Back to Journals » Journal of Healthcare Leadership » Volume 14
The Relationship Between Organizational Commitment and Organizational Justice Among Health Care Workers in Ethiopian Jimma Zone Public Health Facilities
Authors Deressa B ![]() , Adugna K
, Adugna K ![]() , Bezane B
, Bezane B ![]() , Jabessa M
, Jabessa M ![]() , Wayessa G, Kebede A
, Wayessa G, Kebede A ![]() , Tefera G, Demissie Y
, Tefera G, Demissie Y
Received 3 November 2021
Accepted for publication 24 January 2022
Published 3 February 2022 Volume 2022:14 Pages 5—16
DOI https://doi.org/10.2147/JHL.S345528
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Pavani Rangachari
Beshea Deressa,1 Kebebe Adugna,2 Bezawit Bezane,1 Matebu Jabessa,1 Gemechis Wayessa,3 Alemi Kebede,4 Gelila Tefera,1 Yisalemush Demissie1
1Department of health policy and management, Jimma University, Jimma, Ethiopia; 2School of Nursing and midwifery, Jimma University, Jimma, Ethiopia; 3Clinical governance and quality improvement, Jimma Medical Center, Jimma University, Jimma, Ethiopia; 4Department of reproductive health and Nutrition, Jimma University, Jimma, Ethiopia
Correspondence: Gelila Tefera; Beshea Deressa
Department of health policy and management, Jimma University, PO Box: 378, Jimma, Oromia, Ethiopia
, Tel +251 932448617
, Email [email protected]; [email protected]
Background: The healthcare service sector is confronting a global labor shortage. Despite this fact, health care professionals are still highly vulnerable to organizational injustice, which negatively influence organizational commitment, putting an additional burden on the health sector. Thus, this study aimed to investigate the correlation between organizational commitment and organizational justice among health care workers.
Methods: Facility-based cross-sectional study design was conducted among 395 health care professionals in the Jimma zone. Four Hospitals and 10 health centers were involved in the study randomly. The sample was distributed proportionally based on the number of health care workers. To select individuals, a systematic random sampling method was employed. Data were collected through self-report questionnaire using modified Alan and Mayer scale to measure organizational commitment and Niehoff and Moorman scale to measure organizational justice. The validity of the tools was checked using the reliability coefficient alpha and it was > 0.7. The collected data were cleaned and entered into EpiData software version 3.1 and exported to SPSS version 20 for analysis. Descriptive and inferential statistics were done.
Results: This study revealed that 212 (53.7%) of the respondents scored a low level of organizational commitment. About half of the participants, 202 (52.2%), judged organizational justice were fair. All organizational justice dimensions showed a positive and significant correlation with all organizational commitment dimensions. Thus, the finding revealed that overall organizational commitment and organizational justice had a strong and positive correlation (r = 0.695**, P < 0.01). From the regression analysis distributive justice (B = 0.382, 95% CI: 0.31– 0.45), and procedural justice (B = 0.17, 95% CI: 0.06– 0.283) were among the factors affecting organizational commitment.
Conclusion and Recommendation: This study showed a strong link between organizational commitment and organizational justice. This suggests that organizational justice has been recognized as a motivator and factor influencing health care workers’ organizational commitment. As a result, enhancing organizational justice can help to maintain the commitment of healthcare workers and the facility’s capabilities.
Keywords: organizational justice, commitment, health professionals, health care tier system, Ethiopia
Introduction
Justice is vital stuff for understanding organizational features. Organizational justice is defined as an individual’s views about the impartiality of the decision and decision-making process within the organization and the influence of those views on the behavior.1,2 Researches on organizational justice demonstrated that fair treatment has a significant effect on individual employee commitment, satisfaction, and attitudes.3
Organizational justice is mostly theorized in three different concepts as Distributive, procedural, and interactional justice.4 Distributive justice dealt with the perception of employees on the fairness about organizational allocations and the outcomes.5,6 Staffs in one organization compare their outcomes with their counterparts within and outside their organization, such as pay, promotion, and access to resources and inputs. Organizational affiliation, identity, and involvement enhance when people have a positive impression of distributive justice.7 Meanwhile, procedural justice deals with the perceived fairness about the process utilized to determine the organizational outcomes derived from the perceived equity of organizational policies and procedures. This comprises the processes utilized in determining outcomes; voice and process control perspectives.8,9 Interactional justice is concerned with workers’ perception about the fairness of interpersonal views about the fairness of the interpersonal treatment received while implementation. It deals with the way individuals were treated when decisions are made, perceived level of individual feeling if they were being treated fairly with dignity, respect, and provision of explanation on the decision made.10
Organizational sustainability mainly depends on the individuals working in it. Their feeling, thinking, attitude, and behavior had a significant effect on the success and failure of the organization.11 On the other hand, the prevailing of justice in the organization positively affects the emotional wellbeing of the employee.12 Moreover, it also raises need which implies providing a benefit on one’s personal requirements which in turn makes the employee highly committed to the organization.13
Organizational commitment is defined as the relative strength of an individual’s identification with and involvement in a particular organization14 represents the attitudes or tendencies that link the individual to the organization in which these links are very important to the individual and valuable to the organization and overall society.15 Allen and Meyer identified organizational commitment into three different components (affective, continuance, and normative). Accordingly, affective commitment deals with an emotional attachment to, identification with, and participation in the organization, whereas continuance commitment is all about the perceived cost associated with leaving the organization and normative commitment denotes a perceived obligation to remain in the organization.16
A large number of studies4,17–19 have shown that organizational justice is a consistent and significant variable that affects organizational commitment across various settings. Additionally, there is a piece of evidence showing that organizational justice had an indirect effect on organizational commitment through organizational trust and identification.15,20 On the other hand, a study conducted among healthcare professionals found a significant link between moral distress and organizational justice in a reverse way.21
Other studies conducted elsewhere revealed that employees’ perception of organizational justice determines their positive and negative attitudes toward the organization and therefore their organizational commitment. Both organizational justice and organizational commitment are important to make the employees useful for the organization, do useful things for the organization and work heartily.22 In line with this, a study conducted in a specialized hospital in Ethiopia showed that only 72 (32.9%) of nurses score a high level of organizational commitment. Additionally, significant predictors of organizational commitment like educational status, working ward, perceived organizational support, interpersonal relationships, job satisfaction, transformational leadership behavior, and educational qualification were identified in the study.23
On the other hand, there is a finding4 that there is no significant effect on organizational commitment due to organizational justice dimensions, but showed the age of workers as the factor affecting the organizational commitment. Besides, there is evidence disclosing distributive and interactional justice dimensions had a significant impact on organizational commitment, but not procedural justice.24
The healthcare service sector is confronting labor shortage globally, which the World Health Assembly refers to as “a crisis in health.25 Though there is such a crisis in health institutions, health care professionals are still regarded as civil servants who are highly prone to organizational injustice. This imposes a significant adverse effect on their organizational commitment which in turn becomes an extra burden to the health care system.14 When this comes to Ethiopia, though there is shortage of data regarding organizational injustice and its adverse effect on organizational commitment in the healthcare sector, one can estimate that it could not be underestimated. In Ethiopia, the health-care delivery system is divided into three levels: primary, secondary, and tertiary. In Ethiopia, the healthcare delivery system is divided into three levels: primary, secondary, and tertiary. According to studies, Ethiopia faces multiple challenges in delivering health care services at all levels of the health care tier system due to low leadership commitment, a lack of quality health care professionals, inequitable resource distribution, a lack of decentralized planning, and a limited supply.26 With all of these difficulties, the issue of justice and commitment has not been adequately addressed at all levels in the similar period.
Therefore, the main purpose of this study was to examine the relationship between organizational commitment and organizational justice and whether different dimensions of organizational justice can have a different impact on the level of organizational commitment. Accordingly, this study explored how health care professionals in Jimma Zone public health facilities (from primary to tertiary) are entertaining organizational justice and organizational commitment. Because both organizational justice and organizational commitment are the mainstays of the survival of any organization, in which health institutions are the front lines dealing with human health.
Methods and Materials
Study Design and Setting
The facility-based cross-sectional study design was conducted in Jimma Zone public health facilities, Oromia Regional state, from 01 March 2019 to 16 May 2019. Jimma is located 336 km southwest of Addis Ababa, the capital of Ethiopia. The zone was divided into 18 districts and two town administrations. There are seven public hospitals found in the zone; one tertiary, one general, and five primary hospitals. In addition, as the lowest level of the Ethiopian health care tier system, there are 115 health centers with five satellite health posts found in the zone. There were about 2660 health care professionals in the Jimma zone in general. In the selected facilities, 1260 health care professionals were found.
Participants and Sampling Techniques
Population
All health care professionals earned a diploma and above qualification and working in public hospitals or health centers were our source population. Whereas all randomly selected health care professionals, having six months and greater work experience participated in the study. All health care professionals who had less than six months of work experience were excluded.
Sample Size and Sampling Technique
To determine the sample size, single proportion formula was used by considering 62.4% proportion of health care professionals’ organizational commitment from a study conducted in Gurage zone,27 95% confidence level and margin of 0.05 margin of error. The sample size became 354. However, this was greater than 5% of the total population and the source population was less than 10,000. Therefore, the finite correction formula was used. Then, the sample size became 276. Multistage sampling method was used and the probability of all health care professionals in the zone to be included in the sample was not equal. Thus, to solve this problem we have increased the sample size by taking the design effect of 1.5 and the final sample size used to collect the data was 435 including 5% of non-response rate.
One tertiary hospital, one general hospital, three primary hospitals, and ten health centers were randomly selected. Then the sample was proportionally allocated to hospitals and health centers. Finally, individuals were selected through a systematic sampling from each facility using workers’ registration logbooks, and the first participant was selected by lottery method.
Measurement
Organizational Commitment
Modified Alan and Mayer scale was used to measuring organizational commitment.16 The tool consists of an 18-item scale with three dimensions. These dimensions are affective, continuance, and normative commitment. Sample items for each dimension were described. Accordingly, for Affective commitment; “I would be very happy to spend the rest of my career with this organization, for continuance commitment; “Right now, staying with my organization is a matter of necessity as much as desire, and for normative commitment; “Even if it were to my advantage, I do not feel it would be right to leave my organization now. The reliability coefficient alpha of affective commitment, continuance commitment, and normative commitment were 0.73, 0.65, and 0.74, respectively. To facilitate further analysis, the scale was reduced to one item (organizational commitment score) using principal component analysis with an eigenvalue of greater than one and 0.87 KMO (P < 0.001). The extracted item explained 57% of the overall variance and was used during further analysis as a continuous variable.
The organizational justice scale was measured with a modified 19-item scale developed by Niehoff and Moorman.28 Participants indicated the level of their agreement or disagreement with the items on a scale from 1 (strongly disagree) to 5 (strongly agree). The overall organizational justice scale reliability coefficient in this study was 0.94. Specifically, 0.86, 0.92, and 0.91 for coefficient alpha value for distributive, procedural, and interactional justice, respectively.
Study Variables
Dependent Variable
Organizational commitment.
Independent Variables
Organizational justice dimensions score: Distributive justice, procedural justice and interactional justice.
Health Care Workers Related Factors
Age, Sex, Educational level, Marital status, Work experience, Overtime, on job training, professional category, Number of hours usually worked per week, perceived staff adequacy.
Health Facility Characteristics
Types of Health facility, Client-to-provider ratio, on job training.
Data Management and Statistical Analysis
The collected data were entered into EpiData version 3.1 and exported to SPSS version 20 for analysis. Descriptive statistics were employed to describe the study participants in relation to relevant variables. The mean score was calculated for the outcome variable and used to determine the level of organizational commitment and organizational justice. To determine the level of relationship between organizational justice dimensions and organizational commitment dimensions, Spearman correlation coefficient was employed.
To identify potential predictors and changes in organizational commitment in the final model, Hierarchical regression analysis was utilized. Hence, in the first step on the first step, variables of socio-demographic and facility-related characteristics with a p-value of <0.25 in bivariate analysis were included in the multivariable linear regression. Then to look for the independent contribution of the organizational justice, the three organizational dimensions were added to the final regression analysis. Beta and Adjusted R2 were used for interpretation, and statistically significant predictors were declared at a p-value of <0.05 and 95%.
Ethical Considerations
To conduct the study, ethical clearance was obtained from the Institutional Review Board of Jimma University after submitting the proposal. A letter of support was obtained from all participating facilities. Written informed consent was taken from the participants and all the data obtained in due course was kept confidential.
Results
The study included 395 healthcare professionals out of 435 invited participants, for a response rate of 90.8%. More than half 235 (59.5%) of the respondents were male. The participants’ age ranged from 21 to 64. The majority of the participants (83.5%) them aged between 21 and 30 years, with a mean age of 32.6 (SD 4.4). Two hundred nineteen (54%) were single. Concerning the educational qualifications, 246 (62.3%) of them were bachelor degree holders. More than two-thirds of the respondents 276 (69.9%) had less than five years of work experience.
Regarding their profession, 230 (58.2%) were Nurses, 49 (12.4%) were physicians and 37 (9.4%) were laboratory technicians. One hundred eighty-one (45.8%) respondents were from tertiary hospital followed by 90 (22.8%) from the health center (see Table 1).
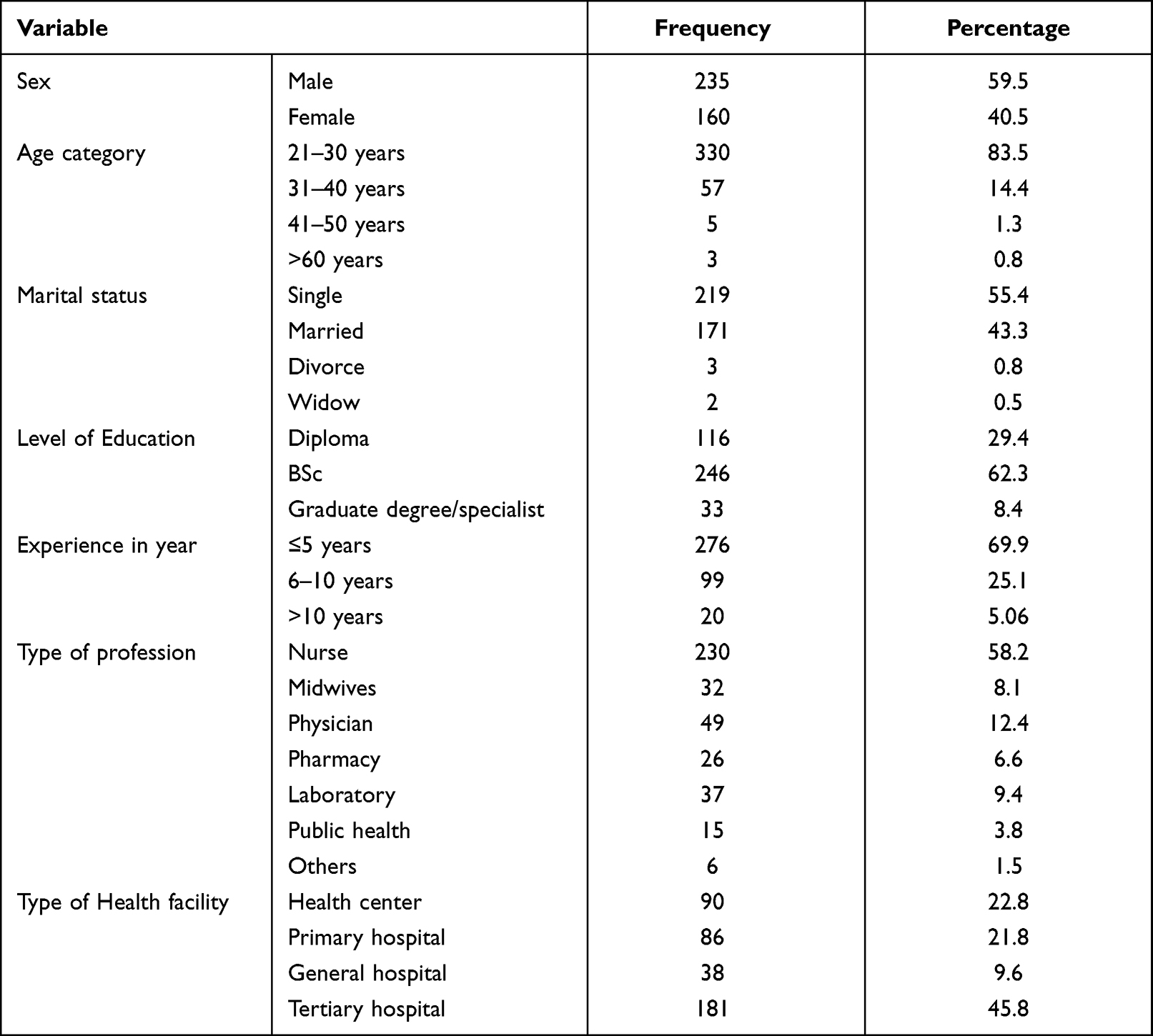 |
Table 1 Socio Demographic Characteristics of Respondents (n = 395) |
On the other hand, when health care professionals were asked on how often they feel the unit staffing is adequate; 143 (36.2%) responded sometimes, 91 (23%) said rarely and 80 (20.3%) never (see Figure 1).
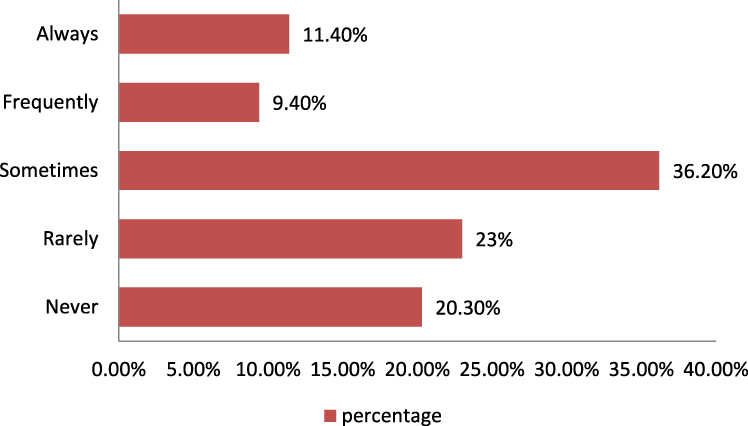 |
Figure 1 The frequency of staff feeling on the adequacy of unit staffing (n=395). |
The overall organizational commitment means a score of the participant was 3.22 (SD 0.7). The affective commitment had the highest mean of 3.11 (SD 0.90), and the lowest mean was for the normative commitment 2.91 (SD 0.71). Whereas the organizational justice mean score was 2.72 (SD: 0.86), in which distributive justice had the highest 2.85 (0.94) followed by interactional justice 2.71 (0.86) (See Table 2).
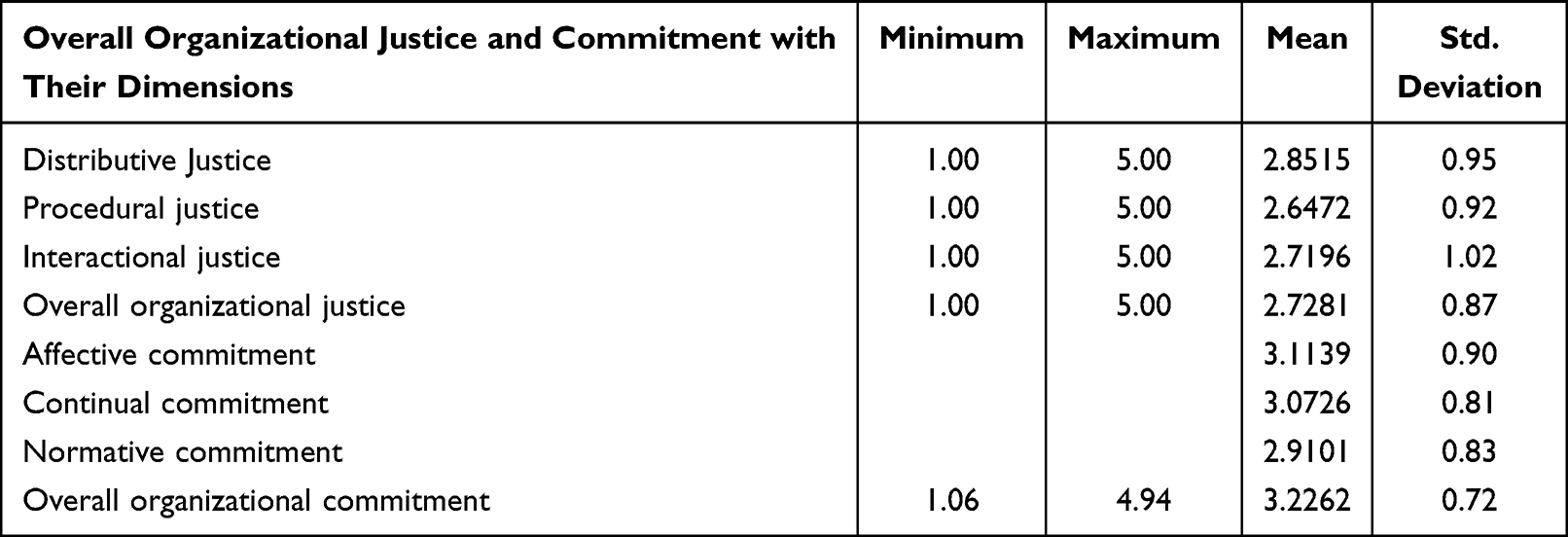 |
Table 2 Mean Score and Standard Deviation of Organizational Commitment and Organizational Justice Dimensions (n = 395) |
This study also indicated that more than half 212 (53.7%) of the health care professionals reported a low level of organizational commitment. Specifically, two-thirds of tertiary hospital respondents (67%) reported low organizational commitment (below mean), whereas the majority (59%) of primary health care workers reported high organizational commitment (see Figure 2).
 |
Figure 2 Perceived level of organizational commitment among health care professionals, in the three-health care tier (Primary to tertiary level), Jimma Zone, south west Ethiopia (n=395). |
On the other hand, 202 (52.2%) participants responded that their perception of organizational justice was regarded as fair scoring above the mean. When observed separately, majority of health care professionals in the primary health care level (65%) reported better fairness of organizational justice practice (see Figure 3).
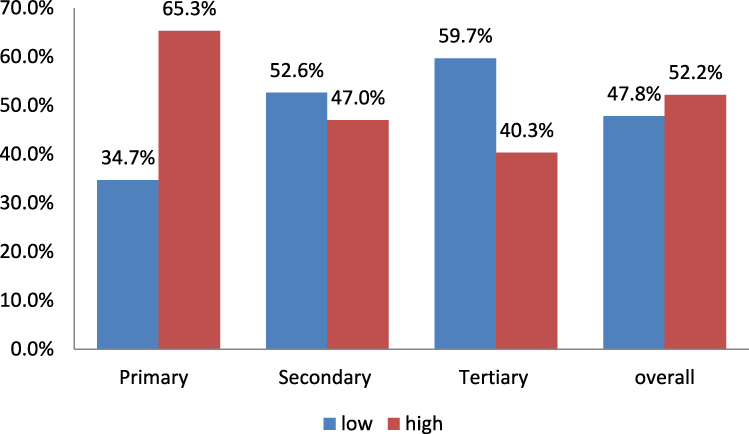 |
Figure 3 Perceived level of organizational justice among health care professionals, in the three-health care tier (primary to tertiary level), Jimma Zone, south west Ethiopia (n=395). |
The Correlates of Organizational Commitment Dimensions and Organizational Justice Dimensions
The study finding indicated that distributive justice was positively and significantly correlated with affective commitment (r = 0.58), continual commitment (r = 0.60), and normative commitment (r = 0.55) normative commitment (r = 0.55). Procedural justice had also a positive and significant correlation with all three dimensions of organizational commitment (affective commitment; r = 0.474, continual commitment; r = 0.56 and normative commitment; r = 0.524). Similarly, interactional justice had a positive and significant correlation with the organizational commitment components (see Table 3).
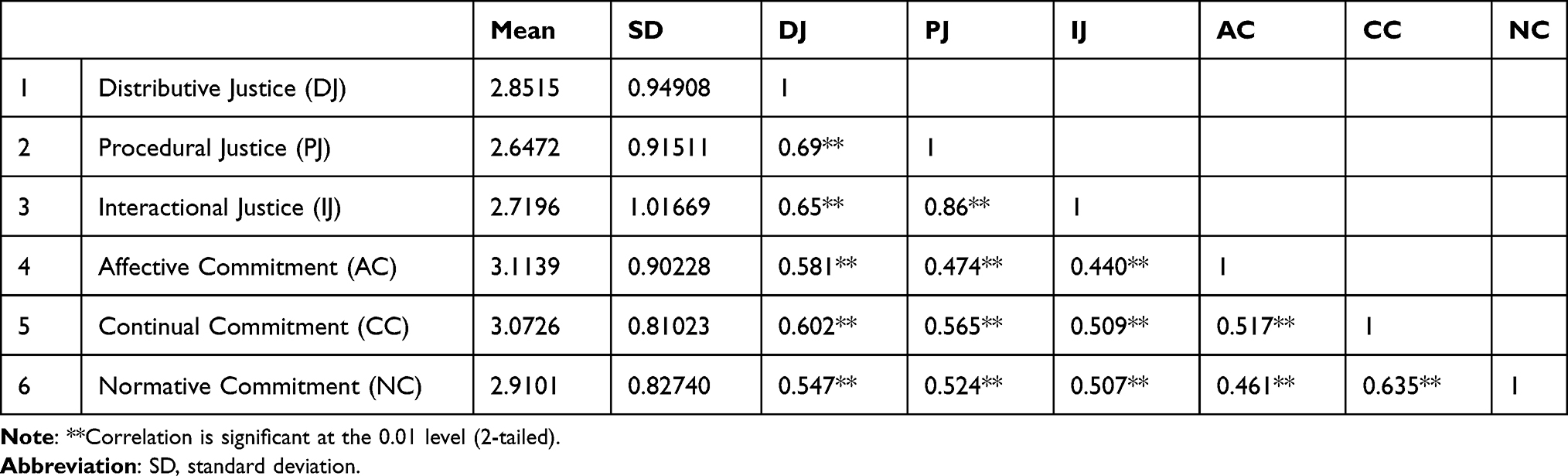 |
Table 3 Correlation Among Dimensions of Organizational Justice and Organizational Commitment (n = 395) |
Moreover, the table below shows the correlation of overall organizational justice and commitment. Thus, the finding revealed that overall organizational commitment is positively correlated with overall organizational justice (r = 0.695**, P < 0.01) (See Table 4).
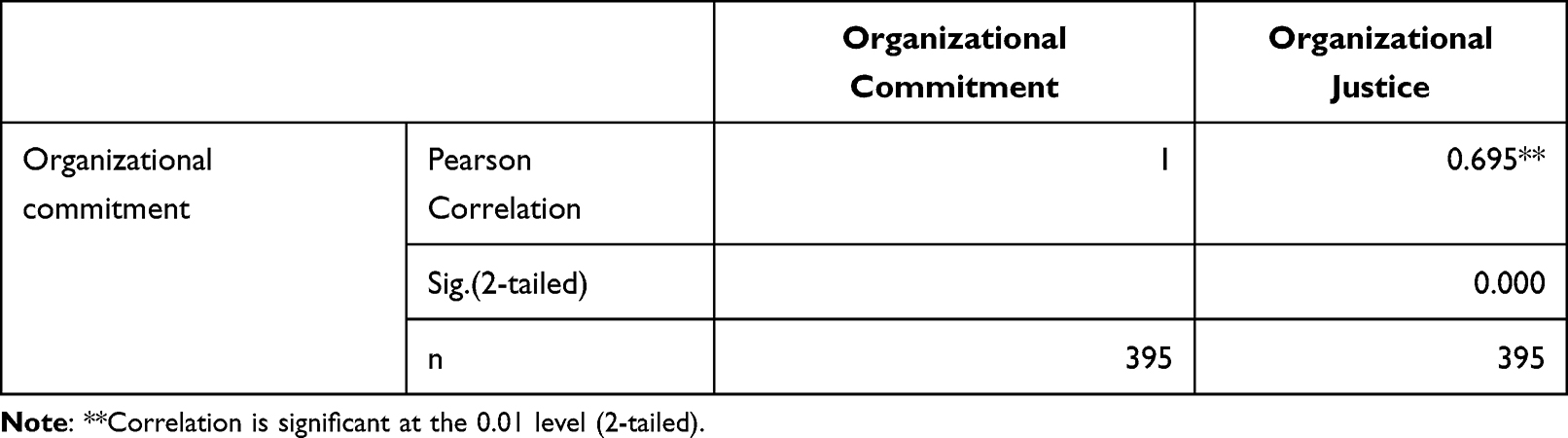 |
Table 4 Overall Correlates of Organizational Commitment and Organizational Justice |
Predictors of Organizational Commitment
To identify potential predictors of organizational commitment on the first step variables (socio-demographic characteristics and facility-related characteristics) with a P-value of <0.25 during bivariate regression were included. All socio-demographic characteristics show no significant effect on organizational commitment, while facility type and educational level were found to be significant predictors of the organizational commitment on the first step. Facility type and educational level were found to be significant predictors of the organizational commitment on the first step. Accordingly, higher organizational commitment score was reported from specialized, general, and primary hospitals compared to the health center staff.
Thus, working in a specialized hospital increases organizational commitment score by 0.411 (P < 0.01, CI: 0.230, 0.592); working in a primary hospital increases organizational commitment score by 2.649 (P = 0.008, CI: 0.062, 0.418) and working in a general hospital increase the organizational commitment score by 2.377 (P = 0.018, CI: 0.051, 0.536). Furthermore, from an educational level, holding a postgraduate degree and above increases the organizational commitment score 2.323 (P = 0.021, CI: 0.045, 0.561) (see Table 5).
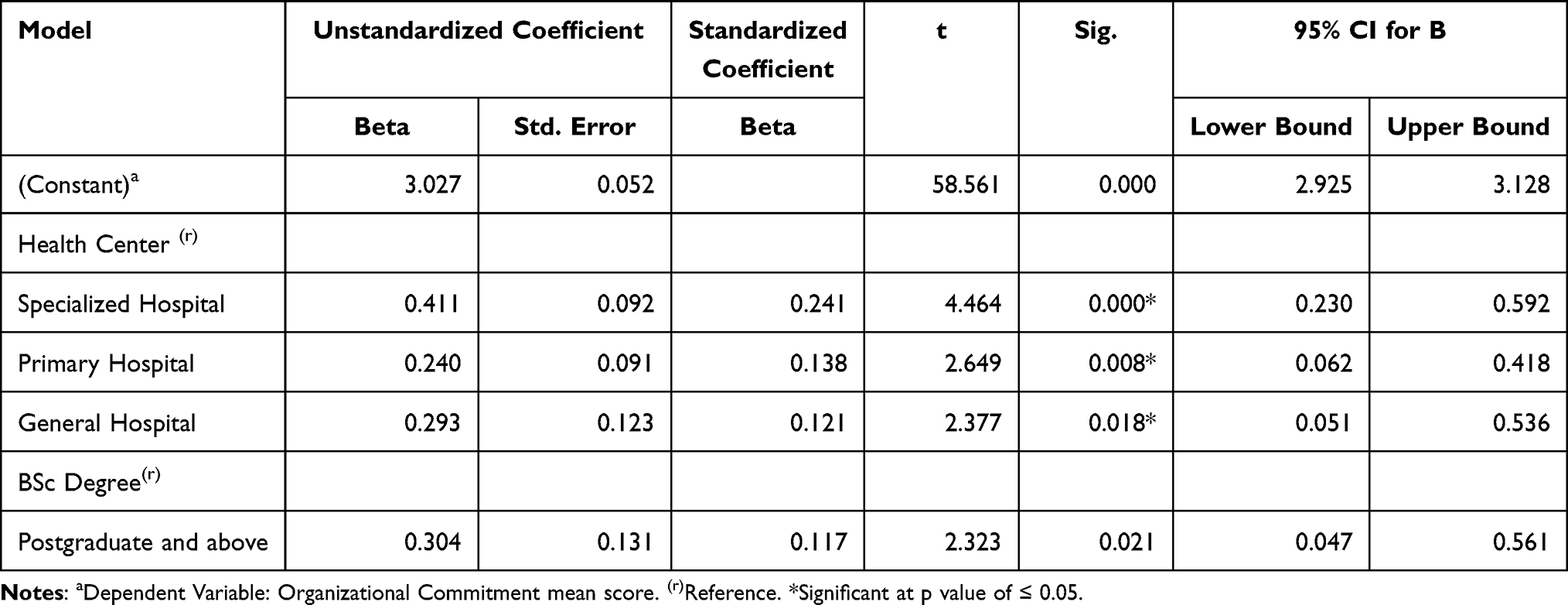 |
Table 5 Socio-Demographic and Facility-Related Factors Affecting Organizational Commitment |
To observe distinctly the influence of organizational justice dimensions on organizational commitment, regression analysis was conducted at the second step. Hence, the regression result shows, except interactional justice, the rest two organizational justice dimensions (distributive and procedural justice) revealed as the predictors of organizational commitment. The unit increase in distributive justice score increases the organizational commitment score by 0.382 (P < 0.01, CI: 0.31–0.45) and a unit increase in procedural justice score increases the organizational commitment score by 0.17 (P < 0.01, CI: 0.058, 0.283). The overall change in organizational commitment due to the organizational justice (interactional, distributive, and procedural) was 0.515 (51.5%) (see Table 6).
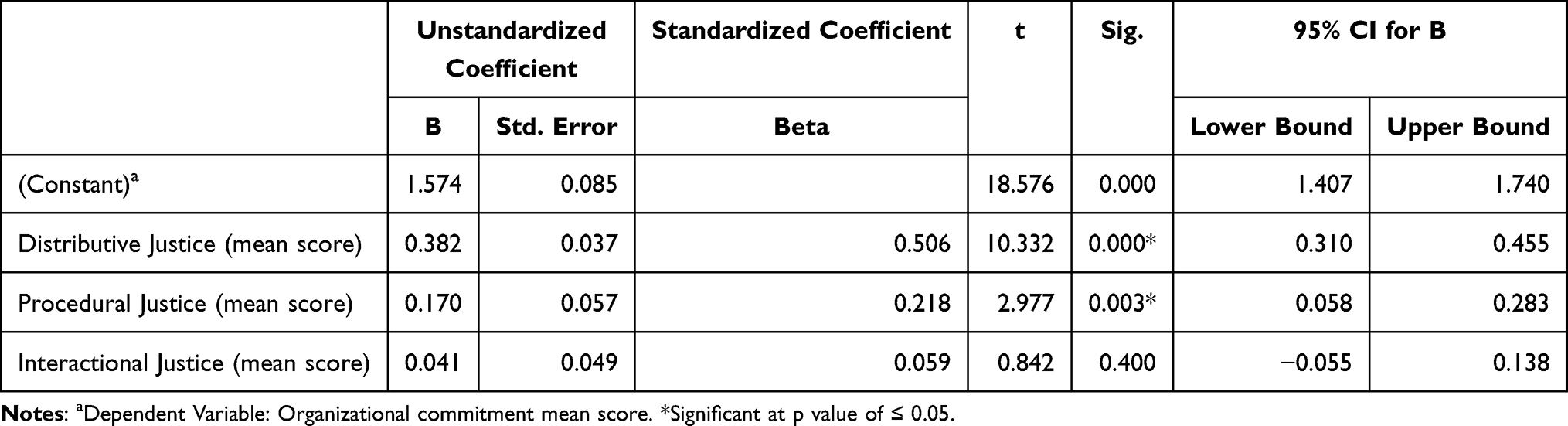 |
Table 6 The Influence of Organizational Justice Dimensions on Organizational Commitment |
Discussion
Organizational justice is a multidimensional concept, and it has been shown for its positive effect on job outcomes, reducing turnover, and organizational effectiveness.29 However, it could be affected by different factors related to personal characteristics, leadership and management, and organizational context and characteristics of the job.30 On the other hand, observance of justice is the key to the organization and its worker’s survival and development.31,32 Therefore, this study was conducted with the aim of determining the level of organizational commitment and organizational justice and their correlation with one another among health care professionals, in public health facilities of Jimma zone, southwest, Ethiopia.
The finding of this study revealed that slightly more than of the respondents (53.7%) scored the low level of organizational commitment. While the rest (46.3%), of them, scored a high level of organizational commitment. The finding of a previous study on organizational commitment and its predictors in Jimma University referral only 72 (32.9%) of the nurses scored a high level of organizational commitment.33 The variation between the study findings could be due to the difference in the settings as the latter one was conducted in a single hospital while ours was conducted in many health facilities, in addition to the time (study period) variation. Normative commitment showed the lowest mean score among the three dimensions of organizational commitment, suggesting that participants feel a sense of obligation to their organization, even if they are unhappy with their role, or suggesting that participants were less obliged to their organization if they are unhappy with their role, they want to peruse better opportunities.
The result showed a positive and significant correlation between organizational justice and organizational commitment (P < 0.05). This means, if employees feel the organization’s treatment is unfair, it will cause strain for them and reduce their commitment. On the other hand, if employees feel that the organization is observed to be fair, they will be motivated to stay in their organization and take more responsibilities and duties.
Equity theory, which was first proposed by Adam,34 well enlightened the association between organizational commitment and organizational justice. It indicated that if staffs perceive their input–outcome ratio to be equivalent to those of the relevant with whom they compare themselves, a state of equity exists and their commitment to their organization will be increased. There are also works of literature elsewhere showing that the organizational justice dimensions had a strong correlation and reported as independent predictors of organizational commitment and its dimensions.32,35,36 This could be explained as, employees, who felt an injustice had a lower level of organizational commitment and could negatively affect the organizational success, and on the other hand, a justice-oriented organization will have highly committed and this will guide toward its mission and targets.
In addition, the result of this study revealed that there were significant positive correlations between dimensions of organizational justice and organizational commitment. Procedural justice is the primary characteristic of organizational justice which is centered on the premise that the fairest and respectful decisions will be made. Moreover, procedural justice consists of, giving the staff the chance to take part in the decision-making process and thus they can be more authorized and inspired to cooperate with the organization. Distributive justice addresses the ownership of good in society. It assumes that there is a large amount of fairness in the distribution of good and therefore, employees believe, equal work should provide them equal outcomes in terms of goods acquired or the ability to acquire good. Interactional justice pertains to the behavior of the leaders and managers as they execute their decisions and authority. All of these characteristics can help the employees to increase their organizational commitment. The results of other studies have also shown that improved dimensions of organizational justice contributed toward a high level of organizational commitment.4,15,37–40
The other result of this study was that among the demographic variables of employees, facility type and level of education were found to have a statistically significant association and thus identified as the independent predictors of organizational commitment. On the other side, except for interactional justice, the other components of organizational justice (distributive and procedural) were found to have a statistically significant association with organizational commitment. The finding indicates that facility type, educational level, perceived distributive and procedural justice could predict the level of organizational commitment.
Facility level (being in a specialized hospital) was the predictor of organizational commitment among the demographic facility-related variables (B = 0.24, P < 0.01). This showed that health care providers working in a specialized hospital were committed to their organization. This could be explained by the delivery of better support facilities and staff resources at the tertiary hospital than the health centers positively and indirectly associated with quality care for patients and better achievements through their impact on staff organizational commitment.41 There was also another study finding which explained the type of organization to influence organizational commitment.42
Educational level (holding a second degree and above) was another variable predicting organizational commitment (B = 0.12, p < 0.01). Healthcare professionals holding a second degree and above had better organizational commitment compared to the lower level. This result is consistent with a study that reported educational level is an independent predictor of organizational commitment in health care settings.43 These findings could be discussed as; providing the opportunity for staff to upgrade their education is a very strategic method to improve the organizational commitment of the staff.
Generally, it showed that these four predictors explain 52% of the total variance in organizational commitment. The other 48% of the variability of organizational commitment can be explained by other variables which were not explained in this study. The explanation for the percentage variability not explained by this study might be due to other factors like power distance,44 identity45 and other factors like the role of individual factors like organization-based self-esteem46 were not addressed as the predicting variables for organizational commitment.
However, our finding is in contrast to other studies which stated that higher levels of educational level have a negative impact on organizational commitment.33,47 This difference could be due to the effect of professional mix in our study, but the rest focused on a single profession only.
The other predictor variables; distributive and procedural justice play an important role in helping organizational commitment. This result was also supported by other studies conducted elsewhere in the globe. The finding was also supported by other studies conducted elsewhere in the globe.19,48 The finding shows, these dimensions of organizational justice have open direct impact on organizational commitment. This means, the more they perceive the organizational justice as fair, the greatest employees’ commitment toward their organization.
Strength and Limitation of the Study
The strength of this study was that health care professionals working in all health care tiers from primary to tertiary were involved, whereas the employment of only a quantitative method might be the limitation of the study.
Conclusion
According to the findings of this study, a significant proportion (47.8%) of healthcare professionals perceived organizational justice practices as unfair. From the three dimensions of organizational justice, distributive justice was perceived as fairest, with the highest score. On the other hand, health care professionals working in the primary health care level perceived fair organizational justice practice compared to those at secondary and tertiary levels.
This study revealed that in general majority of health care professionals in all health care tiers reported a low level of organizational commitment. However, the organizational commitment of primary health care level workers was reported to be high. From organizational commitment dimensions, affective commitment (emotional attachment to, identification with, and participation in the organization) of the participant was reported to be high and moderate for normative commitment (perceived obligation to remain in the organization).
Also, the results of this study revealed that there was a positive and significant correlation between organizational justice and organizational commitment. It was also indicated that organizational justice was found to be a motivational tool and a factor affecting the employees’ organizational commitment. Therefore, to increase health care professionals’ commitment toward their organization, improving organizational justice is required.
Taking into account the effect of organizational justice and its dimensions on the employees’ organizational commitment, health facility leadership should pay more attention to enhancing organizational justice especially on the provision of reward based on the standard (distributive justice) and creating a fair system on performance evaluation and their promotions (procedural justice). Moreover, given the present situation, it is strongly recommended that it should be considered to pay attention in retaining healthcare professionals with a high level of educational level and fulfilling the supportive resources in all types of health facilities. It should be remembered that human capital is the main asset of organizations and their leaders should give due attention to their commitment and attitudes. Finally, further research is recommended to identify why organizational justice and organizational commitment were low in the tertiary level and relatively high in primary level care in the Ethiopian health care system.
Acknowledgments
We thank Jimma University for funding this research project. We are also grateful to all study participants and data collectors.
Disclosure
The authors report no conflicts of interest for this work.
References
1. van den Bos K. Fundamental research by means of laboratory experiments is essential for a better understanding of organizational justice. J Vocat Behav. 2001;58(2):254–259. doi:10.1006/jvbe.2001.1797
2. Cropanzano R, Molina A. Organizational Justice. In: Wright JD, editor. Handbook of Work Stress. International Encyclopedia of the Social & Behavioral Sciences; 2015. doi:10.1016/B978-0-08-097086-8.22033-3
3. Attia S. The relationship between organizational justice and quality performance among healthcare workers: a pilot study. Sci World J. 2014;2014:45.
4. Srivastava UR. Multiple dimensions of organizational justice and work-related outcomes among health-care professionals. Am J Ind Bus Manag. 2015;05:666–685.
5. Colquitt JA. Organizational justice. 2012:526–547.
6. Eisenberger R, Malone GP, Presson WD. Optimizing perceived organizational support to enhance employee engagement. J Occup Health Psychol. 2016. doi:10.1037/ocp0000061
7. Ghasi NC, Ogbuabor DC, Onodugo VA. Perceptions and predictors of organizational justice among healthcare professionals in academic hospitals in South-Eastern Nigeria. BMC Health Serv Res. 2020;20:1–12. doi:10.1186/s12913-020-05187-5
8. Yadav LK, Yadav N. Organizational justice: an analysis of approaches, dimensions and outcomes. NMIMS Manage Rev. 2016;3:1–40.
9. Cox K, Strang L, Søndergaard S. Understanding how organisations ensure that their decision making is fair. RAND Corporation, Santa Monica, Calif., and Cambridge, UK; 2017.
10. Colquitt JA, Scott BA, Rodell JB, et al. Justice at the millennium, a decade later: a meta-analytic test of social exchange and affect-based perspectives. J Appl Psychol. 2013;98:199–236. doi:10.1037/a0031757
11. International A, Journal M, State O. Organisational justice and psychological well-being of employees in the local government service of Osun State, Nigeria. An Int Multidiscip J. 2015;9:55–72.
12. Garg P, Rastogi R, Paul H. Does perception of justice effect psychological well-being of employees?. Int J Soc Syst Sci. 2014;6:264–284. doi:10.1504/IJSSS.2014.065215
13. Majekodunmi E. The influence of organisational justice on employees ’ commitment in manufacturing firms in oyo state, Nigeria: implications for industrial. African J Soc Work. 2015;5:92–130.
14. Wazir MS, Shaikh BT, Ahmed A. National program for family planning and primary health care Pakistan: a SWOT analysis. Reprod Heal. 2013;10:e23.
15. Chen S, Wu W-C, Chang C-S, et al. Organizational justice, trust, and identification and their effects on organizational commitment in hospital nursing staff. BMC Health Serv Res. 2015;15:1–17.
16. Allen NJ, Meyer JP. The measurement and antecedents of affective, continuance, and normative commitment to the organization. J Occup Psychol. 1990;63:1–18.
17. Lee H. An empirical study of organizational justice as a mediator of the relationships among leader-member exchange and job satisfaction, organizational commitment, and turnover intentions in the lodging industry; 2000.
18. Ayana AS, Kaur N, Sharma D. The mediation role of organizational commitment and job satisfaction in the effect of perception of organizational justice on intention to leave: evidence from Ethiopia Textile Industry. Int J Sci Res. 2017;6:2256–2259.
19. Suifan TS. The effect of organizational justice on employees ’ affective commitment the mediating role of job satisfaction. Can Cent Sci Educ. 2019;13:1–12.
20. Sökmen A, Ekmekçioğlu EB. The relationship between organizational justice, organizational commitment and intention to leave: investigating gender difference the relationship between organizational justice, organizational commitment and intention to leave: investigating gender. Int J Bus Manag Invent. 2017;5:27–31.
21. Haghighinezhad G, Atashzadeh-Shoorideh F, Ashktorab T, Mohtashami J, Barkhordari-Sharifabad M. Relationship between perceived organizational justice and moral distress in intensive care unit nurses. Nurs Ethics. 2019;26:460–470. doi:10.1177/0969733017712082
22. Imamoglu SZ, Ince H, Turkcan H, Atakay B. The effect of organizational justice and organizational commitment on knowledge sharing and firm performance. Procedia Comput Sci. 2019;158:899–906. doi:10.1016/j.procs.2019.09.129
23. Teaching S, Israel B, Kifle W, Tigist D, Fantahun W. Organizational commitment and its predictors among nurses working in primary health care: open access organizational commitment and its predictors among nurses working in Jimma University Specialized Teaching Hospital, Southwest Ethiopia. Prim Heal Care Open Access. 2019;7:45.
24. Dorji C, Kaur K. The impact of organizational justice on organizational commitment: a perception study on teachers of Bhutan. Int J Recent Technol Eng. 2019;7:436–440.
25. World Health Organization. Global strategy on human resources for health: workforce 2030; 2016.
26. World Health Organization. Primary health care systems (Primasys). World Heal Organ. 2017;53:1–48.
27. Hailemicael Nima G. Organizational commitment of health professionals and associated factors in government health facilities of Gurage Zone, South Ethiopia. Clin Med Res. 2016;5:82. doi:10.11648/j.cmr.20160505.11
28. Niehoff BP, Moorman RH. Justice as a mediator of the relationship between methods of monitoring and organizational citizenship behavior. Acad Manag J. 1993;36:527–556.
29. Jahangir FMS, Shokrpour NP. Three components of organizational commitment and job satisfaction of hospital nurses in Iran. Health Care Manag. 2009;28:375–380. doi:10.1097/HCM.0b013e3181b3eade
30. Vagharseyyedin S. An integrative review of literature on determinants of nurses′ organizational commitment. Iran J Nurs Midwifery Res. 2016;21(107):107–117. doi:10.4103/1735-9066.178224
31. Seyed Javadin SR, Faraahi MM. How different dimensions of organizational justice affect the different dimensions of job and organizational satisfaction. J Bus Manag. 2009;1:55–70.
32. Rafei-dehkordi F, Mohammadi S, Yektayar M. Relationship of organizational justice and organizational commitment of the staff in general directorate of youth and sports in Chahar Mahal va Bakhtiari Province Pelagia Research Library. Eur J Exp Biol. 2013;3:696–700.
33. Israel B, Kifle W, Tigist D, Fantahun W. Organizational commitment and its predictors among nurses working in Jimma University specialized teaching hospital, Southwest Ethiopia. Prim Heal Care Open Access. 2017;07:1–8.
34. Al-Zawahreh A, Al-Madi F. The utility of equity theory in enhancing organizational effectiveness. Eur J Econ Financ Adm Sci. 2012;46:158–170.
35. Cagliyan V, Attar M, Derra ME. The relationship between organizational justice perception and organizational commitment: a study on dogus otomotiv authorized dealers in Konya. J Fac Econ Adm Sci. 2017;22:599–612.
36. Ari A, Çağlayan HS. Relationship between organizational justice perceptions and organizational commitment levels of school of physical education and sports academicians. J Educ Train Stud. 2017;5:240.
37. Gichira PM, Were SM, Orwa GO. Relationship between perceptions of distributive justice and employee commitment in health sector non-governmental in Kenya. Eur J Hum Resour. 2016;1:1–25.
38. Etim EE, Okudero GO. Effects of employees’ perception of organizational injustice on commitment to work among staff of Lagos state fire service. Asian J Adv Res Rep. 2019;1–8. doi:10.9734/ajarr/2019/v5i130125
39. Al afari TS, Abu Elanain HM. Procedural and distributive justice as mediators of the relationship between interactional justice and work outcomes: an empirical study of the UAE public health care sector. J Appl Bus Res. 2014;30:1091–1108. doi:10.19030/jabr.v30i4.8657
40. Gulluce AC, Ozer S, Erkilic E. The effect of organizational justice perception on organizational commitment among healthcare sector employees. J Bus Manag. 2015;4:16–25. doi:10.12735/jbm.v4i3p16
41. Yu K. Employee organisational commitment and hospital performance. Health Care Manage Rev. 2017;1–27. doi:10.1097/HMR.0000000000000181
42. Kónya V, Matić D, Pavlović J. The influence of demographics, job characteristics and characteristics of organizations on employee commitment. Acta Polytech Hungarica. 2016;13:119–138.
43. Adeniji AA, Osibanjo AO, Iruonagbe TC, et al. From job satisfaction to organizational commitment: the mediating influence of perceived treatment of diversity among Nigeria ’ s public healthcare employees. J Med Sci. 2019;7:2031–2035.
44. This content from DeepDyve R, from DeepDyve R. The relationship between organizational justice and organizational citizenship: the mediating effect of organizational commitment and the moderating role of power distance. Hum Resour Manag Int Dig. 2020;28:7–9. doi:10.1108/HRMID-05-2020-0111
45. Salehi M, Sima HH, Fahimi MA. The relationship between organizational justice and auditors’ professional skepticism with the moderating role of organizational commitment and identity. Curr Psychol. 2020. doi:10.1007/s12144-020-00700-9
46. Minibas-Poussard J, Le Roy J, Erkmen T. The moderating role of individual variables in the relationship between organizational justice and organizational commitment. Pers Rev. 2017;46:1635–1650. doi:10.1108/PR-12-2015-0311
47. Santa-Cruz F. The effect of educational level on job satisfaction and organizational commitment. Int J Hosp Tour Adm. 2016;17:243–259.
48. Malik RA, Alvi AK. Impact of procedural justice and distributive justice on organizational commitment in banking sector of lahore. 2018:501–504.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.