Back to Journals » Psychology Research and Behavior Management » Volume 9
The perception of intuition in clinical practice by Iranian critical care nurses: a phenomenological study
Authors Hassani P, Abdi A ![]() , Jalali R
, Jalali R ![]() , Salari N
, Salari N ![]()
Received 21 November 2015
Accepted for publication 7 January 2016
Published 8 March 2016 Volume 2016:9 Pages 31—39
DOI https://doi.org/10.2147/PRBM.S101040
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Parkhide Hassani,1 Alireza Abdi,1 Rostam Jalali,2 Nader Salari3
1Faculty of Nursing and Midwifery, Shahid Beheshti University of Medical Sciences, Tehran, Iran; 2Faculty of Nursing and Midwifery, Kermanshah University of Medical Sciences, Kermanshah, Iran; 3Department of Biostatistics and Epidemiology, School of Public Health, Kermanshah University of Medical Sciences, Kermanshah, Iran
Background: Intuition as a way of learning in nursing is applied to decision making and judgment in complicated clinical situations. Several studies have been conducted on intuition in clinical settings, but comprehension of this concept is unclear. Moreover, there is a lack of information about intuition in critical care nurses caring for more seriously ill patients. This study aimed to explore Iranian critical care nurses’ understanding of intuition in clinical practice.
Methods: In a descriptive–phenomenological study, 12 nurses employed in critical care units of the hospitals affiliated to Kermanshah University of Medical Sciences were purposively recruited to the study. A semistructured interview was administered, and then written verbatim. The data were managed by MAXQDA 10 software, and qualitative analysis was undertaken using the seven-stage approach of Colaizzi.
Results: Of the 12 nurses who participated in the study, 7 (58.3%) were female and married, and 10 (88.3%) held a bachelor's degree in nursing. The mean and standard deviations of participants' age, job experience, and critical care experience were 36.66±7.01, 13.75±6.82, and 7.66±3.36 years, respectively. Four main themes and eleven sub-themes were elicited from the qualitative analysis; the main themes including “Understanding intuition as a feeling”, “Understanding intuition as a thought”, “Understanding intuition as receiving signs”, and “Understanding intuition as an alarm”. Because they have trust in their own intuition, the nurses made further assessments and paid more attention to patients. They were also better prepared after receiving intuition alarms to perform the appropriate responses, and acting upon the alarms reduced the nurses’ physical and psychological signs.
Conclusion: The findings showed how intuition was understood by the critical care nurses; therefore, these results can be considered to form a theoretical basis for designing other studies. Because of the significant role of intuition in enhancing the nursing care of critically ill patients, it is suggested that more qualitative, quantitative, and trials studies be performed to reinforce intuition in nursing; moreover, to incorporate intuition into nursing curriculums, it should be debated in academic settings.
Keywords: intuition, nurses, critical care, qualitative research
Background
Intuition is a gestalt experience of awareness, which is related to the unconscious mind and cannot be explained by logic.1 This concept entered into nursing in the 1970s at the same time as the analysis of abstract nursing constructs by qualitative approaches.2 Psychology researchers have focused on intuition for four decades and have demonstrated that intuition improves individuals’ job performance by strengthening their decision-making ability.3 Electrophysiological studies have also confirmed the existence of human intuition, and illustrated its origin in the frontal cortex of the brain.4,5 Despite the emphasis of researchers on intuition in nursing, it has been known as a questionable entity.6 However, because of the high quality and accuracy of intuitive judgments, researchers believe in its usefulness;7,8 some are also of the opinion that the decision-making ability of a person is related to his/her intuitive power.8
The nursing profession has advanced significantly over the past 50 years. People are living longer, technology is advancing rapidly, and patients are presenting as more critically ill;9 therefore, a wide variety of ways of knowing (empirical, aesthetic, ethical and personal), cultural beliefs, and values need to be includes in the nursing curriculum.10 However, among the four methods of receiving knowledge in nursing (empirical, aesthetic, personal, and ethical knowing),11,12 intuition is the art of nursing or “esthetic knowing”, as well as “tacit or personal knowing”,6,13 but nursing has just focused onto evidence-based practice and rational-linear ways of thinking and knowing. Hence, these positivist ways are responsible for the failure to incorporate tacit or intuitive knowledge in the educational curriculum. Consequently, the lack of attention to all approaches of knowing, and focusing solely on the “empirical” and “rational” has hindered the enhancement of the intellectual abilities of nursing students.10,14
Several studies have been done on intuition in nursing; accordingly, Benner et al15 theorized that there were five steps to clinical competency in nursing, beginning with the novice and finishing with the expert. In this view, without relying on analytical principles, an expert nurse uses intuition in decision making and judgment.16 However, Cork17 challenges Benner’s theory because of the difficulties involved in assessing and measuring its abstract concepts, as well as inadequate information about how expert nurses comprehend their intuitive capacities. In McCutcheon and Pincombe’s study,18 intuition is the result of a complex synergic interaction between knowledge, experience, and expertise. Furthermore, some studies affirm that intuition is used by clinical nurses facing a moral dilemma in more sophisticated clinical situations,19,20 and that it reduces the mortality of patients in trauma units.21 It also aids the management of crises in unpredictable clinical conditions, and the diagnosis of deterioration in patients in acute situations.22,23
Previous studies have established that “nursing intuition” is still in the qualitative and descriptive stages.24 Limitations of previous studies in viewpoint of Ruth-Sahd25 include:
Unclear definition of intuition, lack of understanding of intuition, failure to identify how the intuitive mind may inform evidence-based practice, no discourse of intuition in education, self-perception of lack of intuitiveness, and fear that an intuitive action may be wrong.25
However, a literature review reveals a lack of studies on intuition in nursing, especially among critical care nurses in Iran and other countries. Hence, the effect of cultural and environmental aspects on intuition26 and the importance of critical care nurses’ decision making in relation to the increased survival rate of critically ill patients27 make it necessary to assess their comprehension of intuition in clinical practice with a view to verifying this concept and justifying its incorporation into the nursing curriculum.
Aim
This study aimed to explore the perception of intuition in clinical practice by Iranian critical care nurses.
Methods
This qualitative study employed the descriptive phenomenological approach. Phenomenology is used to investigate the lived experiences of humans, as established by Edmund Husserl in the early 20th century.28 Phenomenology comprises two approaches, interpretive and descriptive. The interpretative approach, which focuses on the lived experience of participants by incorporating phenomenology and interpretation, analyzes elements of the reflective personal and subjective view of individual experiences and attempts to report on the participant’s experience by considering the researcher’s own view of the world. It recognizes the researcher within the research and analytical process. Indeed, interpretations are based on the researcher’s own conceptions, beliefs, expectations, and experiences.29 The purpose of the descriptive phenomenological approach is to assess the understood experiences of individuals without interference from the researcher’s interpretation of meanings. This requires that researchers bracket all their prior knowledge about the issue.28 Bracketing in descriptive phenomenology is a means of demonstrating the validity of the data collection and analysis process. Therefore, efforts should be made by researchers to put aside their repertoires of knowledge, beliefs, values, and experiences in order to accurately describe participants’ life experiences.30 Descriptive phenomenology is used to get the true meanings by engaging in depth into reality,31 and intuition is an abstract concept and cannot be studied objectively. Therefore, to investigate its essence, the experiences of those participating in its study should be used.32
Participants
The participants were 12 nurses employed in critical care units, specifically recruited from hospitals affiliated to Kermanshah University of Medical Science (KUMS). These five hospitals were selected from 19 governmental centers affiliated to KUMS, and had critical care patients in intensive care units (ICUs) and cardiac care units (CCUs). The inclusion criteria for participants consisted of their having worked in critical care units for at least 3 years, having had experience of intuition in clinical practice, and expressing consent to participate in the study. Nurses who were reluctant to participate in the study or who had not experienced, or could not remember using intuition in their practice, were excluded from the study.
The sample size adequacy was according to the data saturation, with no appearance of new data during the interviews. Saturation in qualitative studies occurs during data gathering and analysis, when, under scrutiny by at least two experts in qualitative research, new information is not obtained.33 In our study, saturation occurred during interview 10. However, for more verification, we carried out two additional interviews. The study was approved by the Ethics Committee of Research Deputy of Shahid Beheshti University of Medical Sciences (SBMU).
Data collection
Permission for data collection was taken from the officials of the research deputy of Shahid Beheshti University of Medical Sciences (SBMU), KUMS, and the hospitals affiliated to KUMS, following which we referred to the critical care units of the hospitals. Additionally, the researcher described two cases of his experiences of using intuition in clinical practice. Nurses who had similar experiences in the use of intuition and the inclusion criteria were identified, and after the topic and objectives of the study were explained, assurance of confidentiality and anonymity of personal information was given, and their written, informed consent was received. A deep, semistructured interview of each of the 12 participants was then conducted, using a questionnaire comprising open questions such as “What is the definition of intuition?” “How do you perceive the intuition signs?” and “What are your experiences of using intuition in clinical practice?” Interviewing has become synonymous with qualitative research and may become the accepted method of data collection irrespective of methodology.34 A semistructured interview is a technique for generating qualitative data and is characterized by open-ended questions that are developed in advance and by prepared probes. In the semistructured interview, the interviewer has a set of questions on an interview schedule, but the interview will be guided by the schedule rather than dictated by it; the interviewer is free to probe interesting areas that arise from participants’ interests or concerns.30 In our study, we applied some other probing questions, for instance, “where did that happen”, “please explain more about [..]”, “what does that mean”, “why did you comprehend that”, and “when did you understand that”? The participants were encouraged to talk freely and to tell stories about intuition in clinical practice in their own words. One interview was performed with each participant. At the end of each, the researcher reminded the participants about her need for a second contact with them via telephone calls to discuss the study findings and to make sure that the study findings reflected their own experiences. The duration of each interview was 30–60 minutes. The interviews were performed in the critical care units during the morning and evening shifts, as agreed by the researcher and the participants. The sampling process lasted about 6 months, from March to August 2015. All the interviews were tape recorded.
Data analysis
MAXQDA 10 software was used for data management, and the data were analyzed as qualitative through the seven-stage approach of Colaizzi.35 This approach is used to elicit the related concepts from the lived experiences of humans, and to organize the anecdotal data into phenomenological studies.36 For this purpose, the following steps were carried out: 1) after each interview, we listened to the audio files repeatedly, transcribed them verbatim, and read the written files several times. 2) After reading the written interviews, we highlighted the meaningfully related statements. 3) A concept representative of each statement was then identified. 4) The researcher then categorized the concepts based on their similarity. 5) The results were subsequently incorporated into bigger categories. 6) An attempt to comprehensively describe the concepts was made. 7) The trustworthiness of the data was verified.
Trustworthiness
The trustworthiness criteria were rigorously tested using several strategies as described by Schwandt et al37 To enhance credibility, the researchers conducted member checks after the first-level analysis and again at several points during data analysis. Finally, participants were asked to review the findings, comment on the accuracy of the interpretations, and confirm descriptions. Credibility was also addressed through peer debriefing; the researchers shared the text summaries, identification of themes, constitutive processes, and final drafts of the findings with colleagues knowledgeable in nursing and qualitative research. The participants varied in demographic characteristics such as age, sex, work location, experience in nursing and critical care units, and, the researchers also believe in the philosophy of qualitative studies, which strengthened the study’s credibility.
To support the study’s dependability, the researchers had prolonged engagement in the study and the texts, with themes scrutinized as an external check by experts in psychology, nursing, and qualitative approaches. We tried the themes to be extracted from the descriptions of the participants with suspension the prior researcher ideas, which revealed the conformability. The researchers believe that transferability of the findings is possible because the sampling was purposive and informational redundancy was achieved. In addition, the descriptions were assessed by three expert nurses apart from the study participants, and our results have enough congruency to their experiences to support transferability.
Results
Of the 12 nurses who participated in the study, 7 (58.3%) were female and married, and 10 (88.3%) had a bachelor’s degree in nursing and 2 had a master’s degree in nursing. The mean and standard deviation of age, job experience, and critical care experience were 36.66±7.01, 13.75±6.82, and 7.66±3.36 years, respectively; these rates varied from 28 to 50 years for age, 5–30 years for job experience, and 4–14 years for critical care experience. Nine of the nurses worked in the ICU and three in the CCU (Table 1).
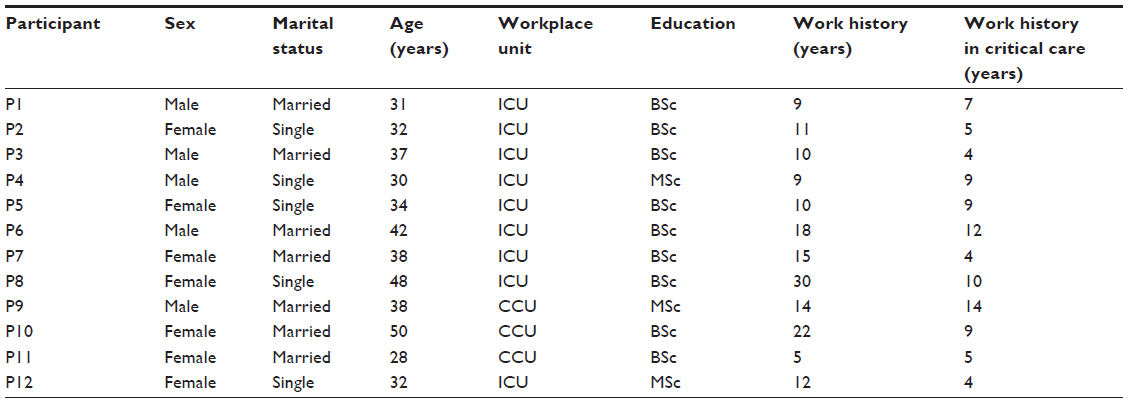 | Table 1 Demographic characteristics of the participants |
From the qualitative analysis of data, four main themes (understanding intuition as a feeling; understanding intuition as a thought; understanding intuition as receiving a sign; and understanding intuition as an alarm) and 11 subthemes emerged (Table 2).
 | Table 2 The themes and subthemes of intuition perception |
Understanding intuition as a feeling
Nearly all the participants declared that they comprehended intuition as a feeling; actually, the perception of intuition as a feeling was the central theme of intuition in nursing, which we identified and separated into “internal feeling”, “inspirational feeling”, “personal feeling”, “sixth-sense feeling”, and “trust feeling”. These feels were very strange to the participants because they did not find any origins for them. As participant 5 (P5) pointed out, it was a “wired state”, or as P10 declared, “I thought many times onto intuition, but I didn’t receive any results”.
Internal feeling
From the viewpoint of eleven of the nurses, intuition was comprehended by the participants as an “internal feeling”. It was an automatic, unconscious, involuntary, and sudden sensation, affected neither by stimuli external to patient conditions nor by any information objectively received from outside. As defined by P5, “that (intuition) is an inner feeling, which at once happens in our inner … this is an internal sense, a person is suddenly involved in it”. The source of this feeling was unknown and solely attributed to the inside of self. “This feeling is quite inner … an internal feeling to an admitted patient in the unit … an internal sense which is created at all” (P11). Another participant, who cared for an old man with pneumonia who was in a stable condition when admitted but later developed complications, stated, “My inner sense told me this patient would be in trouble … unfortunately, it happened … this sense is not anything more talking about [is not debatable], it is an internal feeling” (P4).
Inspirational feeling
Some nurses believed that the intuition that induced them to perform a behavior or informed them of a prediction related to patients came to them by inspiration. P7 stated that most of the time intuition was an inspiration. P6 testified: “It was about two o clock of night (AM), when something inspired me that go and tell this topic to them, it really saved the patient life”, P1 believed, “because I am very close to the patients, this instinctive sense (intuition) inspired me that inform a problem to a person”. Some of the inspirations may be affected by the patients’ moods; for instance, P10, who had two experiences of using intuition in clinical practice, announced: “I felt this person (one of the patients) has great hopes, due to the hopes, God typically protects him, and don’t choose him (choosing for death), because he wanted his live would be persisted, but the one another was cut off (frustrated), want to go, however, I don’t know, how this sense inspired to me (that what happens to these patients).”
Personal feeling
The participants introduced their feelings as “personal”, particularly in relation to the way some nurses concentrated on their patients. One nurse represented, “Sometimes a person feels this sense in themselves, this feeling is his/her own” (P2), and another said, “Maybe the patient is my own, that moment is exclusive to me … I paid attention, I have that sense, or when I looked at them I had that feeling” (P8).
Because of others’ misinterpretation of intuition as personal, not rational, and also immeasurable feelings, the nurses did not discuss their intuition explicitly. P10 said, “Sometimes even I cannot explain it, and really it is not explainable”, and P5 also stated: “The matters such as intuition are not the issues that we could talk about them as open and frankly, because it may be misinterpreted by others (the colleagues), the process is like that they called a mental problem was happened to me, or, what did he say?”
Sixth-sense feeling
Some of the nurses represented their understanding as a sixth-sense feeling, not discernible by the five physiological senses. “In general, perhaps it can be said it is a sixth sense, coming when we do work to patients” (P12). They also remarked that intuition is an illogical sense with no specific reason, which gives some information about the deterioration or recovery of patients without any identifiable symptoms; as stated by P10, “This sixth sense (intuition) could be non-logical, no one thought that elderly man with such symptoms being remained (be improved), any one could not dedicate an account to it”. P7 declared that nurses who have a stronger sixth sense have more intuition, and P3 attributed her intuition entirely to the sixth sense.
Trust feeling
Despite a lack of logical reasons, nearly all the nurses announced that they had more confidence in their intuition. This trust would be enhanced by repeated experiences of the intuitive feeling and the approval of other people. A nurse explained, “I have more trust [in my intuition], because many cases I have felt, really saw its results … whatever the time is going I find it more confidence” (P7). Another described, “I always have confidence to my intuition, without doubt, such as this patient that I sensed he would be critically ill, and happened, the vital signs would be changed, and really happened…” (P12).
Some believed that, although they trusted their intuition, they wanted to try more appropriate measures along with their response to their intuitive feelings. As P7 stated, “I felt what I did could fully answer to the patient, so I had confident to my work … something that came to me I am sure that if I do that, it answer 100%”. Despite the trust in intuition, some nurses need more objective evidences to convince other colleagues of the feeling; as P6 received a trust feeling on pneumothorax of a traumatic patient without any clinical and radiological signs, the doctors and other health care workers denied his feel, but 10 minutes later, when the symptoms began, they adopted it, and the appropriate therapies were started.
Understanding intuition as a thought
Some nurses comprehended intuition as a thought. Although they announced these thoughts came to them when they were placed in certain situations, the thoughts were completely involuntary. At first, the nurses immediately received a thought, so it was fostered as an obsession, from which the subthemes “quick thought” and “obsessive thoughts” were developed.
Quick thought
Intuition was comprehended as a quick thought that sprang up suddenly. The nurses had neither a plan nor any prior background to the intuitive thoughts, and they were formed along with initial visual glimpses of patients. As P8 revealed, “I was looking (at the patient), suddenly came to my brain that my patient will make arrest now”. Another nurse (P10), in response to the question, “how do you use intuition in the clinical workplace?” stated: “The intuition is not a thing we use, it came to the human mind, sometimes I do the regular tasks, I have no any idea to survival or un-survival, to be bettering or worsening the patient, the thought immediately comes to my mind and tell about the state of patient.”
This thought motivated the nurses to do something to help the patient recover; as described by P3, “I was sitting in the station, an unconscious thought (told me) if I take something to the patient, may be changed”.
Obsessive thought
Sometimes, intuition was realized as an obsessive thought. The nurse’s mind was constantly busy with the patients; even though the nurses occasionally went out at work, that thought compelled them to refer to the unit again for administering special care and continually monitoring the patients’ conditions. Consequently, with obsessive thoughts, the nurses gave more attention to the patients. P1 stated, “It was always in my mind to see what the fate of the patient was”. While the obsessive thoughts came, some nurses would be annoyed; as P7 explained, “I was sitting, constantly thinking, at that scenes (in my mind), I saw my patient would be intubated, it was very frustrating”. Some participants attributed these thoughts to their deep involvement in patient care, and being serious to nursing care; as P11 maintained, “now, I have a state where when I would go back to home, my thoughts are here (I am constantly thinking about the patients of the ward). if I work as shallow, these thoughts (intuitive thoughts) would not be created”.
Understanding intuition as receiving signs
The nurses had experienced some signs along with intuition; these signs were categorized into psychological signs and physical signs. Most of the participants declared the psychological signs, but only three of them acknowledged the physical signs. The nurses who experienced psychological signs such as fear, anxiety, apprehension, and worry did not know the origins of the signs. Some nurses stated they also felt a type of discomfort and sadness when they entered the units, and some were waiting for a bad occurrence to take place. P11 affirmed, “There was a fear, a worry, when I am concerned an event will happen, I don’t know what”. Nurses had a desire to do anything to calm themselves. P6 said, “I was restless, I told myself, I must go to do that work”. One of the nurses commented, “in that case, I have no special physical symptoms or (physical) changes (when receiving the intuition), but I engaged mentally (I had psychological signs) and spiritually, my thoughts were busy with patients” (P9). P8 also stated she had experienced terrible anxiety when receiving an intuition of the death of a patient. Some nurses indicated that visceral reactions, such as nausea and vomiting, accompanied their intuitive perceptions; others stated they experienced sweating on the forehead. A nurse expressed it as follows: “I generally get nausea when encountering stress or becoming worried, this happens with intuition too, especially when I have an intuition sense in my private life” (P11). P8 also declared: “My heart rate was bitten rapidly, my body became warm and red”.
Understanding intuition as an alarm
Some nurses understood intuition as an alarm; these alarms happened in the private and working lives of the participants, but were more serious for those who experienced intuition in clinical settings. Those who had lower job experiences and dealt less with intuition took less notice of the alarms, but after seeing their occurrences, they would be more sensitive and took them into account while planning their ministrations. The alarms were about imminent danger, death predictions, and patient recovery.
Imminent danger
Nurses perceived the possible occurrence of deterioration in their patients’ condition in a way that was very clear to them. One nurse reported: “The sense told me, this patient will experience complications in terms of kidney, gastrointestinal and respiratory functions… I myself had this sense, unlike the physician’s opinions” (P4). P12 stated, “Each time, I felt an event would happen, a change in vital signs, in the consciousness or in the size of pupils; these alarms and warnings are more understandable for the nurses who are intuitive”. Some noted that they articulated the ongoing risk to their counterparts; as mentioned by P1, “We told a colleague, if this patient goes to the ward (general ward), they will be intubated and the code (a hospital emergency code) will occur”. Another nurse (P9) stated that, inexplicably, despite the patient being normal in their vital signs, his perception was that “the patient is not good”.
Death prediction
Nearly all the nurses received an alarm that predicted the death of a certain patient; this perception was usually in contrast to their physiological and examination data. P3, who placed a patient from the operation room on the ventilator system, described, “I felt the patient cannot separate from the (ventilator) system”. P6 also declared: “One time, I came to the ICU, circulated around the beds, and unconsciously I knew which patient would die”. This alarm made nurses more ready to offer timely care. One of the nurses (P11), who had been working in CCU for 5 years, explained that one of her patients, who had had a heart attack, had been discharged from the CCU to a general ward, and that despite the stability of cardiac issues such as electrocardiography and vital signs, she had felt the patient would not survive; later, she was informed that the patient had fallen from the bed in the general ward, had suffered a severe head trauma, and finally died because of the head injury.
Patient recovery
Sometimes, when health care workers including physicians and some nurses foresaw a very poor prognosis for the patients, and physicians even ordered a “no code” for them, when participants in the study received an alarm related to the recovery of the patients, they responded more conscientiously and continued medical care without any orders. This was confirmed by P8, who recounted: “The doctor had spoken to the patient’s family explaining the patient had about a 90%–95% chance of dying … I perceived that the patient was not mortal, and did all the nursing care carefully, he went to the operation room without any bleeding, returned, and after 2 days he was discharged.”
Before admitting a patient in ICU, P6 declared, he had perceived the admission of an accident victim, and although the prognosis was critical but against the physician order, his intuition told him “the patient would have remained”. Another nurse (P4), following his intuition alarm, felt assured a certain patient would recover, and injected an adrenalin ampule into the cardiac muscle of the dead patient that the final stage of the resuscitation was ordered by the physician, after which the patient survived.
Discussion
In this study, intuition was understood as “feeling”, “thought”, “sign”, and “alarm”. While there were no identifiable reasons for these perceptions, they have been understood through an unconsciously automatic approach. In accordance with our study, other researchers have suggested various concepts about understanding intuition as a feeling; Ruth-Sahd and Tisdell38 propose that “gut feeling” means an intrinsic immediate feeling without logical cues; they ascribe its origin to spiritual connection to God and numinous entities. In Kosowski and Roberts’ study,39 it was described as a negative sense, using phrases such as “having a very bad feeling”, “feeling uncomfortable”, “feeling there was something terribly wrong”, “something missing”, or that there was “something they had not done”. These perceptions had been integrated into the social, political, and temporal contexts of the clinical settings. Additional to the feelings, a syncretism interpreted as being “outside the rational self also emerged”. As described by Lyneham et al,32 it represented a desire to treat someone with no prompt other than the self-inner response. Coinciding with our results (that the intuition is comprehended as a “thought), the study of Ramezani-Badr et al,40 some of the participants described their intuition as a clinical reasoning strategy using the statement “a certain feeling” or “it suddenly crossed my mind”. This type of decision making had little to do with the findings regarding the patients’ conditions and was inexplicable. It seems the themes and the phrases used to describe the perception of intuition are conclusively received as personal and influenced by particular underlying variables; prior lived experiences and cultural characteristics of individuals were cited as the main factors.26,38 According to Smith,41 because intuition is a complex and mysterious concept, and somehow personal, it cannot be clearly articulated by the nurses in the clinical practice. Moreover, it appears, because the Iranian nurses have faced issues such as “inequality at work”, “too much work”, “lack of promotion”, “job insecurity”, and “lack of management support”, they lack the authority and desire to state or act upon their intuition;42 these warranted further investigation.
In our study, the participants experienced some psychological and physical signs along with understanding of their intuitions. Smith et al43 indicated that emotional awareness is nearly consistent with the psychological signs manifesting as positive and negative experiences, such as intense feelings, apprehension, excitement, and feeling calm and peaceful. They also noted that physical awareness is a knowing that comes from within the body. Interpreted through the five sense organs, it is described as chills down the spine, headaches, muscle tightness, postural tightness, general uneasiness, increased heart rate, racing blood, stomach tightness, jaw clenching, and sweaty palms. In a study by Demir et al,26 these signs have been characterized as “having digestive system symptoms, feeling a stabbing pain in the stomach, hair standing up, tightness in the throat and nausea”. As they emanate from the unconscious and have an uncertain process,44 it seems perceiving the intuition causes physical and psychological response, naturally, which needs more physiological investigations. Compared with other inquiries, the fewer physical signs that occurred in our study may be attributed to diversity in the cultural backgrounds of nurses and their lack of knowledge of intuition in clinical practice. Perhaps the concept has been forgotten, and the signs have been ascribed to other factors.
The results of our study revealed that the nurses had strong confidence in their intuition, which they explained as trust feelings, but because of staff refusal and differences with the rational approach, they were reluctant to discuss it. Trust is also considered a central theme of intuition in other studies.1,43 Miller1 demonstrated that people with more extroverted personalities are mostly self-confident and trust their intuition. Lyneham et al45 illustrated that trust is at the heart of intuition, because nurses who achieved the highest level of clinical competence found that embodied intuition occurred when there was complete trust in the experience of knowing, which served to build confidence in their expert status. However, Iranian nurses who trust their intuition in independent clinical practice46 will be limited in their application of a nursing care plan based on their intuition. Some believed that intuition could be fostered in nurses and nursing students via certain procedures that have been proposed, such as “mind quieting exercises”, “journal writing”, “group brainstorming”, “sharing intuitive exemplars”, “creating a climate of curiosity and questioning that focuses on the experiences of the student”, “promoting creativity with a futuristic perspective, and tolerance for uncertainty among the students”, “developing objectives that focus on process and pattern recognition”, “including intuitive experiences within the nursing process”, and “encouraging students to assess patients using their sense and intuitive hunches”10,43; however, there are no trial and quantitative studies to support these educational techniques.
Following the perception of intuition, the participants paid more attention to the patients by checking their vital signs, carefully administering the medications, and notifying physicians. As in our study, homeopathic physicians also validate their intuitive thoughts using objective data before applying them.47 Additionally, King and Clark48 were of the opinion that logic in an interactional connection could improve patient care. It appears nurses’ attention to intuition increases their concentration on patient symptoms, with implications for fewer complications and mortality. However, we suggested that the nurses must be allowed to participate in the patients’ diagnosis and therapeutic trends, as well as planning a part of their nursing care in light of their intuition.
Conclusion
This study aimed to explore the comprehension of intuition by critical care nurses; during this process, four main themes and 11 subthemes emerged. Intuition was understood as an automatic, subconsciously derived response, and given that participants mostly had confidence in their experience, it was not articulated, but acted upon according to their senses and their reactions to their physical and psychological signs. Consequently, the nurses paid more attention to their patients.
This initial research, indicating the benefits of nursing intuition in Iran, could be used as a theoretical basis for the introduction of the study of intuition in nursing education. If nurses who are unaware of intuition are neglecting its signs and thus inadvertently failing their patients, on account of lack of evidence to incorporate intuition in the nursing curriculum, education about this source of knowledge, as well as establishing qualitative, quantitative, and instrumental development studies and also trials, is advisable.
Limitations
The nurses were unfamiliar with the concept of intuition, and some of them thought it was related to legal issues. To meet this limitation, the researcher introduced two sample experiences to explain intuition in clinical practice.
Acknowledgments
This study was taken from a PhD dissertation on nursing approved by Shahid Beheshti University of Medical Sciences (SBMU). We are grateful to all the officials of the nursing and midwifery school of SBMU, the research deputy and affiliated hospitals of KUMS, and the nurses who participated in the study. No external funding was utilized for this project.
Disclosure
The authors report no conflicts of interest in this work.
References
Miller VG. Characteristics of intuitive nurses. West J Nurs Res. 1995;17(3):305–316. | |
Miller VG. Measurement of self-perception of intuitiveness. West J Nurs Res. 1993;15(5):595–606. | |
Woolley A, Kostopoulou O. Clinical intuition in family medicine: more than first impressions. Ann Fam Med. 2013;11(1):60–66. | |
Horr NK, Braun C, Volz KG. Feeling before knowing why: the role of the orbitofrontal cortex in intuitive judgments – an MEG study. Cogn Affect Behav Neurosci. 2014;14(4):1271–1285. | |
Spottiswoode SJ, May EC. Skin conductance prestimulus response: analyses, artifacts and a pilot study. J Sci Explor. 2003;17(4):617–641. | |
Pearson H. Science and intuition: do both have a place in clinical decision making? Br J Nurs. 2013;22(4):212–215. | |
Dijkstra KA, van der Pligt J, van Kleef GA, Kerstholt JH. Deliberation versus intuition: global versus local processing in judgment and choice. J Exp Soc Psychol. 2012;48(5):1156–1161. | |
Thompson VA. What intuitions are... and are not. Psychol Learn Motiv. 2014;60:35–75. | |
Distler JW. Critical thinking and clinical competence: results of the implementation of student-centered teaching strategies in an advanced practice nurse curriculum. Nurse Educ Pract. 2007;7(1):53–59. | |
Ruth-Sahd LA. Intuition: a critical way of knowing in a multicultural nursing curriculum. Nurs Educ Perspect. 2003;24(3):129–134. | |
Alligood MR. Nursing Theory: Utilization and Application. St Louis, MO: Elsevier Health Sciences; 2013. | |
Speziale HS, Streubert HJ, Carpenter DR. Qualitative Research in Nursing: Advancing the Humanistic Imperative. Philadelphia, PA: Lippincott Williams & Wilkins; 2011. | |
Chaffey L, Unsworth CA, Fossey E. Relationship between intuition and emotional intelligence in occupational therapists in mental health practice. Am J Occup Ther. 2012;66(1):88–96. | |
Welsh I, Lyons CM. Evidence-based care and the case for intuition and tacit knowledge in clinical assessment and decision making in mental health nursing practice: an empirical contribution to the debate. J Psychiatr Ment Health Nurs. 2001;8(4):299–305. | |
Benner PE, Tanner CA, Chesla CA. Expertise in Nursing Practice: Caring, Clinical Judgment, and Ethics. New York, NY: Springer Publishing Company; 2009. | |
Pretz JE, Folse VN. Nursing experience and preference for intuition in decision making. J Clin Nurs. 2011;20(19–20):2878–2889. | |
Cork LL. Nursing intuition as an assessment tool in predicting severity of injury in trauma patients. J Trauma Nurs. 2014;21(5):244–252. | |
McCutcheon HH, Pincombe J. Intuition: an important tool in the practice of nursing. J Adv Nurs. 2001;35(3):342–348. | |
Sonenshein S. The role of construction, intuition, and justification in responding to ethical issues at work: the sensemaking-intuition model. Acad Manage Rev. 2007;32(4):1022–1040. | |
Singer P. Ethics and intuitions. J Ethics. 2005;9(3–4):331–352. | |
Baird C, Kernohan G, Coates V. Outcomes of advanced trauma life support training: questioning the role of observer. Accid Emerg Nurs. 2004;12(3):131–135. | |
Odell M, Victor C, Oliver D. Nurses’ role in detecting deterioration in ward patients: systematic literature review. J Adv Nurs. 2009;65(10):1992–2006. | |
Rew L, Agor W, Emery MR, Harper SC. Intuitive skills in crisis management. Nursingconnections. 2000;13(3):45–54. | |
Rew L, Barrow EM Jr. State of the science: intuition in nursing, a generation of studying the phenomenon. ANS Adv Nurs Sci. 2007;30(1):E15–E25. | |
Ruth-Sahd LA. What lies within: phenomenology and intuitive self-knowledge. Creat Nurs. 2014;20(1):21–29. | |
Demir Y, Denat Y, Khorshid L, Eser I. Cultural validation of the “use of intuition by nursing students scale – Turkish version”. J Transcult Nurs. 2012;23(4):369–376. | |
Hams SP. A gut feeling? Intuition and critical care nursing. Intensive Crit Care Nurs. 2000;16(5):310–318. | |
Reiners GM. Understanding the differences between Husserl (descriptive) and Heidegger (interpretive) phenomenological research. J Nurs Care. 2012;1:119. | |
Rafique R, Hunt N. Experiences and coping behaviours of adolescents in Pakistan with alopecia areata: an interpretative phenomenological analysis. Int J Qual Stud Health Well-being. 2015;10:26039. | |
Chan ZC, Fung Yl, Chien Wt. Bracketing in phenomenology: only undertaken in the data collection and analysis process. Qual Rep. 2013;18(30):1–9. | |
Lopez KA, Willis DG. Descriptive versus interpretive phenomenology: their contributions to nursing knowledge. Qual Health Res. 2004;14(5):726–735. | |
Lyneham J, Parkinson C, Denholm C. Intuition in emergency nursing: a phenomenological study. Int J Nurs Pract. 2008;14(2):101–108. | |
Nixon A, Wild D. PMC34 methodologies for assessing and demonstrating data saturation in Qualitative inquiry supporting patient-reported outcomes research. Value Health. 2008;11(6):A569. | |
Wimpenny P, Gass J. Interviewing in phenomenology and grounded theory: is there a difference? J Adv Nurs. 2000;31(6):1485–1492. | |
Colaizzi P. Psychological research as the phenomenologist views it. In: Valle RS, King M, editors. Existential-phenomenological Alternatives for Psychology. New York, NY: Oxford University Press; 1978; 48–71. | |
Shosha GA. Employment of colaizzi’s strategy in descriptive phenomenology: a reflection of a researcher. Eur Sci J. 2012;8(27):30–43. | |
Schwandt TA, Lincoln YS, Guba EG. Judging interpretations: but is it rigorous? Trustworthiness and authenticity in naturalistic evaluation. New Dir Eval. 2007;2007(114):11–25. | |
Ruth-Sahd LA, Tisdell EJ. The meaning and use of intuition in novice nurses: a phenomenological study. Adult Educ Q. 2007;57(2):115–140. | |
Kosowski MM, Roberts VW. When protocols are not enough. Intuitive decision making by novice nurse practitioners. J Holist Nurs. 2003; 21(1):52–72. | |
Ramezani-Badr F, Nasrabadi AN, Yekta ZP, Taleghani F. Strategies and criteria for clinical decision making in critical care nurses: a qualitative study. J Nurs Scholarsh. 2009;41(4):351–358. | |
Smith A. Exploring the legitimacy of intuition as a form of nursing knowledge. Nurs Stand. 2009;23(40):35–40. | |
Mosadeghrad AM. Occupational stress and turnover intention: implications for nursing management. Int J Health Policy Manag. 2013;1(2):169–176. | |
Smith AJ, Thurkettle MA, dela Cruz FA. Use of intuition by nursing students: instrument development and testing. J Adv Nurs. 2004;47(6):614–622. | |
Newell BR, Shanks DR. Unconscious influences on decision making: a critical review. Behav Brain Sci. 2014;37(1):1–19. | |
Lyneham J, Parkinson C, Denholm C. Explicating Benner’s concept of expert practice: intuition in emergency nursing. J Adv Nurs. 2008;64(4):380–387. | |
Hagbaghery MA, Salsali M, Ahmadi F. A qualitative study of Iranian nurses’ understanding and experiences of professional power. Hum Resour Health. 2004;2(1):9. | |
Brien S, Dibb B, Burch A. The use of intuition in homeopathic clinical decision making: an interpretative phenomenological study. Evid Based Complement Alternat Med. 2011;2011:935307. | |
King L, Clark JM. Intuition and the development of expertise in surgical ward and intensive care nurses. J Adv Nurs. 2002;37(4):322–329. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.