Back to Journals » Clinical Interventions in Aging » Volume 20
The Safety and Effectiveness of Multi-Segment Cortical Bone Trajectory Screws in Adult Degenerative Scoliosis with Stenosis Among the Elderly: Minimum 5-year Follow-up Study
Authors Wang J ![]() , Ding Z, Liu Y
, Ding Z, Liu Y ![]() , Hai Y
, Hai Y ![]()
Received 10 March 2025
Accepted for publication 19 July 2025
Published 28 July 2025 Volume 2025:20 Pages 1125—1135
DOI https://doi.org/10.2147/CIA.S527306
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Zhi-Ying Wu
Jie Wang,1,* Zihao Ding,1,* Yuzeng Liu,1 Yong Hai1– 4
1Department of Orthopedic Surgery, Beijing Chao-Yang Hospital, Capital Medical University, Beijing, 100020, People’s Republic of China; 2Joint Laboratory for Research & Treatment of Spinal Cord Injury in Spinal Deformity, Capital Medical University, Beijing, 100069, People’s Republic of China; 3Laboratory for Clinical Medicine, Capital Medical University, Beijing, 100069, People’s Republic of China; 4Clinical Center for Spinal Deformity, Capital Medical University, Beijing, 100069, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yuzeng Liu, Email [email protected] Yong Hai, Email [email protected]
Purpose: To evaluate the long-term efficacy and safety of multi-segment cortical bone trajectory screws for treating mild adult degenerative scoliosis with stenosis among the elderly.
Patients and Methods: From January 2018 to December 2019, a total of 41 patients of mild adult degenerative scoliosis with stenosis underwent posterior lumbar decompression, bone graft fusion, and internal fixation, which were retrospectively divided into pedicle screw (PS) group and cortical bone trajectory (CBT) screw group according to different internal fixation methods. The operation time, intraoperative blood loss, immobilization, and length of hospital stay were compared between the two groups. The visual analog score (VAS) of low back and leg pain, Oswestry disability index (ODI), Cobb angle, lumbar lordosis (LL) angle, apex vertebral translation (AVT), coronal balance distance (CBD) and sagittal vertical axis (SVA) were compared between the two groups preoperatively and 6 months, 1 year, 5 years postoperatively. Perioperative and follow-up complications were observed.
Results: The CBT group was superior to PS group in operation time, intraoperative blood loss, immobilization, length of hospital stay (P< 0.05). The low back VAS and ODI in CBT group were significantly lower than those in PS group at 6 months, 1 year and 5 years postoperatively (P< 0.05). The leg VAS in CBT group was lower than PS group at 5 years postoperatively (P< 0.05). The incidence of screw loosening and adjacent segment disease 5 years postoperatively in CBT group was significantly lower than that in PS group (P< 0.05).
Conclusion: Multi-segment cortical bone trajectory screws is a safe and effective treatment option for mild adult degenerative scoliosis with stenosis among the elderly. This technique features miniinvasive trauma and quick recovery, which might lead to improved long-term quality of life and a reduction in screw loosening and adjacent segment disease rates.
Keywords: cortical bone trajectory screw, adult degenerative scoliosis, stenosis, elderly
Introduction
Adult degenerative scoliosis (ADS) with stenosis is a challenging disease among the elderly in spinal surgery. Its pathological features include disc degeneration, articular process hyperplasia, and coronal/sagittal imbalance, often leading to intractable low back pain and neurological dysfunction.1,2 Posterior Lumbar Interbody Fusion (PLIF) with pedicle screw (PS) fixation has become the conventional procedure for patients who fail conservative treatment; PLIF can directly decompress spinal canal, relieve nerve compression, improve nerve symptoms, and provide good spinal stability with relatively high fusion rate, but PLIF requires extensive dissection of paravertebral muscles, causing greater damage to paravertebral muscles and greater damage to posterior ligament complex structures; transforaminal lumbar interbody fusion (TLIF) has relatively little damage to the posterior structure and preserves part of the posterior ligament complex, which is beneficial to maintaining the stability of the spinal column after operation, reducing the interference to the nerve tissue in the spinal canal and reducing the risk of nerve injury; however, TLIF has limited operating space for severe intervertebral foraminal stenosis cases, and the decompression effect may be affected to some extent.3–8 However, osteoporosis and biomechanical interference with multi-level fixation in elderly patients may lead to complications such as screw loosening and adjacent segment degeneration (ASD), especially at the lumbar fixation level.9,10
In recent years, cortical bone trajectory (CBT) screw technology has provided a new idea for spinal fixation by innovating the angle of screw implantation and enhancing the anchoring force with high-density cortical bone at the pedicle-vertebral junction.11 Basic research have confirmed that CBT screws significantly improve the pullout resistance of bone-screw interface compared with traditional PS screws.11–13 The entry point of CBT screws is located in the pars interarticularis, which can minimize the destruction of facet joints and thus reduce the incidence of ASD. Moreover, its medial path can reduce the extent of paravertebral muscle dissection, which aligns with accelerated rehabilitation surgery.14 Currently, CBT is mostly used in single-level lumbar degenerative diseases. However, there is no systematic report on whether CBT can maintain scoliosis correction and reduce the risk of complications in multi-level fixation of ADS with stenosis.
This study is the first to compare the clinical efficacy of multi-level CBT screws and PS fixation combined with PLIF (L1-5 or L2-5) in ADS with stenosis among the elderly. Through retrospective analysis, the correction of scoliosis parameters, functional scores, postoperative complications, etc, between the two groups of patients were compared, providing a better solution for ADS with stenosis requiring multi-level fixation.
Materials and Methods
General Information
A retrospective analysis of clinical data of 19 patients (CBT group) who received CBT screw treatment from January 2018 to December 2019 due to ADS with stenosis was conducted. Twenty-two patients (PS group) who received PS treatment due to ADS with stenosis at the same period were selected as a control group. Baseline data of Age, sex, course of disease, bone mineral density, body mass index (BMI), Lenke-Silva type II–III, fusion levels, and follow-up time of the PS group matched with the CBT group (Table 1).
 |
Table 1 Comparison of Baseline Data Between Two Groups |
Inclusion criteria: 1. The diagnosis of ADS with stenosis is explicit; 2. Age>65 years; 3. Cobb angle<20°, vertebral rotation≤II degree (Nash-Moe method); 4. Scoliosis in the lumbar segment; 5. Lenke-Silva type II–III; 6. Horizontal L5 in the coronal plane and the lowest instrumented vertebra is L5; 7. Follow-up for at least 5 years.
Exclusion criteria: 1. Patients with previous spinal surgery; 2. Patients with spinal infection and spinal tumor; 3. Patients who only received decompression at the responsible lumbar segment without internal fixation; 4. Patients who could not tolerate general anesthesia surgery due to severe underlying diseases; 5. Patients with incomplete follow-up data.
Surgical Procedures
After general anesthesia, the patients were placed prone on the operating bed, and the posterior median approach was taken to strip bilateral paravertebral muscles while preserving the posterior ligament complex structure. Select appropriate screws according to preoperative measurement and intraoperative results, PS screws are generally 6.0mm/4.5cm, and CBT screws are generally 5.5mm/3.5cm. The decompression range of the two groups included the inferior articular process, part of the lamina, and part of the superior articular process at multiple responsible levels. For the PS group, the superior articular process was exposed to the outer edge of the articular process, and the herringbone ridge was selected as the entry point for bilateral fixation using the traditional PS internal fixation system. In the CBT group, the fusion segment was not exposed completely, only dissected to the outer edge of the isthmus and fixed bilaterally with a CBT screw fixation system under fluoroscopic guidance. The screw insertion point of the CBT screw was more medial and inferior than that of the traditional PS screw, and it was close to the isthmus (Figures 1–5). Local autogenous bone was obtained during decompression and cut for intervertebral fusion. Polyetheretherketone cages were routinely inserted in several decompression segments. After asymmetrical compression and de-rotation on both sides of the scoliosis, the screw-rod system was locked. Finally, the incision was rinsed, a negative pressure drain was placed under the unilateral paravertebral muscle, and the suture was performed layer by layer.
 |
Figure 1 Illustrative case of adult degenerative scoliosis with stenosis (CBT group). Preoperative X-ray: mild scoliosis, lumbar multi-level disc space narrowing (a and b); preoperative CT: Multi-level lumbar disc degeneration (c); preoperative MRI: multi-level lumbar spinal stenosis (L2/3, L3/4, L4/5), bilateral ligamentum flavum hyperplasia and hypertrophy pressing dural sac, bilateral facet joint hyperplasia and cohesion (d and e); X-ray immediately postoperatively: internal fixation system firmly in place (f and g); CT immediately postoperatively: CBT screws in good position (h); X-ray 5 years postoperatively: scoliosis not aggravated (I and j); CT 5 years postoperatively: “corticalization” phenomenon around screws (red arrows), no loosening of screws (k); MRI 5 years postoperatively: adequate spinal canal decompression, no radiographic ASD occur (l–n). |
 |
Figure 2 Illustrative case of adult degenerative scoliosis with stenosis (CBT group). Preoperative X-ray: mild scoliosis, lumbar multi-level disc space stenosis, osteophyte hyperplasia (a and b); preoperative CT: Lumbar multi-level intervertebral space height decreased, degeneration is obvious (c); preoperative MRI: multi-level stenosis (L2/3, L3/4, L4/5), cauda equina redundancy, dural sac compression obvious (d); X-ray immediately postoperatively: internal fixation system firmly in place (e and f); CT immediately postoperatively: CBT screws in good position (g and h); X-ray 5 years postoperatively: scoliosis not aggravated (i and j); CT 5 years postoperatively: “corticalization” phenomenon around screws (red arrows), no loosening of screws (k); MRI 5 years postoperatively: no radiographic ASD occur (l-n). |
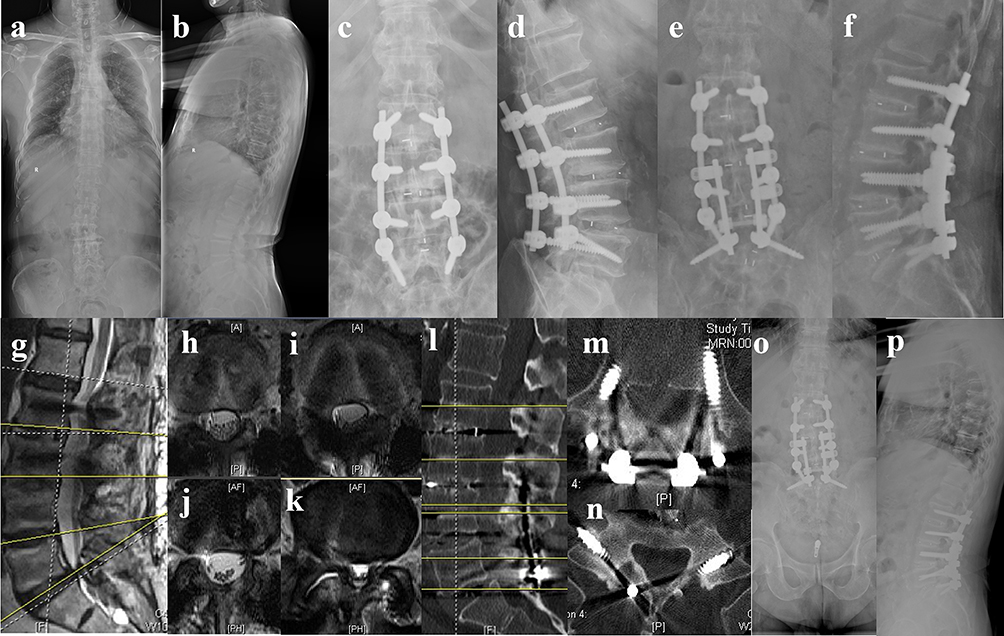 |
Figure 3 Illustrative case of adult degenerative scoliosis with stenosis (PS group). Preoperative X-ray: mild scoliosis, lumbar multi-level disc space stenosis (a and b); X-ray immediately postoperatively: internal fixation system firmly in place (c and d); X-ray immediately after revision surgery: screws in good position (e and f); MRI 5 years postoperatively: spinal stenosis at L5/S1 (g-k); CT immediately after revision surgery: screws in good position (l-n); X-ray 1 year after revision surgery: scoliosis not aggravated (o and p). |
 |
Figure 4 Pedicle screw placement (a); cortical bone trajectory screw placement (b). |
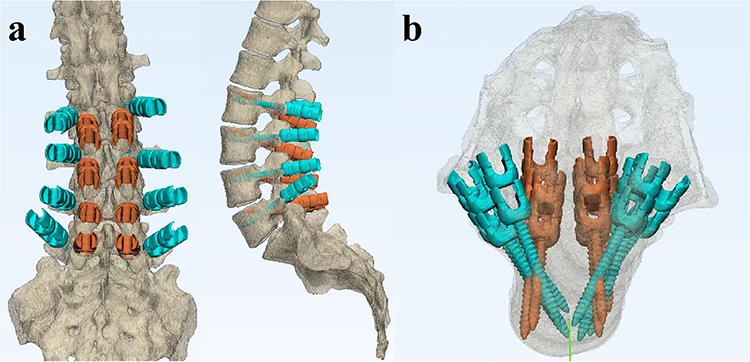 |
Figure 5 Comparison of two screws in anteroposterior and lateral position (a); Comparison of two screws in axial position (b). |
Postoperative Treatment
The patients in both groups received regular dressing changes, an intravenous infusion of cefuroxime sodium for 3 days to prevent incision infection, and regular anti-osteoporosis treatment. When the drainage volume was less than 50mL, and the drainage fluid was light blood, the drainage tube was removed, and the brace was worn for walking. The brace was strictly worn for 3 months. The lumbar spine activity gradually increased after discharge, and regular outpatient reexamination was performed.
Observation Index
Operation time, intraoperative blood loss, immobilization, and length of hospital stay were observed. The visual analog score (VAS) of low back and leg pain, Oswestry disability index (ODI), Cobb angle, lumbar lordosis (LL) angle, apex vertebral translation (AVT), coronal balance distance (CBD), and sagittal vertical axis (SVA) were observed preoperatively and 6 months, 1 year, and 5 years postoperatively. Perioperative and follow-up complications were observed.
Statistical Analysis
SPSS22.0 statistical software was used for analysis. Qualitative data were described by number of cases and percentage (%). The chi-square test/Fisher exact test was used to compare group differences. Quantitative data conforming to normal distribution were expressed by mean±standard deviation (Mean±SD). Independent sample t-test was used for comparison between groups. P<0.05 was regarded as a statistically significant difference.
Results
Comparison of Perioperative Indicators Between Two Groups
Table 2 and Figure 6 show that the CBT group was superior to the PS group in operation time, intraoperative blood loss, immobilization, and length of hospital stay, and the difference was statistically significant (P<0.05).
 |
Table 2 Comparison of Operation Time, Blood Loss, Immobilization and Length of Hospital Stay Between Two Groups |
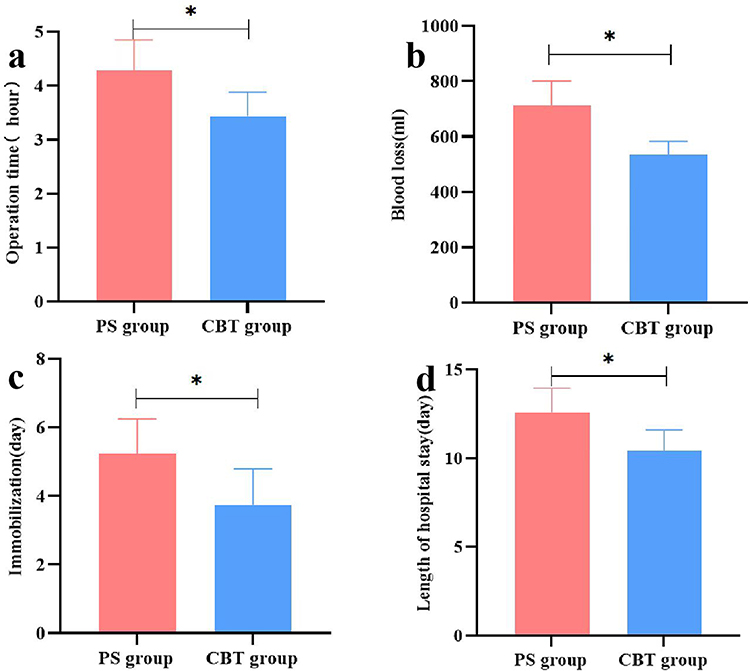 |
Figure 6 Comparison of operation time (a), blood loss (b), immobilization (c), and length of hospital stay (d) between two groups. Note:*P<0.05. |
Comparison of Functional Scores Between Two Groups
Table 3 and Figure 7 show that the low back VAS and ODI in the CBT group were significantly lower than those in the PS group at 6 months, 1 year, and 5 years postoperatively (P<0.05). There was no significant difference in leg VAS between the two groups preoperatively, 6 months, and 1 year postoperatively (P>0.05), but the CBT group was significantly lower than the PS group 5 years postoperatively (P<0.05).
 |
Table 3 Comparison of Low Back VAS, Leg VAS, ODI Between Two Groups |
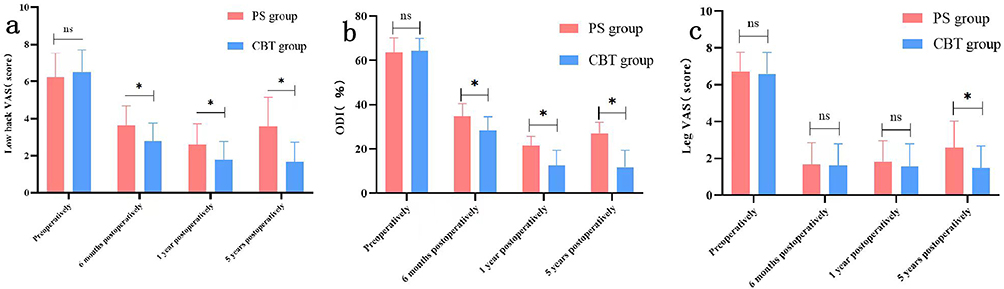 |
Figure 7 Comparison of low back VAS (a), ODI (b), and leg VAS (c) between two groups preoperatively and postoperatively. Note:*P<0.05; ns-the difference was not statistically significant. |
Comparison of the Parameters of Scoliosis Between Two Groups
Table 4 shows that there was no significant difference in Cobb angle, lumbar lordosis (LL) angle, apex vertebral translation (AVT), coronal balance distance (CBD), and sagittal vertical axis (SVA) between the two groups preoperatively and during follow-up (P>0.05).
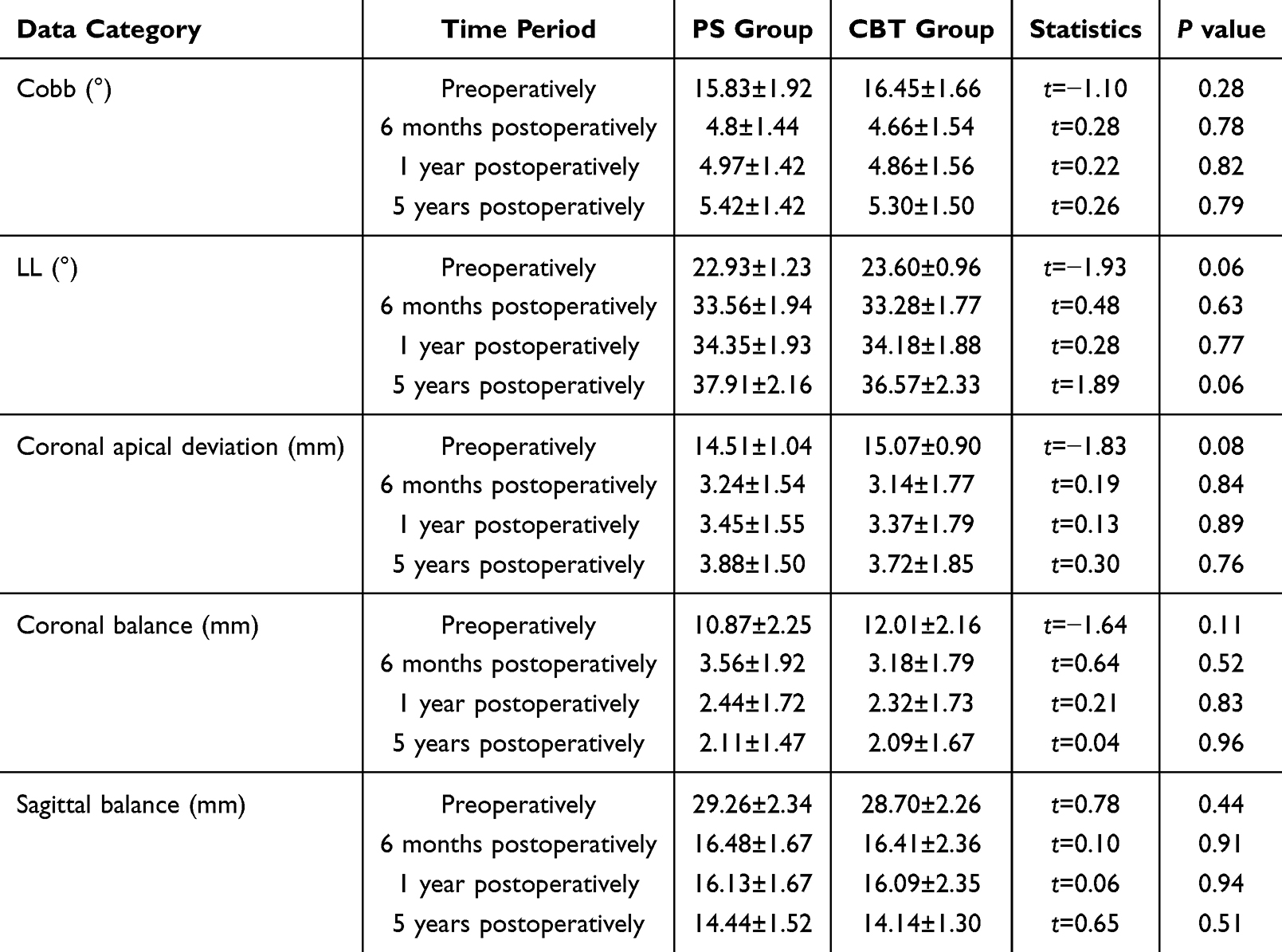 |
Table 4 Comparison of Cobb, LL, Coronal Apical Deviation, Coronal Balance, Sagittal Balance Between Two Groups |
Comparison of Complications Between Two Groups at 5-year Follow-up
Table 5 shows no significant difference in internal fixation fracture, cerebrospinal fluid leak, or cage settlement between the two groups during follow-up (P>0.05). The incidence of screw loosening and ASD in the CBT group was significantly lower than that in the PS group, and the difference was statistically significant (P<0.05).
 |
Table 5 Comparison of the Incidence of Complications Between Two Groups |
Discussion
The surgical goals of ADS with stenosis are to relieve nerve compression, stabilize the decompression segment, restore coronal and sagittal balance, and prevent compensatory deformity of adjacent motor segments.15–17
In recent years, the application of CBT screws in senile degenerative spinal diseases has gradually attracted attention.18–21 This study compared the efficacy of CBT and PS screws in ADS patients with LSS and found that the CBT group was significantly better than the PS group in terms of operation time, intraoperative blood loss, immobilization, and length of hospital stay. The low back VAS and ODI in the CBT group were significantly lower than those in the PS group at 6 months, 1 year, and 5 years postoperatively. The leg VAS in the CBT group was lower than that in the PS group at 5 years postoperatively, which may be related to the higher incidence of ASD in PS group. There were also no significant differences in scoliosis parameters between the two groups preoperatively and during follow-up. These results suggest that in ADS with stenosis, multi-level CBT screw fixation of the lumbar spine can achieve clinical efficacy comparable to PS fixation and shows potential advantages in reducing surgical trauma and accelerating recovery. CBT may be an effective alternative to PS in multi-level fixation, especially in cases with osteoporosis or requiring minimally invasive intervention.
The “cohesive” screw placement path of CBT reduces the dissection of paravertebral muscles, consistent with the reduction in intraoperative bleeding observed in this study. The CBT technique significantly reduced the risk of postoperative muscle atrophy by making smaller incisions and preserving polyfidus muscle attachment points, which explains the superior ODI at 6 months, 1 year, and 5 years postoperatively in the CBT group in this study.
ADS patients often have osteoporosis, and CBT’s cortical bone anchoring properties are more advantageous in this population.22,23 CBT utilizes the mechanical properties of cortical bone in high-density areas to achieve stability by placing screws along the medial-lateral axis of the pedicle.24–26 Biomechanical studies showed that CBT had significantly higher pullout resistance than PS, especially for patients with decreased bone mineral density.27 The rate of screw loosening in the CBT group was significantly lower than that in the PS group in this study, consistent with long-term follow-up results in most studies.18,28 During this more than 5-year follow-up period, no screw loosening occurred in the CBT group. The “Corticalization” phenomenon (Figure 1) was observed around the CBT in the CBT group, which may be related to the change of lumbar stress and the compensation of the human body itself. We suspect that the low rate of screw loosening is related to the advantage of CBT itself and to the “corticalization” phenomenon of screws, which greatly increases screw retention and allows better maintenance of decompression and correction. In the future, we will explain this “corticalization” phenomenon by increasing the sample size and follow-up time.
Because CBT screws were less resistant to rotation than PS, we included patients with ADS who had Cobb angle within 20°and vertebral body rotation within II degrees. Follow-up results showed that the CBT screw could achieve the same correction effect as PS for mild ADS. Lenke-Silva classification is instructive for the treatment of degenerative scoliosis.29 The degenerative scoliosis patients included in this study were Lenke-Silva type II and III, and neither CBT nor PS required fixation to the thoracic spine. In both groups, the fixation level was lumbar (L2-5 or L1-5), which made it easier to observe proximal and distal ASD. The use of CBT screws in degenerative lumbar diseases has been shown to reduce the incidence of ASD compared with PS, which is inseparable from the biomechanical and minimally invasive advantages of CBT screws.30–32 However, previous studies have focused on short-level lumbar fixation. We first explored the use of long-level CBT in ADS, the results of which are consistent with previous studies of short-level lumbar fixation and can still significantly reduce the incidence of ASD. This provides a reference for future surgical treatment of mild ADS with stenosis.
Screw reinforcement materials are commonly used in clinical practice to enhance the fixation effect of pedicle screw and reduce the probability of screw loosening; common screw reinforcement materials include Polymethyl Methacrylate (PMMA), calcium phosphate, calcium sulfate, etc; pedicle screw with reinforcement materials can improve the axial pullout force of screws, especially in osteoporotic vertebral bodies.33–35
Multi-level CBT screw fixation is a safe and effective treatment option for ADS with stenosis among the elderly, which has minimally invasive advantages and good biomechanical properties, especially suitable for osteoporosis patients. However, retrospective study and small sample size are limitations of this study, randomized controlled studies with larger sample sizes and longer follow-ups are needed to verify its long-term efficacy further.
Conclusion
Multi-segment cortical bone trajectory screws is a safe and effective option for mild adult degenerative scoliosis with stenosis among the elderly. This approach is less invasive and promotes faster recovery in this retrospective study, which can enhance long-term quality of life and decrease the risk of screw loosening and ASD. The clinical application time of CBT screws is still short, and large-scale prospective randomized controlled trials and long-term follow-up are lacking to confirm the safety and effectiveness of this surgical method.
Abbreviations
PS, pedicle screw; CBT, cortical bone trajectory; VAS, visual analog score; ODI, Oswestry Disability Index; LL, lumbar lordosis; AVT, apex vertebral translation; CBD, coronal balance distance; SVA, sagittal vertical axis; ASD, adjacent segment disease; ADS, adult degenerative scoliosis; PLIF, posterior lumbar interbody fusion; TLIF, transforaminal lumbar interbody fusion; PMMA, Polymethyl Methacrylate.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Ethics Approval and Informed Consent
The Ethics Committee of the Beijing Chaoyang Hospital of Capital Medical University approved the study, and written informed consent was obtained from participants prior to data collection. This study was conducted in accordance with the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Clinical Research Incubation Program of Beijing Chao-Yang Hospital (CYFH202316).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wang G, Cui X, Jiang Z, et al. Evaluation and surgical management of adult degenerative scoliosis associated with lumbar stenosis. Medicine. 2016;95(15):e3394. doi:10.1097/MD.0000000000003394
2. Asada T, Simon CZ, Singh N, et al. Limited improvement with minimally invasive lumbar decompression alone for degenerative scoliosis with cobb angle over 20°: the impact of decompression location. Spine. 2024;49(15):1037–1045. doi:10.1097/BRS.0000000000004968
3. Bai H, Li Y, Liu C, et al. Surgical management of degenerative lumbar scoliosis associated with spinal stenosis: does the PI-LL matter? Spine. 2020;45(15):1047–1054. doi:10.1097/BRS.0000000000003465
4. Li Y, Zhu Y, Ou Y, et al. Effectiveness of short-segment fixation versus long-segment fixation for degenerative scoliosis with cobb angle 20°~40°: a retrospective observational study. Med Sci Monit. 2020;26:e923656. doi:10.12659/MSM.923656
5. Ramieri A, Miscusi M, Domenicucci M, et al. Surgical management of coronal and sagittal imbalance of the spine without PSO: a multicentric cohort study on compensated adult degenerative deformities. Eur Spine J. 2017;26(Suppl 4):442–449. doi:10.1007/s00586-017-5042-6
6. Phillips FM, Isaacs RE, Rodgers WB, et al. Adult degenerative scoliosis treated with XLIF: clinical and radiographical results of a prospective multicenter study with 24-month follow-up. Spine. 2013;38(21):1853–1861. doi:10.1097/BRS.0b013e3182a43f0b
7. Jun L, Zou T, Wei JJ, et al. Comparison of the effects between oblique lateral interbody fusion (OLIF) and minimally invasive transforaminal interbody fusion (MIS-TLIF) in the treatment of adult degenerative lumbar scoliosis. J Orthop. 2024;58:58–65. doi:10.1016/j.jor.2024.06.035
8. Li X, Chen X, Wang Y, et al. Early outcomes of oblique lateral interbody fusion with posterior fixation versus posterior interbody fusion with fixation for treating adult degenerative scoliosis. J Orthop Surg Res. 2023;18(1):873. doi:10.1186/s13018-023-04363-7
9. Xu F, Zhou S, Zou D, et al. The relationship between S1 screw loosening and postoperative outcome in patients with degenerative lumbar scoliosis. BMC Musculoskelet Disord. 2022;23(1):186. doi:10.1186/s12891-022-05107-0
10. Wang H, Sun Z, Wang L, et al. Proximal fusion level above first coronal reverse vertebrae: an essential factor decreasing the risk of adjacent segment degeneration in degenerative lumbar scoliosis. Global Spine J. 2023;13(1):149–155. doi:10.1177/2192568221994082
11. Santoni BG, Hynes RA, McGilvray KC, et al. Cortical bone trajectory for lumbar pedicle screws. Spine J. 2009;9(5):366–373. doi:10.1016/j.spinee.2008.07.008
12. Chung TT, Chu CL, Hueng DY, et al. A parametric investigation on traditional and cortical bone trajectory screws for transpedicular fixation. BMC Musculoskelet Disord. 2022;23(1):612. doi:10.1186/s12891-022-05477-5
13. Schleifenbaum S, Vogl AC, Heilmann R, et al. Biomechanical comparative study of midline cortical vs. traditional pedicle screw trajectory in osteoporotic bone. BMC Musculoskelet Disord. 2023;24(1):395. doi:10.1186/s12891-023-06502-x
14. Hu JN, Yang XF, Li CM, et al. Comparison of cortical bone trajectory versus pedicle screw techniques in lumbar fusion surgery: a meta-analysis. Medicine. 2019;98(33):e16751. doi:10.1097/MD.0000000000016751
15. Kurra S, Lavelle WF, Silverstein MP, et al. Long-term outcomes of transforaminal lumbar interbody fusion in patients with spinal stenosis and degenerative scoliosis. Spine J. 2018;18(6):1014–1021. doi:10.1016/j.spinee.2017.10.063
16. Kleinstueck FS, Fekete TF, Jeszenszky D, et al. Adult degenerative scoliosis: comparison of patient-rated outcome after three different surgical treatments. Eur Spine J. 2016;25(8):2649–2656. doi:10.1007/s00586-014-3484-7
17. Di Silvestre M, Lolli F, Bakaloudis G. Degenerative lumbar scoliosis in elderly patients: dynamic stabilization without fusion versus posterior instrumented fusion. Spine J. 2014;14(1):1–10. doi:10.1016/j.spinee.2012.10.023
18. Ding H, Hai Y, Liu Y, et al. Cortical trajectory fixation versus traditional pedicle-screw fixation in the treatment of lumbar degenerative patients with osteoporosis: a prospective randomized controlled trial. Clin Interv Aging. 2022;17:175–184. doi:10.2147/CIA.S349533
19. Jarvers JS, Schleifenbaum S, Pfeifle C, et al. Comparison of three different screw trajectories in osteoporotic vertebrae: a biomechanical investigation. BMC Musculoskelet Disord. 2021;22(1):418. doi:10.1186/s12891-021-04254-0
20. Rosinski AA, Mittal A, Odeh K, et al. Alternatives to traditional pedicle screws for posterior fixation of the degenerative lumbar spine. JBJS Rev. 2021;9(7). doi:10.2106/JBJS.RVW.20.00177
21. Zhang Y, Hai Y, Li Y, et al. A nomogram for predicting screw loosening after single-level posterior lumbar interbody fusion utilizing cortical bone trajectory screw: a minimum 2-year follow-up study. Front Surg. 2022;9:950129. doi:10.3389/fsurg.2022.950129
22. Zhang RJ, Li HM, Gao H, et al. Cortical bone trajectory screws used to save failed traditional trajectory screws in the osteoporotic lumbar spine and vice versa: a human cadaveric biomechanical study. J Neurosurg Spine. 2019;30(6):759–766. doi:10.3171/2018.12.SPINE18970
23. Wang Y, Kahaer A, Maimaiti A, et al. Complication, fusion, and revision rate in the lumbar cortical bone trajectory and pedicle screw fixation techniques: a systematic review and meta-analysis. J Orthop Surg Res. 2023;18(1):382. doi:10.1186/s13018-023-03820-7
24. Phan K, Ramachandran V, Tran TM, et al. Systematic review of cortical bone trajectory versus pedicle screw techniques for lumbosacral spine fusion. J Spine Surg. 2017;3(4):679–688. doi:10.21037/jss.2017.11.03
25. Wang J, He X, Sun T. Comparative clinical efficacy and safety of cortical bone trajectory screw fixation and traditional pedicle screw fixation in posterior lumbar fusion: a systematic review and meta-analysis. Eur Spine J. 2019;28(7):1678–1689. doi:10.1007/s00586-019-05999-y
26. Zhang R, Gao H, Li H, et al. Differences in bone mineral density of trajectory between lumbar cortical and traditional pedicle screws. J Orthop Surg Res. 2019;14(1):128. doi:10.1186/s13018-019-1169-y
27. Matsukawa K, Yato Y. Lumbar pedicle screw fixation with cortical bone trajectory: a review from anatomical and biomechanical standpoints. Spine Surg Relat Res. 2017;1(4):164–173. doi:10.22603/ssrr.1.2017-0006
28. Guo S, Zhu K, Yan MJ, et al. Cortical bone trajectory screws in the treatment of lumbar degenerative disc disease in patients with osteoporosis. World J Clin Cases. 2022;10(36):13179–13188. doi:10.12998/wjcc.v10.i36.13179
29. Silva FE, Lenke LG. Adult degenerative scoliosis: evaluation and management. Neurosurg Focus. 2010;28(3):E1. doi:10.3171/2010.1.FOCUS09271
30. Han B, Ding H, Hai Y, et al. May the midline lumbar interbody fusion (MIDLIF) prevent the early radiographic adjacent segment degeneration? A minimum 3-year follow-up comparative study of MIDLIF in L4/5 with cortical bone trajectory screw versus traditional pedicle screw fixation. BMC Musculoskelet Disord. 2022;23(1):480. doi:10.1186/s12891-022-05363-0
31. Li Y, Li Y, Liu Y, et al. Changes in paraspinal muscles and facet joints after minimally invasive posterior lumbar interbody fusion using the cortical bone trajectory technique: a prospective study. Pain Res Manag. 2022;2022:2690291. doi:10.1155/2022/2690291
32. Sakaura H, Miwa T, Yamashita T, et al. Posterior lumbar interbody fusion with cortical bone trajectory screw fixation versus posterior lumbar interbody fusion using traditional pedicle screw fixation for degenerative lumbar spondylolisthesis: a comparative study. J Neurosurg Spine. 2016;25(5):591–595. doi:10.3171/2016.3.SPINE151525
33. Elder BD, Lo SF, Holmes C, et al. The biomechanics of pedicle screw augmentation with cement. Spine J. 2015;15(6):1432–1445. doi:10.1016/j.spinee.2015.03.016
34. Schmoelz W, Heinrichs CH, Schmidt S, et al. Timing of PMMA cement application for pedicle screw augmentation affects screw Anchorage. Eur Spine J. 2017;26(11):2883–2890. doi:10.1007/s00586-017-5053-3
35. Schulze M, Riesenbeck O, Vordemvenne T, et al. Complex biomechanical properties of non-augmented and augmented pedicle screws in human vertebrae with reduced bone density. BMC Musculoskelet Disord. 2020;21(1):151. doi:10.1186/s12891-020-3158-z
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.