Back to Journals » Drug Design, Development and Therapy » Volume 19
The Predictive Value of Initial Trough Concentration of Voriconazole and Procalcitonin in Hepatotoxic Adverse Events
Authors Chen L, Wang X, Wu X, Qin H, Zhu H
Received 15 August 2025
Accepted for publication 17 November 2025
Published 26 November 2025 Volume 2025:19 Pages 10507—10518
DOI https://doi.org/10.2147/DDDT.S560753
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Lijuan Chen,1 Xinwen Wang,1 Xiaoli Wu,1 Haiyan Qin,1 Hongchao Zhu2
1Department of Pharmacy, The Affiliated Huaian No. 1 People’s Hospital of Nanjing Medical University, Huaian, Jiangsu Province, People’s Republic of China; 2Department of Nuclear Medicine, The Affiliated Huaian No. 1 People’s Hospital of Nanjing Medical University, Huaian, Jiangsu Province, People’s Republic of China
Correspondence: Hongchao Zhu, Department of Nuclear Medicine, The Affiliated Huaian No. 1 People’s Hospital of Nanjing Medical University, Huaian, Jiangsu Province, 223300, People’s Republic of China, Email [email protected]
Purpose: This study aimed to evaluate the predictive value of initial trough concentration (Cmin) of voriconazole (VCZ) and procalcitonin (PCT) in hepatotoxic adverse events.
Patients and Methods: A retrospective analysis was performed on clinical data from 170 patients administered VCZ at our institution between January 2021 and July 2025. Risk factors associated with VCZ-induced hepatotoxicity were identified through binary logistic regression analysis. The diagnostic performance of initial VCZ-Cmin and PCT in predicting hepatotoxicity was evaluated using receiver operating characteristic (ROC) curve analysis.
Results: The mean loading dose of VCZ was 9.48 mg/kg, with a maintenance dose of 6.62 mg/kg, and an average initial Cmin of 5.58 mg/L. Hepatotoxicity was observed in 20.59% (35/170) of patients during the treatment period. Multivariate logistic regression analysis, adjusted for confounding factors including weight, maintenance dose, and proton pump inhibitors use, revealed that elevated initial VCZ-Cmin and high PCT levels were significantly associated with hepatotoxicity. ROC curve analysis identified critical thresholds for hepatotoxicity risk: an initial VCZ-Cmin of 5.035 mg/L (AUC=0.663, P=0.003) and a PCT level of 0.835 ng/mL (AUC=0.754, P< 0.001), the predictive probability of their combination was 0.184 (AUC=0.744, P< 0.001). After grouping according to the threshold level of PCT, there was a significant difference in the initial VCZ-Cmin between patients with high PCT levels and those with low PCT levels (P=0.005).
Conclusion: VCZ-induced hepatotoxicity is the common adverse reaction, exhibiting significant associations with elevated initial VCZ-Cmin and increased PCT levels. Both the initial VCZ-Cmin and PCT levels are independent risk factors, and either alone or in combination can predict the occurrence of hepatotoxicity. Among these, PCT levels have the most significant predictive value.
Keywords: voriconazole, initial trough concentration, procalcitonin, hepatotoxicity, therapeutic drug monitoring
Introduction
Voriconazole (VCZ) is a broad-spectrum antifungal agent, serving as the first-line treatment of choice for pulmonary, sinus, and central nervous system aspergillus infections, as well as the preferred therapeutic option for Scedosporium apiospermum infections.1,2 While demonstrating broad-spectrum antifungal activity, VCZ is associated with notable adverse effects, including visual disturbances, neurological manifestations, and hepatotoxicity. Pharmacovigilance data from the French Pharmacovigilance Center, encompassing the initial four-year post-marketing period, identified hepatic function abnormalities as the most frequently reported adverse event.3 Subsequent investigations have consistently demonstrated that hepatotoxicity constitutes the primary cause for VCZ dose reduction or treatment cessation.4,5 A multicenter study conducted by Hamada et al further substantiated these findings, revealing a significantly higher incidence of dose modification or discontinuation due to hepatotoxicity compared to visual disturbances.5 Given its persistent nature and higher prevalence relative to other transient or less frequent adverse effects, VCZ-induced hepatotoxicity warrants comprehensive investigation to elucidate its underlying mechanisms and optimize therapeutic management.6
The relationship between VCZ plasma concentrations and hepatotoxicity remains a subject of ongoing debate in the scientific literature. A meta-analysis conducted by Hanai et al included 25 studies involving a total of 2554 patients. The results indicated that the incidence of hepatotoxicity significantly increased with rising VCZ-Cmin. To prevent VCZ-related adverse events, the study recommended maintaining the optimal VCZ-Cmin at <3.0 µg/mL.7 While some studies have reported associations between elevated VCZ-Cmin (>4.0 or 6.0 mg/L) and increased hepatotoxicity risk, this correlation has not been consistently demonstrated across all investigations.8,9 Notably, a prospective study conducted by Pascual et al observed a numerical increase in hepatotoxicity incidence (from 8% to 19%) when initial VCZ-Cmin exceeded 5.5 mg/L, however, this difference did not reach statistical significance.10 Two recent studies have also demonstrated that there is no correlation between the steady-state VCZ-Cmin and hepatotoxicity,4,11 suggesting that other factors may contribute to the development of hepatotoxicity.
During VCZ therapy, dynamic alterations in patients’ inflammatory status significantly influence the concentrations of inflammatory cytokines. These cytokines exert inhibitory effects on cytochrome P450 isoenzymes through transcriptional regulation, resulting in decreased mRNA expression, protein synthesis, and enzymatic activity.12–14 Consequently, these molecular changes modify VCZ’s metabolic rate, ultimately affecting its plasma concentration.15,16 While procalcitonin (PCT) has been established as a robust biomarker for bacterial infection diagnosis.17 The association between PCT levels and VCZ-Cmin remains poorly characterized in the current literature.
This retrospective study investigated the clinical data of patients with fungal infections who underwent VCZ treatment at our institution in recent years. The primary objectives were to examine the association between the initial VCZ-Cmin and PCT levels, and to evaluate their potential roles as risk factors for hepatotoxicity, as well as their predictive value in hepatotoxic adverse events, aiming to provide evidence-based insights for optimizing the clinical application of VCZ.
Patients and Methods
Patients
This single-center retrospective cohort study was conducted at the Affiliated Huaian No. 1 People’s Hospital of Nanjing Medical University. Patients who received VCZ treatment from January 2021 to July 2025 were included. The inclusion criteria comprised: (1) patients aged≥18 years; (2) a minimum hospital stay of 7 days; and (3) at least one steady-state VCZ-Cmin date obtained, concomitant evaluations were conducted, including comprehensive routine blood analyses, PCT levels, serum albumin concentrations, and additional biochemical parameters, all measured on the same day as the Cmin assessment. The exclusion criteria included: (1) the presence of definitive hepatobiliary diseases, such as viral hepatitis, alcoholic liver disease, autoimmune liver disease, or primary biliary or sclerosing cholangitis; (2) the administration of liver-protective or enzyme-lowering therapies during the study period; and (3) the concurrent use of other medications with established hepatotoxicity, including isoniazid, rifampin, and docetaxel, during VCZ treatment. In this investigation, the VCZ-Cmin was quantitatively assessed using the Siemens Syva Viva-ProE drug concentration analyzer through enzyme-linked immunosorbent assay (ELISA) methodology, while PCT levels were determined via electrochemiluminescence immunoassay (ECLIA). The study was approved by the ethics committee of Huaian No. 1 People’s Hospital (approval number: KY-2023-077-01; date: May 11, 2023).
Data Collection
Patient data were systematically extracted from both electronic and paper-based medical records and subsequently compiled into structured spreadsheets. The collected data encompassed the following key domains: (1) Demographic characteristics, including age, gender, weight, and length of hospital stay; (2) Diagnostic information pertaining to fungal infections and associated comorbidities; (3) Hepatic and renal function parameters, measured both prior to and following VCZ administration, including total bilirubin (TBIL), alkaline phosphatase (ALP), alanine aminotransferase (ALT), aspartate aminotransferase (AST), gamma-glutamyl transferase (γ-GGT), and serum creatinine (SCr); (4) Pharmacological data, including the initial VCZ-Cmin, prescribed dosage, route of administration, treatment course, time of hepatotoxicity occurrence, and concomitant medications; (5) Laboratory parameters obtained on the day of initial VCZ-Cmin measurement, including serum PCT, serum albumin (Alb), white blood cell count (WBC), neutrophil percentage (NEUT%), total cholesterol (TC), and triglyceride (TG) levels.
Definition of Voriconazole-Induced Hepatotoxicity
This investigation utilized the Roussel Uclaf Causality Assessment Method (RUCAM) scale, as revised by Danan and Teschke (2016),18 for the systematic evaluation of drug-induced liver injury (DILI). The assessment parameters incorporated biochemical markers indicative of DILI, with the R value calculated as the ratio of ALT to its upper limit of normal (ULN) divided by the ratio of ALP to its ULN. The R value served as a diagnostic classifier: values≥5 were indicative of hepatocellular injury, values≤2 suggested cholestatic injury, and values between 2–5 denoted mixed injury patterns. The RUCAM scoring system was implemented with the following classification criteria: scores≤0 indicated no drug-related hepatotoxicity; 1–2 points were classified as “unlikely”; 3–5 points as “possible”; 6–8 points as “probable”; and scores >8 as “highly probable”. For the purposes of this study, a RUCAM score ≥6 was established as the threshold indicating that VCZ was likely or highly likely to induce hepatotoxicity. Considering the temporal pattern of VCZ-induced hepatotoxicity, which predominantly manifests within 1–2 weeks of treatment initiation,19 the observation period was standardized to 30 days following the initial dose administration.
Criteria for Assessing the Severity of Hepatotoxicity
The severity of hepatotoxicity was assessed in accordance with the Common Terminology Criteria for Adverse Events (CTCAE) version 5.0,20 as established by the US Department of Health and Human Services. The CTCAE employs a five-tiered grading system to classify adverse events. The reference ULN values for hepatic function parameters, as determined by our institutional laboratory, were defined as follows: TBIL at 26 μmol/L, ALP at 135 U/L, γ-GGT at 60 U/L, AST at 40 U/L, and ALT at 40 U/L.
Dose Adjustment and Therapeutic Drug Monitoring
In this study, therapeutic drug monitoring of VCZ is systematically performed on the 4th or 5th day post-initial administration. A standardized dose adjustment protocol is implemented based on Cmin measurements: for patients exhibiting VCZ-Cmin levels exceeding 5.5 mg/L, irrespective of adverse event manifestation, the dose is reduced by 50%; persistent elevation in concentration warrants an additional 50% reduction, with potential drug discontinuation if clinically indicated. Conversely, when VCZ-Cmin falls below 1 mg/L, a 50% dose escalation is administered. For individuals requiring dose adjustments following the attainment of steady-state trough concentrations during therapy, the new steady-state trough concentration is determined as the concentration measured on or after the fourth day following the dose modification.21
Definition of Initial VCZ-Cmin
In patients administered a loading dose of VCZ (6 mg/kg intravenously every 12 hours for two doses within the initial 24-hour period, followed by 4 mg/kg intravenously every 12 hours or 200 mg orally twice daily), the initial VCZ-Cmin is defined as the concentration measured at or beyond 24 hours post-administration.22
Statistical Analysis
Normally distributed continuous data were expressed as mean value (±standard deviation, SD), while non-normally distributed continuous data were expressed as median (interquartile range, IQR). Categorical variables were expressed as counts (%). In univariate analysis, a Student’s t-test or Mann–Whitney U-test was performed to compare continuous variables, and a Pearson chi-square test or Fisher’s exact test was used to compare categorical variables. Binary logistic regression analysis was employed to conduct multifactorial analysis. The ROC curve was applied to analyze and evaluate the diagnostic value of initial VCZ-Cmin and PCT in voriconazole-induced hepatotoxicity. All statistical analyses were performed using SPSS Statistics version 27 (IBM, Chicago, Illinois, USA). The value of P<0.05 was considered statistically significant.
Results
Basic Patient Information
The demographic and clinical characteristics of the patients are detailed in Table 1. Among the 170 patients, 10 were on prophylactic medication, while 160 were diagnosed with invasive fungal infections. Aspergillus infection was the most common, accounting for 46.47%, followed by Candida infection at 26.47%. The positive rate of the GM test was 12.35%. Among patients treated with VCZ, respiratory diseases were the most common underlying conditions, accounting for 30.59%, followed by cardiovascular diseases and diabetes, each at 17.65%. The average loading dose of VCZ was 9.48 mg/kg/day, with a maintenance dose of 6.62 mg/kg/day. The average treatment duration was 14.29 days, and the average initial Cmin was 5.58 mg/L. Based on the normal reference range of VCZ-Cmin at our hospital (1–5 mg/L), patients were categorized into high initial Cmin (Cmin>5 mg/L), accounting for 54.12%; normal initial Cmin (1 mg/L≤Cmin≤5 mg/L), accounting for 42.35%; and low initial Cmin (Cmin<1 mg/L), accounting for 3.53%.
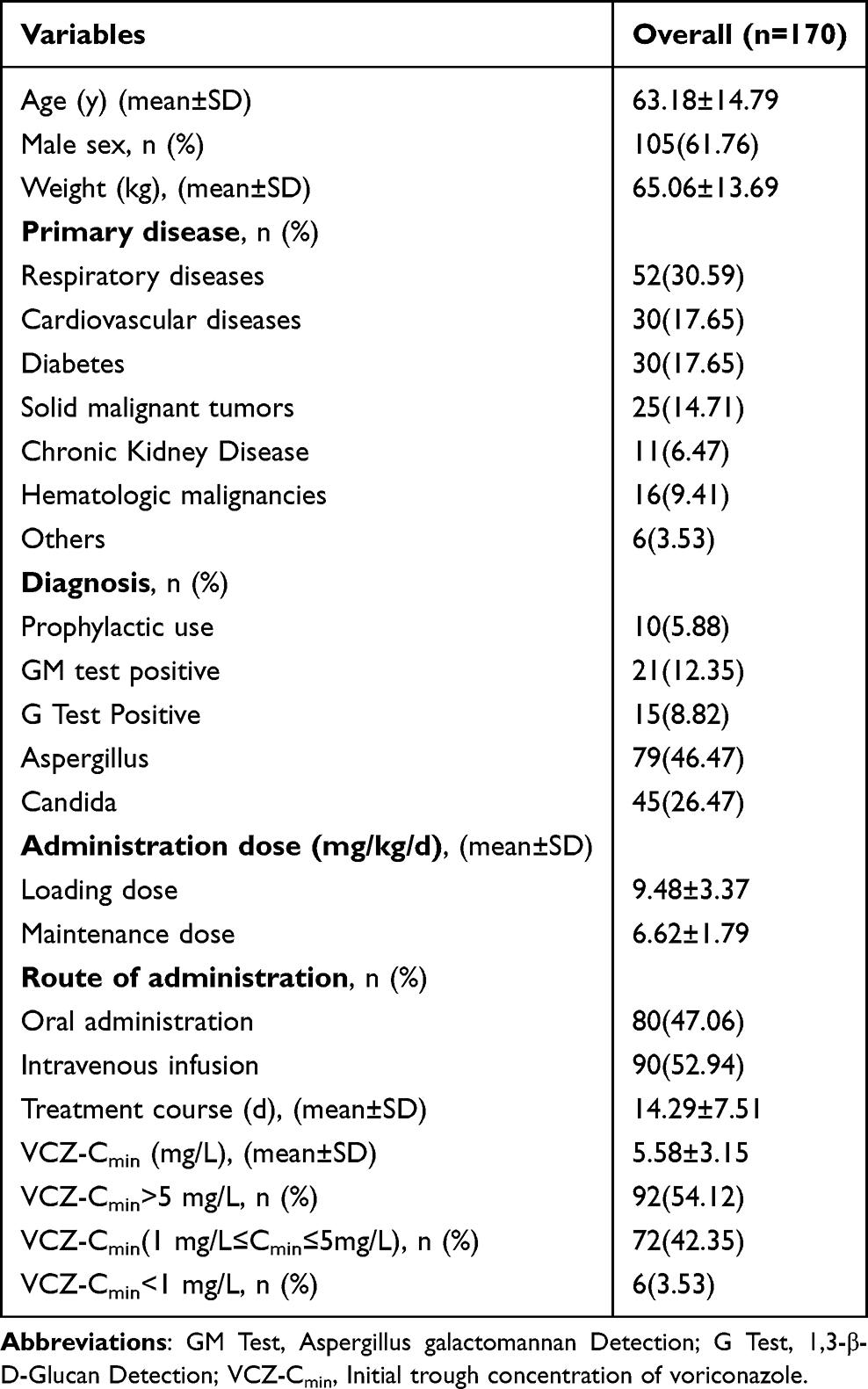 |
Table 1 Demographic and Clinical Characteristics of the Study Patients |
Hepatotoxicity Types Induced by VCZ and Their CTCAE Grades
As presented in Table 2, hepatotoxic reactions were observed in 20.59% (35/170) of patients treated with VCZ. The hepatotoxicity manifestations were categorized as follows: Hepatocellular injury (2.9%, 1/35), cholestatic injury (77.1%, 27/35), and mixed injury (20%, 7/35). Based on the CTCAE grading system, the severity distribution of hepatotoxicity was grade 1 in 25.71% (9/35), grade 2 in 28.57% (10/35), grade 3 in 31.43% (11/35), and grade 4 in 14.29% (5/35), with no grade 5 cases reported. A significant correlation was identified between hepatotoxicity proportion and initial Cmin: the proportion was 71.43% (25/35) when Cmin exceeded 5 mg/L, 28.57% (10/35) when Cmin ranged between 1 mg/L and 5 mg/L, and 0% when Cmin was below 1 mg/L.
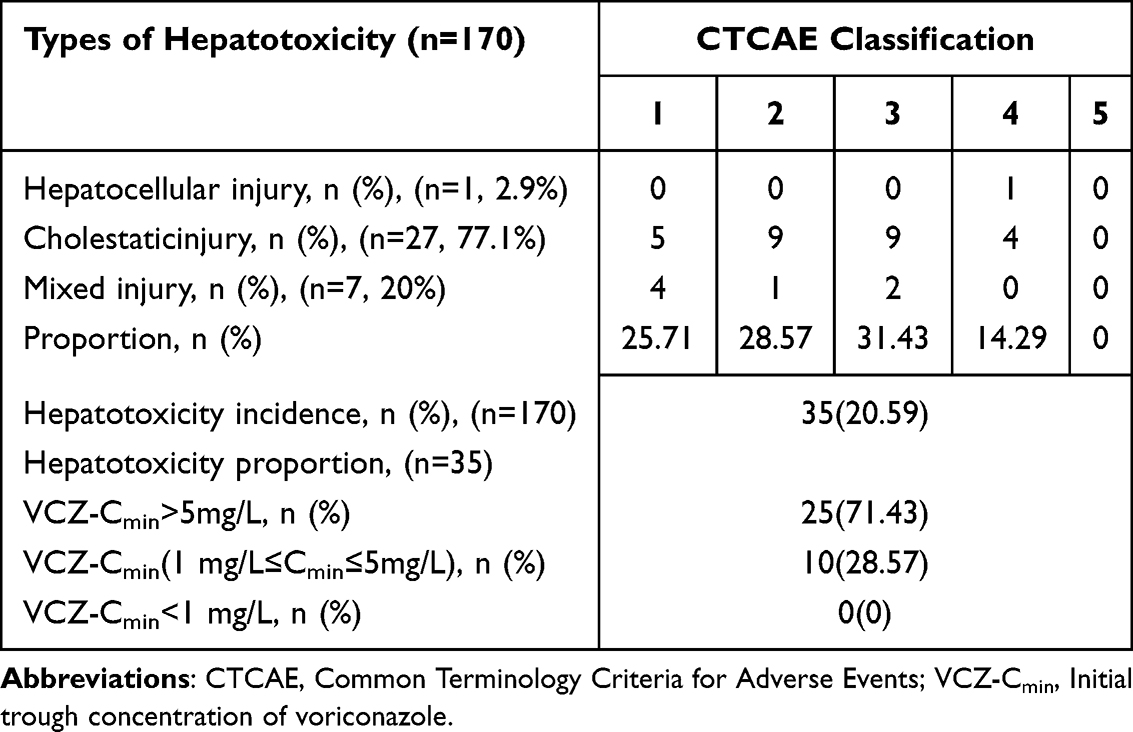 |
Table 2 Hepatotoxicity Types Induced by VCZ and Their CTCAE Grades |
Univariate Analysis Comparison of the Hepatotoxicity Group and the Non-Hepatotoxicity Group in Patients Treated with VCZ
As demonstrated in Table 3, the mean initial VCZ-Cmin in the hepatotoxicity group (6.79 mg/L) was significantly elevated compared to that in the non-hepatotoxicity group (5.27 mg/L; P=0.004). Furthermore, significant differences were observed in several hematological and biochemical parameters between the two groups. Specifically, the hepatotoxicity group exhibited markedly higher levels of WBC, NEUT%, TG, and PCT compared to the non-hepatotoxicity group (P<0.05 for all comparisons).
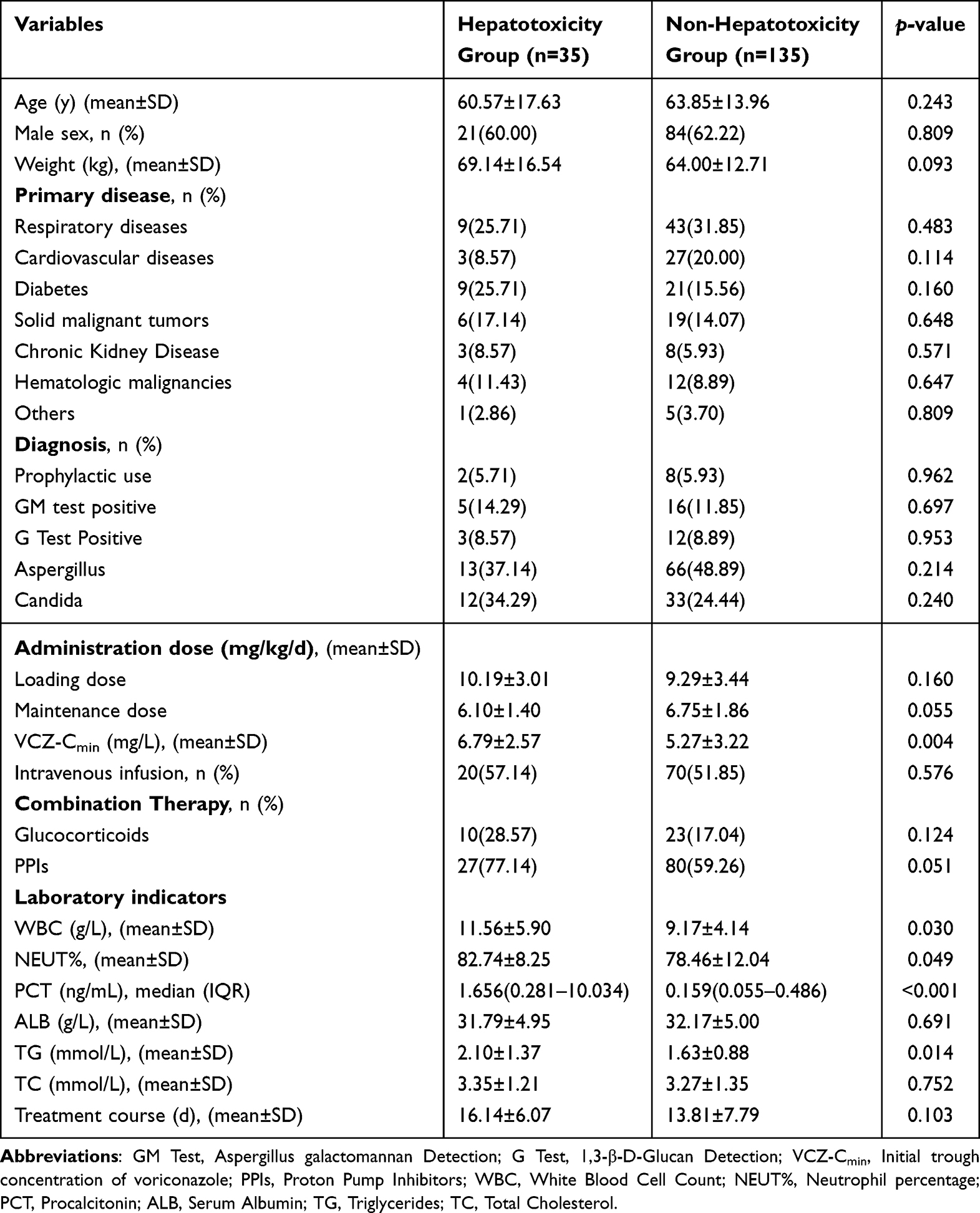 |
Table 3 Comparison of Clinical Data Between the VCZ Hepatotoxicity Group and the Non-Hepatotoxicity Group Using Univariate Analysis |
Multivariate Logistic Regression Analysis of VCZ-Induced Hepatotoxicity
Variables demonstrating a univariate association with P<0.1 in Table 3 were subsequently incorporated into a multivariate binary logistic regression analysis. As presented in Table 4, both elevated initial VCZ-Cmin and increased PCT levels emerged as independent risk factors for VCZ-induced hepatotoxicity, with odds ratios (OR) of 1.161 (95% CI=1.033–1.306, P=0.013) and 1.175 (95% CI=1.064–1.298, P=0.001), respectively. Following multivariate adjustment, the OR values were refined to 1.211 (95% CI=1.046–1.402, P=0.010) and 1.120 (95% CI=1.004–1.248, P=0.041) for these variables.
 |
Table 4 Multivariate Logistic Regression Analysis of VCZ-Induced Hepatotoxicity |
Evaluation of Initial VCZ-Cmin and PCT Levels and Their Combination as Predictive Biomarkers for VCZ-Induced Hepatotoxicity
As demonstrated in Figure 1 and Table 5, the ROC curve analysis demonstrated that specific biomarkers had significant predictive power for VCZ-induced hepatotoxicity. The initial VCZ-Cmin exhibited an AUC of 0.663 (95% CI: 0.573–0.752, P=0.003), while PCT levels demonstrated an AUC of 0.754 (95% CI: 0.663–0.846, P<0.001). Their combination demonstrated an AUC of 0.744 (95% CI: 0.660–0.828, P<0.001). The optimal predictive thresholds for hepatotoxicity were identified as 5.035 mg/L for the initial VCZ-Cmin and 0.835 ng/mL for PCT levels.
 |
Table 5 The Initial VCZ-Cmin and PCT Levels and Their Combination Were Analyzed Using the ROC Curve |
 |
Figure 1 The predictive value of initial VCZ-Cmin and PCT levels and their combination on the risk of voriconazole-induced hepatotoxicity. |
The Influence of PCT Levels on Initial VCZ-Cmin and Associated Hepatotoxic Adverse Events
As demonstrated in Table 6, further analysis demonstrated a significantly higher incidence of hepatotoxicity in patients with PCT levels≥0.835 ng/mL (43.14%, 22/51) compared to those with PCT levels<0.835 ng/mL (10.92%, 13/119), with the difference reaching statistical significance (P<0.001). Furthermore, the mean initial VCZ-Cmin was significantly elevated in the PCT≥0.835 ng/mL group (6.62 mg/L) relative to the PCT<0.835 ng/mL group (5.14 mg/L), with this difference also demonstrating statistical significance (P=0.005).
 |
Table 6 The Impact of PCT≥0.835 ng/mL and PCT<0.835 ng/mL on the Initial VCZ-Cmin and Hepatotoxic Adverse Reactions |
Discussion
The Dutch Pharmacogenetics Working Group has developed a more precise dosage adjustment scheme for VCZ based on pharmacogenomic treatment recommendations. This scheme suggests determining the initial dose according to the patient’s CYP2C19 genotype: for slow metabolizers, the dose should be reduced by 50%; for rapid metabolizers, the dose should be increased by 50%.23 The study by Pascual et al showed that the Cmin of patients in the 8 mg/kg daily dose group was 2.9 mg/L, while the Cmin of patients in the 7 mg/kg daily dose group was 1.7 mg/L.10 Racil et al reported that only 3.1% of patients achieved a Cmin of 5.0 mg/L at conventional dosing levels.24 Hamada et al noted that the median Cmin of patients receiving adequate doses (including loading doses) was 3.9 mg/L, with 30% of patients having an initial Cmin≥5 mg/L and only 7% having an initial Cmin<1.0 mg/L.5 In this study, 170 patients received a daily loading dose of 9.48 mg/kg and a maintenance dose of 6.62 mg/kg. The results showed that 54.12% of patients had an initial Cmin>5.0 mg/L, only 3.53% had an initial Cmin<1.0 mg/L, and the average initial Cmin value was 5.58 mg/L. The present study revealed that patients receiving standard VCZ dosing regimens exhibited significantly higher initial Cmin compared to previously reported values, with a substantial proportion of patients demonstrating Cmin levels exceeding 5.0 mg/L. These findings suggest that the Chinese population predominantly exhibits a poor metabolizer phenotype for VCZ, characterized by reduced hepatic clearance, elevated plasma trough concentrations, and consequently, an increased risk of drug-related adverse events. These observations underscore the critical importance of implementing therapeutic drug monitoring as a standard clinical practice during VCZ therapy to optimize treatment efficacy and minimize toxicity.
A multicenter investigation by Saito et al identified hepatotoxicity in 6.9% of patients undergoing VCZ therapy for fungal infections.25 In contrast, Luong et al observed a significantly higher incidence, with 51% of VCZ-treated patients developing hepatotoxicity, leading to treatment discontinuation in 34% of cases.26 A comprehensive systematic review and meta-analysis conducted by Xing et al reported an intermediate hepatotoxicity rate of 17.7% among VCZ recipients.27 Notably, multiple studies have consistently demonstrated the absence of a significant association between initial VCZ-Cmin and hepatotoxicity risk.4,10 In the present study, hepatotoxicity was observed in 20.59% of 170 patients receiving VCZ, with cholestatic type predominating (77.1% of cases). Hepatotoxicity incidence exhibited a concentration-dependent relationship: 71.43% of patients with initial Cmin>5 mg/L developed hepatotoxicity, compared to 28.57% in the therapeutic range (1–5 mg/L), while no cases were observed at Cmin<1 mg/L. These findings indicate that elevated initial VCZ-Cmin are associated with increased hepatotoxicity risk, which can manifest even within the established therapeutic range (1–5 mg/L), primarily presenting as mild to moderate cholestatic hepatotoxicity.
Through a systematic review and meta-analysis, Jin et al identified that a VCZ-Cmin exceeding 3 mg/L significantly increased the risk of hepatotoxicity in the Asian population.6 Similarly, Hamada et al established a strong correlation between Cmin and the incidence of hepatotoxicity and visual disturbances, with a hepatotoxicity threshold of 3.5 mg/L.5 Shi et al reported that hepatotoxicity, while associated with elevated plasma drug concentrations, could also manifest at lower levels.28 Shen et al further corroborated these findings, demonstrating that steady-state Cmin were predictive of hepatotoxicity, with a critical threshold of 3.61 mg/L.29 In their clinical practice guidelines for VCZ therapeutic drug monitoring, Takesue et al recommended maintaining Cmin below 4.0 mg/L for Asian populations and below 5.5 mg/L for non-Asian populations, with corresponding maintenance doses of 6 mg/kg and 8 mg/kg, respectively, to minimize adverse effects.30 In this investigation, the maintenance dose was established at 6.62 mg/kg. The ROC curve analysis identified an initial Cmin of 5.035 mg/L as a predictive threshold for hepatotoxicity, with an AUC of 0.663. This Cmin value appears elevated compared to prior studies, potentially reflecting interindividual variability in VCZ pharmacokinetics or the complexity of patients’ comorbid conditions. In our institutional clinical protocol, according to the Practice Guidelines of the Therapeutic Drug Monitoring Branch of the Chinese Pharmacological Society, dose adjustment is typically initiated when VCZ-Cmin exceeds 5.5 mg/L.31 However, our ROC analysis revealed a lower critical threshold of 5.035 mg/L for hepatotoxicity prediction. Based on these findings, we recommend considering dose reduction when VCZ plasma concentrations approach 5.1 mg/L, a strategy that may significantly mitigate the risk of hepatotoxicity development or progression.
Emerging evidence suggests that the risk of adverse reactions to VCZ is influenced by multiple determinants, including plasma drug concentration, genetic polymorphisms, advanced age, gender, hepatic and renal dysfunction, drug-drug interactions, and administration routes.32,33 Research indicates that serum albumin levels can serve as a novel biomarker for VCZ clearance.34,35 Hypoalbuminemia may lead to an increase in the free drug concentration of VCZ, thereby elevating the risk of toxic adverse reactions.36 However, this study found no significant statistical difference in serum albumin levels between the hepatotoxicity and non-hepatotoxicity groups, and thus did not further explore the correlation between albumin and VCZ concentration. This result differs from previous literature reports, which may be attributed to the timely supplementary treatment of patients with decreased albumin levels in clinical practice. Notably, recent investigations have highlighted the critical role of systemic inflammation in modulating VCZ pharmacokinetics.37 A study by Zeng et al demonstrated that elevated PCT levels were significantly associated with VCZ-Cmin exceeding the therapeutic threshold of 5.5 mg/L.38 This finding was further corroborated by Cheng et al, who established a significant impact of PCT on VCZ-Cmin in geriatric populations.39 Moreover, Zhou et al quantified this relationship, revealing a significant positive correlation (P<0.05) between PCT levels and VCZ-Cmin, with each two-fold increase in PCT corresponding to a 0.21 mg/L elevation in VCZ-Cmin.40 Our study (Table 6) demonstrated a statistically significant disparity in initial VCZ-Cmin between patients exhibiting PCT levels≥0.835 ng/mL and those with PCT levels<0.835 ng/mL (P=0.005), suggesting that PCT levels may influence VCZ pharmacokinetics. Additionally, the PCT levels≥0.835 ng/mL exhibited a significantly higher incidence of hepatotoxicity compared to the group with PCT levels <0.835 ng/mL (P<0.001), indicating a potential correlation between elevated PCT levels and increased hepatotoxic risk. Logistic regression analysis confirmed elevated PCT levels as an independent risk factor for hepatotoxicity. The ROC curve analysis demonstrated that the AUC values of PCT and its combination with initial VCZ-Cmin were significantly higher than that of initial VCZ-Cmin alone. These findings indicate that PCT may serve as a potential biomarker for therapeutic drug monitoring during VCZ therapy, particularly exhibiting significant clinical application value in predicting VCZ-induced hepatotoxicity.
This investigation is subject to several limitations: Firstly, while CYP2C19 gene polymorphisms are known to influence VCZ pharmacokinetics, patient genotyping was not performed due to experimental constraints. Secondly, the study’s statistical power was constrained by a limited sample size, particularly the paucity of samples with low trough concentrations, which consequently precluded their inclusion in the analysis. Future research should incorporate prospective, large-scale, and multicenter study designs to further elucidate the relationship between initial VCZ-Cmin, PCT levels, and the incidence of hepatotoxicity in clinical populations.
Conclusion
In summary, this study investigated the association between initial VCZ-Cmin and PCT levels with VCZ-induced hepatotoxicity. The results indicated that VCZ-induced hepatotoxicity is the common adverse reaction, exhibiting significant associations with elevated initial VCZ-Cmin and increased PCT levels. Both the initial VCZ-Cmin and PCT level are independent risk factors, and either alone or in combination can predict the occurrence of hepatotoxicity. Among these, the predictive value of PCT level is the most significant. PCT level has a certain influence on the monitoring results of initial VCZ-Cmin. By monitoring VCZ-Cmin and PCT levels as well as their combined indicators, the predictive and diagnostic capabilities for hepatotoxicity can be enhanced, aiding in the identification of patients at risk of hepatotoxicity during VCZ treatment.
Data Sharing Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Ethics Statement
This study was conducted following the Declaration of Helsinki and was approved by the Ethical Committee of the Affiliated Huaian No. 1 People’s Hospital of Nanjing Medical University (Approval No. KY-2023-077-01). All patient data were analyzed in anonymity. Patient consent was waived by the ethics committee, as no individual data were published, nor was any intervention performed on patients.
Acknowledgment
The authors express their profound gratitude to Yu Du and Changchun Cao for their indispensable contributions to this investigation. Their technical proficiency was pivotal in the accurate quantification of VCZ trough concentrations, which constituted an essential methodological element of this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The work received financial supports from the Wu Jieping Medical Foundation Special Research Fund for Drug Therapy (Grant No.320.6750.2025-18-22).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Douglas AP, Smibert OC, Bajel A, et al. Consensus guidelines for the diagnosis and management of invasive aspergillosis, 2021. Intern Med J. 2021;51(S7):143–176. doi:10.1111/imj.15591
2. Hoenigl M, Salmanton-García J, Walsh TJ, et al. Global guideline for the diagnosis and management of rare mould infections: an initiative of the European Confederation of Medical Mycology in cooperation with the International Society for Human and Animal Mycology and the American Society for Microbiology. Lancet Infect Dis. 2021;21(8):e246–e257. doi:10.1016/S1473-3099(20)30784-2
3. Eiden C, Peyrière H, Cociglio M, et al. “Adverse effects of voriconazole: analysis of the French Pharmacovigilance Database. Annals Pharmacother. 2007;41(5):755–763. doi:10.1345/aph.1H671
4. Park WB, Kim NH, Kim KH, et al. The effect of therapeutic drug monitoring on safety and efficacy of voriconazole in invasive fungal infections: a randomized controlled trial. Clin Infect Dis. 2012;55(8):1080–1087. doi:10.1093/cid/cis599
5. Hamada Y, Ueda T, Miyazaki Y, et al. Effects of antifungal stewardship using therapeutic drug monitoring in voriconazole therapy on the prevention and control of hepatotoxicity and visual symptoms: a multicentre study conducted in Japan. Mycoses. 2020;63(8):779–786. doi:10.1111/myc.13129
6. Jin H, Wang T, Falcione BA, et al. Trough concentration of voriconazole and its relationship with efficacy and safety: a systematic review and meta-analysis. J Antimicrob Chemother. 2016;71(7):1772–1785. doi:10.1093/jac/dkw045
7. Hanai Y, Hamada Y, Kimura T, et al. Favorable effects of voriconazole trough concentrations exceeding 1 μg/mL on treatment success and all-cause mortality: a systematic review and meta-analysis. J Fungi. 2021;7(4):306. doi:10.3390/jof7040306
8. Wang T, Zhu H, Sun J, et al. Efficacy and safety of voriconazole and CYP2C19 polymorphism for optimised dosage regimens in patients with invasive fungal infections. Int J Antimicrob Agents. 2014;44(5):436–442. doi:10.1016/j.ijantimicag.2014.07.013
9. Wang Y, Wang T, Xie J, et al. Risk factors for voriconazole-associated hepatotoxicity in patients in the intensive care unit. Pharmacotherapy. 2016;36(7):757–765. doi:10.1002/phar.1779
10. Pascual A, Calandra T, Bolay S, Buclin T, Bille J, Marchetti O. Voriconazole therapeutic drug monitoring in patients with invasive mycoses improves efficacy and safety outcomes. Clin Infect Dis. 2008;46(2):201–211. doi:10.1086/524669
11. Zonios D, Yamazaki H, Murayama N, et al. Voriconazole metabolism, toxicity, and the effect of cytochrome P450 2C19 genotype. J Infect Dis. 2014;209(12):1941–1948. doi:10.1093/infdis/jiu017
12. Aitken AE, Morgan ET. Gene-specific effects of inflammatory cytokines on cytochrome P450 2C, 2B6 and 3A4 mRNA levels in human hepatocytes. Drug Metab Dispos. 2007;35(9):1687–1693. doi:10.1124/dmd.107.015511
13. Aitken AE, Richardson TA, Morgan ET. Regulation of drug-metabolizing enzymes and transporters in inflammation. Annu Rev Pharmacol Toxicol. 2006;46:123–149. doi:10.1146/annurev.pharmtox.46.120604.141059
14. Renton KW. Cytochrome P450 regulation and drug biotransformation during inflammation and infection. Curr Drug Metab. 2004;5(3):235–243. doi:10.2174/1389200043335559
15. van Wanrooy MJ, Span LF, Rodgers MG, et al. Inflammation is associated with voriconazole trough concentrations. Antimicrob Agents Chemother. 2014;58(12):7098–7101. doi:10.1128/AAC.03820-14
16. Encalada Ventura MA, Span LF, van den Heuvel ER, Groothuis GM, Alffenaar JW. Influence of inflammation on voriconazole metabolism. Antimicrob Agents Chemother. 2015;59(5):2942–2943. doi:10.1128/AAC.04789-14
17. Yunus I, Fasih A, Wang Y. The use of procalcitonin in the determination of severity of sepsis, patient outcomes and infection characteristics. PLoS One. 2018;13(11):e0206527. doi:10.1371/journal.pone.0206527
18. Danan G, Teschke R. RUCAM in drug and herb induced liver injury: the update. Int J Mol Sci. 2015;17(1):14. doi:10.3390/ijms17010014
19. Wang T, Miao L, Shao H, et al. Voriconazole therapeutic drug monitoring and hepatotoxicity in critically ill patients: a nationwide multi-centre retrospective study. Int J Antimicrob Agents. 2022;60(5–6):106692. doi:10.1016/j.ijantimicag.2022.106692
20. Department of Health and Human Services. Common Terminology Criteria for Adverse Events (CTCAE) Version 5.0[R]. Bethesda: NIH; 2017.
21. Purkins L, Wood N, Ghahramani P, Greenhalgh K, Allen MJ, Kleinermans D. Pharmacokinetics and safety of voriconazole following intravenous- to oral-dose escalation regimens. Antimicrob Agents Chemother. 2002;46(8):2546–2553. doi:10.1128/AAC.46.8.2546-2553.2002
22. VFEND (voriconazole) for injection, tablets, and oral suspension [prescribing information]. Silver Spring, MD: U.S. Food and Drug Administration; 2019. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/021266s039,021267s050,021630s029lbl.pdf.
23. Zubiaur P, Kneller LA, Ochoa D, et al. Evaluation of voriconazole CYP2C19 phenotype-guided dose adjustments by physiologically based pharmacokinetic modeling. Clin Pharmacokinet. 2021;60(2):261–270. doi:10.1007/s40262-020-00941-8
24. Racil Z, Winterova J, Kouba M, et al. “Monitoring trough voriconazole plasma concentrations in haematological patients: real life multicentre experience. Mycoses. 2012;55(6):483–492. doi:10.1111/j.1439-0507.2012.02186.x
25. Saito T, Fujiuchi S, Tao Y, et al. Efficacy and safety of voriconazole in the treatment of chronic pulmonary aspergillosis: experience in Japan. Infection. 2012;40(6):661–667. doi:10.1007/s15010-012-0322-x
26. Luong ML, Hosseini-Moghaddam SM, Singer LG, et al. Risk factors for voriconazole hepatotoxicity at 12 weeks in lung transplant recipients. Am J Transplant. 2012;12(7):1929–1935. doi:10.1111/j.1600-6143.2012.04042.x
27. Xing Y, Chen L, Feng Y, Zhai Y, Zhou Y, Lu J. Meta-analysis of the safety of voriconazole in definitive, empirical, and prophylactic therapies for invasive fungal infections. BMC Infect Dis. 2017;17(1):798. doi:10.1186/s12879-017-2913-8
28. Shi CC, Li QY, Lin NM. Research advances on the correlation between voriconazole blood concentration and clinical efficacy and safety. Chin J Nosocomiol. 2017;27(4):957–960. doi:10.11816/cn.ni.2016-162645
29. Shen K, Gu Y, Wang Y, et al. Therapeutic drug monitoring and safety evaluation of voriconazole in the treatment of pulmonary fungal diseases. Ther Adv Drug Saf. 2022;13:20420986221127503. doi:10.1177/20420986221127503
30. Takesue Y, Hanai Y, Oda K, et al. Clinical practice guideline for the therapeutic drug monitoring of voriconazole in Non-Asian and Asian adult patients: consensus review by the Japanese Society of Chemotherapy and the Japanese Society of Therapeutic Drug Monitoring. Clin Ther. 2022;44(12):1604–1623. doi:10.1016/j.clinthera.2022.10.005
31. Chen K, Zhang X, Ke X, Du G, Yang K, Zhai S. Individualized medication of voriconazole: a practice guideline of the division of therapeutic drug monitoring, chinese pharmacological society. Ther Drug Monit. 2018;40(6):663–674. doi:10.1097/FTD.0000000000000561
32. Weiss J, Ten Hoevel MM, Burhenne J, et al. CYP2C19 genotype is a major factor contributing to the highly variable pharmacokinetics of voriconazole. J Clin Pharmacol. 2009;49(2):196–204. doi:10.1177/0091270008327537
33. Chu HY, Jain R, Xie H, Pottinger P, Fredricks DN. Voriconazole therapeutic drug monitoring: retrospective cohort study of the relationship to clinical outcomes and adverse events. BMC Infect Dis. 2013;13:105. doi:10.1186/1471-2334-13-105
34. Chantharit P, Tantasawat M, Kasai H, Tanigawara Y. Population pharmacokinetics of voriconazole in patients with invasive aspergillosis: serum albumin level as a novel marker for clearance and dosage optimization. Ther Drug Monit. 2020;42(6):872–879. doi:10.1097/FTD.0000000000000799
35. Khan-Asa B, Punyawudho B, Singkham N, et al. Impact of albumin and omeprazole on steady-state population pharmacokinetics of voriconazole and development of a voriconazole dosing optimization model in Thai patients with hematologic diseases. Antibiotics. 2020;9(9):574. doi:10.3390/antibiotics9090574
36. Vanstraelen K, Wauters J, Vercammen I, et al. Impact of hypoalbuminemia on voriconazole pharmacokinetics in critically ill adult patients. Antimicrob Agents Chemother. 2014;58(11):6782–6789. doi:10.1128/AAC.03641-14
37. Li X, Lai F, Jiang Z, et al. Effects of inflammation on voriconazole levels: a systematic review. Br J Clin Pharmacol. 2022;88(12):5166–5182. doi:10.1111/bcp.15495
38. Zeng G, Wang L, Shi L, et al. Variability of voriconazole concentrations in patients with hematopoietic stem cell transplantation and hematological malignancies: influence of loading dose, procalcitonin, and pregnane X receptor polymorphisms. Eur J Clin Pharmacol. 2020;76(4):515–523. doi:10.1007/s00228-020-02831-1
39. Cheng L, Xiang R, Liu F, et al. Therapeutic drug monitoring and safety of voriconazole in elderly patients. Int Immunopharmacol. 2020;78:106078. doi:10.1016/j.intimp.2019.106078
40. Zhou JX, Xiong CL, Chang ZS, et al. Association of procalcitonin with voriconazole concentrations: a retrospective cohort study. BMC Infect Dis. 2024;24(1):952. doi:10.1186/s12879-024-09862-4
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.