Back to Journals » Psychology Research and Behavior Management » Volume 10
The role of secure attachment, empathic self-efficacy, and stress perception in causal beliefs related to mental illness – a cross-cultural study: Italy versus Israel
Authors Mannarini S ![]() , Reikher A, Shani S, Shani-Zinovich I
, Reikher A, Shani S, Shani-Zinovich I
Received 3 April 2017
Accepted for publication 4 August 2017
Published 9 October 2017 Volume 2017:10 Pages 313—321
DOI https://doi.org/10.2147/PRBM.S138683
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Stefania Mannarini,1 Alisa Reikher,1 Sharon Shani,1 Inbal Shani-Zinovich2
1Department of Philosophy, Sociology, Education and Applied Psychology, Interdepartmental Center for Family Research, University of Padova, Padova, Italy; 2Department of Counseling and Human Development, Faculty of Education, University of Haifa, Mount Carmel, Haifa, Israel
Background: Research suggests that “mental illness etiological beliefs” and attitudes toward mentally ill people are significantly related; it has also been demonstrated that adult attachment style and empathic self-efficacy affect such attitudes. Moreover, community or regional culture has a significant impact on etiology beliefs and attitudes toward the mentally sick.
Materials and methods: We carried out this study in Italy and Israel among psychology students to compare two cultures in regards to causal beliefs of mental disorders and the roles that specific variables, such as secure attachment, empathic self-efficacy, and stress, play in etiological beliefs. The participants (N=305) were students who belonged to two universities: Padua (N=183) and Haifa (N=122). The Many Facet Rasch Model (MFRM) was applied in a cross-cultural perspective to analyze the differential functioning of specific etiological beliefs in relation to the above mentioned variables; the effect of gender and religious beliefs was also entered in the MFRM.
Results: The two cultures reacted differently to the biogenetic and psychosocial causal explanations of mental disorders: Israeli students endorsed the biogenetic causal beliefs model more frequently than the Italians. Among other findings, concerning the biogenetic model, the Italian students were predominantly males, who declared to be religious and reported lower levels of secure attachment than Israelis. On the other hand, the Israeli students who manifested a preference toward the biogenetic explanation were mostly females, who declared not to be religious and who manifested higher levels of secure attachment than the Italians.
Conclusion: This article is expected to contribute to the improvement of the understanding of general public’s etiological beliefs of mental illness. Similarities and differences between the two cultures, Israel and Italy, have been highlighted on the basis of the MFRM analysis. The effect that interpersonal relations, such as attachment style, perceived empathy, and stress, have on etiological beliefs was also investigated.
Keywords: mental illness, stigma, etiological beliefs, attachment, self-efficacy, stress, Italy, Israel, attitudes, empathy
Introduction
“Mental disorders etiological beliefs” have been extensively studied and results have shown that biological and psychosocial factors are the most frequently endorsed types of causes.1–6 Researchers have also suggested that cultural characteristics have a significant effect on etiological beliefs7–10 and that knowledge of mental illness within a population has a preponderant impact on how individuals perceive such disorders.11 In most cases, results showed that individuals perceive mental patients as dangerous and uncontrollable; as a consequence, a discriminating behavior is often manifested against mentally sick people.12–15 The relationship between etiological beliefs and discriminating attitudes toward people with mental illness has been a long-lasting discussion in the literature and research has been carried out in different countries.16–24 Specific characteristics related to causal beliefs in the stigmatization of mentally ill people, such as prejudice, have been studied;21 it was found that people’s dominant feeling is that psychiatric disorders lead to unpredictable behaviors, irresponsibility, and loss of control. This impression is often a prejudice due to a negative stereotype, since different studies demonstrated that the relationship between being a mentally ill patient and being violent does not exist.24 A study conducted in three countries, Germany, Russia, and Mongolia, has analyzed the relationship between mental disorders causal beliefs (MDCBs) and social distance toward mentally ill people.1 Despite the different cultural backgrounds, the results have shown similar trends concerning the attribution of depression and schizophrenia to psychological causes, such as acute stress due to life events. The biological causes, such as brain disease and heredity, are less often indicated for both pathologies, in particular for depression. It is also found that endorsing biological factors as causes of mental disorders is associated with a greater desire for social distance. Stigmatization and expectations typical of specific community cultures have been also demonstrated to affect how people respond to health problems.25,26 Schomerus et al27 analyzed 17 representative population studies that examine aspects of the stigma of mental illnesses. Seven surveys were carried out in Europe, five in North America, three in New Zealand, and one each in Brazil and Ethiopia. The results suggested that a significant effect on how people who belong to different cultures perceive mental disorders and tend to stigmatize them exists in particular regarding variables such as blaming, perceived unpredictability, dangerousness, emotional reactions, and desire for distance. Pescosolido et al28 studied the relations between causal beliefs and attitudes toward mental illness in different cultures and confirm the effect that culture can have on those relations. The results evidence as well that, although the popularity of the biological model has been increasing recently, holding a neurobiological conception of mental disorders increases the likelihood of support for treatment, but generally does not improve the attitude toward the mentally sick. Schomerus et al have also demonstrated that stigmatization is a cluster of different attitudes and that they are differently attributed to different mental disorders.27 Cheng29 in his study on Asian Americans’ and European Americans’ stigma level in response to biological and social explanations of depression, concluded that, although genetics plays a role in the development of mental illness and in particular depression, giving special importance to a social expectation for the origin of depression may help to reduce stigma mainly for Asian Americans. In this perspective, among other research, Mannarini and Boffo’s study4 with Italian students suggests that schizophrenia is definitely attributed to biogenetic causes, whereas participants’ beliefs about anxiety, depression, and bulimia split up between a psychosocial etiology and an interaction of biogenetic and psychosocial factors. As far as alcohol and drug addictions are concerned, the participants’ beliefs distributed almost equally in relation to three causal beliefs categories: psychosocial, biopsychosocial, and biogenetic. In the same study, MDCBs are also evaluated in relation to mental disease treatments,30 where the majority of participants declare that the best treatment for schizophrenia should follow a medical approach; regarding anxiety, depression, bulimia, and alcohol and drug addiction with similar probability values, they recommend a psychological, a medical, and an integrated treatment approach. Studies have also been conducted on specific interpersonal variables which might impact on stigma, such as empathy and adult attachment.31 Although empathy is a construct difficult to be defined, research suggests that it may be a predictor of stigma.31–33 The role of attachment in the relationship between empathy and stigma has also been analyzed;30 Britton and Fuendeling34 have noted that it is in particular a secure attachment style which is related to the capacity of recognizing others’ needs. Among other variables, stress has assumed an important place in many studies on stigmatization and its impact on interpersonal relationships has been analyzed in the past and in recent years.35,36 As Eisenberg et al point out a person’s ability to regulate one’s own emotions has an important role in social interactions; emotional regulation capacity increases the ability to experience empathy. Research demonstrates that emotional distress includes emotional responses, such as anxiety or discomfort, which might affect negatively the capacity to recognize the condition and the needs of others.
People who are frequently anxious tend to feel insecure, express hostility, be aggressive, and experience communication difficulties.36
Aims
The present study aims to deepen the understanding of individuals’ causal beliefs and attitudes regarding mental disorders, and to further improve the knowledge about the impact that cultural characteristics might have on etiological beliefs among people who belong to two cultures, Italy and Israel.
The justification for choosing variables such as secure attachment, empathic self-efficacy, and stress perception is found in the nature of the individual’s relation with the others and with people with mental illness in particular.37,38 Such relation seems to be multifaceted and composed of many processes which interact and are characterized by discriminating attitudes and behaviors, more specifically by confidence when facing others,39 by the capacity of perceiving the impact that one’s own efficacy can have on others,40 by being able to manifest one’s own feeling when stressed in particular situations.41 The definition of a structure characterized by the above mentioned variables describes the relation between mental disorder causal beliefs and the above mentioned constructs helping to better understand specific situations which might conduct to stigmatizing attitudes and behaviors. Italy and Israel are compared in this study.4,42,43
Hypotheses of differences between the participants’ responses that belong to the two countries are expected due to social events and daily situations that people experience in those cultures. Regarding Israel, while analyzing the problem of mental disorder stigmatization, the study by Tal et al42 discusses specific deliberations and suggestions to face such problems in a society which is particularly complex from the historical, cultural, and also religious points of view. Further, result from Gelkopf et al43 reported the prevalence of post-traumatic stress disorders among people with severe mental illness in Israel. As far as Italy is concerned, the national survey by Munizza et al44 analyzes public beliefs and attitudes toward mental disorders discussing the problem of stigmatization in the cultural and social context typical of the Italian regions.
In this study, when referring to the causal beliefs system, biogenetic and psychosocial causal attributions are hypothesized to be the two poles of a continuum, as identified in previous research.3,21 In line with Webb et al’s study,31 a relation is then hypothesized between causal explanations of mental illness constructs and secure attachment measures; hypotheses of associations of causal belief constructs with empathic self-efficacy and stress perception measures are also formulated. The importance of gender45 and of religious beliefs46 as demonstrated in the literature is also suggested when accounting for the participants’ attributes in the analysis. Holzinger et al45 in their review, on gender differences in public beliefs and attitudes about mental disorder in Western countries, demonstrated that women seem to favor psychosocial conceptualizations of mental illness more than men and, consequently, they recommend nonmedical sources of help and endorse psychotherapy. As far as religion is concerned, Wesselman et al46 in their study on religious beliefs about mental illness and social support preferences, observed that participants who declared to be religious, besides indicating biogenetic causes and medical treatments, predominantly also indicated spiritual causes and preference for giving spiritual support to the mentally ill.
Following these hypotheses, a latent structure is expected to represent the relations of MDCB constructs with empathy, attachment, stress, gender, and religious beliefs, in a cross-cultural perspective.
Materials and methods
Participants
This study made use of a convenient sample involving 305 participants, including psychology students from the University of Padua, Italy (N=183) and from the University of Haifa, Israel (N=122). As far as the Italian students were concerned, the mean age was 24.38, 65% were female, 16% declared to be religious, and 63% declared to have been in contact with the mentally ill. The Israeli students’ mean age was 24.35, 58% were female, 17% declared to be religious, and 69% affirmed to have experienced direct contact with a mentally ill person.
The project was approved by the Ethical Committee for Psychological Research of the University of Padua (protocol number 1734). The participants’ informed consent for confidential data treatment was part of the questionnaire package, and all participants signed this consent. The authorization of Haifa University Staff involved in this study was also obtained.
Instruments
MDCBs scale
In order to collect data in relation to specific constructs typical of causal beliefs related to mental illness from psychology students both in Italy and in Israel, the MDCB scale3 was chosen for the following main reasons: 1) the scale has been recently validated with psychology students; 2) it allows us to assess both biogenetic and psychosocial causal beliefs toward mental illness in general; 3) it is a practical instrument where the biogenetic and psychosocial causal attributions are demonstrated to be the two poles of a continuum. The scale consists of 30 items, where 13 items describe specific biological-genetic causal beliefs constructs and the 17 remaining items describe the psychosocial beliefs constructs. Examples of item contents for the biological-genetic causal belief constructs and for the psychosocial causal belief ones as they were elaborated in the MDCB are “The kind of nervous system you are born with has little to do with the possibility that you become or not a psychotic” and “A social environment lacking of future perspective could be a fertile ground for the onset of mental illness”, respectively.
The MDCB is a five-point Likert-type scale. High scores indicate a tendency to endorse biological-genetic causal beliefs. In order to be applied to Israeli psychology students, it was translated into Hebrew, adopting the back translation procedure. Internal consistency was calculated for the Israeli participants as 0.86.
Attachment style questionnaire (ASQ)
The ASQ39,47 consists of 40 items rated on an agreement Likert-type scale. On the basis of studies conducted by Mannarini and Boffo,39 the five original subscales converged into three main attachment constructs: confidence (6 items; feeling secure and self-confident), avoidance (17 items; discomfort with closeness and relationships as secondary), and anxiety (14 items; need for approval and preoccupation with relationships). In this study, only the confidence subscale was used. For the Israeli students, it was translated into Hebrew, adopting the back translation procedure. Internal consistency was calculated for the Israeli participants to be 0.84.
Perceived empathic self-efficacy (PESE) scale
This scale40,48 was developed to assess the individual’s perception of the impact that efficacy can have on the others, which means it was devised to assess the individual’s perceived empathic ability. The scale includes 12 items to be graded on a five-level Likert-type scale. High scores reflect the perception of a positive impact of self-efficacy. The scale was translated into Hebrew, adopting the back translation procedure. The alpha coefficient was 0.83.
Perceived stress scale (PSS)
The PSS41 consists of 12 items and its purpose is to examine the extent to which the individual judges his/her life as being heavily stressed in particular situations, and refers to feeling stressed in recent times. The questions are evaluated on a four-level Likert-type scale. High score reflects a high level of stress. The reliability coefficient in the original research was 0.85. The scale was translated into Hebrew, adopting the back translation procedure. The reliability coefficient tested in this study was 0.87.
Data analysis
According to the mono-dimensionality assumption of Rasch modeling, the Many Facet Rasch Model (MFRM)49 was applied in this study, not only to estimate latent trait parameters for persons and causal beliefs items as measured by the MDCB scale, but also to model a structure which allowed us to take into account more complex situations, such as the interactions of causal beliefs items with the participants’ cultures, gender, and religious beliefs, and also the interactions with different levels of secure attachment, empathic self-efficacy, and stress perception.
To do so at a formal level, besides the two parameters for persons and items, parameters for the two cultures (Italy and Israel), for gender, for religious belief, for secure attachment, for empathy, and for stress were introduced in the model. Before incorporation into the model, the variables secure attachment, empathy, and stress, and their distributions were categorized on the basis of three percentile levels: low (≤33%), medium (between 33% and 66%), high (>66%). After estimating the parameters, concerning the control fit evaluation of the parameter measures, the many-facet program reports two fit statistics for each measure, the mean square outfit statistic and the mean square infit statistic, which describe how much the data fit the model requirements.50 A value within the range of 0.70–1.30 indicates a satisfactory fit of the empirical data to the model.51 In the program, a chi-square statistic is also calculated for each parameter to verify whether its categories or levels are significantly different, that is, whether they measure different aspects of that specific variable or not. As it has already been pointed out, the many-facets program can also check for interactions between the model parameters.50 In this study, the interaction analyses were intended to detect the differential functioning of each causal beliefs item in relation to all the other variables. The MFRM program allowed, within the characteristics of the Student’s t distribution, to compare Italy and Israel, genders, different religious beliefs, and different levels of the other variables, for each item. Before presenting the results, it is noteworthy that all measures are located on a continuum (latent trait) which represents the etiological beliefs from the psychosocial (low negative measures) model to the biomedical one (high positive measures), where the mean value is 0.00.
Results
Person and item
The data showed a mean of −0.36 and a standard error (SE) of 0.27 for the person measures. The infit and outfit statistics presented satisfactory values, both being equal to 1.00. The range for the person measures was from −2.80 to 1.62 and the corresponding range for the SE values was 0.25–0.32. The average negative value showed that participants’ responses tended in general toward the psychosocial pole of the MDCBs latent dimension. All the item measures showed a good fit to the model, with infit and outfit statistics values in the range 0.70–1.30, confirming the solidity of the MDCBs3 dimension. Internal consistency assessed by the Cronbach coefficient was 0.87.
Italy and Israel
Both Italian and Israeli measures, −0.30 (SE =0.02) and 0.30 (SE =0.02) respectively, had a good fit (between 0.89 and 1.18). Italian and Israeli responses differed significantly (chi-square =374.6, df =1, p=0.00), and since the Israeli students presented a higher mean than the Italians, it showed that the Israeli students tended toward the biogenetic causal beliefs model more than the Italians.
Secure attachment, empathic self-efficacy, and stress perception
All three levels, high, medium, and low, of the secure attachment measures, 0.24 (SE =0.03), −0.04 (SE =0.02), and −0.20 (SE =0.03) respectively, had a good fit (between 0.84 and 1.13). The causal beliefs related to mental illness at the three levels of secure attachment differed significantly (chi-square =131.1, df =2, p=0.00), showing that persons with high levels of secure attachment preferred the biogenetic model to explain the origin of mental disorders. As far as empathic self-efficacy was concerned, as measured by the PESE scale, the three levels, high, medium, and low, −0.08 (SE =0.03), 0.02 (SE =0.03), and 0.06 (SE =0.03) respectively, had a good fit (between 0.92 and 1.15). The three levels differed significantly (chi-square =13.5, df =2, p=0.00), showing that persons with high levels of empathic self-efficacy endorsed preferably (−0.08) a psychosocial model to explain the origin of mental disorders. Considering the stress levels, high, medium, and low, as measured by the PSS, all measures, −0.08 (SE =0.03), −0.24 (SE =0.02), and 0.32 (SE =0.03) respectively, had a good fit (between 0.99 and 1.02). The three levels differed significantly (chi-square =249.3, df =2, p=0.00), showing that persons with low levels of stress perception preferred a biogenetic model to explain the origin of mental health problems.
Gender and religious belief
Both males’ and females’ measures, −0.13 (SE =0.02) and 0.13 (SE =0.02) respectively, had a good fit (between 0.94 and 1.11). Male and female responses differed significantly (chi-square =70.8, df =1, p=0.00), showing that females tended toward the biogenetic causal beliefs model more than males. As far as religious beliefs were concerned, both religious and nonreligious students’ measures, 0.29 (SE =0.02) and −0.29 (SE =0.02) respectively, had a good fit (between 0.96 and 1.06). Religious and nonreligious students’ responses differed significantly (chi-square =349.3, df =1, p=0.00), showing that religious students tended toward the biogenetic causal beliefs model more than nonreligious students.
In conclusion, considering all the variables entered in the MFRM, the following profile emerged from the participants’ responses: Italian and Israeli students’ MDCBs differed, namely a tendency of the Israelis’ beliefs toward the biogenetic model is noted; not distinguishing the Italian from the Israeli participants, in general the biogenetic model was endorsed preferentially by females, with a religious belief, with high levels of secure attachment, with low levels of perceived empathy, and with low levels of stress. Considering the psychosocial model, this was endorsed preferentially by males with low levels of secure attachment, high levels of empathic self-efficacy, and high levels of stress.
Italians versus Israelis regarding gender, religious beliefs, secure attachment, perceived empathy, and stress
In order to compare the two cultures in regards to the variables entered in the model, the MFRM program was run separately for Italians and Israelis. Etiological belief measures and SE values were then obtained for each category and level of each variable. The two cultures’ measures were then compared, namely contrast measures were calculated and, by means of the Student’s t distribution, their validity was tested. Table 1 presents the measures as they are distributed on the MDCBs latent dimension for Italians and Israelis, relative to gender, religious beliefs, secure attachment, perceived empathy, and stress together with contrast measures. For illustrative purpose, for each contrast value, the content of an item typical of that contrast result is also presented.
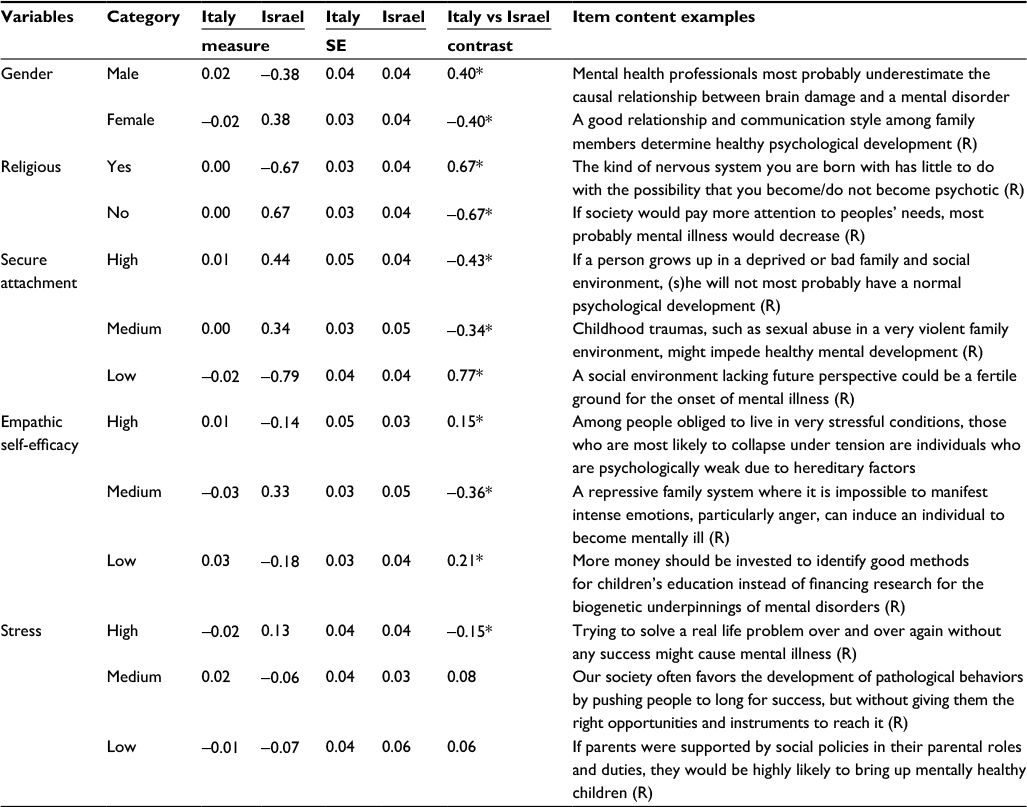 | Table 1 Etiological belief measures: all participants, Italy and Israel Notes: *p<0.001. (R) represents a reversed item. A positive contrast value means that the Italians attributed mental disorders to biogenetic causes more often than the Israelis. A negative contrast value means that the Israelis attributed mental disorders to biogenetic causes more often than the Italians. Abbreviation: SE, standard error. |
In Table 1, as far as Italian students are concerned, and recalling that, according to the MFRM analysis, the mean value for the estimated measures is 0.00, the profile which emerged is characterized by values very close to the mean for all variables. Considering a few values located slightly above the mean toward the biogenetic model, the following profile can be outlined: males (0.02), with a high level of secure attachment (0.01), with a rather low level of empathy (0.03), and with a medium level of stress (0.02). Israeli students showed more defined and well characterized measures than Italians for most of the variables; a profile toward the biogenetic model can be drawn as follows: females (0.38), without a specific religious belief (0.67), with a high/medium level of secure attachment (0.44, 0.34), with a medium level of perceived empathy (0.33), and with a high level of stress (0.13). In Table 1, the contrast measures describe the difference between the Italian and the Israeli measures. A positive contrast measure means that Italians attributed mental disorders to biogenetic causes more often than Israelis. On the contrary, a negative contrast means that Israelis attributed mental disorders to biogenetic causes more often than Italians. There are five positive contrast values out of the 11 significant ones, showing that Italian males (0.40), with a religious belief (0.67), with a low level of secure attachment (0.77), and with both high and low levels of perceived empathy (0.15, 0.21) endorsed the biogenetic model more often than the Israelis. Instead, Israeli females (−0.40), with no specific religious belief (−0.67), with high and medium levels of secure attachment (−0.43, −0.34), with a medium level of perceived empathy (−0.36), and with a high level of stress (−0.15) chose the biogenetic model more often than the Italians. Italians and Israelis did not show any significant contrast in relation to medium and low levels of stress, being in both cases, very close to the mean value (0.08, 0.06).
As anticipated, the MFRM program can also check for interactions between the model parameters.42 In this study, interaction analyses were performed in order to verify the differential functioning of each mental disorder causal belief item regarding Italian students versus Israeli students, in relation to all the variables. To do so, within the characteristics of the Student’s t distribution, Italy versus Israel was compared regarding all the variables. Results showed that 27 out of the 30 MDCB items were significantly (p<0.05) affected by culture; namely, they showed differential functioning when Italian students were compared with the Israelis. To represent some significant examples, in Table 1, specific item contents are presented for each contrast value.
Discussion
According to the general objective of this study, the latent trait analysis (MFRM)50 evidenced interpretable results related to the role that gender, religious belief, secure attachment, empathic self-efficacy, and stress perception play on Italian and Israeli students’ causal beliefs related to mental illness as measured by the MDCBs scale.3 In summary, according to the hypothesis, a latent structure emerged that represents the relations among the variables entered in the MFRM in a cross-cultural perspective. The analyses evidenced the following main results.
The average measure of the participants’ responses to the MDCB items tended in general (N=305) toward the psychosocial model to explain the mental illness etiology, whereas Italian (N=183) and Israeli (N=122) responses differed significantly, showing that the Israeli students endorsed the biogenetic causal beliefs model more frequently than the Italians. Item contents such as “The cause of most of people’s psychological problems is situated in the brain”, “Some people are born with a kind of emotional instability that makes it easy for them to become mentally disturbed” and “Most of the people who suffer from psychological problems are born with some psychological deficiency”, represent the biogenetic model preferred by the Israeli students. Meyerstein52 presents a Jewish perspective on causal beliefs and clinical work by examining underlying values and attitudes of Israeli people that relate to mental health and illness. In that study, common symptoms and also family issues that have roots in culture are explored and people’s beliefs about mental illness causes, stigma, and clinical work are considered from both the psychosocial and medical points of view. Results show that the medical point of view is often privileged by the respondents. Meyerstein52 also dedicated specific attention to some special communities in Israel and found that also the spiritual perspective occupies a relevant space to explain the etiology of mental illness.
Considering gender, females tended toward the biogenetic causal beliefs model more than males. However, this result does not seem to be largely against the endorsement of biogenetic causal explanations, since in many studies no gender differences have been observed.45
As far as religion was concerned, religious students tended toward the biogenetic causal beliefs model more than nonreligious students.46
In general, individuals with high levels of secure attachment preferred the biogenetic model to the psychosocial one in order to explain the origin of mental disorders. In other words, a biogenetic explanation, which does not imply any social or psychological responsibility, seems to characterize persons who feel self-confident, comfortable, and not preoccupied with interpersonal relationships. This result is accompanied by low levels of perceived empathic ability, that is, the individual perceives oneself as rather inefficient regarding the others. As referred to MDCBs, feeling self-confident with interpersonal relationships in general does not mean believing in his/her own capacity to affect the others. These results do not seem to fall in line with the findings of Webb et al31 which evidence a positive relation between fearful attachment and low levels of empathy. Webb et al31 suggest that attachment style may influence the relationship between empathy and discriminating attitudes, in a way that adults who are fearfully attached do not seek personal relationships with others and would feel less empathic toward somebody who is demonstrating socially inappropriate behaviors.
Persons who do not feel particularly stressed preferred a biogenetic model to explain the origin of mental health problems, excluding the psychosocial implications of mental disorders. A majority endorsed sentences such as “Some people are born mentally unstable and are doomed to spend part of their life in mental health care institutions”, “Mental health professionals most probably underestimate the causal relation between a brain damage and a mental disorder”, “Some people are born with a biologically based tendency to present a certain psychological disorder, which then becomes manifest during their development”. These results shed new light on other studies’ findings which show that emotional distress includes emotional responses, such as anxiety and discomfort, which might influence the capacity to recognize others needs and social implications.35,36
Results of the analysis conducted separately for Italians and Israelis show that Italian students’ measures describe a profile characterized by values very close to the mean for all variables; both biogenetic and psychosocial models as measured by the MDCB questions are not very clearly specified. However, Israeli students’ results evidence a much clearer profile through the variables toward the biogenetic explanation of the mental disorders etiology. In order to better understand the analogies and the differences between Italian and Israeli measures, contrast values were calculated and their statistical significance was tested. As shown in Table 1, the contrast values associated with gender, religious belief, and attachment style were particularly significant, allowing a better understanding of the main differences between the two cultures, namely that the Italian students who endorsed the biogenetic model were males, who declared to be religious, and reported lower levels of secure attachment than Israelis. On the contrary, the Israeli students who manifested a preference toward the biogenetic explanation were females, with no specific religious belief, and who manifested higher levels of secure attachment than the Italians.
Conclusion
The results of this study represent a contribution to the discussion on MDCBs and on specific interpersonal relationship variables, together with participants’ gender and religious beliefs in a cross-cultural perspective. This research, conducted at a latent trait level, finds space among a large number of other studies on the same issues, in part confirming their findings, but also showing some different aspects, in particular regarding the relations between interpersonal variables such as attachment style, perceived empathy, and stress. In order to better understand the contribution that this study represents and to consider new perspectives for future research, it is worth mentioning, among others, a particularly significant study conducted recently by Pescosolido53 in which the author reports on the general population’s attitudes, behavioral dispositions, and MDCBs that targeted stigma in the past, and discusses the implications this issue has at present; new research lines for future studies and intervention efforts are indicated. Considering the limits of the present study, further studies should be carried out at a population level, that take into consideration the effect that interpersonal relationship variables, gender, different levels of age, and cultural levels have on the individual’s understanding of mental illness.
According to Pescosolido’s suggestions,53 it is also necessary to point out that fundamental questions remain that are critical for shedding light on people’s understanding of mental illness and etiological beliefs and even more on social fault lines of a society that produces prejudice and discrimination which heavily impact the lives of mentally ill individuals and their family members.54,55
Author contributions
SM, AR, and SS conceived and designed the study; SM, AR, SS, and IS-Z managed data collection. SM performed the analysis and wrote the manuscript. SM, AR, and SS contributed to data discussion and interpretation. All authors read, critically revised, and approved the final manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
Dietrich S, Beck M, Bujantugs B, Kenzine D, Matschinger H, Angermeyer MC. The relationship between public causal beliefs and social distance toward mentally ill people. Aust N Z J Psychiatry. 2004;38(5):348–354. | ||
Jorm AF. Mental health literacy: public knowledge and beliefs about mental disorders. Br J Psychiatry. 2000;177:396–401. | ||
Mannarini S, Boffo M. Assessing mental disorder causal beliefs: a latent dimension identification. Community Ment Health J. 2013;49(6):686–693. | ||
Mannarini S, Boffo M. Anxiety, bulimia, drug and alcohol addiction, depression, and schizophrenia: what do you think about their aetiology, dangerousness, social distance, and treatment? A latent class analysis approach. Soc Psychiatry Psychiatr Epidemiol. 2015;50(1):27–37. | ||
Schomerus G, Borsche JH, Matschinger H, Angermeyer MC. Public knowledge about causes and treatment for schizophrenia. A representative population study. J Nerv Ment Dis. 2006;194:622–624. | ||
Sears PM, Pomerantz AM, Segrist DJ, Rose P. Beliefs about the biological (vs. nonbiological) origins of mental illness and the stigmatization of people with mental illness. Am J Psychiatr Rehabil. 2011;14(2):109–119. | ||
Abdullah T, Brown TL. Mental illness stigma and ethnocultural beliefs, values, and norms: an integrative review. Clin Psychol Rev. 2011;31(6):934–948. | ||
Angermeyer MC, Matschinger H. Social distance toward the mentally ill: results of representative surveys in the Federal Republic of Germany. Psychol Med. 1997;27(1):131–141. | ||
Srinivasan TN, Thara R. Beliefs about causation of schizophrenia: do Indian families believe in supernatural causes. Soc Psychiatry Psychiatr Epidemiol. 2001;36(3):134–140. | ||
Yang LH, Pearson VJ. Understanding families in their own context: schizophrenia and structural family therapy in Beijing. J Fam Ther. 2002;24(3):233–257. | ||
Furnham A, Malik R. Cross-cultural beliefs about “depression”. Int J Soc Psychiatry. 1994;40(2):106–123. | ||
Farina A, Felner RD. Employment interviewer reactions to former mental patients. J Abnorm Psychol. 1973;82(2):268–272. | ||
Hinshaw SP. The Mark of Shame: Stigma of Mental Illness and an Agenda for Change. New York: Oxford University Press; 2007. | ||
Read J, Baker S. Not Just Sticks and Stones: A Survey of the Stigma, Taboos and Discrimination Experienced by People with Mental Health Problems. London, UK: MIND; 1996. | ||
Wahl O. Mental Health Consumers’ experience of stigma. Schizophr Bull. 1999;25(3):467–478. | ||
Angermeyer MC, Matschinger H. Causal beliefs and attitudes to people with schizophrenia. Br J Psychiatry. 2005;186:331–334. | ||
Cook TM, Wang JL. Causation beliefs and stigma against depression: results from a population based study. J Affect Disord. 2011;133:86–92. | ||
Jorm AF, Griffiths KM. The public’s stigmatizing attitudes towards people with mental disorders: how important are biomedical conceptualizations? Acta Psychiatr Scand. 2008;118(4):315–321. | ||
Lincoln TM, Arens E, Berger C, Rief W. Can anti-stigma campaigns be improved? A test of the impact of biogenetic vs psychosocial causal explanations on implicit and explicit attitudes to schizophrenia. Schizophr Bull. 2008;34(5):984–994. | ||
Mehta S, Farina A. Is being ‘‘sick’’ really better? Effect of the disease view of mental disorder on stigma. J Soc Clin Psychol. 1997;16:405–419. | ||
Read J, Harre N. The role of biological and genetic causal beliefs in the stigmatization of ‘mental patients’. J Ment Health. 2001;10:223–235. | ||
Rusch N, Angermeyer MC, Corrigan PW. Mental illness stigma: concepts, consequences, and initiatives to reduce stigma. Eur Psychiatry. 2005;20:529–539. | ||
Rusch LC, Kanter JW, Brondino MJ. A comparison of contextual and biomedical models of stigma reduction for depression with a nonclinical undergraduate sample. J Nerv Ment Dis. 2009;197(2):104–111. | ||
Walker I, Read J. The differential effectiveness of psychosocial and biogenetic causal explanations in reducing negative attitudes toward ‘‘mental illness’’. Psychiatry. 2002;65:313–325. | ||
Demir B, Broussard B, Goulding SM, Compton MT. Beliefs about causes of schizophrenia among police officers before and after crisis intervention team training. Community Ment Health J. 2009;45(5):385–392. | ||
Corrigan PW. Resolving mental illness stigma: should we seek normalcy or solidarity? Br J Psychiatry. 2016;208(4):314–315. | ||
Schomerus G, Lucht M, Holzinger A, Matschinger H, Carta MG, Angermeyer MC. The stigma of alcohol dependence compared with other mental disorders: a review of population studies. Alcohol Alcohol. 2011;46(2):105–112. | ||
Pescosolido BA, Martin JK, Long JS, Medina TR, Phelan JC, Link BG. “A disease like any other”? A decade of change in public reactions to schizophrenia, depression, and alcohol dependence. Am J Psychiatry. 2010;167(11):1321–1330. | ||
Cheng ZH. Asian Americans and European Americans’ stigma levels in response to biological and social explanations of the depression. Soc Psychiatry Psychiatr Epidemiol. 2015;50(5):767–776. | ||
Mannarini S, Boffo M, Balottin, L. Beliefs about the patient’s role in the psychotherapeutic relationship: a latent trait perspective. Test Psychom Methodol Appl Psychol. 2013;20(3):277–294. | ||
Webb M, Peterson J, Willis SC, et al. The role of empathy and adult attachment in predicting stigma toward severe and persistent mental illness and other psychosocial or health conditions. J Ment Health Couns. 2016;38(1):62–78. | ||
Aragona M, Kotzalidis G, Puzella A. The many faces of empathy, between phenomenology and neuroscience. Arch Psychiatr Psychother. 2013;4:5–12. | ||
Dziobek I. Towards a more ecologically valid assessment of empathy. Emot Rev. 2012;4(1):18–19. | ||
Britton PC, Fuendeling JM. The relations among varieties of adult attachment and the components of empathy. J Soc Psychol. 2005;145(5):519–530. | ||
Eisenberg N, Fabes RA, Murphy B, et al. The relations of emotionality and regulation to dispositional and situational empathy-related responding. J Pers Soc Psychol. 1994;66(4):776–797. | ||
Mills H, Reiss N, Dombeck M. Self-efficacy and the perception of control in stress reduction. Disorders & Issues – Stress Reduction and Management. Available from: http://www.mentalhelpnet. 2008. Accessed March 1, 2017. | ||
Jones EE, Farina A, Hastorf AH, Markus H, Miller DT, Scott RA. Social Stigma: The Psychology of Marked Relationships. New York: W H Freeman; 1984. | ||
Feldman DB, Crandall CS. Dimensions of mental illness stigma: what about mental illness causes social rejection? J Soc Clin Psychol. 2007;26(2):137–154. | ||
Mannarini S, Boffo M. The relevance of security: a latent domain of attachment relationships. Scand J Psychol. 2014;55(1):53–59. | ||
Caprara GV. La valutazione dell’autoefficacia [Self-efficacy evaluation]. Trento: Erickson; 2001. Italian. | ||
Cohen S, Kamarick T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. 1983;24(4):385–396. | ||
Tal A, Roe D, Corrigan PW. Mental illness stigma in the Israeli context: deliberations and suggestions. Int J Soc Psychiatry. 2007;53(6):547–563. | ||
Gelkopf M, Roe D, Werbeloff N, et al. The prevalence of full and partial posttraumatic stress disorder among people with severe mental illness in Israel. J Nerv Ment Dis. 2013;201(3):244–250. | ||
Munizza C, Argentero P, Coppo A, et al. Public beliefs and attitudes towards depression in Italy: a national survey. PloS One. 2013;8(5): e63806. | ||
Holzinger A, Floris F, Schomerus G, Carta MG, Angermeyer MC. Gender differences in public beliefs and attitudes about mental disorder in western countries: a systematic review of population studies. Epidemiol Psychiatr Sci. 2012;21:73–85. | ||
Wesselman ED, Day M, Graziano WG, Dohert EF. Religious beliefs about mental illness influence social support preferences. J Prev Interv Community. 2015;43(3):165–174. | ||
Feeney JA, Noller P, Hanrahan M, Sperling MB. Assessing adult attachment. In: Berman WH, editor. Attachment in Adults: Clinical and Developmental Perspectives. New York: Guilford Press; 1994:128–152. | ||
Bandura AB, Locke EA. Negative self-efficacy and goal effects revisited. J Appl Psychol. 2003;88(1):87–99. | ||
Linacre JM. Many-Facet Rasch Measurement. Chicago, IL: MESA Press; 1989. | ||
Linacre JM. A User’s Guide to FACETS: Rasch-Model Computer Programs [software manual]. Chicago, IL: Winsteps; 2005. | ||
Bond GT, Fox CM. Applying the Rasch Model. Fundamental Measurement in Human Sciences. Mahwah, New Jersey: Erlbaum; 2001. | ||
Meyerstein I. A Jewish spiritual perspective on psychopathology and psychotherapy: a clinician’s view. J Relig Health. 2004;43(4):329–341. | ||
Pescosolido B. The public stigma of mental illness: what do we think; what do we know; what can we prove? J Health Soc Behav. 2013;54(1):1–21. | ||
Piatt EE, Munetz MR, Ritter C. An examination of premature mortality among decedents with serious mental illness and those in the general population. Psychiatr Serv. 2010;61(7):663–668. | ||
Mannarini S, Boffo M. An implicit measure of associations with mental illness versus physical illness: response latency decomposition and stimuli differential functioning in relation to IAT order of associative conditions and accuracy. PLoS One. 2014;9(7):e101911. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.