Back to Journals » International Journal of Women's Health » Volume 17
The Relationship Between Early Pregnancy Depression, Social Support, and Hypertensive Disorders of Pregnancy: A Prospective Cohort Study in Xuzhou, China
Authors Chen S, Liu N, Yang M, Zhang Z, Duan M, Wang P
Received 20 August 2025
Accepted for publication 9 December 2025
Published 15 December 2025 Volume 2025:17 Pages 5497—5508
DOI https://doi.org/10.2147/IJWH.S562003
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Vinay Kumar
Shiyi Chen,1,* Nana Liu,1,* Mingxi Yang,1 Zhifan Zhang,2 Meng Duan,2 Peian Wang1
1Xuzhou Central Hospital, Affiliated Xuzhou Clinical College of Xuzhou Medical University, Xuzhou, Jiangsu, People’s Republic of China; 2Xuzhou Medical University, Xuzhou, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Peian Wang, Email [email protected]
Background: Hypertensive disorders of pregnancy (HDP) are major causes of maternal-neonatal morbidity/mortality. Emerging evidence links early pregnancy depression to HDP, but the interaction of social support, including its potential mediating and moderating roles remains understudied. This prospective cohort study explored the associations between early pregnancy depression, social support, and HDP risk in Xuzhou, China.
Methods: A cohort of 1,406 pregnant women at ≤ 12weeks gestation were recruited from a hospital in Xuzhou, China, between July 2024 and July 2025. Depression symptoms and social support were assessed using the Edinburgh Postnatal Depression Scale (EPDS) and the Social Support Rating Scale (SSRS), respectively. HDP was diagnosed according to ISSHP-2021 criteria following participants until delivery. Associations were evaluated using multivariate logistic regression, mediation, and interaction analyses.
Results: Among the participants, 122 (8.6%) cases of HDP were diagnosed. After adjusting for confounders, early pregnancy depression (EPDS ≥ 13) significantly increased the risk of HDP (aOR = 2.63, CI: 1.67– 4.09, p < 0.001). Conversely, high social support (SSRS ≥ 45) was a protective factor against HDP (aOR = 0.42, 95% CI: 0.20– 0.85, p < 0.001). Mediation analysis further revealed that social support partially mediated the depression-HDP association, accounting for 13.6% of the total effect.
Conclusion: This prospective study demonstrates that first-trimester depressive symptoms increase the risk of HDP, and social support not only directly protects women but also partially mediates the adverse effect of depression. Our findings highlight that early psychological screening and enhancing social support during the first trimester could be crucial strategies for HDP prevention.
Keywords: HDP, social support, depression, early pregnancy, prospective cohort study
Introduction
Hypertensive disorders of pregnancy (HDP), which include gestational hypertension, pre-eclampsia, and eclampsia, are among the leading causes of maternal and neonatal morbidity and mortality worldwide.1 The global prevalence of HDP is estimated to be increasing, posing a significant public health burden.2 In China, the condition affects approximately 5–10% of pregnancies, aligning with or slightly exceeding global averages and highlighting its clinical importance within the region.3
Concurrently, perinatal depression is a prevalent complication, with meta-analyses indicating a point prevalence of around 20% among pregnant women in Mainland China.4 Although the pathophysiology and risk factors for HDP have been thoroughly studied, less is known about the involvement of psychosocial factors, including mental health and social support in the early stages of pregnancy,5,6 which warrants more research. According to recent research, biological processes include dysregulation of the hypothalamus-pituitary-adrenal (HPA) axis and an increased inflammatory response may be two ways that maternal depression during the early stages of pregnancy may contribute to the development of HDP. In the meantime, maternal inflammation and oxidative stress may have a detrimental effect on fetal neurodevelopment, raising the possibility of unfavorable results for both the mother and the newborn.7–10
The first trimester represents a critical window of fetal-placental development and profound maternal cardiovascular adaptation.11,12 This period of significant hormonal and physiological fluctuation coincides with a high susceptibility to mood disturbances, making it a pivotal time for early screening and intervention.13 Investigating the interplay between psychological risk factors and HDP onset during this early phase through a prospective design could yield valuable insights for prevention, yet evidence from such studies remains limited.14–16
Social support is a well-established protective factor against stress and a key determinant of mental and physical health. Within the Chinese cultural context, family harmony and strong social networks (eg, support from husbands, parents, and relatives) are deeply valued and play a particularly central role in an individual’s health management.17 This cultural specificity may profoundly influence how social support modulates the risk of depression and HDP, though this interaction is underexplored in international literature. While previous studies have independently demonstrated the beneficial effects of social support on both maternal mental health and HDP risk,18,19 its potential role as either a mediator or moderator in the depression-HDP pathway is not well defined. Elucidating this mechanism is crucial for developing targeted, effective interventions.
Therefore, the novelty of this study lies in its prospective cohort design to: (1) simultaneously assess depressive symptoms and social support levels specifically during the first trimester; and (2) rigorously test the dual mechanistic roles of social support—both as a mediator and a moderator—in the relationship between depression and HDP development in a Chinese population. This study aims to investigate: (a) the association between first-trimester depressive symptoms and the risk of incident HDP; (b) the direct protective effect of social support on HDP risk; and (c) the potential mediating and moderating effects of social support in this association.
MaterialS and Methods
Study Design and Participants
The obstetrics outpatient clinic at Xuzhou Central Hospital recruited 1,406 singleton pregnant women in their first trimester (gestational weeks ≤12) between July 2024 and July 2025 for this prospective cohort study. The requirements for inclusion were: 1) be at least 18 years old; 2) get a pregnancy test at the hospital where the study is being done; and 3) voluntarily give their informed consent to participate in the study. Exclusion criteria were as follows: 1) miscarriages or twin or multiple births; 2) women with pre-existing hypertension; and 3) pregnant women with mental illness or cognitive impairments. Our conceptual framework is presented in Figure 1. Ethical approval was granted by the Institutional Ethics Committee (Approval No. XZXY-LK-20250328-0036). This study was performed in line with the principles of the Declaration of Helsinki. All consent procedures were witnessed by clinic staff and documented in research records.
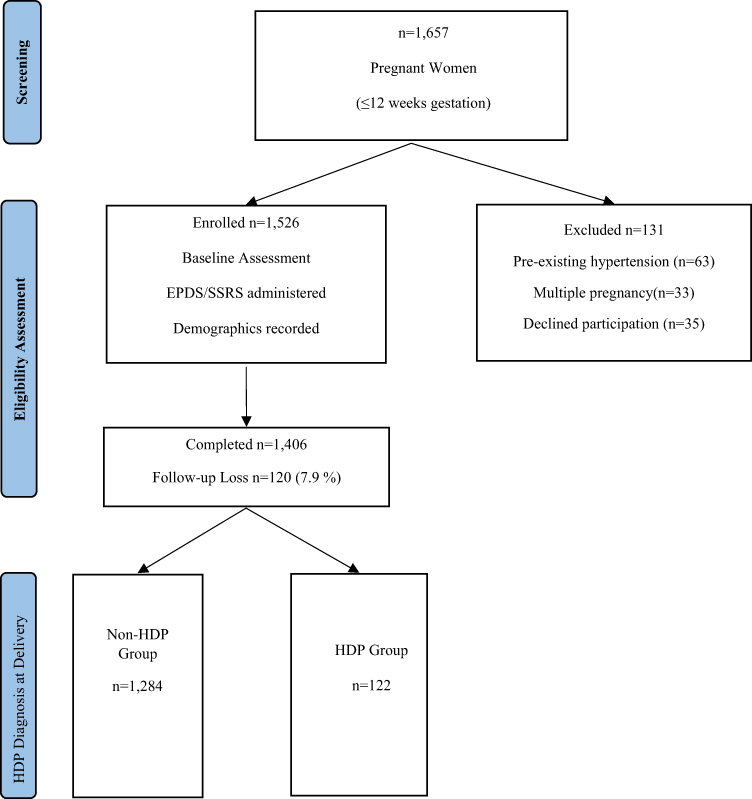 |
Figure 1 Participant flow diagram with exclusion criteria and outcome stratification. |
A self-designed general information questionnaire was one of the face-to-face questionnaires that study participants filled out at baseline (around 12 weeks) to collect sociodemographic information on the mothers, including pre-pregnancy BMI, educational level, occupational status, as well as pre-pregnancy smoking and alcohol consumption. Additional information about the number of births, maternal age, and family history of hypertension was gathered from medical records.
Measures and Instruments
Depressive symptoms were evaluated using the Chinese version of the Edinburgh Postnatal Depression Scale (EPDS),20 a 10-item self-report questionnaire validated and widely used in the Chinese perinatal population.21 Participants with a total score of ≥13 were classified as having significant depressive symptoms, as recommended for the Chinese prenatal context.22 Social support was measured with the Social Support Rating Scale (SSRS),23 which quantifies objective, subjective, and utilization support domains. The SSRS has also demonstrated good reliability and validity in Chinese pregnant populations (Cronbach’s α = 0.935).24,25 Higher SSRS scores indicate more social support; low support is indicated by scores below 35, moderate support by scores between 35 and 45, and high social support by scores over 45.
Outcome Ascertainment
The incidence of HDP served as the study’s outcome event. The hospital information system and phone follow-ups were used to collect data on pregnancy outcomes. The primary outcome—hypertensive disorders of pregnancy (HDP)—was diagnosed per ISSHP-2021 criteria:26–28 1) Gestational hypertension (GH): Persistent SBP ≥140 mmHg and/or DBP ≥90 mmHg after 20 weeks, two readings ≥4 hours apart (severe cases: ≥15 minutes if SBP ≥160/DBP ≥110 mmHg), and no proteinuria. 2) Preeclampsia (PE): GH + any of: Proteinuria (spot urine protein/creatinine ≥0.3 or 24h protein ≥300 mg); Organ dysfunction: Renal (creatinine ≥1.1 mg/dL); Hepatic (ALT/AST >2×ULN); Neurological (eclampsia, visual disturbances); Hematological (platelets <100×109/L). 3) Eclampsia: PE + unexplained seizures. Diagnoses were confirmed via hospital records and supplemented by structured telephone follow-ups for delivery outcomes.
Data Collection and Quality Control
Data collection procedures included face-to-face surveys and medical records review. The EPDS and SSRS were administered at baseline (mean gestation 11.9 ± 0.8 weeks), with no repeat measurements conducted. Quality control measures included training of enumerators, double-entry data verification, and random checks of 10% of the questionnaires for accuracy.
Statistical Analysis
Data organization was performed using Excel 2016, and statistical analysis was conducted using SPSS 27.0. Results for normally distributed variables were shown as mean ± standard deviation, and t-tests were used to compare groups. Chi-square tests were used for intergroup comparisons, and categorical data were presented as frequencies and percentages (n%). The associations between early pregnancy depression, social support, and HDP were examined using multifactorial logistic regression models, with OR and 95% CI calculated.
Model 1 assessed the association between first-trimester depression (EPDS ≥13) and the risk of HDP. Model 2 assessed the association between social support (SSRS score, as a continuous or categorical variable) and the risk of HDP. These models were adjusted for a priori selected covariates that are established determinants of both depression and HDP based on existing literature,9,14,16,29 including: maternal age, parity, pre-pregnancy BMI, education level, occupation, smoking status, alcohol use, and family history of hypertension. Diet quality and physical activity were not measured; we acknowledge this as a potential source of residual confounding.
The mediation and moderation analyses were conducted using the PROCESS macro for SPSS30 and the mediation package in R31 for robust causal mediation analysis, ensuring the consistency of findings across different statistical frameworks. A priori power analysis using GPower software indicated that the sample size of 1,406 provided adequate power (>80%) to detect medium effect sizes for the primary analyses.31
Causal Mediation Analysis: To quantify the causal mechanisms, we performed a formal causal mediation analysis using the nonparametric bootstrap method with 1000 simulations.31 This analysis estimated:
The Average Causal Mediation Effect (ACME): the indirect effect of depression on HDP operating through social support.
The Average Direct Effect (ADE): the direct effect of depression on HDP not explained by the mediator.
The Total Effect: the sum of the direct and indirect effects.
The Proportion Mediated: the proportion of the total effect explained by the mediator.
Moderation Analysis: To test if social support moderated the relationship between depression and HDP, we used PROCESS macro (Model 1) by introducing a depression × social support interaction term into the logistic regression model. The significance of the moderation effect was assessed by comparing the goodness-of-fit between the nested models (with and without the interaction term) using a likelihood ratio test (LRT).
A two-tailed p-value < 0.05 was considered statistically significant for all analyses. Bootstrap confidence intervals that did not include zero were considered evidence of a significant effect.
Results
Of the 1,526 pregnant women enrolled at under 12 weeks of gestation, 1,406 (92.5%) were retained for final analysis. Among these, 122 (8.6%) were diagnosed with hypertensive disorders of pregnancy (HDP). The baseline characteristics of the study participants, stratified by HDP status, are presented in Table 1. Significant differences were observed between the HDP and non-HDP groups regarding maternal age, parity, pre-pregnancy BMI, depression status, and social support level (all p < 0.001).
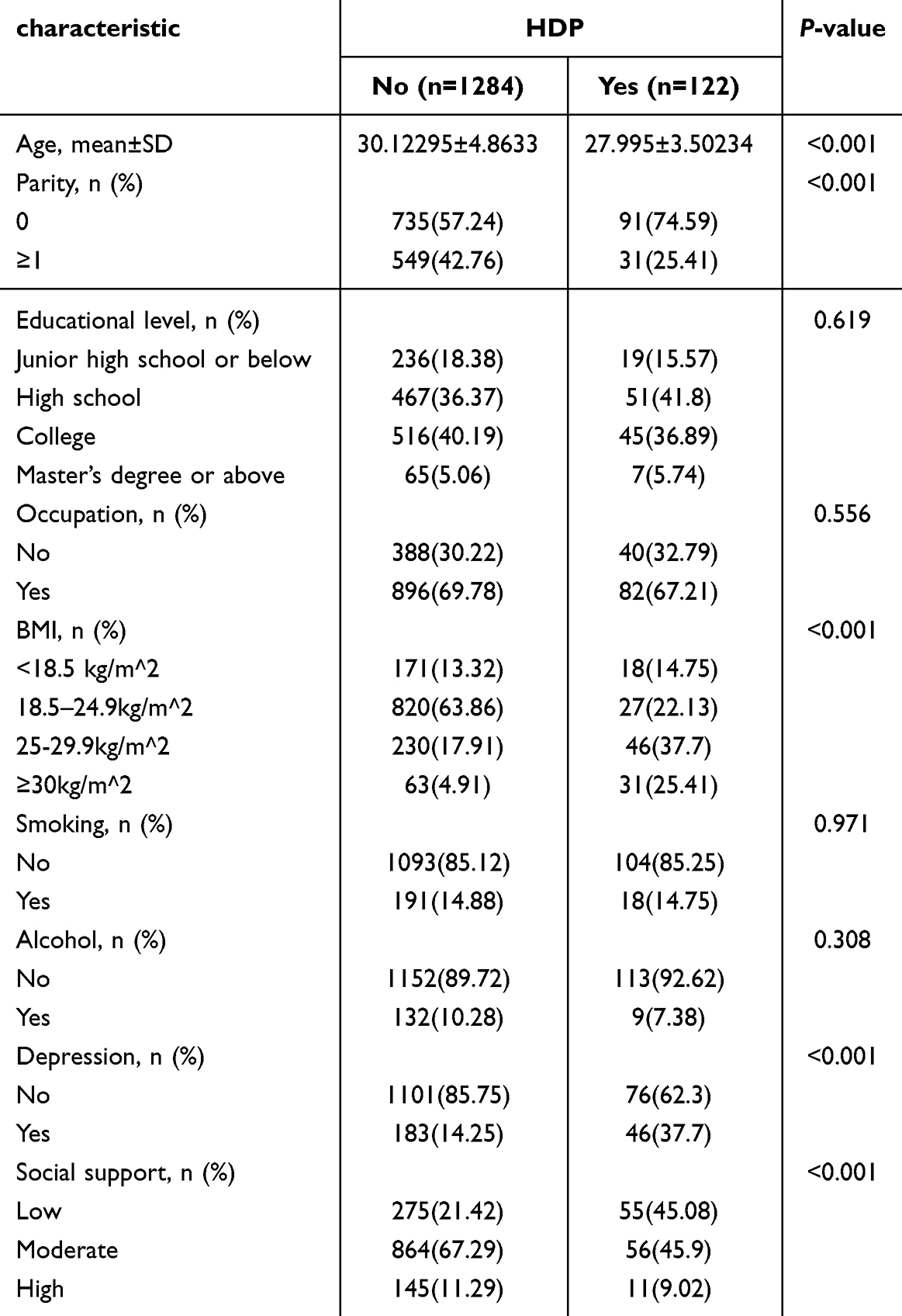 |
Table 1 Baseline Maternity Characteristics in the First Trimester and HDP Outcomes |
Multivariable logistic regression models were constructed with early-pregnancy depression and social support scores as independent variables and incident HDP as the dependent variable. In unadjusted analysis, clinically significant depression (EPDS ≥13) was associated with a nearly 3.5-fold increase in the risk of HDP (OR = 3.64, 95% CI: 2.43–5.40, p < 0.001). Participants with moderate and high social support demonstrated approximately one-third the risk of HDP compared to the low-support group (see Table 2).
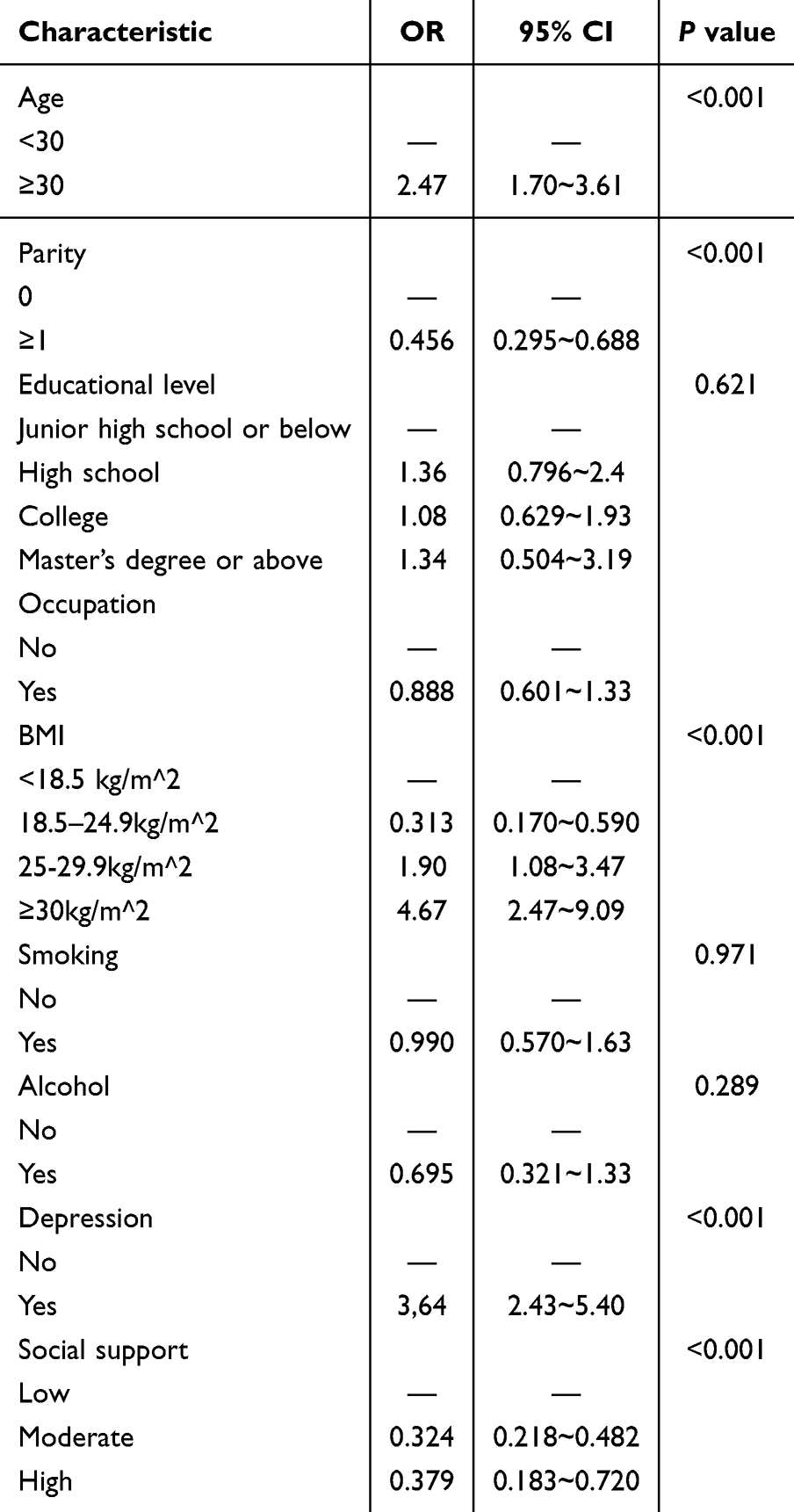 |
Table 2 Results of a Univariate Analysis of the Effects Of Depression and Social Support Scores on HDP in the First Trimester |
After adjustment for confounders including maternal age, parity, and pre-pregnancy BMI, the associations between depression, social support, and HDP risk were attenuated but remained statistically significant. As summarized in Figure 2 and detailed in Table 3, women with depression in early pregnancy had a 2.6-fold increased risk of HDP (adjusted Odds Ratio [aOR] = 2.63, 95% CI: 1.67–4.09, p < 0.001). Concurrently, both moderate (aOR = 0.36, 95% CI: 0.24–0.56, p < 0.001) and high social support (aOR = 0.42, 95% CI: 0.20–0.85, p < 0.001) demonstrated independent protective effects against HDP compared to low social support.
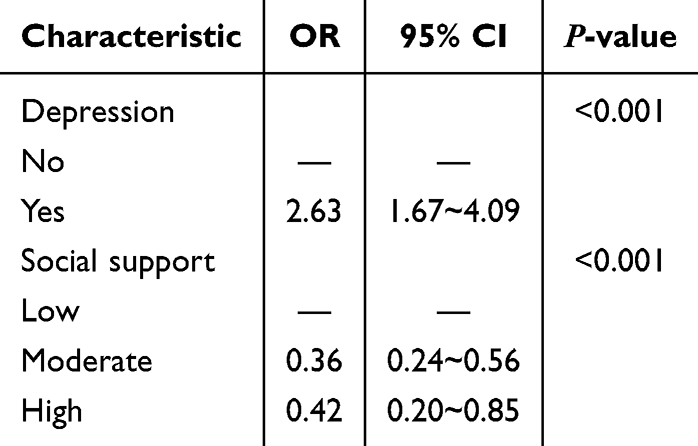 |
Table 3 Multivariate Logistic Regression Analysis Results of Depression and Social Support Scores in the First Trimester on the Impact of HDP |
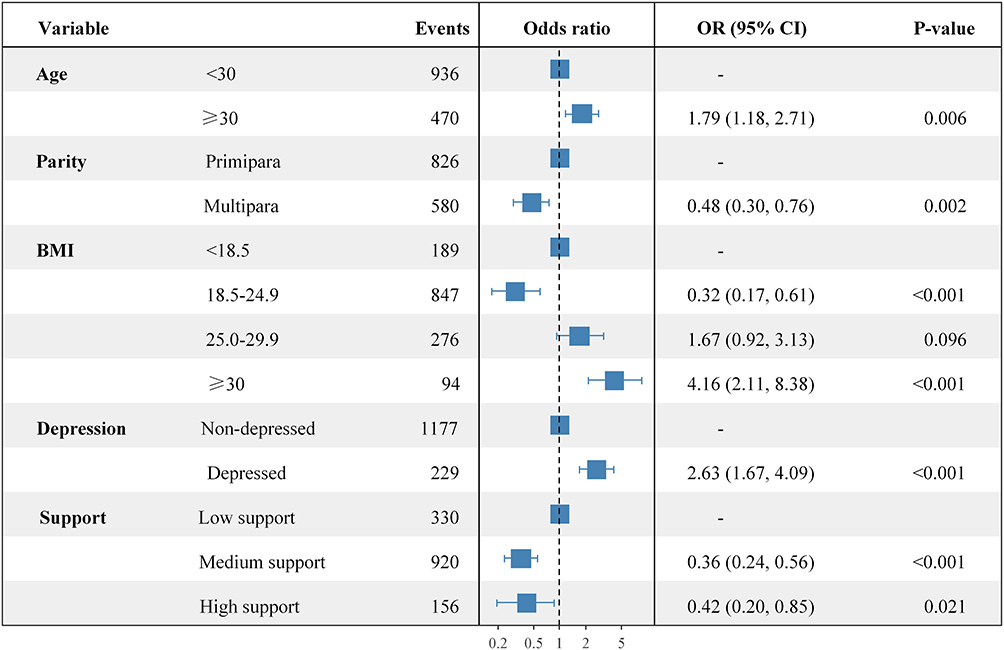 |
Figure 2 Forest Plot of Adjusted Odds Ratios for HDP Risk Factors.Forest plot displaying the adjusted odds ratios (aORs) and 95% confidence intervals for factors associated with hypertensive disorders of pregnancy. The vertical line of unity (aOR = 1) is shown. |
To elucidate the potential pathway through which social support operates, we performed a mediation analysis. The path model illustrating these relationships is presented in Figure 3. The results, detailed in Table 4, indicated that the total effect of depression on HDP was significant (Effect = 0.0919, 95% CI: 0.0496–0.1400). A significant portion of this effect was mediated by social support (Mediated Effect = 0.0126, 95% CI: 0.0035–0.0250), accounting for 13.6% of the total association between early pregnancy depression and HDP.
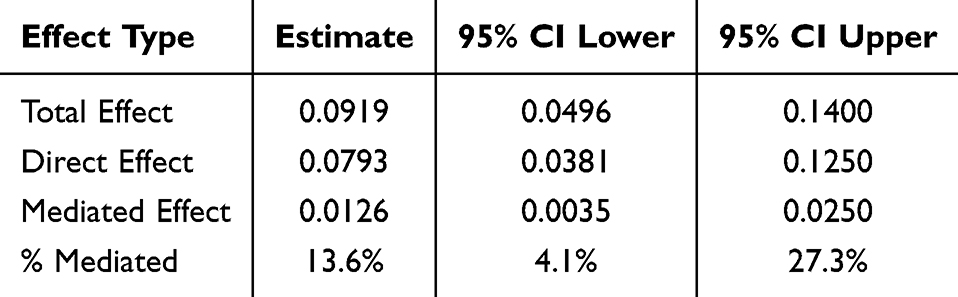 |
Table 4 Mediation Analysis of Social Support in the Depression-HDP |
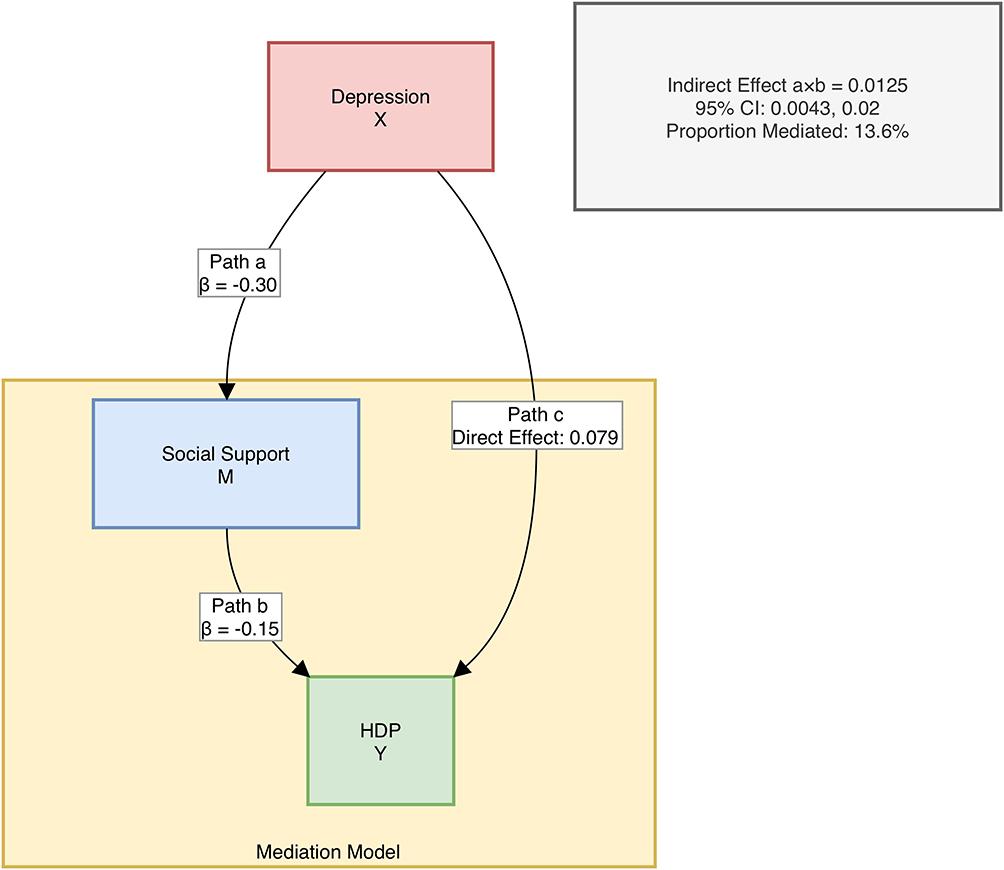 |
Figure 3 The Mediating Role of Social Support in the Depression-HDP Pathway.Schematic diagram illustrating the significant mediating pathway of social support. Values on the arrows are standardized coefficients (β). The indirect effect (a×b) was significant, accounting for 13.6% of the total effect of depression on HDP. |
Finally, we explored the potential buffering role of social support by testing for an interaction between depression and social support in the regression model. The inclusion of the interaction term led to a marginal improvement in model fit (ΔDeviance = 5.95, Δdf = 2, P = 0.051; Table 5), suggesting a potential moderating role of social support in the depression-HDP relationship, consistent with theoretical models. Although this interaction did not reach conventional statistical significance, further investigation with larger samples or more precise measurement tools is warranted to clarify this effect.
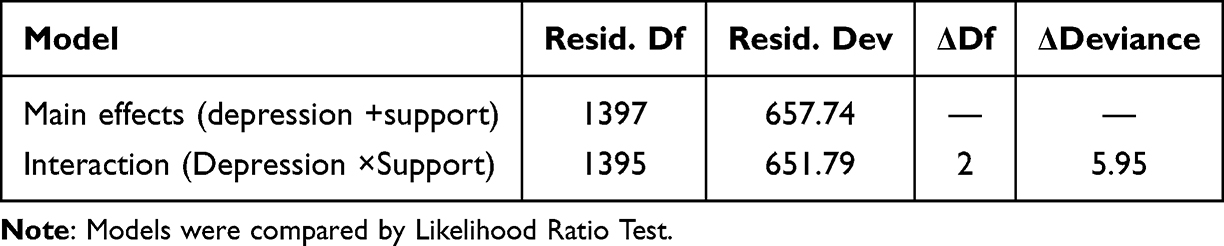 |
Table 5 Model Comparison Testing the Interaction Between Depression and Social Support |
Discussion
Principal Findings
In this prospective cohort of Chinese pregnant women, we identified a strong association between first-trimester depressive symptoms and subsequent HDP risk. Importantly, we found that a significant portion of this association was mediated by the level of perceived social support.
Comparison with Literature
Previous research has consistently linked antenatal depression with adverse outcomes, including HDP, with studies highlighting the role of inflammatory pathways, neuroendocrine dysregulation, and behavioral factors in this association.14,32,33 While some studies have examined the link between social support and HDP, findings have been inconsistent, with some studies showing protective effects of social support.34–36 Our findings contribute to this literature by demonstrating the importance of early pregnancy in HDP development and the potential mediating role of social support in mitigating the effects of depression.
Possible Mechanisms
The observed association between depression and HDP may involve biological pathways such as autonomic dysregulation, neuroendocrine disruption, and behavioral risk factors (eg, poor sleep, unhealthy lifestyle).37–39 Social support may mitigate these effects by reducing stress, enhancing coping mechanisms, and promoting mental well-being.40,41 These mechanisms align with the observed protective role of social support in reducing HDP risk.
Strengths and Limitations
The strengths of our study include the prospective cohort design, the use of validated instruments for measuring depression and social support, and the comprehensive statistical analysis. However, there are several limitations. First, the use of self-reported measures for depression and social support may introduce bias. Second, residual confounding from unmeasured factors such as diet, stress, and genetics cannot be ruled out. Third, our study was conducted in a single center in Xuzhou, China, which limits the generalizability of our findings to other populations. Future studies should address these limitations by using larger, multi-center samples and incorporating additional measures to control for potential confounders.
Implications for Practice and Research
Our findings have important implications for prenatal care. They suggest that routine depression screening at the first prenatal visit could help identify women at risk for HDP and allow for early intervention.42 Implementing targeted social support interventions, such as structured peer-support groups, WeChat-based counselling, or hospital-community linked doula programmes, could offer a scalable strategy to mitigate HDP risk within the Chinese maternity-care system.43,44
To translate this evidence into action, future research should pursue several key directions. Multi-center prospective studies and randomized controlled trials are needed to validate our mediation findings and conclusively determine whether enhancing social support can reduce HDP incidence among depressed pregnant women.45–47 Furthermore, integrating biomarkers of stress (inflammatory cytokines, HPA-axis hormones) into these studies will help elucidate the underlying biological pathways and identify the subgroups of women most likely to benefit from psychosocial interventions.48
Conclusions
In conclusion, first-trimester depression is a significant risk factor for HDP, while social support serves both protective and mediating roles. Integrating early depression screening and social support enhancement into routine prenatal care could be a viable strategy for HDP prevention. Future multi-center studies are needed to confirm these findings and explore underlying biological pathways.
Data Sharing Statement
The de-identified dataset generated during this study is not publicly available due to patient privacy restrictions under Chinese medical ethics regulations but is accessible from the corresponding author upon reasonable request. Data requests require approval by the Xuzhou Central Hospital Institutional Review Board.
Ethics Approval and Consent to Participate
The Xuzhou Central Hospital Institutional Review Board granted ethical approval for the study protocol, and each participant signed a written informed consent form (XZXY-LK-20250328-0036).
Acknowledgments
We thank the medical staff of Xuzhou Central Hospital for their assistance in data collection.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Consent for Publication
Written informed consent for publication was obtained from all participants.
Funding
This work was supported by the Xuzhou Central Hospital (YLZLXZ24K008).
Disclosure
The authors declare no competing interests in this work.
References
1. Chappell LC, Cluver CA, Tong S, Tong S. Pre-eclampsia. Lancet. 2021;398(10297):341–354. doi:10.1016/S0140-6736(20)32335-7
2. Abalos E, Cuesta C, Grosso AL, Chou D, Say L. Global and regional estimates of preeclampsia and eclampsia: a systematic review. Eur J Obstet Gynecol Reprod Biol. 2013;170(1):1–7. doi:10.1016/j.ejogrb.2013.05.005
3. Li X, Zhang W, Lin J, et al. Hypertensive disorders of pregnancy and risks of adverse pregnancy outcomes: a retrospective cohort study of 2368 patients. Hum. Hypertens. 2021;35(1):65–73.
4. Nisar A, Yin J, Waqas A, et al. Prevalence of perinatal depression and its determinants in Mainland China: a systematic review and meta-analysis. J Affective Disorders. 2020;277:1022–1037. doi:10.1016/j.jad.2020.07.046
5. Howard LM, Molyneaux E, Dennis CL, Rochat T, Stein A, Milgrom J. Non-psychotic mental disorders in the perinatal period. Lancet. 2014;384(9956):1775–1788. doi:10.1016/S0140-6736(14)61276-9
6. Tang X, Lu Z, Hu D, Zhong X. Influencing factors for prenatal stress, anxiety and depression in early pregnancy among women in Chongqing, China. J Affective Disorders. 2019;253:292–302. doi:10.1016/j.jad.2019.05.003
7. Lahti-Pulkkinen M, Girchenko P, Robinson R, et al. Maternal depression and inflammation during pregnancy. Psychol. Med. 2020;50(11):1839–1851. doi:10.1017/S0033291719001909
8. Lin D, Chen Y. Maternal depression and preeclampsia: effects on the maternal and offspring’s mental and physical health. Heart and Mind. 2022;6(1):16–21. doi:10.4103/hm.hm_41_21
9. Shay M, MacKinnon AL, Metcalfe A, et al. Depressed mood and anxiety as risk factors for hypertensive disorders of pregnancy: a systematic review and meta-analysis. Psychol med. 2020;50(13):2128–2140. doi:10.1017/S0033291720003062
10. Conde A, Figueiredo B, Tendais I, et al. Mother’s anxiety and depression and associated risk factors during early pregnancy: effects on fetal growth and activity at 20–22 weeks of gestation. J Psychosomatic Obstet Gynecol. 2010;31(2):70–82. doi:10.3109/01674821003681464
11. Burton GJ, Fowden AL. The placenta: a multifaceted, transient organ. Philosophical transactions of the Royal Society of London. Series B, Biol Sci. 2015;370(1663):20140066. doi:10.1098/rstb.2014.0066
12. Sanghavi M, Rutherford JD. Cardiovascular physiology of pregnancy. Circulation. 2014;130(12):1003–1008. doi:10.1161/CIRCULATIONAHA.114.009029
13. Lancaster CA, Gold KJ, Flynn HA, Yoo H, Marcus SM, Davis MM. Risk factors for depressive symptoms during pregnancy: a systematic review. Am J Clin Exp Obstet Gynecol. 2010;202(1):5–14. doi:10.1016/j.ajog.2009.09.007
14. Alder J, Fink N, Bitzer J, Hösli I, Holzgreve W. Depression and anxiety during pregnancy: a risk factor for obstetric, fetal and neonatal outcome? A critical review of the literature. J Matern Fetal Neonatal Med. 2007;20(3):189–209.
15. Grigoriadis S, VonderPorten EH, Mamisashvili L, et al. The impact of maternal depression during pregnancy on perinatal outcomes: a systematic review and meta-analysis. J Clini Psych. 2013;74(4):8615. doi:10.4088/JCP.12r07968
16. Zhang S, Ding Z, Liu H, et al. Association between mental stress and gestational hypertension/preeclampsia: a meta-analysis. Obstetrical Gynecol Surv. 2013;68(12):825–834. doi:10.1097/OGX.0000000000000009
17. Ngai FW, Chan SW. Stress, maternal role competence, and satisfaction among Chinese women in the perinatal period. Res Nurs Health. 2012;35(1):30–39. doi:10.1002/nur.20464
18. Cheng CY, Pickler RH. Effects of stress and social support on postpartum health of Chinese mothers in the United States. Res Nurs Health. 2009;32(6):582–591.
19. Gariépy G, Honkaniemi H, Quesnel-Vallée A. Social support and protection from depression: systematic review of current findings in Western countries. Br J Psychiatry. 2016;209(4):284–293. doi:10.1192/bjp.bp.115.169094
20. Cox JL, Holden JM, Sagovsky R. Detection of postnatal depression. Development of the 10-item edinburgh postnatal depression scale. Br J Psychiatry. 1987;150:782–786. doi:10.1192/bjp.150.6.782
21. Lee DT, Yip SK, Chiu HF, et al. Detecting postnatal depression in chinese women. validation of the chinese version of the edinburgh postnatal depression scale. Br J Psychiatry. 1998;172:433–437. doi:10.1192/bjp.172.5.433
22. Lau Y, Wang Y, Yin L, Chan KS, Guo X. Validation of the mainland Chinese version of the EdinburHDP postnatal depression scale in Chengdu mothers. Int. J. Nurs. Stu. 2010;47(9):1139–1151. doi:10.1016/j.ijnurstu.2010.02.005
23. Xiao S. Theoretical basis and research application of social support rating scale. J Clini Psych. 1994;4(2):98.
24. Yang Y, Wei BR, Guo SB. Development of a social resource support scale for pregnant women with gestational diabetes and its test of validity and reliability. chinese. J Nurs. 2022;57(12):1499–1506.
25. Shiwen S, Junqin L, Huilian P. Survey and analysis on present situation of social support and family care for pregnant women with fetal abnormality. J Nurs Rehabil. 2018.
26. Brown MA, Magee LA, Kenny LC, et al. International Society for the Study of Hypertension in Pregnancy (ISSHP). Hypertensive Disorders of Pregnancy: ISSHP classification, diagnosis, and management recommendations for international practice. hypertension. 2018;72(1):24–43.
27. Wu P, Green M, Myers JE. Hypertensive disorders of pregnancy. BMJ. 2023;e071653. doi:10.1136/bmj-2022-071653
28. Magee LA, Smith GN, Bloch C, et al. Guideline No. 426: hypertensive disorders of pregnancy: diagnosis, prediction, prevention, and management. J Obstet Gynaecology Canada. 2022;44(5):547–571. doi:10.1016/j.jogc.2022.03.002
29. Winkel S, Einsle F, Pieper L, Höfler M, Wittchen HU, Martini J. Associations of anxiety disorders, depressive disorders and body weight with hypertension during pregnancy. Arch Women’s Mental Health. 2015;18:473–483. doi:10.1007/s00737-014-0474-z
30. Hayes AF. (2017). introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach. Guilford publications.
31. Tingley D, Yamamoto T, Hirose K, Keele L, Imai K. Mediation: r package for causal mediation analysis. J. Stat. Softw. 2014;59:1–38. doi:10.18637/jss.v059.i05
32. Agrawal A, Wenger NK. Hypertension during pregnancy. Curr Hypertens Rep. 2020;22(9):64. doi:10.1007/s11906-020-01070-0
33. Rouleau CR, Tomfohr-Madsen LM, Campbell TS, Letourneau N, O’Beirne M, Giesbrecht GF. The role of maternal cardiac vagal control in the association between depressive symptoms and gestational hypertension. Biol. Psychol. 2016;117:32–42. doi:10.1016/j.biopsycho.2016.02.002
34. Al-Mutawtah M, Campbell E, Kubis HP, Erjavec M. Women’s experiences of social support during pregnancy: a qualitative systematic review. BMC Pregnancy Childbirth. 2023;23(1):782. doi:10.1186/s12884-023-06089-0
35. Hinton L, Dumelow C, Hodgkinson J, et al. ‘Nesting networks’: women’s experiences of social network support in hiHDP-risk pregnancy. Midwifery. 2023;120:103622. doi:10.1016/j.midw.2023.103622
36. Havranek EP, Mujahid MS, Barr DA, et al. Social determinants of risk and outcomes for cardiovascular disease: a scientific statement from the American Heart Association. Circulation. 2015;132(9):873–898. doi:10.1161/CIR.0000000000000228
37. Njukang NE, Thomas Obinchemti EGBE, Sama M, Yoah TA, Kamgno J. Determinants of behavioral risk factors of hypertensive disorders in pregnancy. Obstet Gynaecol Res. 2020;3(3):172–189.
38. Qiu W, Cai X, Zheng C, Qiu S, Ke H, Huang Y. Update on the relationship between depression and neuroendocrine metabolism. Front Neurosci. 2021;15:728810. doi:10.3389/fnins.2021.728810
39. Fang H, Tu S, Sheng J, Shao A. Depression in sleep disturbance: a review on a bidirectional relationship, mechanisms and treatment. J Cell & Mol Med. 2019;23(4):2324–2332. doi:10.1111/jcmm.14170
40. Żyrek J, Klimek M, Apanasewicz A, et al. Social support during pregnancy and the risk of postpartum depression in Polish women: a prospective study. Sci Rep. 2024;14(1):6906. doi:10.1038/s41598-024-57477-1
41. Nylen KJ, O’Hara MW, Engeldinger J. Perceived social support interacts with prenatal depression to predict birth outcomes. J. Behav. Med. 2013;36:427–440. doi:10.1007/s10865-012-9436-y
42. Avalos LA, Chen H, Li DK. Antidepressant medication use, depression, and the risk of preeclampsia. CNS spectrums. 2015;20(1):39–47.
43. Norazman CW, Lee LK. The influence of social support in the prevention and treatment of postpartum depression: an intervention-based narrative review. Women’s Health. 2024;20(17455057241275587).
44. Zheng Z, Feng T, Xu J, Zhang X, Yu X. An evaluation of the health economics of postnatal depression prevention and treatment strategies in China: a cost-effectiveness analysis. Healthcare. 2024;12(11):1076. doi:10.3390/healthcare12111076
45. Anbari K, Baharvand P, Khosravi P. Comparing anxiety and perceived social support in hypertensive and non-hypertensive pregnant women in khorramabad, Western Iran. Iranian. J Nurs Midwifery Res. 2025;30(4):572–578.
46. Caplan M, Keenan-Devlin LS, Freedman A, et al. Lifetime psychosocial stress exposure associated with hypertensive disorders of pregnancy. Am. J. Perinatol. 2021;38(13):1412–1419. doi:10.1055/s-0040-1713368
47. Bedaso A, Adams J, Peng W, Sibbritt D. The relationship between social support and mental health problems during pregnancy: a systematic review and meta-analysis. Reproductive Health. 2021;18:1–23. doi:10.1186/s12978-021-01209-5
48. Wu D, Chen S, Zhong X, Zhang J, Zhao G, Jiang L. Prevalence and factors associated with antenatal depressive symptoms across trimesters: a study of 110,584 pregnant women covered by a mobile app-based screening programme in Shenzhen, China. BMC Pregnancy Childbirth. 2024;24(1):480. doi:10.1186/s12884-024-06680-z
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.