Back to Journals » Research and Reports in Urology » Volume 12
The Protective Effect of Lycopene on Prostate Growth Inhibitory Efficacy by Decreasing Insulin Growth Factor-1 in Indonesian Human Prostate Cancer Cells
Authors Tjahjodjati, Sugandi S, Umbas R, Satari M
Received 28 September 2019
Accepted for publication 24 March 2020
Published 17 April 2020 Volume 2020:12 Pages 137—143
DOI https://doi.org/10.2147/RRU.S232745
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jan Colli
Tjahjodjati,1 Suwandi Sugandi,1 Rainy Umbas,2 Mieke Satari3
1Department of Urology, Faculty of Medicine, Padjadjaran University, Hasan Sadikin Hospital, Bandung, Indonesia; 2Department of Urology, Faculty of Medicine University of Indonesia, Cipto Mangunkusumo Hospital, Jakarta, Indonesia; 3Doctoral Program, Faculty of Medicine, Padjadjaran University, Bandung, Indonesia
Correspondence: Tjahjodjati Jl. Pasteur No. 38, Sukajadi, Bandung, Indonesia
Tel +628 161866048
Email [email protected]
Introduction: Lycopene has been discussed as a potential effector in the prevention and therapy of prostate cancer. It is red, lipophilic and naturally occurring in many fruits and vegetables, such as tomatoes. Several growth factors, including insulin-like growth factor 1 (IGF-1), play important roles in carcinogenesis and metastasis. IGF-1 is a mitogen that plays important roles in the regulation of proliferation, differentiation, and apoptosis. Binding of IGF-1 to its cognate membrane receptor activates Ras/Raf/MAP kinase signaling pathways, which regulate cell-cycle progression, cell survival, and transformation. Lycopene has its protective effect, which affects multiple IGF-1-activated signaling pathways. Lycopene stimulates apoptosis through intrinsic pathways, by stimulating the pro-apoptotic factor of the mitochondrial cavity such as the Bax/Bak protein (an apoptotic promotor). Although tomatoes are widely consumed in Indonesia, there is no research study about the effect of lycopene on prostate cancer in Indonesia. Hence, this study is conducted to measure the influence of lycopene on the level of IGF-1 in Indonesian human prostate cancer cells.
Materials and Methods: Prostate cancer cells were studied. In this experimental study, cells were taken from patients with Gleason score 6 and divided into 5 groups: 2 control groups and 3 treatment groups, which were given 1 μM, 2 μM and 4 μM of lycopene, respectively. Measurement of mean IGF-1 level was performed by ELISA. A comparative analysis was performed by two-way ANOVA.
Results: The result showed that there was a significant difference in mean IGF-1 levels in the provision of various concentrations of lycopene and time of observation (p< 0.05). Increased level of mean IGF-1 appeared on 2μM dose of lycopene at 48 hours observation and began to decline in 72 hours observation. This happened also on 4μM lycopene at 24 hours observation and began to decline in 48 hours observation (p< 0.05).
Conclusion: Lycopene could be administered as adjuvant therapy for prostate cancer patients to increase apoptosis, and eventually inhibit the progressivity of cancer cells.
Keywords: prostate cancer, lycopene, insulin growth factor-1
Introduction
Prostate cancer is one of the most common urology malignancy in adult men. There were an estimated 782,600 new cases and 254,000 cancer death related to prostate cancer in 2007 globally.1,2 The incidence of this disease continues to rise in various countries. In Indonesia, the incidence of prostate cancer was 4.5–9.8 per 100,000 population in 2002 and had increased to 7.5 – 14 per 100,000 in 2008.3,4 Previously a study was conducted by Safriadi et al at RSUP Hasan Sadikin Bandung showed increasing trend of prostate cancer cases in 2004–2011.5 Until now, the exact cause of prostate cancer is not yet known, however, some reports suggest that there are several risk factors for prostate cancer like genetic and environment. Nutrition also plays an important role in the occurrence of prostate cancer.6 An observational study in Mediterranean communities showed that high consumption of fruits and veges was associated with a low incidence of malignancies.7–9 Tambunan and Umbas reported that nutrients that have protective effects against risk and prostate cancer are tomato/lycopene, soy, cruciferous veges, green tea, and other polyphenolic compounds.10
Tomatoes are widely consumed in Indonesia. Tomato and its products are the main sources of lycopene. Lycopene is a 40-carbon acyclic carotenoid containing 11 conjugated double bonds and belongs to a subgroup of carotenes comprising only hydrogen and carbon atoms.11 Research about the effects of tomatoes on the risk of prostate cancer still continues, however, the results of the study, there are some supporting results and some are not supporting the effects of tomatoes. Several studies that supported include Mills et al in the 1970s whom conducted a 6-year cohort study of 14,000 Seventh-day adventist men and found that men who consumed more than 5 servings of tomatoes and their products each week have a lower risk of prostate cancer than men who eat less than one serving of tomatoes or a product every week.12 In the Health Professional Follow-up Study (HPFS) report of 47,000 health workers in 1995, it was found that among the fruits that could potentially decrease the incidence of prostate cancer were raw tomatoes and strawberries.13 A case–control study in Minnesota found that people who consumed tomatoes more than 14 times per month had a lower risk of prostate cancer than those who ate tomatoes less than 3 times per month.14
Studies regarding lycopene as supplementary therapy for prostate cancer also continuously conducted. Kucuk et al in their studies reported that lycopene administration in prostate cancer patients before radical prostatectomy reduced the surgical incision and extension of extraprostatic tumors and decreased diffuse pattern of High-Grade Prostatic Intraepithelial Neoplasm (HGPIN).15 Ansari and Gupta studied lycopene administration in 20 prostate cancer patients who had been refractory to androgens and revealed that 5% of patients had a complete response of normal Prostate-Specific Antigen (PSA) and no signs of illness for 8 weeks.16 Furthermore, 35% of patients had PSA regression, 50% of patients with stable PSA levels, and only 15% experienced progression.
The effect of lycopene in limiting prostate cancer cell growth in vitro was also reported. Siler et al found that lycopene could increase the rate of necrosis in mice prostate cells, and this phenomenon corresponds to the decrease in local androgen regulatory signals and the expression of IGF-1 and interleukin 6 (IL-6).17 Some of the inhibitory mechanisms of lycopene have been recognized, for instance, antioxidants, cell progression inhibitor, apoptotic induction, and insulin growth factor type 1 (IGF-1) inhibitors.9,14,16,18 It has been known that the increase of IGF-I serum levels correlated with the increasing risk of cancer, including prostate cancer. The excessive expression of IGF-1 on prostatic epithelium correlated with the incidence of prostatic intraepithelial neoplasm (PIN) in transgenic rats. This implied that IGF-1 was not only correlated with the risk of prostate cancer but also engaged in tumorigenesis by inducing cell proliferation and disrupting apoptosis.18–22 The inhibitory effect of IGF-1 by lycopene could be an important key for inhibiting malignancies development in the prostate.
Although tomatoes are widely consumed in Indonesia, there is no research study about the effect of lycopene on prostate cancer in Indonesian people. Therefore, this study is conducted to measure the influence of lycopene on the level of insulin-like growth factor-1 (IGF-I) in Indonesian human prostate cancer cells.
Methods
Cell Culture
Materials of this study were tissue of prostate cancer obtained from prostate cancer patients admitted to Dr Hasan Sadikin General Hospital Bandung, who had undergone radical prostatectomy with Gleason score 6. The tissue obtained from radical prostatectomy then underwent frozen section examination conducted by pathologic anatomic pathology specialist to determine the location of prostate cancer. About 1 gram of specimen was taken from area where shown positive for prostate cancer. It was placed in transport media contained with a solution of Dulbecco’s modification of eagle’s minimal essential medium (DMEM/F12) and antibiotic (penicillin100 U/mL, streptomycin 100 μg/mL, amphotericin B 250 μg/mL and gentamicin 50 μg/mL).20 It was transported on special media at temperature 4°C to Bio Technology (Biotec) Laboratory in Rajawali Hospital, then underwent culture and sub-culture in culture flasks to attain enough number of cells to be researched. The total amount of cells used in each treatment is determined using a hemocytometer.
Lycopene Extraction and Other Reagents
We used lycopene reagents from Sigma Aldrich with code name L9879-Sigma Aldrich. Lycopene is a naturally occurring red pigment, which belongs to the family of carotenoids. It is available on 1, 5, 10 mg in the sealed ampule. We used 1 mg ampule of Lycopene reagents in our study.
Lycopene Treatment on Cell Culture
Prostate cancer tissue culture was divided into 5 groups with 2 control groups (groups A and B) and 3 treated groups (groups C, D, and E). Each group consisted of 500,000 cells in a petri dish. Lycopene extract was dissolved in DMSA into 1 µM, 2 µM, and 4 µM concentrates. Each group was treated with different solutions: Group A was neither treated with lycopene nor DMSA; group B was treated with DMSA alone, and groups C–E was treated with 1 µM, 2 µM, and 4 µM of lycopene, respectively (Figure 1). All groups were incubated at 37°C and in 5% CO2 for 24 hours, 48 hours, and 72 hours.
 |
Figure 1 Grouping of lycopene treatment in human prostate cancer cell culture. |
Measurement of IGF-1 Concentration
Treated cell proteins were isolated by washing them with PBS and adding 50 µL of Complete M-Lysis according to schedule. The cell was shaken for 10 minutes. The lysed cell was transferred to a new tube and kept at −80° C . Briefly, 100 µL of each standard solution and sample was added to the well to then shaken and incubated at 4°C overnight. After overnight incubation, the samples were consecutively incubated with a 1x detection antibody, HRP-Streptavidin, and TMB one-step substrate with washing between each step. The measurement of IGF-1 concentration was conducted at a wavelength of 450 nm. Measurement of IGF-1 protein was performed using the methods listed on the human IGF-1 ELISA kit (Abcam).
Statistical Analysis
Analysis using two-factor analysis of variance (ANOVA) with F-test α =5% using SPSS version 21.0 for Windows was performed.
Ethical Clearance
The study has obtained ethical clearance in accordance with the Declaration of Helsinki from the health research ethics committee from the Faculty of Medicine, Universitas Padjadjaran, Bandung. This study also received written informed consent provided by the patients for prostate tissue use.
Results
The average level of IGF-1 after treatment of prostate cancer cells with lycopene of various concentrations is described in Table 1. Table 1 shows that group treated with 1 µM lycopene (group C) had no difference in average IGF-1 level, compared to control groups (groups A and B) when observed for either 24 hours, 48 hours and 72 hours. Change in average IGF-1 level to 0.760 ng/mL was shown in the group treated with 2 µM lycopene (Group D) when observed for 48 hours, while the IGF-1 level dropped to 0.690 ng/mL when observed for 72 hours. Treatment of the cells using 4 µM of lycopene resulted in an increased average IGF-1 level compared to control groups to 0.785 ng/mL when observed for 24 hours, on the contrary, it dropped to 0.680 ng/mL and 0.515 ng/mL when observed for 48 and 72 hours respectively. Based on Table 2, the average IGF-1 level in various lycopene concentrations demonstrates significant difference (p<0.05). Furthermore, it showed that to average IGF level in various observation times where 48 hours observation time shows a higher average IGF-1 level compared to 24 hours and 72 hours (p<0.05). Change in the average IGF-1 level is shown in Figure 2.
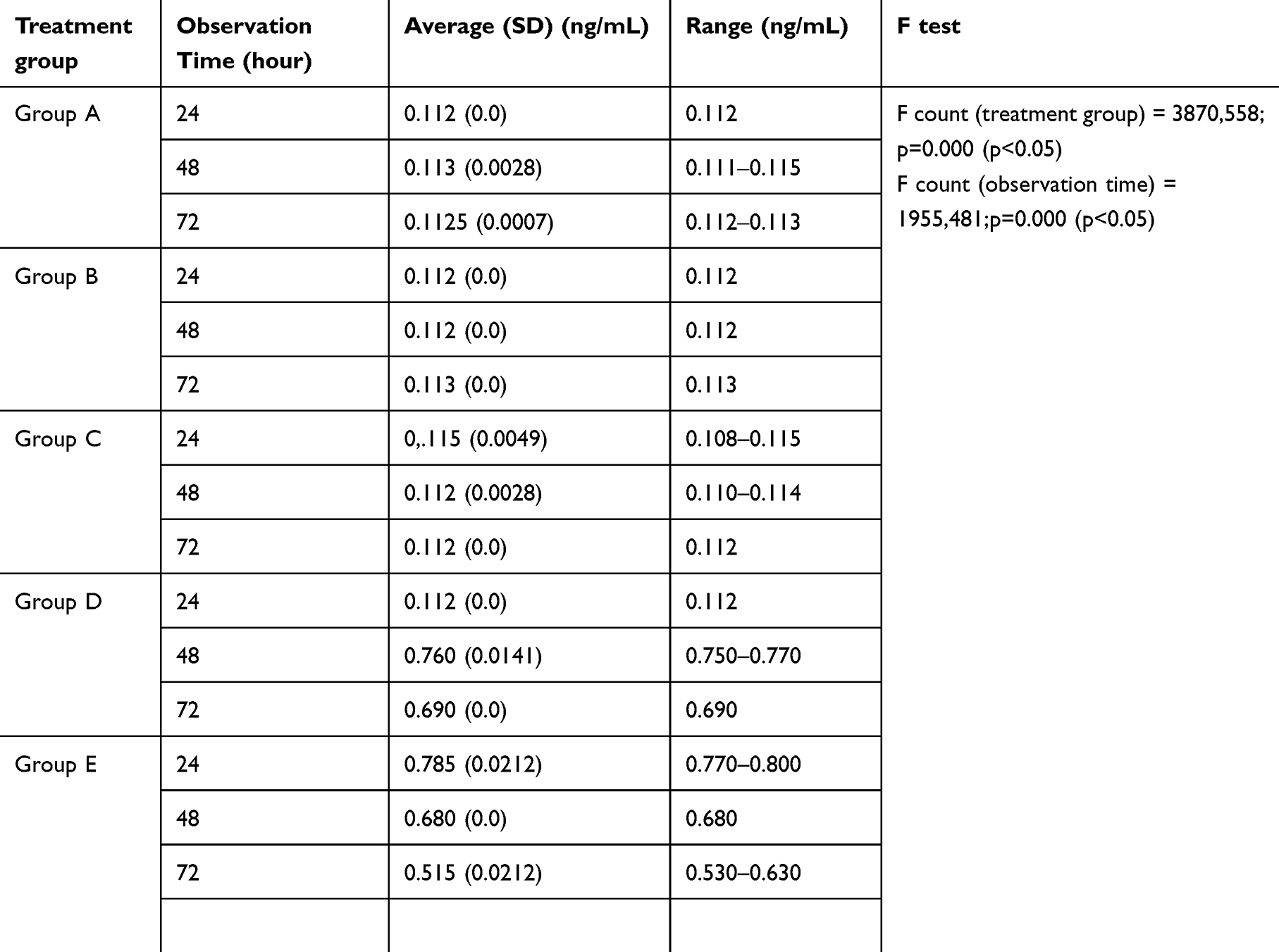 |
Table 1 Average IGF-1 Level Based on Lycopene Concentrations and Observation Time |
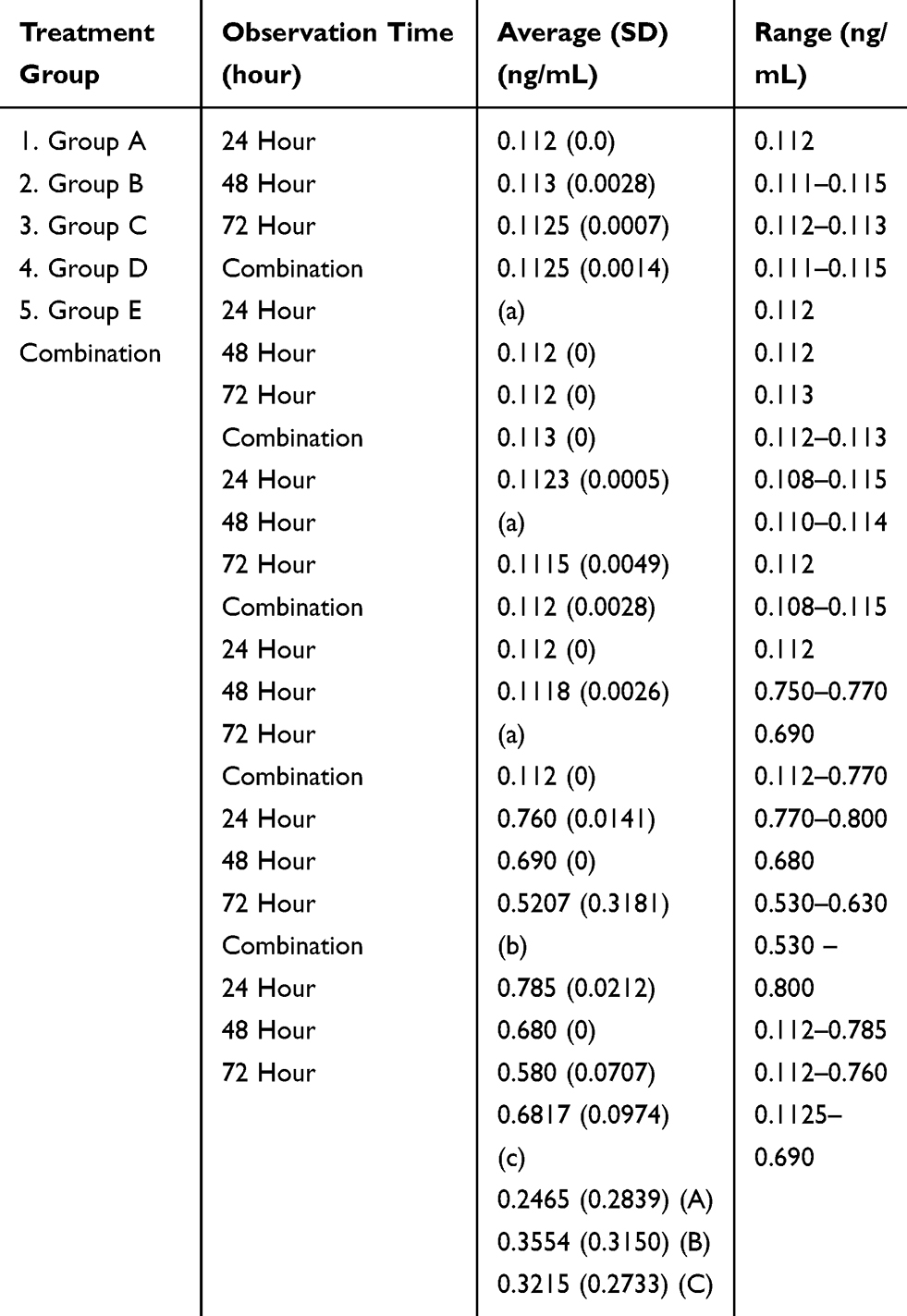 |
Table 2 Difference in Average of IGF-1 Level from Combination Treatment Based on Factorial Scheme Analysis |
 |
Figure 2 Average IGF-1 level on various lycopene concentrations and observation time. |
Discussion
Many studies explain the role of lycopene as an anti-cancer agent for prostate cancer. The inhibitory mechanism of lycopene towards prostate cancer cells occurs through the inhibition of IGF-1 transduction signal via the blocking of IGF-1 expression and IGF-1 receptor. Thus, it leads to cessation of MAPK pathway stimulation and ultimately, the failure of cell proliferation. Many studies regarding the role of lycopene in prostate cancer, either using animal experimentation or even human subjects and cell lines, gives controversial results. It is important to carry out the same research on lycopene and its role on prostate cancer, especially on Indonesian.
This study used prostate cancer cell tissues culture from Indonesian patient that were given lycopene with different dosages and different times of observation. The result showed that 2μM concentration of lycopene could degrade the IGF-1 level with an observation time of 72 hours. Similar results found in the treated group with 4μM concentration of lycopene that observed for 48 hours. From these results, it seems that increasing lycopene concentration will affect the faster IGF-1 level decreases. From Sapuntzakis MS et al, 1μM, 0.5μM, 1μM and 5μM of lycopene can inhibit the LNCaP prostate cancer cell growth significantly.23 The cell cycle progression is also repressed by lycopene as proven by Palozza et al Lycopene at the concentration of 2.5 μM-10μM can reduce the DI cyclin that plays a role in the G0/G1 and reduces the ROS production significantly.24
An interesting issue in our study was how the decrease in IGF-1 rate begins with an increase whether it is given a lycopene concentration of 2 μM or 4 μM as shown in 1. This incidence was not found in previous research. The average increase of the IGF-1 rate in the beginning of this study was thought to occur as an effect of the antioxidant that causes an elimination of reactive oxygen species. Reactive oxygen species is a chemical substance that is reactive to fat, protein and DNA, while also acts as a secondary carrier of cell signals and is needed in various biological processes in a normal cell. In normal physiology, ROS are maintained in homeostasis where production and elimination are balanced and aids cellular processes such as proliferation, differentiation and adaptation towards metabolic and immunologic stress. When there is an imbalance, the biological response towards cancer cells will be different. At a low or medium level, ROS will act as a molecular signal that maintains cancer cell proliferation, differentiation, life sustainability and metastasis till ROS can be considered an oncogenic substance. At this concentration, ROS acts as a trigger for DNA mutation and can stimulate the phosphorylation of mitogen-activated protein kinase (MAPK) and extracellular signal-regulated kinase (ERK), D1 cyclin and JUN N terminal (JNK). High level of ROS might induce cell death and massive cell damage. High ROS level on cancer cell might cause failure in activating P38-MAPK bond which eventually leads to cancer cell death; hence, high ROS level acted as antiproliferation and apoptosis.25,26
This study showed that with prostatic cancer cell death after administration of 2 µM lycopene and 48 hours of observation, there caused leakage of IGF-1 from intracellular to extracellular space; causing IGF-1 level to increase compared to control group. Due to death of some of the cancer cells, there was a decrease in IGF-1 expression and caused gradual decrease in average IGF-1 level. This also occurred with administration of 4 µM lycopene.
The previous study by Liu et al elaborates the mechanism of action of lycopene towards IGF-1 by inhibiting transduction of Dihydrotestosterone (DHT) signaling which might suppress IGF-1 expression.19 DHT forms a complex with beta-catenin and androgen receptor to modulate the expression of several genes, including IGF-1.19 Lycopene also acts in increasing serine phosphorylation effect on Akt and GSK3β, and tyrosine phosphorylation of GSK3, which disturbed growth of cell.19 Kanagaraj et al stated that administration of lycopene might induce production of IGF binding protein-3 (IGFBP-3) which might cause decrease the amount of IGF-1 to bind with IGF-1R. This caused inhibition of proliferation through MAPK pathway and PI3Akt.22 As explained by Wang, lycopene increasing insulin growth factor binding protein (IGFBP) that would bind with IGF-1; thus, IGF-1 unable to bind with its receptor. There was also inhibition of the insulin receptor of the phosphorylation process, expression of cyclin D1, and then blockage the cell cycle.27
Limited observation time to only up to 72 hours became a limitation in this study; therefore, it was assumed that the reduction of IGF-1 level had not yet reached maximum level. Another limitation was that the proliferation of prostate cancer cells through subculture did not achieve an appropriate number of cells to conduct repeated measurement for more than twice. Furthermore, prostatic cancer tissues that fulfilled inclusion criteria were limited; and there was no calculation of the number of prostatic cancer cells (colony) based on concentration and observation time was not after lycopene administration.
It could be concluded from this study that there were differences in IGF-1 levels on Indonesian human prostatic cancer cells by administration of various concentrations of lycopene and observation time. Lycopene could be administered as an adjuvant for advance Gleason 6 stage prostatic cancer patients to increase apoptosis, and eventually, inhibit the progressivity of cancer cells. There should be further research to explore the effect of lycopene in IGF-1 level directly on humans.
Acknowledgment
The abstract of this paper was presented at the 39th Congress of the Societe Internationale d’Urologie as a poster presentation/conference talk with interim findings.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Crawford E. Epidemiology of prostate cancer. Urology. 2003;62(Supplement 6 A):3–11. doi:10.1016/j.urology.2003.10.013
2. American Cancer Society. Global cancer facts & figures. 2nd edition. Atlanta: American Cancer Society;2011.
3. Sim HG. Changing demography of prostate cancer in asia. Eur J Cancer. 2005;41(6):834–845. doi:10.1016/j.ejca.2004.12.033
4. Sugandi S. Referal pattern of urologic malignancy in indonesia. Br J Urol. 1989;63(1):1–3. doi:10.1111/j.1464-410X.1989.tb05111.x
5. Safriadi. Prostatektomi radikal: morbiditas dan mortalitas di rsup dr. Hasan sadikin bandung. Indonesian j Cancer. 2013;7(1):23–28.
6. Abouassaly RTI, Platz EA, Klein EA. Epidemiology, etiology, and prevention of prostate cancer. In: Dalam Wein Aj Kl, Novick AC, Partin AW, Peters CA, eds. Campbell-Walsh Urology.
7. Vecchia L. Mediterranean epidemiological evidence on tomatoes and the prevention of digestive-tract cancers. Proc Soc Exp Biol Med. 1998;218(2):125–128. doi:10.3181/00379727-218-44276
8. Rao AV. Review, role of antioxidant lycopene in cancer and heart disease. J Am Coll Nutr. 2000;19:5,563–569. doi:10.1080/07315724.2000.10718953
9. Basu A, Imrhan V. Tomatoes versus lycopene in oxidative stress and carcinogenesis: conclusions from clinical trials. Eur J Clin Nutr. 2007;61(3):295–303. doi:10.1038/sj.ejcn.1602510
10. Umbas T. Peran fakotr nutrisi pada pencegahan kanker prostat. Indonesian J Cancer. 2014;8(3):135–140.
11. Agarwal S, Rao AV. Tomato lycopene and its role in human health and chronic diseases. CMAJ. 2000;163(6):739–774.
12. Mills PKBW, Phillips RL, Fraser GE,. Cohort study of diet, lifestyle, and prostate cancer in adventist men. Cancer Epidemiol Biomarkers Prev. 1989;64:598–604.
13. Hadley CME, Schwartz SJ, Clinton SK. Tomatoes, lycopene, and prostate cancer: progress and promise. Exp Biol Med. 2002;227(10):869–880. doi:10.1177/153537020222701006
14. E G. A review of epidemiologic studies of tomatoes, lycopene, and prostate cancer. Exp Biol Med. 2002;227(10):852–859. doi:10.1177/153537020222701003
15. Kucuk SF, Sakr W, Djuric Z, et al. Phase II randomized clinical trial of lycopene supplementation before radical prostatectomy. Cancer Epidemiol Biomarkers Prevo. 2001;10:861–868.
16. Ansari MSGN. Lycopene: a novel drug therapy in hormone refractory metastatic prostate cancer. Urol Oncol. 2004;22(5):415–420. doi:10.1016/S1078-1439(04)00122-X
17. Siler UHA, Spitzer V, Seifert N, et al. Lycopene effects on rat normal prostate and prostate tumor tissue. J Nutr. 2005;135:1050S–1052S.
18. Wertz KSU, Regina G. Lycopene: modes of action to promote prostate health. Biochem Biophys. 2004;430(1):127–134. doi:10.1016/j.abb.2004.04.023
19. Liu X, Allen JD, Arnold JT, Blackman MR. Lycopene inhibits IGF-i signal transduction and growth in normal prostate epithelial cells by decreasing DHT-modulated IGF-i production in co-cultured reactive stromal cells. Carcinogenesis. 2008;29(4):816–823. doi:10.1093/carcin/bgn011
20. Grzmil MHB, Thelen P, Schweyer S, Burfeind P. Blockade of the type i IGF receptor expression in human prostate cancer cells inhibits proliferation and invasion, up-regulates IGF binding protein-3, and suppresses MMP-2 expression. J Pathol. 2004;202(1):50–59. doi:10.1002/path.1492
21. Le HAJ, McFann KK, Blackman MR. DHT and testosterone, but not DHEA or E 2, differentially modulate IGF-I, IGFBP-2, and IGFBP-3 in human prostatic stromal cells. Am J Physiol Endocrinol Metab. 2006;290(5):E952–960. doi:10.1152/ajpendo.00451.2005
22. Kanagaraj PVM, Ravisankar B, Anbalagan J, Aruldhas MM, Arunakaran J. Effect of lycopene on insulin-like growth factor-i, IGF binding protein-3 and IGF type-i receptor in prostate cancer cells. J Cancer Res Clin Oncol. 2007;133(6):351–359. doi:10.1007/s00432-006-0177-6
23. Sapuntzakis MS, Bowen PE. Role of lycopene and tomato products in prostate health. Biochim Biophys Acta. 2005;1740(2):202–205. doi:10.1016/j.bbadis.2005.02.004
24. Paola Palozzaa MC, Simonea R, Catalanoa A, Boninsegnaa A, Paola LGM, Ranellettib FO. Lycopene Induces Cell Growth Inhibition by Altering Mevalonate Pathway and Ras Signalling.
25. Gorrini Chiara HI, Mak TW. Modulation of oxidative stress as an anticancer strategy. Nature Rev. 12:931–947.
26. Glasauer A, Chandel NS. Targeting antioxidants for cancer therapy. Biochem Pharmacol. 2014;92(1):90–101. doi:10.1016/j.bcp.2014.07.017
27. Wang XD. Lycopene metabolism and its biological significance. Am J Clin Nutr. 2012;96(5):1214–1222. doi:10.3945/ajcn.111.032359
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.