline lens.1 According to this theory, accommodation is lost with age due to a decline in the elasticity of the crystalline lens.5 However, as the range of near vision can vary among presbyopic patients, both phakic and pseudophakic, the concept of pseudoaccommodation was introduced.6 This term encompasses not only the optical and anatomical features of the eye that increase the depth of field but also advancements in pseudoaccommodative intraocular lenses (IOLs).
Pseudoaccommodation
Diffractive or refractive multifocal IOLs and extended-depth-of-field (EDOF) IOLs, are gaining popularity among ophthalmologists and patients due to their ability to reduce dependence on glasses and significantly improve quality of life.7,8 However, these lenses are not without drawbacks. Patients often report reduced contrast sensitivity under low light conditions (mesopic contrast) and positive dysphotopsia.9 Additionally, not all patients are suitable candidates for pseudo-accommodative IOLs.
Corneal or macular diseases—such as Fuchs’ dystrophy, age-related macular degeneration (AMD), or epiretinal membrane—can impair postoperative visual outcomes and are generally considered contraindications for pseudo-accommodative IOL implantation.10 Furthermore, patients with high visual quality expectations or occupations requiring high-contrast vision are often deemed unsuitable for multifocal or EDOF IOLs.11
While monofocal IOLs do not enhance accommodation by definition, certain optical and anatomical characteristics, such as astigmatism, pupil size, and corneal aberrations, can improve pseudoaccommodation. Identifying these features during the preoperative assessment is essential.
This review examines the anatomical and optical factors that influence the range of near vision in both phakic and pseudophakic patients.
Measurement of Pseudoaccommodation
Pseudoaccommodation has been investigated in numerous studies using both objective and subjective methods. In subjective methods, it is influenced by factors such as target type, target size, and testing conditions.12,13 In phakic eyes, the measurement of pseudoaccommodation requires pharmacologic blockage of the ciliary body. A commonly used subjective method for measuring pseudoaccommodation is the defocus curve. In this test, additional lenses are sequentially superimposed on the distance correction, ranging from +1.50 D to −2.50 D in incremental steps.14 For each lens addition, distance visual acuity is assessed. Although the criteria for assessing pseudoaccommodation vary among studies, the most commonly used benchmark in pseudophakic eyes is the defocus level corresponding to a visual acuity of 0.20 logMAR.15
Objective measurements of pseudoaccommodation can be obtained using aberrometers.16 Wavefront analysis provides optical quality metrics, and the through-focus visual Strehl optical transfer function (VSOTF) has been proposed as a method for evaluating pseudoaccommodation in both phakic and pseudophakic eyes.17,18 This method determines the dioptric range at which the image quality parameter declines to a cut-off level, with specific cut-off values varying across studies.
In real-life scenarios, the assessment of pseudoaccommodation is often performed using distance, intermediate, and near vision testing, providing a direct measure of functional improvement.19 In many studies, this assessment is further complemented by the incorporation of the defocus curve. However, the effectiveness of visual acuity measurements depends on standardized testing conditions.20,21 The use of a wide variety of vision charts at different testing distances leads to inconsistencies and makes the results difficult to compare.22,23
Role of Astigmatism in Pseudoaccommodation
Although numerous studies have investigated the role of astigmatism in pseudoaccommodation, a consensus has not yet been reached (Table 1). A theoretical study by Sawusch and Guyton demonstrated that a refraction of −1.0/+0.75 (sphere/cylinder) provides the best overall visual acuity for both near and distance vision.24 Interestingly, this combination of refractive errors offered better near and distance visual acuity than 0.5 diopter of myopia.
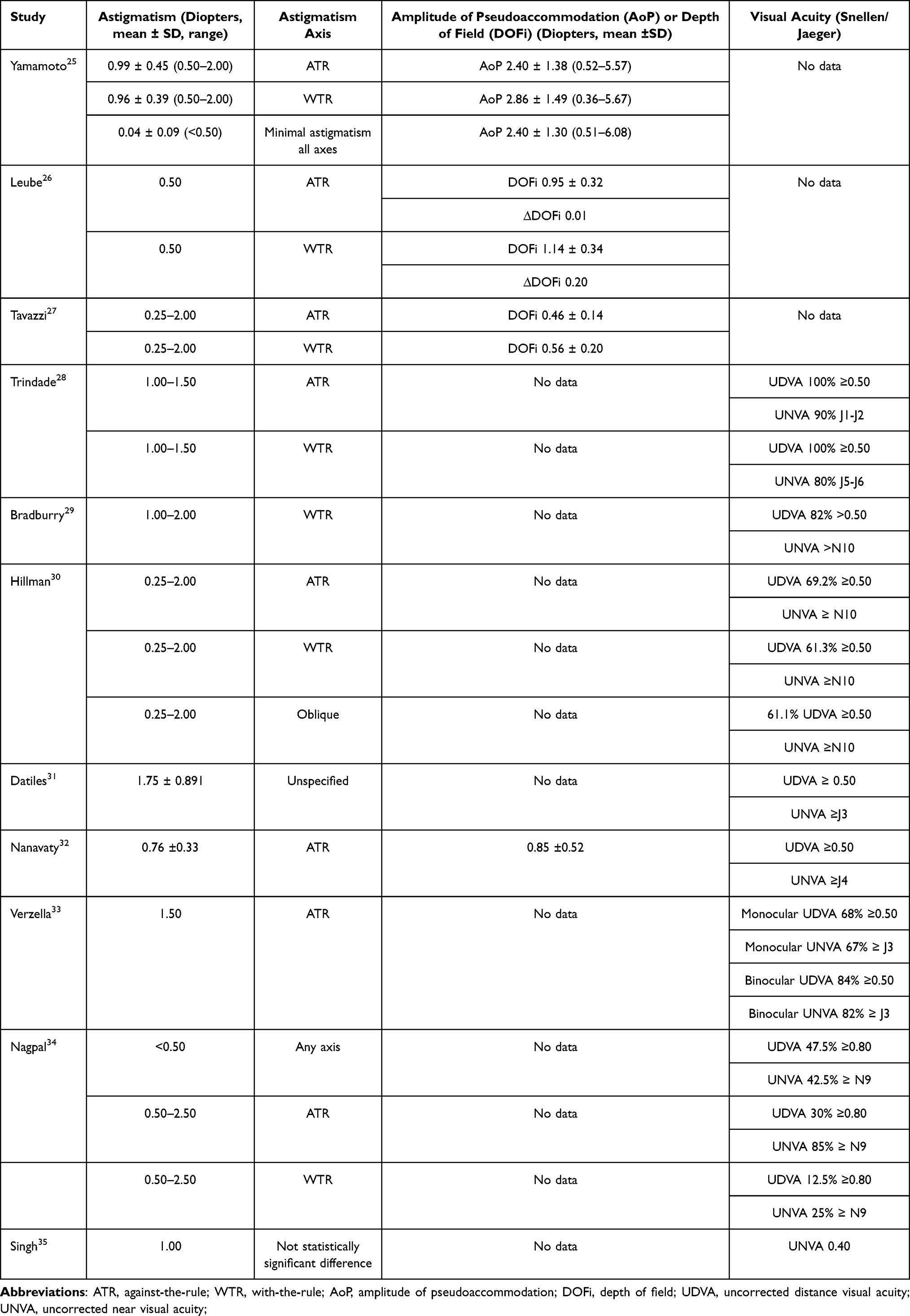 |
Table 1 Summary of the Effects of Astigmatism on Pseudoaccommodation, Depth of Field and Visual Acuity |
In contrast, Bradbury et al found that patients with myopic astigmatism and no residual spherical error are more likely to achieve functional near and distance vision.29 Other clinical studies have highlighted that a specific type of astigmatism—against-the-rule (ATR) astigmatism enhances depth of field. Verzella, Calossi, and Nanavaty et al reported that ATR astigmatism of less than 1.5 D allows independence from glasses for both near and distance vision.32,33
Additionally, a study on phakic emmetropes by Tsukamoto et al found that accommodation induces significant ATR astigmatism.36 On the other hand, Yamamoto et al observed that while there were no significant differences in pseudoaccommodation between pseudophakic patients with ATR and with-the-rule (WTR) astigmatism, patients with ATR astigmatism exhibited a statistically significant correlation between pupil diameter or higher-order aberrations (HOA) and pseudoaccommodation.25
Contrarily, a randomized controlled trial by Savage et al involving phakic presbyopes did not show any advantage of ATR astigmatism for near vision.37 Similarly, Kamiya et al found no significant effect of astigmatism on pseudoaccommodation.38
Role of Pupil Diameter
Increasing theoretical and clinical evidence indicates that pupil diameter is critical in visual quality. Interestingly, both excessively large and excessively small pupils can degrade the retinal image.39–41 Larger pupils increase spherical aberration, while smaller pupils cause light diffraction at the pupil’s edge.
The near reflex induces miosis, leading to the hypothesis that a narrower pupil enhances depth of field and supports near vision. This hypothesis has been validated in clinical studies, as summarized in Table 2. However, due to the confounding effects of spherical aberration and the Stiles-Crawford effect, a precise quantitative relationship between pupil diameter, pseudoaccommodation, and visual quality remains elusive.42 Tucker and Charman studied external apertures in cycloplegic patients and found that depth of field ranged from 1D with an 8 mm pupil to 3D with a 1 mm pupil.43 Similarly, Charman and Whitefoot observed that depth of field was highest for a 1 mm pupil, decreased up to 5 mm, and then plateaued.44
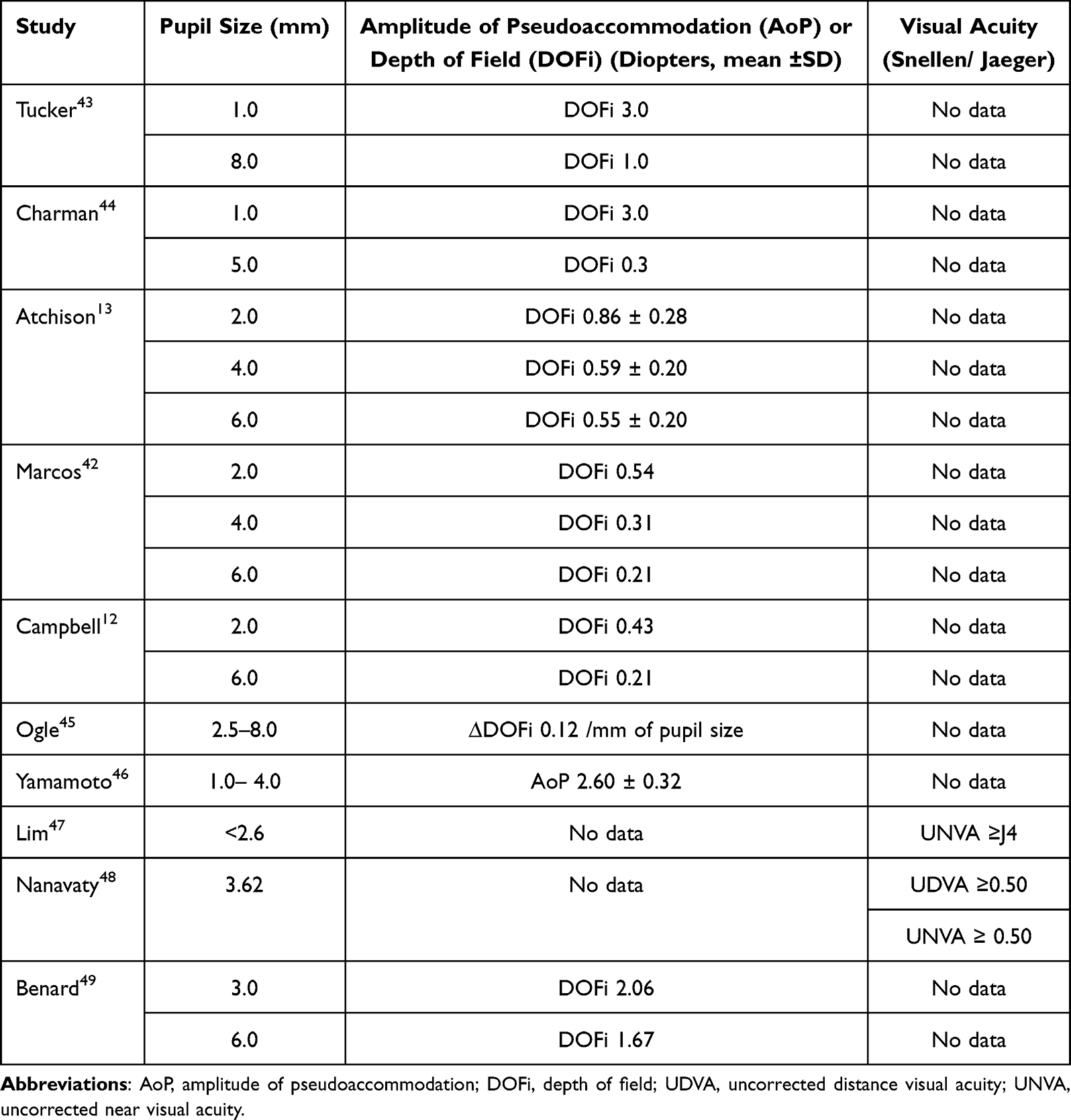 |
Table 2 Summary of the Effect of Pupil Size on Pseudoaccommodation, Depth of Field and Visual Acuity |
A computational modelling study by Xu et al highlighted the trade-off between the improved depth of field associated with smaller pupils and the image quality degradation caused by diffraction.50 Diffraction effects were most significant for pupil sizes under 2 mm, while maximum image quality was achieved with pupil diameters between 2.5 and 4.5 mm.
Additionally, in pseudophakic eyes, depth of field for a given pupil diameter was found to inversely correlate with visual acuity better than Snellen 20/20.51
Eye Drops
The role of pupillary diameter in increasing depth of field is well established, making pharmacologic constriction of the pupil a promising approach to managing presbyopia. Pilocarpine, a muscarinic receptor agonist, addresses presbyopia through a dual mechanism of action: it stimulates muscarinic receptors in the iris sphincter and ciliary body muscles, inducing miosis to enhance depth of field and promoting ciliary muscle contraction to improve accommodation.52 However, chronic use of pilocarpine can lead to side effects that may limit its adoption.53 To mitigate these adverse effects, various formulations have been developed. Non-steroidal anti-inflammatory agents, steroids, and brimonidine have been added to pilocarpine solutions to reduce inflammatory responses or ciliary body contraction.54,55 Additionally, sympathomimetics such as naphazoline have been included to decrease conjunctival vasodilation.56
Proprietary solutions with reduced side effects have also gained Food and Drug Administration (FDA) approval. Notably, the FDA has recently approved an optimized formulation of pilocarpine eye drops for correcting presbyopia in humans.57 Vuity (AGN-190584, Allergan, USA) eye drops, containing 1.25% pilocarpine hydrochloride, demonstrated efficacy in the Gemini 1 and Gemini 2 clinical trials.58 These trials showed that 31% of participants aged 40 to 55 achieved an improvement of three or more lines in near visual acuity without losing more than one line of corrected distance visual acuity. Importantly, near vision in GEMINI was assessed under strictly defined mesopic, high-contrast conditions (≈3.2–3.5 cd/m2), whereas distance and intermediate visual acuities were tested under standard photopic lighting. Vuity was found to have an acceptable safety and tolerability profile, with the most commonly reported adverse effects being headaches, conjunctival hyperaemia, and difficulty transitioning focus between near and distant objects.58
CSF-1 (Qlosi, Orasis Pharmaceuticals, USA) eye drops, containing 0.4% pilocarpine hydrochloride, were also approved by the Food and Drug Administration (FDA) in 2023.59 Phase 3 NEAR-1 and NEAR-2 clinical trials showed that 40.1% of participants in the CSF-1 group achieved an improvement of three or more lines in near visual acuity.60 In contrast to GEMINI, the NEAR program reported near vision testing more broadly under mesopic (low-light), high-contrast conditions without specifying an exact luminance level, while distance vision was again assessed under photopic lighting. CSF-1 demonstrated an acceptable safety profile, with most adverse events reported as mild and transient.60
Carbachol, a non-selective acetylcholine receptor agonist, has been investigated in combination with brimonidine. Studies by Abdelkader et al found this combination to be effective.61,62 Brimochol PF (Visus Therapeutics, USA), containing 2.25% carbachol and 0.1% brimonidine, completed its first phase 3 clinical trial, BRIO-I.63 The primary endpoint—achieving at least a three-line improvement in near visual acuity—was met by 49.4% of participants. The most common adverse effects were eye irritation and headache.63
Aceclidine is a selective muscarinic agonist that produces pupil miosis and improves depth of focus with minimal ciliary stimulation. In the Phase 3 CLARITY 1 and 2 trials, the lead formulation LNZ100 (1.75% aceclidine) achieved the primary endpoint, with 71% of participants demonstrating a ≥3-line improvement in near visual acuity at 3 hours post-dose, and sustained effect up to 10 hours.64 LNZ101 (aceclidine with brimonidine) showed similar efficacy but no superiority. Based on these results, LNZ100 was selected as the lead candidate and subsequently received FDA approval in 2025 for the treatment of presbyopia.65
Higher-Order Aberrations
Various studies have explored the role of high-order aberrations (HOAs), particularly spherical aberration, in pseudoaccommodation, as summarized in Table 3. The findings of some studies appear contradictory, which can be attributed to the frequent mixing of two distinct representations of spherical aberration: longitudinal spherical aberration and the Zernike representation of spherical aberration (Z(4,0)).66
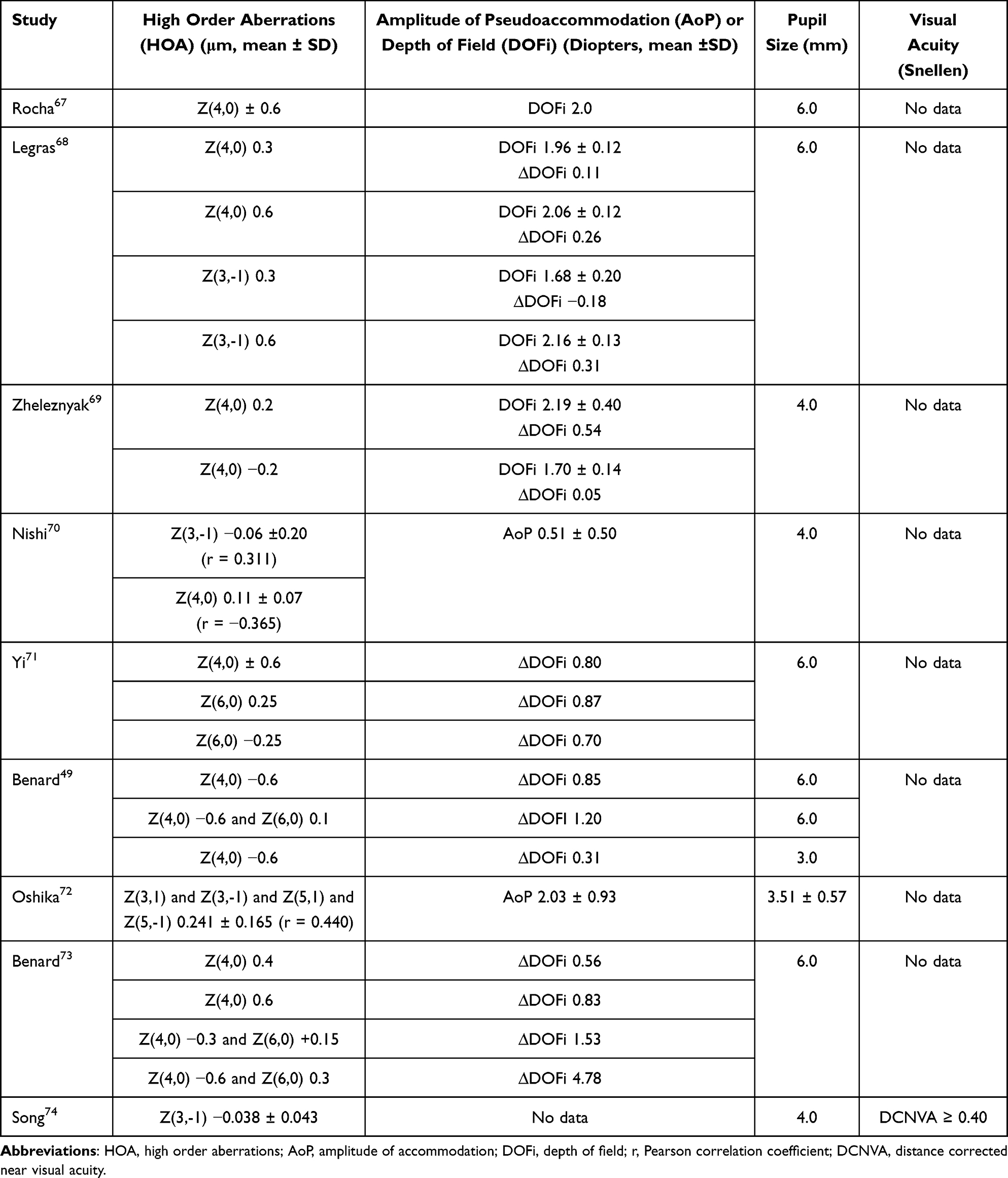 |
Table 3 Summary of the Effects of High Order Aberrations on Pseudoaccommodation, Depth of Field and Visual Acuity |
For longitudinal spherical aberration, an optical system with positive spherical aberration focuses peripheral rays in front of paraxial rays, while negative spherical aberration results in the opposite behavior. In contrast, the Zernike representation shows that positive spherical aberration causes a hyperopic defocus of paraxial rays, with peripheral rays focusing in front of them. Therefore, the interpretation of research findings must align with the specific representation of spherical aberration used in the study.
Given these considerations, it is unsurprising that Rocha et al demonstrated that inducing positive or negative spherical aberration using adaptive optics can enhance the depth of field and pseudoaccommodation range by up to 2 diopters.67 Similarly, recent research on a novel monofocal IOL designed to induce positive Zernike spherical aberration found that negative Zernike spherical aberration is not the only way to increase the depth of field.75
However, to optimize pseudoaccommodation in an optical system using an IOL that induces positive Zernike spherical aberration, the refractive target for IOL implantation should be slightly myopic.75
Furthermore, Nanavaty et al analyzed the depth of field in patients after implantation of aspheric and spherical IOLs and found that reducing total spherical aberration might decrease the depth of field.76
Notably, Nishi et al reported that vertical coma, rather than spherical aberration, correlates more strongly with pseudoaccommodation.70 Despite this, current surgical methods for presbyopia correction often rely on the induction of spherical aberration. Aspheric ablation profiles are commonly employed in laser refractive surgery for presbyopia treatment. Additionally, extended depth of field IOLs—such as the MiniWell (Sifi, Italy), Lucidis (Swiss Advanced Vision, Switzerland) and LuxSmart (Bausch and Lomb) utilize the induction of spherical aberration within the optical system of the eye.77
Finally, Hickenbotham et al observed that while spherical aberration can increase the depth of field, it also reduces distance-corrected visual acuity.78 It is important to note that spherical aberration levels exceeding 0.56μm can significantly degrade image quality and should be carefully managed during surgical interventions.79
Limitations of Studies on Factors Affecting Pseudoaccommodation
Research exploring the impact of pupil size, higher-order aberrations, and astigmatism on pseudoaccommodation faces several important limitations. First, most studies are cross-sectional or small in sample size, limiting the ability to infer causality or generalize results. Second, methodological heterogeneity—including non-standardized lighting conditions, inconsistent visual acuity cut-offs, and variable definitions of pseudoaccommodation—reduces comparability across studies. Third, many investigations rely on subjective testing methods, such as defocus curves or near vision charts, which are influenced by target type, testing distance, and patient cooperation. Together, these limitations highlight the need for standardized, prospective, and adequately powered studies to clarify the role of optical and anatomical factors in pseudoaccommodation.
Intraocular Lenses – Quest for Restoring of Accommodation
It has been suggested that pseudoaccommodation following the implantation of a monofocal IOL may be influenced by the forward movement of the IOL during accommodative effort. Several studies have investigated changes in IOL position during near fixation or after drug-induced ciliary body contraction. For example, Kriechbaum et al found that pilocarpine induces a more pronounced forward movement of the lens, potentially overestimating pseudophakic accommodation compared to measurements taken during near fixation.80 Similarly, Marchini et al, using high-frequency ultrasound, observed significant anterior movement of the IOL in response to accommodative stimuli.81 Findl et al, utilizing partial coherence interferometry (PCI) biometry, reported that forward movement of the IOL could result in an accommodative response of up to 1 diopter (D).82
Other studies have explored how the design of monofocal IOL affects the extent of anterior movement. Vamosi et al compared the single-piece Akreos Disc IOL with the three-piece Acrysof MA60MB during near vision fixation, finding that the three-piece lens demonstrated greater accommodative movement.83 This observation was attributed to the 10-degree optic-haptic angulation in the three-piece IOL. Cleary et al compared the bag-in-the-lens IOL with a standard monofocal IOL and found no significant differences in forward movement during near fixation or pilocarpine stimulation.84
These findings have motivated the development of shape-changing IOLs designed to provide functional near visual acuity for pseudophakic patients. Examples include the 1CU (HumanOptics AG, Erlangen, Germany), Tetraflex KH3500 (Lenstec, FL, USA), Crystalens AT-45 (Bausch and Lomb, NY, USA), and Crystalens HD (Bausch and Lomb, NY, USA).85 While patients initially demonstrated accommodation of up to 2 D following implantation of these lenses, this effect diminished over time, likely due to fibrosis of the capsular bag.86 Additionally, some studies reported high rates of posterior capsule opacification with these lenses.87
Intraocular Lenses – Current Perspective
Ribeiro et al has proposed recently a novel functional classification of IOLs based primarily on their defocus curves which is a measure of their range of pseudoaccommodation.88 The intraocular lenses were divided into the partial range of field IOLs and the full range of field IOLs. The primary difference lies in their defocus curve performance at the level of visual acuity of 0.2 logMAR. The former have less than 2.3 D of defocus and the latter at least 2.3D of defocus. Furthermore, the partial range of field IOLs are divided into narrow <1.2D, enhance ≥1.2 and <1.58, and extend ≥1.58 and <2.3). Standardized functional categories—such as those based on defocus curves—compel evaluation of IOLs according to specific, objective criteria. This, in turn, allows meaningful comparison between lenses from different manufacturers, facilitates evidence-based selection of IOLs for individual patients, and improves preoperative counseling by setting realistic expectations regarding near, intermediate, and distance vision outcomes.
Partial Range-of-Field IOLs
Monofocal IOLs
Monofocal lenses differ in their optical properties, particularly in the spherical aberration they introduce to the optical system. In a virgin eye, positive spherical aberration from the cornea is neutralized by negative aberration from the lens.89 After cataract removal and implantation of a spherical monofocal IOL, the optical system is predominantly influenced by the positive spherical aberration of the cornea.90 Evidence suggests that implanting a monofocal IOL with negative spherical aberration to counteract corneal aberrations can improve night vision. For example, Yagci et al demonstrated that aspheric IOLs enhance photopic visual quality, while Raina et al showed that they improve contrast sensitivity in pediatric eyes.91,92 A meta-analysis comparing aspheric and spherical IOLs concluded that spherical lenses may reduce overall visual quality.93
However, the impact of these differences on pseudoaccommodation remains unclear. It has been proposed that aspheric IOLs might decrease, increase, or have no effect on pseudoaccommodation compared to spherical IOLs. Kozhaya et al recently utilized a wavefront simulator and found that positive spherical aberration, unlike negative spherical aberration, do not enhance pseudoaccommodation.94 This finding contrasts with some in vivo studies, which reported improved near vision after spherical IOL implantation.95 However, these studies often fail to control for pupil size during near vision assessment and pupil size might have a greater influence on near vision than spherical aberration.96 This is supported by Nanavaty et al who compared the aspheric Acri.Smart 36A IOL with the spherically neutral Akreos MI60 IOL and observed that the spherical IOL produced a smaller depth of field.97
Enhanced Monofocal IOLs
Recent advancements in the field include enhanced monofocal IOLs which are based either on the principle of additional spherical aberration (RayONE EMV, Rayner, UK), adjusted curvature to allow for increased refraction in the center of the lens (Tecnis Eyhance, Johnson and Johnson, USA; Vivinex Impress, Hoya, Japan) or polynomial surface design (Isopure, BVI Medical, USA).98 These lenses are designed to improve intermediate vision without impairment of quality of distance vision. Their defocus curve performance at the level of visual acuity of 0.2 logMAR is ≥1.2 and <1.58. Table 4 presents summary of visual outcomes of enhanced monofocal IOLs.
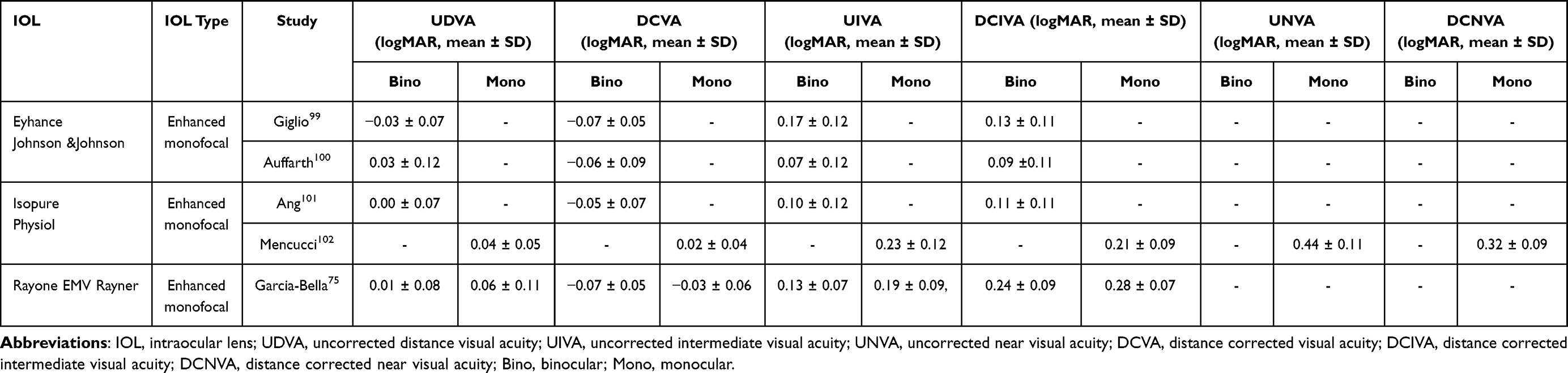 |
Table 4 Summary of Visual Acuity Outcomes with Enhanced Monofocal Intraocular Lenses |
Extended Depth-of-Field Lenses
Initially, EDOF lenses were referred to as extended depth of focus lenses. However, it is crucial to note that these lenses extend the depth of field, as the term “field” in optics refers to the object plane. Compared to monofocal IOL, EDOF lenses have a narrower depth of focus. This limitation occurs because EDOF lenses do not concentrate all light energy into a single focal point, making them more susceptible to small position-related dysphotopsias and reductions in visual quality.4
The American Academy of Ophthalmology defines EDOF lenses as those providing a depth of field at least 0.5 diopter greater than that of a monofocal lens at a visual acuity of 0.2 logMAR. Furthermore, at least 50% of eyes implanted with an EDOF lens must achieve a distance-corrected intermediate visual acuity (DCIVA) of 0.2 logMAR or better. Additionally, the mean DCIVA at 67 cm must exceed that achieved with a monofocal lens control. Recently, Ribeiro et al introduced a classification system for IOLs, redefining EDOF lenses as extended range of field (EROF) lenses. According to this classification, such lenses must deliver a visual acuity of at least 0.2 logMAR with a defocus range between ≥1.58 D and <2.3 D.88
Various optical principles are utilized in designing EDOF lenses. Common approaches include diffraction, refraction, the pinhole effect, the induction of spherical aberration, or wavefront modulation to extend the depth of field. Examples of diffractive EDOF lenses include the Symphony (Johnson & Johnson, USA) and AT LARA (Zeiss, Germany). Lenses utilizing spherical aberration include Lucidis and Mini-Well, while the Vivity lens employs wavefront modulation.103 The latest developments also feature purely refractive EDOF designs, such as the Puresee (Tecnis, USA).104
In terms of depth of field and visual quality, EDOF lenses occupy a middle ground between monofocal and multifocal IOLs (Table 5). Compared to monofocal IOLs, EDOF lenses reduce the need for glasses but offer inferior near vision performance compared to multifocal IOLs.7 Although studies indicate that EDOF lenses provide lower overall visual quality than monofocal lenses, they are associated with fewer undesirable visual phenomena, such as glare and halos, compared to multifocal IOLs.105,106
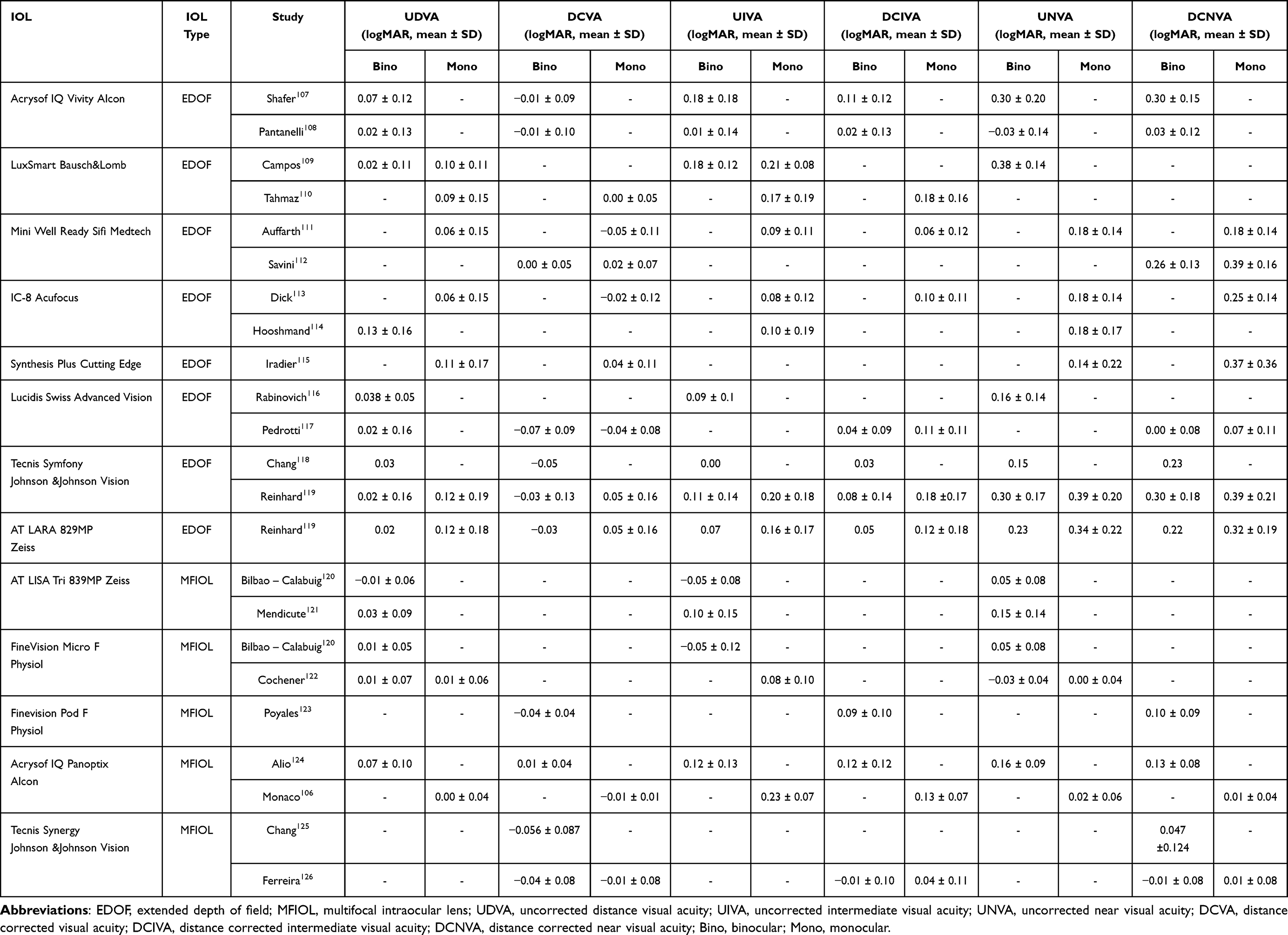 |
Table 5 Summary of Visual Acuity Outcomes with Extended Depth-of-Field and Multifocal IOLs |
Full Range of Field IOLs
Ribeiro et al classify an IOL as having a full range of field if it achieves a defocus curve of 2.3D or greater for visual acuity of 0.2 logMAR.88 This category includes trifocal and bifocal lenses with both low and high add powers.
Bifocal and multifocal IOLs were developed to provide pseudophakic patients with independence from glasses for near vision, as well as for near and intermediate vision, respectively. A recent study comparing the trifocal PanOptix (Alcon, USA) with the monofocal IOL SA60AT (Alcon, USA) found that 80% of patients in the multifocal group never required reading glasses, compared to only 8% in the monofocal group.127 Table 5 provides summary of visual acuity outcomes for multifocal IOLs.
The most popular technical solutions in bifocal and multifocal lenses include diffractive echelette designs, which split light into multiple foci. An alternative approach is the introduction of symmetric or asymmetric refractive surfaces with different focal lengths.8 Examples of diffractive lenses include the PanOptix (Alcon, USA), AT LISA (Zeiss, Germany), and FineVision (Physiol, Belgium), while refractive designs are represented by lenses such as the Lentis MPlus (Teleon Surgical).128
While multifocal and bifocal IOLs provide functional near vision, studies indicate that their implantation is associated with positive dysphotopsias, such as glare and halos.129,130 These effects make such lenses less suitable for patients who require high-quality vision, such as professional drivers. Although 30–60% of patients report dysphotopsias after multifocal IOL implantation these symptoms typically diminish over time, with only about 5% of patients finding them bothersome six months post-surgery.127
Principles of Laser Vision Correction
Various laser vision correction techniques have been developed to address pseudoaccommodation and presbyopia. Similar to concepts in IOL design, dedicated ablation profiles have been created to enhance depth of field. These laser procedures can be categorized into three main groups: PresbyLASIK, Custom-Q, and Presbyond.131
The term PresbyLASIK encompasses various corneal-based treatments for presbyopia, including the AMO VISX presbyopia-correcting profile (AMO Development LLC, Milpitas, CA, USA), SUPRACOR (Technolas Perfect Vision GmbH, Munich, Germany), and PresbyMAX (Schwind eye-tech-solutions, Kleinoshteim, Germany).
The PresbyMAX technique is further divided into three subtypes: symmetric, micro-monovision, and hybrid.132 PresbyMAX symmetric creates a biaspheric cornea, with a central zone targeting −1.9D and a peripheral zone targeting −0.4D.133 PresbyMAX micro-monovision involves setting different refractive targets for the dominant and non-dominant eyes, such as 0D/-1.5D for the dominant eye and −0.8D/-2.3D for the non-dominant eye.132 PresbyMAX hybrid resembles micro-monovision but targets a lower degree of myopia in the dominant eye, aiming for −0.1D and −0.9D in the peripheral and central zones, respectively.134 All these techniques aim to create corneal multifocality, with the central area optimized for near vision and the peripheral area for distance vision.
Supracor produces multifocal corneal profile by creating a central elevation of approximately 12 μm within the central 3-mm zone to provide a near addition of about 1.75 D.135 This is surrounded by an aberration-optimized transition zone designed to preserve intermediate and distance vision. Distance correction is performed according to the baseline ametropia, with a target refraction of emmetropia or −0.50 D.
Custom-Q (Alcon Laboratories, Inc., Fort Worth, TX, USA) focuses on inducing a hyperprolate cornea in the non-dominant eye, which adds negative spherical aberration. Combined with a refractive target of −0.5D in the non-dominant eye and a distance-corrected dominant eye, this approach improves depth of field.136,137
Finally, Laser Blended Vision (LBV), originally developed by Dan Reinstein, integrates micromonovision (−1.5D in the non-dominant eye), the induction of spherical aberration, and neuroadaptation to extend depth of field.138 Studies indicate that Presbyond, an example of LBV, induces negative spherical aberration (Zernike coefficient (4,0)) to achieve this extended depth of field.138,139
Clinical Outcomes of Laser Vision Correction
PresbyLASIK
Uthoff et al assessed PresbyMAX symmetric (target +1.5 D) in presbyopes with hyperopia, emmetropia, or myopia.140 Overall, 83% could read standard newspaper print and UNVA better than 0.3 LogRAD was seen in 90% of emmetropes and 80% of hyperopes and myopes. UDVA of 0.1 LogMAR or better was achieved by 83% overall (100% hyperopes, 80% emmetropes, 70% myopes). CDVA loss ≥1 line occurred in 50% of hyperopes and emmetropes and 30% of myopes.
Baudu et al conducted one of the largest investigations of PresbyMAX symmetric, enrolling 358 presbyopic patients presenting with either myopia or hyperopia.133 At six months postoperatively, binocular uncorrected distance visual acuity (UDVA) better than 20/25 was achieved in 70% of the myopic cohort and 74% of the hyperopic cohort, while uncorrected near visual acuity (UNVA) of J3 or better was attained by 94% and 87% of patients, respectively. The authors also reported a retreatment rate of 19% in both groups.
PresbyMAX hybrid produced superior outcomes compared with PresbyMAX symmetric in the study by Luger et al134,141 At one year, 93% of patients achieved binocular UDVA of 20/20 or better. In subgroup analysis, 100% of myopes attained UDVA of 20/25 or better, while 94% of hyperopes achieved UDVA of 20/20 or better. Binocular UNVA of J2 or better was observed in 93% of myopes and 88% of hyperopes. Loss of ≥2 lines of CDVA occurred in 7% of myopes and 6% of hyperopes. Retreatment was required in 19% of cases and 3% underwent reversal of the treatment; after retreatment all patients achieved UDVA of 20/25 or better.
Ang et al evaluated Supracor in 69 hyperopic eyes of 58 patients, divided into three groups: bilateral Supracor, Supracor with contralateral hyperopic LASIK, and Supracor with no treatment in the fellow eye.135 Across all groups, 100% achieved binocular UDVA better than 20/25 and 93% UNVA of J2 or better, with no significant intergroup differences.
Pajic et al investigated Supracor with micro-monovision in myopic presbyopes and reported favorable outcomes at 6 months: 86% achieved UDVA of 20/20, 92% attained UIVA of 20/20, and 78% reached UNVA of 20/20. UNVA of 20/20 was seen in 36% of dominant and 64% of nondominant eyes, results comparable to those reported in hyperopic presbyopes.142
Jackson et al reported the study using the AMO VISX platform for central presbyLASIK, conducted in hyperopic presbyopes.143 At 1 year, all 25 patients achieved binocular UDVA of 20/25 or better and UNVA of J3 or better, while a loss of two lines of CDVA was observed in 10%.
Custom Q
Yin et al evaluated 138 hyperopic presbyopes and reported 1-year outcomes.144 Patients with a ΔQ of −0.8 achieved binocular UDVA of 20/16 and UNVA of J2. Overall, 100% attained UDVA of 20/25 or better and UNVA of J3 or better; however, 6% lost one line of CDVA and 13% required retreatment. Similarly, Courtin et al studied 65 patients and found 91% achieved UDVA of 20/20 or better and 81% UNVA of J3 or better.
Presbyond
Reinstein et al studied Presbyond in hyperopic, emmetropic, and myopic presbyopes.138,145,146 In hyperopes, 86% achieved CDVA of 20/20 and all had binocular CDVA ≥20/40, 81% read J2 and all reached at least J5. No patient lost ≥2 CDVA lines, however 22% required retreatment. Among emmetropes, 95% achieved UDVA of 20/20 and 96% UNVA of J2 or better, with no ≥2-line CDVA loss. Myopic patients achieved binocular UDVA of 20/20, with 99% attaining UNVA of J5 or better and 96% J2 or better.
Conclusions
In conclusion, modern approaches to presbyopia correction combine optical, pharmacological, and surgical strategies to enhance near vision and depth of field. Most current interventions—such as advanced intraocular lenses, miotic eye drops, and corneal or laser procedures—exploit the principles of pseudoaccommodation, although their mechanisms and outcomes differ. While these approaches can reduce spectacle dependence and improve functional vision, limitations such as dysphotopsia, reduced contrast sensitivity, and variability in patient selection remain key challenges for future research.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Helmholtz H. Ueber die Accommodation des Auges. Archiv für Ophthalmologie. 1855;1(2):1–19. doi:10.1007/BF02720789
2. Ravalico G, Baccara F. Apparent accommodation in pseudophakic eyes. Acta Ophthalmol. 1990;68(5):604–606. doi:10.1111/j.1755-3768.1990.tb04797.x
3. Langenbucher A, Huber S, Nguyen NX, Seitz B, Gusek-Schneider GC, Küchle M. Measurement of accommodation after implantation of an accommodating posterior chamber intraocular lens. J Cataract Refract Surg. 2003;29(4):677–685. doi:10.1016/s0886-3350(02)01893-x
4. Riaz KM, Wendelstein JA, Koch DD. Depth of field or depth of focus? J Cataract Refract Surg. 2024;50(12):1291–1292. doi:10.1097/j.jcrs.0000000000001548
5. Charman WN. The eye in focus: accommodation and presbyopia. Clin Exp Optom. 2008;91(3):207–225. doi:10.1111/j.1444-0938.2008.00256.x
6. Glasser A. Accommodation: mechanism and measurement. Ophthalmol Clin North Am. 2006;19(1):1–12. doi:10.1016/j.ohc.2005.09.004
7. Liu J, Dong Y, Wang Y. Efficacy and safety of extended depth of focus intraocular lenses in cataract surgery: a systematic review and meta-analysis. BMC Ophthalmol. 2019;19(1):198. doi:10.1186/s12886-019-1204-0
8. Alio JL, Plaza-Puche AB, Férnandez-Buenaga R, Pikkel J, Maldonado M. Multifocal intraocular lenses: an overview. Survey Ophthalmol. 2017;62(5):611–634. doi:10.1016/j.survophthal.2017.03.005
9. de Vries NE, Webers CA, Touwslager WR, et al. Dissatisfaction after implantation of multifocal intraocular lenses. J Cataract Refract Surg. 2011;37(5):859–865. doi:10.1016/j.jcrs.2010.11.032
10. Yeu E, Cuozzo S. Matching the patient to the intraocular lens: preoperative considerations to optimize surgical outcomes. Ophthalmology. 2021;128(11):e132–e141. doi:10.1016/j.ophtha.2020.08.025
11. Braga-Mele R, Chang D, Dewey S, et al. Multifocal intraocular lenses: relative indications and contraindications for implantation. J Cataract Refract Surg. 2014;40(2):313–322. doi:10.1016/j.jcrs.2013.12.011
12. Campbell FW. The depth of field of the human eye. Opt Acta. 1957;4(4):157–164. doi:10.1080/713826091
13. Atchison DA, Charman WN, Woods RL. Subjective depth-of-focus of the eye. Optom Vis Sci. 1997;74(7):511–520. doi:10.1097/00006324-199707000-00019
14. Gupta N, Wolffsohn JSW, Naroo SA. Optimizing measurement of subjective amplitude of accommodation with defocus curves. J Cataract Refract Surg. 2008;34(8):1329–1338. doi:10.1016/j.jcrs.2008.04.031
15. MacRae S, Holladay JT, Glasser A, et al. Special report: American Academy of Ophthalmology Task Force consensus statement for extended depth of focus intraocular lenses. Ophthalmology. 2017;124(1):139–141. doi:10.1016/j.ophtha.2016.09.039
16. Win-Hall DM, Glasser A. Objective accommodation measurements in pseudophakic subjects using an autorefractor and an aberrometer. J Cataract Refract Surg. 2009;35(2):282–290. doi:10.1016/j.jcrs.2008.10.033
17. Yi F, Iskander DR, Collins MJ. Estimation of the depth of focus from wavefront measurements. J Vis. 2010;10(4):3. doi:10.1167/10.4.3
18. Pérez-Merino P, Birkenfeld J, Dorronsoro C, et al. Aberrometry in patients implanted with accommodative intraocular lenses. Am J Ophthalmol. 2014;157(5):1077–1089. doi:10.1016/j.ajo.2014.02.013
19. Hayashi K, Manabe S, Hayashi H. Visual acuity from far to near and contrast sensitivity in eyes with a diffractive multifocal intraocular lens with a low addition power. J Cataract Refract Surg. 2009;35(12):2070–2076. doi:10.1016/j.jcrs.2009.07.010
20. Jackson A, Bailey I. Visual Acuity. Optometry Pract. 2004;5.
21. Bennett AG. Ophthalmic test types. A review of previous work and discussions on some controversial questions. Br J Physiol Opt. 1965;22(4):238–271.
22. Williams MA, Moutray TN, Jackson AJ. Uniformity of visual acuity measures in published studies. Invest Ophthalmol Visual Sci. 2008;49(10):4321–4327. doi:10.1167/iovs.07-0511
23. Moutray TN, Williams MA, Jackson AJ. Change of visual acuity recording methods in clinical studies across the years. Ophthalmologica. 2008;222(3):173–177. doi:10.1159/000126080
24. Sawusch MR, Guyton DL. Optimal astigmatism to enhance depth of focus after cataract surgery. Ophthalmology. 1991;98(7):1025–1029. doi:10.1016/s0161-6420(91)32182-1
25. Yamamoto T, Hiraoka T, Oshika T. Apparent accommodation in pseudophakic eyes with refractive against-the-rule, with-the-rule and minimum astigmatism. Br J Ophthalmol. 2016;100(4):565–571. doi:10.1136/bjophthalmol-2015-307032
26. Leube A, Ohlendorf A, Wahl S. The influence of induced astigmatism on the depth of focus. Optom Vis Sci. 2016;93(10):1228–1234. doi:10.1097/OPX.0000000000000961
27. Tavazzi S, Vlasak N, Zeri F. Effects of lens-induced astigmatism at near and far distances. Clin Optom. 2023;15:105–117. doi:10.2147/OPTO.S405472
28. Trindade F, Oliveira A, Frasson M. Benefit of against-the-rule astigmatism to uncorrected near acuity. J Cataract Refract Surg. 1997;23(1):82–85. doi:10.1016/s0886-3350(97)80155-1
29. Bradbury JA, Hillman JS, Cassells-Brown A. Optimal postoperative refraction for good unaided near and distance vision with monofocal intraocular lenses. Br J Ophthalmol. 1992;76(5):300–302. doi:10.1136/bjo.76.5.300
30. Hillman JS, Bradbury JA. Apparent accommodation by myopic astigmatism with monofocal intraocular lenses. Eur J Implant Refractive Surg. 1990;2(2):101–104. doi:10.1016/S0955-3681(13)80333-4
31. Datiles MB, Gancayco T. Low myopia with low astigmatic correction gives cataract surgery patients good depth of focus. Ophthalmology. 1990;97(7):922–926. doi:10.1016/s0161-6420(90)32480-6
32. Nanavaty MA, Vasavada AR, Patel AS, Raj SM, Desai TH. Analysis of patients with good uncorrected distance and near vision after monofocal intraocular lens implantation. J Cataract Refract Surg. 2006;32(7):1091–1097. doi:10.1016/j.jcrs.2006.03.021
33. Verzella F, Calossi A. Multifocal effect of against-the-rule myopic astigmatism in pseudophakic eyes. Refract Corneal Surg. 1993;9(1):58–61.
34. Nagpal KM, Desai C, Trivedi RH, Vasavada AR. Is pseudophakic astigmatism a desirable goal? Indian J Ophthalmol. 2000;48(3):213–216.
35. Singh A, Pesala V, Garg P, Bharadwaj SR. Relation between uncorrected astigmatism and visual acuity in pseudophakia. Optom Vis Sci. 2013;90(4):378–384. doi:10.1097/OPX.0b013e318288afb5
36. Tsukamoto M, Nakajima K, Nishino J, Hara O, Uozato H, Saishin M. Accommodation causes with-the-rule astigmatism in emmetropes. Optom Vis Sci. 2000;77(3):150–155. doi:10.1097/00006324-200003000-00014
37. Savage H, Rothstein M, Davuluri G, El Ghormli L, Zaetta DM. Myopic astigmatism and presbyopia trial. Am J Ophthalmol. 2003;135(5):628–632. doi:10.1016/s0002-9394(02)02223-7
38. Kamiya K, Kawamorita T, Uozato H, Kasugai H, Shimizu K. Effect of astigmatism on apparent accommodation in pseudophakic eyes. Optom Vis Sci. 2012;89(2):148–154. doi:10.1097/OPX.0b013e31823ededa
39. Stern B, Gatinel D. Impact of pupil size and corneal spherical aberrations on the performance of monofocal intraocular lenses: an experimental model. Biomed Opt Express. 2024;15(11):6433–6448. doi:10.1364/BOE.530708
40. Oshika T, Tokunaga T, Samejima T, Miyata K, Kawana K, Kaji Y. Influence of pupil diameter on the relation between ocular higher-order aberration and contrast sensitivity after laser in situ keratomileusis. Invest Ophthalmol Visual Sci. 2006;47(4):1334–1338. doi:10.1167/iovs.05-1154
41. Leibowitz H. The effect of pupil size on visual acuity for photometrically equated test fields at various levels of luminance*. J Opt Soc Am. 1952;42(6):416–422. doi:10.1364/JOSA.42.000416
42. Marcos S, Moreno E, Navarro R. The depth-of-field of the human eye from objective and subjective measurements. Vision Res. 1999;39(12):2039–2049. doi:10.1016/s0042-6989(98)00317-4
43. Tucker J, Charman WN. The depth-of-focus of the human eye for Snellen letters. Am J Optom Physiol Opt. 1975;52(1):3–21. doi:10.1097/00006324-197501000-00002
44. Charman WN, Whitefoot H. Pupil diameter and the depth-of-field of the human eye as measured by laser speckle. Opt Acta. 1977;24(12):1211–1216. doi:10.1080/713819479
45. Ogle KN, Schwartz JT. Depth of focus of the human eye. J Opt Soc Am. 1959;49(3):273–280. doi:10.1364/josa.49.000273
46. Yamamoto S, Adachi-Usami E. Apparent accommodation in pseudophakic eyes as measured with visually evoked potentials. Invest Ophthalmol Vis Sci. 1992;33(2):443–446.
47. Lim DH, Han JC, Kim MH, Chung ES, Chung TY. Factors affecting near vision after monofocal intraocular lens implantation. J Refract Surg. 2013;29(3):200–204. doi:10.3928/1081597X-20130129-06
48. Nanavaty MA, Mukhija R, Ashena Z, Bunce C, Spalton DJ. Incidence and factors for pseudoaccommodation after monofocal lens implantation: the monofocal extended range of vision study. J Cataract Refract Surg. 2023;49(12):1229–1235. doi:10.1097/j.jcrs.0000000000001302
49. Benard Y, Lopez-Gil N, Legras R. Subjective depth of field in presence of 4th-order and 6th-order Zernike spherical aberration using adaptive optics technology. J Cataract Refract Surg. 2010;36(12):2129–2138. doi:10.1016/j.jcrs.2010.07.022
50. Xu R, Wang H, Jaskulski M, Kollbaum P, Bradley A. Small-pupil versus multifocal strategies for expanding depth of focus of presbyopic eyes. J Cataract Refract Surg. 2019;45(5):647–655. doi:10.1016/j.jcrs.2019.01.015
51. Sergienko NM, Kondratenko YN, Tutchenko NN. Depth of focus in pseudophakic eyes. Graefes Arch Clin Exp Ophthalmol. 2008;246(11):1623–1627. doi:10.1007/s00417-008-0923-3
52. Renna A, Vejarano LF, De la Cruz E, Alio JL. Pharmacological treatment of presbyopia by novel binocularly instilled eye drops: a pilot study. Ophthalmol Ther. 2016;5(1):63–73. doi:10.1007/s40123-016-0050-x
53. Zimmerman TJ, Wheeler TM. Miotics: side effects and ways to avoid them. Ophthalmology. 1982;89(1):76–80. doi:10.1016/s0161-6420(82)34866-6
54. Benozzi J, Benozzi G, Orman B. Presbyopia: a new potential pharmacological treatment. Med Hypothesis Discov Innov Ophthalmol. 2012;1(1):3–5.
55. Haghpanah N, Alany R. Pharmacological treatment of presbyopia: a systematic review. Eur J Transl Myol. 2022;32(3). doi:10.4081/ejtm.2022.10781
56. Vargas V, Vejarano F, Alio JL. Near vision improvement with the use of a new topical compound for presbyopia correction: a prospective, consecutive interventional non-comparative clinical study. Ophthalmol Ther. 2019;8(1):31–39. doi:10.1007/s40123-018-0154-6
57. Institutional/corporate author. Vuity - pilocarpine ophthalmic solution for presbyopia. Med Lett Drugs Ther. 2022;64(1643):17–18.
58. GOt W, Price FW, Wirta D, et al. Safety and efficacy of AGN-190584 in individuals with presbyopia: the GEMINI 1 phase 3 randomized clinical trial. JAMA Ophthalmol. 2022;140(4):363–371. doi:10.1001/jamaophthalmol.2022.0059
59. Institutional/corporate author. Qlosi - pilocarpine 0.4% ophthalmic solution for presbyopia. Med Lett Drugs Ther. 2025;67(1719):5–6. doi:10.58347/tml.2025.1719b
60. Holland E, Karpecki P, Fingeret M, et al. Efficacy and safety of CSF-1 (0.4% Pilocarpine Hydrochloride) in presbyopia: pooled results of the NEAR phase 3 randomized, clinical trials. Clin Ther. 2024;46(2):104–113. doi:10.1016/j.clinthera.2023.12.005
61. Abdelkader A. Improved presbyopic vision with miotics. Eye Contact Lens. 2015;41(5):323–327. doi:10.1097/ICL.0000000000000137
62. Abdelkader A, Kaufman HE. Clinical outcomes of combined versus separate carbachol and brimonidine drops in correcting presbyopia. Eye Vis. 2016;3:31. doi:10.1186/s40662-016-0065-3
63. Safety and Efficacy Study BRIMOCHOLTM PF and Carbachol PF in Subjects With Emmetropic Phakic or Pseudophakic Presbyopia NCT05270863. Available from: https://clinicaltrials.gov/study/NCT05270863?term=brimochol%20pf&rank=1.
64. LENZ Therapeutics I. LENZ Therapeutics Announces Positive Topline Data from Phase 3 CLARITY Presbyopia Trials. Available from: https://ir.lenz-tx.com/news-events/press-releases/detail/11/lenz-therapeutics-announces-positive-topline-data-from-phase-3-clarity-presbyopia-trials.
65. clinicaltrials.gov. Phase 3 Safety Study for the Treatment of Presbyopia Subjects NCT05753189 Available from: https://clinicaltrials.gov/study/NCT05753189?term=LNZ%20100&rank=2.
66. Stern B, Gatinel D. Comment on: impact of spherical aberration on visual quality and depth of focus. J Cataract Refract Surg. 2024;50(12):1297–1298. doi:10.1097/j.jcrs.0000000000001551
67. Rocha KM, Vabre L, Chateau N, Krueger RR. Expanding depth of focus by modifying higher-order aberrations induced by an adaptive optics visual simulator. J Cataract Refract Surg. 2009;35(11):1885–1892. doi:10.1016/j.jcrs.2009.05.059
68. Legras R, Benard Y, Lopez-Gil N. Effect of coma and spherical aberration on depth-of-focus measured using adaptive optics and computationally blurred images. J Cataract Refract Surg. 2012;38(3):458–469. doi:10.1016/j.jcrs.2011.10.032
69. Zheleznyak L, Jung H, Yoon G. Impact of pupil transmission apodization on presbyopic through-focus visual performance with spherical aberration. Invest Ophthalmol Vis Sci. 2014;55(1):70–77. doi:10.1167/iovs.13-13107
70. Nishi T, Nawa Y, Ueda T, Masuda K, Taketani F, Hara Y. Effect of total higher-order aberrations on accommodation in pseudophakic eyes. J Cataract Refract Surg. 2006;32(10):1643–1649. doi:10.1016/j.jcrs.2006.05.020
71. Yi F, Iskander DR, Collins M. Depth of focus and visual acuity with primary and secondary spherical aberration. Vision Res. 2011;51(14):1648–1658. doi:10.1016/j.visres.2011.05.006
72. Oshika T, Mimura T, Tanaka S, et al. Apparent accommodation and corneal wavefront aberration in pseudophakic eyes. Invest Ophthalmol Vis Sci. 2002;43(9):2882–2886.
73. Benard Y, Lopez-Gil N, Legras R. Optimizing the subjective depth-of-focus with combinations of fourth- and sixth-order spherical aberration. Vision Res. 2011;51(23–24):2471–2477. doi:10.1016/j.visres.2011.10.003
74. Song IS, Kim MJ, Yoon SY, Kim JY, Tchah H. Higher-order aberrations associated with better near visual acuity in eyes with aspheric monofocal IOLs. J Refract Surg. 2014;30(7):442–446. doi:10.3928/1081597X-20140530-01
75. García-Bella J, Burgos-Blasco B, Vidal-Villegas B, Garzón N, Villanueva C, García-Feijoo J. Visual and refractive outcomes after bilateral implantation of an enhanced monofocal intraocular lens: prospective study. J Cataract Refract Surg. 2024;50(6):585–590. doi:10.1097/j.jcrs.0000000000001422
76. Nanavaty MA, Spalton DJ, Boyce J, Saha S, Marshall J. Wavefront aberrations, depth of focus, and contrast sensitivity with aspheric and spherical intraocular lenses: fellow-eye study. J Cataract Refract Surg. 2009;35(4):663–671. doi:10.1016/j.jcrs.2008.12.011
77. Kanclerz P, Toto F, Grzybowski A, Alio JL. Extended depth-of-field intraocular lenses: an update. Asia Pac J Ophthalmol. 2020;9(3):194–202. doi:10.1097/apo.0000000000000296
78. Hickenbotham A, Tiruveedhula P, Roorda A. Comparison of spherical aberration and small-pupil profiles in improving depth of focus for presbyopic corrections. J Cataract Refract Surg. 2012;38(12):2071–2079. doi:10.1016/j.jcrs.2012.07.028
79. Reinstein DZ, Archer TJ, Couch D, Schroeder E, Wottke M. A new night vision disturbances parameter and contrast sensitivity as indicators of success in wavefront-guided enhancement. Slack Incorporated Thorofare NJ. 2005;S535–S540.
80. Kriechbaum K, Findl O, Koeppl C, Menapace R, Drexler W. Stimulus-driven versus pilocarpine-induced biometric changes in pseudophakic eyes. Ophthalmology. 2005;112(3):453–459. doi:10.1016/j.ophtha.2004.09.021
81. Marchini G, Pedrotti E, Modesti M, Visentin S, Tosi R. Anterior segment changes during accommodation in eyes with a monofocal intraocular lens: high-frequency ultrasound study. J Cataract Refract Surg. 2008;34(6):949–956. doi:10.1016/j.jcrs.2008.02.018
82. Findl O, Kriechbaum K, Menapace R, et al. Laserinterferometric assessment of pilocarpine-induced movement of an accommodating intraocular lens: a randomized trial. Ophthalmology. 2004;111(8):1515–1521. doi:10.1016/j.ophtha.2003.12.057
83. Vamosi P, Nemeth G, Berta A. Pseudophakic accommodation with 2 models of foldable intraocular lenses. J Cataract Refract Surg. 2006;32(2):221–226. doi:10.1016/j.jcrs.2005.08.059
84. Cleary G, Spalton DJ, Gala KB. A randomized intraindividual comparison of the accommodative performance of the bag-in-the-lens intraocular lens in presbyopic eyes. Am J Ophthalmol. 2010;150(5):619–627e1. doi:10.1016/j.ajo.2010.06.003
85. Alió JL, Alió Del Barrio JL, Vega-Estrada A. Accommodative intraocular lenses: where are we and where we are going. Eye and Vision. 2017;4(1):16. doi:10.1186/s40662-017-0077-7
86. Mastropasqua L, Toto L, Falconio G, et al. Longterm results of 1 CU accommodative intraocular lens implantation: 2-year follow-up study. Acta Ophthalmol Scand. 2007;85(4):409–414. doi:10.1111/j.1600-0420.2006.00866.x
87. Alió JL, Ben-nun J, Rodríguez-Prats JL, Plaza AB. Visual and accommodative outcomes 1 year after implantation of an accommodating intraocular lens based on a new concept. J Cataract Refract Surg. 2009;35(10):1671–1678. doi:10.1016/j.jcrs.2009.04.043
88. Ribeiro F, Dick HB, Kohnen T, et al. Evidence-based functional classification of simultaneous vision intraocular lenses: seeking a global consensus by the ESCRS Functional Vision Working Group. J Cataract Refract Surg. 2024;50(8):794–798. doi:10.1097/j.jcrs.0000000000001502
89. Artal P, Berrio E, Guirao A, Piers P. Contribution of the cornea and internal surfaces to the change of ocular aberrations with age. J Opt Soc Am a Opt Image Sci Vis. 2002;19(1):137–143. doi:10.1364/josaa.19.000137
90. Smith G, Cox MJ, Calver R, Garner LF. The spherical aberration of the crystalline lens of the human eye. Vision Research. 2001;41(2):235–243. doi:10.1016/S0042-6989(00)00206-6
91. Yagci R, Uzun F, Acer S, Hepsen IF. Comparison of visual quality between aspheric and spherical IOLs. Eur J Ophthalmol. 2014;24(5):688–692. doi:10.5301/ejo.5000452
92. Raina UK, Gupta A, Bhambhwani V, Bhushan G, Seth A, Ghosh B. The optical performance of spherical and aspheric intraocular lenses in pediatric eyes: a comparative study. J Pediatr Ophthalmol Strabismus. 2015;52(4):232–238. doi:10.3928/01913913-20150520-03
93. Schuster AK, Tesarz J, Vossmerbaeumer U. The impact on vision of aspheric to spherical monofocal intraocular lenses in cataract surgery: a systematic review with meta-analysis. Ophthalmology. 2013;120(11):2166–2175. doi:10.1016/j.ophtha.2013.04.011
94. Kozhaya K, Kenny PI, Esfandiari S, Wang L, Weikert MP, Koch DD. Effect of spherical aberration on visual acuity and depth of focus in pseudophakic eyes. J Cataract Refract Surg. 2024;50(1):24–29. doi:10.1097/j.jcrs.0000000000001314
95. Rocha KM, Soriano ES, Chamon W, Chalita MR, Nosé W. Spherical aberration and depth of focus in eyes implanted with aspheric and spherical intraocular lenses: a prospective randomized study. Ophthalmology. 2007;114(11):2050–2054. doi:10.1016/j.ophtha.2007.01.024
96. Holladay JT, Kozhaya K. Reply: impact of spherical aberration on visual quality and depth of focus. J Cataract Refract Surg. 2024;50(12):1298–1299. doi:10.1097/j.jcrs.0000000000001552
97. Nanavaty MA, Spalton DJ, Gala KB. Fellow-eye comparison of 2 aspheric microincision intraocular lenses and effect of asphericity on visual performance. J Cataract Refract Surg. 2012;38(4):625–632. doi:10.1016/j.jcrs.2011.10.039
98. Fernández J, Rocha-de-Lossada C, Zamorano-Martín F, Rodríguez-Calvo-de-Mora M, Rodríguez-Vallejo M. Positioning of enhanced monofocal intraocular lenses between conventional monofocal and extended depth of focus lenses: a scoping review. BMC Ophthalmol. 2023;23(1):101. doi:10.1186/s12886-023-02844-1
99. Giglio R, Vinciguerra AL, Presotto M, et al. Visual outcomes and patient satisfaction after bilateral implantation of an enhanced monofocal intraocular lens: a single-masked prospective randomized study. Int Ophthalmol. 2024;44(1):112. doi:10.1007/s10792-024-02946-9
100. Auffarth GU, Gerl M, Tsai L, et al. Clinical evaluation of a new monofocal IOL with enhanced intermediate function in patients with cataract. J Cataract Refract Surg. 2021;47(2):184–191. doi:10.1097/j.jcrs.0000000000000399
101. Ang RET, Stodulka P, Poyales F. Prospective randomized single-masked study of bilateral isofocal optic-design or monofocal intraocular lenses. Clin Ophthalmol. 2023;17:2231–2242. doi:10.2147/OPTH.S425352
102. Mencucci R, Morelli A, Cennamo M, Roszkowska AM, Favuzza E. Enhanced monofocal intraocular lenses: a retrospective, comparative study between three different models. J Clin Med. 2023;12(10). doi:10.3390/jcm12103588
103. Megiddo-Barnir E, Alió JL. Latest development in extended depth-of-focus intraocular lenses: an update. Asia-Pac J Ophthalmol. 2023;12(1):58–79. doi:10.1097/APO.0000000000000590
104. Alarcon A, Del Aguila Carrasco A, Gounou F, Weeber H, Cánovas C, Piers P. Optical and clinical simulated performance of a new refractive extended depth of focus intraocular lens. Eye. 2024;38(Suppl 1):4–8. doi:10.1038/s41433-024-03041-0
105. Rodov L, Reitblat O, Levy A, Assia EI, Kleinmann G. Visual outcomes and patient satisfaction for trifocal, extended depth of focus and monofocal intraocular lenses. J Refract Surg. 2019;35(7):434–440. doi:10.3928/1081597x-20190618-01
106. Monaco G, Gari M, Di Censo F, Poscia A, Ruggi G, Scialdone A. Visual performance after bilateral implantation of 2 new presbyopia-correcting intraocular lenses: trifocal versus extended range of vision. J Cataract Refract Surg. 2017;43(6):737–747. doi:10.1016/j.jcrs.2017.03.037
107. Shafer BM, McCabe C, Reiser H, Newsom TH, Berdahl J. The REVIVE study: long term outcomes of a novel non-diffractive extended vision IOL versus monofocal control IOL. Clin Ophthalmol. 2022;16:3945–3950. doi:10.2147/OPTH.S390380
108. Pantanelli SM, O’Rourke T, Bolognia O, Scruggs K, Longenecker A, Lehman E. Vision and patient-reported outcomes with nondiffractive EDOF or neutral aspheric monofocal intraocular lenses. J Cataract Refract Surg. 2023;49(4):360–366. doi:10.1097/j.jcrs.0000000000001123
109. Campos N, Loureiro T, Rodrigues-Barros S, et al. Preliminary clinical outcomes of a new enhanced depth of focus intraocular lens. Clin Ophthalmol. 2021;15:4801–4807. doi:10.2147/OPTH.S344379
110. Tahmaz V, Siebelmann S, Koch KR, Cursiefen C, Langenbucher A, Hoerster R. Evaluation of a novel non-diffractive extended depth of focus intraocular lens - first results from a prospective study. Curr Eye Res. 2022;47(8):1149–1155. doi:10.1080/02713683.2022.2074046
111. Auffarth GU, Moraru O, Munteanu M, et al. European, multicenter, prospective, non-comparative clinical evaluation of an extended depth of focus intraocular lens. J Refract Surg. 2020;36(7):426–434. doi:10.3928/1081597X-20200603-01
112. Savini G, Balducci N, Carbonara C, et al. Functional assessment of a new extended depth-of-focus intraocular lens. Eye. 2019;33(3):404–410. doi:10.1038/s41433-018-0221-1
113. Dick HB, Piovella M, Vukich J, Vilupuru S, Lin L, Clinical I. Prospective multicenter trial of a small-aperture intraocular lens in cataract surgery. J Cataract Refract Surg. 2017;43(7):956–968. doi:10.1016/j.jcrs.2017.04.038
114. Hooshmand J, Allen P, Huynh T, et al. Small aperture IC-8 intraocular lens in cataract patients: achieving extended depth of focus through small aperture optics. Eye. 2019;33(7):1096–1103. doi:10.1038/s41433-019-0363-9
115. Iradier MT, Cruz V, Gentile N, Cedano P, Pinero DP. Clinical outcomes with a novel extended depth of focus presbyopia-correcting intraocular lens: pilot study. Clin Ophthalmol. 2021;15:1215–1221. doi:10.2147/OPTH.S297985
116. Rabinovich M, Ceresara G, Aramburu Del Boz A, Al Khatib D, Crespe M, Bovet J. Visual outcomes after implantation of lucidis EDOF IOL. J Ophthalmol. 2022;2022:5100861. doi:10.1155/2022/5100861
117. Pedrotti E, Bonacci E, Kilian R, et al. Quality of vision and outcomes after bilateral implantation of pseudo-non diffracting beam IOL. Front Med Lausanne. 2023;10:1085280. doi:10.3389/fmed.2023.1085280
118. Chang DH, Janakiraman DP, Smith PJ, et al. Visual outcomes and safety of an extended depth-of-focus intraocular lens: results of a pivotal clinical trial. J Cataract Refract Surg. 2022;48(3):288–297. doi:10.1097/j.jcrs.0000000000000747
119. Reinhard T, Maier P, Bohringer D, et al. Comparison of two extended depth of focus intraocular lenses with a monofocal lens: a multi-centre randomised trial. Graefes Arch Clin Exp Ophthalmol. 2021;259(2):431–442. doi:10.1007/s00417-020-04868-5
120. Bilbao-Calabuig R, Llovet-Rausell A, Ortega-Usobiaga J, et al. Visual outcomes following bilateral lmplantation of two diffractive trifocal intraocular lenses in 10 084 eyes. Am J Ophthalmol. 2017;179:55–66. doi:10.1016/j.ajo.2017.04.013
121. Mendicute J, Kapp A, Levy P, et al. Evaluation of visual outcomes and patient satisfaction after implantation of a diffractive trifocal intraocular lens. J Cataract Refract Surg. 2016;42(2):203–210. doi:10.1016/j.jcrs.2015.11.037
122. Cochener B, Vryghem J, Rozot P, et al. Clinical outcomes with a trifocal intraocular lens: a multicenter study. J Refract Surg. 2014;30(11):762–768. doi:10.3928/1081597X-20141021-08
123. Poyales F, Perez R, Lopez-Brea I, Zhou Y, Rico L, Garzon N. Comparison of visual performance and patient satisfaction outcomes with two trifocal IOLs with similar optical design but different materials. Clin Ophthalmol. 2020;14:3237–3247. doi:10.2147/OPTH.S273641
124. Alio JL, Plaza-Puche AB, Alio Del Barrio JL, et al. Clinical outcomes with a diffractive trifocal intraocular lens. Eur J Ophthalmol. 2018;28(4):419–424. doi:10.1177/1120672118762231
125. Chang DH, Hu JG, Lehmann RP, Thompson VM, Tsai LH, Thomas EK. Clinical performance of a hybrid presbyopia-correcting intraocular lens in patients undergoing cataract surgery in a multicenter trial. J Cataract Refract Surg. 2023;49(8):840–847. doi:10.1097/j.jcrs.0000000000001205
126. Ferreira TB, Ribeiro FJ, Silva D, Matos AC, Gaspar S, Almeida S. Comparison of refractive and visual outcomes of 3 presbyopia-correcting intraocular lenses. J Cataract Refract Surg. 2022;48(3):280–287. doi:10.1097/j.jcrs.0000000000000743
127. Modi S, Lehmann R, Maxwell A, et al. Visual and patient-reported outcomes of a diffractive trifocal intraocular lens compared with those of a monofocal intraocular lens. Ophthalmology. 2021;128(2):197–207. doi:10.1016/j.ophtha.2020.07.015
128. Rampat R, Gatinel D. Multifocal and Extended Depth-of-Focus Intraocular Lenses in 2020. Ophthalmology. 2021;128(11):e164–e185. doi:10.1016/j.ophtha.2020.09.026
129. Hovanesian JA, Jones M, Allen Q. The vivity extended range of vision IOL vs the PanOptix Trifocal, ReStor 2.5 active focus and ReStor 3.0 multifocal lenses: a comparison of patient satisfaction, visual disturbances, and spectacle Independence. Clin Ophthalmol. 2022;16:145–152. doi:10.2147/opth.S347382
130. Gundersen KG, Potvin R. Trifocal intraocular lenses: a comparison of the visual performance and quality of vision provided by two different lens designs. Clin Ophthalmol. 2017;11:1081–1087. doi:10.2147/opth.S136164
131. Fernández J, Molina-Martín A, Rocha-de-Lossada C, Rodríguez-Vallejo M, Piñero DP. Clinical outcomes of presbyopia correction with the latest techniques of presbyLASIK: a systematic review. Eye. 2023;37(4):587–596. doi:10.1038/s41433-022-02175-3
132. Shetty R, Brar S, Sharma M, Dadachanji Z, Lalgudi VG. PresbyLASIK: a review of PresbyMAX, supracor, and laser blended vision: principles, planning, and outcomes. Indian J Ophthalmol. 2020;68(12):2723–2731. doi:10.4103/ijo.IJO_32_20
133. Baudu P, Penin F, Arba Mosquera S. Uncorrected binocular performance after biaspheric ablation profile for presbyopic corneal treatment using AMARIS with the PresbyMAX module. Am J Ophthalmol. 2013;155(4):636–647,647.e1. doi:10.1016/j.ajo.2012.10.023
134. Luger MH, McAlinden C, Buckhurst PJ, Wolffsohn JS, Verma S, Arba Mosquera S. Presbyopic LASIK using hybrid bi-aspheric micro-monovision ablation profile for presbyopic corneal treatments. Am J Ophthalmol. 2015;160(3):493–505. doi:10.1016/j.ajo.2015.05.021
135. Ang RE, Cruz EM, Pisig AU, Solis ML, Reyes RM, Youssefi G. Safety and effectiveness of the SUPRACOR presbyopic LASIK algorithm on hyperopic patients. Eye Vis. 2016;3:33. doi:10.1186/s40662-016-0062-6
136. Vargas-Fragoso V, Alió JL. Corneal compensation of presbyopia: PresbyLASIK: an updated review. Eye Vis. 2017;4:11. doi:10.1186/s40662-017-0075-9
137. Stival LR, Figueiredo MN, Santhiago MR. Presbyopic excimer laser ablation: a review. J Refract Surg. 2018;34(10):698–710. doi:10.3928/1081597x-20180726-02
138. Reinstein DZ, Carp GI, Archer TJ, Gobbe M. LASIK for presbyopia correction in emmetropic patients using aspheric ablation profiles and a micro-monovision protocol with the Carl Zeiss Meditec MEL 80 and VisuMax. J Refract Surg. 2012;28(8):531–541. doi:10.3928/1081597x-20120723-01
139. Ganesh S, Brar S, Gautam M, Sriprakash K. Visual and refractive outcomes following laser blended vision using non-linear aspheric micro-monovision. J Refract Surg. 2020;36(5):300–307. doi:10.3928/1081597x-20200407-02
140. Uthoff D, Pölzl M, Hepper D, Holland D. A new method of cornea modulation with excimer laser for simultaneous correction of presbyopia and ametropia. Graefes Arch Clin Exp Ophthalmol. 2012;250(11):1649–1661. doi:10.1007/s00417-012-1948-1
141. Luger MH, Ewering T, Arba-Mosquera S. One-year experience in presbyopia correction with biaspheric multifocal central presbyopia laser in situ keratomileusis. Cornea. 2013;32(5):644–652. doi:10.1097/ICO.0b013e31825f02f5
142. Pajic B, Pajic-Eggspuehler B, Mueller J, Cvejic Z, Studer H. A novel laser refractive surgical treatment for presbyopia: optics-based customization for improved clinical outcome. Sensors. 2017;17(6):1367.
143. Jackson WB, Tuan KM, Mintsioulis G. Aspheric wavefront-guided LASIK to treat hyperopic presbyopia: 12-month results with the VISX platform. J Refract Surg. 2011;27(7):519–529. doi:10.3928/1081597x-20101110-02
144. Wang Yin GH, McAlinden C, Pieri E, Giulardi C, Holweck G, Hoffart L. Surgical treatment of presbyopia with central presbyopic keratomileusis: one-year results. J Cataract Refract Surg. 2016;42(10):1415–1423. doi:10.1016/j.jcrs.2016.07.031
145. Reinstein DZ, Archer TJ, Gobbe M. LASIK for myopic astigmatism and presbyopia using non-linear aspheric micro-monovision with the Carl Zeiss Meditec MEL 80 Platform. J Refract Surg. 2011;27(1):23–37. doi:10.3928/1081597x-20100212-04
146. Reinstein DZ, Couch DG, Archer TJ. LASIK for hyperopic astigmatism and presbyopia using micro-monovision with the Carl Zeiss Meditec MEL80 platform. J Refract Surg. 2009;25(1):37–58. doi:10.3928/1081597x-20090101-07
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.