Back to Journals » Therapeutics and Clinical Risk Management » Volume 21
The Relationship Between the Time Until Penile Fracture Repair and Post-Operative Erectile Dysfunction
Received 6 April 2025
Accepted for publication 3 August 2025
Published 11 August 2025 Volume 2025:21 Pages 1249—1258
DOI https://doi.org/10.2147/TCRM.S527293
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Garry Walsh
Yekta Bıçak,1 Onur Dede2
1Urology, Diyarbakır Gazi Yaşargil Education Research Hospital, Diyarbakır, Turkiye; 2Urology, Dicle University Faculty of Medicine Hospital, Diyarbakır, Turkiye
Correspondence: Yekta Bıçak, Email [email protected] Onur Dede, Email [email protected]
Aim: Although penile fracture is a rare condition, the damage it may cause afterwards is challenging for patients. We aimed to investigate the relationship between late presentation to the hospital and the frequency of erectile dysfunction (ED) in patients with penile fractures.
Methods: In our cross-sectional, retrospective study, the frequency and severity of ED were calculated according to the International Index of Erectile Function (IIEF) scoring in patients with penile fracture admitted to Dicle University Hospital in the inter-operative period between the event and the operation and the subsequent controls. The relationship between these two conditions was analysed.
Results: Forty-six patients who met the inclusion criteria were included in our study. The mean age was 37 (28– 46) years. The mean preoperative IIEF was 25 (20– 28), and the mean postoperative IIEF was 21.3 (15– 27). The mean event-operation time was 9 (6– 15) hours. The rate of sexual intercourse was 50%, trauma was 30%, development after masturbation was 11%, and other causes were 9%.
Conclusion: Penile fracture is a real urological emergency, and as urologists, we need to intervene as early as possible in patients experiencing this condition. We found that patients who presented to the hospital more than 12.5 hours after penile fracture had a significantly higher risk of developing ED or worsening ED in the subsequent period.
Keywords: urological surgery, penile fracture, erectile dysfunction
Introduction
Penile erection is a complex psychoneurovascular event involving smooth muscle relaxation, increased arterial inflow, and reduced venous outflow. This process relies on the coordinated action of neuromodulators, smooth and striated muscles, and the tunica albuginea. The penis is primarily supplied by the internal pudendal artery, with contributions from pelvic arterial branches.1
In the flaccid state, cavernosal and arterial wall smooth muscles maintain low blood flow and oxygen pressure (PO2 ≈ 35 mmHg). Following sexual stimulation, neurotransmitters released from cavernosal nerves relax these muscles, leading to arteriole dilation, sinusoidal expansion, and blood entrapment. This causes the corpus cavernosum to expand and elongate, while venous outflow is restricted by compression of the tunica albuginea and emissary veins. Full erection is achieved when PO2 rises and intracavernosal pressure reaches ~100 mmHg. Rigid erection occurs when pressure exceeds 100 mmHg due to contraction of the ischiocavernosus muscles.2
Detumescence unfolds in three stages: initial pressure rise due to smooth muscle contraction (onset), gradual pressure decline as venous outflow resumes (slow), and rapid pressure drop as full venous drainage occurs (rapid phase).3
Erectile dysfunction (ED) is defined as the inability to achieve or maintain an erection sufficient for sexual intercourse. The term replaced “impotence” following its adoption by the NIH in 1992.4 ED affects approximately 20 million men globally. Prevalence increases with age, with 40% of men over 50 affected, yet only 5% seek medical help.5 In the US, ED rates range between 32–52%,6 while a study in Türkiye reported a prevalence of 69.2%.7
ED is classified into three categories: organic, psychogenic, and mixed. Organic ED (70–75%) is linked to chronic diseases, aging, medications, surgeries, smoking, alcohol, or trauma. Psychogenic ED (10–30%) mainly affects younger individuals and is triggered by psychological issues such as performance anxiety or relationship difficulties. Mixed ED involves both components.8
Diagnosis begins with thorough history-taking and physical examination to avoid unnecessary tests. Tools such as the International Index of Erectile Function (IIEF) are used to evaluate severity. The IIEF-5, widely used in clinical settings, categorizes ED severity based on a 30-point scale.9 Diagnostic tests like the Nocturnal Penile Tumescence and Rigidity Test (NPTR) help differentiate organic from psychogenic causes and are considered the gold standard.10
Treatment begins with lifestyle changes targeting reversible risk factors. Psychological therapy is recommended when mental health plays a role. Hormonal imbalances such as hypogonadism or hyperprolactinaemia are addressed with hormone therapy.11,12
First-line pharmacological treatment includes PDE-5 inhibitors (sildenafil, vardenafil, tadalafil), which enhance erection via the NO–cGMP pathway. Sildenafil and vardenafil last ~4 hours, while tadalafil is effective for up to 36 hours.13–15 Additional options include intraurethral alprostadil (MUSE) and intracavernosal injections, though side effects limit their use.16
Vacuum erection devices are non-invasive alternatives that use negative pressure to increase penile blood flow but may cause discomfort during ejaculation.17 Surgical interventions, such as correcting venous leaks, arterial revascularisation, or implanting penile prostheses, are considered when other treatments fail. Three-piece prostheses offer high satisfaction rates and natural results.18
Penile fracture is a rupture of the tunica albuginea in an erect penis, typically caused by sudden blunt trauma during sexual activity, vigorous masturbation, or direct impact. While conservative treatment may lead to complications like fibrosis, erectile dysfunction (ED), and plaque formation, early surgical intervention generally yields more effective outcomes. The injury triggers an inflammatory cascade involving lymphocytes, basophils, and monocytes, which induces oxidative stress, endothelial damage, and long-term fibrotic changes.19,20
This rare urological emergency was first described by Dr. Abul Kasem nearly 1000 years ago. Its incidence ranges from 1 in 100,000 to 1 in 1,000,000, with higher reporting rates in North America.21 It commonly occurs during sexual intercourse, particularly in positions like “woman on top”, which are associated with increased fracture risk.22
Diagnosis is primarily clinical, based on the patient’s report of a sudden cracking sound, pain, loss of erection, and penile swelling or bruising. Ruptures are often unilateral (1–3 cm), and if Buck’s fascia is torn, hematoma may spread to the scrotum and perineum. A firm, immobile hematoma—known as the “rolling sign”—can often be palpated.23 Urethral injury occurs in ~10% of cases, with increased risk in bilateral cavernosal tears. Urethral bleeding may also be present.24
Ultrasound is a cost-effective, non-invasive diagnostic tool with an 86% detection rate for tunica tears. However, it may miss subtle injuries. More advanced imaging techniques like Doppler ultrasound and MRI are preferred for their superior accuracy.25
Treatment is usually surgical unless the injury is very minor and non-disruptive. Conservative therapy (cold application, compression, anti-inflammatory drugs) is rarely recommended today due to the risk of long-term complications. Since the 1980s, surgery has become the standard approach, particularly to prevent ED, plaque, or vascular fistulas.26
Surgical Options Include
- Vertical penile incision for localized access while preserving neurovascular structures.
- Sub-coronal degloving incision, which allows full exposure of the corpus and urethra, preferred if urethral damage is suspected, despite higher risk of edema or necrosis.
- If urethral injury is ruled out, a catheter is placed, hematomas are drained, and bleeding vessels are ligated. In arterial injuries, microsurgical repair may be performed.26
Postoperative care includes pain control, antibiotics, rest, and avoidance of sexual activity for 4–6 weeks. Hormonal therapy may be used temporarily to suppress erections. Follow-up over 6 months includes physical exams, symptom evaluation, and use of the IIEF-5 or IIEF-15 to assess erectile function.27
The main aim of this study was to investigate the relationship between the time from the time of the incident to hospital admission and the development of postoperative ED in patients with penile fractures.
Materials Methods
In the study, 52 penile fracture patients admitted to the Urology Outpatient Clinic or Emergency Department of Dicle University Hospital between 01.01.2017 and 01.03.2023 were analyzed. Since the surgical procedures and follow-up process were conducted retrospectively, the Dicle University Faculty of Medicine Clinical Research Ethics Committee waived the requirement for written informed consent. After excluding one patient who refused to participate in the study, one patient who could not be reached and four patients with bilateral penile fracture and urethral injury, the remaining 46 patients were included in the study. All patient data has been anonymised prior to analysis in accordance with corporate and ethical principles to ensure confidentiality. The patients were divided into two groups according to the duration of hospitalization as above and below 12.5 hours. These groups were compared in terms of preoperative and postoperative characteristics and IIEF scores.
Patients who were not included in the study included those who refused to participate, those who did not have the knowledge and skills to complete the questionnaires, those who underwent surgery other than penile fracture, and those with urethral injury accompanying penile fracture. During follow-up examinations, physical examination, anamnesis, routine preoperative blood analysis and IIEF questionnaires were performed.
The questionnaires included a 7-question sociodemographic form including patients’ age, gender, education level, chronic diseases and regular medication use. In addition, the International Index of Erectile Function (IIEF-15) was used to assess ED. Using the Turkish version of this questionnaire, the first five questions and question 15 were used to assess erectile function. The other questions were related to orgasmic function, sexual desire, sexual satisfaction and general satisfaction. The IIEF questionnaire we applied in the preoperative period was applied immediately after the physical examination. Postoperative IIEF tests were administered at the third visit after discharge (sixth month follow-up).
Patients were diagnosed by physical examination and USG when necessary. All patients included in the study underwent the same surgical protocol and the mean operation time was 30–60 minutes. There was no patient with an outlier operation time; therefore, operation times were not used in comparisons. The preoperative blood samples were not specific blood values and were routinely used in all surgical patients; therefore, we did not use blood parameters in the comparisons.
Data analysis was performed using IBM SPSS Statistics 25.0 program. Descriptive statistics were presented as mean ± standard deviation, median (minimum-maximum), frequency and percentage (%). The distribution characteristics of the data were evaluated by Kolmogorov–Smirnov test. Independent sample t test was used to analyze parametric data. Pearson’s Chi-square test and Fisher’s Exact test were used when appropriate for the comparison of categorical variables. When determining the cut-off value in ROC curve analysis, the point where the sensitivity and specificity are closest and highest, known as “optimal cut-off at sensitivity = specificity”, was selected. In all analyses, p ≤ 0.05 was accepted as the limit of statistical significance.
Results
The mean age of the 46 patients was 37 years. Comorbidities and risk factors such as hypertension, diabetes, smoking, and previous surgeries were generally low. Most patients were not using any regular medications, and none had a history of alcohol use or oncologic treatment. The average preoperative IIEF score was 25, with nearly half of the patients having no ED. The most common cause of fracture was sexual intercourse, followed by trauma. Pain was the most frequent presenting symptom. Fractures were most often located proximally and more commonly occurred on the right side. The median time from injury to surgery was 9 hours (Table 1).
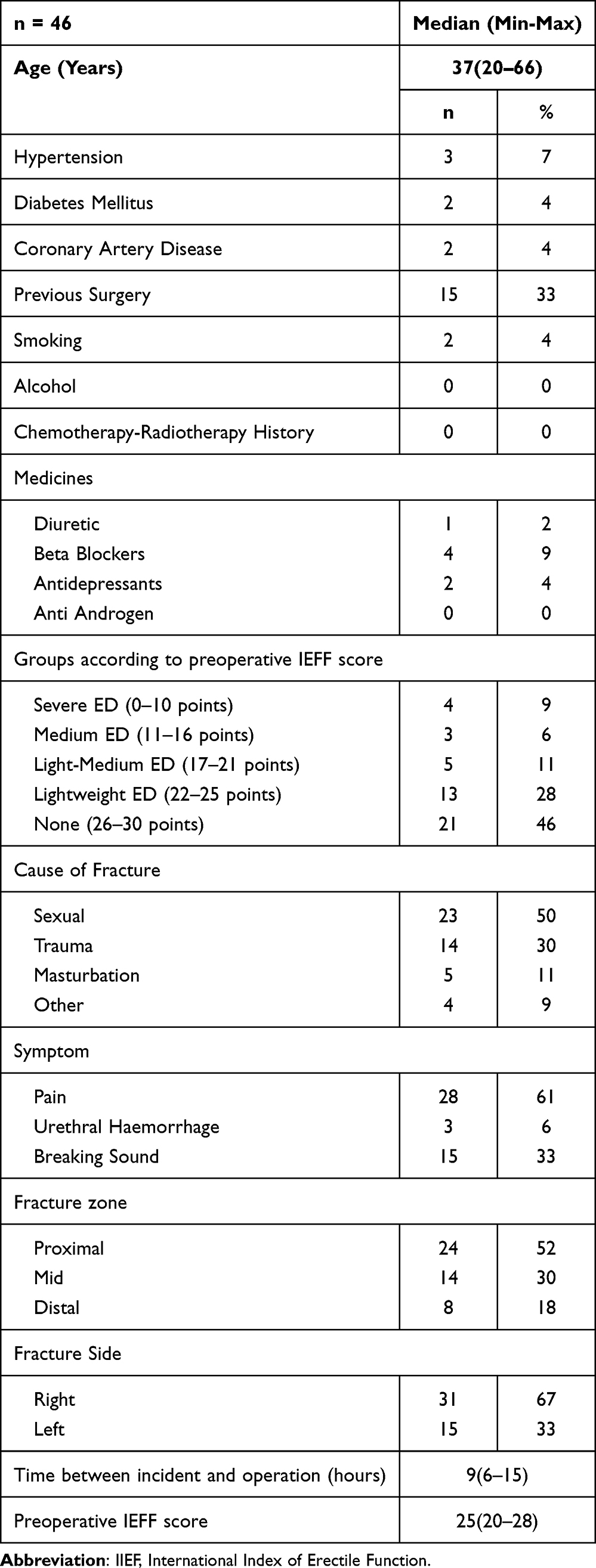 |
Table 1 General Demographic Characteristics of the Patients |
At the sixth postoperative month, 36% of patients had normal erectile function, while severe ED was observed in 13%. A significant negative correlation was found between postoperative IIEF scores and both diuretic use (p = 0.023) and the time from injury to surgery (p = 0.003). No other patient characteristics showed a statistically significant association with postoperative erectile function (Table 2).
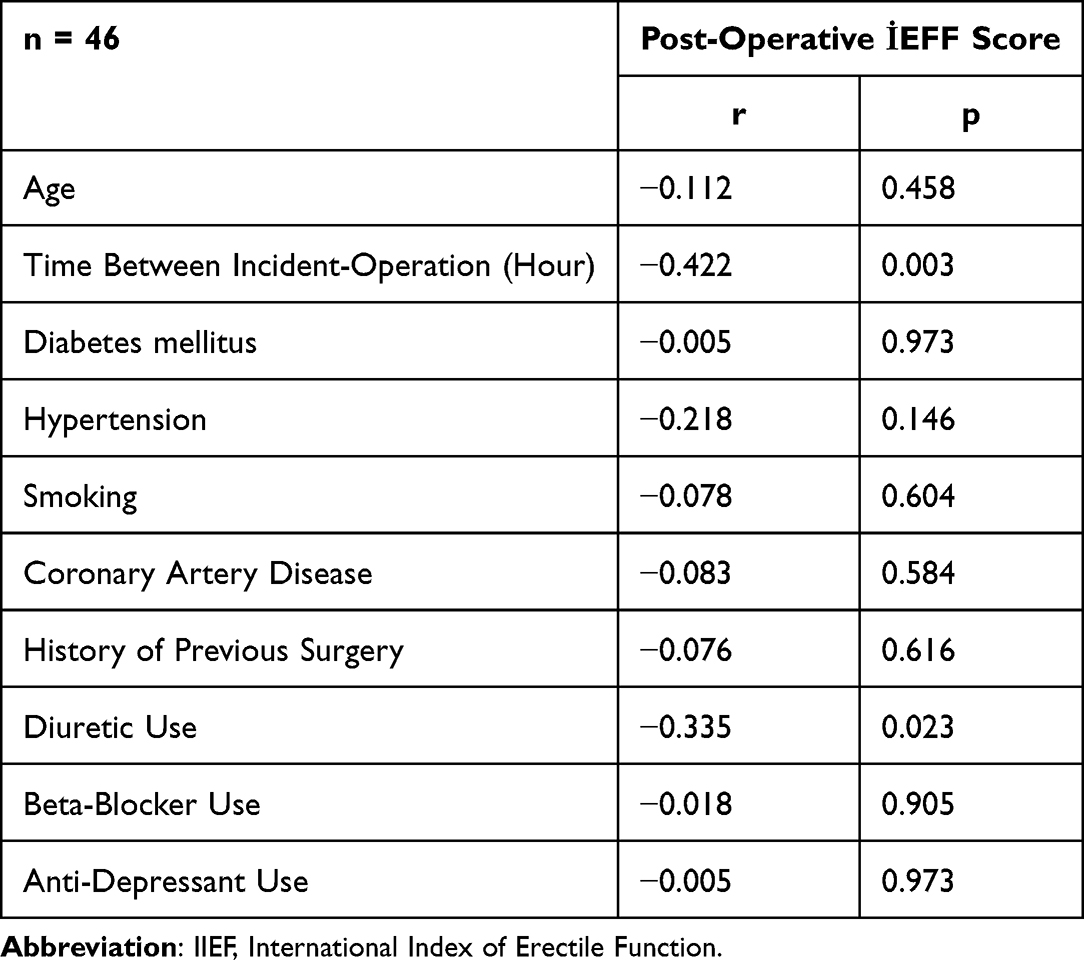 |
Table 2 Correlation Analysis of Postoperative IIEF Scores with Patient Characteristics |
When patients were grouped based on the presence or absence of ED at the sixth postoperative month, a significantly longer time between injury and surgery was associated with ED (p = 0.010). Additionally, the presence of typical symptoms at presentation was significantly associated with the development of ED (p=0.029). No other variables, including age, comorbidities, medication use, or fracture characteristics, showed a significant difference between groups (Table 3).
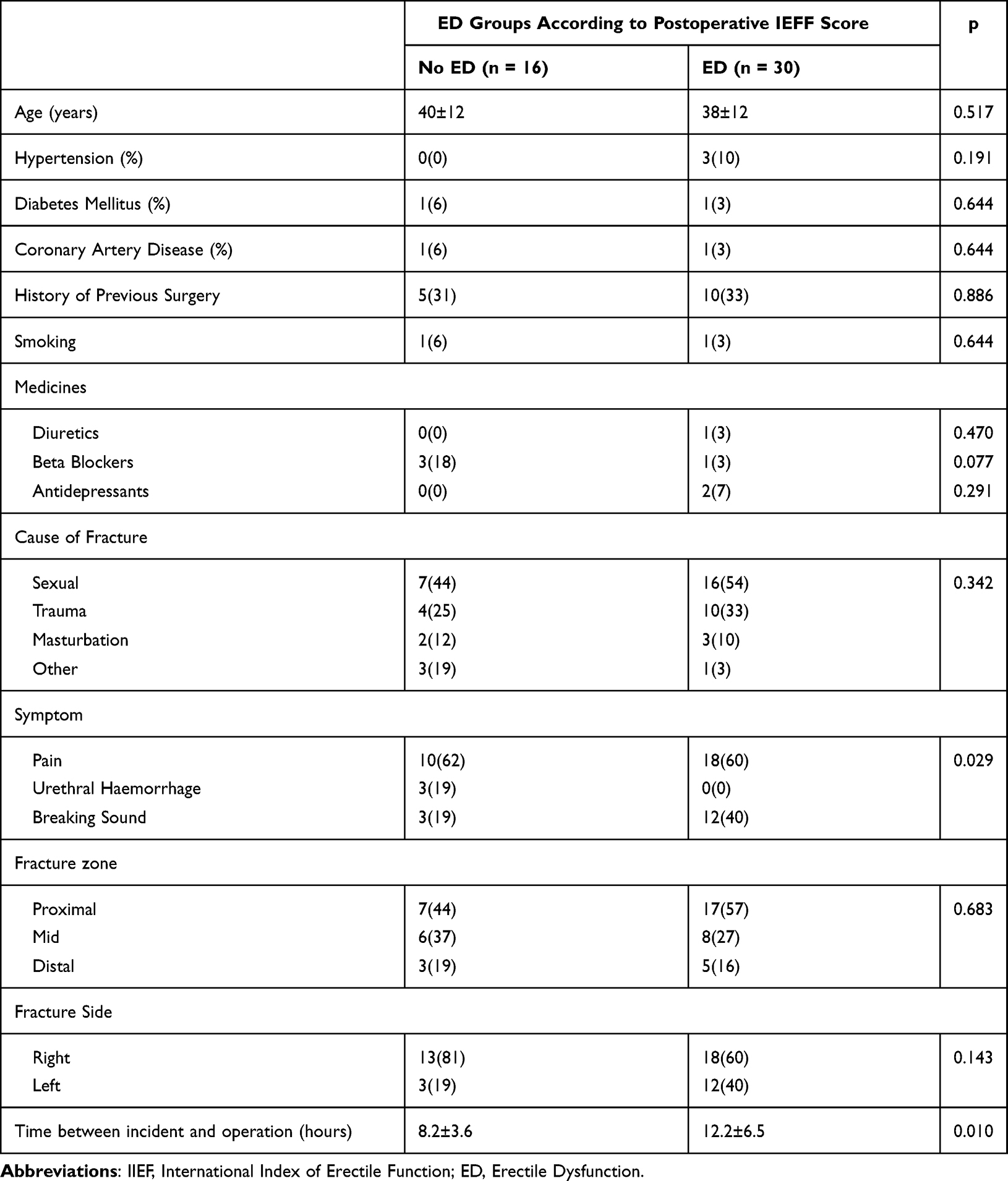 |
Table 3 Association of Postoperative IIEF Score with Other Conditions |
Patients were grouped based on a 12.5-hour cut-off time between injury and surgery, determined using ROC curve analysis. A significant association was found between early presentation and right-sided fractures (p = 0.024). Additionally, lower preoperative IIEF scores were linked to delayed hospital admission (p = 0.028). The most notable finding was that patients with a surgery delay longer than 12.5 hours had significantly lower postoperative IIEF scores (p<0.001). No other variables were significantly associated with the timing of surgery (Table 4).
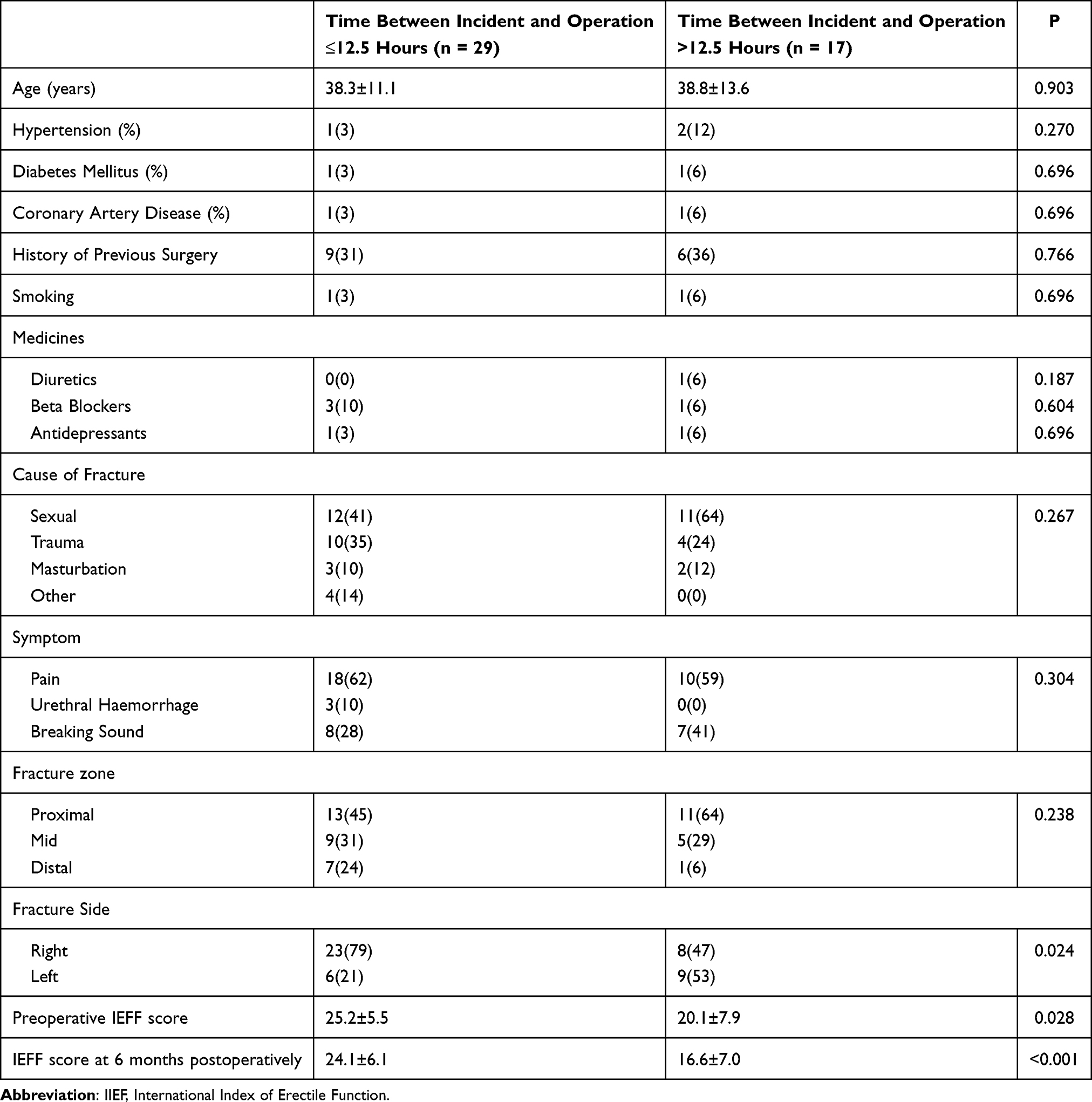 |
Table 4 The Relationship Between the Variables and the Time Between the Incident and the Operation |
ROC curve analysis showed that an event-to-operation time of 8.5 hours did not significantly predict the presence of postoperative ED (p = 0.051). However, a cut-off value of 12.5 hours was significantly associated with the development of severe ED, with a sensitivity of 83% and specificity of 70% (p = 0.038) (Figure 1).
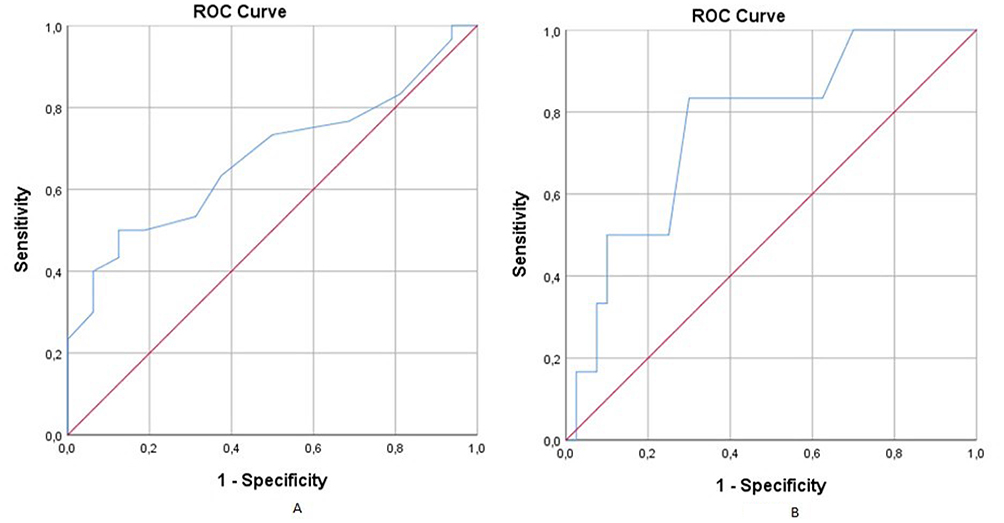 |
Figure 1 ROC curves showing the presence or absence of ED according to the time between the event and Operation. (A) It shows the detection of ED when the cut-off value of time between event and operation is accepted as 8.5 hours. AUC: 0.676, 95% CI (0.522–0.830) Sensitivity 63%, Specificity 63% (p = 0.051). (B) It shows the detection of severe ED when the cut-off value of time between event and operation is accepted as 12.5 hours. AUC: 0.765, 95% CI (0.572–0.957) Sensitivity 83%, Specificity 70% (p = 0.038).). |
Discussion
In humans, sexual response is organised by neurological, hormonal and vascular interactions depending on the stimuli. Stimulus-dependent sexual desire can be roughly described as plateau phase, orgasm and resolution. Disruption in any of these steps causes sexual dysfunction. Sexual dysfunction in men is called ED.
There is a frequent association between ED and hypertension (HT). HT predisposes ED with decreased nitric oxide (NO) production and increased oxidative stress. In addition, antihypertensive drugs may also increase the risk of ED. While ED is observed in 40% of patients diagnosed with HT, this rate is around 20% in patients who do not use drugs.28 In our study, the association of HT was low at 7% because of the young patient population. Similarly, coronary artery disease (CAD) is also associated with ED. Endothelial dysfunction is found in 80% of patients with ED, and the risk of experiencing a cardiovascular event within 5 years increases in these patients.29 In our study, the association of CAD was found to be 4% because the population was young.
Penile fracture is characterised by tearing of the tunica albuginea as a result of blunt trauma to the erect penis. The incidence is approximately 1/100.000 to 1/1.000.000. While the tunica albuginea has an average thickness of 2 mm in a flaccid penis, it becomes thinner up to 0.25–0.5 mm in erection and becomes sensitive to trauma.30
In the literature, the most common cause of penile fracture is trauma during sexual intercourse (33–60%) (20,26). In our study, this rate was found to be 50%, which is compatible with other studies. Especially positions in which the woman is on top, and the “dog-style” position are factors that increase the risk of trauma.31 Other reasons include complex penile manipulation for detumescence, which is common in Middle Eastern societies. In a study conducted in Turkiye, it was reported that this condition caused penile fracture with a rate of 59.45%.32 In our study, this cause was found to be 9%. In addition, forced masturbation was found in 11% and trauma in 30%.
In penile fracture, the injury is usually unilateral and urethral injury is rare. In the literature, the rate of bilateral penile fracture and urethral injury varies between 10–20%.33 This rate was reported as 3% in Japanese studies,34 28% in British studies35 and 35% in a study conducted in Iran.36 In our study, four patients (8%) with bilateral fracture and urethral injury were excluded. This finding is consistent with other studies and shows urethral injury is a rare but important complication.
Although penile fracture is a urological emergency, late presentation of patients due to embarrassment increases the risk of complications. In a study conducted in Turkiye, the mean presentation time was reported to be 9 hours.32 Similarly, the mean presentation time in our study was 9 hours. The mean age of the patient group was generally low (37 in our study), which decreases the rates of concomitant chronic diseases and drug use.
The frequency of ED after penile fracture varies between 53–68% in patients treated conservatively.37,38 Therefore, conservative treatment is not recommended except for minimal ruptures and surgical intervention is preferred. The risk of fibrosis and ED is higher after conservative treatment compared to surgical treatment.
In penile fracture patients, International Index of Erectile Function (IIEF) scoring is evaluated preoperatively and postoperatively (usually 6 months). In the literature, the mean preoperative IIEF score ranged between 22 and 26.9, while the postoperative score was reported to range between 20 and 25.8.36,39,40 Our study’s mean preoperative IIEF score was 25, and the mean postoperative score was 21.3. These findings are compatible with other studies.
A significant correlation was found between the development of postoperative ED, the use of diuretics, and the time between the event and the operation. In addition, the risk of ED development was lower in patients with more symptoms, which was associated with their early presentation.
Our patients underwent surgery immediately after admission to the hospital. When the time between the event and the operation was analysed, no significant correlation was found between preoperative and postoperative IIEF scores based on 8.5 hours. However, this relationship became significant at 12.5 hours (Figure 1). In the literature, there are studies showing that surgeries performed up to 24 hours are not associated with the development or severity of ED.41 However, our study and some other studies show that delayed surgery increases the risk of ED.42
Conclusion
Penile fracture is a rare but urological emergency. Penile fracture is an important risk factor for ED, and therefore, surgical treatment should be considered as the first option. Given the late presentation of patients due to embarrassment, it is recommended not to delay surgical intervention after hospital admission. Every patient who is suitable for surgery should be operated immediately because prolongation of the process increases the risk of many complications, especially ED. The main conclusion of our study is that if the time between the event and surgical intervention exceeds 12.5 hours, the risk of developing ED or the severity of existing ED increases. Therefore, early surgical intervention in penile fracture plays a critical role in preventing long-term sexual dysfunction.
Ethics and Consent Statement
Our study was approved by Dicle University Faculty of Medicine Clinical Research Ethics Committee on 12.04.2023 with protocol number 285. The study protocol was designed in accordance with the Declaration of Helsinki.
Our study started retrospectively after the approval of the ethics committee and no written informed consent was obtained since both the operation and follow-up process of the patients were retrospective.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gratzke C, Angulo J, Chitaley K, et al. Anatomy, physiology, and pathophysiology of erectile dysfunction. J Sex Med. 2010;7(1 Pt 2):445–475. doi:10.1111/j.1743-6109.2009.01624.x
2. Sattar AA, Salpigides G, Vanderhaeghen JJ, et al. Cavernous oxygen tension and smooth muscle fibers: relation and function. J Urol. 1995;154(5):1736–1739. doi:10.1016/S0022-5347(01)66772-7
3. Bosch RJ, Benard F, Aboseif SR, et al. Penile detumescence: characterization of three phases. J Urol. 1991;146(3):867–871. doi:10.1016/S0022-5347(17)37950-8
4. NIH Consensus Development Panel on Impotence. NIH consensus conference: impotence. JAMA. 1993;270(1):83–90. doi:10.1001/jama.1993.03510010089036
5. Solstad K, Hertoft P. Frequency of sexual problems and dysfunction in middle-aged Danish men. Arch Sex Behav. 1993;22(1):51–58. doi:10.1007/BF01552912
6. Slag MR, Moreley EJ, Elson MK. Impotence in medical clinic outpatients. JAMA. 1983;249(13):1736. doi:10.1001/jama.1983.03330370046029
7. Turkish Erectile Dysfunction Prevalence Study Group; Akkus E, Kadıoğlu A, Esen A, et al. Prevalence and correlates of erectile dysfunction in Turkiye: a population-based study. Eur Urol. 2002;41(3):298–304. doi:10.1016/S0302-2838(02)00027-1
8. Lizza EF, Rosen RC. Definition and classification of erectile dysfunction: report of the nomenclature committee of the international society of impotence research. Int J Impot Res. 1999;11(3):141–143. doi:10.1038/sj.ijir.3900396
9. Rosen RC, Riley A, Wagner G, et al. The international index of erectile function (IIEF): a multidimensional scale for assessment of erectile dysfunction. Urology. 1997;49(6):822–830. doi:10.1016/S0090-4295(97)00238-0
10. Zou Z, Lin H, Zhang Y, Wang R. The role of nocturnal penile tumescence and rigidity (NPTR) monitoring in the diagnosis of psychogenic erectile dysfunction: a review. Sex Med Rev. 2019;7(3):442–454. doi:10.1016/j.sxmr.2018.10.005
11. Hatzichristou D, Rosen RC, Derogatis LR, et al. Recommendations for the clinical evaluation of men and women with sexual dysfunction. J Sex Med. 2010;7(1 Pt 2):337–348. doi:10.1111/j.1743-6109.2009.01619.x
12. Isidori AM, Buvat J, Corona G, et al. A critical analysis of the role of testosterone in erectile function: from pathophysiology to treatment—a systematic review. Eur Urol. 2014;65(1):99–112. doi:10.1016/j.eururo.2013.08.048
13. Kulkarni SS, Patil CS. Phosphodiesterase 5 enzyme and its inhibitors: update on pharmacological and therapeutical aspects. Methods Find Exp Clin Pharmacol. 2004;26(10):789–799. doi:10.1358/mf.2004.26.10.872561
14. Başar MM, Tuğlu D. PDE5 inhibitörlerinin karşılaştırmalı çalışması. Androloji Bülteni. 2005;21:99–102.
15. MUSE Study Group; Padma-Nathan H, Goldstein I, Payton T, et al. Treatment of men with erectile dysfunction with transurethral alprostadil (Medicated urethral system for erection, MUSE). N Engl J Med. 1997;336(1):1–7. doi:10.1056/NEJM199701023360101
16. Vrijhof HJ, Delaere KP. Vacuum constriction devices in erectile dysfunction: acceptance and effectiveness in patients with impotence of organic or mixed aetiology. Br J Urol. 1994;74(1):102–104. doi:10.1111/j.1464-410X.1994.tb16555.x
17. Lewis RW. Long-term results of penile prosthetic implants. Urol Clin North Am. 1995;22(4):847–856. doi:10.1016/S0094-0143(21)00698-4
18. Koifman L, Barros R, Júnior RA, Cavalcanti AG, Favorito LA. Penile fracture: diagnosis, treatment, and outcomes of 150 patients. Urology. 2010;76(6):1488–1492. doi:10.1016/j.urology.2010.05.043
19. Eke N. Fracture of the penis. Br J Surg. 2002;89(5):555. doi:10.1046/j.1365-2168.2002.02075.x
20. Wespes E, Libert M, Simon J, Schulman CC. Fracture of the penis: conservative versus surgical treatment. Eur Urol. 1987;13(3):166–168. doi:10.1159/000472765
21. Mahapatra TP, Kumar S. Reverse coitus: mechanism of urethral injury in male partner. J Urol. 1990;144(6):1467. doi:10.1016/S0022-5347(17)39770-7
22. Garaffa G, Raheem AA, Ralph DJ. Penile fracture and penile reconstruction. Curr Urol Rep. 2011;12(6):427–431. doi:10.1007/s11934-011-0201-5
23. Cumming J, Jenkins JD. Fracture of the corpora cavernosa and urethral rupture during sexual intercourse. Br J Urol. 1991;67(3):327. doi:10.1111/j.1464-410X.1991.tb15146.x
24. Uder M, Gohl D, Takahashi M, et al. MRI of penile fracture: diagnosis and therapeutic follow-up. Eur Radiol. 2002;12(1):113–120. doi:10.1007/s003300101051
25. Mydlo JH, Gershbein AB, Macchia RJ. Nonoperative treatment of patients with presumed penile fracture. J Urol. 2001;165(2):424–425. doi:10.1097/00005392-200102000-00017
26. Hatzichristodoulou G, Dorstewitz A, Gschwend JE, Herkommer K, Zantl N. Surgical management of penile fracture and long-term outcome on erectile function and voiding. J Sex Med. 2013;10(5):1424–1430. doi:10.1111/jsm.12107
27. Ekeke ON, Eke N. Fracture of the penis in the Niger Delta region of Nigeria. J West Afr Coll Surg. 2014;4(3):1–19.
28. Doumas M, Douma S. Sexual dysfunction in essential hypertension: myth or reality? J Clin Hypertens. 2006;8(4):269–274. doi:10.1111/j.1524-6175.2006.04708.x
29. Kirby M, Jackson G, Betteridge J, Friedli K. Is erectile dysfunction a marker for cardiovascular disease? Int J Clin Pract. 2001;55(9):614–618. doi:10.1111/j.1742-1241.2001.tb11141.x
30. Miller S, McAninch JW. Penile fracture and soft tissue injury. In: McAninch JW, editor. Traumatic and Reconstructive Urology. Philadelphia, PA: W.B. Saunders; 1996:693–698.
31. Agrawal SK, Morgan BE, Shafique M, et al. Experience with penile fractures in Saudi Arabia. Br J Urol. 1991;67(6):644–646. doi:10.1111/j.1464-410X.1991.tb15232.x
32. Eryıldırım B, Tahran F, Erbay E, Faydacı G, Şirin G, Kuyumcuoğlu U. Penil fraktür: etyoloji ve erken cerrahi tedavi. Androloji Bülteni. 2005;1304–6861.
33. Muentener M, Suter S, Hauri D, et al. Long-term experience with surgical and conservative treatment of penile fracture. J Urol. 2004;172(2):576–579. doi:10.1097/01.ju.0000131594.99785.1c
34. Sawh SLO, O’Leary MP, Ferreira MD, et al. Fractured penis: a review. Int J Impot Res. 2008;20(4):366–369. doi:10.1038/ijir.2008.12
35. Gupta N, Goyal P, Sharma K, et al. Penile fracture: role of ultrasound. Transl Androl Urol. 2017;6(3):580–584. doi:10.21037/tau.2017.03.38
36. Mirzazadeh M, Fallahkarkan M, Hosseini J. Penile fracture epidemiology, diagnosis, and management in Iran: a narrative review. Transl Androl Urol. 2017;6(2):158–166. doi:10.21037/tau.2016.12.03
37. Mydlo JH. Surgeon experience with penile fracture. J Urol. 2001;166(2):526–529. doi:10.1016/S0022-5347(05)65975-7
38. El-Bahnasawy MS, Gomha MA. Penile fractures: the successful outcome of immediate surgical intervention. Int J Impot Res. 2000;12(5):273–277. doi:10.1038/sj.ijir.3900571
39. Barros R, Schulze L, Ornellas AA, et al. Relationship between sexual position and severity of penile fracture. Int J Impot Res. 2017;29(5):207–209. doi:10.1038/ijir.2017.24
40. Kozacioglu Z, Ceylan Y, Aydogdu O, et al. An update of penile fractures: long-term significance of the number of hours elapsed until surgical repair on long-term outcomes. Turk J Urol. 2017;43(1):25–29. doi:10.5152/tud.2016.39129
41. Kozacioglu Z, Degirmenci T, Arslan M, Mehmet B, Bulent Y, Minareci S. Long-term significance of the number of hours until surgical repair of penile fractures. Urol Int. 2011;87(1):75–79. doi:10.1159/000325589
42. Koifman L, Cavalcanti AG, Manes CH, R Filho D, Favorito LA. Penile fracture: experience in 56 cases. Int Braz J Urol. 2003;29(1):359. doi:10.1590/S1677-55382003000100007
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.