Back to Journals » Clinical Optometry » Volume 13
The Prevalence and Determinant Factors of Self-Reported Depressive Symptoms Among Elderly People with Visual Impairment Attending an Outpatient Clinic in Ethiopia
Authors Yimer YM, Buli MB, Nenko G, Mirkena Y ![]() , Kassew T
, Kassew T ![]()
Received 28 November 2020
Accepted for publication 27 January 2021
Published 17 February 2021 Volume 2021:13 Pages 63—72
DOI https://doi.org/10.2147/OPTO.S294618
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Mr Simon Berry
Yassin Mohammed Yimer,1 Mengistu Bekele Buli,2 Goshu Nenko,3 Yohannes Mirkena,3 Tilahun Kassew3
1Mental Health Unit, Eka Kotebie Referral Hospital, Addis Ababa, Ethiopia; 2Mental Health Unit, Amanuel Mental Specialized Hospital, Addis Ababa, Ethiopia; 3Department of Psychiatry, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Correspondence: Tilahun Kassew
Department of Psychiatry, College of Medicine and Health Sciences, University of Gondar, P.O. Box: 196, Gondar, Ethiopia
Tel +251918410710
Email [email protected]
Background: Depression among older adults with visual impairment is the commonest psychiatric problem and causes a range of effects in on disability and progression of visual health outcomes that may even end in death. In Ethiopia, there are gaps in the detection of the comorbidity of mental health problems especially depressive symptoms among those older people. This study aimed to assess the prevalence of self-reported depressive symptoms and determinant factors among the elderly people with visual impairment attending the ophthalmologic outpatient clinic.
Methods: A group of 423 elderly people with visual impairment invited by systematic random sampling technique to took part in the interview for this cross-sectional study at Menelik II referral hospital, Addis Ababa, Ethiopia from January to June 2019. Descriptive statistics like frequency, percentage, mean and standard deviation were used to summarize the distribution of the data. Binary logistic regression analysis was employed to examine the associated factors. An adjusted odds ratio with a 95% confidence interval was used for reporting the result, and a p-value of < 0.05 was considered as statistically significant.
Results: The prevalence of self-reported depressive symptoms among elderly people with visual impairment was 26.7% with a 95% confidence interval (22.6– 30.8). Widowhood, single and/divorced [Adjusted Odds Ratio (AOR)= 3.17, 95% CI: 1.71, 5.91]; [AOR=2.70, 95% CI: 1.35, 5.38], respectively, poor social support [AOR=4.34, 95% CI: 1.84, 10.24], severe level [AOR=2.63, 95% CI: 1.73, 6.63] and longer duration (> 5 years) of the illness [AOR=3.15, 95% CI: 1.60, 6.19] were the factors significantly associated with higher odds of depressive symptoms.
Conclusion: The Prevalence of self-reported depressive symptoms among elderly people with visual impairment in Ethiopia was high. Public health interventions targeting risky individuals with high depressive symptoms are needed to reduce depressive symptoms and to prevent disability and poor medical illnesses outcomes related to depressive symptoms.
Keywords: depressive symptoms, depression, elderly, visual impairment, Ethiopia
Introduction
According to the World Health Organization (WHO), visual impairment defined as a decreased ability to see with the visual acuity worse than 20/70 (moderate and severe low vision) but equal to or better than 20/400 (legal blindness) in the better eye, even with corrective lenses.1 Visual impairment is one of the major public health problems worldwide, especially in developing countries where 90% of the blind live. It particularly affects the older population, and one of the most feared forms of medical disability.2–4 Studies indicate that Ethiopia is one of the world’s highest rates of blindness populations especially in the elderly.5,6
By the year 2020 depression was expected to be the major cause of disease burden for older populations.7 As a result, the burden on both eye care and mental health care for people with a visual impairment (VI) is expected to increase. Elderly people with VI are more likely to suffer from mental illness particularly depression.8,9 The WHO currently ranks it as the third most prevalent disabling condition globally.10 Depression is the most common psychiatric disorder and carries a high burden in terms of treatment costs, the effect on families and careers, as well as a loss of workplace productivity.11,12 Depressive symptoms were high among visually disabled individuals especially in advanced age due to restricted activities of daily living, reading and social activities, and presence of psychosocial stressors like loss of their loved one, retirement and loneliness.13,14
A depressive disorder is frequently found as comorbid among patients with visually impaired and most of the time it is underdiagnosed.15 There is a high rate of self-reported depressive symptoms in advanced age people with low vision. Up to 3% of the elderly persons suffer from major depression, 8%-16% of the elderly have clinically significant depressive symptoms.16,17 The presence of depressive symptoms among visually impaired elderly results in negative impacts, such as taking poor care for their eyes, poor adherence to treatment, and worsening the progression of vision loss and a further reduction in social participation.3,18 As a result, the association between visual function and depression could be further complicated because depressive symptoms might adversely affect a person’s self-reported visual function.19,20
Depressive symptoms in the elderly with VI are affected by the types/levels of illness. Low/mild levels of VI can relief from depressive symptoms compared to a severe level of VI. Globally, the estimated prevalence of depressive symptoms among elderly people with eye/ocular diseases ranged from 5.4%-57.0% with a pooled prevalence of 25%.21–23 Regarding the type of disease categories, the highest prevalence of depression was 29% revealed from dry eye disease (DED), followed by 25% among patients with glaucoma, 24% for age-related macular degeneration (AMD) and 23% for cataract.12,24 Moreover, a recent review reported that a person with eye disease was 1.6 times more likely to suffer from depression compared to healthy control.23 Those cases are most likely happening due to the inability to recognize mental health problems results from comorbid disorders.
Researchers reported that socio-demographic factors such as advanced age, female sex, widowed/divorced, lower educational status, rural residence, and low social support were the predictors of self-reported depressive symptoms among elderly people with VI.25,26 Clinical factors including longer duration of illness, moderate and severe level of the VI, experiencing mental illness, and comorbid medical illness are also the correlates for depressive symptoms.27–30 Moreover, the use of substances such as alcohol, Khat and smoking cigarette/tobacco products are the other predictors’ for depressive symptoms.29,31,32 These factors are the important contributors to increase the likelihood of self-reported depressive symptoms among those population group in low- and middle-income countries. So, this study did look into the predictors associated with self-reported depressive symptoms in those groups.
Despite the high prevalence and impact of depressive symptoms among elderly people with VI, it is often under-recognized and unmanaged, and its predictors also not yet well studied. Therefore, information about the depressive symptoms and its association in the elderly with VI is important for designing and implementing strategies to reduce depression. In Ethiopia, depression is studied in different chronic medical disorders among elderly people like cardiovascular disorder, diabetic mellitus, hypertensive and asthma those showed a high prevalence. However, there is no a study of self-reported depressive symptoms among elderly people with VI in low-income countries including Ethiopia. The current study aimed to assess the prevalence and determinant factors of self-reported depressive symptoms among elderly people with VI attending the ophthalmologic outpatient clinic.
Methods and Materials
Study Settings and Populations
An institution-based cross-sectional study was conducted on elderly patients with visual impairment who had follow-up at the ophthalmologic department in Menelik II referral hospital, Addis Ababa, Ethiopia from January to June 2019. Menelik II referral hospital is the only ophthalmologic referral hospital that gives a large service for patients with eye diseases from the whole directions of the country. Patients aged 60 years and above, and who were on ophthalmologic follow-ups at the hospital were included. While those who were too medically and mentally ill, and having difficulty to communicate in the conversation/deaf were excluded.
Sample Size Determination
The sample size is calculated by using single population proportion formula:
n = (Zα/2)2 * P (1-P)/d2
Where n=sample size
Z= reliability coefficient at 5% significance level (α = 0.05), Zα/2 = 1.96
P = estimated proportion is assuming as 50% (0.5)
d=Margin of error as 5% (d = 0.05).
n = (1.96)2 * 0.5 (1–0.5)/(0.05)2 =384
By adding 10% non-response rate the final sample size was 423.
A total of 423 elderly patients with VI (vision loss and blindness) such as glaucoma, cataract, refractive errors, diabetic retinopathy, trachoma, dry eye disease, age-related macular degeneration were invited for interviews using the systematic random sampling technique.
Data Collection Tools
Self-reported depressive symptoms were assessed by using the Geriatric Depression Scale (GDS) having fifteen items to screen the prevalence of depression. The GDS-15 was developed specifically for older people and places less emphasis on somatic symptoms than do other generic depression scales. It asks respondents to answer “yes” or “no “from 1 to 15 questions about how they have felt in the past week and rated as 0 if response for the asked question is “no” and 1 if response for asked questions is yes. The total score ranges from 0 to 15. A cut off total score greater or equal to six (≥6) considered as having depression. This cut off point has been shown to yield a good combination of high sensitivity (91%) with a diagnosis of depression combined with an acceptable specificity (72%).33 The Cronbach’s alpha result of the tool in this study was 0.90 which is reliable.
The Oslo Social Support Scale (OSSS), which had three items, was used to assess the level of the participant’s social support. The scale ranged from 3 to 14, and the scores 3–8, 9–11, and 12–14 showing “poor”, “moderate”, and “strong” social support, respectively.34 Visual impairment in this study means that the individuals with the score of 6/18 of the visual acuity (VA) which examined by the ophthalmology professional.35 Individuals with the visual acuity (VA) score of 0.66–0.33 considered as mild level, a score of 0.33–0.12 indicates moderate level; and a score of less than or equal to 0.1 considered as severe level visual impairment.36 Items on socio-demographic (sex, age, marital status, educational level, residence, employment status and living with), clinical factors (severity/level of VI, duration of illness, having co-morbid medical and mental illnesses and experiencing surgical management), substance use (alcohol, Khat and smoking cigarettes/tobacco products) were adopted from previous studies.25,27,30,32
Data Collection Procedures
The data were collected using a structured questionnaire by both interviews and reviews of patient records. We have used standardized and structured questions which help to ask each candidate the same questions in the same order. The questionnaire contained socio-demographic characteristics, clinical-related conditions, substance use, social support (OSSS) and GDS-15 questions. Data were collected by five trained nurses by the Amharic version of the questionnaire for five months. The questionnaire was first prepared in English and translated to Amharic, the working language of Ethiopia, and back to English to maintain consistency. In view of understanding the local culture and language, data collectors were recruited from their expertise. Two days of training was given for data collectors and supervisor. The training entails; understanding of the purpose of the study, ways of recruiting eligible participants, seeking consent, discussion on questionnaire, potential challenges and possible solutions. The collected data was checked daily by the principal investigator and supervisor for completeness and consistency. The necessary feedback was provided back daily for the data collectors throughout the study period.
Data Processing and Analysis
The data were cleaned, coded and entered in the computer using EpiData 3.1 and analyzed by using STATA 14. Descriptive and bi-variable binary logistic regression analyses were employed to see the frequency distribution and assess the correlation between independent variables and depression, respectively. Variables with p-value <0.1 during the bi-variable logistic regression were selected for the multivariable logistic regression. The Adjusted odds ratio with a 95% confidence interval was used to report the results of factors associated with self-reported depression, and a p-value of < 0.05 was considered as statistically significant. The Hosmer-Lemeshow goodness and maximum likelihood was 0.64 to check the model fitness.
Ethical Approval and Consent to Participate
Ethical clearance and approval was obtained from the joint ethical review committee of the University of Gondar and Amanuel mental specialized hospital (AMSH). The Official letter of cooperation was submitted to the Addis Ababa health bureau and then a formal letter of permission was obtained from the health bureau. This study was conducted in accordance with the Declaration of Helsinki. Before data collection, the aim of the study was explained verbally to the participants and after their willingness, written permission was obtained before the interviews. So an informed written consent was obtained from the participants and confidentiality was maintained by omitting their identification.
Results
Socio-Demographic Characteristics of the Participants
A total of 423 participants took part in the study with a response rate of 97.3%. Nearly two-thirds of the study participants (63.4%) were males; 266 (64.6%) were married, and 148 (34%) were between 71and 80 years of age with the mean age of 72.63 ±6.53 years. Nearly half of the respondents (48.1%) were had not job and/retired at this moment; 169 (41%) were attended primary school; 265 (64.3%) were rural dwellers (Table 1).
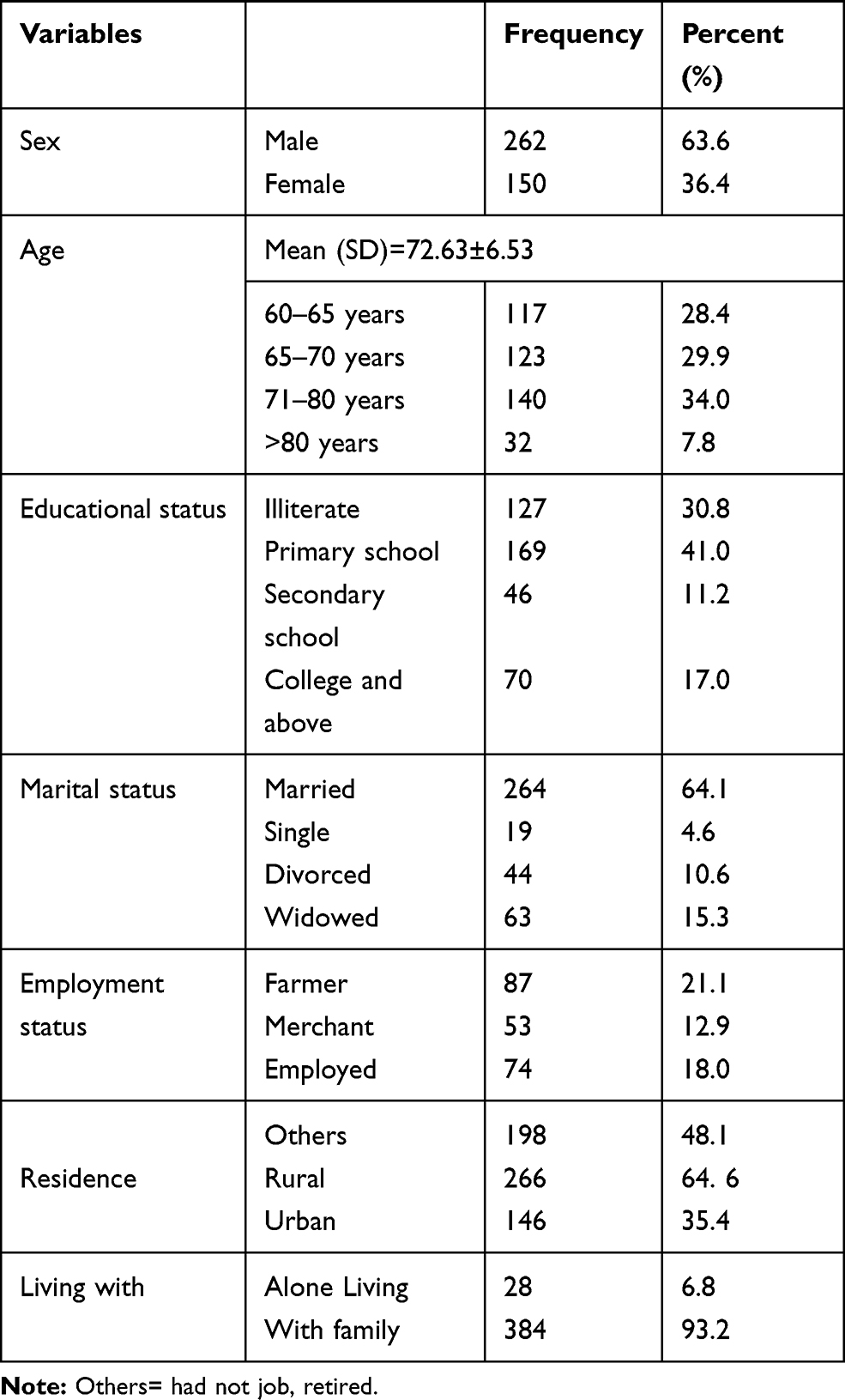 |
Table 1 Socio-Demographic Characteristics of the Study Participants with Visual Impairment at Menelik II Referral Hospital, Addis Ababa, Ethiopia, 2019 (n=412) |
Illness and Family-Related Characteristics of the Study Participants
Of the respondents, 159 (38.6%) were had a moderate level of VI; and 166 (40.3%) were living with the impairment for more than five years. More than half of the participants (55.8%) had undertaken surgical management after they have been exposed to illnesses such as cataract, glaucoma and refractive illness. Nearly one-third of the participants (33%) had cataract; 79 (19.2%) had experienced mental illness in their life; and 87 (21.1%) had a family history of mental illness (Table 2).
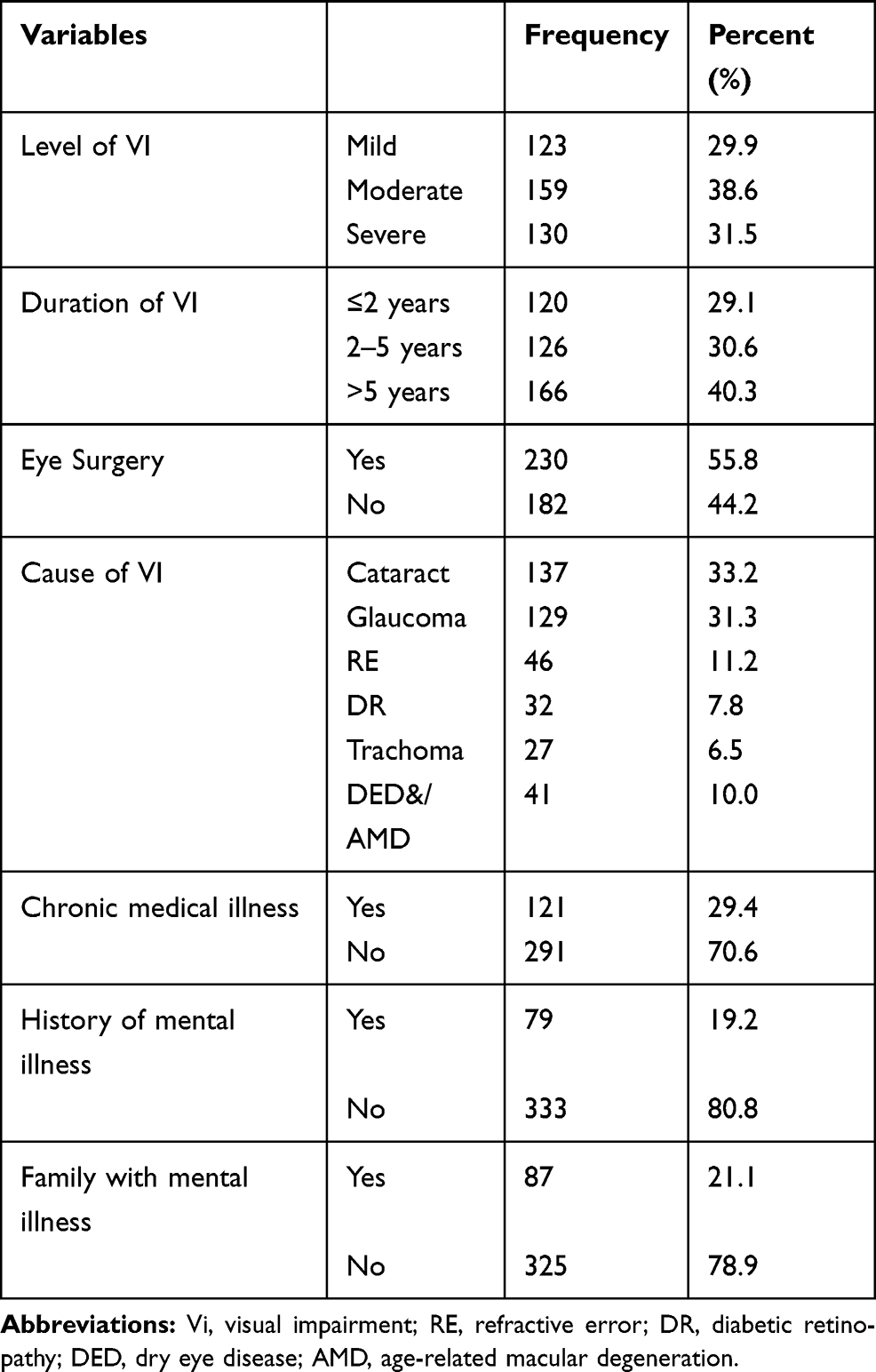 |
Table 2 Illness and Family-Related Conditions of Participants with Visual Impairment at Menelik II Referral Hospital, Addis Ababa, Ethiopia, 2019 (n=412) |
Social Support and Substance Use Information of the Participants
Of the respondents, 183 (44.4%), 154 (37.4%) and 75 (18.2%) had poor, medium and good social support, respectively. At the moment, nearly one-fourth of the participants (25.7%) were using different types of substances; of those 81 (19.7%), 48 (11.7%) and 35 (8.5%) were using alcohol, tobacco, and Khat, respectively.
Prevalence of Self-Reported Depressive Symptoms
The prevalence of self-reported depressive symptoms among elderly people with VI was 26.7% (n=110) with a 95% CI of 22.6 to 30.8. According to the type of the illness, the prevalence of depression among patients with glaucoma, cataract, diabetic retinopathy, DED, and/AMD, refractive error, and trachoma was 38.2%, 20.9%, 16.4%, 10%, 9.1%, and 5.5%, respectively. The Cross-tabulation showed that there was a significant correlation and prevalence rates differences between self-reported depressive symptoms and ocular diseases type (p<0.002) (Table 3).
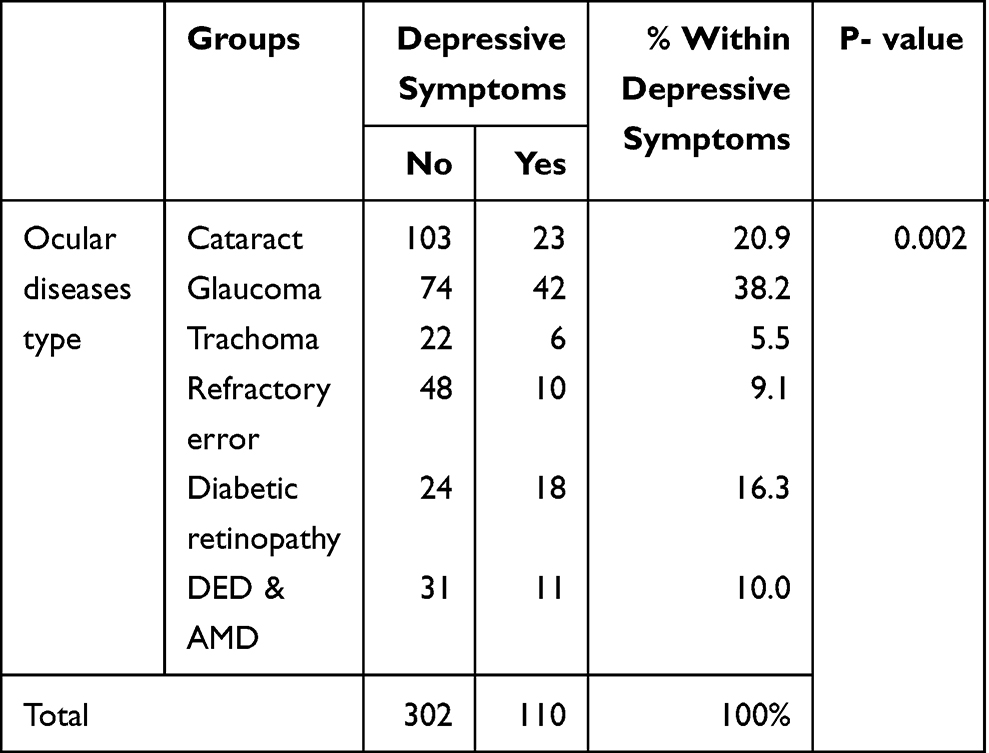 |
Table 3 Cross-Tabulation Showed Prevalence of Self-Reported Depressive Symptoms According to Each Ocular Disease |
Factors Associated with Depression Among Elderly Patients with VI
The bivariate binary logistic regression showed that sex, age, marital status, educational status, residence, social support, level of visual impairment, duration of illness, substances use at the moment, and history of mental illness were the factors found to be significantly associated with depression at p-value <0.1. The result of the multivariate logistic regression analysis indicated that widowhood, and single and/divorced in marital status, poor social support, a severe level of VI, and longer duration of illness (>5 years) were significantly associated with depression at p-value <0.05 (Table 4).
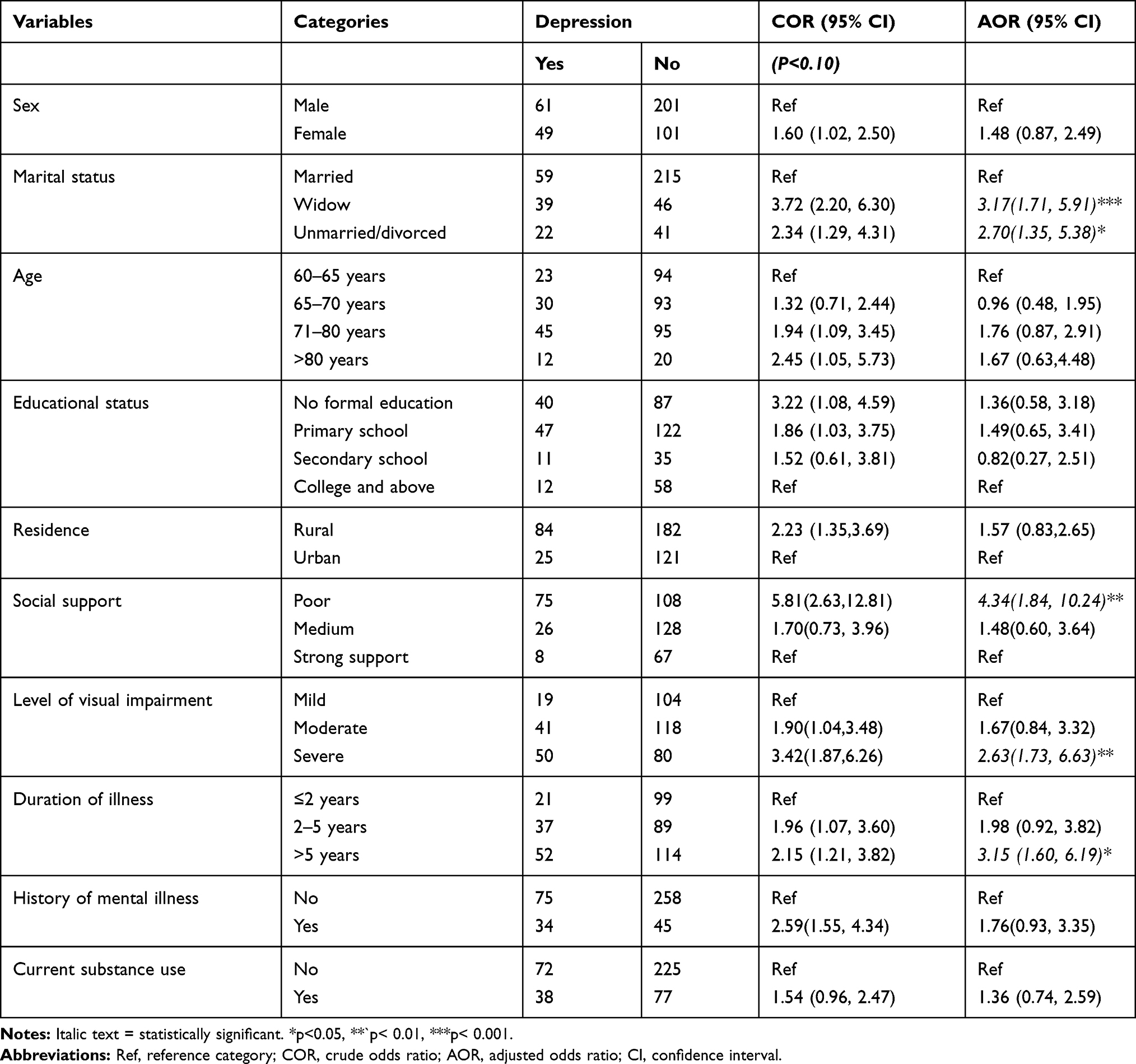 |
Table 4 Bi-Variable and Multi-Variable Binary Logistic Regression of Factors Associated with Depressive Symptoms Among Elderly Patients with VI at Menelik II Referral Hospital, 2019 (n=412) |
Being widowed and unmarried and/divorced in marital status were 3 and 2.70 times more likely to have depressive symptoms compared to those who were married (AOR) = 3.17 95% CI (1.71, 5.91)]; [AOR=2.70 95% CI (1.35, 5.38)], respectively. The elder visually impaired patients who had poor social support had 4 times [AOR=4.34, 95% CI (1.84, 10.24)] higher odds of self-reported depressive symptoms as compared with those who had good social support. The odds of having depressive symptoms among individuals with severe VI was 2.63 times more likely [AOR=2.63 95% CI (1.73, 6.63)] than those with mild VI. The odds of having self-reported depressive symptoms was 3 times [AOR=3.15, 95% CI: 1.60, 6.19] higher among older visually impaired individuals with longer duration (>5 years) of the illness as compared to those with short duration (≤2 years) of the illness.
Discussion
Vision impairment is one of the leading causes of disability in elder people and is associated with reduced quality of life, and increased the occurrence of depression.37 In turn, depression could cause a further decline in quality of life and health status, and aggravate the disability caused by visual impairment.18 This study attempted to assess the prevalence and determinant factors of depressive symptoms among the elder visually impaired people in Ethiopia.
In this study, the prevalence of self-reported depressive symptoms among elderly people with VI was 26.7% with a 95% CI of 22.6 to 30.8. The finding was in line with the studies in Armenia (28%),25 Malaysia (27.8%37 and New Zealand (29.4%).31 Conversely, our finding was higher than those of studies conducted in West Africa,29 South Korea,24 Britain39 and United States.40 The reason for the variation might be due to study population and depressive symptoms screening tools differences. For example: adult patients with Glaucoma aged ≥18 years were interviewed by using Zung Self-Rating Depression Scale (SDS) in West Africa’s study, and Center for Epidemiologic Studies-Depression scale (CES-D) tool was used in the South Korea study. While in this study, patients aged 60 years and above who were on follow-up for VI were interviewed by using GDS tool. It is expected that the variation of the magnitude of self-reported depressive symptoms resulted when data is collected by using different screening tools, and when the participants were adults’ vs older people. Besides, the discrepancy of this finding with that of the findings of studies conducted out of Ethiopia might be due to socio-economic and cultural differences. For example, in this study the participants were in low income countries, while counterpart studies were in middle and high-income countries. Because it is fact that reporting depressive symptoms have differ across countries and subpopulations, and having a good personal income during older age is an important protective factor for depressive symptoms in those people.
On the other hand, the finding of this study was lower than other previous studies conducted in Finland,38 Netherland24 and Australia.41 The discrepancy could be due to the variations in study population and screening tools used to measure depressive symptoms. For instant: In this study, the participants were patients aged 60 years and above who were on follow-up for VI at a referral hospital. The depressive symptoms were also measured using GDS through a face-to-face interviewing. On the opposite, the participants were patients with sensory impairment at age 75 years and older at a population basis using the Zung Depression Status Inventory (DSI) in the Finland study. Self-reported depressive symptoms could be increased in advanced age as the patients’ age increases and in the presence of additional sensory impairment. In addition, the participants were elderly people with age-related macular degeneration, and depression was assessed using Goldberg anxiety and depression scale (GAD) in the Australian study. Advanced age and age-related degeneration causes depressive symptoms due to restricted activities of daily living, and presence of psychosocial stressors like loss of their loved one, retirement and loneliness.14,42 Moreover, the data was collected through telephone interview in Netherland’s study. It is also expected that the variation of the prevalence of depressive symptoms resulted when data is collected through different techniques like face –to-face interview vs telephone interview. As a result these findings were supposed to higher prevalence of depressive symptoms compared to the current one.
Most of the factors associated with self-reported depressive symptoms in this study were similar with those of previous studies in different population groups. Widowhood, single and/divorced aged people with VI were more likely to have depressive symptoms compared to those who were living with their couple. Marital status was reported from different clinical and community-based studies as the main risk factors for depressive symptoms among older people.39,43 Being widowhood, unmarried and/divorced is one of the most devastating life events that are most associated with negative stress among older persons in particular report less well-being and more symptoms of depression compared to married individuals. This report was also consistent with other previous studies.28,36
Social support is the important contributor for self-reported depressive symptoms in which the odds of depressive symptoms was higher among older people with VI who had poor social support compared to good social support. This could be because visually impaired patients concerning social support, it is more plausible that low level of received social support will lead to an increased likelihood of loneliness. Again, the vision loss is also causes isolation and loneliness.14 Furthermore, Their families and community do not understand the psycho-social impact of the vision loss, and not support them. These reasons again cause the frequent occurrence of depressive symptoms. This finding was supported by other previous studies.14,44 Looking at the assumption on the relationship, social support seems to be a crucial factor for developing interventions in reducing loneliness among visually impaired older people to combating the impact of depressive symptoms.3
This study revealed that the elderly people with severe level of VI were more likely to have depressive symptoms than those with mild level of VI. This result was supported by other previous studies.8,25 This is the fact that persons who have a severe level of VI either one eye is blind or reduce the level of vision in both eyes were more commonly exposed to develop depressive symptoms than a mild level of visual impairment. In addition, this evidenced by that the cause of visual loss had an impact on levels of depressive symptoms. For example, the diagnosis of cataract, glaucoma, refractive errors, and age-related macular degeneration are chronic, progressive diseases leading to severe vision loss. Furthermore, little is known regarding the treatment for these disorders that can slow the progression and restore of vision. This result in functional impairment again can cause depressive symptoms.
Moreover, in this study, duration of the illness was significantly associated with self-reported depressive symptoms in elderly people with VI. The elderly people with longer duration of the VI (>five years) were more likely to have depressive symptoms as compared to those with shorter duration of the impairment. This finding is consistent with that of other studies.45,46 This might be due to that the longer the duration of the impairment, the more affects every aspect of patients’ life such as physical and mental health, family, social life, finances, and employment. This is especially common if VI is untreated properly for a long period. Then it results in depressive symptoms.
One of the main limitation of this work might be that the visual acuity was assessed using a simple, portable chart and the cause of visual loss was obtained from a medical record review. Secondly, since the interviewer bias is common, the data collectors may be preconceived and clouds their judgment about an interviewee on having of self-reported depressive symptoms that makes the interview less objective to determine the accurate magnitude of self-reported depressive symptoms in the survey. Additionally, it is difficult to determine the causal relationship between factors depressive symptoms owing to its cross-sectional nature.
Conclusion
The prevalence of self-reported depressive symptoms among elderly people with VI in Ethiopia was high. Widowhood, single and/divorced, poor social support, severe level and longer duration (>5 years) of the illness were factors associated with higher odds of self-reported depressive symptoms. Early intervention and integrating treatment services for co-existing mental disorders and Visual impairment is important, since depressive symptoms are common among elder people with visual impairment. Interventions targeted among widowhood, single and/divorced patients with severe level and longer duration of the illness, the special treatment, where it is offered and provide treatment for ocular diseases are recommended to reduce depressive symptoms and to prevent disability and poor medical illnesses. Interventions focused at identifying patients’ social support and strengthening community support systems is needed to prevent depressive symptoms. Again, appropriate early treatment of co-morbidities helps to improve patient and family quality of life.
Abbreviations
AMD, Age-related Macular Degeneration; AOR, Adjusted Odds Ratio; CI, Confidence Interval; DED, Dry Eye Disease; GDS, Geriatric Depression Scale; VA, Visual Acuity; VI, Visual Impairment; WHO, World Health Organization.
Data Sharing Statement
All the datasets used to the study are available within the manuscript.
Ethical Approval and Consent to Participate
Ethical clearance and approval was obtained from the joint ethical review committee of the University of Gondar and Amanuel mental specialized hospital (AMSH). The Official letter of cooperation was submitted to the Addis Ababa health bureau and then a formal letter of permission was obtained from the health bureau. This study was conducted in accordance with the Declaration of Helsinki. Before data collection, the aim of the study was explained verbally to the participants and after their willingness, written permission was obtained before the interviews. So an informed written consent was obtained from the participants and confidentiality was maintained by omitting their identification.
Acknowledgments
The authors acknowledge the University of Gondar and Amanuel’s mental specialized hospital for funding the study. We extend our gratitude to data collectors, supervisors and study participants for their time and effort.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
University of Gondar covers the cost (financial support) for personal expenditure, material fulfillment, transportation required for the study.
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. Organization WH. Prevention of Blindness and Visual Impairment. ICD Update and Revision Platform: Change the Definition of Blindness; 2011.
2. Aga AA. Avoidable visual impairment among elderly people in a slum of Addis Ababa. Ethiopian J Health Dev. 2001;15:2.
3. Horowitz A, Brennan M, Reinhardt JP. Prevalence and risk factors for self-reported visual impairment among middle-aged and older adults. Res Aging. 2005;27(3):307–326.
4. Deepthi R, Kasthuri A. Visual and hearing impairment among rural elderly of south India: a community‐based study. Geriatr Gerontol Int. 2011;1(12):116–122.
5. Bizuneh ZY, Tsega A, Addis Y, Admassu F. Knowledge Of Glaucoma And Associated Factors Among Adults In Gish Abay Town, Northwest Ethiopia. 2019.
6. Mehari ZA. A study of ocular morbidity of patients attending ophthalmic outreach services in rural Ethiopia. Int J Med Med Sci. 2013;3(4):450–454.
7. Organization WH. Global Data on Visual Impairments 2010. Geneva: WHO; 2012:1–5.
8. Rovner BW, Ganguli M. Depression and disability associated with impaired vision: the MoVies Project. J Am Geriatr Soc. 1998;46(5):617–619.
9. Woledesenbet MA, Shumet Mekonen S, Sori LM, Abegaz TM. Epidemiology of depression and associated factors among asthma patients in Addis Ababa, Ethiopia. Psychiatry Journal. 2018;2018.
10. Depression W. Other Common Mental Disorders: Global Health Estimates. Geneva: World Health Organization; 2017:1–24.
11. Kempen GIJM, Zijlstra GAR. Clinically relevant symptoms of anxiety and depression in low-vision community-living older adults. Am J Geriatric Psychiatry. 2014;22(3):309–313. doi:10.1016/j.jagp.2012.08.007
12. Tastan S, Iyigun E, Bayer A, Acikel C. Anxiety, depression, and quality of life in Turkish patients with glaucoma. Psychol Rep. 2010;106(2):343–357. doi:10.2466/pr0.106.2.343-357
13. McDonnall MC. Risk factors for depression among older adults with dual sensory loss. Aging Ment Health. 2009;13(4):569–576. doi:10.1080/13607860902774410
14. Verstraten P, Brinkmann W, Stevens N, Schouten J Loneliness, adaptation to vision impairment, social support and depression among visually impaired elderly. Paper presented at: International Congress Series. 2005.
15. Eramudugolla R, Wood J, Anstey KJ. Co-morbidity of depression and anxiety in common age-related eye diseases: a population-based study of 662 adults. Front Aging Neurosci. 2013;5:56. doi:10.3389/fnagi.2013.00056
16. Organization WH. The World Health Report 2001: Mental Health: New Understanding, New Hope. World Health Organization; 2001.
17. Alwan A, MacLean DR, Riley LM, et al. Monitoring and surveillance of chronic non-communicable diseases: progress and capacity in high-burden countries. Lancet. 2010;376(9755):1861–1868. doi:10.1016/S0140-6736(10)61853-3
18. Jones GC, Rovner BW, Crews JE, Danielson ML. Effects of depressive symptoms on health behavior practices among older adults with vision loss.. Rehabil Psychol. 2009;54(2):164. doi:10.1037/a0015910
19. Rovner BW, Casten RJ, Tasman WS. Effect of depression on vision function in age-related macular degeneration. Arch Ophthalmol. 2002;120(8):1041–1044.
20. Brody BL, Gamst AC, Williams RA, et al. Depression, visual acuity, comorbidity, and disability associated with age-related macular degeneration. Ophthalmology. 2001;108(10):1893–1900.
21. Rahman MS, Rahman MA, Ali M, et al. Determinants of depressive symptoms among older people in Bangladesh. J Affect Disord. 2020;264:157–162.
22. Wenxue L, Zhong B, Xiujun L, et al. Depressive symptoms among the visually disabled in Wuhan: an epidemiological survey. Shanghai Arch Psychiatry. 2013;25(5):306.
23. Zheng Y, Wu X, Lin X, Lin H. The prevalence of depression and depressive symptoms among eye disease patients: a systematic review and meta-analysis. Sci Rep. 2017;7:46453.
24. van der Aa HP, Comijs HC, Penninx BW, van Rens GH, van Nispen RM. Major depressive and anxiety disorders in visually impaired older adults. Invest Ophthalmol Vis Sci. 2015;56(2):849–854.
25. Giloyan A, Harutyunyan T, Petrosyan V. Visual impairment and depression among socially vulnerable older adults in Armenia. Aging Ment Health. 2015;19(2):175–181.
26. Cho GE, Lim DH, Baek M, Lee H, Kim SJ, Kang SW. Visual impairment of Korean population: prevalence and impact on mental health. Invest Ophthalmol Vis Sci. 2015;56(8):4375–4381.
27. Noran NH, Izzuna MG, Bulgiba AM, Mimiwati Z, Ayu SM. Severity of visual impairment and depression among elderly Malaysians. Asia Pacific J Public Health. 2009;21(1):43–50.
28. Bernabei V, Morini V, Moretti F, et al. Vision and hearing impairments are associated with depressive–anxiety syndrome in Italian elderly. Aging Ment Health. 2011;15(4):467–474.
29. Akindipe TO, Aina F, Onakoya A. Risk of depression and subjective quality of life among attendees of a West African glaucoma clinic. Int J Med Med Sci. 2011;1(2):432–435.
30. Evans JR, Fletcher AE, Wormald RP. Depression and anxiety in visually impaired older people. Ophthalmology. 2007;114(2):283–288.
31. Hayman KJ, Kerse NM, La Grow SJ, Wouldes T, Robertson MC, Campbell AJ. Depression in older people: visual impairment and subjective ratings of health. Optometry Vision Sci. 2007;84(11):1024–1030.
32. Kim KW, Han SB, Han ER, et al. Association between depression and dry eye disease in an elderly population. Invest Ophthalmol Vis Sci. 2011;52(11):7954–7958.
33. Yesavage JA, Brink T, Rose TL, et al. Development and validation of a geriatric screening scale: a preliminary report. J Psychiatr Res. 1983;17(1):37–49.
34. Dalgard OSDC, Lehtinen V, Vazquez-Barquero JL, et al. Negative life events, social support and gender difference in depression. Soc Psychiatry Psychiatr Epidemiol. 2006;41(6):444–451.
35. Bazargan M, Baker RS, Bazargan SH. Sensory impairments and subjective well-being among aged African American persons. J Gerontol B Psychol Sci Soc Sci. 2001;56(5):P268–P278.
36. Hong T, Mitchell P, Burlutsky G, Gopinath B, Liew G, Wang JJ. Visual impairment and depressive symptoms in an older Australian cohort: longitudinal findings from the Blue Mountains Eye Study. Br J Ophthalmol. 2015;99(8):1017–1021.
37. Carrière I, Delcourt C, Daien V, et al. A prospective study of the bi-directional association between vision loss and depression in the elderly. J Affect Disord. 2013;151(1):164–170.
38. Lupsakko T, Mäntyjärvi M, Kautiainen H, Sulkava R. Combined hearing and visual impairment and depression in a population aged 75 years and older. Int J Geriatr Psychiatry. 2002;17(9):808–813.
39. Schaan B. Widowhood and depression among older Europeans—The role of gender, caregiving, marital quality, and regional context. J Gerontology Series B. 2013;68(3):431–442.
40. Zhang X, Bullard KM, Cotch MF, et al. Association between depression and functional vision loss in persons 20 years of age or older in the United States, NHANES 2005–2008. JAMA Ophthalmol. 2013;131(5):573–581.
41. Mathew RS, Delbaere K, Lord SR, Beaumont P, Madigan MC. Depressive symptoms and quality of life in people with age‐related macular degeneration. Ophthalmic Physiol Optics. 2011;31(4):375–380.
42. Kempen GI, Ballemans J, Ranchor AV, van Rens GH, Zijlstra GR. The impact of low vision on activities of daily living, symptoms of depression, feelings of anxiety and social support in community-living older adults seeking vision rehabilitation services. Quality Res. 2012;21(8):1405–1411.
43. Organization WH. Depression and Other Common Mental Disorders: Global Health Estimates. World Health Organization; 2017.
44. O’Donnell C. The greatest generation meets its greatest challenge: vision loss and depression in older adults. J Vis Impair Blind. 2005;99(4):197–208.
45. Geerlings SW, Beekman ATF, Twisk Jwr DJHD, Van Tilburg W. Duration and severity of depression predict mortality in older adults in the community. Psychol Med. 2002;32(4):609.
46. Ribeiro MVMR, Hasten-Reiter Júnior HN, Ribeiro EAN, Jucá MJ, Barbosa FT, Sousa-Rodrigues C. Association between visual impairment and depression in the elderly: a systematic review. Arq Bras Oftalmol. 2015;78(3):197–201.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.