Back to Journals » Medical Devices: Evidence and Research » Volume 18
The Performance of Blow-by Method Using Pediatric Non-Rebreathing Mask for Oxygen Delivery During Transport of Pediatric Patients: A Laboratory Study
Authors Sangsungnern P ![]() , Thanharak S, Chanthawong S
, Thanharak S, Chanthawong S ![]() , Silarat S, Ruenhunsa T
, Silarat S, Ruenhunsa T ![]() , Charoensuk C
, Charoensuk C
Received 6 September 2025
Accepted for publication 14 November 2025
Published 22 November 2025 Volume 2025:18 Pages 573—578
DOI https://doi.org/10.2147/MDER.S565302
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Peerapong Sangsungnern, Saran Thanharak, Sarinya Chanthawong, Suparit Silarat, Thitinuch Ruenhunsa, Chanapat Charoensuk
Department of Anesthesiology, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand
Correspondence: Sarinya Chanthawong, Department of Anesthesiology, Faculty of Medicine, Khon Kaen University, Khon Kaen, 40002, Thailand, Tel +66 43 363 060, Email [email protected]
Purpose: The blow-by method using a pediatric non-rebreathing mask (PNRM) is commonly employed to maintain oxygenation during transport of pediatric patients after general anesthesia. This study aimed to evaluate the performance of the blow-by method using a PNRM with an oxygen flow rate of 10 liters per minute (LPM) during simulated transport of pediatric patients.
Patients and Methods: This laboratory study was simulated along a 32-meter corridor from the pediatric operating room to the post-anesthesia care unit at Srinagarind Hospital. A pediatric mannequin was positioned laterally on a transport trolley. A PNRM delivering oxygen at 10 LPM was placed at distances of 0, 5, and 10 cm from the mannequin’s nose. The fraction of inspired oxygen (FiO2) at the mannequin’s nose was measured every 2 meters along the corridor. Each distance condition was tested 10 times. The primary outcome was whether the blow-by method could maintain FiO2 above 40% at all measurement points during simulated patient transport.
Results: Oxygen delivery was adequate only when the PNRM was placed at 0 cm from the nose, with a mean FiO2 of 86.9 ± 0.3%, In contrast the mean FiO2 values at 5 and 10 cm was 28.5 ± 0.3%, and 24.1 ± 0.1%, respectively. The mean FiO2 difference between 0 and 5 cm was 58.4% (95% CI: 56.8– 60.1; p < 0.001), and between 0 and 10 cm was 62.8% (95% CI: 61.5– 64.1; p < 0.001).
Conclusion: The blow-by method using PNRM positioned at 0 cm from pediatric mannequin’s nose provided adequate oxygenation throughout transport. Clinically, therefore, maintaining a close PNRM position is essential.
Keywords: children, desaturation, fraction of inspired oxygen, oxygen therapy, post anesthesia care, transportation
Introduction
Desaturation following general anesthesia (GA) in spontaneously breathing pediatric patients during transport from the operating room (OR) to the post-anesthesia care unit (PACU) has been reported in 21% to 28% of cases.1–6 This high incidence can be attributed to the residual effects of GA, which cause airway collapse, ventilation-perfusion mismatch, and reduced functional residual capacity (FRC), and the unique respiratory physiology of pediatric patients, both of which increase the risk of hypoxemia.6,7 Pediatric patients, especially those under 6–8 years, are at higher risk of desaturation than adults owing to their smaller and more compliant airways, higher oxygen consumption, lower FRC, and immature respiratory control.8 Desaturation may result in critical consequences, including neurological injury from prolonged cerebral hypoxia, cardiovascular instability such as bradycardia and hypotension, and a heightened risk of cardiac arrest, which has been reported in up to 44% of desaturation events.9 Additionally, as many as 80% of pediatric patients in the immediate post-anesthetic period are uncooperative and may not tolerate direct contact with oxygen delivery devices on their face. For this reason, oxygen supplementation during transport is currently recommended to prevent desaturation in these patients.5,6,10 The oxygen blow-by method is commonly used for pediatric oxygenation. It involves directing oxygen flow—via oxygen tubing, corrugated tubing, or a face mask—toward the patient’s nose and mouth from a short distance, without direct contact. While this method is less reliable in delivering a specific fraction of inspired oxygen (FiO2), it may be better tolerated by pediatric patients after GA, who often resist face-contact devices.10,11
The blow-by method using a pediatric non-rebreathing mask (PNRM) is commonly employed to provide oxygenation for pediatric patients during transport after general anesthesia (GA). Previous studies have shown that this method can deliver oxygen concentrations ranging from 30% to 40%, depending on the flow rate and the distance between the PNRM and the patient’s face.12,13 However, these studies were conducted under static conditions with immobilized patients. The performance of the blow-by method using a PNRM during actual transport remains unclear. Movement of the transport trolley may generate airflow around the patient and the oxygen delivery system, potentially altering the oxygen direction and diluting the delivered FiO2. Therefore, this study aimed to determine the FiO2 delivered using the blow-by method with a PNRM during the transport of a pediatric mannequin from the OR to the PACU at a normal walking speed. The blow-by method using a PNRM was selected in this study because it represents the routine practice in our institution.
Materials and Methods
Test protocol
This was a laboratory study simulated in the OR and PACU at Srinagarind Hospital, Khon Kaen University. A pediatric mannequin was placed in the left lateral decubitus position on a transport trolley. A PNRM delivering oxygen at 10 liters per minute (LPM) was placed at the level of the mannequin’s nose. The distance between the PNRM and the mannequin’s nose was tested at three distances: 0 cm (group 1), 5 cm (group 2), and 10 cm (group 3), as illustrated in Figure 1. The FiO2 was measured using an oxygen sensor (Philips IntelliVue G5 anesthetic gas module), with the gas sampling line tip placed at the mannequin’s nose. The oxygen sensor was calibrated according to manufacturer’s recommendations to ensure measurement accuracy. The study was conducted along a 32-meter corridor connecting the pediatric OR and PACU, which included three turning points at 8, 18, and 26 meters. There were two doors in the corridor connecting the pediatric OR and PACU—one between the pediatric OR and the corridor, and the other between the corridor and the PACU—both of which were kept open to minimize airflow disruption. Floor markings were placed every 2 meters to maintain a constant walking speed and to standardize FiO2 measurements.
 |
Figure 1 The distances of 0 cm (A), 5 cm (B), and 10 cm (C) from the mannequin’s nose using a pediatric non-rebreathing mask. |
Precision testing was conducted and repeated five times to verify test reproducibility. Each group was tested 10 times, for a total of 30 tests, to minimize random variability and enhance measurement reliability. All tests were performed by a single investigator to ensure a consistent walking speed of approximately one meter per second, reflecting the average pace of routine patient transport along the corridor. A second investigator recorded the FiO2 at every 2-meter interval and documented the duration of each test.
The run time for each test was recorded as a characteristic of each group. The primary outcome was to determine whether the blow-by method using a PNRM with an oxygen flow rate of 10 LPM could maintain an FiO2 greater than 40% at every 2-meter interval along the corridor during pediatric patient transport. An FiO2 above 40% is recommended to ensure adequate oxygenation during transport; therefore, 40% was selected as the cut-point for safe oxygen delivery. The secondary outcome was to assess the mean FiO2 differences between group 1 and group 2, group 1 and group 3, and group 2 and group 3.
Statistical Analysis
Statistical analysis was performed using IBM SPSS Statistics for Windows (Version 27.0; IBM Inc, Armonk, NY). Continuous data were presented as mean and standard deviation (SD) or median and interquartile range (IQR), as appropriate. One-way analysis of variance (ANOVA) was used to assess statistically significant differences among the three groups and to evaluate mean differences in FiO2 between group 1 and 2, group 1 and 3, and group 2 and 3, with 95% confidence intervals (CI). A p-value less than 0.05 was considered statistically significant.
Results
A total of 30 tests were conducted, with 10 tests per group for run time measurement. The average run times were 31.98 ± 0.87, 33.31 ± 1.42, and 32.80 ± 1.37 seconds in groups 1, 2, and 3, respectively (p = 0.070).
The mean FiO2 percentages at the starting point (0 m) and at the PACU (32 m) with an oxygen flow rate of 10 L/min were 86.90 ± 2.18%, 28.60 ± 1.96%, and 24.10 ± 0.32% in groups 1, 2, and 3, respectively (p < 0.001). At a 0 cm distance from the face (group 1), the blow-by method maintained adequate oxygenation (FiO2 > 40%) throughout the entire transport distance, as shown in Figure 2.
 |
Figure 2 The mean fraction of inspired oxygen at distances of 0 cm (Group 1), 5 cm (Group 2), and 10 cm (Group 3) from the mannequin’s nose using a pediatric non-rebreathing mask. Abbreviations: FiO2, fraction of inspired oxygen; Group 1, pediatric non-rebreathing mask at 0 cm from the mannequin’s nose; Group 2, pediatric non-rebreathing mask at 5 cm; Group 3, pediatric non-rebreathing mask at 10 cm. |
The mean FiO2 at each 2-meter interval differed significantly among the three groups (p < 0.001), as shown in Table 1. Pairwise comparisons also revealed statistically significant differences in mean FiO2 between all groups (Table 2). The mean difference in FiO2 between group 1 and group 2 was 58.30 (95% CI: 56.35–60.25; p < 0.001), between group 1 and group 3 was 62.80 (95% CI: 62.80–64.37; p < 0.001), and between group 2 and group 3 was 4.50 (95% CI: 3.09–5.90; p < 0.001).
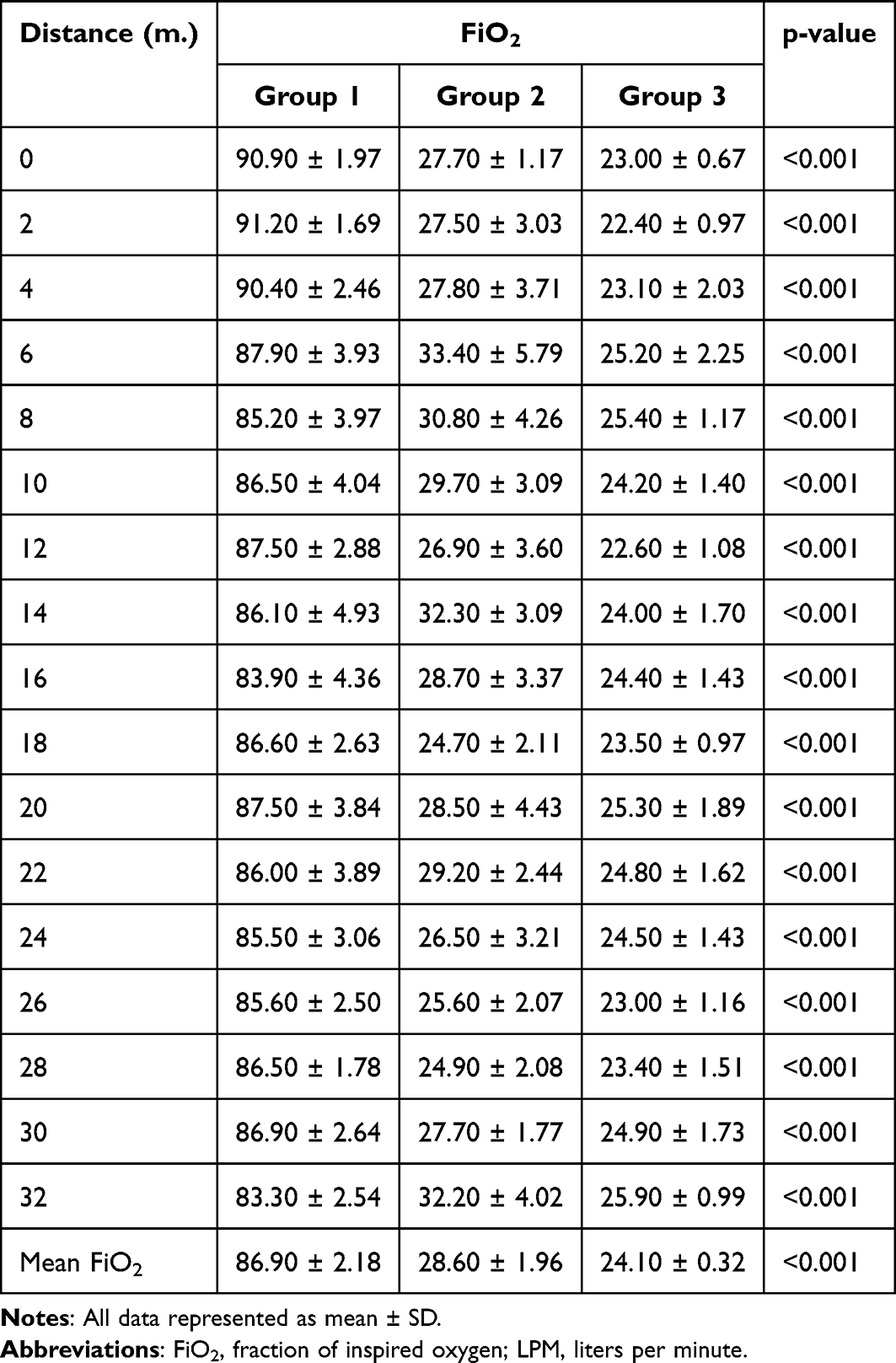 |
Table 1 The FiO2 at Distances of 0 cm (Group 1), 5 cm (Group 2), and 10 cm (Group 3) From the Mannequin’s Nose Using a Pediatric Non-Rebreathing Mask with an Oxygen Flow Rate of 10 LPM |
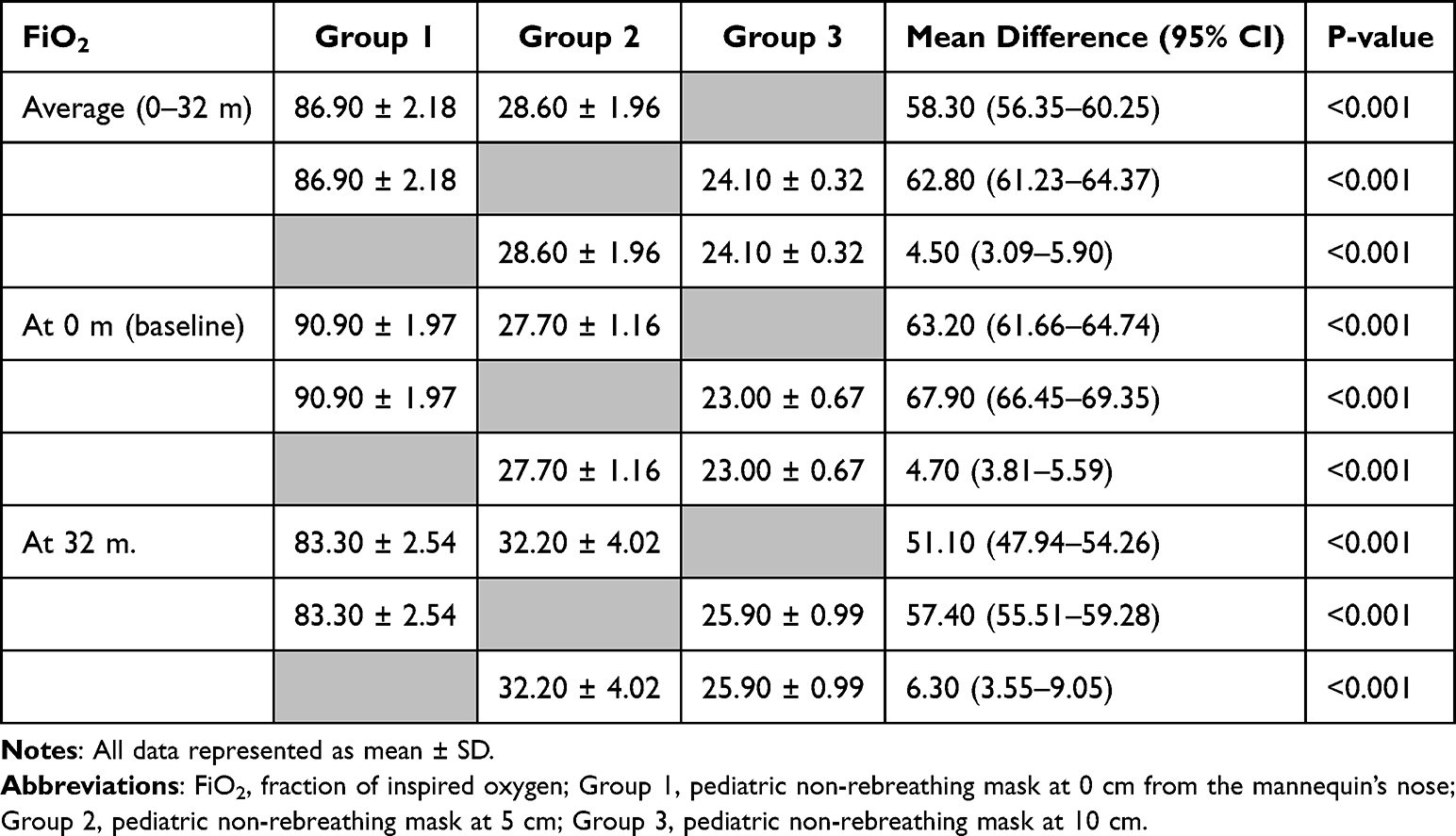 |
Table 2 Mean Differences of FiO2 at 0 m, 32 m and Average Distance (0–32 m) Among Three Groups |
Discussion
Desaturation following general anesthesia in pediatric patients during transport from the operating room to the post-anesthetic care unit (PACU) is common.1–6 To prevent this, oxygen administration via the blow-by method with an FiO2 greater than 40% is generally recommended. Previous studies by Davies et al12 and Blake et al13 found that using a PNRM with an oxygen flow rate of 10–15 LPM, held 5–10 cm from the face of an immobilized pediatric patient, could consistently deliver an FiO2 of 30–40%.
In our study, conducted under transport conditions using a PNRM, only group 1—where the mask was placed 0 cm from the mannequin’s nose—provided adequate oxygenation (FiO2 > 40%) throughout transport, with a mean FiO2 of 86.90 ± 2.18%. In contrast, placing the PNRM at 5 cm (group 2) and 10 cm (group 3) resulted in mean FiO2 levels of 28.60 ± 1.96% and 24.10 ± 0.32%, respectively, which are inadequate for safe oxygenation. These results differ from previous studies and may be attributed to aerodynamic factors and the effect of distance on the direction and volume of oxygen flow during transport.
Our study also demonstrated that when both the patient and the oxygen delivery device were stationary at the starting point of the corridor (0 m), a PNRM delivering oxygen at 10 LPM, placed 5 cm or 10 cm from the mannequin’s face, failed to achieve an FiO2 > 40%. Therefore, to ensure adequate oxygenation in immobilized patients, the PNRM should be positioned as close to the patient’s face as possible.
Our findings are supported by the study of Barends et al10 which evaluated various oxygen delivery devices and flow rates for supplemental oxygen during transport. They reported that devices delivering oxygen at 10 LPM should be positioned at 0 cm from the face to achieve an FiO2 > 50%. Interestingly, they also found that the Mapleson C system, even when placed 5 cm from the face, could maintain an FiO2 > 50%. This suggests that the type of oxygen delivery device may influence the FiO2 delivered.
This study has several limitations. The oxygen measurements may have been subject to delay due to the use of a gas sampling line required by the oxygen sensor. Uncontrolled air currents along the corridor could also have influenced FiO2 measurements. Additionally, for safety reasons, the study was conducted using mannequins, which eliminates patient-related variability such as airway patency, spontaneous breathing pattern, and patient movement. Further studies in pediatric patients are needed to evaluate various oxygen delivery devices, different oxygen flow rates, and the effects of varying transport speeds.
Conclusion
The blow-by method using a pediatric non-rebreathing mask placed 0 cm from the mannequin’s nose maintained adequate oxygenation throughout transport, whereas placements at 5 and 10 cm failed to maintain an FiO2 greater than 40%. In real pediatric patients, FiO2 may vary depending on factors such as aerodynamics during transport, the distance between the device and the patient’s nose, the type of oxygen device, and patient factors, including cooperation and breathing pattern.
Acknowledgments
The authors would like to thank the anesthesia personnel at Srinagarind Hospital, Faculty of Medicine, Khon Kaen University for their kind assistance. We would also like to acknowledge Dr. Dylan Southard for editing this manuscript via the Publication Clinic at Khon Kaen University, Thailand.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Pullerite J, Burrows FA, Roy WL. Arterial desaturation in healthy children during transfer to the recovery room. Can J Anaesth. 1987;34(5):470–473. doi:10.1007/BF03014352
2. Amar D, Brodman LE, Winikoff SA, Hollinger I. An alternative oxygen delivery system for infants and children in the post-anaesthesia care unit. Can J Anaesth. 1991;38(1):49–53. doi:10.1007/BF03009163
3. Mamie C, Habre W, Delhumeau C, Barazzone Argiroffo C, Morabia A. Incidence and risk factors of perioperative respiratory adverse events in children undergoing elective surgery. Pediatr Anesth. 2004;14(3):218–224. doi:10.1111/j.1460-9592.2004.01169.x
4. Bunchungmongkol N, Somboonviboon W, Suraseranivongse S, Vasinanukorn M, Chau-in W, Hintong T. Pediatric anesthesia adverse events: the Thai anesthesia incidents study (THAI Study) database of 25,098 cases. J Med Assoc Thai. 2007;90(10):2072–2079.
5. Hintong T, Klanarong S, Suksompong S, Chua-in W, Chatmongkolchat S, Werawatganon T. The Thai anesthesia incident monitoring study (Thai AIMS) of oxygen desaturation in the post-anesthetic care unit. J Med Assoc Thai. 2008;91(10):1531–1538.
6. Oofuvong M, Ratprasert S, Chanchayanon T. Risk prediction tool for use and predictors of duration of postoperative oxygen therapy in children undergoing non-cardiac surgery: a case-control study. BMC Anesthesiol. 2018;18(1):137. doi:10.1186/s12871-018-0595-4
7. Patel R, Norden J, Hannallah RS. Oxygen administration prevents hypoxemia during post-anesthetic transport in children. Anesthesiology. 1988;69(4):616–617. doi:10.1097/00000542-198810000-00030
8. Di Cicco M, Kantar A, Masini B, Nuzzi G, Ragazzo V, Peroni D. Structural and functional development in airways throughout childhood: children are not small adults. Pediatr Pulmonol. 2021;56(1):240–251. doi:10.1002/ppul.25169
9. Christensen R, Voepel-Lewis T, Lewis I, Ramachandran SK, Malviya S. Pediatric cardiopulmonary arrest in the postanesthesia care unit: analysis of data from the American heart association get with the guidelines-resuscitation registry. Pediatr Anesth. 2013;23(6):517–523. doi:10.1111/pan.12154
10. Barends CRM, Yavuz P, Molenbuur B, Absalom AR. Performance of blow-by methods in delivering oxygen to pediatric patients during transport: a laboratory study. Pediatr Anesth. 2018;28(12):1142–1147. doi:10.1111/pan.13515
11. Walsh BK, Smallwood CD. Pediatric oxygen therapy: a review and update. Respir Care. 2017;62(6):645–661. doi:10.4187/respcare.05245
12. Davies P, Cheng D, Fox A, Lee LL. The efficacy of noncontact oxygen delivery methods. Pediatrics. 2002;110(5):964–967. doi:10.1542/peds.110.5.964
13. Blake DF, Shih EM, Mateos P, Brown LH. The efficacy of oxygen wafting using different delivery devices, flow rates and device positioning. Australas Emerg Nurs J. 2014;17(3):119–125. doi:10.1016/j.aenj.2014.05.002
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.