Back to Journals » Clinical Interventions in Aging » Volume 18
The Relationship Between Sarcopenia, Cognitive Impairment, and Cerebral White Matter Hyperintensity in the Elderly
Authors Zhang K ![]() , Zhang K, Liu Q, Wu J
, Zhang K, Liu Q, Wu J
Received 13 January 2023
Accepted for publication 22 March 2023
Published 31 March 2023 Volume 2023:18 Pages 547—555
DOI https://doi.org/10.2147/CIA.S404734
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zhi-Ying Wu
Kangrui Zhang,1,2,* Kangdi Zhang,3,* Qiuwan Liu,2 Juncang Wu2
1Graduate School, Bengbu Medical College, Bengbu, 233000, People’s Republic of China; 2Department of Neurology, The Second People’s Hospital of Hefei, Hefei, 230000, People’s Republic of China; 3Graduate School, Anhui Medical University, Hefei, 230000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Juncang Wu, Department of Neurology, The Second People’s Hospital of Hefei, Hefei, 230000, People’s Republic of China, Email [email protected]
Purpose: To explore the relationship between sarcopenia-related indices, cognitive impairment and cerebral white matter hyperintensities.
Patients and methods: Ninety-five hospitalized older adults aged 60 years and older were used in this study. Three sarcopenia-related indicators were measured: hand grip strength (Measured with a spring-type dynamometer), gait speed (6m step speed method), and appendicular skeletal muscle mass (ASM, bioelectrical impedance). Sarcopenia was defined according to the Asian Working Group for Sarcopenia (AWGS) criteria. Cognitive function was assessed using Montreal Cognitive Assessment (MoCA). Cerebral white matter hyperintensity was assessed using 3.0T superconducting magnetic resonance imaging.
Results: In both men and women, these three indices of sarcopenia were significantly and negatively correlated with WMH grades, except for appendicular skeletal muscle mass and WMH grades in women. Scores on the MoCA scale were significantly positive correlated with grip strength, and ASM, both in men and women. After adjusting for confounders and WMHs, regression analyses showed an increased incidence of cognitive impairment in patients with sarcopenia relative to those without sarcopenia.
Conclusion: Lower sarcopenia-related indices were significantly associated with cognitive impairment. WMHs may be one of the factors linking sarcopenia and cognitive function.
Keywords: hand grip strength, gait speed, muscle mass, cognition, white matter hyperintensity
Introduction
Cognitive function in elderly people is highly related to Skeletal Muscle Health.1 Several recent studies have reported a correlation between either gait speed or handgrip strength and cognitive function.2–4 In 2013, Verghese et al proposed a new syndrome the “motoric-cognitive risk” (MCR) syndrome, which is a pre-dementia syndrome characterized by cognitive impairment and slow gait.5
The European Working Group on Sarcopenia (EWGSOP) first published a consensus on sarcopenia in 2010, defining sarcopenia as an age-related syndrome of decreased muscle mass, decreased muscle strength, and/or decreased somatic function.6 The Asian Working Group on Sarcopenia (AWGS) proposed in 2014, recommended the application of a bioelectrical impedance analyzer (BIA) to measure skeletal muscle content (ASM) in the extremities,7 and in 2019 the concept of possible sarcopenia, which is slower gait speed and lower grip strength.8
It has been shown that decreased gait speed and handgrip strength are associated with cerebral white matter hyperintensities (WMHs).9,10 A close association between cerebral WMHs and cognitive impairment has been reported in studies that also include meta-analyses.11–13 The above results suggest that sarcopenia may be mediated through WMHs leading to cognitive impairment. However, there are some studies that did not find a significant association between sarcopenia and cognitive impairment.14–17 In addition, few studies have assessed the potential mechanisms between sarcopenia and cognitive impairment.
Methods
Study Subjects
Inpatients attending the Department of Neurology at the Second People’s Hospital of Hefei, Anhui Medical University from June 2021 to October 2022 were recruited for the study. Inclusion criteria: (1) age between 60 and 85 years; (2) high signal in the white matter of the brain as indicated by cranial MRI; (3) ability to write and speak normally and to complete questionnaires; (4) freedom of movement and ability to complete gait and grip strength; (5) informed and agreed to participate in this study. Exclusion criteria: (1) Comorbid wasting disease, severe organ insufficiency, or symptomatic cardiovascular events, such as malignancy, gastrointestinal disease, coronary artery disease, etc; (2) Cannot perform grip strength, gait speed tests, or body composition measurements; (3) Recent history of surgery, trauma; (4) Inability to communicate and complete the scale properly for various reasons. The final sample available for analysis consisted of 95 participants (48 males and 47 females), excluding 32 subjects. 1 was unable to perform grip strength testing due to upper extremity disability; 4 were unable to measure gait speed and body composition due to intolerance of physical activity; 18 participants refused to participate in body composition or physical activity assessments for personal reasons; and 7 others were missing some covariates data. The participants were fully informed about the nature of the study and signed an informed consent form. This study was approved by the clinical trial ethics committee of the Second People’s Hospital of Hefei and conducted in accordance with the principles of the Declaration of Helsinki.
Measurement of Sarcopenia-Related Indices
Based on the diagnostic criteria of the Asian Working Group on Sarcopenia (AWGS), low muscle mass and low muscle strength, and/or poor physical performance are defined as sarcopenia.8
Appendicular Skeletal Muscle Mass (ASM)
Muscle mass was measured using bioelectrical impedance analysis (BIA) (Inbody 120, Korea). ASM is calculated as “skeletal muscle mass of the extremities/height squared”. Low muscle mass was defined as appendicular skeletal muscle mass (ASM) less than 7.0 kg/m2 and 5.7 kg/m2 in men and women, respectively.8
Physical Performance
Gait speed is the simplest, quickest and safest method of assessing physical performance. Participants were asked to walk 6 m at normal speed from a moving starting point and the time taken was recorded and the average time of the two trials was analyzed as the result. Low step speed is defined as <1.0 m/s.8
Muscle Strength
Muscle strength was assessed by measuring hand grip strength using a spring-type dynamometer (EH101; Camry, Zhongshan, China). Participants were asked to maximize isometric contraction force twice with their dominant hand and analyzed using the maximum readings. Low muscle strength was defined as grip strength <28 kg and <18 kg for men and women, respectively.8
Magnetic Resonance Imaging and Assessment of White Matter Hyperintensities
Fazekas visual grade scale18 was used to grade white matter hyperintensities. The cranial scans were performed using a 1.5T superconducting magnetic resonance imaging (MRI) machine (Siemens Avanto, Germany) with axial FLAIR (TE: 110 ms, TR: 9000 ms, flip angle (FA): 90, reversal time: 2400 ms, FOV: 14×23 cm, slice thickness: 5 mm), axial T2WI (TE: 85 ms, TR: 5000 ms, FA: 90 FOV: 14×23 cm, slice thickness: 5 mm), and coronal T2WI (TE: 85 ms, TR: 3500 ms, FA: 150, FOV: 20×20 cm, SL: 3 mm). All WMH data were collected under the supervision of certified neuroradiologists and in a manner that was blind to demographic, sarcopenic, and cognitive data. The Fazekas scoring system scores periventricular WMH (PVH) and deep subcortical WMH (DSH) bilaterally. For PVH: 0=no WMH; 1=capsule or pencil shaped around the lateral ventricle; 2=smooth halo at the lateral ventricle margin; 3=irregular high density extending into the deep white matter. For DSH: 0=no WMH; 1=dotted WMH lesions deep in the subcortex; 2=beginning confluence of WMH lesions; 3=large confluent areas. The PVH and DSH scores were summed to obtain the Fazekas score, ranging from 0 to 6. Fazekas were graded according to their scores: Level 0 (0 points); Level 1 (1 to 2 points); Level 2 (3 to 4 points); and Level 3 (5 to 6 points).
Assessment of Cognitive Function
Participants’ cognitive function was measured by an experienced neurologist using Montreal Cognitive Assessment (MoCA), which has high sensitivity and specificity characteristics in detecting mild cognitive impairment (MCI) and Alzheimer’s disease (AD).19 MOCA covers a wide range of cognitive domains, including attention and concentration, executive function, memory, language, visuospatial structure skills, abstract thinking, computation, and orienting power.19 Criteria for the presence of cognitive impairment: the illiterate group≤13 points, the elementary school group≤19 points, and the middle school and higher group≤24 points.20
Evaluation of Risk Factors
Patients’ cases were reviewed and information on age, gender, education, smoking and alcohol consumption, past medical history, medication history, and body mass index (BMI) was collected. Fasting venous blood was collected from patients in the morning to measure total cholesterol, triglyceride, High-density lipoprotein cholesterol (HDL), and fasting glucose. Height, weight, heart rate, and blood pressure measurements were performed by a trained nurse. Blood pressure and heart rate were measured after the participants had rested for at least 15 minutes in a seated position.
Statistical Analysis
The questionnaire data were entered and analyzed using Epidata 3.1 and SPSS 23.0, respectively. Continuous variables obeying normal distribution were described using mean ± standard deviation (x±s), and comparisons between groups were made by t-test or analysis of variance. Categorical variables were expressed as frequency (percentage) [n(%)], and dichotomous and unordered multi-categorical variables were compared between groups using the x2 test. Ordinal logistic regression was used to analyze the effect of different sarcopenia-related indices on cerebral white matter high signal. Binary logistic regression was used to analyze the effect of different sarcopenia-related indices and cerebral white matter hyperintensities on cognitive impairment. The test level was 0.05, and p<0.05 was considered a statistically significant difference.
Results
Participant Characteristics
Among the 95 participants (48 males and 47 females) who were available for analysis, 27 (28.4%) had cognitive impairment, of which 27.1% were males and 29.8% were females. The clinical characteristics of the study population by presence or absence of cognitive impairment are shown in Table 1. We found that members with cognitive impairment tended to be older, female, lighter in weight, and had a lower BMI (P<0.05, Table 1). In both men and women, sarcopenia-related indices, grip strength, gait speed, and ASM were significantly associated with cognitive impairment.
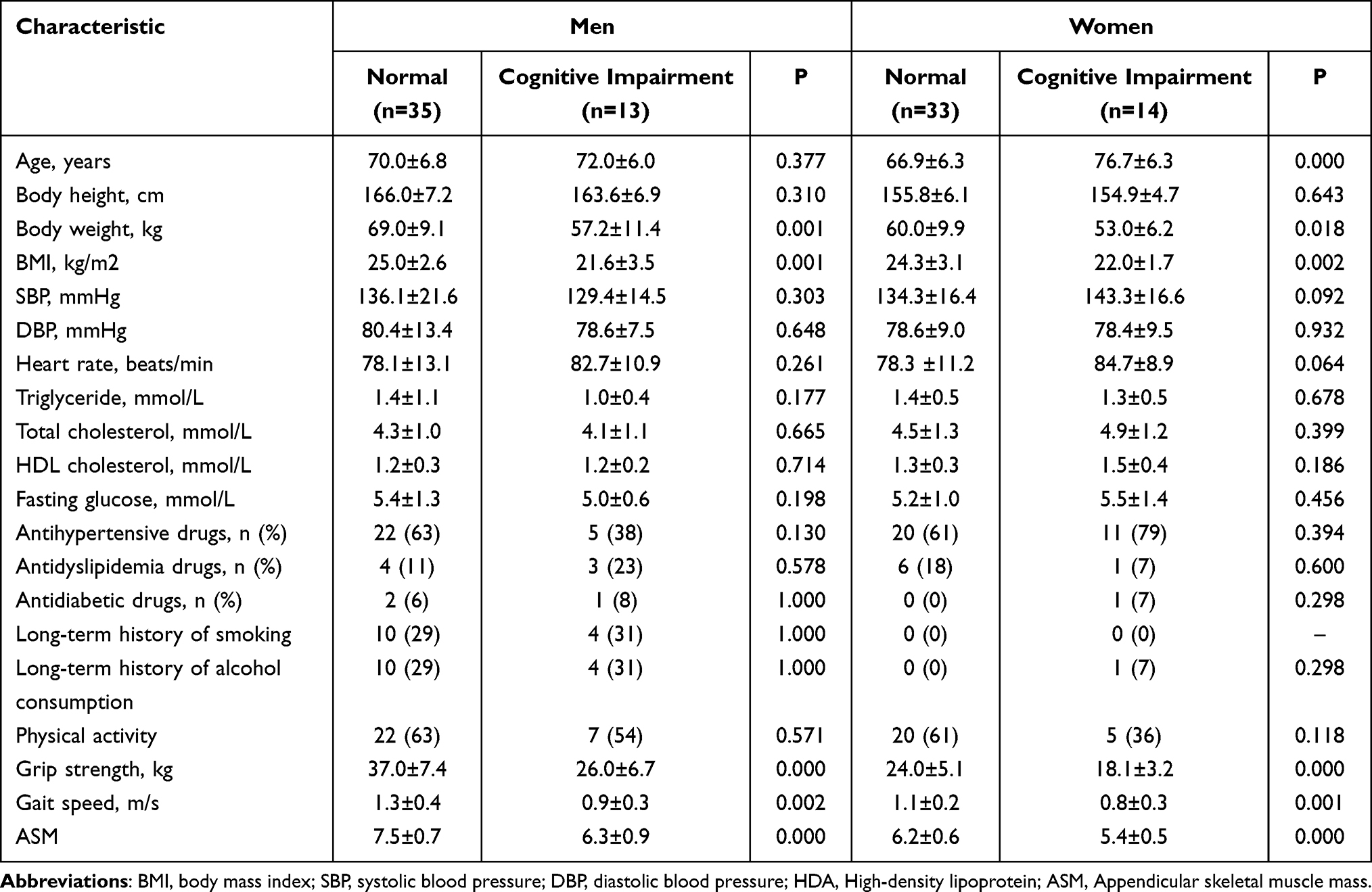 |
Table 1 Clinical Characteristics of Men and Women Study Participants by Presence or Absence of Cognitive Impairment |
Sarcopenic Indices and White Matter Hyperintensities
Figure 1 shows the grip strength, gait speed and appendicular skeletal muscle mass divided into 3 levels. In both men and women, these three indices of sarcopenia were significantly and negatively correlated with WMH grades, except for appendicular skeletal muscle mass and WMH grades in women. However, sarcopenia-related indices were not linearly related to WMH grades, especially gait speed in men and grip strength in women.
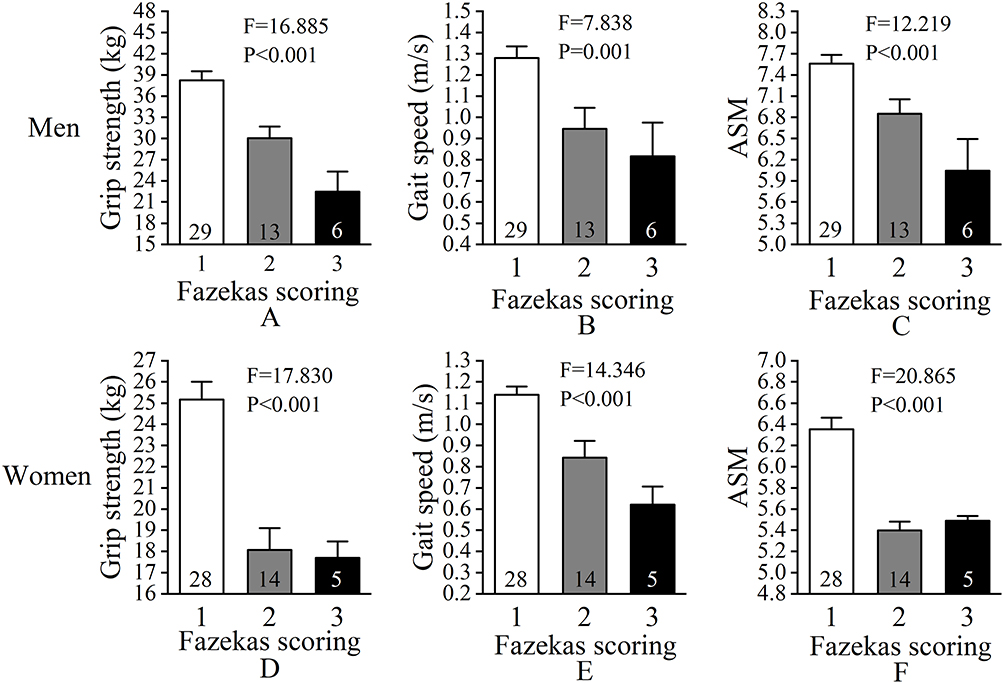 |
Figure 1 White matter hyperintensity and sarcopenic indices. The numbers in the columns indicate the number of subjects. Values are mean ± SEM. (A) The relationship between grip strength and WMHs in men. (B) The relationship between gait speed and WMHs in men. (C) The relationship between ASM and WMHs in men. (D) The relationship between grip strength and WMHs in women. (E) The relationship between gait speed and WMHs in women. (F) The relationship between ASM and WMHs in women. |
Odds ratios of sarcopenia-related indices for the presence of WMHs are shown in Table 2. Even after adjustment for possible confounders, the three sarcopenia-related indices were significantly associated with WMHs in women, whereas grip strength and ASM were significantly associated with WMHs in men.
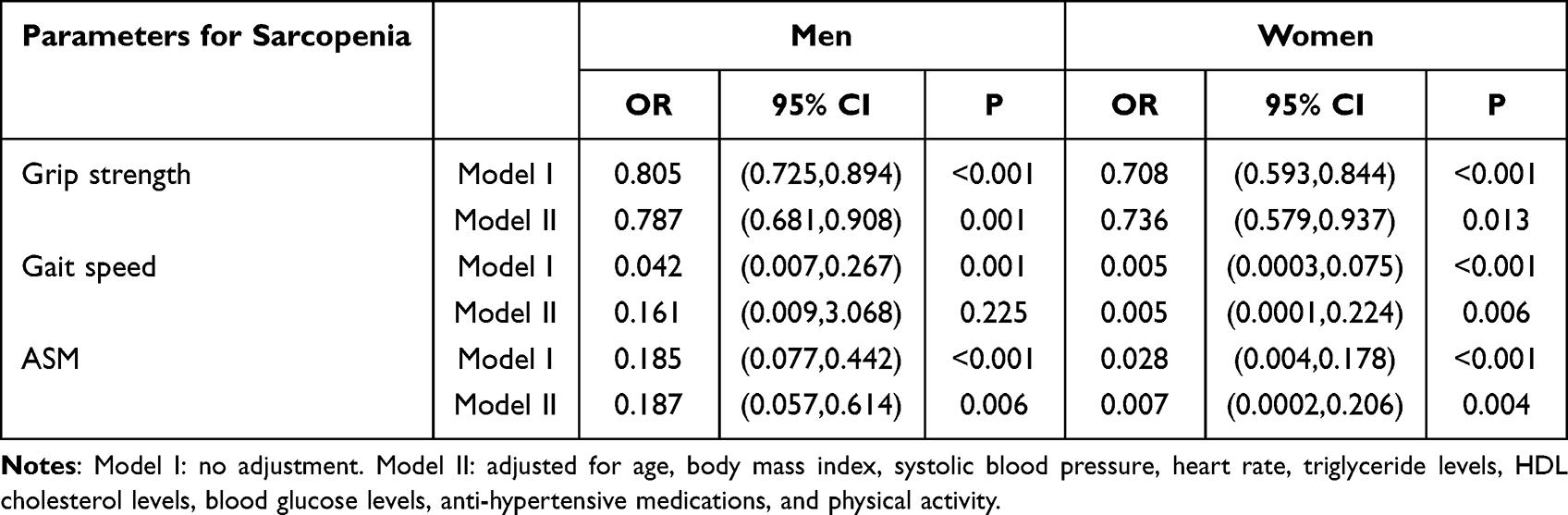 |
Table 2 Multifactorial Analysis of Various Indicators of Sarcopenia and White Matter Hyperintensities |
Sarcopenic Indices and Cognitive Impairment
Scores on the MoCA scale were significantly positive correlated with grip strength (men: r=0.543, P<0.001; women: r=0.332, p=0.023), gait speed (men: r=0.537, P<0.001; women: r=0.399, p=0.005), and ASM (men: r=0.524, P=P<0.001; women: r=0.418, p=0.003), both in men and women (Figure 2).
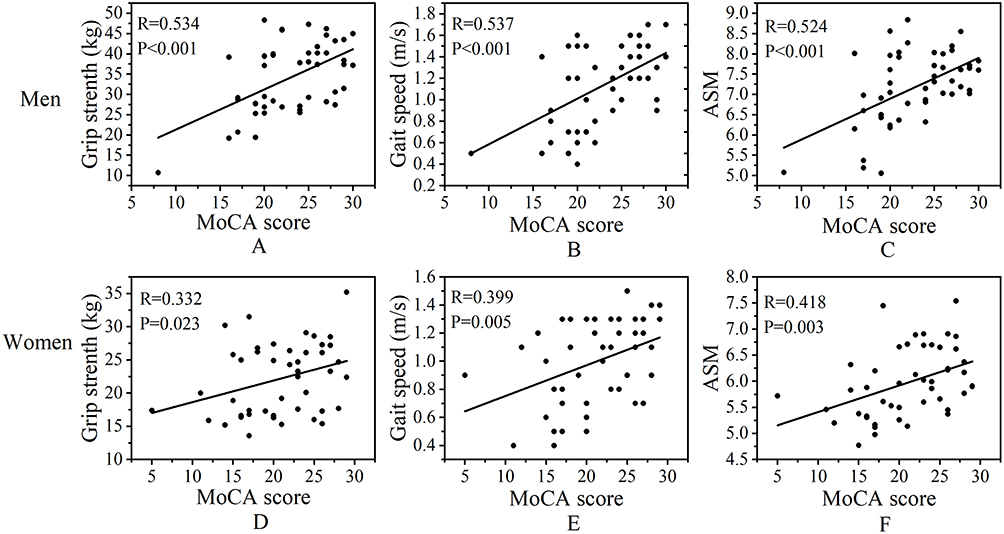 |
Figure 2 Scatter plots show the relationship between the Montreal Cognitive Assessment (MoCA) scores and handgrip strength, gait speed, and ASM in men and women. (A) The relationship between grip strength and MoCA score in men. (B) The relationship between gait speed and MoCA score in men. (C) The relationship between ASM and MoCA score in men. (D) The relationship between grip strength and MoCA score in women. (E) The relationship between gait speed and MoCA score in women. (F) The relationship between ASM and MoCA score in women. |
In a logistic regression model, after adjusting for age, body mass index, systolic blood pressure, heart rate, triglyceride levels, HDL cholesterol levels, blood glucose levels, antihypertensive medications, and physical activity, we found that the risk of cognitive impairment decreased with increasing grip strength in the men’s population (OR=0.74, P=0.020), and the prevalence of cognitive impairment decreased with increasing ASM metrics in the men’s population (OR=0.07, P=0.025) (Table 3). Among women, there was no such association.
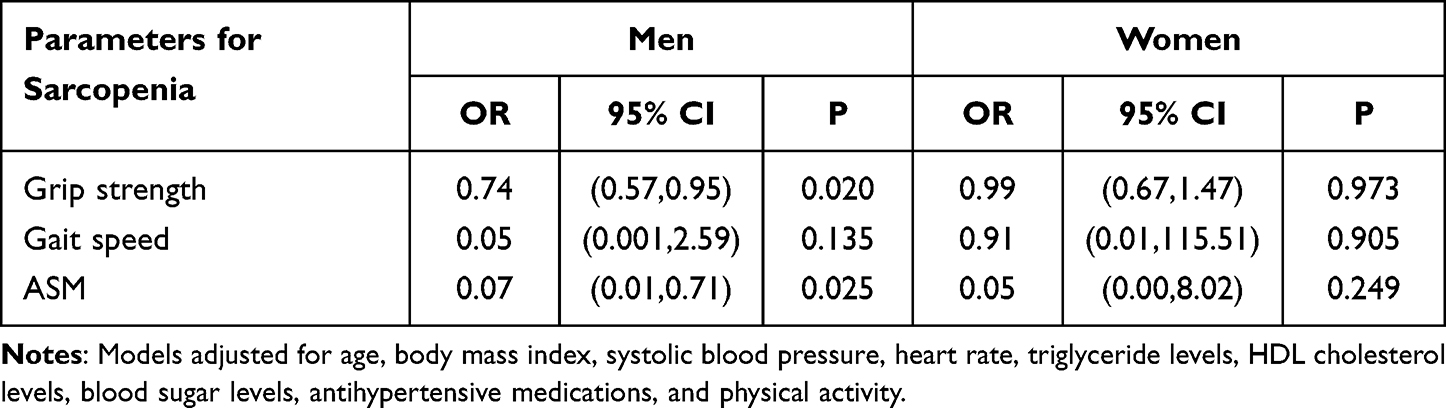 |
Table 3 Multifactorial Analysis of Various Indicators of Sarcopenia and Cognitive Impairment |
Presence of Sarcopenia and Cognitive Impairment
Odds ratios with and without sarcopenia and cognitive impairment are shown in Table 4. After adjusting for confounders, regression analysis revealed an increased prevalence of cognitive impairment in patients with sarcopenia relative to those without sarcopenia (OR=31.59, 95% CI=5.87–170.11, P<0.001). The same results remained after adding the variable adjusting for brain WMHs grading to the regression model.
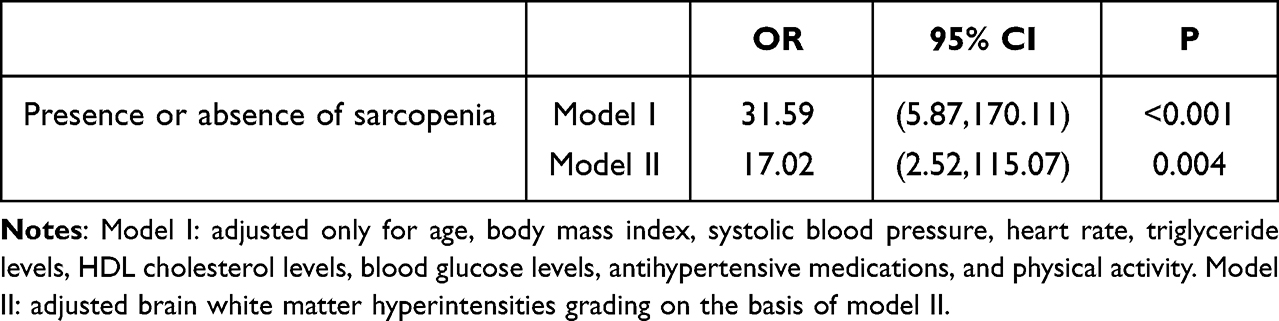 |
Table 4 Analysis of the Effect of Sarcopenia on Cognitive Impairment |
Discussion
Our study showed that sarcopenia was significantly associated with brain WMHs and cognitive test scores. Among the sarcopenia-related indices, grip strength, gait speed and ASM were also associated with cognitive function in older adults. These findings suggest that sarcopenia, one of the five major aging syndromes, plays a crucial role in cognitive impairment in the elderly hospitalized population.
Several cross-sectional and longitudinal studies have explored the association between sarcopenia and cognitive impairment, with results that are not entirely uniform. Peng et al included 15 cross-sectional studies in a meta-analysis that included 10,410 older adults from diverse settings including community, hospital, and clinic settings in Asia, Europe, and the Americas, and the adjusted dominance ratio showed that patients with sarcopenia were 2.25 times more likely to have mild cognitive impairment than those without sarcopenia (95% CI: 1.70–2.97).21 Jin et al did not find a significant association or linear trend between handgrip strength and total MMSE scores in a large cross-sectional study, after adjusting for possible confounders, in either men or women.15 Again, the relationship between sarcopenia and cognitive impairment has been inconsistently concluded in several longitudinal studies. A longitudinal study from Baltimore Longitudinal Study of Aging (BLSA) reported a 19% increased risk of MCI/AD for every 0.05m/s slower walking speed at low activity fragmentation (HR, 1.19[95% CI, 1.07–1.32]), while walking speed was not associated with MCI/AD risk at high activity fragmentation (HR, 1.01[95% CI, 0.93–1.10]).14 Results from a prospective cohort of Italian community residents over 65 years of age did not find a significant association between low grip strength at baseline and cognitive impairment as assessed by MMSE.22 A longitudinal cohort study with an average follow-up time of 5.6 years showed that adults with more severe baseline sarcopenia had an increased risk of developing Alzheimer’s disease, mild cognitive impairment, and a faster rate of cognitive decline.23 Salinas-Rodríguez et al conducted a cohort study showing that immediate verbal recall in cognitive function in patients with sarcopenia (P<0.01), delayed verbal recall (P=0.03), forward number breadth (P=0.05), and semantic word fluency (P<0.01) were lower than those without sarcopenia.24 The reasons for these differences may be as follows: (1) There are some differences in the diagnostic boundaries of sarcopenia by different consensus; (2) The instruments used to measure sarcopenia and the scales used to assess cognitive impairment are different; (3) Study population differences; (4) For longitudinal studies, the interval of follow-up time is different.
Our study is similar to previous findings and further explores potential mechanisms underlying the link between sarcopenia and cognitive impairment. Previous studies have shown that decreases in gait speed and handgrip strength are correlated with WMHs.9,10 Our study explored the correlation of cerebral WMHs with other indicators of sarcopenia, such as muscle mass and hand grip strength, and cerebral WMHs have also been shown to be associated with cognitive impairment.11,12 Therefore, a series of causal relationships between sarcopenia, WMHs, and cognitive impairment remains to be negotiated.
Some relevant studies, including the mate analysis, have reported WMHs as a potential of risk factor for cognitive impairment.11–13 A study13 that included data from multiple cohorts showed that WMH was associated with cognitive decline and Alzheimer’s disease (AD) neuropathology in either mild cognitive impairment (MCI), AD, or cognitively normal (CN) participants. In CN participants, high WMH volume was associated with cognitive decline that occurred over a period of approximately 10 years. WMH is a much greater predictive factor of cognition than age in MCI/AD. This is in line with our hypothesis. In our study, we observed that sarcopenia-related indices were also associated with WMHs, although this association differed between men and women, at the same time as between sarcopenia-related indices. In men, grip strength, gait speed, and ASM were significantly correlated with WMHs, but the association between gait speed and WMHs disappeared after adjusting for confounders. And interestingly, the correlations between grip strength, gait speed and ASM with WMHs were consistently present in women, regardless of whether they were adjusted for confounders. This result suggests that there may be other, as yet unidentified, potential factors influencing the association of grip strength and ASM with cognition in men, as well as the association of three sarcopenia-related indicators with WMHs in women.
In the correlation analysis, MoCA scores were positively correlated with the three sarcopenia-related indicators. The presence or absence of sarcopenia was associated with cognitive impairment when analyzed regardless of gender, and the relationship persisted even after adjustment for WMHs. After adjusting for confounders, only grip strength and ASM were associated with cognitive impairment in the multifactorial analysis among men, and no correlation existed among women. The above results suggest that there may be some unknown confounding factors or pathologies that associate grip strength and ASM with cognitive function in women, which contribute to the differences between men and women. In a cross-sectional study of a large group of community residents in Korea, sarcopenia and slow gait speed were associated with cognitive impairment in men, while in women only slow gait speed was associated with cognitive impairment.25
Resistance exercise and nutritional supplements can significantly improve somatic function, muscle mass and strength.26,27 The combination of food and nutrients is ideal to counteract cognitive decline,28 and physical activity can prevent/slow the pathological processes associated with dementia.29 This evidence suggests that sarcopenia may be a useful target for interventions to prevent cognitive decline and that interventions for cognitive impairment should be combined with interventions for sarcopenia. When a patient shows signs of cognitive decline, family members or physicians should be alert to the possibility of cognitive dysfunction emerging.
Our study has the following strengths. The MoCA scale was used in our study to detect the presence of cognitive impairment, which is able to distinguish between different clinical dementia syndromes in the early stages of the disease with high sensitivity and specificity. In addition, we assessed a total of three indices related to sarcopenia and defined sarcopenia according to the latest guidelines.
There are several noteworthy limitations to our study. First, this was a cross-sectional study and therefore a causal relationship between sarcopenia and cognition could not be determined. In addition, since all participants were elderly inpatients, selection bias due to survival cannot be excluded, so we may have overestimated the prevalence of sarcopenia, WMHs, or cognitive impairment. Finally, generalizability to other diverse backgrounds may be limited by the fact that all participants were from one city in China.
Conclusion
In summary, we explored the intricate relationship between sarcopenia and its associated indicators, WMHs, and cognitive impairment in hospitalized older adults, and found that grip strength, gait speed, and ASM were modestly but significantly related to WMHs and cognitive impairment. WMHs may be a possible factor in sarcopenia leading to cognitive impairment. Sarcopenia may be a helpful intervention target to prevent cognitive impairment. Future longitudinal studies may go a step further in determining the complex cause-and-effect relationship.
Ethics Approval and Informed Consent
The studies involving human participants were reviewed and approved by the Clinical Trial Ethics Committee of the Second People’s Hospital of Hefei (NO.2019-071). Written informed consent was obtained from all participants and in accordance with the principle of the Helsinki Declaration.
Acknowledgments
We are grateful to the study participants and the staff of the Department of Neurology of the Second People’s Hospital of Hefei for their cooperation in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the project of “Borrowing to Subsidy” of Hefei Independent Innovation Policy (J2019Y01).
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. Sui SX, Williams LJ, Holloway-Kew KL, et al. Skeletal muscle health and cognitive function: a narrative review. Int J Mol Sci. 2020;22(1):255. doi:10.3390/ijms22010255
2. Chen X, Han P, Yu X, et al. Relationships between sarcopenia, depressive symptoms, and mild cognitive impairment in Chinese community-dwelling older adults. J Affect Disord. 2021;286:71–77. doi:10.1016/j.jad.2021.02.067
3. Pieruccini-Faria F, Sarquis-Adamson Y, Anton-Rodrigo I, et al. Mapping associations between gait decline and fall risk in mild cognitive impairment. J Am Geriatr Soc. 2020;68(3):576–584. doi:10.1111/jgs.16265
4. McGrath R, Vincent BM, Hackney KJ, Robinson-Lane SG, Downer B, Clark BC. The longitudinal associations of handgrip strength and cognitive function in aging Americans. J Am Med Dir Assoc. 2020;21(5):634–639.e1. doi:10.1016/j.jamda.2019.08.032
5. Verghese J, Wang C, Lipton RB, Holtzer R. Motoric cognitive risk syndrome and the risk of dementia. J Gerontol a Biol Sci Med Sci. 2013;68(4):412–418. doi:10.1093/gerona/gls191
6. Cruz-Jentoft AJ, Baeyens JP, Bauer JM, et al. Sarcopenia: European consensus on definition and diagnosis: report of the European Working Group on sarcopenia in older people. Age Ageing. 2010;39(4):412–423. doi:10.1093/ageing/afq034
7. Chen LK, Liu LK, Woo J, et al. Sarcopenia in Asia: consensus report of the Asian working group for sarcopenia. J Am Med Dir Assoc. 2014;15(2):95–101. doi:10.1016/j.jamda.2013.11.025
8. Chen LK, Woo J, Assantachai P, et al. Asian working group for sarcopenia: 2019 consensus update on sarcopenia diagnosis and treatment. J Am Med Dir Assoc. 2020;21(3):300–307.e2. doi:10.1016/j.jamda.2019.12.012
9. van de Schraaf SAJ, Rhodius-Meester HFM, Aben L, et al. Slowing: a vascular geriatric syndrome? J Am Med Dir Assoc. 2022;23(1):47–53.e2. doi:10.1016/j.jamda.2021.07.031
10. Duchowny KA, Ackley SF, Brenowitz WD, et al. Associations between handgrip strength and dementia risk, cognition, and neuroimaging outcomes in the UK biobank cohort study. JAMA Netw Open. 2022;5(6):e2218314. doi:10.1001/jamanetworkopen.2022.18314
11. Hu HY, Ou YN, Shen XN, et al. White matter hyperintensities and risks of cognitive impairment and dementia: a systematic review and meta-analysis of 36 prospective studies. Neurosci Biobehav Rev. 2021;120:16–27. doi:10.1016/j.neubiorev.2020.11.007
12. Hilal S, Liu S, Wong TY, et al. White matter network damage mediates association between cerebrovascular disease and cognition. J Cereb Blood Flow Metab. 2021;41(8):1858–1872. doi:10.1177/0271678X21990980
13. Habes M, Pomponio R, Shou H, et al. The brain chart of aging: machine-learning analytics reveals links between brain aging, white matter disease, amyloid burden, and cognition in the iSTAGING consortium of 10,216 harmonized MR scans. Alzheimers Dement. 2021;17(1):89–102. doi:10.1002/alz.12178
14. Tian Q, Studenski SA, An Y, et al. Association of combined slow gait and low activity fragmentation with later onset of cognitive impairment. JAMA Netw Open. 2021;4(11):e2135168. doi:10.1001/jamanetworkopen.2021.35168
15. Jin YL, Xu L, Jiang CQ, et al. Association of hand grip strength with mild cognitive impairment in middle-aged and older people in Guangzhou biobank cohort study. Int J Environ Res Public Health. 2022;19(11):6464. doi:10.3390/ijerph19116464
16. Ishii H, Makizako H, Doi T, Tsutsumimoto K, Shimada H. Associations of skeletal muscle mass, lower-extremity functioning, and cognitive impairment in community-dwelling older people in Japan. J Nutr Health Aging. 2019;23(1):35–41. doi:10.1007/s12603-018-1110-9
17. Samper-Ternent R, Reyes-Ortiz C, Ottenbacher KJ, Cano CA. Frailty and sarcopenia in Bogotá: results from the SABE Bogotá Study. Aging Clin Exp Res. 2017;29(2):265–272. doi:10.1007/s40520-016-0561-2
18. Fazekas F, Chawluk JB, Alavi A, Hurtig HI, Zimmerman RA. MR signal abnormalities at 1.5 T in Alzheimer’s dementia and normal aging. AJR Am J Roentgenol. 1987;149(2):351–356. doi:10.2214/ajr.149.2.351
19. Nasreddine ZS, Phillips NA, Bédirian V, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53(4):695–699. doi:10.1111/j.1532-5415.2005.53221.x
20. Lu J, Li D, Li F, et al. Montreal cognitive assessment detecting cognitive impairment in Chinese elderly individuals: a population-based study. J Geriatr Psychiatry Neurol. 2011;24(4):184–190. doi:10.1177/0891988711422528
21. Peng TC, Chen WL, Wu LW, et al. Sarcopenia and cognitive impairment: a systematic review and meta-analysis. Clin Nutr. 2020;39(9):2695–2701. doi:10.1016/j.clnu.2019.12.014
22. Veronese N, Stubbs B, Trevisan C, et al. What physical performance measures predict incident cognitive decline among intact older adults? A 4.4 year follow up study. Exp Gerontol. 2016;81:110–118. doi:10.1016/j.exger.2016.05.008
23. Beeri MS, Leugrans SE, Delbono O, Bennett DA, Buchman AS. Sarcopenia is associated with incident Alzheimer’s dementia, mild cognitive impairment, and cognitive decline. J Am Geriatr Soc. 2021;69(7):1826–1835. doi:10.1111/jgs.17206
24. Salinas-Rodríguez A, Palazuelos-González R, Rivera-Almaraz A, Manrique-Espinoza B. Longitudinal association of sarcopenia and mild cognitive impairment among older Mexican adults. J Cachexia Sarcopenia Muscle. 2021;12(6):1848–1859. doi:10.1002/jcsm.12787
25. Kim M, Won CW. Sarcopenia is associated with cognitive impairment mainly due to slow gait speed: results from the Korean Frailty and Aging Cohort Study (KFACS). Int J Environ Res Public Health. 2019;16(9):1491. doi:10.3390/ijerph16091491
26. Yoshimura Y, Bise T, Shimazu S, et al. Effects of a leucine-enriched amino acid supplement on muscle mass, muscle strength, and physical function in post-stroke patients with sarcopenia: a randomized controlled trial. Nutrition. 2019;58:1–6. doi:10.1016/j.nut.2018.05.028
27. Takeuchi I, Yoshimura Y, Shimazu S, et al. Effects of branched-chain amino acids and vitamin D supplementation on physical function, muscle mass and strength, and nutritional status in sarcopenic older adults undergoing hospital-based rehabilitation: a multicenter randomized controlled trial. Geriatr Gerontol Int. 2019;19(1):12–17. doi:10.1111/ggi.13547
28. Dominguez LJ, Veronese N, Vernuccio L, et al. Nutrition, physical activity, and other lifestyle factors in the prevention of cognitive decline and dementia. Nutrients. 2021;13(11):4080. doi:10.3390/nu13114080
29. Vancampfort D, Solmi M, Firth J, et al. The impact of pharmacologic and nonpharmacologic interventions to improve physical health outcomes in people with dementia: a meta-review of meta-analyses of randomized controlled trials. J Am Med Dir Assoc. 2020;21(10):1410–1414. doi:10.1016/j.jamda.2020.01.010
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.