Back to Journals » Journal of Healthcare Leadership » Volume 14
The Relation Between Organizational Justice and Counter-Productive Work Behavior Among Health Care Professionals in Jimma Zone Public Health Institutions
Authors Adugna K ![]() , Birhanu B
, Birhanu B ![]() , Kebede A
, Kebede A ![]() , Abraham G, Asefa Y, Gezahign M
, Abraham G, Asefa Y, Gezahign M ![]() , Gunja G, Gelana B
, Gunja G, Gelana B ![]()
Received 27 May 2022
Accepted for publication 29 July 2022
Published 6 August 2022 Volume 2022:14 Pages 119—130
DOI https://doi.org/10.2147/JHL.S365129
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Pavani Rangachari
Kebebe Adugna,1 Bezawit Birhanu,2 Alemi Kebede,3 Gelila Abraham,2 Yisalemush Asefa,2 Matebu Gezahign,2 Gemechis Gunja,4 Beshea Gelana2
1School of Nursing, Jimma University, Jimma, Oromia, Ethiopia; 2Department of Health Policy and Management, Jimma University, Jimma, Oromia, Ethiopia; 3Department of Reproductive Health and Nutrition, Jimma University, Jimma, Oromia, Ethiopia; 4Clinical Governance and Quality Improvement, Jimma Medical Center, Jimma University, Jimma, Oromia, Ethiopia
Correspondence: Kebebe Adugna, School of Nursing, Jimma University, PO Box: 378, Jimma, Oromia, Ethiopia, Tel +251 910071501, Email [email protected] Beshea Gelana, Department of health policy and management, Jimma University, PO Box: 378, Jimma, Ethiopia, Tel +251 921833996, Email [email protected]
Background: Counterproductive behavior costs organizations and their members which will ultimately affect work-related outcomes and organizational success. Organizational justice has the potential to affect the level of counter productive behavior. However, there is a paucity of studies to show the link between counterproductive behavior and organizational justice dimensions in the Ethiopian health care system context. Therefore, the purpose of this research was to look into the link between organizational justice, and counterproductive work behavior among health care professionals.
Methods: The 395 study participants were chosen using a facility-based cross-sectional study methodology. A proportionate stratified systematic random sampling technique was deployed to select study participants from health facilities. Data was gathered using a structured self-report questionnaire by CWB Scale that was developed by Spector and Fox (2005) with Cronbach’s alpha of an average of (0.84– 0.87). Data was obtained, cleaned, and entered by Epidata3.1. Finally, for descriptive and inferential statistical analysis, the data was exported to SPSS version 23.0.
Results: According to the findings, 159 (40.3%) of the study participants engaged in counterproductive job activities. Organizational justice was assumed to be fair by about half of the respondents, 202 (52.2%). Distributive Justice (=− 0.141, p.05) was found to be a significant and negative predictor of counterproductive work behavior in the regression analysis. Age (β=− 0.014, p< 0.05), the average number of hours worked every week (β=− 0.009, p< 0.05), and experience (β=0.016, p< 0.05) were found to be significant predictors of the counterproductive work behaviors.
Conclusion and Recommendation: This study indicated that distributive justice show significant contribution in reduction of counterproductive work behaviour.As a result, improving organizational justice can aid to reduce counterproductive work behavior which in turn increases the facility’s productivity.
Keywords: counterproductive, work behavior, organizational justice, health care professional, Ethiopia
Introduction
For a better understanding of organizational characteristics, justice is a crucial fact. Justice in the workplace is a term used to refer to individuals’ perceptions about the fairness of decisions and decision-making processes within organizations and the influences of those perceptions on the behavior of fairness in organizational contexts.1,2 Fair treatment has a considerable impact on individual satisfaction, absenteeism, dedication, and attitudes, according to a study on organizational justice.3,4
Organizational justice is generally identified as three or four specific types of justice, each referring to fairness perceptions in a specific set of work contexts: Interactional justice, distributive justice, and procedural justice (sometimes broken down further into informational justice and interpersonal justice).5,6 Employee perceptions of the fairness of organizational assignments, as well as the outcomes, were addressed by distributive justice.7,8 Distributive justice conveys a sense of concern for employee well-being and their contribution to organizational success when rewards and resources are fairly distributed, while procedural justice is concerned with decision-making procedures being equitable, and Interactional justice is worried about supervisors treating employees with dignity and respect.9,10
The long-term viability of an organization is largely determined by the people that work there. Their emotions, thoughts, attitudes, and actions all had a significant impact on the organization’s success or failure.11 On the other side, the presence of justice within the organization has a good impact on the employee’s emotional well-being.12 Furthermore, it raises needs, which implies delivering a benefit based on one’s needs, resulting in the worker becoming extremely engaged with the firm.13
In the context of health, the word “organizational justice” relates to how fair healthcare professionals perceive workplace procedures, interactions, and outcomes. These insights can influence attitudes, and behavior for good or ill, successively having a positive or negative impact on work-related outcomes, and organizational success.14 Counterproductive work behaviors(CWBs) are one among such behavior which is defined as “voluntary behavior that violates significant organizational norms and in so doing threatens the well-being of an organization and its members or both” which could harm the interest of the organization either directly or indirectly by hurting the staff which resultantly reduces their effectiveness.15–19
CWBs have five main dimensions: 1. Abuse: It consists of harmful behaviors directed toward coworkers that harm either physically or psychologically through making threats, nasty comments, ignoring the person, or undermining the person’s ability to work effectively. 2. Production Deviance: it’s the purposeful failure to perform job tasks effectively the way they are speculated to be performed. 3. Sabotage: it’s defacing or destroying property belonging to the employer; intentional wasting the materials within the organization, and purposely dirtying or littering the place of labor. 4. Theft: Stole something belonging to your employer, delaying the duties to induce an extra-time salary. 5. Withdrawal: It consists of behaviors that restrict the number of your time working but is required by the organization. It includes absence, arriving late or leaving early, and taking longer breaks than authorized.20
CWB involves a broad range of negative organizational behaviors of aggressive or negative nature that will involve acts of production deviance, withdrawal, offending colleagues, and poor quality work.21 It should be noted that these negative organizational behaviors have negative direct impacts on employees and organizations. These impacts involve social, financial, and psychological impacts, like low levels of production, commitment, job loyalty, and job satisfaction. Such impacts also involve an increase in the rates of employees turnover and absence from work.17
Research has shown that CWBs threaten the organization and therefore the general health of its members. For example, it’s been stated that 58% of female workers potentially face mobbing behaviors, and 24% face sexual harassment. Besides, it was found that 25% of employees within the USA lose their jobs due to the misuse of the web. Further, thefts exist in the majority of workplaces. At the same time, CWB is additionally said to cause major economic loss.22
Organizations stand to lose a lot of dollars through employees theft and sabotage costing over four billion dollars additionally to human-related costs like low morale, turnover, suffering stress-related problems, have decreased productivity, and lost work time,23,24 and thanks to these it must not be overlooked, and interventions must be taken to reduce the higher risk of potential loss because of CWB because these not only affect the organization but also the well-being and performance of employees within the workplace.25
Subjecting the workers to unjust (unequal) treatment shall not make them feel unsatisfied merely. They shall also develop feelings of anger toward the organization that makes them do certain acts, like (slow down, theft and corruption), negative behaviors, negligence, and resistance to alter which results in a decrease in the employee’s organizational loyalty level.26 Contrary to the current, if the worker is treated fairly, he/she shall display positive attitudes and high morale and feel happy with his/her workgroup leading him to possess high levels of job loyalty, belonging, and display positive.27
The major aspects of organizational justice are represented in fighting against employees’ sense of being treated unfairly and using power cruelly or controlling employees cruelly shall lead the oppressed workgroups to create negative attitudes, perform negative behaviors and develop feelings of self-hatred. It shall also cause the occurrence of conflicts between employees.28
The findings in the preceding literature are primarily from developed countries and other African countries but did not include all types health care professionals from multidisciplinary team and also did not address all levels of the three-tier systems. There is no evidence from Ethiopia about the counterproductive behavior and organizational justice relationships of healthcare organizations. According to studies, Ethiopia faces numerous challenges in providing quality health care services at all levels of the three-tier system due to a variety of factors including a shortage of qualified healthcare workers, a lack of leadership commitment, unequal resource distribution, and limited supplies.29 These intrinsic or extrinsic challenges may have its own role in contributing toward the negative work related outcomes. Thus, we aimed to identify the level of counterproductive behaviours and its relationship with organizational justice in health care setting found in the Jimma Zone in Southwest Ethiopia.
Materials and Methods
Study Setting and Design
The study was conducted in Jimma Zone. There are 18 districts and one town administration in the zone. In the Jimma zone, there are seven hospitals (one referral and teaching hospital, one general hospital, and five primary hospitals), as well as 115 health centers and 520 health poststhe. In the Jimma zone public health facilities, there is 2500 health care personnel of all types.
The populations being served by the public health facilities are estimated to be more than 20 million annually including people from border zones and South Sudan while the Jimma University Medical center has a Lion share. From December 2019 to January 2019, a facility-based cross-sectional investigation was undertaken.
Population
The source population was all health care workers (Physicians, Nurses, Midwives, Public health officers, Laboratory, pharmacy, Environmental, and Anesthesia) working in public health institutions in the Jimma zone, southwest Ethiopia. The study population was all selected health care workers. Whereas the included people in this study were who had worked for at least six months. Private health care institutions were excluded from the study to avoid double counting since government health workers could possibly part-timer in the private institution.
Sampling Procedure and Sample Size Determination
The sample size was determined using the single population proportion formula by considering a 50% proportion as there is no study at a 95% of confidence interval level. The formula for calculating the sample size (n) is:

Where n= Minimum sample size
p= an estimate of the prevalence rate for the population
d= the margin of the sampling error
Zα/2 = standard normal variance (1.96)2 is mostly 5% ie, with 95% confidence level
n = (1.96)2x0.5 (1–0.5)
(0.05) 2
n= 384
For possible non-response, 10% of the calculated sample was added and the overall sample size was 422.
Health-care facilities were chosen at random. The sample was then proportionally distributed to hospitals and health centers based on the number of healthcare personnel they have. Finally, respondents were chosen using a systematic sample of workers’ registration logbooks from each facility, with the first participant chosen by lottery.
Data Collection Procedure
The data were collected by using a pre-tested structured interviewer-administered questionnaire through face-to-face interviews.
Measurement
CWB Scale developed by Spector and Fox (2005) with the Cronbach’s alpha of an average of (0.84–0.87) was adopted which has five subscales of abuse (harmful and malicious behaviors that affect other people), production deviance (purposely doing the job incorrectly or allowing errors to occur), sabotage (destroying the physical environment), theft and withdrawal (avoiding work, absence work or tardiness).20 The questions were carefully designed and worded as properly as possible to minimize response bias and non-response bias. To reduce response bias, the properly targeted respondents for the survey were identified by an interviewer-administered questionnaire, and the framing of neutral questions was also taken into consideration. Questions and answers on the Likert Scale were thoroughly examined, and anonymous replies were permitted. Responses are made on a five-point frequency scale of never, once or twice, once or twice per month, once or twice a per week, or every day. Data was collected by 10 trained data collectors. A modified 19-item scale with an overall reliability coefficient of 0.94 was used to measure justice.30
Study Variables
Variable that is dependent: counterproductive work behavior.
Variables That are Not Dependent
Dimensions of organizational justice, Health care professionals’ related factors, Health facility characteristics.
Statistical Analysis and Data Management
Each completed questionnaire was assigned a unique code after the data was reviewed for completeness. Epidata version 3.1 was used to enter the data, which was then exported to SPSS version 23 for analysis. The study population was described using descriptive statistics with key factors. The outcome variable’s mean score was generated and used to assess the extent of counterproductive work behavior and organizational fairness. The Spearman correlation coefficient was used to measure the level of association between organizational justice dimensions and counterproductive work behavior aspects.
Hierarchical regression analysis was used to explore possible predictors and changes in counterproductive work behavior in the final model. As a result, variables of socio-demographic and facility-related features with a p-value of less than 0.25 in bivariate analysis were included in the multivariable linear regression in the first phase. The three organizational dimensions were then added to the final regression analysis to search for the independent impact of organizational justice. For interpretation, Beta and Adjusted R2 were used, and statistically significant predictors were declared at a p-value of 0.05 and a 95% confidence interval.31
Ethical Considerations
Jimma University’s Institutional Review Board granted ethical approval to conduct research. Furthermore, permission was obtained from all Selected zonal offices and administrators of public health facilities. Informed written consent from a healthcare professional was obtained. The respondents’ privacy and dignity were protected by keeping all information anonymous and confidential. This paper follows the principles outlined in the Helsinki Declaration.
Result
From a total of 422 questionnaires, 395 were returned which made the overall response rate for this study 93.6%. The reason for incompleteness was the absence of health care professionals on three repeated visits and lack of interest. Most of the respondents 235(59.5%) were male. The predominant age range was 21 to 30 years old 330(83.5%). Most respondents 246 (62.3%) had a bachelor’s degree. Nearly half 219(55.4%) were single, and the majority of the 276(69.9%) have experience of fewer than five years. Most participants 230(58.2%) were nurses (Table 1).
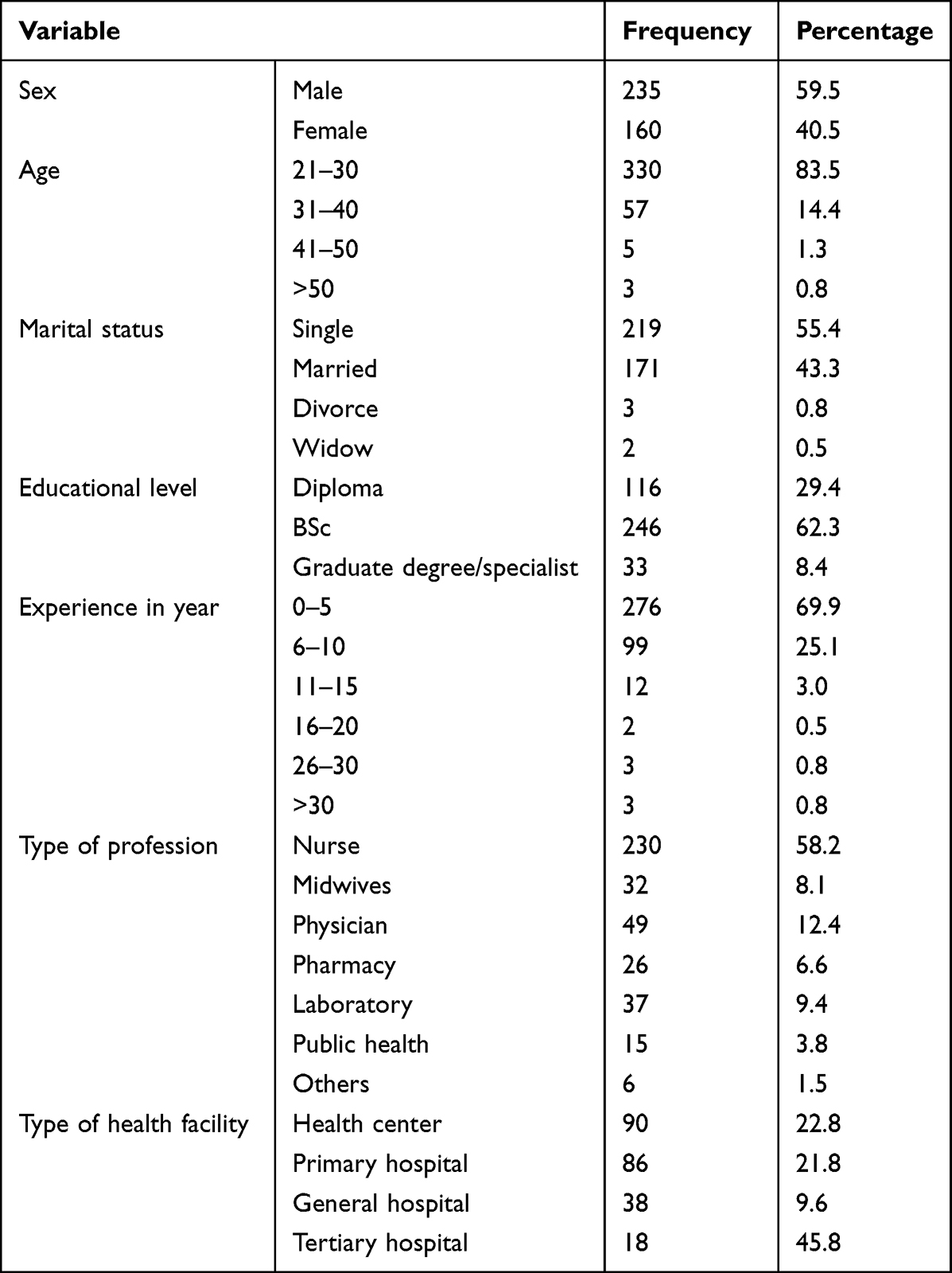 |
Table 1 Socio-Demographic Characteristics of Counterproductive Work Behavior and Organizational Justice Dimensions (n = 395) |
The overall mean of organizational justice was 2.7281 (SD 0.86159) in distributive justice had a higher mean score of 2.8515(SD 0.94908, and procedural justice had the lowest mean score of 2.6472(SD 0.91424). Where the counterproductive work behaviors mean score was 1.7308 (SD 0.75492), in which abuse had the highest mean score of 1.7562 (SD 0.78058) and theft had the lowest mean score of 1.6739 (SD 0.84048) (Table 2).
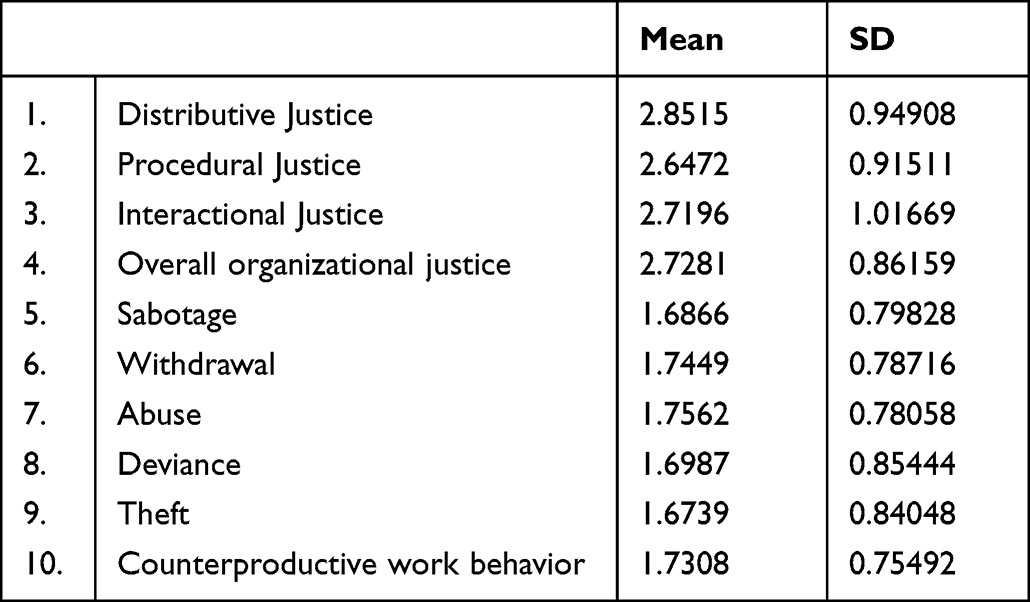 |
Table 2 Mean Score and Standard Deviation of Counterproductive Work Behavior and Organizational Justice Dimensions (n = 395) |
The study showed more than half of the people who work in the healthcare industry 236(59.7%) practiced non-Counterproductive work behavior (NCWB). Specifically, 137(59.6%) nurses, 13(40.6%) midwives, 32(65.3%) physicians, 14(53.8%) of pharmacy, 26(70.3%) laboratories, and 10(66.7%) public health reported NCWB (Figure 1).
 |
Figure 1 Perceived level of counterproductive work behaviors among health care professionals in Jimma Zone public health facility, southwest Ethiopia (n=395). |
The result showed that about half of health care workers’ 206 (52.2%) perception of organizational justice was fair. Specifically, 117(56.8%) nurses, 16(50%) midwives, 28(57.1%) physicians, 17(65.4%) of pharmacy, 20(54.1%) laboratories, and 8(53.3%) public health reported fair justice (Figure 2).
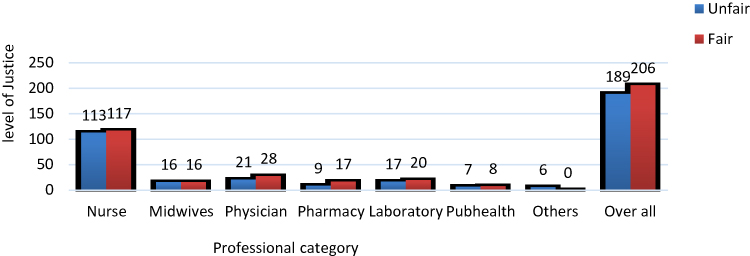 |
Figure 2 Perceived level of organizational justice among health care professionals in Jimma Zone public health facilities, Southwest Ethiopia (n=395). |
Among 235 male employees, 92(23.3%) have shown behaviors of CWB. Among 160 female employees, 67(17.0%) have shown the behaviors of CWB (Figure 3).
 |
Figure 3 Gender wise Level of occurrence of CWB among Health care professionals in Jimma Zone, Southwest Ethiopia (n=395). |
This study indicated one third (33.4%) of employees from the age group of 21–30 have shown the CWB (Figure 4).
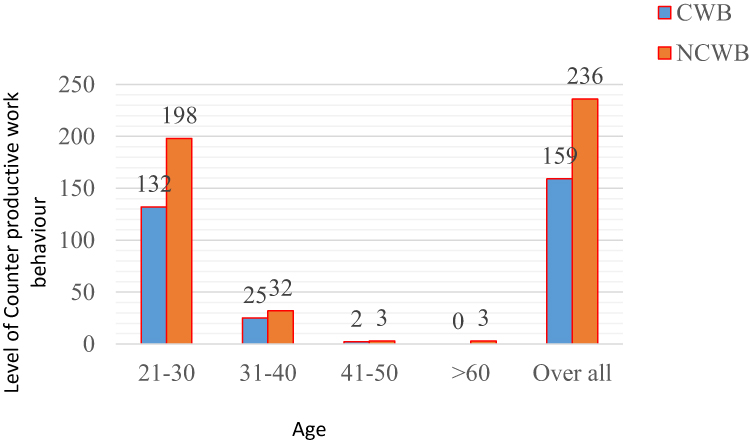 |
Figure 4 Age-wise Level of occurrence of CWB among Health care professionals in Jimma Zone, Southwest Ethiopia (n=395). |
Similarly, this study showed about one-third of 119(30.1%) employees having experience from 0–5 years have shown the CWB (Figure 5).
 |
Figure 5 Percentage of employees in different work experience groups showing CWB among Health care professionals in Jimma Zone, Southwest Ethiopia (n=395). |
The Relationship Between Organizational Justice and Counter-Productive Work Behavior
This study showed that distributive justice was not significantly associated with all five types of the dimension of CWB (sabotage, withdrawal, abuse, deviance, theft). But procedural justice was positively and significantly associated with counter-productive work behavior dimensions sabotage (r=0.14), withdrawal (r=0.14), abuse (r=0.15), deviance (r=0.12), and theft (r=0.12). This study also stated interactional justice had a positive and significantly associated with all five dimensions of counter-productive work behavior dimensions sabotage (r=0.13), withdrawal (r=0.12), abuse (r=0.16), deviance (r=0.10), theft (r=0.13) (Table 3).
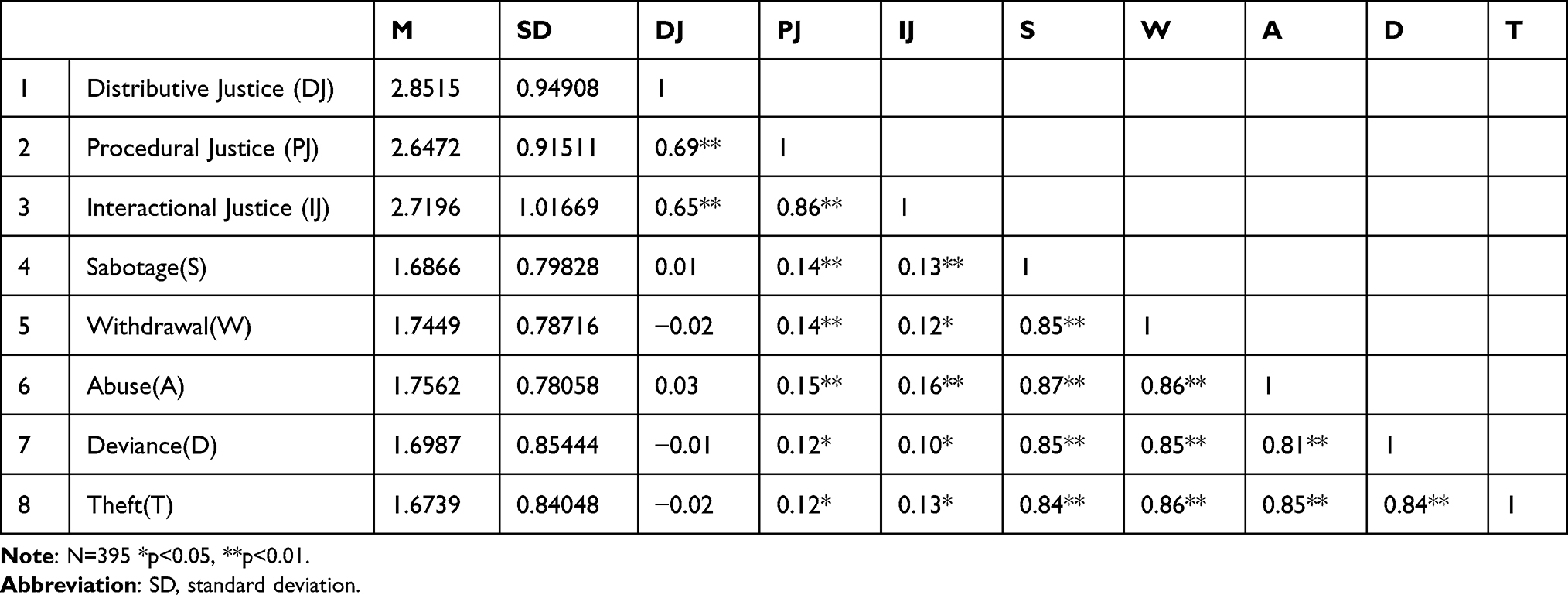 |
Table 3 Correlation Among Dimensions of Organizational Justice and Dimensions of Counterproductive Work Behaviors (n = 395) |
Furthermore, the study result showed that counterproductive work behavior is negatively associated about overall organizational fairness (r = −0.238**P < 0.05) (Table 4).
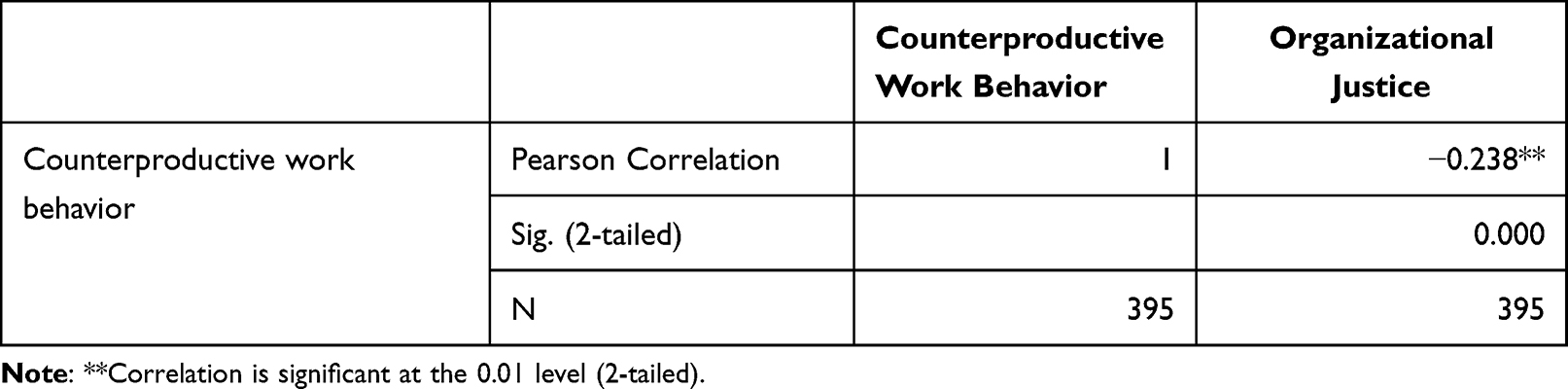 |
Table 4 Overall Correlates of Organizational Justice, and Counterproductive Work Behaviors |
Socio-Demographic and Facility-Related Factors Affecting CWB
Variables such as (age, the average number of hours worked every week, experience in years, educational level, type of profession, type of health facility, and salary) in bivariate regression models with a P-value of <0.25 were included in the first phase. Age, the average number of hours worked every week, and experience in years were found to be significant predictors of the CWB in multivariate regression. Thus, the increase in age by one unit decreases the CWB by −0.014 (P =0.032, CI: −0.026, −0.001). Similarly, the increase in the average number of hours worked every week by one unit decreases the CWB by −0.009 (P =0.027, CI: −0.018, −0.001). But, the increase in the experience by one unit increases the CWB by 0.016 (P =0.042 CI: 0.001, 0.032) (Table 5).
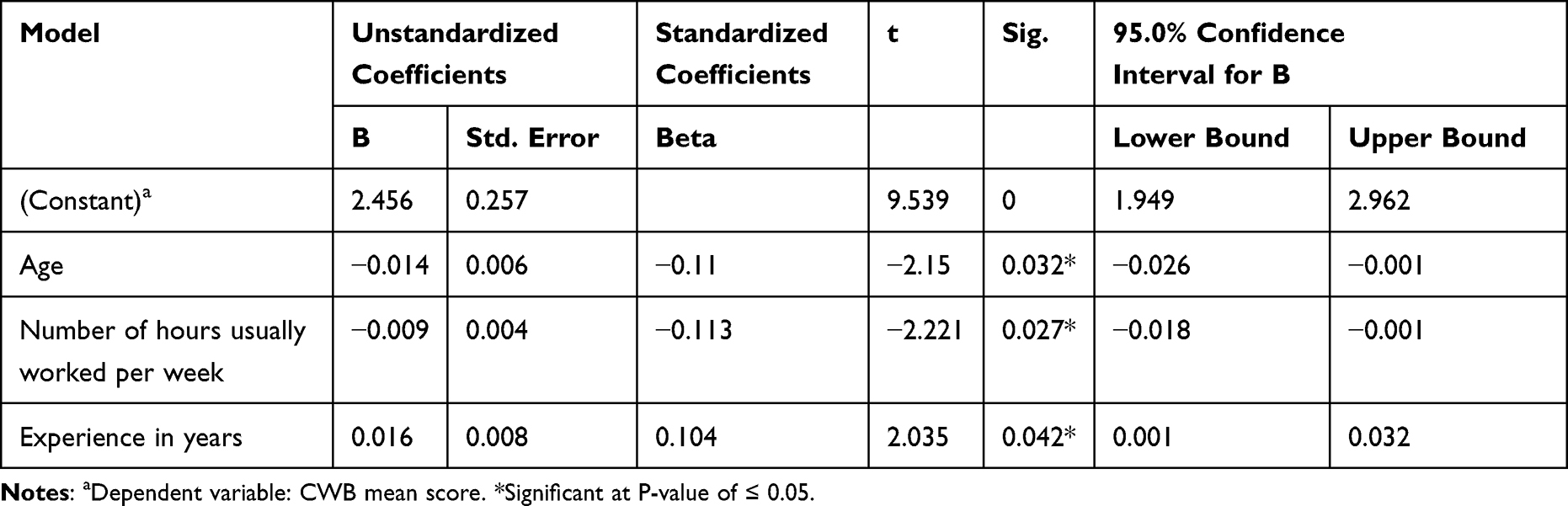 |
Table 5 Predictors of Socio-Demographic and Facility-Related Factors Affecting CWB |
The Influence of Organizational Justice Dimensions on CWB
The second step of the regression analysis revealed that distributive justice was the only justice dimension that was significantly associated with CWB. Thus, the increase in the distributive justice score by one unit decreases the CWB score by −0.141(P =0.011, CI: −0.249, −0.033) (Table 6).
 |
Table 6 The Influence of Organizational Justice Dimensions on CWB |
Discussion
Organizational justice is a comprehensive notion that has grown more important in avoiding counterproductive work behavior because of its favorable impact on job outcomes, attrition, and organizational success.14,32 It could, however, be influenced by a variety of elements such as personal traits, organizational context, leadership and management, and job qualities.33 On the other hand, the organization’s and its workers’ survival and development are dependent on the application of justice.34,35 As a result, this study was carried out to establish the level of CWB and organizational justice in Jimma zone, southwest Ethiopia, among health care workers in public health facilities and their relationship with one another.
In this study, 159(40.3%) of employees have counterproductive work behavior among which 92(23.3%) are males and 67(17.0%) are females. The majority of 132(33.4%) of employees from the age group of 21–30 and 119(30.1%) of employees having experience from 0–5 years have shown the CWB. We found that abuse had the highest correlations with the other variables and abuse was most strongly correlated with sabotage and withdrawal which is incongruent with a study in Bengaluru, India in which 49% of employees have counterproductive work behaviors. The extent of occurrence of CWB is extremely high in females (93%), a greater number of employees from the age group of 26–30 have shown the CWB, 23% of employees engage within the theft dimension of CWB. The least correlated CWBs are Production deviance and Sabotage.25 The differences in the study findings could be related to differences in the study settings (the latter was conducted only in hospitals, whereas ours was conducted in a variety of health facilities), as well as differences in time (study period).
In this study distributive Justice (β=−0.141, p< 0.05) significantly and negatively predicted counterproductive work behavior which is similar to studies in Israel,36 Iraq,37 and Pakistan.38 This means, that if employees feel about organizational allocations are unfair, it makes them violate organizational norms and form negative attitudes, and carry out negative behaviors that threaten the well-being of an organization and its members either directly or indirectly.
Another finding of this study revealed that among socio-demographic and facility-related characteristics, age and the average number of hours worked every week, and experience in years were discovered to be strong CWB predictors. The only significant predictor of the CWB among the organizational justice components was distributive justice (distributive, interactional, and procedural justice). The findings suggest that age, the average number of hours worked every week, experience, and distributive justice may all be factored in predicting the level of CWB.
The unit increase in age decreases the CWB by (β=−0.014, P =0.032) which is similar to other studies.39,40 This is to means that older employees are more likely to engage in organizational citizenship behavior and less likely to engage in CWB than younger employees.41
Similarly, this study result outlined the unit increase in the average number of hours worked every week decreases the CWB by (β=−0.009, P =0.027) which is congruent with a study conducted by Jayanthi & Vanniarajan, 2012 that stated working long hours could serve as an indicator of commitment and productivity in some organizations but incongruent with studies outlined working long hours has direct and indirect ramification for workers and organizations such as counterproductive behavior.42,43
This study result showed that the unit increase in experience increases the CWB by (β=0.016, P =0.042) which is congruent with Hockey’s compensatory regulatory-control model (1993, 1997)44,45 and job-demand resource model46 but incongruent with study reveals that experience does not show in any significance in counterproductive work behaviors of employees.25
The increase in distributive justice score by one unit decreases the CWB score by −0.141(β=−0.141 P<0.05) which is similar to other studies that state that distributive justice has a significant negative effect on CWB.47–49 This research demonstrates that this aspect of organizational justice has a direct and open impact on CWB. This indicates that the less CWB they provide to their company, the more distributive justice they consider fair.
Strength and Limitation of the Study
The study’s strength was that it included health care personnel from all levels of care, from primary to tertiary and all type of health care professionals from multidisciplinary team, but it also had a weakness in that it used only a quantitative method.
Conclusion
This study indicated that there is a link between distributive justice and the counterproductive work behavior dimension. Distributive justice shows a significant contribution to the reduction of counterproductive work behavior. As a result, improving distributive justice can aid to reduce counterproductive work behavior which in turn increases the facility’s productivity. More than half of healthcare professionals in all healthcare settings reported NCWB.
To minimize counterproductive work behavior, organizations should ensure distributive justice in making decisions. Finally, further research is recommended using both quantitative, and qualitative methods which participate both health care professionals, and leaders on large scale In Ethiopia.
Acknowledgments
The cooperation of Jimma University for this research project is much appreciated. We would also like to thank all of the study participants and data collectors.
Disclosure
The authors have declared that they have no conflicts of interest in this study.
References
1. Paul E, Levy C, Christina N. Can reward systems influence the creative individual? Handbook of Organizational Creativity. Elsevier Science; 2004.
2. Lavelle J, Rupp D, Brockner J. Taking a multifoci approach to the study of justice, social exchange, and citizenship behavior: the target similarity model. J Manag. 2007;33(6):841–866.
3. Attia S. The relationship between organizational justice and quality performance among healthcare workers: a pilot study. Sci World J. 2014;2014. doi:10.1155/2014/757425
4. Colquitt J, Conlon D, Wesson M, Porter C, Ng K. Justice at the millennium: a meta-analytic review of 25 years of organizational justice research. J Appl Psychol. 2001;86(3):425. doi:10.1037/0021-9010.86.3.425
5. Srivastava U. Multiple dimensions of organizational justice and work-related outcomes among health-care professionals. Am J Ind Bus Manag. 2015;05(11):666–685.
6. Byrne Z, Cropanzano R. The history of organizational justice: the founders speak. Justice Workplace Theory Pract. 2001;2(1):3–26.
7. Colquitt J. Organizational justice. 2012:526–547.
8. Eisenberger R, Malone G, Presson W, Eisenberger R. Optimizing perceived organizational support to enhance employee engagement. J Occup Health Psychol. 2016;23:151–162. doi:10.1037/ocp0000061
9. Rhoades L, Eisenberger R. Perceived organizational support: a review of the literature. J Appl Psychol. 2002;87(4):698. doi:10.1037/0021-9010.87.4.698
10. Loi R, Hang-Yue N, Foley S. Linking employees’ justice perceptions to organizational commitment and intention to leave: the mediating role of perceived organizational support. J Occup Organ Psychol. 2006;79(1):101–120. doi:10.1348/096317905X39657
11. Ajala EM, Bolarinwa KO. Organisational justice and psychological well-being of employees in the local government service of Osun State, Nigeria. Int Multidiscip J. 2015;9(39):55–72.
12. Garg P, Rastogi R, Paul H. Does perception of justice effect psychological well-being of employees? Does perception of justice effect psychological well-being of employees? Int J Soc Syst Sci. 2014;6:264–284. doi:10.1504/IJSSS.2014.065215
13. Majekodunmi E. The influence of organisational justice on employees ’ commitment in manufacturing firms in oyo state, Nigeria: implications for industrial. Afr J Soc Work. 2015;5(1):92–130.
14. Hoy W, Tarter C. Organizational justice in schools: no justice without trust. Int J Educ Manag. 2004;18:250–259. doi:10.1108/09513540410538831
15. Robinson S, Bennett R. A typology of deviant workplace behaviors: a multidimensional scaling study. Acad Manage J. 1995;38(2):555–572.
16. Bennett R, Robinson S. Development of a measure of workplace deviance. J Appl Psychol. 2000;85(3):349. doi:10.1037/0021-9010.85.3.349
17. Ramshida A, Manikandan K. Organizational commitment as a mediator of counterproductive work behavior and organizational culture. Int J Soc Sci Interdiscip Res. 2013;2(2):59–69.
18. Berry C, Carpenter N, Barratt C. Do other-reports of counterproductive work behavior provide an incremental contribution over self-reports? A meta-analytic comparison. J Appl Psychol. 2012;97(3):613. doi:10.1037/a0026739
19. Yen C, Teng H. The effect of centralization on organizational citizenship behavior and deviant workplace behavior in the hospitality industry. Tour Manag. 2013;36:401–410. doi:10.1016/j.tourman.2012.10.003
20. Spector P, Fox S, Penney L, Bruursema K, Goh A, Kessler S. The dimensionality of counterproductivity: are all counterproductive behaviors created equal? J Vocat Behav. 2006;68(3):446–460. doi:10.1016/j.jvb.2005.10.005
21. Khan A, Quratulain S, Crawshaw J. The mediating role of discrete emotions in the relationship between injustice and counterproductive work behaviors: a study in Pakistan. J Bus Psychol. 2013;28(1):49–61. doi:10.1007/s10869-012-9269-2
22. Mount M, Ilies R, Johnson E. Relationship of personality traits and counterproductive work behaviors: the mediating effects of job satisfaction. Pers Psychol. 2006;59(3):591–622. doi:10.1111/j.1744-6570.2006.00048.x
23. O’Leary-Kelly A, Griffin R, Glew D. Organization-motivated aggression: a research framework. Acad Manage Rev. 1996;21(1):225–253. doi:10.2307/258635
24. Frost A. Ensure dishonesty doesn’t pay. Hum Resour. 2007;2007:71.
25. Roopa D, Nanjundeswaraswamy T, Swamy D. An exploratory study on counterproductive work behaviors of nurses. Int J Eng Manag Res. 2016;6(3):685–692.
26. Dadi V. The black British clerical workers response to psychological contract violation. Int J Hum Resour. 2012;2(4):69–82.
27. Priesemuth M, Arnaud A, Schminke M. Bad behavior in groups: the impact of overall justice climate and functional dependence on counterproductive work behavior in work units. Group Organ Manag. 2013;38(2):230–257. doi:10.1177/1059601113479399
28. Brimecombe M, Magnusen M, Bunds K. Navigating the storm: a counterproductive work behavior and leadership case study in a division I FBS school. Sport Manag Rev. 2014;17(2):219–237. doi:10.1016/j.smr.2013.03.001
29. World Health Organization. Primary Health Care Systems (Primasys). World Health Organization; 2017:1–48.
30. Niehoff B, Moorman R. Justice as a mediator of the relationship between methods of monitoring and organizational citizenship behavior. Acad Manage J. 1993;36(3):527–556.
31. Deressa B, Adugna K, Bezane B, et al. The relationship between organizational commitment and organizational justice among health care workers in Ethiopian Jimma Zone public health facilities. J Healthc Leadersh. 2022;14:5. doi:10.2147/JHL.S345528
32. Jahangir F, Shokrpour N. Three components of organizational commitment and job satisfaction of hospital nurses in Iran. Health Care Manag. 2009;28(4):375–380. doi:10.1097/HCM.0b013e3181b3eade
33. Vagharseyyedin S. An integrative review of literature on determinants of nurses’ organizational commitment. Iran J Nurs Midwifery Res. 2016;21(2):107. doi:10.4103/1735-9066.178224
34. Seyed J, Faraahi M, Taheri A. How different dimensions of organizational justice affect the different dimensions of job and organizational satisfaction. 2009.
35. Rafei-Dehkordi F, Mohammadi S, Yektayar M. Relationship of organizational justice and organizational commitment of the staff in general directorate of youth and sports in Chahar Mahal Va Bakhtiari Province. Eur J Exp Biol. 2013;3(3):696–700.
36. Chernyak-Hai L, Tziner A. Relationships between counterproductive work behavior, perceived justice and climate, occupational status, and leader-member exchange. Rev Psicol Trab Las Organ. 2014;30(1):1–12. doi:10.5093/tr2014a1
37. Ansari M, Maleki S, Mazraeh S, Arab-Khazaeli H. Individual, job, and organizational predictors of counterproductive work behavior. J Basic Appl Sci Res. 2013;3(4):74–86.
38. Saleem F, Gopinath C. Injustice, counterproductive work behavior and mediating role of work stress. Pak J Commer Soc Sci. 2015;9(3):683–699.
39. Pletzer J. Why older employees engage in less counterproductive work behavior and in more organizational citizenship behavior: examining the role of the HEXACO personality traits. Personal Individ Differ. 2021;173:110550. doi:10.1016/j.paid.2020.110550
40. O’Driscoll M, Roche M. Age, organizational citizenship behaviors, and counterproductive work behaviors. In: Pachana NA, editor. Encyclopedia of Geropsychology. Singapore: Springer; 2017:113–122. doi:10.1007/978-981-287-082-7_196
41. Ng T, Feldman DC. The relationship of age to ten dimensions of job performance. J Appl Psychol. 2008;93(2):392–423. doi:10.1037/0021-9010.93.2.392
42. Morris M, Messal C, Meriac J. Core self-evaluation and goal orientation: understanding work stress. Hum Resour Dev Q. 2013;24(1):35–62. doi:10.1002/hrdq.21151
43. Rodríguez I, Kozusznik M, Peiró J. Development and validation of the Valencia Eustress-Distress Appraisal Scale. Int J Stress Manag. 2013;20(4):279. doi:10.1037/a0034330
44. Hockey G, Wiethoff M. Cognitive-energetical control mechanisms in the management of work demands and psychological health. Adv Space Biol Med. 1993;3:139–150.
45. Hockey G. Compensatory control in the regulation of human performance under stress and high workload: a cognitive-energetical framework. Biol Psychol. 1997;45(1–3):73–93. doi:10.1016/S0301-0511(96)05223-4
46. Jones F, Fletcher B. Job control and health. Handb Work Health Psychol. 1996;1996:33–50.
47. Devonish D, Greenidge D. The effect of organizational justice on contextual performance, counterproductive work behaviors, and task performance: investigating the moderating role of ability-based emotional intelligence. Int J Sel Assess. 2010;18(1):75–86. doi:10.1111/j.1468-2389.2010.00490.x
48. El Akremi A, Vandenberghe C, Camerman J. The role of justice and social exchange relationships in workplace deviance: test of a mediated model. Hum Relat. 2010;63(11):1687–1717. doi:10.1177/0018726710364163
49. Colquitt J, Scott B, Rodell J, et al. Justice at the millennium, a decade later: a meta-analytic test of social exchange and affect-based perspectives. J Appl Psychol. 2013;98(2):199. doi:10.1037/a0031757
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.