Back to Journals » International Journal of Women's Health » Volume 18
The Positive Association Between RCII and Endometriosis and Its Integration into a Clinical Predictive Model: A Cross-Sectional Study
Authors Wu H, Shan F, Ye M, Zhou H ![]() , Jiao J, Zhong Z, Wu Y
, Jiao J, Zhong Z, Wu Y ![]()
Received 18 September 2025
Accepted for publication 25 December 2025
Published 8 January 2026 Volume 2026:18 568706
DOI https://doi.org/10.2147/IJWH.S568706
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Vinay Kumar
Haochan Wu,1,* Fangfang Shan,1,* Mengmeng Ye,1 Hui Zhou,1,2 Jie Jiao,3 Zhaoxia Zhong,4 Yibo Wu1,2
1Human Reproductive Medicine Center, Affiliated Hospital of Jiangnan University, Wuxi, People’s Republic of China; 2Human Genetic and Reproduction Center, Affiliated Hospital of Jiangnan University, Wuxi, People’s Republic of China; 3Department of Obstetrics and Gynecology, Affiliated Hospital of Jiangnan University, Wuxi, People’s Republic of China; 4Department of Obstetrics and Gynecology, Donghai People’s Hospital, Donghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yibo Wu, Affiliated Hospital of Jiangnan University, Wuxi, People’s Republic of China, Email [email protected] Zhaoxia Zhong, Department of Obstetrics and Gynecology, Donghai People’s Hospital, 299Fuguo Road, Donghai, Donghai, People’s Republic of China, Email [email protected]
Introduction: Studies indicate that endometriosis (EMs) is associated with inflammation and metabolic abnormalities. The Remnant Cholesterol Inflammatory Index (RCII) concurrently reflects both inflammatory and metabolic status. However, the relationship between RCII and EMs remains unclear. Therefore, this study aims to investigate the association between RCII and EMs and explore the potential of RCII as a risk predictor for EMs.
Methods: Making use of information from the 1999– 2006 NHANES database, we investigated the connection between natural logarithm-transformed RCII (lnRCII) and EMs employing logistic regression analysis, restricted cubic spline (RCS) models, and subgroup analysis approaches. Finally, a nomogram was constructed based on feature variables selected via LASSO regression to enhance the interpretability of the predictive model.
Results: After adjusting for potential confounding factors, lnRCII demonstrated a substantial positive correlation with the risk of EMs. For each 1-standard-deviation increase in lnRCII, the EMs’ risk increased by 25% (fully adjusted model OR = 1.250, 95% CI: 1.266– 1.461, P = 0.006). Furthermore, a linear relationship between lnRCII and EMS was observed via RCS analysis. According to subgroup analysis, the relationship between lnRCII and EMS has a consistent association across the majority of the population. (P for interaction > 0.05).
Conclusion: In the US population, RCII was substantially linked to a higher risk of EMs, suggesting that the lipid metabolism-inflammation axis may represent a potential target for intervention in the prevention or treatment of EMs.
Keywords: remnant cholesterol inflammatory index, endometriosis, cross-sectional study, NHANES
Introduction
Endometriosis(EMs) is a chronic condition that severely impacts female reproductive health, pathologically characterized by ectopic development of endometrial cells outside the uterus.1 Endometrium-like tissues may proliferate in extrauterine sites such as ovaries, fallopian tubes, and other pelvic structures, forming cysts or scar tissue.2 This pathological process can further trigger complications, including ovarian cancer.3,4 Research shows that 190 million women of childbearing age are affected by EMs, which have a prevalence of 5% to 10%.5 Among affected women, 50–70% experience pelvic pain and 30–50% develop infertility.6 This severely impacts quality of life and mental health, posing a substantial burden on global health.7,8 Direct laparoscopic sight of lesions, followed by histological confirmation, is still the gold standard for diagnosing endometriosis.9 However, as this is an invasive procedure, most patients do not receive a diagnosis until around 7 to 8 years after the onset of symptoms, which may result in infertility and the advancement of the condition.10 Therefore, identifying its associated risk factors and investigating easily accessible biomarkers are crucial for the early diagnosis and treatment of EMs.
In recent years, the relationship between lipid metabolism and inflammation in various diseases has garnered widespread attention. Studies indicate that remnant cholesterol is closely associated with atherosclerosis, inflammatory status, and the risk of systemic diseases.11,12 In EMs research, cholesterol and its related biomarkers are considered potentially significant in the onset and progression of this disease.13,14 Existing research has demonstrated that elevated remnant cholesterol(RC) levels may be associated with the development and progression of endometriosis.15 Furthermore, inflammatory indicators such as high-sensitivity C-reactive protein (hs-CRP) and neutrophil-to-lymphocyte ratio have increasingly revealed clinical relevance in endometriosis studies.16,17 This may be related to the promotion of lesion proliferation, invasion, and neurovascular network formation through the induction of vascular endothelial growth factor (VEGF) expression in ectopic endometrium by cholesterol metabolism and inflammation, as angiogenesis is a fundamental mechanism for the growth and maintenance of endometrioma lesions.18–20
Although previous research has looked into the relationship between cholesterol metabolism, inflammatory indicators and EMs, the Residual Cholesterol Inflammation Index (RCII) as a predictive risk factor for endometriosis remains unexplored. The RCII has been demonstrated to be associated with metabolic syndrome, the occurrence of cardiovascular diseases, and related mortality.21,22 RCII is not a simple composite index; its design is based on a clear pathophysiological mechanism through which RC promotes inflammation. This mechanism includes phagocytosis by macrophages to form foam cells, activation of inflammasomes (such as NLRP3), and increased oxidative stress leading to an inflammatory state.23,24 Systemic inflammation, in turn, results in elevated inflammatory markers (such as C-reactive protein). Therefore, RCII is designed to reflect the synergistic or amplifying effect between lipid abnormalities and systemic inflammatory response, offering greater integrative and pathophysiological significance than using RC or CRP alone. EMs is widely recognized as a chronic inflammatory disease, characterized by extensive infiltration of inflammatory cells and high expression of pro-inflammatory factors (such as TNF-α, IL-1β, IL-6) in the peritoneal microenvironment and local lesions.25 RC contributes to inflammation by increasing oxidized lipid products and may also influence estrogen metabolism, which plays a key role in EMs.26 Consequently, we propose that the RCII metric is well-suited to capture this coexisting state of high lipids and high inflammation, potentially serving as an effective biomarker for identifying the risk or severity of EMs. Evaluating the relationship between RCII and EMs will provide novel insights for early diagnosis and intervention of this disease. Therefore, the purpose of this study is to look at the relationship between the RCII and the risk of EMs.
Methods
Study Population
The National Health and Nutrition Examination Survey (NHANES) database was used in the analysis of this study. Since 1999, NHANES has routinely gathered nutritional and health information from Americans, encompassing demographics, anthropometric measurements, laboratory indicators, dietary habits, and health status. The database features substantial volume and high authenticity. NHANES collects data using a stratified, multistage probability sampling technique to guarantee national representativeness. We included women aged 20 to 54 years from the 1999–2006 cycles who were diagnosed with EMs through self-report or ICD codes, and who had complete lipid profile and inflammatory marker data. By excluding participants with incomplete data, we ensured the accuracy and representativeness of the study population. Ultimately, 2,316 qualified subjects were included, comprising 2,145 in the non-EMs group and 171 in the EMs group. The inclusion process is illustrated in Figure 1. Following the NHANES study protocol, which was authorized by the National Center for Health Statistics’ (NCHS) Research Ethics Review Board, each participant gave written informed consent.
 |
Figure 1 A flowchart illustrating the screening process for selecting endometriosis participants. |
Exposure and Outcome Variables
The variable related to exposure in this investigation was the RCII, calculated using the formula: RCII = [TC - (HDL-C + LDL-C)] (mg/dL) × hsCRP (mg/L)/10.27 Because of the skewed distribution of RCII, a natural logarithmic transformation was applied to obtain lnRCII (Figure 2). All subsequent statistical analyses were based on this transformed variable. All hematological and biochemical parameters in RCII were measured in participants after a fasting period of at least 9 hours. Enzymatic assays were used to directly measure serum total cholesterol and triglycerides, whereas serum HDL-C was measured via direct immunoassays or enzymatic assays following serum depletion of apolipoprotein B-containing lipoproteins using heparin-Mn2+ precipitation. LDL-C was estimated using the Friedewald equation: LDL-C=TC−HDL-C−TG/5 (mg/dL). C-reactive protein was measured by a latex-enhanced solution method. Detailed specimen collection and processing instructions are described in the NHANES Laboratory/Medical Technologists Procedures Manual (LPM). The outcome variable in this study was endometriosis (EMs). Data were obtained through questionnaires, where participants answering “YES” to “Told by doctor had endometriosis?” were classified as having EMs.28
 |
Figure 2 Distribution of RCII before ((a)RCII) and after ((b)InRCII) natural log transformation. |
Covariates
Beyond laboratory indicators related to RCII, we collected additional covariates including: demographic information (age, race, educational background, status in marriage, household income), smoking status, alcohol consumption, body mass index (BMI), triglycerides, fasting blood glucose (FBG), insulin, glycated hemoglobin, age at menarche, menstrual regularity, and clinical chronic diseases (diabetes, hypertension, dyslipidemia). Data on comorbidity were collected through self-reported surveys. Three groups were identified based on smoking status: never smokers (less than 100 cigarettes), past smokers (those who had smoked more than 100 cigarettes but do not smoke now), and current smokers (those who have smoked more than 100 cigarettes and smoke regularly or sometimes). Alcohol intake was defined as consuming 12 or more drinks during one’s lifetime, with relevant data obtainable from the file labelled “ALQ”.
Statistical Methods
In this research, we grouped participants according to their status of endometriosis diagnosis. For continuous variables, weighted Student’s t-tests were employed, and for the data with categories, we used weighted chi-square tests. Categorical variables are displayed as proportions, while continuous variables are expressed as mean and standard deviation. We investigated the association between the natural logarithm-transformed RCII (lnRCII) and EMS using weighted logistic regression analysis and multivariate modelling. Three logistic regression models were constructed with progressive adjustments for different confounding factors: Model 1 adjusted for no confounding factors; Model 2 adjusted for age, race, education level, marital status, and income level; Model 3 adjusted for all variables except C-reactive protein, total cholesterol, low-density lipoprotein cholesterol, and high-density lipoprotein cholesterol. We employed restricted cubic spline (RCS) models to visualize the dose-response connection between lnRCII and EMS. Subgroup analysis was conducted to assess the robustness of the relationship between lnRCII and EMs. Furthermore, the Least Absolute Shrinkage and Selection Operator (LASSO) regression model was employed to screen 15 feature variables. Finally, a nomogram was constructed based on the selected 15 variables to enhance the interpretability of the predictive model outcomes.
All statistical analyses were conducted using the DecisionLinnc1.0 software—an intelligent platform supporting multilingual scripting (eg, Python, R, Java, C++) with cloud computing capabilities.29 Its core functionalities encompass data processing, analytical operations, and visualization. Following the Centers for Disease Control and Prevention’s recommendations and considering the complex, multistage, clustered design of NHANES, all statistical analyses employed fasting subsample weights to ensure national representativeness.
Results
Baseline Characteristics
Table 1 presents the demographic characteristics and health information of the study participants. This study included 2,316 participants, comprising 171 EMs patients and 2,145 non-EMs individuals. The results indicated that the differences between the EMs and non-EMs were statistically significant (p<0.05) regarding age, race, education level, cholesterol, triglycerides, C-reactive protein, menstrual regularity, hyperlipidemia, smoking status, and InRCII.
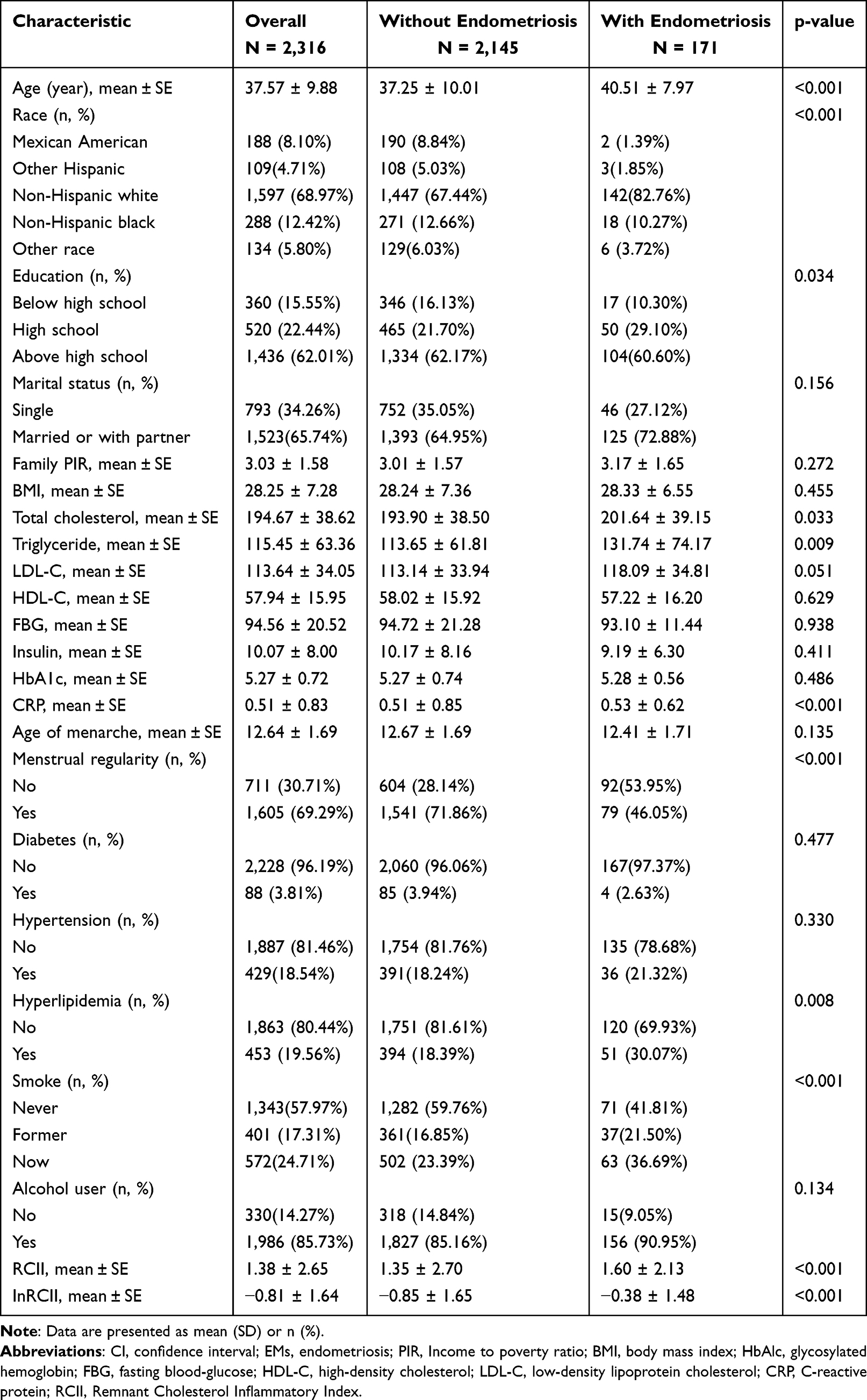 |
Table 1 Baseline Characteristics of Women Participants from the NHANES 1999–2006, Weighted |
Association Between InRCII and EMs
The correlation between InRCII and EMs was analyzed using weighted logistic regression, with results presented in Table 2. When analyzing InRCII as a continuous variable, we observed increased EMs risk with rising InRCII across all three models (Unadjusted model: OR = 1.200, 95% CI [1.090, 1.321], P = 0.001; Partially adjusted model: OR = 1.203, 95% CI [1.088, 1.330], P = 0.001; Fully adjusted model: OR = 1.250, 95% CI [1.070, 1.461], P = 0.006). This association remained statistically significant after converting InRCII to categorical tertiles. In the fully adjusted model, individuals in T3 exhibited a 120.6% higher likelihood of developing EMs (OR = 2.206, 95% CI [1.266, 3.845], P = 0.007). Additionally, the trend test showed statistical significance (P for trend = 0.006). Restricted cubic spline analysis in Figure 3 further revealed a linear positive correlation between InRCII and EMs (P overall = 0.001; P for non-linearity = 0.239).
 |
Table 2 Weighted Logistic Regression Analysis of InRCII and EMs |
 |
Figure 3 Dose-Response Relationship Between InRCII and EMs. |
Subgroup Analysis
We conducted subgroup studies to evaluate the stability of the relationship between InRCII and EMs across different populations. As shown in Figure 4, the results indicate that the positive correlation between InRCII and EMs persists regardless of stratification by age, race, education level, income, marital status, smoking, alcohol consumption, hypertension, hyperlipidemia, diabetes, or menstrual regularity (P for interaction > 0.05).
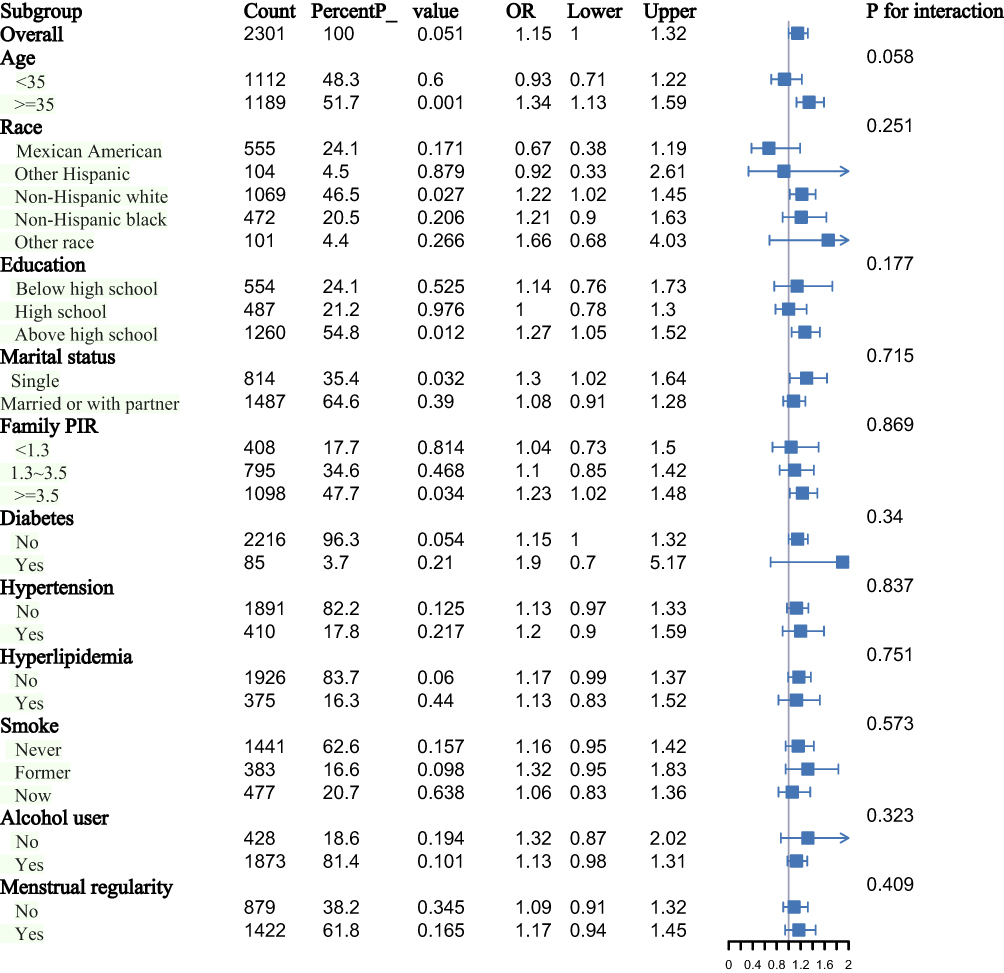 |
Figure 4 Forest plot of subgroup analysis for relationships between InRCII and EMs. |
Construction of Predictive Models
In this study, LASSO regression was employed to screen for significant variables. As illustrated in Figure 5, 15 variables were ultimately identified: age, race, education level, marital status, family income level, fasting glucose, insulin, triglycerides, smoking status, alcohol consumption, diabetes, hyperlipidemia, age at menarche, and menstrual regularity. Based on these 15 identified risk factors, a nomogram was developed in Figure 6. By summing the points corresponding to each variable characteristic, the probability of EMs occurrence can be estimated.
 |
Figure 5 LASSO penalized regression analysis was used to identify factors associated with EMs (a) Cross Validation Error (CVM) plot for different Log Lambda values. (b) The coefficient trajectory for each variable as Log Lambda changes. |
 |
Figure 6 Nomograms for EMs risk prediction. |
Discussion
This study involving 2,316 participants demonstrates a significant positive association between InRCII and EMs. In particular, a 25% increased risk of EMs was linked to every 1-standard-deviation rise in InRCII, and this relationship remained independent of other risk factors. RCS analysis revealed a linear association between lnRCII and EMs. Subgroup analysis demonstrated the stability of this association across diverse populations. Relevant variables were then screened using the LASSO regression model. Using the significant factors that were found, a nomogram prediction model was constructed. This model is not merely a simple statistical tool. First, the key variables included in this nomogram were selected through LASSO regression, which helps avoid directly incorporating a large number of potentially irrelevant or collinear variables into the final model. Second, InRCII remained in the model after LASSO screening, providing preliminary evidence that it is an independent influencing factor for endometrioma even when numerous competing factors are considered. Furthermore, this model quantifies the independent contribution of each screened risk factor. Most importantly, the nomogram visualizes the complex regression equation, allowing clinicians or researchers to assign points based on specific variable values of individual patients (such as InRCII level, age, etc.) and intuitively observe the predicted probability of EMs for that individual. This significantly enhances the model’s interpretability and potential convenience for clinical application.
EMs is a gynecological disorder characterized by estrogen dependency and chronic inflammatory features. Its fundamental pathology manifests as functional endometrial tissue occurring outside the uterine cavity, such as in the ovaries, fallopian tubes, and peritoneum.30 Its development may involve interactions among multiple contributing factors. Before this, numerous studies utilizing the NHANES database have investigated risk factors associated with EMs. Results consistently demonstrate that inflammation and metabolism play crucial roles in the pathogenesis and progression of EMs. For instance, Chen et al revealed an association between EMs and remnant cholesterol (RC), advising that cholesterol metabolism status should be monitored in EMs patients.15 The dietary inflammatory index and EMs were found to be related by Hu et al, indicating that non-pharmacological methods may lessen or enhance EMs symptoms.31 Consequently, the RCII, which integrates markers of cholesterol metabolism and inflammation, not only reflects lipid metabolic imbalance but also serves as a composite index of chronic inflammatory status. It likely possesses stronger predictive capability than individual lipid or inflammatory markers and has been employed to assess risks for cardiovascular diseases.22,27 The results of this investigation confirm that lnRCII is a reliable risk biomarker for EMs. Although lnRCII may serve as a promising biomarker for predicting EMs, the specific biological mechanisms underlying this association remain incompletely understood. According to current research, the observed positive association between lnRCII levels and EMs can be explained by several possible processes. These mechanisms primarily involve ectopic endometrial implantation and invasiveness, local and systemic inflammatory microenvironments, hormonal dysregulation (eg, estrogen hypersensitivity), immune evasion accompanied by reduced natural killer cell activity, and neuroendocrine dysfunction.32–37
Studies indicate that both cholesterol metabolism and inflammatory responses play crucial roles in numerous pathological conditions, particularly in autoimmune and endocrine-related disorders. Literature reports that peritoneal fluid from EMs patients is rich in inflammatory cytokines (eg, IL-1β, IL-6, TNF-α), chemokines (eg, MCP-1, RANTES), oxidative stress products, and bioactive lipid molecules (eg, prostaglandins).25 These substances participate in local endometrial cell adhesion, invasion, angiogenesis and neurogenesis.38 Research indicates that abnormal cholesterol metabolism may influence the development of endometriosis by promoting chronic inflammation.39 For instance, cholesterol accumulation can activate the immune system, triggering cytokine release and thereby exacerbating inflammatory responses.40,41 This occurs because cholesterol metabolism disorders affect the functionality of macrophages, dendritic cells, and NK cells, impairing their ability to recognize and clear ectopic endometrial cells.42 Animal experiments further demonstrate that endometrial lesions in the peritoneal cavity of high-fat diet mice were larger than those in normal-diet controls.43 Immunohistochemistry revealed extensive infiltration of macrophages within the lesions, accompanied by abundant oxidized lipid deposits.44,45 Cholesterol serves as a key precursor for steroid hormone synthesis, such as estrogen. In EMs patients, the inflammatory microenvironment induces increased aromatase activity, which facilitates the metabolism of cholesterol into estrogen.46 This process activates the ERK1/2 signalling pathway, thereby promoting the proliferation and invasion of ectopic endometrial tissue.47 Additionally, non-HDL-C components (such as LDL-C and VLDL-C) are prone to oxidation into oxLDL, and these oxidized forms bind to TLR4 receptors, activating both the NF-κB signalling pathway and the NLRP3 inflammasome pathway.48 Such lipid signalling molecules enhance inflammatory responses and facilitate immune escape within the ectopic lesions of endometriosis.49 Decreased HDL-C levels often trigger subsequent inflammation, whereby inflammatory factors (eg, IL-1β, VEGF) activate vascular endothelial cells and nerve growth factor expression, thereby promoting lesion persistence.50,51 In summary, elevated RCII levels indicate a state of potential immune tolerance in individuals, creating an immunoprotective environment conducive to the implantation, invasion, and sustained survival of endometriotic lesions.
Together, these findings demonstrate the intricate relationship that exists between metabolic dysregulation, inflammation and EMs. RCII provides a more comprehensive risk prediction by combining RC and CRP/hsCRP. The application of machine learning facilitates a thorough evaluation of RCII’s predictive performance. From a clinical application perspective, the InRCII addresses critical limitations of existing diagnostic and risk assessment tools. While imaging examinations such as laparoscopy serve as the gold standard, they are invasive, costly, and associated with low patient compliance, making them unsuitable for large-scale screening in the general population. Serum biomarkers like CA125 suffer from insufficient specificity and are susceptible to interference from benign gynecological conditions. In contrast, the lipid and inflammatory indicators involved in the InRCII are readily obtainable, offering the advantages of being non-invasive, low-cost, and easy to perform, thereby demonstrating strong clinical applicability. Based on the findings of this study, which confirmed a significantly elevated risk of disease onset in the high-InRCII group, this index can be applied for primary screening in the general population of women of reproductive age. It enables the rapid identification of high-risk individuals and guides further clinical examinations, thereby improving early diagnosis efficiency and reducing disease burden. Additionally, RCII can be utilized for monitoring therapeutic efficacy and assessing disease progression in EMs. Given the established link between residual cholesterol and cardiovascular risk, our findings suggest that EMs patients with elevated RCII may require concurrent monitoring of their metabolic health. First and foremost, because it is a cross-sectional research, it is unable to determine if higher RCII causes or results from EMs. Secondly, the diagnosis of EMs was obtained from NHANES participants via self-reported questionnaires, which may introduce misinformation. Additionally, we failed to take into consideration confounding variables that may skew the results, such as physical activity and prior pelvic surgery.
Before clinical application, prospective cohort studies are required to further validate the reliability of RCII in predicting endometrioma (EMs) and to evaluate its predictive accuracy, clinical utility, and cost-effectiveness as a potential target for public health interventions. A large-sample, multi-center cohort study could be established to collect RCII levels from diverse populations and EMs patients at different disease stages. This would facilitate the creation of a longitudinal tracking database to clarify relationships between RCII and clinical indicators, including disease severity, pain scores, and recurrence rates. Integrating RCII with biomarkers such as CA125, VEGF, IL-6, and miRNA to establish multi-indicator prediction models can enhance diagnostic specificity and sensitivity. If subsequent validation confirms favourable predictive performance of RCII, consideration could be given to incorporating it into routine gynecological examinations for women, particularly for high-risk populations with a history of dysmenorrhea or infertility.
Conclusion
This cross-sectional investigation shows a strong correlation between the risk of EMs and high RCII levels. And we utilized machine learning methods for model prediction. These findings indicate that RCII holds promise as a potential biomarker for EMs, offering new avenues for future diagnosis, treatment, and personalized risk prediction of EMs with broad application prospects. But large-scale prospective cohort studies are necessary before considering the application of RCII in clinical practice.
Abbreviations
NHANES, National Health and Nutrition Examination Survey; RCII, Remnant Cholesterol Inflammatory Index; EMs, Endometriosis; FPG, Fasting blood-glucose; HbA1c, Glycosylated hemoglobin; PIR, Income to poverty ratio; HDL-C, High-density cholesterol; LDL-C, Low-density lipoprotein cholesterol; CRP, C-reactive protein; LASSO, Least absolute shrinkage and selection operator; RCS, Restricted cubic spline; OR, Odds ratio; CI, Confidential interval; ML, Machine learning.
Data Sharing Statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found below: https://www.cdc.gov/nches/nhanes.
Ethics Approval and Consent to Participate
The study was approved by the Institutional Review Board of the CDC’s National Center for Health Statistics, and all participants provided written informed consent. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. All analyses were conducted in accordance with NHANES guidelines (https://www.cdc.gov/nchs/nhanes/irba98.htm) with written informed consent given by all participants and ethical approval granted by the NCHS research ethics review board (https://www.cdc.gov/nchs/nhanes/about/erb.html).
According to item 1 (conducting research using legally obtained public data or data generated through observation without interfering with public behavior) and 2 (conducting research using anonymized information data) of Article 32 of the Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects dated February 18, 2023, China, this research is exempt from ethical review.
Acknowledgments
Haochan Wu and Fangfang Shan are co-first authors for this study. The authors express their gratitude towards the participants and staff of the NHANES database for their noteworthy contributions.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Informed Consent Statement
All participants provided informed consent during the data collection process by the NHANES protocol.
Funding
This project was supported by the Wu Jieping Medical Foundation (320.6750.2024-6-100) and the General Project of Wuxi Health Commission (M202408, M202418).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Taylor HS, Kotlyar AM, Flores VA. Endometriosis is a chronic systemic disease: clinical challenges and novel innovations. Lancet. 2021;397(10276):839–13. doi:10.1016/S0140-6736(21)00389-5
2. Chapron C, Marcellin L, Borghese B, Santulli P. Rethinking mechanisms, diagnosis and management of endometriosis. Nat Rev Endocrinol. 2019;15(11):666–682. doi:10.1038/s41574-019-0245-z
3. Yoldemir T. Evaluation and management of endometriosis. Climacteric. 2023;26(3):248–255. doi:10.1080/13697137.2023.2190882
4. McHale MT. New insights in endometriosis subtypes and ovarian cancer risk. JAMA. 2024;332(6):460–461. doi:10.1001/jama.2024.12357
5. Ellis K, Munro D, Clarke J. Endometriosis is undervalued: a call to action. Front Glob Womens Health. 2022;3:902371. doi:10.3389/fgwh.2022.902371
6. U LRM, Chiappa V, Ceccaroni M, et al. Epidemiology of infertility in women with endometriosis. Best Pract Res Clin Obstet Gynaecol. 2024;92:102454. doi:10.1016/j.bpobgyn.2023.102454
7. Koller D, Pathak GA, Wendt FR, et al. Epidemiologic and genetic associations of endometriosis with depression, anxiety, and eating disorders. JAMA Netw Open. 2023;6(1):e2251214. doi:10.1001/jamanetworkopen.2022.51214
8. Eisenberg VH, Decter DH, Chodick G, Shalev V, Weil C. Burden of endometriosis: infertility, comorbidities, and healthcare resource utilization. J Clin Med. 2022;11(4):1133. doi:10.3390/jcm11041133
9. Agarwal SK, Chapron C, Giudice LC, et al. Clinical diagnosis of endometriosis: a call to action. Am J Obstet Gynecol. 2019;220(4):354.e1–354.e12. doi:10.1016/j.ajog.2018.12.039
10. Ghai V, Jan H, Shakir F, Haines P, Kent A. Diagnostic delay for superficial and deep endometriosis in the United Kingdom. J Obstet Gynaecol. 2020;40(1):83–89. doi:10.1080/01443615.2019.1603217
11. Deng YQ, Tang MH, Zhang KX, et al. Association between remnant cholesterol and the risk of atherosclerotic cardiovascular disease in a community population in Shanghai. Zhonghua Liu Xing Bing Xue Za Zhi. 2025;46(6):935–941. doi:10.3760/cma.j.cn112338-20241018-00641
12. Kraaijenhof JM, Kerkvliet MJ, Nurmohamed NS, et al. The role of systemic inflammation in remnant cholesterol associated cardiovascular risk: insights from the EPIC-Norfolk study. Eur J Prev Cardiol. 2025:zwaf037. doi10.1093/eurjpc/zwaf037.
13. Jiang P, Zhang X, Huang H, Sun Z, Hu W, Li Y. Study on the relationship between the non-HDL/HDL cholesterol ratio (NHHR) and endometriosis: a cross-sectional analysis utilizing the NHANES dataset. Lipids Health Dis. 2025;24(1):179. doi:10.1186/s12944-025-02590-x
14. Zhou G, Ren J, Huang Q, et al. Gene associations of lipid traits, lipid-lowering drug-target genes and endometriosis. Reprod Biomed Online. 2024;49(1):103856. doi:10.1016/j.rbmo.2024.103856
15. Chen Z, Li R, Guo J, Ye X, Zhou Y, Cao M. Association between remnant cholesterol (RC) and endometriosis: a cross-sectional study based on NHANES data. Lipids Health Dis. 2025;24:2. doi:10.1186/s12944-024-02422-4
16. Verit FF, Hilali NG. Comparing high-sensitivity C-reactive protein (hs-CRP) with CRP as a soluble serum marker for the diagnosis of women with endometriosis. Fertil Steril. 2010;94(3):e51. doi:10.1016/j.fertnstert.2010.05.038
17. Gorun OM, Ratiu A, Citu C, et al. The role of inflammatory markers NLR and PLR in predicting pelvic pain in endometriosis. J Clin Med. 2024;14(1):149. doi:10.3390/jcm14010149
18. Ates C, Dilbaz B, Ergani SY, Atabay F. The effect of antiangiogenic agent aflibercept on surgically induced endometriosis in a rat model. Cir Cir. 2024;92(1):10–19. doi:10.24875/CIRU.23000072
19. Ma C, Huang W, Wang H, et al. Oxidized LDL promotes EMS-induced angiogenesis by increasing VEGF-A expression and secretion by endometrial cells. Mol Med. 2022;28(1):151. doi:10.1186/s10020-022-00582-6
20. Anvari Aliabad R, Hassanpour K, Norooznezhad AH. Cannabidiol as a possible treatment for endometriosis through suppression of inflammation and angiogenesis. Immun Inflamm Dis. 2024;12(8):e1370. doi:10.1002/iid3.1370
21. Chen X, Chen J, Gong H, Fan Y, Luo Y. Association of Remnant Cholesterol Inflammation Index as potential marker of metabolic syndrome: a cross-sectional study from NHANES and CHARLS. Medicine. 2025;104(46):e46052. doi:10.1097/MD.0000000000046052
22. Wang Y, Bi L, Li Q, Wang Q, Lv T, Zhang P. Remnant cholesterol inflammatory index and its association with all-cause and cause-specific mortality in middle-aged and elderly populations: evidence from US and Chinese national population surveys. Lipids Health Dis. 2025;24:155. doi:10.1186/s12944-025-02580-z
23. Ding Y, Gong W, Zhang S, et al. Protective role of sirtuin3 against oxidative stress and NLRP3 inflammasome in cholesterol accumulation and foam cell formation of macrophages with ox-LDL-stimulation. Biochem Pharmacol. 2021;192:114665. doi:10.1016/j.bcp.2021.114665
24. Karel P, Barbora M, Hana B, et al. Human macrophage pro-inflammatory polarization in response to free cholesterol and cholesterol remnants. Physiol Rep. 2025;13(10):e70367. doi:10.14814/phy2.70367
25. Monsanto SP, Edwards AK, Zhou J, et al. Surgical removal of endometriotic lesions alters local and systemic proinflammatory cytokines in endometriosis patients. Fertil Sterility. 2016;105(4):968–977.e5. doi:10.1016/j.fertnstert.2015.11.047
26. Wu R, Li F, Wang S, et al. Epigenetic programming of estrogen receptor in adipocytes by high-fat diet regulates obesity-induced inflammation. JCI Insight. 2025;10(19):e173423. doi:10.1172/jci.insight.173423
27. Chen J, Wu Q, Liu H, et al. Predictive value of remnant cholesterol inflammatory index for stroke risk: evidence from the China health and Retirement Longitudinal study. J Adv Res. doi:10.1016/j.jare.2024.12.015
28. Chen W, Xiao K, Zhou C, Cheng J, Zeng Z, Zhang F. Association of composite dietary antioxidant index and endometriosis risk in reproductive—age women: a cross-sectional study using big data-machine learning approach. Front Nutr. 2025;12:1572336. doi:10.3389/fnut.2025.1572336
29. Ren X, Jiang M, Han L, Zheng X. Association between triglyceride-glucose index and chronic kidney disease: a cohort study and meta-analysis. Nutr, Metab Cardiovasc Dis. 2023;33(6):1121–1128. doi:10.1016/j.numecd.2023.03.026
30. Imperiale L, Nisolle M, Noël JC, Fastrez M. Three types of endometriosis: pathogenesis, diagnosis and treatment. state of the art. J Clin Med. 2023;12(3):994. doi:10.3390/jcm12030994
31. Hu PW, Yang BR, Zhang XL, et al. The association between dietary inflammatory index with endometriosis: NHANES 2001–2006. PLoS One. 2023;18(4):e0283216. doi:10.1371/journal.pone.0283216
32. Luo Y, Wang D, Chen S, Yang Q. The role of miR-34c-5p/Notch in epithelial-mesenchymal transition (EMT) in endometriosis. Cell Signal. 2020;72:109666. doi:10.1016/j.cellsig.2020.109666
33. Patel BG, Lenk EE, Lebovic DI, Shu Y, Yu J, Taylor RN. Pathogenesis of endometriosis: interaction between Endocrine and inflammatory pathways. Best Pract Res Clin Obstet Gynaecol. 2018;50:50–60. doi:10.1016/j.bpobgyn.2018.01.006
34. Vallvé-Juanico J, Houshdaran S, Giudice LC. The endometrial immune environment of women with endometriosis. Human Reproduction Update. 2019;25(5):565–592. doi:10.1093/humupd/dmz018
35. Zondervan KT, Becker CM, Missmer SA. Endometriosis. N Engl J Med. 2020;382(13):1244–1256. doi:10.1056/NEJMra1810764
36. Chantalat E, Valera MC, Vaysse C, et al. Estrogen receptors and endometriosis. Int J Mol Sci. 2020;21(8):2815. doi:10.3390/ijms21082815
37. Ortiz R, Gemmill JAL, Sinaii N, et al. Hypothalamic-pituitary-adrenal axis responses in women with endometriosis-related chronic pelvic pain. Reprod Sci. 2020;27(10):1839–1847. doi:10.1007/s43032-020-00201-x
38. Zhou WJ, Yang HL, Shao J, et al. Anti-inflammatory cytokines in endometriosis. Cell. Mol. Life Sci. 2019;76(11):2111–2132. doi:10.1007/s00018-019-03056-x
39. Herup-Wheeler T, Shi M, Harvey ME, et al. High-fat diets promote peritoneal inflammation and augment endometriosis-associated abdominal hyperalgesia. bioRxiv - Physiology. doi:10.1101/2023.11.09.566474
40. Melo AS, Rosa-e-Silva JC, Rosa-e-Silva ACJ, et al. Unfavorable lipid profile in women with endometriosis. Fertil Sterility. 2010;93(7):2433–2436. doi:10.1016/j.fertnstert.2009.08.043
41. Ito A, Suganami T. Lipid metabolism in myeloid cell function and chronic inflammatory diseases. Front Immunol. 2025;15. doi:10.3389/fimmu.2024.1495853
42. Zou G, Wang J, Xu X, et al. Cell subtypes and immune dysfunction in peritoneal fluid of endometriosis revealed by single-cell RNA-sequencing. Cell Biosci. 2021;11(1). doi:10.1186/s13578-021-00613-5
43. Heard ME, Melnyk SB, Simmen FA, Yang Y, Pabona JMP, Simmen RCM. High-fat diet promotion of endometriosis in an immunocompetent mouse model is associated with altered peripheral and ectopic lesion redox and inflammatory status. Endocrinology. 2016;157(7):2870–2882. doi:10.1210/en.2016-1092
44. Scheerer C, Bauer P, Chiantera V, Sehouli J, Kaufmann A, Mechsner S. Characterization of endometriosis-associated immune cell infiltrates (EMaICI). Arch Gynecol Obstetrics. 2016;294(3):657–664. doi:10.1007/s00404-016-4142-6
45. Domínguez F, Ferrando M, Díaz-Gimeno P, et al. Lipidomic profiling of endometrial fluid in women with ovarian endometriosis†. Biology of Reproduction. 2017;96(4):772–779. doi:10.1093/biolre/iox014
46. Xue B, Wu S, Sharkey C, et al. Obesity-associated inflammation induces androgenic to estrogenic switch in the prostate gland. Prostate Cancer and Prostatic Diseases. 2020;23(3):465–474. doi:10.1038/s41391-020-0208-4
47. Wu YT, Ma SY, Sun WQ, et al. TRIM65 promotes invasion of endometrial stromal cells by activating ERK1/2/C-myc signaling via ubiquitination of DUSP6. J Clin Endocrinol Metab. 2021;106(2):526–538. doi:10.1210/clinem/dgaa804
48. Zhong Y, Liu C, Feng J, Li JF, Fan ZC. Curcumin affects ox-LDL-induced IL-6, TNF-α, MCP-1 secretion and cholesterol efflux in THP-1 cells by suppressing the TLR4/NF-κB/miR33a signaling pathway. Exp Ther Med. 2020;20(3):1856–1870. doi:10.3892/etm.2020.8915
49. Tsai HW, Huang MT, Wang PH, Huang BS, Chen YJ, Hsieh SL. Decoy receptor 3 promotes cell adhesion and enhances endometriosis development. J Pathol. 2017;244(2):189–202. doi:10.1002/path.5000
50. Ellulu MS, Patimah I, Khaza’ai H, Rahmat A, Abed Y. Obesity and inflammation: the linking mechanism and the complications. Arch Med Sci. 2017;13(4):851–863. doi:10.5114/aoms.2016.58928
51. Nanda A, T K, Banerjee P, et al. Cytokines, angiogenesis, and extracellular matrix degradation are augmented by oxidative stress in endometriosis. Ann Lab Med. 2020;40(5):390–397. doi:10.3343/alm.2020.40.5.390
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.