Back to Journals » Patient Preference and Adherence » Volume 15
The Relationship on Exercise Anticipation, Function and Self-efficacy in Patients After Knee Surgeries Over Six Months: An Observational Study
Authors Chen X, Zheng D, Ma H, Luo W ![]()
Received 5 August 2021
Accepted for publication 19 October 2021
Published 2 November 2021 Volume 2021:15 Pages 2431—2441
DOI https://doi.org/10.2147/PPA.S332202
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Naifeng Liu
Xiaoying Chen,1,* Dezhi Zheng,2,* He Ma,3 Wen Luo2
1The 2nd Ward of Knee Trauma Department, Tianjin Hospital, Tianjin, People’s Republic of China; 2The 2nd Ward of Joint Surgery Department, Tianjin Hospital, Tianjin, People’s Republic of China; 3The Emergency Treatment Department, Tianjin Hospital, Tianjin, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wen Luo
The 2nd Ward of Joint Surgery Department, Tianjin Hospital, No. 406 Jiefangnan Road, Tianjin, 300211, People’s Republic of China
Tel +86 22-131 1619 0054
Email [email protected]
Aim: To explore the association between the exercise anticipation, function and self-efficacy in patients after knee surgeries over six months and to identify the predictors for rehabilitation.
Methods: This observational study used the cross-sectional survey method and was divided into two stages: (1) designing the experimental video materials and answer cards about exercise anticipation, and (2) analyzing the correlation of the level of exercise anticipation, knee function, modified gait efficacy scale (mGES), self-efficacy for rehabilitation outcome scale (SER), self-efficacy for exercise scale (SEE), time up and go task (TUG) and knee joint angle in walking. We used IBM SPSS modeler 18.0 software for establishing the Bayesian network data mining model, which can identify strong positive and negative associations.
Results: A total of 110 patients were included in this study. Our research confirmed that the exercise anticipation score exhibited the significant correlation with SER (r=0.552, P< 0.01), SEE (r=0.457, P< 0.01), TUG (r=− 0.419, P< 0.01) and knee joint angle in walking (r=− 0.342, P< 0.01). There is only one parent node of exercise expectation, that is, rehabilitation self-efficacy, which shows that the rehabilitation self-efficacy of patients after knee surgery is directly related to their ability to judge exercise expectation. Meanwhile this study verified the model results, and the area under the ROC curve (AUC) is 0.572 (755/1320), indicating that the prediction performance is acceptable.
Conclusion: This preliminary study confirmed that improving the exercise anticipation and rehabilitation self-efficacy is an important method of enhancing the knee function in patients after knee surgeries over six months. In the future, the long-term effect of the exercise anticipation and self-efficacy should be researched.
Keywords: exercise anticipation, function, self-efficacy, knee surgeries
Background
The knee joint is an important joint in the body which plays a vital role in daily life.1 Due to diseases, trauma and so on, for example, knee osteoarthritis, rheumatoid arthritis, sports injuries, or fractures, the knee joint has often been seriously injured or deformed.2 Knee fractures including distal femur fractures, patella fractures, and proximal tibia fractures, have been reported at an incidence rate of approximately 9/105 per year in the US.3 Knee fractures have the characteristics of complex types, which usually lead to lower function and quality of life.4,5 In the 20-year nationwide cohort study in Denmark, the researchers observed that overall incidence rate of knee fractures increased 12% to 70/105 while the incidence rate that were surgically treated has increased 35% to 23/105.6 Meanwhile, the study found that people who had the complexity of knee fractures will face future challenges, for example, treatment burden, incidences and so on.7 The study provides the strong evidence for proper hospital resource allocations.7
Rehabilitation is the important progress in patients after knee surgeries. The researchers confirmed that is the significant relationship between the results of rehabilitation and education. Following knee surgery, a large number of patients would be required to perform rehabilitation at home by themselves.8–10 Anticipation is a process in which people use the existing information to pre-judge the coming events.11 When the existing information is updated, people’s expected results will change accordingly. The process of motion anticipation is more complex than simple motion perception, which involves not only the perceptual processing of current information, but also the integration of current information and background knowledge.12 Although sports expectation is closely related to decision-making and judgment, from the process of information processing, there is expectation before decision-making and judgment.13
Exercise is important during the rehabilitation process including an understanding of what kind of exercise is experienced during rehabilitation.14 By understanding what factors motivate patients in the rehabilitation process, physiotherapists will be better able to support patients to comply with the rehabilitation process.15 It is, therefore, of interest to explore injured patients’ exercise for adherence to rehabilitation. To explore factors, we chose the cross-sectional survey and Bayesian analysis, which contributes to increased knowledge of patients’ phenomena.
Self-efficacy is the important concept in Bandura’s social cognitive theory.16 It refers to the individuals’ self-confidence to accomplish a unique behavior in different conditions.17 Now, the study on self-efficacy has been used in different fields, for example diseases self-management, school education and so on.18 Many researchers showed that self-efficacy is closely related to people’s actual ability.
We hypothesized that there was a significant correlation between motor expectation and knee function in patients after knee surgeries over six months. The purpose of this study has investigated the exercise anticipation and influenced factors for patients with knee trauma during rehabilitation after surgeries and to explore the relationship of them.
Method
Design
This observational study used the cross-sectional survey method and is divided into two stages: (1) designing the experimental video materials and answer cards about exercise anticipation; (2) collecting the data of the exercise anticipation and scales in patients after knee surgeries over six months between February and May in 2021.
Participants
We used a convenience sample, participants were recruited from outpatients after knee surgeries over six months. The Hospital Research Ethics Committee approved the study protocol. To be eligible, participants must have reported the condition of physical action, who have ability independently. Participants were excluded if they reported any of the following: history of postoperative complications; lower extremity injury again within six months of the study that resulted in continued pain or dysfunction; or any vestibular, balance, or connective tissue disorder. All participants provided written informed consent, this study was approved by the hospital.
Procedures
Exercise Anticipation
The video material of this experiment selected action clips (MP4) from the video of knee rehabilitation training in Loyola University Medical School, Chicago, USA. The training materials were two videos with duration of 90 seconds and 30 seconds, respectively. The freeze-frame time of the video was the moment when the patient was ready to move in different directions. (1) Task 1: judging the motor direction of different points of “1”, “2”, “3”, “4”, and “5” of the single leg in the video, the subjects were required to judge the moving direction of the patient in the screen as quickly and accurately as possible. The first task consisted of four cycles. (2) Task 2: judging the jumping direction of double legs in the video. The subjects were asked to judge the jumping direction of the patient as quickly and accurately as possible. Fill in the test card according to the corresponding direction, and each task also has three seconds to judge. The second task included five cycles. Fill in the test card according to the corresponding number, and each task has three seconds to judge. Both tasks were evaluated by the accuracy of the subjects.
Scales
Modified Gait Efficacy Scale (mGES)
The English version modified gait efficacy scale designed by Newell, which consisted of 10 items and assessed a person’s self-efficacy on walking safely in different conditions,19 as described on different surfaces, step over an obstacle, up and down the wayside or the stairs, and long-distance walking. The individuals selected the score in the statement “How much confidence do you have that you would be able to safely…”. This scale used the 11-point Likertgrade scoring, the range of the score was from 0 to 100, where 100 meant the patient has the best gait self-efficacy. The Chinese version mGES has been confirmed that has high internal consistency (Cronbach’s α coefficient 0.928).20
Self-efficacy for Rehabilitation Outcome Scale (SER)
The English version self-efficacy for rehabilitation outcome scale has been designed by Waldrop et al, which contained 12 items for different behaviors on rehabilitation.21 The subjects of this scale were the patients after knee or hip surgery, which has been used to examine the patients’ self-efficacy on physical rehabilitation behaviors. The scale used the 11-point Likert scoring, with the score was ranging from 0 to 120. The scale can examine the patients’ self-efficacy under different situations, for example, pain, having emotional distress and so on. The study confirmed that the English version SER has high internal consistency (Cronbach’s α coefficient 0.94) in patients after different knee surgeries. Meanwhile, the Chinese version SER showed good reliability and validity in previous studies. The Chinese version SER has high internal consistency in patients after total knee arthroplasty.22
Self-efficacy for Exercise Scale (SEE)
The English version self-efficacy for exercise scale has been developed by Resnick et al, which has been used to assess the peoples’ self-efficacy on exercise.23 The English version SEE has a high internal consistency in previous studies. The Chinese version SEE has been translated and validated by Lee et al, which has acceptable internal consistency.24 The Chinese version SEE consists of nine items, with each item ranged between 0 (no confidence at all) and 9 (very confident), providing the range of score from 0 to 90. Higher score indicates better self-efficacy on exercise in daily living.
Function American Knee Society Score (Function AKSS)
The function AKSS measured the knee function from the walking distance (50 points) and the act of climbing and descending stairs (50 points).25 The range of score is from 0 to 100, which the best score indicted the individual can walking unlimited distances, climbing and descending stairs independently.26–28The function AKSS is currently the scale of choice in the world for assessment of knee function in patients with different knee diseases or after knee surgeries.29
Instrumentation
Gait video has been recorded by the digital camera SONY Alpha 9 ultra wide angle, resolution 1280×720 pixels at 50 frames per second. The FE24–70 mm lens F2.8 GM at the minimum available zoom can be used. It was located perpendicular to the patient at three meters and one meter above the floor. We analyzed the gait parameters in this study by Kinovea software. This is a free 2D motion analysis software, which can be used to assess kinematic parameters that allow us to analyze video without markers.30 Kinovea usually can be used by researchers to analyze athletes’ running or jumping.31 We measured the knee angle in this study. Drawing the first line between the reference points of greater trochanter and femoral condyle, another line between femoral condyle and external malleolus. The angle formed between the two lines would be used for calculating the range of the knee joint. The neutral position of the knee has been considered as 180°. Range has been calculated by the following equation: 180-(angle obtained by Kinovea), positive values represented flexion, negative values represented extension. 0~10° is the ideal level, which means that the affected knee joint can effectively carry load during walking. The greater the angle which means the worse the weight-bearing ability of the affected limb.31
Meanwhile, patients have been required to assess time up and go test (TUG) in this research, instructed to rise from the armless chair (45 cm height), walk three meters and turn around at a cone placement, walk back, and sit again.32 They were instructed to walk at a normal pace without walking aids and shoes. Time has been recorded when patients’ buttocks were lifted off the chair to stand and ceased when the buttocks touched the seat when returning to sitting position. This task was performed three times consecutively, and the averages have been used in analysis. Time up and go test has excellent reliability in older adults.32 Evaluation criteria: less than 10 seconds: free to move, 11~19 seconds: most of them can move independently, 20~29 seconds: unstable activity, more than 30 seconds: activity disorder.33
Statistical Analysis
Pearson’s correlation in different scales and scores was used to indicate the consistency and relationship of the contents in exercise anticipation. If the score of the exercise anticipation showed a normal distribution, Pearson’s correlation analysis has been chose; otherwise, Spearman correlation analysis has been chosen. A P-value of <0.05 indicates statistical significance. In this research, we selected a two-sided test to analyze whether these factors could be correlations. The correlation coefficient has been used by values: weak correlation (0.20–0.39), moderate correlation (0.40–0.59), strong correlation (0.60–0.79) and very strong correlation (0.80–1.0).34,35
Meanwhile, in this study we set up the Bayesian network model of the scores in exercise anticipation, function and modified gait efficacy scale. We carried out data cleaning and conversion in the original data. In the research, the main scores and assignments have been shown in Table 1. In this study, Genie 2.3 (developed by the Decision Systems Laboratory, the University of Pittsburgh) was considered as the effective tool to finish the Bayesian network parameter learning by using EM algorithm. And the network parameters are repeatedly iterated by using the accident data; the conditions for the termination of calculation are as follows: (1) the variation of the posterior probability for single risk factor is less than 1%; (2) the cumulative variation of posterior probability for the entire network is less than 15%.36,37
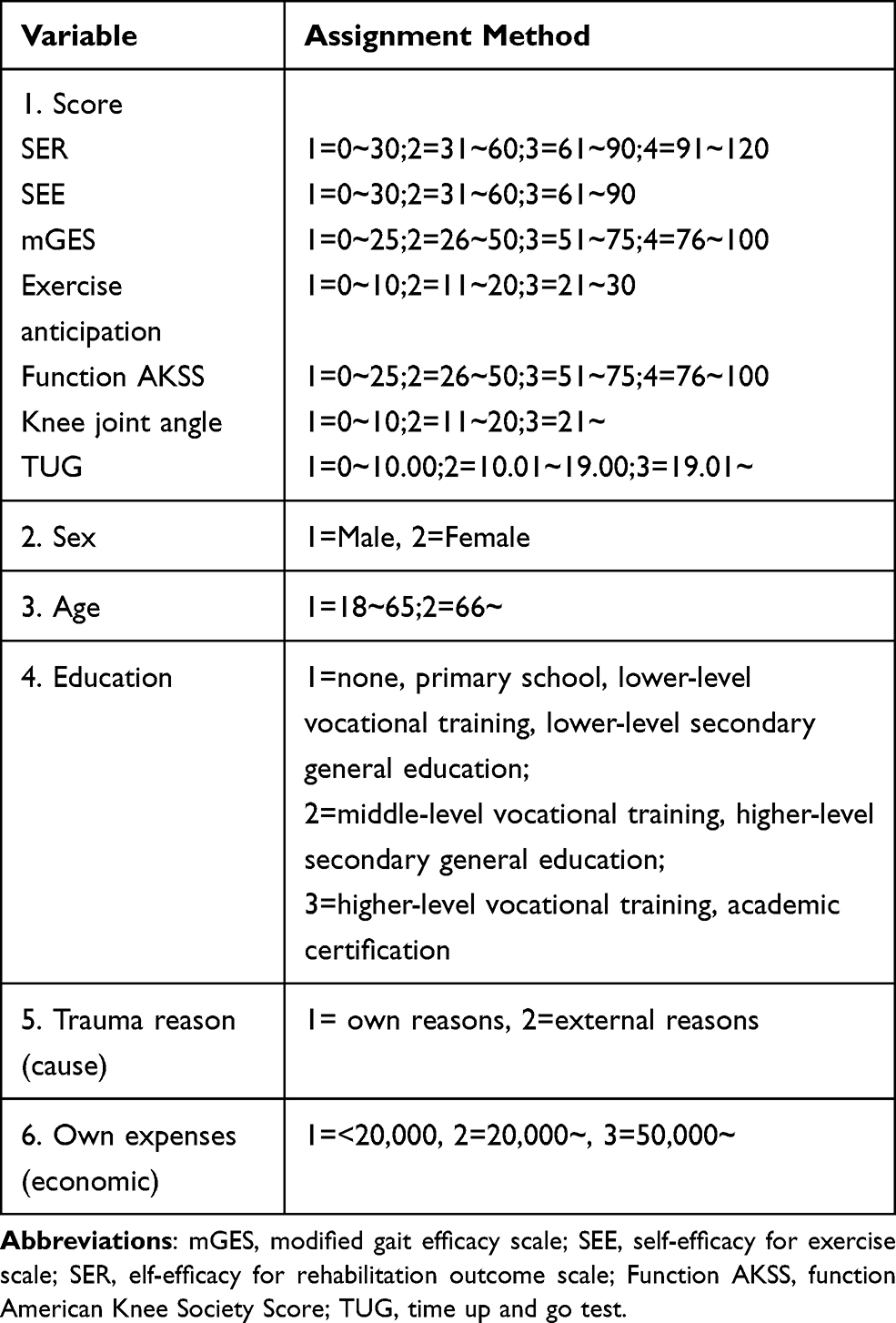 |
Table 1 The Main Variables and Assignments |
Results
Patients
Of the 115 participants have been recruited, five participants were excluded because of interrupting test subjectively, leaving 110 for analysis. The score and demographic characteristics of the included participants have been shown in Table 2. The average score of the participants who completed exercise anticipation was 15.25 and the standard deviation was 4.6, which has not shown the normal distribution (Figure 1).
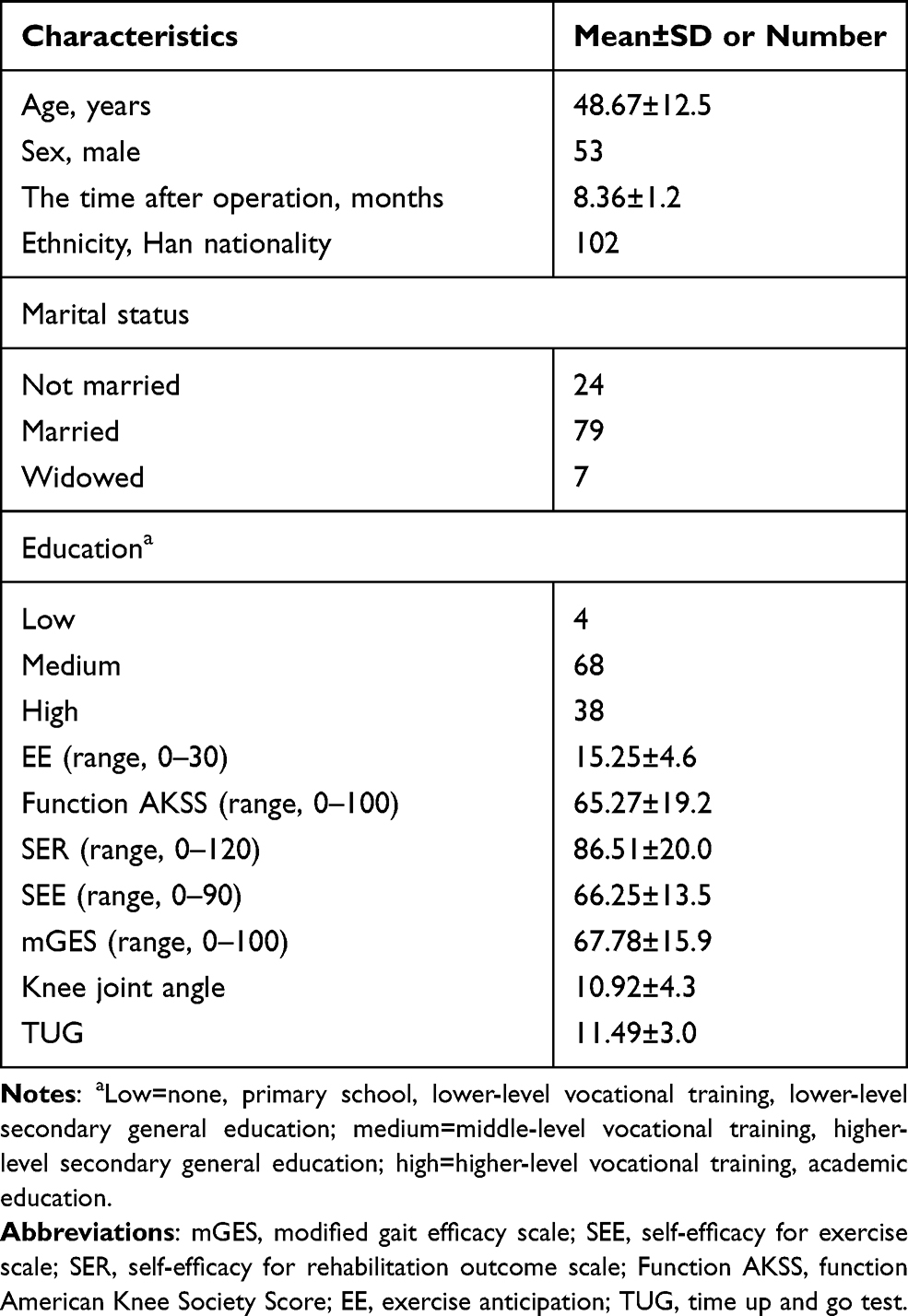 |
Table 2 Sample Characteristics (N=110) |
 |
Figure 1 Patients’ EE score distribution. Mean=15.25, standard deviation (line)=4.6, N=110. Abbreviation: EE, exercise anticipation. |
Correlation
In this research, the results of the Spearman analysis have confirmed that the exercise anticipation score has weak or moderate correlation with other scales. The results have shown that exercise anticipation score exhibited a weak and significant correlation with mGES (r=0.315, P<0.01) and function KSS (r=0.354, P<0.01). Meanwhile, we found that exercise anticipation score exhibited a moderate and significant correlation with SER (r=0.552, P<0.01) and SEE (r=0.457, P<0.01) (Table 3). The results in this study showed that the exercise anticipation has significant correlation with TUG (r=−0.419, P<0.01) and knee joint angle in walking (r=−0.342, P<0.01). In addition, the study found that the exercise anticipation score has no correlation with other factors (sex, age, education, trauma reason, and own expenses).
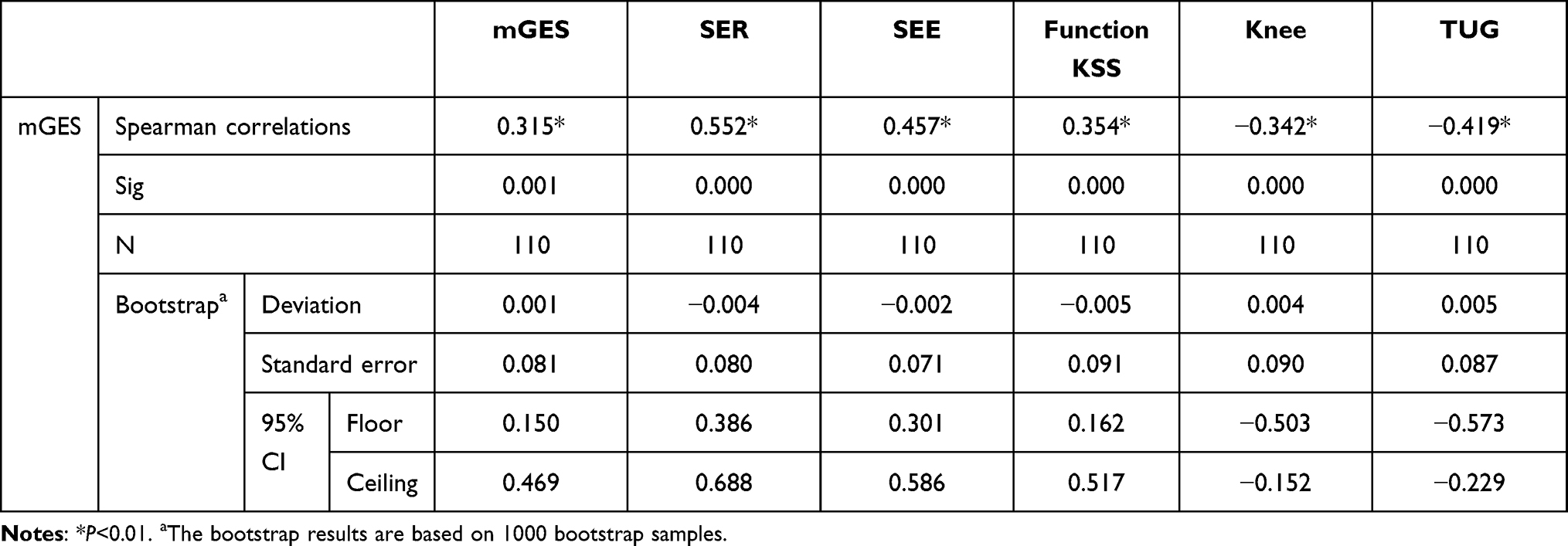 |
Table 3 Spearman Correlations Between Exercise Anticipation and Other Scales |
Bayesian Learning Networks of Exercise Anticipation
The maximum expectation is selected through the Bayesian network parameter learning tool (Genie), EM method carries out parameter learning. The learning results are shown in Figure 2, which comprehensively reflects the overall situation of structural learning and parameter learning of rehabilitation risk model of patients in the middle stage after knee surgery. The directed arc represents the causal relationship between Bayesian network nodes. In the figure, there is only one parent node of exercise expectation, that is, rehabilitation self-efficacy, which shows that the rehabilitation self-efficacy of patients after knee surgery is directly related to their ability to judge exercise expectation. Meanwhile this study verified the model results, and the area under the ROC curve (AUC) is 0.572 (755/1320), indicating that the prediction performance is acceptable. The sensitivity analysis showed that rehabilitation self-efficacy (0.294) and knee function score (0.336) were sensitive indicators to predict the expected level of exercise.
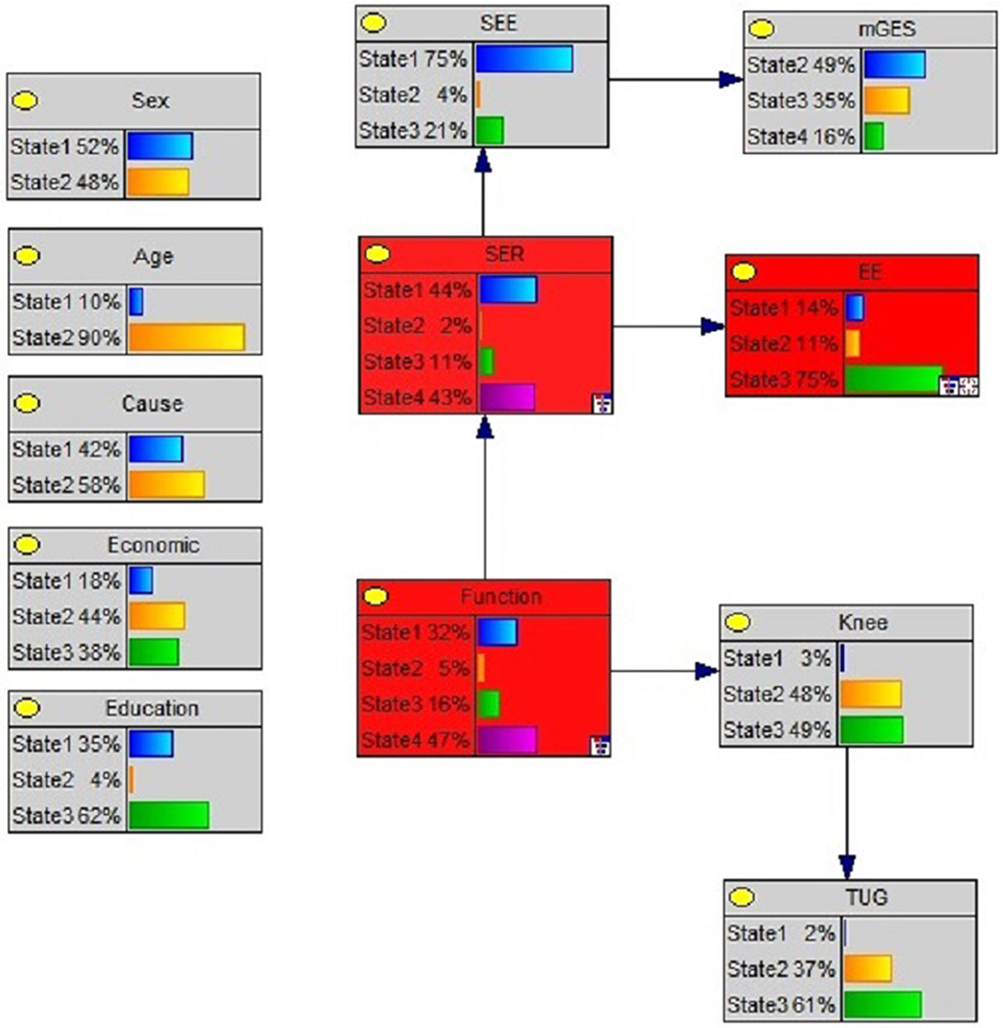 |
Figure 2 The Bayesian networks of exercise anticipation (EE). |
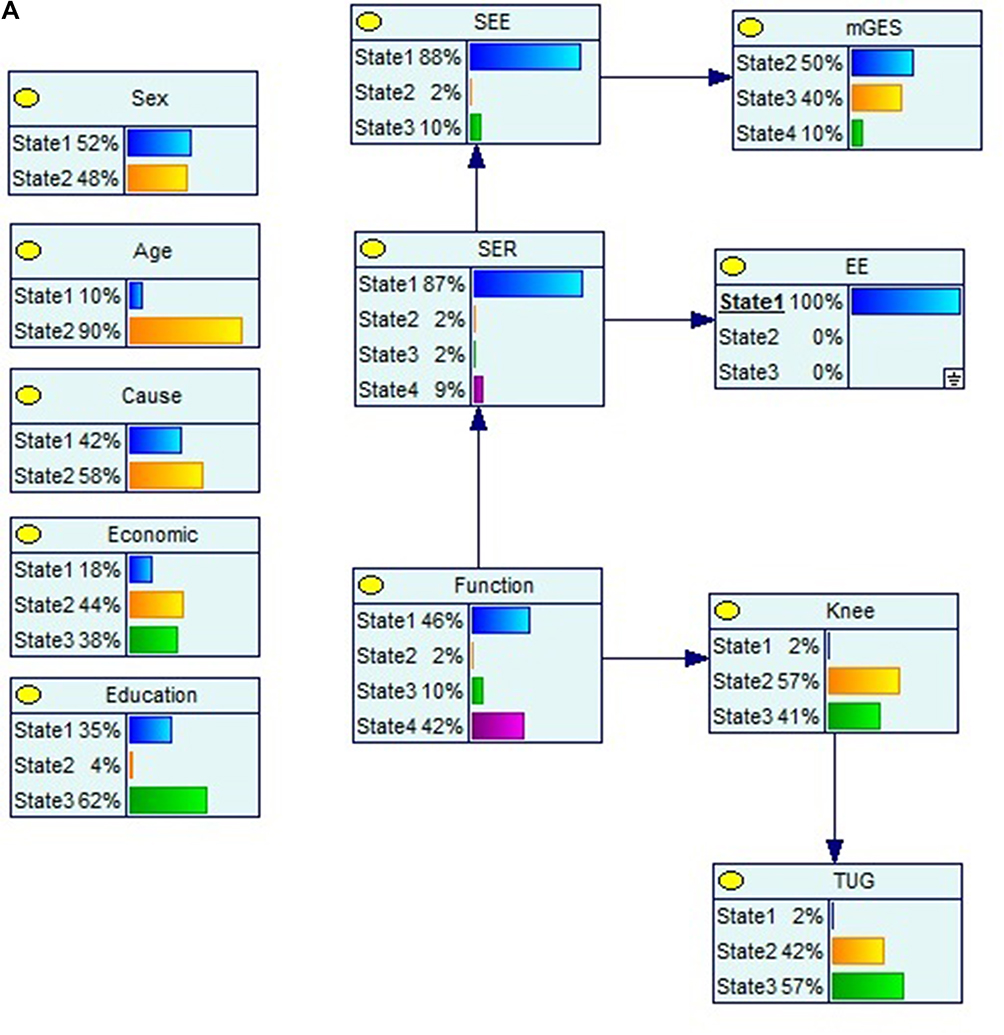 |
Figure 3 (A) Continued. |
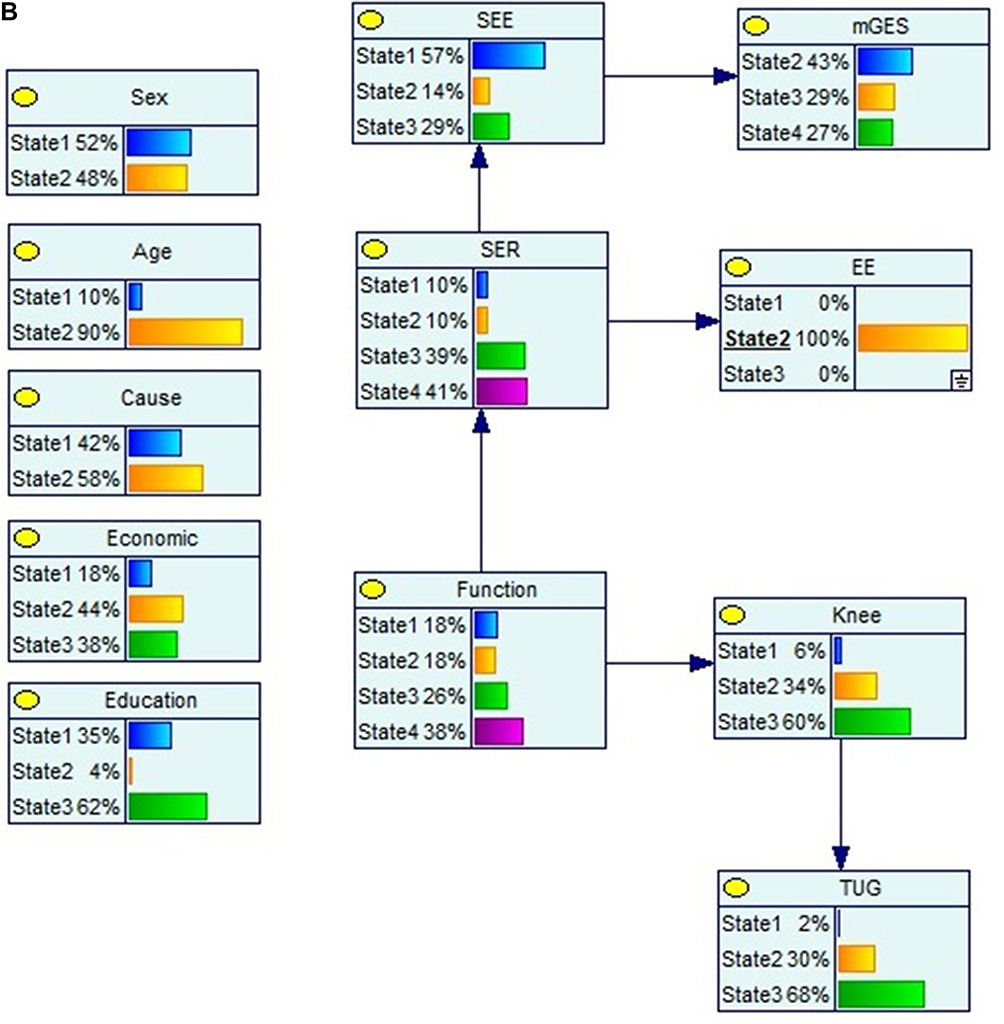 |
Figure 3 (B) Continued. |
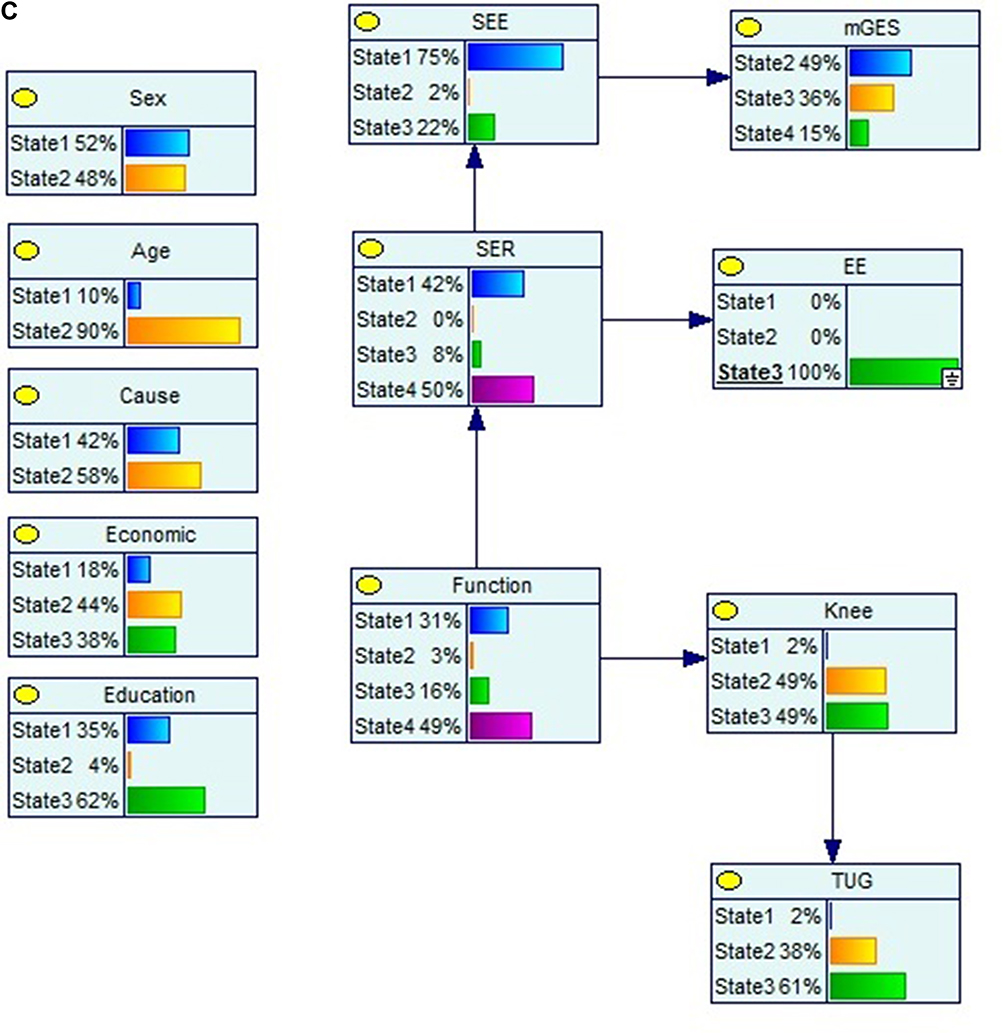 |
Figure 3 (A) Causal reasoning in Bayesian networks. (B) Causal reasoning in Bayesian networks. (C) Causal reasoning in Bayesian networks. |
Bayesian network can also carry out cause reasoning, that is, the process of finding the cause when the result state is known. According to the content of Figure 3A, the motion expectation is initialized to 1, which shows that the probability distribution of its influencing factors has changed. Figure 3A compared with Figure 2, when all value of EE was 1, the value 1 of SER increases from 44% to 87%, and the value 1 of SEE increases from 75% to 88%. Figure 3B compared with Figure 2, when all value of EE was 2, the value 2 of knee joint angle decreases from 48% to 34%, and the value 3 of TUG increases from 61% to 88%. When all value of EE was 3, the condition has been shown in Figure 3C. Figure 3C compared with Figure 2, when all value of EE was 3, the value 4 of SER increases from 43% to 50%.
Discussion
This study assessed the correlation and relationship were between the exercise anticipation and other scales in patients after knee surgeries more than six months. The findings of this research have shown that the level of exercise anticipation has significant correlation with gait parameters (TUG and knee joint angle in walking) and self-efficacy, for example, exercise, gait, and rehabilitation. Improving the level of exercise anticipation is an efficient method in rehabilitation in patients after knee surgeries for a long time.
By the Bayesian learning networks, we found that the rehabilitation self-efficacy has the important predictors of the exercise anticipation in patients after knee surgeries for six months. Meanwhile, the results showed that the relationship of the self-efficacy, function score and exercise anticipation have been confirmed. The results showed that the function level and the rehabilitation self-efficacy were the important predictors of the exercise anticipation. In the future, the clinicians and therapists can improve the knee function by rehabilitation self-efficacy and exercise anticipation. Meanwhile, the study found that the sex, age, cause, economic, and education level have no relationship with the exercise anticipation in Bayesian learning networks. The level of exercise anticipation has the correlation of the knee joint angle in walking, which confirmed that has the correlation between the exercise anticipation and the protected ability in patients after knee surgeries for six months.
The effect of exercise anticipation has been confirmed in athletes and teenagers. By improving the ability on exercise anticipation, the player’s competitions would be enhanced significantly, especially i badminton, tennis, and opponent events.38,39 Self-efficacy has been used in different fields, such as self-management of chronic diseases.40 But the study of the exercise anticipation and the self-efficacy on patients with trauma is very scarce in the world. This is the first research of the exercise anticipation on patients with knee trauma.
Gait parameters have been called the “gold standard” in assessing the lower limb function.33 Our results showed that the exercise anticipation and knee joint angle in walking are the important predictors of the TUG in patients after knee surgeries over six months. This research confirmed that the objective indicators are consistent with the supervisor’s feelings in patients after knee surgeries over six months. In the process of rehabilitation, the doctors and therapists should pay attention to patient's feelings. But this is a preliminary work that needs confirmation by further study.
This study has some limitations. Firstly, the number of participants involved in this study is limited, so we cannot carry out a deeper analysis, for example, establishing parameter model. Secondly, owing to the lack of funding for study, we were unable to perform the total Bayesian inference in this research. Despite the above limitations, the results of this study were well supportive of the correlation in self-efficacy, function, and exercise anticipation in patients after knee surgeries for the long-term. Improving the exercise anticipation and rehabilitation self-efficacy is a valid method on the rehabilitation of patients after knee surgeries.
Conclusion
This study confirmed that improving the exercise anticipation and rehabilitation self-efficacy is an important method for enhancing the knee function in patients after knee surgeries over six months. The rehabilitation self-efficacy is the direct influencing predictor of exercise anticipation in patients after knee surgeries over six months. In the future, the long-term effect of the exercise anticipation and self-efficacy should be researched.
Data Sharing Statement
The data sets generated and analyzed during the current study are not publicly available because the Ethical Guidelines for Epidemiological Research by the Chinese Government prohibit researchers from providing their research data to other third-party individuals.
Ethics Approval and Consent to Participant
The current study was approved by the Institutional Ethical Review Board of Tianjin Hospital (No. TJYY-2020-YLS-086) and has been conducted in accordance with the Ethical Guidelines for Epidemiological Research by the Chinese Government and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. All study participants provided written informed consent by the completion and submission of the survey.
Disclosure
The authors report no conflicts interests in this work.
References
1. Parvizi J, Jain N, Schmidt AH. Periprosthetic knee fractures. J Orthop Trauma. 2008;22:663–671. doi:10.1097/BOT.0b013e31816ed989
2. Parvizi J, Seel MJ, Hanssen AD, et al. Patellar component resection arthroplasty for the severely compromised patella. Clin Orthop Relat Res. 2002;396:356–361. doi:10.1097/00003086-200204000-00041
3. Johnston AT, Tsiridis E, Eyres KS, et al. Periprosthetic fractures in the distal femur following total knee replacement: a review and guide to management. Knee. 2012;19(3):156–162. doi:10.1016/j.knee.2011.06.003
4. Maestro A, Rodriguez L, Lopis JA. Periprosthetic knee fractures. Rev Ortop Traumatol Ed Lat Am. 2008;52:179–187.
5. Althausen PL, Lee MA, Finkemeier CG, et al. Operative stabilization of supracondylar femur fractures above total knee arthroplasty: a comparison of four treatment methods. J Arthroplasty. 2003;18:834–839. doi:10.1016/S0883-5403(03)00339-5
6. Schroder HM, Berthelsen A, Hassani G, et al. Cementless porous-coated total knee arthroplasty: 10-year results in a consecutive series. J Arthroplasty. 2001;16:559–567. doi:10.1054/arth.2001.23565
7. Della Rocca GJ, Leung KS, Pape HC. Periprosthetic fractures: epidemiology and future projections. J Orthop Trauma. 2011;25(2):66–70. doi:10.1097/BOT.0b013e31821b8c28
8. Holliday RC, Antoun M, Playford ED. A survey of goal-setting methods used in rehabilitation. Neurorehabilit Neural Repair. 2005;19(3):227–231. doi:10.1177/1545968305279206
9. Chen KH, Chen PC, Liu KC, et al. Wearable sensor-based rehabilitation exercise assessment for knee osteoarthritis. Sensors-Basel. 2015;15(2):4193–4211. doi:10.3390/s150204193
10. Amann M, Dempsey JA. Locomotor muscle fatigue modifies central motor drive in healthy humans and imposes a limitation to exercise performance. J Physiol. 2008;586(1):161–173. doi:10.1113/jphysiol.2007.141838
11. Podlog L, Dimmock J, Miller J. A review of return to sport concerns following injury rehabilitation: practitioner strategies for enhancing recovery outcomes. Phys Ther Sport. 2011;12:36–42. doi:10.1016/j.ptsp.2010.07.005
12. Norlin T, Tranaeus Fitzgerald U, Alricsson M. Barriers to and possibilities of returning to play after a severe soccer injury: a qualitative study. Eur J Physiother. 2016;18:179–184. doi:10.3109/21679169.2016.1174296
13. Levy AR, Polman RC, Clough PJ. Adherence to sport injury rehabilitation programs: an integrated psycho-social approach. Scand J Med Sci Sports. 2008;18:798–809. doi:10.1111/j.1600-0838.2007.00704.x
14. Krustrup P, Nielsen JJ, Krustrup BR, et al. Recreational soccer is an effective health-promoting activity for untrained men. Br J Sports Med. 2009;43:825–831. doi:10.1136/bjsm.2008.053124
15. Chan DK, Hagger MS. Self-determined forms of motivation predict sport injury prevention and rehabilitation intentions. J Sci Med Sport. 2012;15:398–406. doi:10.1016/j.jsams.2012.03.016
16. Bandura A. Self-efficacy: toward a unifying theory of behavior change. Psychol Rev. 1977;84(2):191–215. doi:10.1037/0033-295X.84.2.191
17. Lev EL. Bandura’s theory of self-efficacy: applications to oncoIogy. Sch Inq Nurs Pract. 1997;11:21–37.
18. Bandura A. Cognitive regulators. In: Bandura A, editor. Social Foundations of Thought and Action: A Social Cognitive Theory. Englewood Cliffs, NJ: Prentice-Hall; 1986:467–480.
19. Newell AM, Van Swearingen JM, Hile E, et al. The modified gait efficacy scale: establishing the psychometric properties in older adults. Phys Ther. 2012;92(2):318–328. doi:10.2522/ptj.20110053
20. An X, Zhang XL, Liu Y, et al. Validation of the Chinese version of the modified Gait Efficacy scale for patients removing Ilizarov external fixation device for over one year. Patient Perfer Adher. 2020;14:1307–1315. doi:10.2147/PPA.S250440
21. Waldrop D, Lightsey OR, Ethington CA, et al. Self-efficacy, optimism, health competence and recovery from orthopedic surgery. J Couns Psychol. 2007;48:233–238. doi:10.1037/0022-0167.48.2.233
22. Wang HY, Hu YL, Hu SL, et al. The reliability and validity assessment of the Chinese version rehabilitation self-efficacy scale. Chin J Mod Nurs. 2014;20(3):268–270.
23. Resnick B, Palmer MH, Jenkins LS, et al. Path analysis of efficacy expectations and exercise behavior in older adults. J Adv Nurs. 2000;31(6):1309–1315. doi:10.1046/j.1365-2648.2000.01463.x
24. Lee LL, Perng SJ, Ho CC, et al. A preliminary reliability and validity study of the Chinese version of the self-efficacy for exercise scale for older adults. Int J Nurs Stud. 2009;46(2):230–238. doi:10.1016/j.ijnurstu.2008.09.003
25. Gioe TJ, Pomeroy D, Suthers K, et al. Can patients help with long-term total knee arthroplasty surveillance? Comparison of the American Knee Society Score self-report and surgeon assessment. Rheumatology (Oxford). 2009;48(2):160–164. doi:10.1093/rheumatology/ken439
26. Insall JN, Dorr LD, Scott RD, et al. Rationale of the Knee Society clinical rating system. Clin Orthop Relat Res. 1989;24(8):13–14.
27. Medalla GA, Moonot P, Peel T, et al. Cost-benefit comparison of the Oxford Knee score and the American Knee Society score in measuring outcome of total knee arthroplasty. J Arthroplasty. 2009;24:652–656. doi:10.1016/j.arth.2008.03.020
28. Bremner-Smith AT, Ewings P, Weale AE. Knee scores in a ‘normal’ elderly population. Knee. 2004;11:279–282. doi:10.1016/j.knee.2003.06.001
29. Lingard EA, Katz JN, Wright RJ, et al. Validity and responsiveness of the Knee Society Clinical Rating System in comparison with the SF-36 and WOMAC. J Bone Joint Surg Am. 2001;83:1856–1864. doi:10.2106/00004623-200112000-00014
30. Damsted C, Nielsen RO, Larsen LH. Reliability of video-based quantification of the knee and hip angle at foot strike during running. Int J Sports Phys Ther. 2015;10:147–154.
31. Damsted C, Larsen LH, Nielsen RO. Reliability of video-based identification of foot strike pattern and video time frame at initial contact in recreational runners. Gait Posture. 2015;42:32–35. doi:10.1016/j.gaitpost.2015.01.029
32. Lee SH, Han JH, Jin YY, et al. Poor physical fitness is independently associated with mild cognitive impairment in elderly Koreans. Biol Sport. 2016;33:57–62. doi:10.5604/20831862.1185889
33. Mirelman A, Weiss A, Buchman AS, et al. Association between performance on timed up and go sub-tasks and mild cognitive impairment: further insights into the links between cognitive and motor function. J Am Geriatr Soc. 2014;62:673–678. doi:10.1111/jgs.12734
34. Browne MW, Cudeck R. Alternative Ways of Assessing Model Fit: Testing Structural Equation Models. Newbury Park: Sage Publications; 1993:136–162.
35. Terwee CB, Bot SD, de Boer MR, et al. Quality criteria were proposed for measurement properties of health status questionnaires. J Clin Epidemiol. 2007;60:34–42. doi:10.1016/j.jclinepi.2006.03.012
36. Lim SS, Vos T, Flaxman AD, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the global burden of disease study. Lancet. 2013;380:2224–2260. doi:10.1016/S0140-6736(12)61766-8
37. Eggers KM, Ellenius J, Dellborg M, et al. Artificial neural network algorithms for early diagnosis of acute myocardial infarction and prediction of infarct size in chest pain patients. Int J Cardiol. 2007;114:366–374. doi:10.1016/j.ijcard.2005.12.019
38. Fernández-Granero MA, Sánchez-Morillo D, León-Jiménez A, et al. Automatic prediction of chronic obstructive pulmonary disease exacerbations through home telemonitoring of symptoms. Biomed Mater Eng. 2014;24:3825–3832.
39. Bates DW, Saria S, Ohno Machado L, et al. Big data in healthcare: using analytics to identify and manage high-risk and high-cost patients. Health Affair. 2014;33:1123–1131. doi:10.1377/hlthaff.2014.0041
40. Rehm J, Baliunas D, Borges GLG, et al. The relation between different dimensions of alcohol consumption and burden of disease: an overview. Addiction. 2010;105:817–843. doi:10.1111/j.1360-0443.2010.02899.x
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.