Back to Journals » Psychology Research and Behavior Management » Volume 19
The SCCAI and Mayo Endoscopic Severity Scores Are Positively Correlated with QIDS-SR16 Depression Scores in Patients with Ulcerative Colitis
Authors Yang Z, Pang S, Jiang C, Zong Y
Received 16 October 2025
Accepted for publication 27 December 2025
Published 8 January 2026 Volume 2026:19 574826
DOI https://doi.org/10.2147/PRBM.S574826
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Igor Elman
Ziqi Yang,1,* Shu Pang,1,* Chunyan Jiang,1 Ye Zong2– 4
1Department of General Medicine, Beijing Friendship Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Department of Gastroenterology, Beijing Friendship Hospital, Capital Medical University, Beijing, People’s Republic of China; 3National Clinical Research Center for Digestive Diseases, Beijing, People’s Republic of China; 4Beijing Key Laboratory for Early Gastrointestinal Cancer Diagnosis and Therapy, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chunyan Jiang, Email [email protected] Ye Zong, Email [email protected]
Background: Ulcerative colitis (UC) is often accompanied by depressive symptoms, yet the association between disease activity and depression remains insufficiently characterized.
Objective: To evaluate the correlations between SCCAI scores, Mayo endoscopic severity scores, and QIDS-SR16 depression scores in patients with UC.
Methods: This cross-sectional study included 106 hospitalized UC patients from January 2023 to December 2024. Disease activity was assessed using the Simple Clinical Colitis Activity Index (SCCAI), and endoscopic severity was assessed with the Mayo score in a subsample (n = 54). Depressive symptoms were evaluated using QIDS-SR16. Multivariable linear regression and restricted cubic spline models were applied to examine linear and nonlinear associations.
Results: A 1-point increase in SCCAI score was associated with a 0.41-point increase in QIDS-SR16 score (β = 0.41, 95% CI: 0.19– 0.63, P < 0.001). A 1-point increase in the Mayo score corresponded to a 1.07-point increase in QIDS-SR16 (β = 1.07, 95% CI: 0.24– 1.90, P = 0.015). Restricted cubic spline analysis revealed a nonlinear association between SCCAI and QIDS-SR16, with greater sensitivity of depressive symptoms at lower SCCAI levels.
Conclusion: In this cross-sectional real-world study, both clinical disease activity (SCCAI) and endoscopic severity (Mayo score) were independently and positively correlated with depressive symptom burden in UC patients. These findings support incorporating routine depression screening into UC clinical management to facilitate timely detection and intervention.
Keywords: ulcerative colitis, SCCAI, mayo score, depressive symptoms, QIDS-SR16
Introduction
Research Background
Inflammatory bowel disease (IBD), encompassing Crohn’s disease (CD) and ulcerative colitis (UC), is characterized by chronic intestinal inflammation. Over recent decades, its incidence has risen substantially worldwide, particularly in industrializing regions. In China, the age-standardized incidence increased from approximately 1.2–1.7 per 100,000 in 1990 to 2.7–3.4 per 100,000 in 2019, with an average annual growth rate of around 2.5%, similar to East Asia (2.54%).1,2 IBD affects not only gastrointestinal physiology but also imposes a considerable mental health burden.3 Systematic reviews and cohort studies report that 21%–25% of IBD patients experience depressive symptoms, with some European cohorts reporting up to 28%.4,5 Female sex, active disease, and older age are major risk factors.6 Depression and anxiety significantly reduce quality of life (eg, lower SIBDQ/IBDQ scores), and are associated with increased work impairment and social dysfunction.3,7 Furthermore, depression may exacerbate intestinal inflammation through the gut–brain axis—via neuroimmune, endocrine, and autonomic mechanisms—leading to a higher risk of relapse.8 Meta-analytic evidence has shown strong bidirectional interactions between psychological disorders and IBD activity, including the gut-brain effect in IBD populations.9 Depression is linked to higher hospitalization, relapse risk, and increased healthcare utilization.10,11 Although CD patients may exhibit slightly higher psychological comorbidity compared with UC, rates are elevated in both groups relative to the general population.12 However, recognition and treatment of depression and anxiety remain inadequate, particularly among socially disadvantaged groups.13 Growing evidence also suggests that treating depression and anxiety can improve IBD inflammatory activity, strengthening the biological plausibility of gut–brain interactions.14 In addition, recent mechanistic reviews highlight neuroimmune pathways (eg, cytokine signaling, microglial activation) that contribute to maintenance of gut–brain dysregulation in IBD.15 Given these findings, clarifying the interplay between disease activity and depressive symptoms in UC, particularly within Chinese cohorts—which remain underrepresented in existing literature—is clinically important.
Current Status of Research
The Simple Clinical Colitis Activity Index (SCCAI) is widely used to evaluate UC activity, while the Quick Inventory of Depressive Symptomatology Self-Rated 16-item (QIDS-SR16) is an established unidimensional tool for assessing depressive symptoms.16,17 Recent multicenter and prospective cohort studies have demonstrated moderate to strong correlations between patient-reported disease activity (eg, SCCAI or P-SCCAI) and depressive symptoms measured by PHQ-9 or other standardized scales.18–21 However, several research gaps remain within Chinese UC populations. First, although SCCAI includes items related to general well-being and emotional state, potential conceptual overlap with depression scales has not been sufficiently addressed. Meta-analytic evidence suggests that symptom overlap may influence correlation strength, underscoring the need for sensitivity analyses. Second, the clinical utility of QIDS-SR16 has not been extensively evaluated in Chinese UC cohorts, despite its potential advantages over PHQ-9 or HADS, including stronger psychometric unidimensionality and better discrimination of depressive severity. Furthermore, biological and behavioral pathways link psychological status to disease course. Stress-induced dysregulation of the hypothalamic–pituitary–adrenal axis, neuroimmune activation, and reduced medication adherence may all exacerbate UC activity.22 Social and economic factors also influence disease outcomes by shaping psychological well-being.23 As acknowledged by the 2020 international consensus, routine mental health screening—via instruments such as PHQ-9 or QIDS-SR16—should be incorporated into UC management.24 Therefore, this study aims to (1) examine the relationship between SCCAI and QIDS-SR16 scores in a Chinese UC cohort, (2) evaluate whether endoscopic severity (Mayo score) influences depressive symptom burden, and (3) perform sensitivity analyses to account for potential overlap between SCCAI well-being items and depressive symptom measures.
Materials and Methods
Study Design
This study employed a cross-sectional design and included 106 patients diagnosed with UC who visited either the outpatient department or were hospitalized in the inpatient gastroenterology unit of our hospital between January 2023 and December 2024. To enhance reproducibility, we clarified that patients were recruited consecutively based on the availability of same-day clinical assessment and endoscopy. Data were collected through standardized questionnaires and electronic medical records, covering patients’ demographic information (gender, age, BMI), clinical characteristics, disease duration, treatment status, laboratory markers (CRP, ESR, etc)., endoscopic Mayo score (0–3), Simple Clinical Colitis Activity Index (SCCAI, 0–12), and the QIDS-SR16 self-rated depression scale. To ensure temporal alignment of assessments, SCCAI, laboratory tests, and QIDS-SR16 were administered within the same clinical visit, and for patients who underwent endoscopy, Mayo scoring was performed within ±7 days of questionnaire completion. Linear regression models were used to adjust for potential confounders, and restricted cubic spline (RCS) regression with four knots placed at the 5th, 35th, 65th, and 95th percentiles was performed to explore nonlinear associations. All analyses explicitly tested linearity assumptions, homoscedasticity, and normality of residuals. Missing data were removed using complete-case analysis, as missingness was <5%. This study adhered to the Declaration of Helsinki and was approved by the Ethics Committee of Beijing Friendship Hospital (Approval No.: 2022-P2-428-02). All patients provided written informed consent. Retrospective clinical data were processed under strict anonymization. This study was performed in accordance with the Declaration of Helsinki (as revised in 2013).
Study Population
Inclusion Criteria
(1) Age 18–70 years; (2) Confirmed UC diagnosis per the 2018 Beijing Consensus; (3) Ability and willingness to complete questionnaires and provide clinical information; (4) Stable disease control for comorbid diabetes, hepatitis B, HIV, or immune-related conditions; (5) No abdominal organ malignancy in the past 3 years.
Exclusion Criteria
(1) Age <18 or >70; (2) Unclear UC diagnosis; (3) Use of immunosuppressive drugs within the past year; (4) History of abdominal organ malignancy within 3 years; (5) Severe hepatic, renal, or hematologic dysfunction; (6) Poorly controlled chronic diseases or acute psychiatric instability affecting questionnaire validity.
Data Collection
Demographic and Clinical Information
Demographics (gender, age, height, weight) were extracted from electronic medical records.
Clinical Data
Included UC subtype, disease duration, medication exposure (5-ASA, corticosteroids, immunomodulators, biologics), previous psychiatric history, and socioeconomic indicators when available. Laboratory tests included CRP, ESR, CBC, ALT, AST, ALP, GGT, and albumin. Blood tests were performed on the same day as the questionnaires whenever possible, and always within 72 hours.
Endoscopic Assessment
Endoscopic activity was assessed using the Mayo score (0–3). For patients who had recent colonoscopy, only procedures performed within ±7 days of QIDS-SR16 administration were included. Mayo was treated as both: an ordinal variable (0–3) a categorical variable for subgroup analysis depending on analysis requirements.
Assessment of Depressive Symptoms
Depressive symptoms were evaluated using the QIDS-SR16 scale, containing 16 items scored 0–3 each. Total scores ranged 0–27, with higher scores indicating more severe depression.
Questionnaires were self-administered in a quiet environment and independently checked by trained research staff. Patients with incomplete questionnaires were excluded from analysis (complete-case approach).
Statistical Analysis
All analyses were conducted using R 4.2.2 (packages: rms, stats, psych) and SPSS 25.0. Continuous variables with normal distribution were expressed as mean ± SD and compared using t-tests; non-normal variables were expressed as median (IQR) and compared using Mann–Whitney U-tests. Categorical variables were analyzed using χ2-tests. Pearson correlation coefficients were used to examine linear associations, with r values explicitly reported. Multivariable linear regression models were used to assess the associations of SCCAI and Mayo scores with QIDS-SR16, adjusting for the following covariates: gender, age, permanent residence, smoking status, alcohol consumption, and BMI. Restricted cubic splines (RCS) with four knots were applied to test potential nonlinear relationships. Model diagnostics included: Residual normality tests; Homoscedasticity checks; Variance inflation factors; Adjusted R2 values. No multiple testing correction was applied due to the exploratory nature of the secondary analyses, which is acknowledged in the Discussion. A P-value <0.05 was considered statistically significant.
Quality Control
Research personnel were fixed throughout the study and underwent unified training on questionnaire administration and clinical data extraction. All investigators followed a standardized operating protocol to ensure consistency in timing, administration, and verification of questionnaires. Patient information was anonymized, and no identifiable data were disclosed (Tables 1–4).
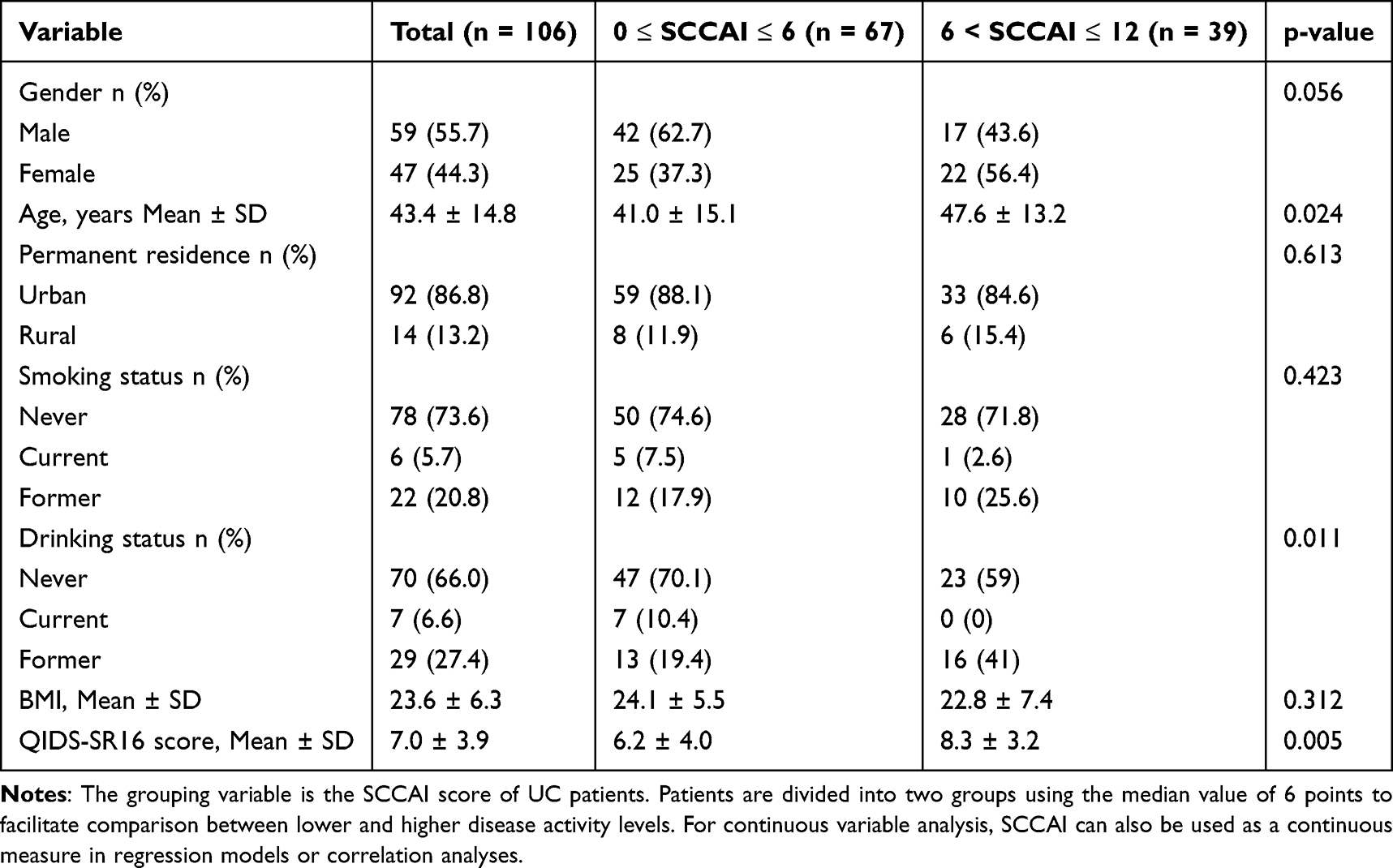 |
Table 1 Demographic Data of 106 UC Patients |
 |
Table 2 Multivariate Regression Analysis of SCCAI Scores and QIDS-SR16 Depression Scores in UC Patients |
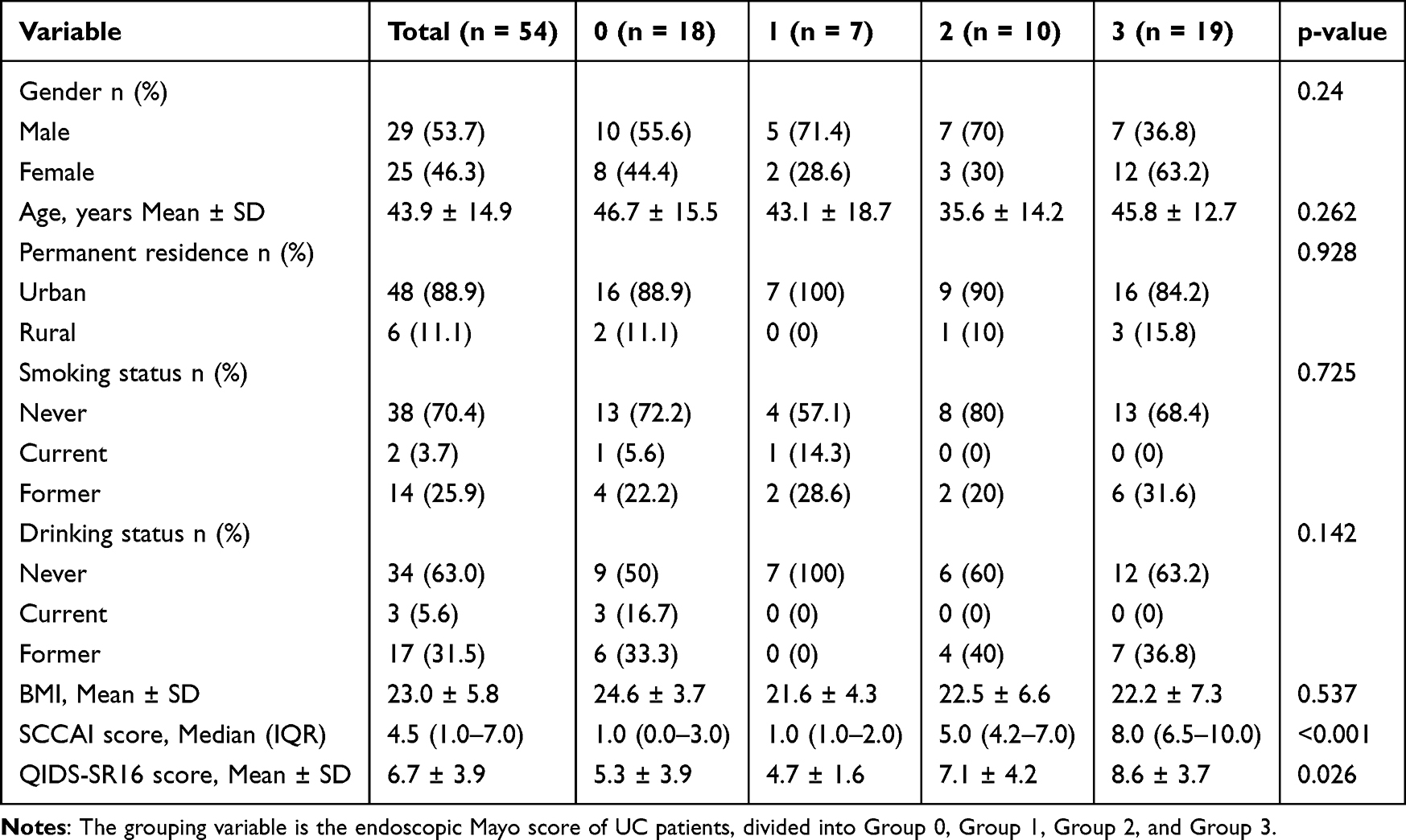 |
Table 3 Demographic Data of 54 UC Patients |
 |
Table 4 Multivariate Regression Analysis of Endoscopic Mayo Score and QIDS-SR16 Depression Scores in UC Patients |
Results
The results of this study are presented in two parts. The first part included 106 UC patients, comprising 59 males and 47 females, with a mean age of 43.4 years (range 18–76 years). All patients completed collection of basic information, SCCAI scores, and QIDS-SR16 depression scores. The second part, based on the first dataset, excluded patients without endoscopic results. Analysis was performed on the remaining 54 UC patients with Mayo endoscopic scores, including 29 males (53.7%) and 25 females (46.3%), with a mean age of 43.8 years (range 18–76 years). All patients completed collection of basic information, QIDS-SR16 depression scores, SCCAI scores, and Mayo scores.
Demographic and Clinical Characteristics of 106 UC Patients
As shown in Figure 1, the 106 UC patients were divided into two groups based on SCCAI scores: low (0–6) and high (7–12). Multiple indicators were compared between the two groups. To provide clarity and transparency, all analyses explicitly accounted for potential confounders, including gender, age, residence, smoking, alcohol consumption, and BMI, as pre-specified in the Methods section. Basic characteristics: Gender, residence, smoking, and BMI showed no significant differences between groups (p = 0.056, 0.613, 0.423, 0.312). Age: The 7–12 group had a significantly higher mean age than the 0–6 group (47.6 ± 13.2 vs 41.0 ± 15.1 years, p = 0.024). Alcohol consumption: Significant differences were observed between groups (p = 0.011), with a higher proportion of non-drinkers in the low SCCAI group. QIDS-SR16 depression score: The 7–12 group had a significantly higher mean QIDS-SR16 score than the 0–6 group (8.3 ± 3.2 vs 6.2 ± 4.0, p = 0.005). QIDS-SR16 scores range from 0–27 as per scale instructions, and figure annotations clarify this range. In summary, age, alcohol consumption, and QIDS-SR16 scores differed significantly across SCCAI groups, while gender, residence, smoking status, and BMI did not. These findings provide foundational data for further analyses.
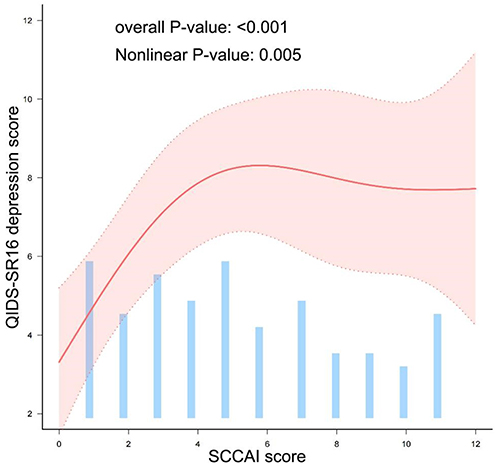 |
Figure 1 Restricted cubic spline analysis of QIDS-SR16 and SCCAI scores. Notes: The solid line represents the adjusted association between SCCAI and QIDS-SR16 scores. Shaded area indicates 95% confidence intervals. RCS model includes four knots located at the 5th, 35th, 65th, and 95th percentiles of SCCAI scores. Model adjusted for potential confounders: gender, age, permanent residence, smoking status, alcohol consumption, and BMI. Nonlinear P value = 0.005, indicating a significant nonlinear association. Sensitivity analyses excluding the SCCAI happiness item produced similar results, confirming robustness against potential item overlap. |
Relationship Between SCCAI Scores and QIDS-SR16 Depression Scores in 106 UC Patients
Linear regression analysis revealed a significant correlation between SCCAI and QIDS-SR16 scores. The unadjusted correlation coefficient was 0.36 (95% CI: 0.16–0.56, p = 0.001). After adjusting for potential confounders (gender, age, residence, smoking, alcohol consumption, BMI), the adjusted correlation coefficient was 0.41 (95% CI: 0.19–0.63, p < 0.001). Each 1-point increase in SCCAI corresponds to a 0.41-point increase in QIDS-SR16 (β = 0.41, 95% CI: 0.19–0.63, P < 0.001). Additionally, restricted cubic spline (RCS) regression with four knots (5th, 35th, 65th, 95th percentiles) confirmed a significant nonlinear relationship (nonlinear P = 0.005), suggesting that increases in SCCAI have a greater impact on depressive symptoms at lower SCCAI levels, with the effect stabilizing at higher scores. Sensitivity analysis excluding the SCCAI happiness item showed consistent results, indicating robustness against item overlap.
Demographic and Clinical Characteristics of 54 UC Patients with Mayo Scores
As shown in Figure 1, 54 UC patients were grouped by Mayo scores (0, 1, 2, 3). QIDS-SR16 scores: Significant differences were observed among Mayo groups (p = 0.026), with QIDS-SR16 scores tending to increase with higher Mayo scores. SCCAI scores: Differences among Mayo groups were highly significant (p < 0.001), with higher Mayo scores corresponding to higher SCCAI scores, confirming the internal consistency of clinical and endoscopic severity. Other factors: Age, gender, residence, smoking, alcohol consumption, and BMI showed no significant differences across Mayo groups (p = 0.24, 0.238, 0.931, 0.739, 0.138, 0.537).
Relationship Between Mayo Scores and QIDS-SR16 Depression Scores in 54 UC Patients
Linear regression analysis revealed a significant correlation between endoscopic Mayo scores and QIDS-SR16 scores. The unadjusted correlation coefficient was 1.17 (95% CI: 0.41–1.94, p = 0.004). After adjusting for potential confounders (gender, age, residence, smoking, alcohol consumption, BMI), the adjusted coefficient was 1.07 (95% CI: 0.24–1.9, p = 0.015). Each 1-point increase in Mayo score corresponds to a 1.07-point increase in QIDS-SR16, indicating that higher endoscopic severity is associated with more pronounced depressive symptoms. Given the small sample in some Mayo subgroups (eg, n=7 for Mayo 1), results should be interpreted cautiously, and sensitivity analyses using ordinal versus categorical modeling confirmed overall trends without overfitting.
Fitted Curve of SCCAI and QIDS-SR16 Depression Scores
Figure 1 shows the RCS-fitted relationship between SCCAI and QIDS-SR16 scores. Overall, QIDS-SR16 scores increased with SCCAI scores and then plateaued. Specifically, when SCCAI scores were 0–6, QIDS-SR16 scores increased markedly, peaking around an SCCAI score of 6; beyond 6, QIDS-SR16 scores fluctuated slightly but remained relatively stable Adjusted covariates included gender, age, residence, smoking, alcohol, and BMI. Confidence intervals are shown in Figure 1.
These findings indicate a significant nonlinear association between clinical disease activity and depressive symptoms in UC patients, with a more pronounced effect at lower SCCAI levels, providing evidence to guide mental health assessment in clinical practice.
Discussion
This study found that SCCAI scores and Mayo endoscopic severity scores in patients with UC were positively correlated with QIDS-SR16 depression scores, suggesting that higher disease activity is associated with more pronounced depressive symptoms.25 Both SCCAI and Mayo scores are commonly used tools for assessing UC activity and can effectively reflect patients’ clinical and endoscopic inflammatory status.26 Previous studies have shown that Mayo endoscopic scores are significantly associated with quality of life and psychological well-being, particularly during periods of active disease.27
The QIDS-SR16 is a reliable and sensitive tool for assessing depression, providing a comprehensive measure of symptom severity. Compared with traditional scales such as HADS and BDI, the use of QIDS-SR16 in chronic disease populations is increasing, capturing multidimensional aspects of depressive symptoms in greater detail.21 In this study, the QIDS-SR16 provided a standardized method to quantify depressive symptoms in UC patients, allowing for comparison across different levels of disease activity.
The biological basis of this correlation may involve the “bidirectional gut–brain axis” mechanism. On one hand, intestinal inflammation can promote proinflammatory cytokines such as IL-6 and TNF-α to cross the blood–brain barrier, inhibit hippocampal neurogenesis, and induce depressive-like behaviors.28 On the other hand, depression can activate the hypothalamic–pituitary–adrenal (HPA) axis, elevate cortisol levels, and promote Th17 cell differentiation in colonic mucosa, exacerbating inflammation.22 Furthermore, recent multi-omics and microbiome studies indicate that gut microbiota and their metabolites play a crucial role in regulating the gut–brain axis, influencing both inflammatory responses and neurotransmitter metabolism.24
Previous literature has reported a close relationship between UC disease activity and psychological health.29 However, this study further quantified the association using the QIDS-SR16 scale, representing an innovative approach. Studies combining SCCAI and Mayo scores with psychological assessment remain limited. By analyzing the relationship of QIDS-SR16 with both scoring systems, this study reinforces the clinical relevance of depressive symptoms in relation to disease activity. The Mayo score, focusing on endoscopic mucosal inflammation and assessed by professional endoscopists, offers high objectivity, whereas some studies rely more on subjective symptom scores, which may introduce bias.30
Our study also suggests a potential nonlinear threshold effect between SCCAI scores and depression risk: for SCCAI ≤ 6, depression risk increases linearly with score; for SCCAI > 6, the risk plateaus, which may relate to patient adaptation in severe disease.31 This finding highlights that the relationship between disease activity and depressive symptoms is not strictly proportional, underscoring the need for careful clinical evaluation. Future studies with larger samples and longitudinal follow-up are needed to validate these findings and explore the role of gut–brain axis-related biomarkers in UC patients with depression.32
This study contributes to a deeper understanding of the mental health status of UC patients and emphasizes the importance of routine depression screening in clinical practice. Depression is highly prevalent among patients with chronic diseases, and international guidelines recommend regular screening in high-risk populations for early identification and intervention.33 In practice, a two-step screening process using standardized tools such as the PHQ-9 has been shown to provide good sensitivity and specificity, improving depression detection rates.34 Routine psychological management should be integrated into UC disease activity assessment to achieve holistic patient care and reduce the negative impact of depression on disease progression and quality of life.35
By identifying high-risk patients, clinicians can implement targeted psychological interventions, including counseling, pharmacotherapy, or multidisciplinary management, thereby improving overall prognosis and quality of life in UC patients.36 Studies show that timely psychological intervention can alleviate depressive symptoms and reduce hospitalization and mortality rates in chronic disease populations.37,38 Importantly, integrating mental health assessment within UC management pathways provides opportunities for early referral and coordinated care, enhancing patient outcomes and adherence to treatment plans.
This study is relatively representative, including patients with varying disease courses and activity levels, and employed multivariable analysis to control for potential confounders, enhancing the reliability of the results. However, some limitations remain. First, patients were mainly recruited from tertiary care centers, which may introduce selection bias and limit applicability to mild cases.39 Second, the sample size was relatively small, which may affect external validity. Third, as a cross-sectional study, while significant correlations were observed, causal relationships between disease activity and depressive symptoms cannot be determined, and dynamic changes over time are difficult to capture. While widely recognized, scales such as PHQ-9 may require further validation across different cultural and socioeconomic contexts.40 Finally, this study focused only on UC patients, excluding other types of IBD. Future research should expand sample sizes, adopt longitudinal designs, and examine differences across populations (eg, ethnicity, socioeconomic status) to obtain more generalizable and causal conclusions, providing more precise guidance for individualized UC management.
Conclusion
This study demonstrates a significant positive association between disease activity, as measured by SCCAI and Mayo endoscopic scores, and depressive symptoms assessed by QIDS-SR16 in patients with ulcerative colitis. Higher disease activity is correlated with more pronounced depressive symptoms, with a potential nonlinear threshold effect observed for SCCAI scores. These findings highlight the importance of incorporating routine depression screening into UC management to facilitate timely detection and intervention, and emphasize the need for holistic patient care that addresses both physical and psychological aspects of the disease.
Given the cross-sectional design, causal relationships cannot be established. Future longitudinal studies with larger, more diverse populations are warranted to validate these findings, explore underlying mechanisms, and evaluate the impact of disease-modifying treatments and psychological interventions on depression risk in UC patients.
Ethics
Ethics approval number: 2022-P2-428-02. Medical Research Registration System registration number: MR-11-23-007533.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. Chunyan Jiang and Ye Zong are co-corresponding authors.
Disclosure
The authors declare no conflicts of interest. This study was funded by the National Key R&D Program (2023YFC2507300), with support covering study design, data collection, and analysis. The funding agency did not participate in data interpretation or manuscript writing and had no influence on the study outcomes.
References
1. Barberio B, Zamani M, Black CJ, et al. Prevalence of symptoms of anxiety and depression in patients with inflammatory bowel disease: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2021;6(5):359–10. doi:10.1016/S2468-1253(21)00014-5
2. Gao X, Tang Y, Lei N, et al. Symptoms of anxiety/depression is associated with more aggressive inflammatory bowel disease. Sci Rep. 2021;11(1):1440. doi:10.1038/s41598-021-81213-8
3. Dubinsky MC, Dotan I, Rubin DT, et al. Burden of comorbid anxiety and depression in patients with inflammatory bowel disease: a systematic literature review. Expert Rev Gastroenterol Hepatol. 2021;15(9):985–997. doi:10.1080/17474124.2021.1911644
4. Bisgaard TH, Poulsen G, Allin KH, et al. Longitudinal trajectories of anxiety, depression, and bipolar disorder in inflammatory bowel disease: a population-based cohort study. EClinicalMedicine. 2023;59:101986. doi:10.1016/j.eclinm.2023.101986
5. Tarar ZI, Zafar MU, Farooq U, et al. Burden of depression and anxiety among patients with inflammatory bowel disease: results of a nationwide analysis. Int J Colorectal Dis. 2022;37(2):313–321. doi:10.1007/s00384-021-04056-9
6. Al-Aamri H, Al-Huseini S, Chan MF, et al. Clinical predictors of depression among patients with inflammatory bowel diseases: a cross-sectional analytical study from Oman. Oman Med J. 2022;37(2):e352. doi:10.5001/omj.2022.48
7. Sciberras M, Karmiris K, Nascimento C, et al. Mental health, work presenteeism, and exercise in inflammatory bowel disease. J Crohns Colitis. 2022;16(8):1197–1201. doi:10.1093/ecco-jcc/jjac037
8. Bartocci B, Dal Buono A, Gabbiadini R, et al. Mental illnesses in inflammatory bowel diseases: mens sana in corpore sano. Medicina. 2023;59(4). doi:10.3390/medicina59040682
9. Fairbrass KM, Lovatt J, Barberio B, Yuan Y, Gracie DJ, Ford AC. Bidirectional brain-gut axis effects influence mood and prognosis in IBD: a systematic review and meta-analysis. Gut. 2022;71(9):1773–1780. doi:10.1136/gutjnl-2021-325985
10. Kochar B, Barnes EL, Long MD, et al. Depression is associated with more aggressive inflammatory bowel disease. Am J Gastroenterol. 2018;113(1):80–85. doi:10.1038/ajg.2017.423
11. Kim S, Lee S, Han K, et al. Depression and anxiety are associated with poor outcomes in patients with inflammatory bowel disease: a nationwide population-based cohort study in South Korea. Gen Hosp Psychiatry. 2023;81:68–75. doi:10.1016/j.genhosppsych.2023.01.015
12. Massironi S, Pigoni A, Vegni E, et al. The burden of psychiatric manifestations in inflammatory bowel diseases: a systematic review with meta-analysis. Inflamm Bowel Dis. 2025;31(5):1441–1459. doi:10.1093/ibd/izae206
13. Sheehan JL, Jordan AA, Newman KL, et al. Are depression and anxiety underdiagnosed in socially vulnerable patients with inflammatory bowel disease? Inflamm Bowel Dis. 2024;30(10):1696–1706. doi:10.1093/ibd/izad246
14. Seaton N, Hudson J, Harding S, et al. Do interventions for mood improve inflammatory biomarkers in inflammatory bowel disease?: a systematic review and meta-analysis. EBioMedicine. 2024;100:104910. doi:10.1016/j.ebiom.2023.104910
15. Ge L, Liu S, Li S, et al. Psychological stress in inflammatory bowel disease: psychoneuroimmunological insights into bidirectional gut-brain communications. Front Immunol. 2022;13:1016578. doi:10.3389/fimmu.2022.1016578
16. Golovics P, Gonczi L, Reinglass J. Patient reported outcomes, partial MAYO score and SCCAI are equally accurate in predicting mucosal healing in UC: preliminary results from a prospective study. J Crohn’s Colitis. 2020;14(Supplement_1):S613–S614. doi:10.1093/ecco-jcc/jjz203.901
17. Taleban S, Stewart KO, Li DK, et al. Clinical activity and quality of life indices are valid across ulcerative colitis but not Crohn’s disease phenotypes. Dig Dis Sci. 2016;61(9):2627–2635. doi:10.1007/s10620-016-4180-8
18. Golovics PA, Gonczi L, Reinglas J, et al. Sa466 patient reported outcomes, partial mayo score and sccai are equally accurate in predicting mucosal healing in UC: final results from a prospective study. Gastroenterology. 2021;160(6):
19. Bewtra M, Brensinger CM, Tomov VT, et al. An optimized patient-reported ulcerative colitis disease activity measure derived from the Mayo score and the simple clinical colitis activity index. Inflamm Bowel Dis. 2014;20(6):1070–1078. doi:10.1097/MIB.0000000000000053
20. Walsh AJ, Ghosh A, Brain AO, et al. Comparing disease activity indices in ulcerative colitis. J Crohns Colitis. 2014;8(4):318–325. doi:10.1016/j.crohns.2013.09.010
21. Rush AJ, Trivedi MH, Ibrahim HM, et al. The 16-item quick inventory of depressive symptomatology (QIDS), clinician rating (QIDS-C), and self-report (QIDS-SR): a psychometric evaluation in patients with chronic major depression. Biol Psychiatry. 2003;54(5):573–583. doi:10.1016/s0006-3223(02)01866-8
22. Dragasevic S, Stankovic B, Kotur N, et al. Psychological distress is associated with inflammatory bowel disease manifestation and mucosal inflammation. Inflamm Bowel Dis. 2025;31(6):1567–1573. doi:10.1093/ibd/izae180
23. Gracie DJ, Guthrie EA, Hamlin PJ, et al. Bi-directionality of brain-gut interactions in patients with inflammatory bowel disease. Gastroenterology. 2018;154(6):1635–1646.e3. doi:10.1053/j.gastro.2018.01.027
24. Tiles-Sar N, Neuser J, De Sordi D, et al. Psychological interventions for treatment of inflammatory bowel disease. Cochrane Database Syst Rev. 2025;4(4):CD006913. doi:10.1002/14651858.CD006913.pub3
25. Gao K, Su M, Sweet J, et al. Correlation between depression/anxiety symptom severity and quality of life in patients with major depressive disorder or bipolar disorder. J Affect Disord. 2019;244:9–15. doi:10.1016/j.jad.2018.09.063
26. Golovics P, Gonczi L, Reinglass J, et al. P364 patient reported outcomes, partial MAYO score and SCCAI are equally accurate in predicting mucosal healing in UC: final results form a prospective study. J Crohn’s Colitis. 2021;15(Supplement_1):S381–S382. doi:10.1093/ecco-jcc/jjab076.488
27. Aniwan S, Bruining DH, Park SH, et al. The combination of patient-reported clinical symptoms and an endoscopic score correlates well with health-related quality of life in patients with ulcerative colitis. J Clin Med. 2019;8(8):1171. doi:10.3390/jcm8081171
28. Craig CF, Filippone RT, Stavely R, et al. Neuroinflammation as an etiological trigger for depression comorbid with inflammatory bowel disease. J Neuroinflammation. 2022;19(1):4. doi:10.1186/s12974-021-02354-1
29. Abu Sneineh A, Haj Ali S, Al-Masri A, et al. Prevalence of anxiety and depressive symptoms in ulcerative colitis patients in Jordan and its relationship to patient-reported disease activity. Sci Rep. 2022;12(1):7682. doi:10.1038/s41598-022-11911-4
30. Mohammed Vashist N, Samaan M, Mosli MH, et al. Endoscopic scoring indices for evaluation of disease activity in ulcerative colitis. Cochrane Database Syst Rev. 2018;1(1):CD011450. doi:10.1002/14651858.CD011450.pub2
31. Ghosh S, Sensky T, Casellas F, et al. A global, prospective, observational study measuring disease burden and suffering in patients with ulcerative colitis using the pictorial representation of illness and self-measure tool. J Crohns Colitis. 2021;15(2):228–237. doi:10.1093/ecco-jcc/jjaa159
32. Scaldaferri F, D’onofrio AM, Calia R, et al. Gut microbiota signatures are associated with psychopathological profiles in patients with ulcerative colitis: results from an italian tertiary IBD center. Inflamm Bowel Dis. 2023;29(11):1805–1818. doi:10.1093/ibd/izad091
33. Costantini L, Pasquarella C, Odone A, et al. Screening for depression in primary care with Patient Health Questionnaire-9 (PHQ-9): a systematic review. J Affect Disord. 2021;279:473–483. doi:10.1016/j.jad.2020.09.131
34. Dano S, Lan HH, Macanovic S, et al. Two-step screening for depressive symptoms in patients treated with kidney replacement therapies: a cross-sectional analysis. Nephrol Dial Transplant. 2023;38(5):1318–1326. doi:10.1093/ndt/gfac262
35. Califf RM, Wong C, Doraiswamy PM, et al. Importance of social determinants in screening for depression. J Gen Intern Med. 2022;37(11):2736–2743. doi:10.1007/s11606-021-06957-5
36. Jedel S, Beck T, Swanson G, et al. Mindfulness intervention decreases frequency and severity of flares in inactive ulcerative colitis patients: results of a Phase II, randomized, placebo-controlled trial. Inflamm Bowel Dis. 2022;28(12):1872–1892. doi:10.1093/ibd/izac036
37. Oh SJ, Choi CH, Jung SA, et al. Anxiety and depression are associated with poor long-term quality of life in moderate-to-severe ulcerative colitis: results of a 3-year longitudinal study of the MOSAIK cohort. Gut Liver. 2025;19(2):253–264. doi:10.5009/gnl240146
38. Schlee C, Uecker C, Bauer N, et al. Multimodal stress reduction and lifestyle modification program for patients with ulcerative colitis: a qualitative study. BMC Complement Med Ther. 2022;22(1):60. doi:10.1186/s12906-021-03478-w
39. Kundu R, Shi X, Morrison J, et al. A framework for understanding selection bias in real-world healthcare data. J R Stat Soc Ser a Stat Soc. 2024;187(3):606–635. doi:10.1093/jrsssa/qnae039
40. Carroll HA, Hook K, Perez O, et al. Establishing reliability and validity for mental health screening instruments in resource-constrained settings: systematic review of the PHQ-9 and key recommendations. Psychiatry Res. 2020;291:113236. doi:10.1016/j.psychres.2020.113236
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.