Back to Journals » Patient Related Outcome Measures » Volume 11
The Role of Attachment Styles and Communication Skills in Predicting Nursing and Medical Students’ Perception of Elder Abuse
Authors Salehi A, Gholamzadeh S, Javadi M
Received 4 September 2019
Accepted for publication 17 December 2019
Published 23 January 2020 Volume 2020:11 Pages 11—19
DOI https://doi.org/10.2147/PROM.S229908
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Lynne Nemeth
Ammar Salehi,1 Sakineh Gholamzadeh,2 Mostafa Javadi3
1Fatemeh Nursing and Midwifery School, Shiraz University of Medical Sciences (SUMS), Shiraz, Iran; 2Community-Based Psychiatric Care Research Center, Shiraz University of Medical Sciences (SUMS), Shiraz, Iran; 3Nursing and Midwifery School, Shahid Sadoughi University of Medical Sciences, Yazd, Iran
Correspondence: Sakineh Gholamzadeh
Community-Based Psychiatric Care Research Center, Shiraz University of Medical Sciences (SUMS), Shiraz, Iran
Tel +987 136474257
Fax +987136279135
Email [email protected]
Background: The knowledge and abilities of nurses and physicians in perceiving and dealing with abuse are necessary for the improvement of older people’s health. Therefore, the aim of this study was to investigate the role of attachment styles and communication skills in predicting nursing and medical students’ perception of elder abuse in Yazd, Iran.
Methods: The present study was a descriptive cross-sectional design that was conducted in the form of multistage sampling on 397 nursing and medical students at Shahid Sadoughi University of Medical Sciences in Yazd, Iran. The Elderly Caregiving Questionnaire (ECQ), Adults’ Attachment Styles Inventory (AAI), and the revised version of the Communication Skills Questionnaire were used for data collection. Data were analyzed using the SPSS version 22 software.
Results: The findings revealed that the participants had an appropriate understanding of elder abuse. The highest level of perception of elder abuse was in the dimension of psychological abuse (24.5± 5.22) and the lowest level was related to the dimension of physical abuse (21.7± 4.74). Additionally, a positive significant relationship was found between the score of students’ perception of abuse, and secure and avoidant attachment styles as well as students’ communication skills (p< 0.01). According to regression analysis, these predictors explained 8.6% of the observed variance in the students’ perception of elder abuse.
Conclusion: These findings indicate that attachment styles influenced the individual’s perception of elder abuse. Therefore, in future planning and research, this should be given more attention.
Keywords: elder abuse, perception, student, nursing, medical, attachment styles, communication
Introduction
Improving living conditions as well as increasing longevity and life expectancy has led to the phenomenon of aging in today’s societies, especially in developing countries. In 2017, it was estimated that 13% of the global population were aged 60 or over.1 According to the 2016 population census in Iran, 9.28% of the populations were older people. It was predicted that the percentage of older people in Iran by 2025 and 2050 will reach 10% and 30%, respectively.2 Increasing age is associated with many physical and psychological challenges. One study found that 92.2% of the Iranian elderly population suffered from at least one chronic disease.3 Frailty and disruption of physical health can increase the risk of elder abuse and reduce the ability of older people to protect themselves or make themselves free from the abusive situation.4 The rate of abuse among older people in their own home has been reported to be 67–73.3%.5,6 In a systematic review in Iran, the prevalence of elder abuse was reported between 17.1% and 87.8%.7 The terminology that was used to explain the elder abuse has changed over the years. The most commonly used definition for elder abuse is the one recognized by the World Health Organization (WHO). Accordingly, it can be said that a single or repeated act or an absence of appropriate action, happening through any relationship is elder abuse where there is a desire for trust which results harm or pain to an older person. Such a definition encompasses some items, including the psychological, financial, physical, social and sexual abuse, and intentional and unintentional neglect. Moreover, it can consist of both criminal and non-criminal acts.8 Elder abuse is one of the examples of violation of older rights that can result in serious and lasting problems for older people.9 Studies have indicated that one quarter to two thirds of the professional staff are not able to identify the cases that are considered as definitely abusive.10 Uncertainty about what behaviors are considered normal or typical and what behaviors are meant abusive is one of the barriers to detecting abuse. As doctors and nurses are among individuals who deal with abuse issues, they should have an appropriate perception of abuse and be able to properly identify the case of elder abuse.11
The lack of appropriate communication may deteriorate the health care providers’ capacity to recognize the case of elder abuse or neglect. Creating a therapeutic relationships and trust can ease the disclosure of abuse by the elderly patients.12 Those patients that are satisfied with their physician’s communication are more likely to share relevant and detailed information about their exact problems and follow the prescribed treatment.13,14 The attachment style of care providers may affect their professional interaction with patients as well as their perceptions of elder mistreatment. Ainsworth et al (2015) described three attachment styles as secure, anxious/ambivalent, and anxious/avoidant.15 The roles of these styles in adults’ relationships were explored by Hazan and Shaver.16 Individuals with the secure attachment style assume their relationships with others to be stable, available, and responsive. As a result, they are more successful in establishing and communicating with others.17 As a result, they are more successful in establishing and communication with others, while avoiding behaviors that may cause patients to be reluctant to disclose their problems, having a negative effect on the patient’s recovery.18
Investigating the role of attachment styles within the context of the provider-patient communication has been recommended by several researchers.19–21 A systematic review of the literature also suggested evidence for a link between health care provider attachment styles and their interaction with patients.22 Understanding attachment styles may be useful for teaching clinical communication in medical and nursing education. The attachment style also influences the health care worker’s perception of elder abuse. Studies have shown that the anxious–preoccupied attachment style is significantly related to the abuse perception in different cultures.23 Given the lack of studies, the researcher decided to identify the role of attachment styles and communication skills in predicting nursing and medical students’ perceptions of elder Abuse in Yazd City, Iran.
Methods
Design and Sampling
This is a descriptive cross-sectional study, which was done in the academic year of 2014–2015 on nursing and medical students studying at Shahid Sadoughi University of Medical Sciences in Yazd- Iran. Out of 750 students, 397 students were selected. Sampling was performed according to the field of study and academic semester using the random method. The sample size of 397 students was determined based on a correlation coefficient of 0.14, α = 0.05 and β = 0.20 (power= 80%) and using the med calc software. The nursing students from the first to last years of education were included. The medical students also entered the study from both the basic and clinical degrees.
Inclusion and Exclusion Criteria
Inclusion criteria included: willingness to participate in the study and signing the written consent form. However, unwillingness to continue the study, being a guest students, and inadequate response led to exclusion from the study.
Data Collection
After approval of the project by the Ethics Committee affiliated with Shiraz University of Medical Sciences (Code: 93–7261), the researcher referred to the students and provided explanations about the purpose of the study. The participants were ensured that their answers would be kept strictly confidential. The questionnaires were provided to the subjects and sufficient explanations were given on how to respond to questions. Participants filled out study questionnaires including demographics questionnaire, Attachment Style Inventory, Elderly Caregiving Questionnaire, and communication skills questionnaire.
Measurements
Instruments used in the present study were as follows: Adults’ Attachment Styles Inventory (AAI), which was developed by Hazen and Shaver.16 This was a self-reporting tool that was adapted to adults’ relationships and has 15 questions: 5 questions investigate anxious/ambivalent attachment, 5 questions exploring avoidant attachment, and the last 5 questions explor secure attachment. The questions were answered based on a five-point scale (never=0 to almost always=4).The dominant attachment style is the style that gained the highest score. The psychometric property of this questionnaire in Iran was assessed by Rahimian Boogar et al (2007). For reliability, the correlation coefficient of the questionnaire (Cronbach’s alpha) was 0.77 for secure, 0.81 for avoidant, 0.83 anxious/ambivalent subscales, and 0.75 for the total scale.24
Elderly Caregiving Questionnaire was used to explore the perceptions of elder abuse.23 The questionnaire was consisted of 30 items and it was used for measuring the judgment of the respondents on behaviors towards older people that might be considered abusive or typical. The questionnaire consisted of five subscales as followed: psychological abuse (for example, the caregiver screams at older people and calls them foul names), psychological neglect (for example, the caregiver ignores older people most of the time, rarely speaks with him/her and/or listens to his/her), physical abuse (for example, the caregiver hits the elderly person), physical negligence (caregiver neglects feeding older people) and financial abuse (the caregiver takes the older individual’s money without asking him/her). There are also five-filler items (for example, the caregiver takes the elderly out of the house). The participants assess each caregiver’s in a six-point Likert scale, the score of which ranges from 1 (non-abusive or non-typical) to 6 (highly abusive or highly typical). The score range without taking five filler items was between 25 and 150 with an average of 87.5. The higher score indicated higher perception of abusiveness or the typicality of behaviors.
To use this questionnaire in Iranian culture, it was first translated into Persian by a bilingual translator. Another translator was asked to translate it back to English. Subsequently, the content of these versions were adapted and some minor changes were made. The Persian version of the questionnaire was given to eight nursing faculty members who were familiar with the field of aging and psychiatric nursing for content validity. For reliability, 50 students were asked to complete the questionnaire twice within a 10-day interval. The test re-test reliability was obtained as 0.81 and the coefficient of Cronbach’s alpha was 0.90.
The revised version of the Queen Dom communication skills questionnaire was used for collecting data on communication skills. This scale was developed by Jerabek (2004) for measuring communication skills in adults and has 34 items (sentences) which described communication skills.25 The respondents were asked to read each item and specify the adaptation of his/her present condition with the content of the item on a 5-point Likert-type scale which ranges from 1 to 5 (never to always). The communication skills explored in this test included 5 skills consisting of listening skill, understanding verbal and nonverbal message, and insight to the communication process, emotional regulation, and assertiveness. The range of scores was from a minimum of 34 to a maximum of 170, scores of 34 to 68, poor communication skills, scores of 68 to 102, moderate communication skills, and scores of higher than 102, show strong communication skills.26 In Iran, Hosseinchari and Fadakar (2005) performed a study to investigate the psychometric analysis of the revised version of Queen Dom communication skills questionnaire. The reliability coefficient (Cronbach’s alpha coefficient) of the questionnaire was found to be 0.71, and test re-test reliability has been reported as 0.79.27
Data Analysis
Descriptive statistical analyses were used for describing the study variables. The independent t-test was used for comparing the mean score of abuse perception among nursing and medical students. The Pearson’s correlation coefficient was used to explore the relationship between the communication skills, attachment style, and perceptions of elder abuse. Finally, the linear regression analysis was used for determining the relationship of attachment styles and communication skills in predicting the perceptions of students of elder abuse.
Results
Subject’s Characteristics
In this study, 397 qualified participants (120 nursing and 277 medical students) with the mean age of 22.3± 3.4 years participated. The respondents were predominantly female (52.6%) and single (79.1%). The mean and standard deviation of the perceptions of elder abuse and its subscales were presented in Table 1.
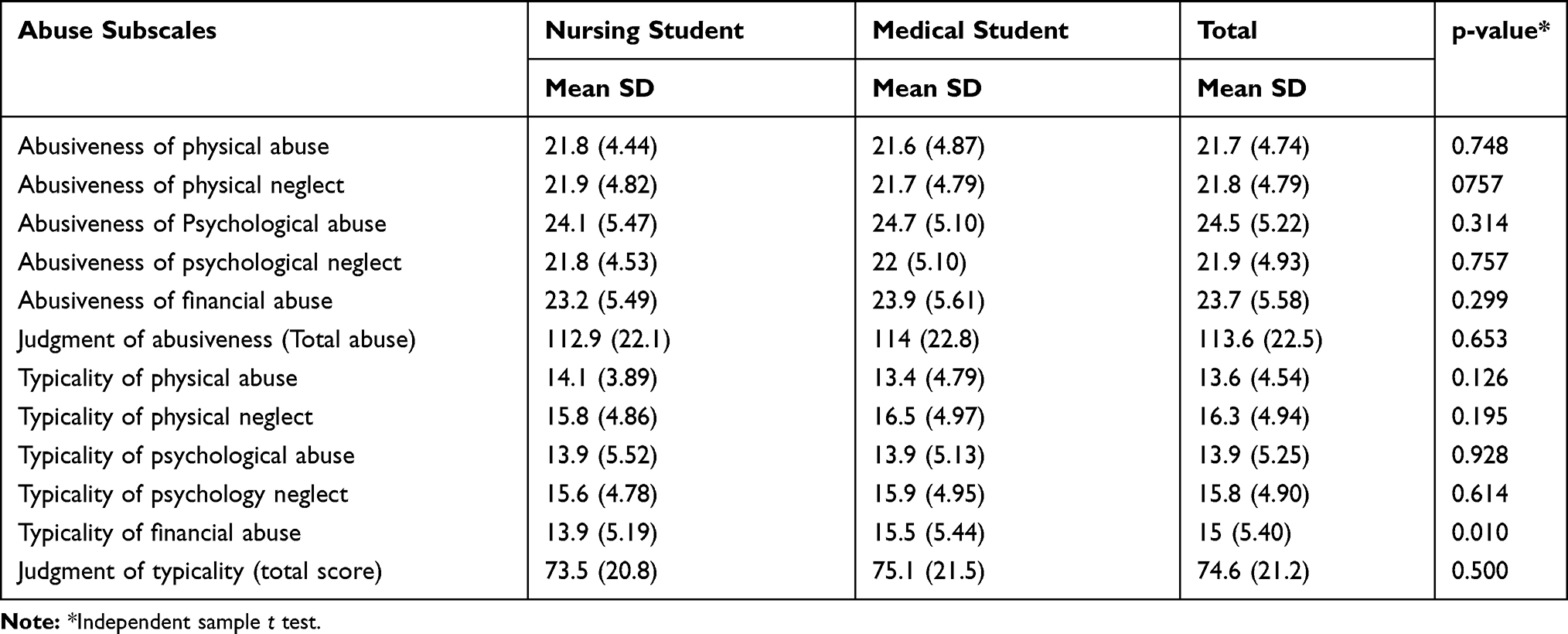 |
Table 1 Comparison of the Mean Score of Student’s Perception of Elder Mistreatment as Abusiveness or Typicality |
Outcomes
Perceptions of the abusiveness and typicality of elder mistreatment
As shown in Table 1, The mean score of student’s perceptions of elder abuse was 113.6± 22.5, which indicates higher perception.
The results showed that the highest score for the abusiveness of the behavior was related to the psychological dimension of abuse(24.5± 5.22) and the least one was for the physical dimension of abuse (21.7± 4.74). Physical and psychological neglect was also less understood as mistreatment. The independent samples t-test showed that there was no statistical difference between the two nursing and medical groups in any of the 5 subscales in terms of perceptions of elder abuse (t (392) =0.450, p =0.653). Also, for the perception of the typicality of elder abuse, the highest score was related to physical neglect (16.3± 4.94) and the lowest score was related to physical abuse (13.6± 4.54). There was no difference between the nursing and medical students in any of the dimensions of the typicality of behaviors, except for the financial dimension (t (389) =0.0675, p =0.500) (Table 1).
Students’ Attachment Styles
Mean total scores for both nursing and medical students with secure, avoidant, and ambivalent attachment styles were measured to be respectively 12.8± 2.57, 8.87± 1.98, and 9.30± 3.07. The findings indicated that most of the students had secure attachment style (Table 2). The independent-samples t-test was done to compare the mean score of attachment style between nursing and medical students. No significant statistical difference was found between two groups (p>0.05).
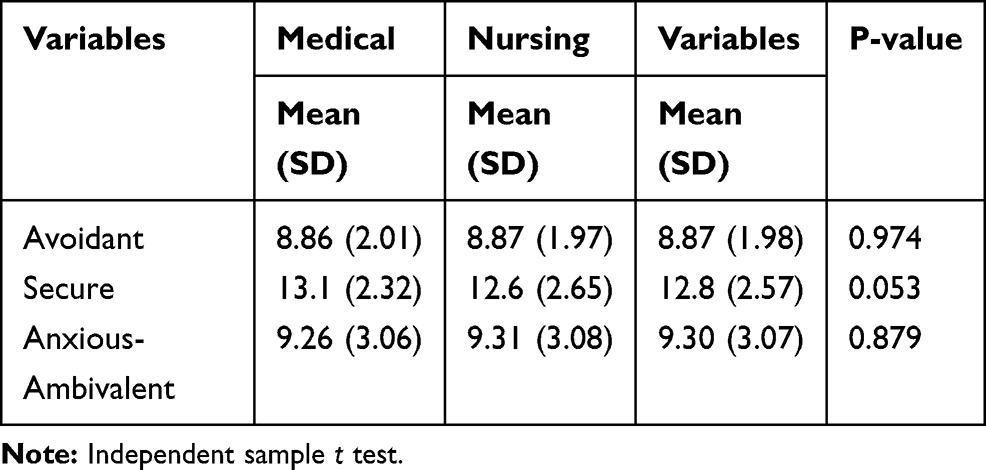 |
Table 2 Comparison of Attachment Style Score Between Nursing and Medical Students |
Communication Skills
The mean score of communication skills (109.2±8.4) was also high in both groups according to the range of scores (28–170). The highest score of communication skills was related to understanding verbal and nonverbal message (30 ±3.25) and the lowest score was for assertiveness (14.5±2.25). To compare the communication skills in nursing and medical students, the independent-samples t-test was performed. There was not found any significant statistical difference between the communication skills of the groups (p>0.05). However, in the domain of listening skill, a significant statistical difference was reported between medical (M=19.4, SD=2.59) and nursing (M=20, SD=2.38) students (t (395) =−2.11, p =0.035). Listening skill was higher in nursing students compared to medical students (Table 3).
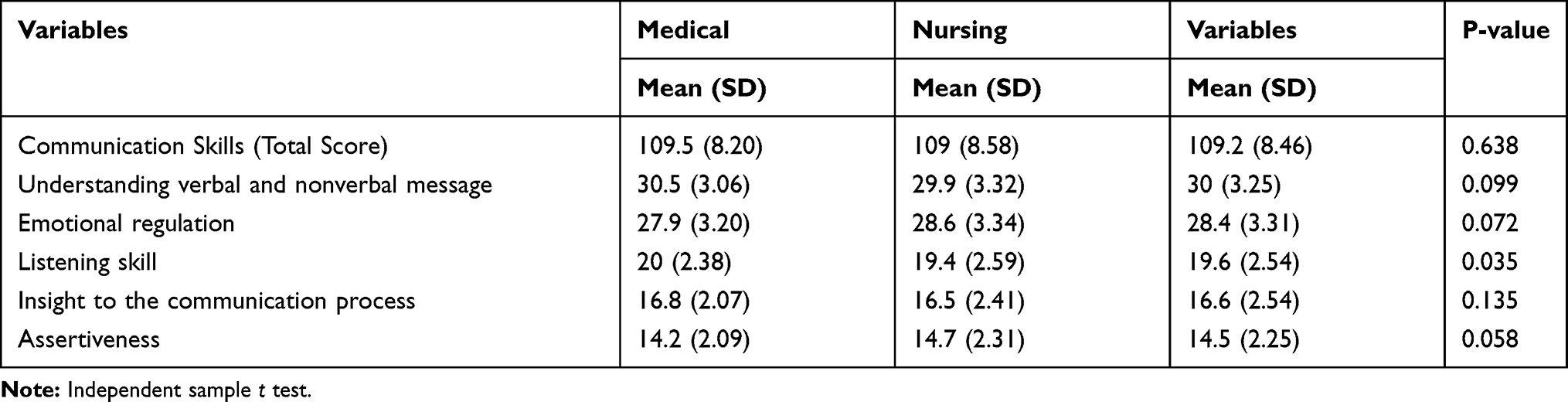 |
Table 3 Comparison of Communication Skills Between Nursing and Medical Students |
The Results of Pearson’s Correlation
As shown in Table 4, there was a positive significant relationship between the student’s avoidant and secure attachment style and their perception of elder abuse as abusiveness (p<0.01, r=0.139 and p<0.001, r=0.205, respectively). However, no significant relationship was found between the ambivalent style and perception of elder abuse (p>0.05, r=−0.043). In relation to typical behaviors, an inverse significant correlation was found between the students’ avoidant attachment style and their perspectives of elder abuse as typicality of abuse (r=0.122, p < 0.05).
 |
Table 4 Correlations Between Student’s Attachment Style and Their Judgment of Elder Mistreatment as Abusiveness (n =397) |
In fact, the students with a dismissive style of avoidant attachment tended to consider elder abuse more typical (Table 5). In addition, a significant linear relationship was found between students’ communication skills and the score of perception of elder abuse (p<0.001, r=0.22).
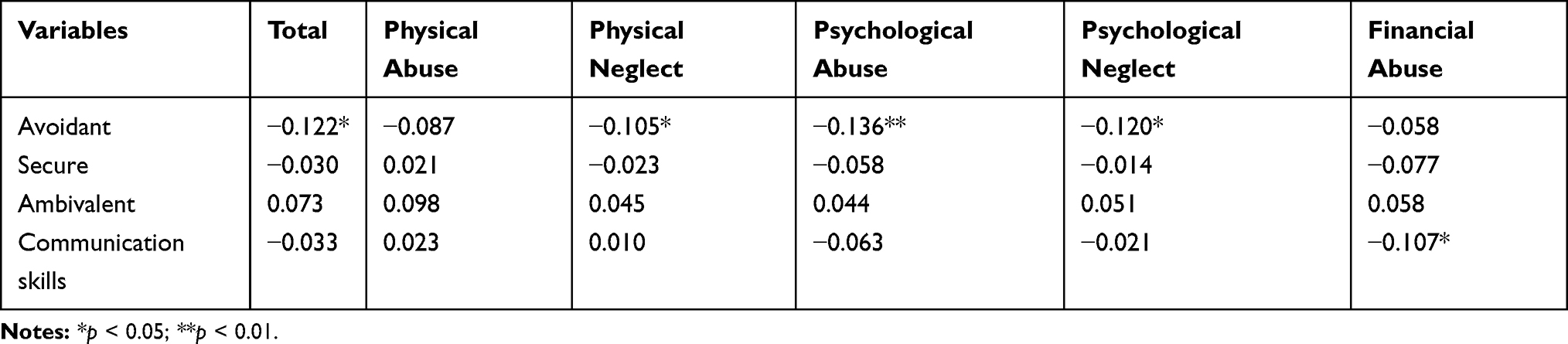 |
Table 5 Correlations Between Student’s Attachment Style and Their Judgment of Elder Mistreatment as Typicality (n =397) |
Multiple Linear Regression Analyses
Multiple regression analysis was performed to assess if the attachment styles and communication skill significantly predicted participants’ perception of abusive behaviors (Table 6). The results of the regression indicated that these predictors explained 8.6% of the observed variance in the perception of elder abuse [(R2 =0.086, F (3,393) =12.26, p<0.001] in the students. In addition, the result of regression analysis indicated that the avoidant attachment style explained 1.5% of the observed variance in the students judgment of typicality of abuse [(R2 =0.015, F (1,390) =5.86 p=0.016)].
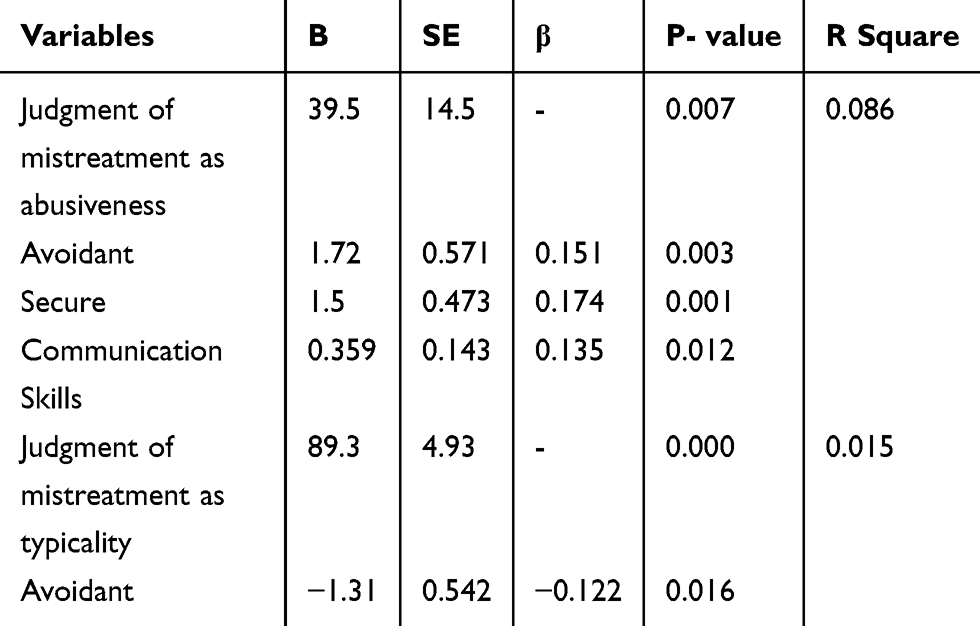 |
Table 6 Prediction Role of Attachment Style and Communication Skill in the Student’s Judgment of Elder Mistreatment as Abusive or Typicality |
Discussion
Results showed that both nursing and medical students had a good understanding of abusive behaviors. However, in a study by Ahmed and colleagues in Malaysia, nurses and doctors had a poor understanding of elder abuse and neglect. In addition, in the study by Daly and Coffey (2010), there was a lack of certainty about what constituted elder abuse among nurses.28 Differences in results are probably due to the cultural difference. In perceiving and defining the elder abuse, cultural values and beliefs play a pivotal role. Abusive behavior in one culture may be completely different as to what considers abusive in another culture.29 In the current study, both nursing and medical students perceived psychological and financial abuse to be significantly more abusive and physical abuse considered less abusive than other forms of mistreatment. These results were consistent with those of Korean students and were inconsistent with those of American students. In the Malley-Morrison et al’s (2008) study, American students perceived the physical form of abuse more abuse than psychological abuse. In contrast, the Korean students considered the psychological form of abuse more abuse than the physical form.23
Moreover, the high prevalence of psychological and financial abuse in Iran can also lead to a greater understanding of these types of elder abuse. In a study (2016), which was conducted in Iran, elder abuse was very high in the aspects of financial and psychological ones and the lowest prevalence was related to the physical abuse.30 In Iran, Islamic doctrine highly emphasizes respecting older people and these teachings can influence individuals’ perceptions of psychological abuse. However, there is a need for more studies on the role of culture and other individual variables on the perception of elder abuse. Also, in the present study, students showed a slight perception of physical abuse. Similarly, in the study of Bahraminejad et al nurses also showed a slight perception of physical abuse.31 The cause of inadequate understanding of physical abuse is that they are in line with other health-related problems in older people. In addition, older patients may also refrain to disclose abuse due to the need and dependence of care and medical and financial support. Moreover, in various studies conducted in Iran, physical abusive behavior was the least frequent,32 which might be influenced by lack of understanding of this kind of mistreatment. Regarding negligence, the results also showed that physical and psychological neglect was perceived less as mistreatment. Both nursing and medical students also considered various forms of physical neglect as significantly more typical than the other forms of mistreatment. In fact, physical and psychological neglect not considered as a form of elder mistreatment in both groups of students. However, in another study, psychological neglect was the most commonly reported form of abuse, followed by “neglect or abandonment”.33 In a study in Portugal psychological neglect was the most frequently reported type of maltreatment.34 Reasons for inadequate perception of neglect by students can be related to lack of knowledge about definition of elder abuse and neglect and its clinical presentation. Mallay Morrison found that one quarter to two thirds of professional staff were unable to understand the abusive behaviors that were considered definitely abusive.23 Improving student knowledge of abusive and negligence incidents towards older people enable them to properly perceive and diagnose abusive situations and intervene.35
Concerning students’ attachment styles, most students had the secure attachment style that was consistent with the results of other studies. For example, in a study in Iran, the attachment style of most nursing students was secure.20 Furthermore, Kaya in a study in Turkey, showed a higher prevalence of the secure attachment style among nursing students.36 However, for medical students, in the study of Asgharinejad et al and Ahadi et al the most attachment style in medical students was the avoidant and then secures style.37,38 Also, in the study of Williams et al in Australia, insecure attachment style has been reported as dominant style.39 The attachment style of nurses and doctors can affect their quality of care. Khodabakhsh and colleague stated that the secure attachment had a positive effect on empathy that led to appropriate communication with patients.20 In a cohort study of 82 Turkish nursing students, Kaya reported that the therapeutic relationship with patients has been influenced by the different attachment styles and empathic responsiveness of nurses.36
In the present study, a positive significant relationship was found between the secure and avoidant attachment styles and the overall score of abusive perceptions. However, the ambivalent style showed no significant relationship with abuse perceptions. In contrast, Malley-Morrison et al showed no relationship between the perception of abusiveness and attachment styles in American students. However, in Korean students, a negative correlation was found between the fearful style and student’s perception of abuse. Those students who had a fearful style had considered mistreatment behaviors less abusive.23 The reason for such contradictions may be related to different populations, cultures, questionnaire and different classifications of attachment styles.
In addition, the results of the current study presented a positive significant association between the students’ communication skills and their perceptions of elder mistreatment and abuse. Communication between doctors and patients enables patients to share essential information needed for an accurate diagnosis of health-related problems. It also helps doctors to have a better perception of their patient’s problems and possibility lead to better symptom management.40 Future programs of elder abuse detection and prevention should consider these factors.
These findings should be replicated with other healthcare staff in different settings. In addition, because the Elderly Caregiving Questionnaire was used for the first time in Iran, it is better to assess its psychometric properties in future studies. The ECQ questionnaire used in this study did not measure the dimension of sexual abuse, which is a limitation of this study.
Conclusion
The results show that nursing and medical students have a proper understanding of elder abuse. However, psychological abuse is recognized by students more abusive than other types of elder abuse. Given that nurses and physicians often take care of elderly people, alertness towards elder abuse is one part of their task. However, a lack of practical training on elder abuse and neglect has been recognized as an obstacle.41 As has been suggested in different studies,41–43 it’s going to be necessary to provide more comprehensive content on elder abuse within the medical and nursing student’s program to better prepare future students by enhancing their basic perception and knowledge of elder abuse. Considering the effect of communication skills and attachment style on students’ perceptions of elder abuse, individual characteristics should be included in future planning. Based on the findings of this study and those of other studies,44–46 further research is suggested to validate these findings and to determine their effect in more detail within the broader context of clinical practice before conducting educational interventions.
Acknowledgment
The researchers would like to express their gratitude to the students who participated in this study and collaborated in the production of this article.
Disclosure
The authors have declared that they had no competing interests.
References
1. United Nations. Department of economic and social affairs, population division,‘World population Prospects; 2017. Available from: https://population.un.org/wpp/.
2. Statistical Centre of Iran. Findings of the 2016 National Population and Housing Census. Tehran; 2016. Available from: https://www.unescap.org/sites/default/files/Session6_Iran_Population_and_Housing_Census2016_Census_WS_24-26Jan2018.pdf.
3. Esmaeili Shahmirzadi S, Shojaeizadeh D, Azam K, Salehi L, Tol A, Moradian Sorkhkolaei M. The impact of chronic diseases on the quality of life among the elderly people in the east of Tehran. J Payavard Salamat. 2012;6(3):225–235.
4. Lachs MS, Pillemer K. Elder abuse. Lancet. 2004;364(9441):1263–1272. doi:10.1016/S0140-6736(04)17144-4
5. Newton JP. Abuse in the elderly–a perennial problem. Gerodontology. 2005;22(1):1–2. doi:10.1111/ger.2005.22.issue-1
6. Buka P, Sookhoo D. Current legal responses to elder abuse. Int J Older People Nurs. 2006;1(4):194–200. doi:10.1111/opn.2006.1.issue-4
7. Molaei M, Etemad K, Taheri Tanjani P. Prevalence of elder abuse in Iran: a systematic review and meta analysis. Iran J Ageing. 2017;12(2):242–253.
8. World Health Organization(WHO). “Elder abuse.” Ageing and life-course 2016. Available from: https://www.who.int/ageing/projects/elder_abuse/en/.
9. Payne BK. An integrated understanding of elder abuse and neglect. J Crim Justice. 2002;30(6):535–547. doi:10.1016/S0047-2352(02)00175-7
10. Hempton C, Dow B, Cortes-Simonet EN, et al. Contrasting perceptions of health professionals and older people in Australia: what constitutes elder abuse? Int J Geriatr Psychiatry. 2011;26(5):466–472. doi:10.1002/gps.2549
11. Christianson AL. Perceptions of Elder Abuse [M.S.]. Ann Arbor: Medical College of Ohio at Toledo; 2001.
12. Phelan A. The role of the nurse in detecting elder abuse and neglect: current perspectives. Nurs Res Rev. 2018;8(1):15–22. doi:10.2147/NRR.S148936
13. Charlton CR, Dearing KS, Berry JA, Johnson MJ. Nurse practitioners’ communication styles and their impact on patient outcomes: an integrated literature review. J Am Acad Nurse Pract. 2008;20(7):382–388. doi:10.1111/jaan.2008.20.issue-7
14. Clever SL, Jin L, Levinson W, Meltzer DO. Does doctor-patient communication affect patient satisfaction with hospital care? Results of an analysis with a novel instrumental variable. Health Serv Res. 2008;43(5 Pt 1):1505–1519. doi:10.1111/j.1475-6773.2008.00849.x
15. Ainsworth MDS, Blehar MC, Waters E, Wall SN. Patterns of Attachment: A Psychological Study of the Strange Situation. Psychology Press; 2015.
16. Hazan C, Shaver PR. Attachment as an organizational framework for research on close relationships. Psychol Inq. 1994;5(1):1–22. doi:10.1207/s15327965pli0501_1
17. Bowlby J. Attachment and Loss: Separation, Anger and Anxiety.
18. Maguire P, Pitceathly C. Key communication skills and how to acquire them. BMJ. 2002;325(7366):697–700. doi:10.1136/bmj.325.7366.697
19. Fletcher I, McCallum R, Peters S. Attachment styles and clinical communication performance in trainee doctors. Patient Educ Couns. 2016;99(11):1852–1857. doi:10.1016/j.pec.2016.05.019
20. Khodabakhsh M. Attachment styles as predictors of empathy in nursing students. J Med Ethics Hist Med. 2012;5:8.
21. Cherry MG, Fletcher I, O’Sullivan H, Dornan T. Emotional intelligence in medical education: a critical review. Med Educ. 2014;48:468–478. doi:10.1111/medu.2014.48.issue-5
22. Cherry MG, Fletcher I, O’Sullivan H. The influence of medical students’ and doctors’ attachment style and emotional intelligence on their patient-provider communication. Patient Educ Counsell. 2013;93:177–187. doi:10.1016/j.pec.2013.05.010
23. Malley-Morrison K, You HS, Mills RB. Young adult attachment styles and perceptions of elder abuse: a cross-cultural study. J Cross Cult Gerontol. 2000;15(3):163–184. doi:10.1023/A:1006748708812
24. Rahimian Boogar E, Nouri A, Oreizy H, Molavi H, Foroughi Mobarake A. Relationship between adult attachment styles with job satisfaction and job stress in nurses. Iran J Psychiatry Clin Psychol. 2007;13(2):148–157.
25. Jerabek I. Communication Skills Inventoryrevised. Body-Mind QueenDom. Available from: http://www.queendom.com/comunic.html.2004.
26. Yousefi F. The relationship between emotional intelligence and communication skills in university students. J Iran Psychol. 2006;3(9):5–13.
27. Hosseinchari M, Fadakar M. Effect of University on communication skills based on the comparison of secondary and college students. Sci J Shahed Univ. 2005;12(15):21–32.
28. Daly J, Coffey A. Staff perceptions of elder abuse: Joan Daly and Alice Coffey present findings from a study in Ireland that revealed a high level of uncertainty among staff about what constitutes abuse of residents in long-term care. Nurs Older People. 2010;22(4):33–37. doi:10.7748/nop2010.05.22.4.33.c7735
29. Tatara T. Understanding Elder Abuse in Minority Populations. Washington DC: Psychology Press, Taylor & Francis; 1999.
30. Taghadosi M, Gilasi H, Sadrollahi A. The prevalence of elder abuse and associated factors among the elderly in Kashan city, Iran. J Basic Res Med Sci. 2016;3(2):26–34. doi:10.18869/acadpub.jbrms.3.2.26
31. Bahramnezhad F, Navab E, Bakhshi R, AsadiNoughabi A. Nurses\’perception in Tehran of Elder Abuse. Iran J Geriatric Nurs. 2016;2(4):61–69. doi:10.21859/jgn.2.4.61
32. Nassiri H, Heravi Karimooi M, Jouybari L, Sanagoo A, Chehrehgosha M. The prevalence of elder abuse in Gorgan and Aq-Qala cities, Iran in 2013. Iran J Ageing. 2016;10(4):162–173.
33. Bezerra-Flanders W, Clark JC. Perspectives on elder abuse and neglect in Brazil. Educ Gerontol. 2006;32(1):63–72. doi:10.1080/03601270500338641
34. Mercurio AE, Nyborn J. Cultural definitions of elder maltreatment in Portugal. J Elder Abuse Negl. 2006;18(2–3):51–65. doi:10.1300/J084v18n02_04
35. Werner P, Eisikovits Z, Buchbinder E. Lay persons’ emotional reactions toward an abused elderly person. J Elder Abuse Negl. 2006;17(2):63–76. doi:10.1300/J084v17n02_04
36. Kaya N. Attachment styles of nursing students: a cross-sectional and a longitudinal study. Nurse Educ Today. 2010;30(7):666–673. doi:10.1016/j.nedt.2010.01.001
37. Asgharinejad M, Danesh E. Relation between attachment styles and happiness level and agreement in marital affairs in married students of university. Counsel Res Devel. 2005;4(14):69–90.
38. Ahadi B, Bagheri N. Relationship between loneliness and self-esteem with students’attachment styles. Thought Behav Clin Psychol. 2009;6:69–78.
39. Williams B, Brown T, McKenna L, Beovich B, Etherington J. Attachment and empathy in Australian undergraduate paramedic, nursing and occupational therapy students: a cross-sectional study. Collegian. 2017;24(6):603–609. doi:10.1016/j.colegn.2016.11.004
40. Goold S, Lipkin M. The doctor–patient relationship. J Gen Intern Med. 1999;14(S1):26–33. doi:10.1046/j.1525-1497.1999.00267.x
41. Pickering CE, Ridenour K, Salaysay Z, Reyes-Gastelum D, Pierce SJ. EATI Island–A virtual-reality-based elder abuse and neglect educational intervention. Gerontol Geriatr Educ. 2018;39(4):445–463. doi:10.1080/02701960.2016.1203310
42. Lo SK, Lai CK, Tsui CM. Student nurses’ perception and understanding of elder abuse. Int J Older People Nurs. 2010;5(4):283–289. doi:10.1111/j.1748-3743.2009.00196.x
43. Fisher JM, Rudd MP, Walker RW, Stewart J. Training tomorrow’s doctors to safeguard the patients of today: using medical student simulation training to explore barriers to recognition of elder abuse. J Am Geriatr Soc. 2016;64(1):168–173. doi:10.1111/jgs.13875
44. Cherry MG, Fletcher I, O’Sullivan H. Exploring the relationships among attachment, emotional intelligence and communication. Med Educ. 2013;47:317–325. doi:10.1111/medu.2013.47.issue-3
45. Cherry MG, Fletcher I, O’Sullivan H. Validating relationships among attachment, emotional intelligence and clinical communication. Med Educ. 2014;48(10):988–997. doi:10.1111/medu.2014.48.issue-10
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.