Back to Journals » Clinical Interventions in Aging » Volume 14
The prevalence of depression and the association between depression and kidney function and health-related quality of life in elderly patients with chronic kidney disease: a multicenter cross-sectional study
Authors Wang WL ![]() , Liang S
, Liang S ![]() , Zhu FL
, Zhu FL ![]() , Liu JQ
, Liu JQ ![]() , Wang SY, Chen XM
, Wang SY, Chen XM ![]() , Cai GY
, Cai GY ![]()
Received 2 February 2019
Accepted for publication 4 April 2019
Published 15 May 2019 Volume 2019:14 Pages 905—913
DOI https://doi.org/10.2147/CIA.S203186
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zhi-Ying Wu
Wen-Ling Wang,1,2 Shuang Liang,1 Fang-Lei Zhu,1 Jie-Qiong Liu,1 Si-Yang Wang,1 Xiang-Mei Chen,1 Guang-Yan Cai1
On behalf of the C-OPTION study group
1Department of Nephrology, Chinese PLA General Hospital, Chinese PLA Institute of Nephrology, State Key Laboratory of Kidney Diseases, National Clinical Research Center for Kidney Diseases, Beijing Key Laboratory of Kidney Disease, Beijing, People’s Republic of China; 2General Internal Medicine Department, the Fifth Medical Center of Chinese PLA General Hospital, Beijing, People’s Republic of China
Purpose: The prevalence of depression and the relationship between depression and kidney function and health-related quality of life (HRQOL) are not well understood in elderly patients with predialysis chronic kidney disease (CKD). This study aimed to evaluate the prevalence of depression and the association between depression and kidney function and HRQOL.
Patients and methods: In this cross-sectional study, 1079 elderly participants with CKD were recruited at 32 clinical centers located within 26 cities throughout 24 provinces in China. Demographic information and laboratory analyses were collected. Symptoms of depression were assessed using the 15-item Geriatric Depression Scale (GDS-15). HRQOL was evaluated using the Kidney Disease Quality of Life-36 (KDQOL-36) instrument.
Results: The prevalence of depression was 23.0%. The estimated glomerular filtration rate (eGFR) was negatively correlated with the GDS score whether it was treated as a categorical variable (r=−0.097, P=0.001) or as a continuous variable (r=−0.100, P=0.001). Marital status, education level, history of CVD and diabetes, CKD stage and proteinuria confirmed to be independent and significant predictors of depression in patients with CKD. Compared with CKD 1–2 patients, we observed an increase of 0.541 and 4.171 in the odds for developing depression in patients CKD 4 (odds ratio [OR] =1.541; P=0.031) and CKD 5 (odds ratio [OR] =5.171; P<0.001), respectively. We observed negative and significant correlations with the GDS score for the following components: PCS (r=−0.370, P<0.001), MCS (r=−0.412, P<0.001), burden of kidney disease (r=−0.403, P<0.001), symptoms and problems of kidney disease (r=−0.360, P<0.001) and effects of kidney disease (r=−0.355, P<0.001). Depression was an independent and significant predictor of all the subcomponents of the HRQOL.
Conclusions: The prevalence of depression in elderly patients with CKD was high and was negatively correlated with kidney function. Depression had a major negative impact on HRQOL.
Keywords: chronic kidney disease, health-related quality of life, depression, aging, kidney function
Introduction
Chronic kidney disease (CKD) is a worldwide public health problem. The prevalence of CKD in the general population is approximately 10–13%.1–3 With increased age, the prevalence of CKD increases significantly. Data from the 2011–2012 National Health and Nutrition Examination Survey (NHANES) showed that the prevalence of CKD was 31.5% for those 65–79 years old, and it was as high as 65.0% in those over 80 years old.4 The prevalence of CKD in people aged 60–69 years and older than 70 years was 18% and 24.2%, respectively, which was much higher than 10.8% in the general population in China.5 Elderly patients with CKD were more likely to suffer mortality than to progress to end-stage renal disease (ESRD) due to complications and comorbidities.6,7 They also had a high prevalence of geriatric syndromes, including depression, cognitive impairment and malnutrition.8–10
Depression is a common and significant psychiatric disorder in ESRD patients. The reported prevalence of depression varies from 23% to 46% in patients with ESRD or in dialysis populations.11–13 Studies have shown the effect of depression on dialysis, mortality, hospitalization and quality of life in these patients.14–16 However, there are relatively few studies about the prevalence of depression in elderly patients with early-stage CKD.17,18 The association between the level of renal function measured by estimated glomerular filtration rate (eGFR) and depression is ambiguous, and the association between depression and its risk factors, especially biological factors such as systemic inflammation, is not known.
Health-related quality of life (HRQOL) is an important outcome and prognostic predictor in patients with CKD. The Kidney Disease Quality of Life-36 (KDQOL-36) instrument, a globally accepted tool, is a simple and important mechanism to evaluate the HRQOL of patients with CKD. The relationship between HRQOL and depression in patients with ESRD is well established.19,20 However, little is known about the association between depression and HRQOL in the early stages of CKD in China.
We conducted a multicenter prospective cohort study of Chinese elderly patients with CKD. The baseline data, including the Geriatric Depression Scale (GDS) score and KDQOL-36, were obtained. In this population study, we aimed to examine the prevalence of depression and its association with kidney function and HRQOL in elderly Chinese CKD patients.
Materials and methods
Study design and participants
This study was a multicenter, cross-sectional, noninterventional study of elderly Chinese patients (above 60 years of age) with CKD and included 32 clinical centers located within 26 cities throughout 24 provinces in China. All of these clinical centers were renal departments from different hospitals. Altogether, 1163 Chinese elderly patients with predialysis CKD were enrolled in the study. Eighty-four patients were excluded because they refused to participate in the survey. Finally, a total of 1079 patients were included between March 2017 and November 2018. CKD was diagnosed as follows: a history of CKD for more than three months; eGFR less than 60 ml/min/1.73 m2 or albumin-to-creatinine ratio (ACR) more than 30 mg/g or proteinuria more than 150 mg/24 h. GFR was estimated with the CKD Epidemiology Collaboration (CKD-EPI) creatinine equation.21 We defined eGFR categories as follows: Stage 1, ≥90 mL/min/1.73 m2; Stage 2, 60–89 mL/min/1.73 m2; Stage 3, 30–59 mL/min/1.73 m2; Stage 4, 15–29 mL/min/1.73 m2, Stage 5, <15 mL/min/1.73 m2, respectively.22
We excluded participants if they (1) were participating in other interventional clinical trials; (2) were receiving dialysis; (3) were diagnosed as having acute kidney injury; (4) had a history of renal or other transplantation; (5) had an active malignancy or metastatic cancer within 24 months prior to screening; (6) had severe heart failure (New York Heart Association function class III or IV); (7) had HIV infection; (8) had isolated hematuria; and (9) were unable to communicate with researchers or unable to complete the study procedure even if assisted and otherwise unable to comply with the study protocol.23
Cardiovascular disease (CVD) history, hypertension and diabetes mellitus were recorded in detail. A history of CVD was defined as myocardial infarction, angina pectoris, cerebrovascular accident, transient ischemic attack, peripheral artery disease or revascularization, diagnosed in the medical history.24 Hypertension was defined as systolic blood pressure (SBP)≥140 mmHg or diastolic blood pressure (DBP)≥90 mmHg on repeated measurements, or both, or as the use of antihypertensive drugs, or both.25 Diabetes was defined as a fasting glucose level ≥7.0 mmol/L, glycated hemoglobin ≥6.5%, or use of antidiabetic drugs.26 This study was conducted in accordance with the Declaration of Helsinki. It was approved by the Ethics Committee of the Chinese PLA General Hospital (No. S2016-100–02), and all patients gave their written informed consent before their inclusion in the study.
Demographic information and laboratory analysis
Information regarding age, sex, marital status, education, annual household income, and history of smoking and alcohol use was collected from patients. Marital status included married and others (single, divorced, widowed). Body mass index (BMI) was obtained within 1 week of blood sample collection from the patients. Blood samples were collected in the morning after an overnight fast. White blood cells, neutrophils, lymphocytes, platelets, hemoglobin, serum albumin, total cholesterol, triglycerides, high-density lipoprotein, low-density lipoprotein, serum calcium and phosphate, serum creatinine, and serum uric acid were collected for each participant. We also collected urinary protein excretion. The neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) were calculated as the ratio of the neutrophils and platelets to lymphocytes, and both were obtained from the same automated blood sample during admission to the study.
Depressive symptoms
Symptoms of depression were assessed using the GDS-15, a reliable and well-validated measure of depressive symptoms in elderly patients in Chinese subjects.27 This self-administered questionnaire contains 15 yes/no questions. Scores range from 0 to 15, with higher scores indicating greater severity. A GDS score of 5 or more was defined as the presence of depressive symptoms,18 which have been shown to have high sensitivity (97%) and specificity (95%) in cases of major depressive disorders from structured diagnostic interviews.27
Health-related quality of life
HRQOL was assessed using the KDQOL-36 instrument, which was introduced in 1994 and is specific to kidney disease.28 The Chinese version of the KDQOL-36 has been validated.29 The KDQOL-36 has 36 items: the 12-item Short-Form Health Survey (SF-12) and another 24 kidney disease-specific targeted domains. The kidney disease-specific targeted domains comprise three scales: burden of kidney disease (4 items), symptoms and problems of kidney disease (12 items), and effects of kidney disease (8 items). Since our study participants were not on dialysis, one question related to dialysis was omitted from the KDQOL-36. The SF-12 measured eight dimensions of health-related functioning [physical functioning (PF), role-physical (RP), bodily pain (BP), general health (GH), vitality (VT), social functioning (SF), role-emotional (RE) and mental health (MH)]. Responses were scored (0–100), and a higher score reflected a better HRQOL.30 The SF-12 scores were aggregated into a physical component summary (PCS) and a mental component summary (MCS) .31
Statistical analysis
The variables were expressed as the mean ± SD, median (interquartile range, IQR) or percentage, as appropriate. Groups were compared by independent t-test, the Mann-Whitney U test or χ2 analysis, as appropriate. As many values were not normally distributed, Spearman’s rank correlation (Rho) was used to determine correlations. The individual impact of several confounding factors on the variance of a continuous variable was assessed by building multivariate regression models, and if the dependent variable was dichotomous, the assessment was conducted by building multivariate logistic regressions. The predictors were accepted according to a forward stepwise algorithm (inclusion criteria: P<0.05, exclusion criteria: P>0.10). Analyses were performed with IBM SPSS 25.0 software (SPSS Institute, IBM, USA). All P-values were two-sided. Statistical significance was set at the level of P<0.05.
Results
Patient characteristics
A total of 1163 participants were recruited. There was an overall response rate of 93% (1079/1163), with 84 nonresponders removed from the analyses (Table 1). The mean age of the patients who responded to the questionnaire was 68.8±6.6 years and included more men (62.7%). Nonresponders were significantly older (74.6±8.5 years, P<0.001) and had a lower eGFR (45.13±23.70 mL/min/1.73 m2) than responders (54.90±32.22 mL/min/1.73 m2). Nonresponders were more likely to suffer from diabetes than were responders. There were no significant differences in hypertension and CVD between the two groups.
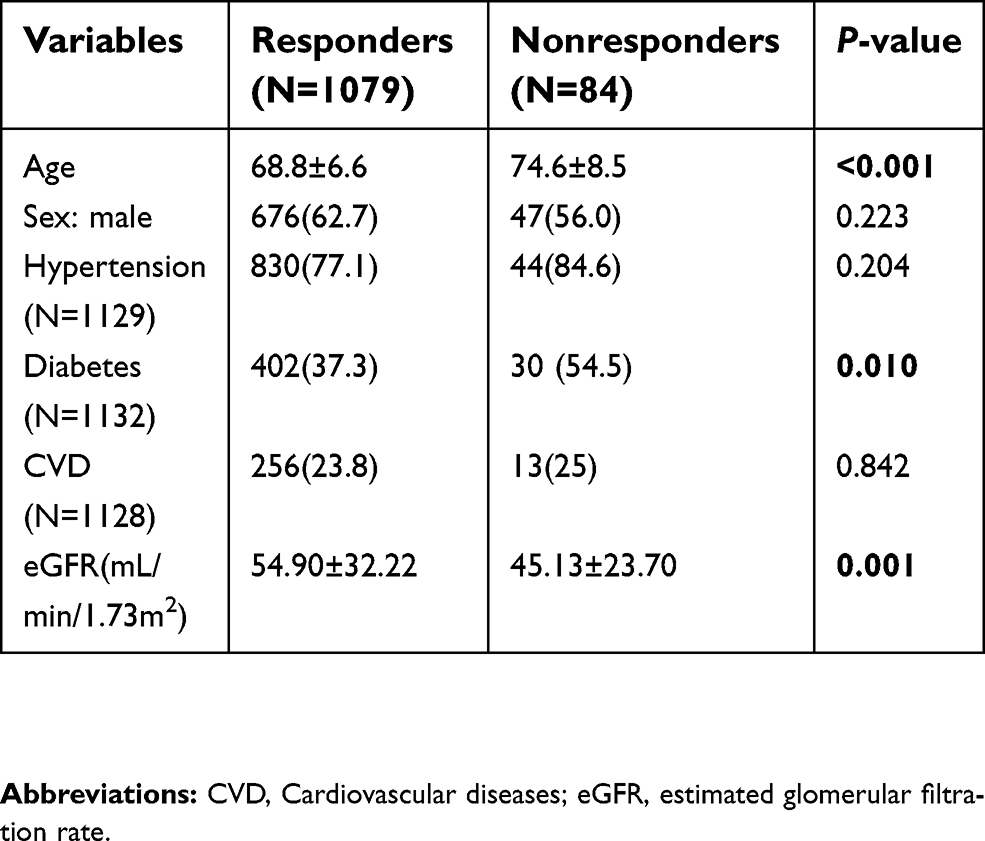 | Table 1 Characteristics of responders and nonresponders |
Characteristics of the 1079 participants are shown in Table 2. The prevalence of CKD complications and comorbidities was as follows: 77.1% had hypertension, 37.3% had diabetes, and 23.7% had cardiovascular diseases. The prevalence of depressive symptoms was 23.0% (N=248). Compared with nondepressed patients, depressed patients were more likely to be single, divorced or widowed and to have lower education levels, higher rates of CVD, higher phosphate levels and proteinuria, and lower GFR and hemoglobin. However, patients who had diabetes seemed to have a lower rate of depression than nondiabetic patients. There were no significant differences between depressed and nondepressed patients in the other characteristics.
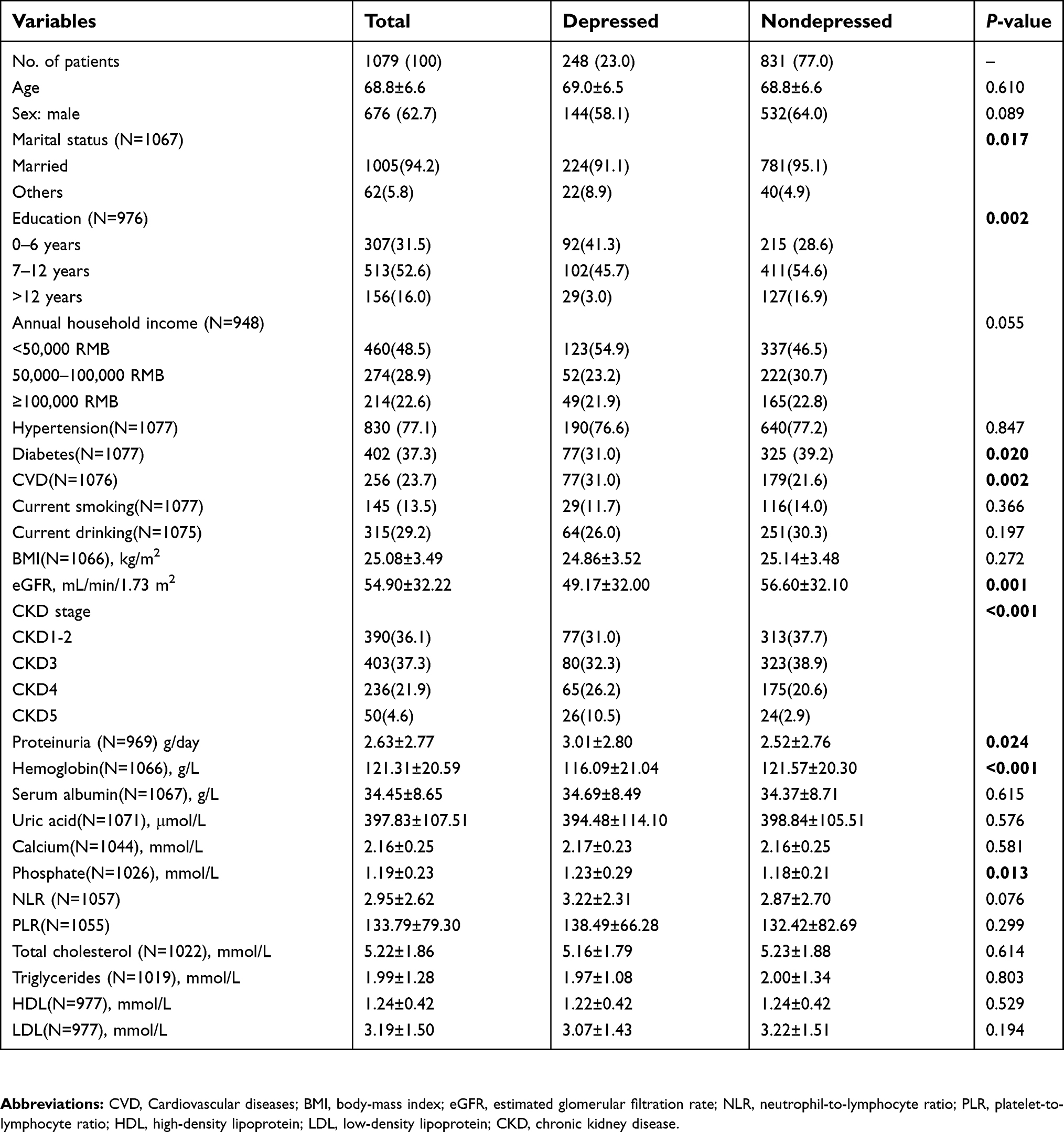 | Table 2 Characteristics of CKD patients by depressive symptoms |
Association between depressive symptoms and kidney function
The association between depressive symptoms and kidney function is presented in Figure 1. The eGFR was negatively correlated with the GDS score whether it was treated as a categorical variable (r=−0.097, P=0.001) or as a continuous variable (r=−0.100, P=0.001).
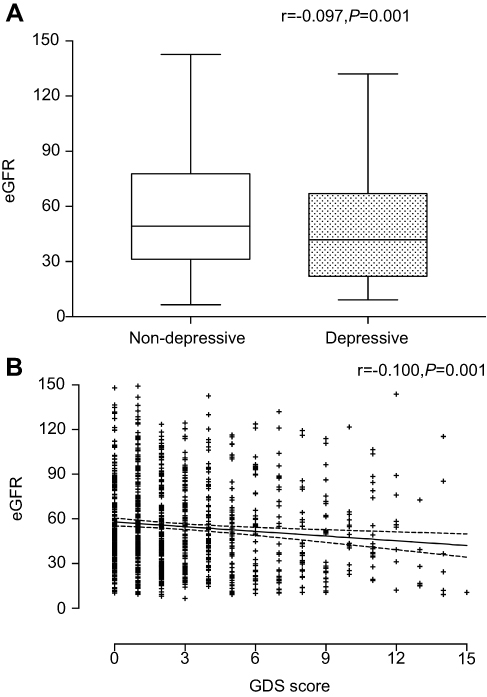 | Figure 1 Association between depressive symptoms and eGFR.Abbreviations: eGFR, estimated glomerular filtration rate; GDS, Geriatric Depression Scale. |
Correlates of depressive symptoms in patients with CKD
We created a multivariate logistic regression model with the presence of depression as an outcome and with the following as predictors: age, sex, marital status, education, diabetes, CVD, CKD stage, and proteinuria, hemoglobin and phosphate levels. The final regression equation was validated according to a forward stepwise algorithm, having an inclusion threshold criterion for predictors of a P-value for goodness of fit lower than or equal to 0.05 and an exclusion threshold of a P-value higher than 0.10. In the final regression equation, the following predictors were accepted: marital status, education, diabetes, CVD, CKD stage and proteinuria.
According to our model, the incidence of depression was significantly associated with single, divorced or widowed status; lower education level; presence of CVD; absence of diabetes; CKD Stages 4 and 5; and increased proteinuria. The impact of significant predictors on the development of depression is presented in Table 3. Compared with CKD 1–2 patients, we observed an increase of 0.541 and 4.171 in the odds of developing depression in patients with CKD 4 (odds ratio [OR] =1.541; P=0.031) and CKD 5 (odds ratio [OR] =5.171; P<0.001), respectively.
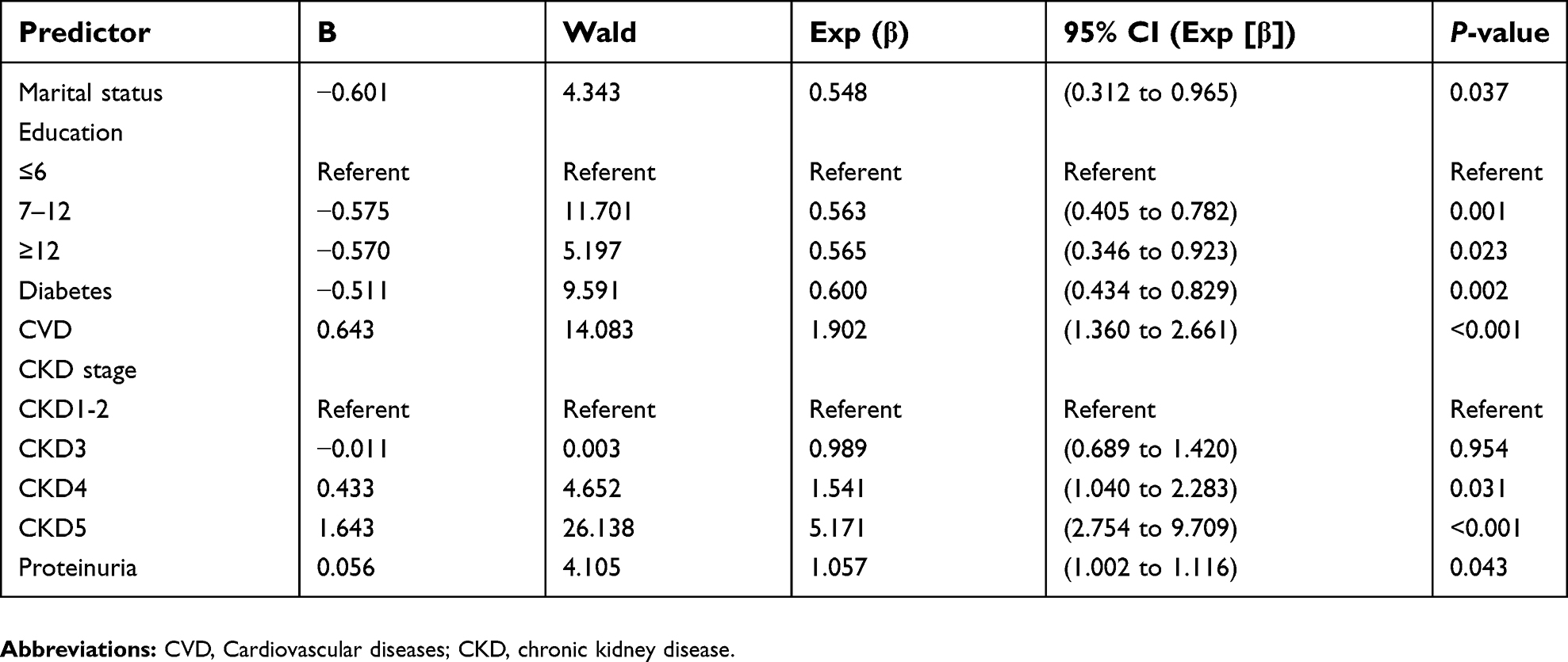 | Table 3 Multiple logistic regression analysis parameters (dependent variable - depression) |
Depressive symptoms influence the HRQOL
Results of the eight generic domains and summary scores and the scores for kidney disease-specific health concerns are displayed in Table 4. Patients in the depressed group were significantly more likely to have low scores for GH, PF, BP, RE, MH, VT, SF, PCS, MCS, burden of kidney disease, symptoms and problems of kidney disease and effects of kidney disease and high scores for RP. Since PCS and MCS were summary scores, individual components were not further analyzed separately.
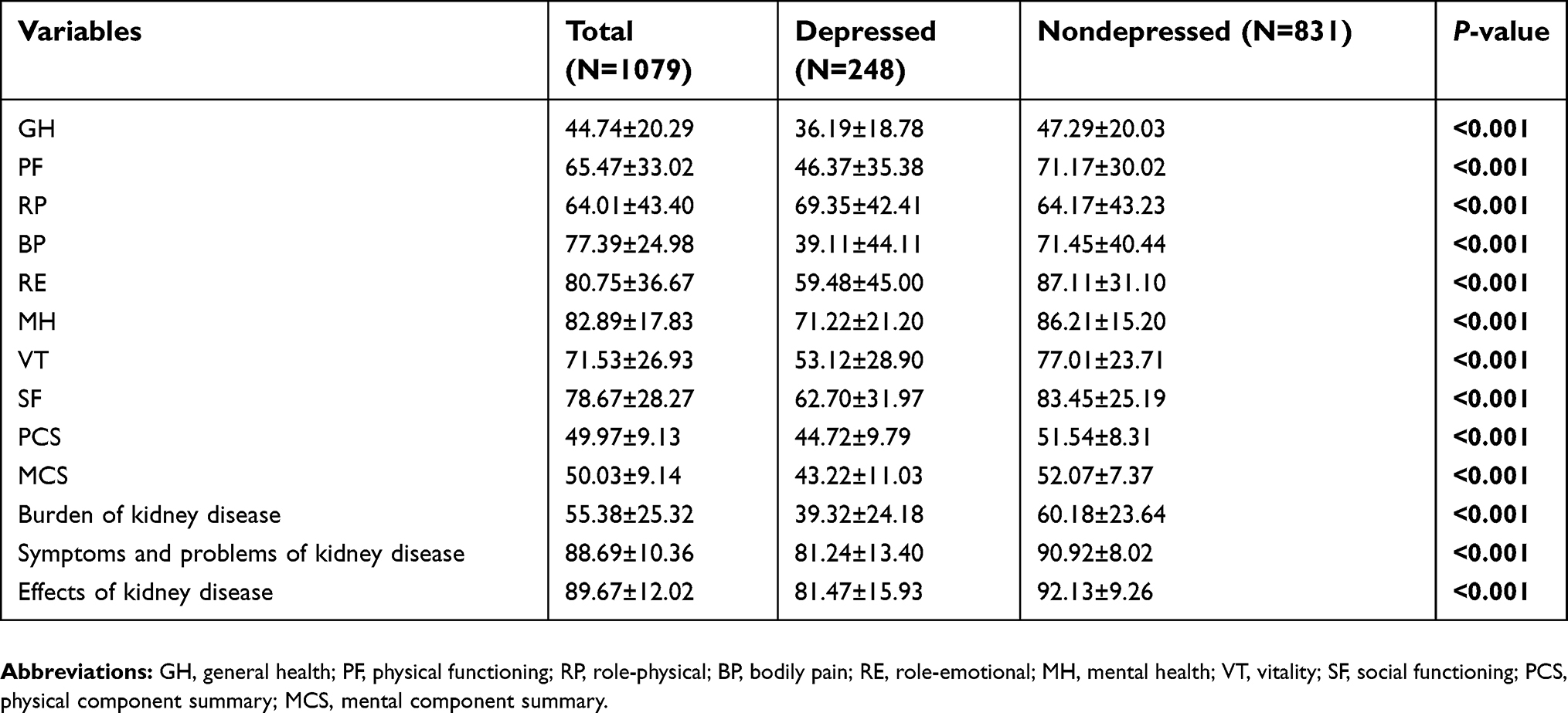 | Table 4 HRQOL components of CKD patients by depressive symptoms |
Regarding the subcomponents of the HRQOL, we observed that PCS (r=−0.370, P<0.001), MCS (r=−0.412, P<0.001), burden of kidney disease (r=−0.403, P<0.001), symptoms and problems of kidney disease (r=−0.360, P<0.001) and effects of kidney disease (r=−0.355, P<0.001) had negative and significant correlations with the GDS score. After adjusting for factors such as age, sex, BMI, diabetes, CVD, proteinuria and eGFR, which may possibly impact HRQOL, the relationship between depression and the subcomponents of the HRQOL also existed (Table 5).
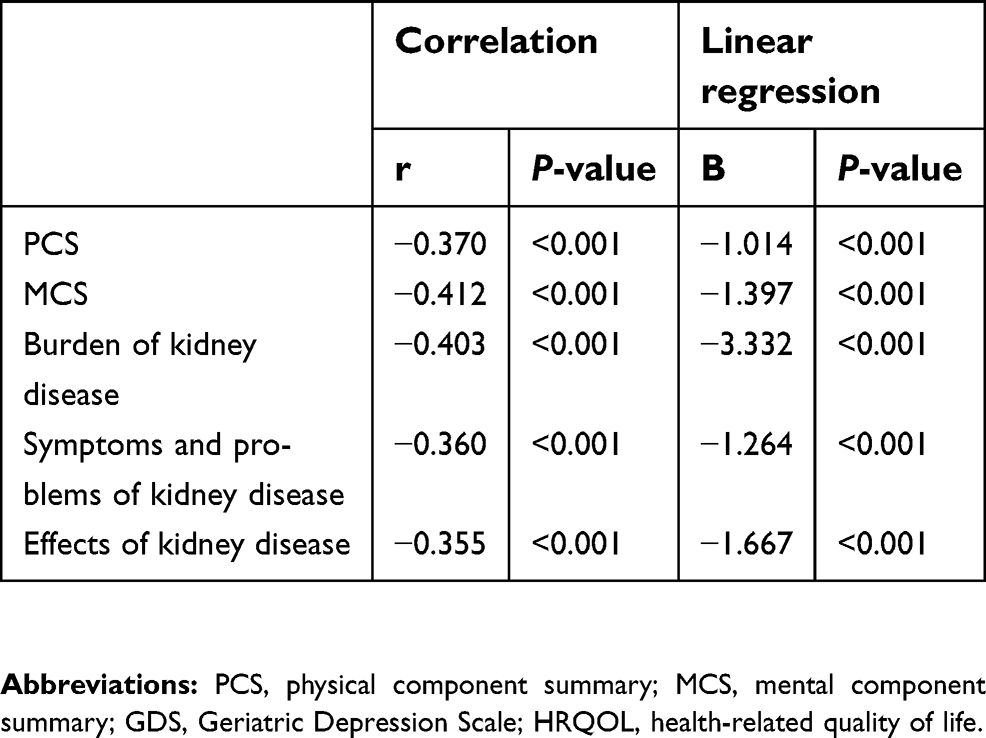 | Table 5 Correlation and linear regression between GDS score and HRQOL subscales |
Discussion
Depression is a very common but complex problem among individuals with CKD. In this multicenter cross-sectional elderly CKD data set, the prevalence of depression was 23.0%. By comparison, the prevalence of depression was reported to be approximately 1.1–3.3% in the general population, 12–18% in patients with diabetes and 15–23% in patients with coronary heart disease.32,33 The prevalence of depression in our study was similar to that reported by a meta-analysis. In that study, the prevalence rate was 26.5% in patients with Stages 1–5 CKD.11 However, the rate was relatively higher than that reported in a previous study (12.8%), which may be because the patients were all community-dwelling adults.18 Another study also reported that the prevalence of depression among elderly medical inpatients (18.1%) was significantly higher than that among community-dwelling elderly people (11.6%).34 The prevalence of depression was high in CKD patients. The presence of depression may have a serious negative impact on the global health and well-being of the patients. They may exhibit poor adherence behaviors, have a poor response to treatment and require much social support.
There was a significant difference in kidney function between patients with depressive symptoms and nondepressive symptoms in our study. Patients with CKD Stages 4 and 5 had a high risk of depression. In 2018, Liu et al demonstrated that the estimated glomerular filtration rate was associated with depressive symptoms. In their study, patients with CKD Stages 1–3 were included. Depressive symptoms were defined as GDS score ≥6, and eGFR was calculated by the Cockcroft-Gault (CG) equation.35 However, in 2009, Hedayati et al concluded that depression did not vary significantly among patients with different CKD stages.36 The evidence for an association between the level of renal function measured by eGFR and depression was indefinite. Since cross-sectional studies cannot explain the causal relationship, longitudinal studies are needed to verify the relationship between depression and eGFR.
Low eGFR and proteinuria are signs of severe renal impairment that could require dialysis or kidney transplantation. These patients were more susceptible to experiencing psychological diseases. In 2012, Liborio et al reported that proteinuria was associated with depression in primary glomerulopathy patients with preserved renal function.37 In our study, we also concluded that proteinuria was associated with depression in elderly CKD patients.
The association between being unmarried, having a low educational level and having CVD and the occurrence of depressive symptoms in CKD patients has been shown in our study. However, the association with age and sex was not revealed. Variations in participants’ demographic characteristics and the type of study design might be the reasons for the discrepancy. In our study, we found that patients with diabetes seemed to have a low rate of depression, which was not consistent with a previous study.38 This might be because some patients with diabetes were excluded due to a lack of response to the survey or to a refusal to participate in our study.
HRQOL is an important outcome in CKD. We observed that PCS, MCS, burden of kidney disease, symptoms and problems of kidney disease and effects of kidney disease had negative and significant correlations with the GDS score. Longitudinal data from hemodialysis patients demonstrated that depression was related to a reduction of 1.09 and 4.52 points in HRQOL, as evaluated by PCS and MCS, respectively.39 Previous studies have not reported a relationship between depression and the kidney disease-specific targeted domains. In our study, depression was independently related to HRQOL following multiple regression analyses. The presence of depression may influence the patient’s attention and interest in the management of the disease, leading to a deterioration of kidney function and HRQOL. Thus, early identification of depression and active interventions should be considered to reduce the burden of kidney disease and to relieve the symptoms and problems related to kidney disease.
There were also several limitations to this study. First, the analysis used a cross-sectional design, and therefore, longitudinal relationships between the factors and depression could not be established. Second, the patients who did not agree to participate or were excluded were actually older, had lower GFRs and had diabetes, which would induce possible biases that might affect the results. Third, there was no drug information in the study: we did not account for the effects of medication on the prevalence of depression and on the relationships between depression and HRQOL.
While the study primarily explained the correlation between depression and HRQOL in a multicenter study in elderly Chinese CKD patients, more information will be reported after acquiring the follow-up data. Some treatments, including psychosocial interventions and aerobic exercise, were found to be effective in relieving depression.40,41 The early identification of depression and active interventions should be considered to improve overall well-being and the HRQOL of these patients. Clinical trials evaluating whether treatment interventions benefit HRQOL in CKD patients with depression are warranted.
Conclusion
The prevalence of depression in elderly CKD patients is high and correlates with kidney function and all aspects of HRQOL. The integration of depression and HRQOL assessment into routine clinical practice may be important and clinically beneficial for elderly Chinese CKD patients.
Acknowledgments
The authors thank all the patients and collaborators of the C-OPTION study group. This work was funded by the National Key Technology R&D Program (2015BAI12B06).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Coresh J, Astor BC, Greene T, Eknoyan G, Levey AS. Prevalence of chronic kidney disease and decreased kidney function in the adult US population: third National Health and Nutrition Examination Survey. Am J Kidney Dis. 2003;41(1):1–12. doi:10.1053/ajkd.2003.50007
2. Hallan SI, Coresh J, Astor BC, et al. International comparison of the relationship of chronic kidney disease prevalence and ESRD risk. J Am Soc Nephrol. 2006;17(8):2275–2284. doi:10.1681/ASN.2005121273
3. Chadban SJ, Briganti EM, Kerr PG, et al. Prevalence of kidney damage in Australian adults: the AusDiab kidney study. J Am Soc Nephrol. 2003;14(7 Suppl 2):S131–138.
4. Murphy D, McCulloch CE, Lin F, et al. Trends in prevalence of chronic kidney disease in the United States. Ann Intern Med. 2016;165(7):473–481. doi:10.7326/M16-0273
5. Zhang L, Wang F, Wang L, et al. Prevalence of chronic kidney disease in China: a cross-sectional survey. Lancet. 2012;379(9818):815–822. doi:10.1016/S0140-6736(12)60033-6
6. Fassett RG. Current and emerging treatment options for the elderly patient with chronic kidney disease. Clin Interv Aging. 2014;9:191–199. doi:10.2147/CIA.S39763
7. Maw TT, Fried L. Chronic kidney disease in the elderly. Clin Geriatr Med. 2013;29(3):611–624. doi:10.1016/j.cger.2013.05.003
8. Bautovich A, Katz I, Smith M, Loo CK, Harvey SB. Depression and chronic kidney disease: A review for clinicians. Aust N Z J Psychiatry. 2014;48(6):530–541. doi:10.1177/0004867414528589
9. Wang H, Fang C, Cai L, Dong B, Deng J. Chronic kidney disease and cognitive impairment among the very old in China. Aging Clin Exp Res. 2016;28(3):475–482. doi:10.1007/s40520-015-0433-1
10. Windahl K, Faxen Irving G, Almquist T, et al. Prevalence and risk of protein-energy wasting assessed by subjective global assessment in older adults with advanced chronic kidney disease: results from the EQUAL study. J Ren Nutr. 2018;28(3):165–174. doi:10.1053/j.jrn.2017.11.002
11. Palmer S, Vecchio M, Craig JC, et al. Prevalence of depression in chronic kidney disease: systematic review and meta-analysis of observational studies. Kidney Int. 2013;84(1):179–191. doi:10.1038/ki.2013.77
12. Teles F, Azevedo VF, Miranda CT, et al. Depression in hemodialysis patients: the role of dialysis shift. Clinics (Sao Paulo). 2014;69(3):198–202. doi:10.6061/clinics/2014(03)10
13. Cirillo L, Cutruzzula R, Somma C, et al. Depressive symptoms in dialysis: prevalence and relationship with uremia-related biochemical parameters. Blood Purif. 2018;46(4):286–291. doi:10.1159/000491014
14. Lacson E
15. Lacson E
16. Bujang MA, Musa R, Liu WJ, Chew TF, Lim CTS, Morad Z. Depression, anxiety and stress among patients with dialysis and the association with quality of life. Asian J Psychiatr. 2015;18:49–52. doi:10.1016/j.ajp.2015.10.004
17. Kim JW, Moon SJ, Kim HJ, Lee DG. Relationship between chronic kidney disease and depression in elderly Koreans using the 2013 Korea National Health and Nutrition Examination Survey data. Korean J Fam Med. 2017;38(3):156–162. doi:10.4082/kjfm.2017.38.3.156
18. Feng L, Yap KB, Ng TP. Depressive symptoms in older adults with chronic kidney disease: mortality, quality of life outcomes, and correlates. Am J Geriatr Psychiatry. 2013;21(6):570–579. doi:10.1016/j.jagp.2012.12.020
19. Jung HY, Jang HM, Kim YW, et al. Depressive symptoms, patient satisfaction, and quality of life over time in automated and continuous ambulatory peritoneal dialysis patients: a prospective multicenter propensity-matched study. Medicine (Baltimore). 2016;95(21):e3795. doi:10.1097/MD.0000000000004864
20. Debnath S, O‘Connor J, Hura C, Kasinath B, Lorenzo C. Quality of life and depression among mexican americans on hemodialysis: a preliminary report. Ther Apher Dial. 2018;22(2):166–170. doi:10.1111/1744-9987.12642
21. Levey AS, Stevens LA, Schmid CH, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150(9):604–612.
22.
23. Liang S, Wang WL, Zhu FL, et al. Chinese observational prospective study of ageing population with chronic kidney disease (C-OPTION): a study protocol. BMJ Open. 2018;8(2):e019457. doi:10.1136/bmjopen-2017-019457
24. Jie KE, Zaikova MA, Bergevoet MW, et al. Progenitor cells and vascular function are impaired in patients with chronic kidney disease. Nephrol Dial Transplant. 2010;25(6):1875–1882. doi:10.1093/ndt/gfp749
25. James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311(5):507–520. doi:10.1001/jama.2013.284427
26. Ene-Iordache B, Perico N, Bikbov B, et al. Chronic kidney disease and cardiovascular risk in six regions of the world (ISN-KDDC): a cross-sectional study. Lancet Globl Health. 2016;4(5):e307–e319. doi:10.1016/S2214-109X(16)00071-1
27. Nyunt MS, Fones C, Niti M, Ng T-P. Criterion-based validity and reliability of the Geriatric Depression Screening Scale (GDS-15) in a large validation sample of community-living Asian older adults. Aging Ment Health. 2009;13(3):376–382. doi:10.1080/13607860902861027
28. Hays RD, Kallich JD, Mapes DL, Coons SJ, Carter WB. Development of the Kidney Disease Quality of Life (KDQOL™) instrument. Qual Life Res. 1994;3:329–338.
29. Tao X, Chow SK, Wong FK. Determining the validity and reliability of the Chinese version of the Kidney Disease Quality of Life Questionnaire (KDQOL-36). BMC Nephrol. 2014;15:115. doi:10.1186/1471-2369-15-115
30. Hays RD, Kallich JD, Mapes DL, et al. Kidney Disease Quality of Life Short Form (KDQOL-SFTM), version 1.3: a manual for use and scoring. Available from:
31. C L L, E Y T, Gandek B, Fong DYT. The SF-36 summary scales were valid, reliable, and equivalent in a Chinese population. J Clin Epidemiol. 2005;58(8):815–822. doi:10.1016/j.jclinepi.2004.12.008
32. Gu L, Xie J, Long J, et al. Epidemiology of major depressive disorder in mainland china: a systematic review. PLoS One. 2013;8(6):e65356. doi:10.1371/journal.pone.0065356
33. Katon WJ. Epidemiology and treatment of depression in patients with chronic medical illness. Dialogues Clin Neurosci. 2011;13(1):7–23.
34. Li N, Chen G, Zeng P, et al. Prevalence of depression and its associated factors among Chinese elderly people: A comparison study between community-based population and hospitalized population. Psychiatry Res. 2016;243:87–91. doi:10.1016/j.psychres.2016.05.030
35. Liu Q, Y X L, Hu ZH, Jiang X-Y, Li S-J, Wang X-F. Reduced estimated glomerular filtration rate is associated with depressive symptoms in elder Chinese: A population-based cross-sectional study. Neurosci Lett. 2018;666:127–132. doi:10.1016/j.neulet.2017.12.029
36. Hedayati SS, Minhajuddin AT, Toto RD, Morris DW, Rush AJ. Prevalence of major depressive episode in CKD. Am J Kidney Dis. 2009;54(3):424–432. doi:10.1053/j.ajkd.2009.03.017
37. Liborio AB, Santos JP, Minete NF, et al. Proteinuria is associated with quality of life and depression in adults with primary glomerulopathy and preserved renal function. PLoS One. 2012;7(5):e37763. doi:10.1371/journal.pone.0037763
38. Ahlawat R, Tiwari P, D‘Cruz S. Prevalence of depression and its associated factors among patients of chronic kidney disease in a public tertiary care hospital in India: a cross-sectional study. Saudi J Kidney Dis Transpl. 2018;29(5):1165–1173. doi:10.4103/1319-2442.243972
39. Belayev LY, Mor MK, Sevick MA, et al. Longitudinal associations of depressive symptoms and pain with quality of life in patients receiving chronic hemodialysis. Hemodial Int. 2015;19(2):216–224. doi:10.1111/hdi.12247
40. Lopes AA, Lantz B, Morgenstern H, et al. Associations of self-reported physical activity types and levels with quality of life, depression symptoms, and mortality in hemodialysis patients: the DOPPS. Clin J Am Soc Nephrol. 2014;9(10):1702–1712. doi:10.2215/CJN.12371213
41. Cukor D, Ver Halen N, Asher DR, et al. Psychosocial intervention improves depression, quality of life, and fluid adherence in hemodialysis. J Am Soc Nephrol. 2014;25(1):196–206. doi:10.1681/ASN.2012111134
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.