Back to Journals » Clinical Ophthalmology » Volume 14
The Paradigm Shift of Ophthalmology in the COVID-19 Era
Authors Campos A ![]() , Oliveira N, Martins J, Arruda H, Sousa J
, Oliveira N, Martins J, Arruda H, Sousa J
Received 23 June 2020
Accepted for publication 6 August 2020
Published 14 September 2020 Volume 2020:14 Pages 2625—2630
DOI https://doi.org/10.2147/OPTH.S267427
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
António Campos,1– 3 Nuno Oliveira,1 Joana Martins,1 Henrique Arruda,1 João Sousa1,3,4
1Department of Ophthalmology, Centro Hospitalar de Leiria EPE, Leiria 2410-197, Portugal; 2Institute for Clinical and Biomedical Research (iCBR), Faculty of Medicine, University of Coimbra, Coimbra 3000-548, Portugal; 3ciTechCare, Center for Innovative Care and Health Technology, Polytechnic Institute of Leiria, Leiria 2411-901, Portugal; 4Medical Sciences Department, Faculty of Health Sciences, University of Beira Interior, Covilhã, Portugal
Correspondence: António Campos
Centro Hospitalar de Leiria EPE, Rua de Santo André, Leiria 2410-197, Portugal
Tel +351 244 81700
Email [email protected]
Objective: To describe how a fixed regimen of intravitreal injections (IVI) was helpful to continue activity during the COVID-19 outbreak and lockdown and to address basic conditions to resume activity.
Methods: A fixed regimen of IVI was conceived to significantly reduce the number of visits while keeping a number of injections related to the best outcomes. We retrospectively collected data of surgeries performed in 2019 and in the first seven months of 2020 and from OCTs in the first semester of 2020.
Results: IVI per month, from January to July 2020, were 304, 291, 256, 204, 276, 297 and 322, respectively. Phacoemulsification surgeries in the same period were 397, 408, 171, 0, 304, 391 and 389. Posterior vitrectomies were 23, 21, 17, 10, 21, 28 and 25. Laser sessions were 44, 26, 33, 17, 23 and 33, respectively. OCTs dropped from a mean of 25.7 per day in the first half of March 2020 to 5.8 per day in the second half of March. A mean of 6.5 OCTs per day was made in April, rising to 19.1 in May and 39.5 in June.
Conclusion: It was possible to keep the ophthalmological activity during the pandemic outbreak due to the existence of a pre-scheduled fixed regimen for IVI and to the availability of personal protective equipment. The air-borne nature of the peril we are facing addresses the need to evaluate the physical conditions of health facilities, including ventilation, size of waiting and consult rooms and the need to avoid elevators.
Keywords: COVID-19, SARS-CoV-2, fixed regimen, intra-vitreal injections, resume activity, RT-PCR testing
Introduction
Central retinal vein occlusion (CRVO), branch retinal vein occlusion (BRVO), age-related macular degeneration (AMD) and diabetic macular edema (DME) are the most prevalent diseases needing and depending on intravitreal injections (IVI) as the standard of care. Evidence relates outcomes with number of visits and number of injections.1–5
Visits are key points for anatomical and functional evaluations and anchors for decision making and planning future treatments. However, visits do not treat patients, IVI do. When treatment decisions depend on visits, patients are at risk of falling short from the expected outcomes.
In late 2019 our department suffered an increased demand of outpatients over the Medical Retina Unit. Constraints of available trained personnel drove us to an evidence-based decision to decrease follow-up visits, leaving room for first appointments, eg, general physicians’ or private practitioners’ referrals. A fixed regimen protocol was conceived and got ethical approval by the Institutional Board on late November 2019, becoming an institution guideline of good clinical practice on the 14th of January 2020 (Supplementary Figure 1).
On March 2, 2020, Portugal reported the first positive case of SARS-CoV-2. On March 12, the red level of alert was declared and on March 16, the first death from COVID-19 was reported. Two days later, the state of emergency was declared (lockdown) and the Portuguese Council of Ophthalmology recommended the suspension of all routine practices, a position supported by others in different extents.6–8 As IVI are sight-saving procedures, we did not cancel any pre-scheduled IVI, regardless of the nature of the underlying disease.
Patients’ temperature was checked and surgical face masks were provided at the hospital entrance for patients who had none. Patients were questioned about symptoms, contacts and travelling history before being admitted to the operatory room (OR) and wore surgical face masks during surgery. Filtering face piece respirators KN95 (China GB2626-2006) and goggles were available for surgeons and surgical masks for other health professionals. KN95 face masks were also available for the ophthalmologists and nurses attending the emergency and the laser rooms. Optical Coherence Tomography scans (OCTs) were not cancelled, but technicians’ teams were split in fortnight turnovers. However, there was an increasing missing rate of patients scheduled for OCTs. Routine visits were cancelled until the first week of May and substituted by phone calls and telemedicine, whenever necessary.
We are facing a different sort of challenge now: how to accommodate the usual huge number of patients previous to the COVID-19 outbreak in the waiting rooms, while respecting the new demands from the healthcare authorities to reduce the number of waiting patients to a half or one-third.9 Issues such as the use of personal protective equipment, the size of waiting rooms, ventilation, adherence to disinfection protocols, choose of whom to treat based on the disease natural evolution and the need to prioritize treatment visits over monitoring visits, were addressed recently.10–12 Fixed regimens with the number of injections per year based on the best outcomes may be a good option.2,3,13
Another topic is whom to test for detection of SARS-CoV-2 RNA before undergoing ophthalmic surgery. Should viral RNA detection by RT-PCR testing be asked for all asymptomatic patients undergoing topical anesthetic procedures, such as phacoemulsification or intra-vitreal injections? There is no consensus among ophthalmologists on who should be tested for SARS-CoV-2, because evidence of the virus in the conjunctiva and tears is elusive.14,15
In the Portuguese current panorama, most hospitals just resumed activity, with reduced numbers. The trend will soon be to resume activity at full length. The combination of departments based on upper floors of towered hospitals with tiny waiting rooms and massive outpatient attendance will be a huge challenge for many hospitals.
Patients and Methods
We made a model of treating new patients in a fixed regimen for one year, based on a Treat and Extend (T&E) rationale, reducing the number of follow-up visits to 1 or 2 per year (Figure 1). Based on evidence, we adopted a loading dose protocol of 6 monthly injections for CRVO, 3 monthly injections for BRVO and AMD, and 5 monthly injections for DME. Thereafter, we followed a fixed protocol, extending intervals after the loading dose, based on a T&E regimen. The total number of injections per year was related to the best outcomes reported, and adjustments were not necessary before the first year.1–4,13 Patients were scheduled for the whole year of 2020. Patients outside this protocol, and undergoing treatment for more than one year, were changed to bimonthly injections with aflibercept (if they were not stable in a bimonthly regimen with ranibizumab).
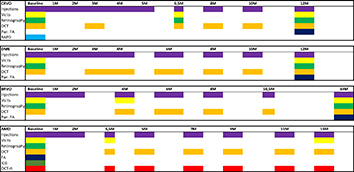 |
Figure 1 Fixed regimen for intravitreal injections in the first year of treatment based on a treat and extend protocol and aiming to spare as many visits as possible. |
Data related to surgical procedures were retrospectively collected, including laser treatments, regarding total values of 2019 and per month from January to July 2020. Strabismus surgery, Oculoplastic surgery, Lacrimal duct surgery and Minor surgery data were not included.
Results
After the state of emergency being declared, we experienced a significant patient missing rate up to 70% at times, for a fortnight, until the end of the first week of April 2020. At the beginning of April we phoned most of the missing patients to reassure them that security measures were re-enforced, and treatments were all re-scheduled. Symptomatic patients, SARS-CoV-2 positive patients and contacts, were postponed until they were RT-PCR negative, except for emergency surgeries that were performed in a COVID-dedicated OR (one room with negative pressure and special requirements12 in the Central OR Unit, attended by all specialties). Phacoemulsification procedures were suspended during the month of April, but retinal and emergency surgeries continued. Data on surgical procedures for the whole year of 2019 and for each month of 2020 are displayed in Table 1. OCTs dropped from a mean of 25.7 per day in the first half of March 2020 to 5.8 per day in the second half of March. A mean of 6.5 OCTs per day were made in April, rising to 19.1 in May and 39.5 in June. Non-contact tonometry was suspended in April and contact tonometry with disposable probes was performed in selected patients (Icare® tonometer, Revenio Corporation, Vantaa, Finland). Non-contact tonometry resumed in early June.
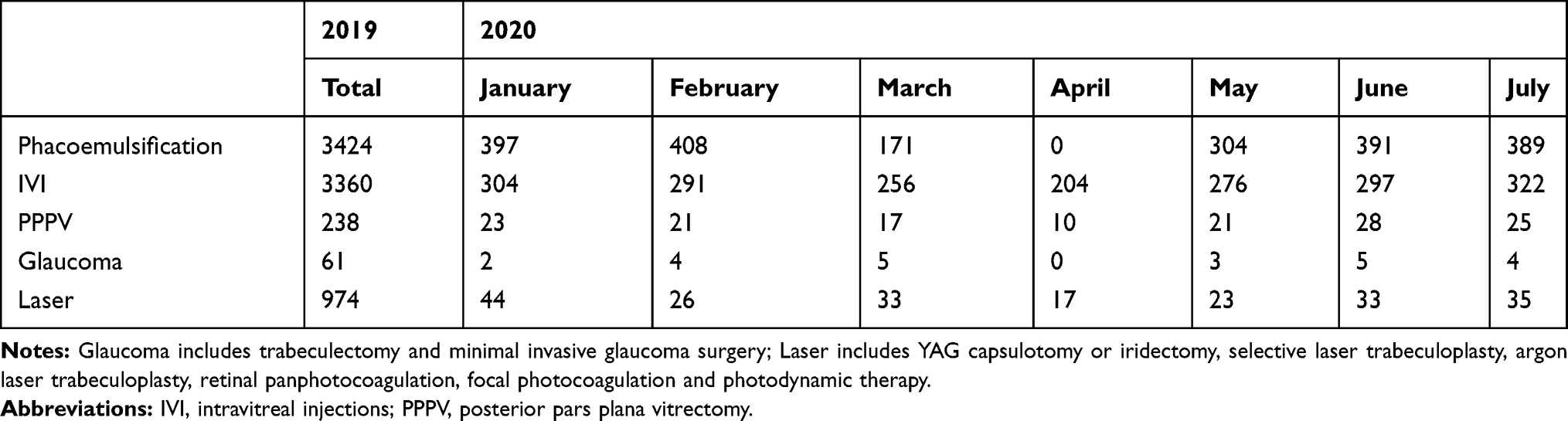 |
Table 1 Ophthalmic Surgeries Performed in the Department in the Year of 2019 and for Each Month of 2020 |
Discussion
Until the end of 2019, a T&E regimen was used with a 3-monthly injection loading dose protocol and adjusting intervals depending on OCT evaluation prior to injection on the same day. Nevertheless, we observed several shortcomings of this protocol: delay in evaluation or adjustments, a considerable amount of DME patients failing to respond to the loading dose, but more importantly, a significant amount of CRVO patients with recurrence of macular edema and the development of macular gliosis, atrophy and permanent vision loss. Those shortcomings and the need to reduce the number of monitoring visits lead to the conception of a fixed treatment protocol.
The number of injections in the new fixed protocol for CRVO was based on the results of the 6-monthly loading dose in the CRUISE study5 that showed better outcomes than the minimum of 3+pro re nata (PRN) in the CRYSTAL study.16 Although the 6 monthly injection protocol of the BRAVO study4 showed a slightly better outcome than the minimum of 3+PRN protocol of the BRIGHTER study,17 we followed a 3+T&E rationale because BRVO does not have the same severe complications as ischemic CRVO and our regimen was not reactive. A loading dose of 3+T&E rationale was adopted for AMD as the higher gain happens within this period18 and the best results at one year are obtained with a mean of 8 injections.19 A loading dose of 5 injections was adopted for DME due to the existence of late responders2,20 and the results being better with 8–9 injections in the first year (Figure 1).3,21
Even though cataract surgery stopped for the whole month of April during the lockdown, we were able to continue IVI without monitoring visits. Missing patients were called home, reassured and re-scheduled. OCTs were not interrupted, since technicians were split in fortnight turnovers. As no member of the department’s personnel got infected, medical or non-medical, this model contributed to enforce the confidence and set the grounds for a rapid return to an almost normal activity as it is displayed in Table 1. The only difference we have now is the scheduling of visits in intervals of 30 minutes.
Asymptomatic professionals or patients are not tested for SARS-CoV-2. Testing asymptomatic healthcare professionals and patients submitted to procedures that do not or may not generate aerosol would not be feasible or cost-effective.22 Furthermore, most reports found a small prevalence of SARS-CoV-2 in the conjunctiva and tears of symptomatic patients only.14,23 RT-PCR tests will have difficulties surpassing the demand, once all specialties resume. Besides, the test does not protect the OR, since it must be disinfected according to the institutional rules.12 The test does not protect the health personnel either, since a negative RT-PCR test does not fully negate the possibility that an individual is infected, and the test is not a vaccine but a sort of snapshot of the moment the swab was collected, therefore it seems to be pointless to test unsuspected asymptomatic health professionals.24,25 Moreover, viral RNA may last for a lot longer than the period of infectivity26 and rapid serologic testing may lead to a sensation of a false security due to the lack of sensitivity and specificity for an acute infection.24 Keeping the patient with a face mask and using closed surgical drapes are simple measures to protect the staff and the patient in the OR. Considering that there is a substantial amount of undocumented infection cases,27 that patients need to be at a close distance for being examined, that sometimes they remain at a close range from the ophthalmologist for a long period of time as in laser treatments,28 the ophthalmologists may be particularly exposed in the office or consult rooms. In the OR, patients wear face masks and surgical closed drapes act as a barrier, there is proper room ventilation and size, and the risk of producing positive SARS-CoV-2 aerosols is very low in the asymptomatic patient.22
The fact that our colleague Dr. Li Wenliang was infected while assisting outpatients at the consult room and died from COVID-19,29,30 the short distance between the patient and the ophthalmologist at the slit lamp microscope and the long duration of laser photocoagulation, raises the question whether the eye doctor might be more vulnerable at the office room rather than in the OR, since proper size and ventilation may not be adequate in offices or outpatient consult rooms.28
Despite we kept activity during the lockdown and resumed surgery at full-length, we realize that healthcare facilities may substantially differ in their conditions. We perform the IVI in the OR. Some facilities use dedicated rooms instead of the OR. However, some of these rooms may not have the same standard of ventilation as an OR, a critical factor in a place shared by a high number of individuals. We did not suffer from shortage of personal protective equipment. Entering or circulating inside the hospital without wearing a face mask is, and was, strictly forbidden right from the start, consult rooms have windows that are kept opened as well as doors while observing patients, and accompanying persons are seldom allowed.8 The waiting room is an open space seating area at the major hall entrance, where patients wait seated in front of TV monitors and are called by number. The whole department is based on the ground floor, including the three ORs of the Ambulatory Surgery Unit, therefore patients do not need to use elevators or stairs. When maximum capacity of the waiting room is reached, patients wait outside. All these measures decrease the viral load that has been related with the infection rate and the severity of the disease.31
Conclusions
In order to prioritize treatments over monitoring, evidence-based fixed regimens and OCTs on the day of injection may be a good adaptation to the pandemic period. Keeping patients with face masks while being operated and the use of filtering face piece respirators seem to be proper for interventions under topical anesthesia. RT-PCR testing of asymptomatic patients in ophthalmology seems to be indicated for patients undergoing general anesthesia only. Perhaps one lesson learned from this pandemic peril is that physicians should wear face masks at the emergency attendance rooms endlessly, as dentists do, even after the pandemic crisis subsides. Hospitals need to have wide waiting rooms and departments with high levels of patients’ attendance benefit from being located in ground floors. Small multiple buildings with multiple ground floor entrances by means of an implantation in hilly grounds, surrounded by outdoor spaces, rather than huge towered buildings, may be more suitable as hospitals in the nearest future.
Ethics Approval
This study was developed after approval from the Quality and Patient Security and Ethical Committees of the Leiria Hospital.
Acknowledgments
JM and HA volunteered to assist COVID-19 patients at the emergency dedicated tent and ward in the months of March, April and May 2020.
We thank Anália Carmo, MD, MSc, PhD, http://orcid.org/0000-0002-7704-4736, from the Laboratory of Molecular Biology/Virology, Clinical Pathology Department, Centro Hospitalar e Universitário de Coimbra, Coimbra, Portugal, for counselling about testing SARS-CoV-2 in the Ophthalmic practice.
Author Contributions
All authors made a significant contribution to the work reported, being involved in the conception, study design, execution, acquisition of data, analysis and interpretation. AC and HA have drafted the manuscript and arranged the figures. All authors substantially revised the article. All authors agreed on the journal this work should be submitted to. All authors reviewed and agreed on all versions of the article before submission, during revision, the final version accepted for publication, and any significant changes introduced at the proofing stage. Authors agree to take responsibility and be accountable for the contents of the article.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests for this work. The authors have no proprietary or commercial interest in any materials discussed in this article.
References
1. Holz FG, Tadayoni R, Beatty S, et al. Multi-country real-life experience of anti-vascular endothelial growth factor therapy for wet age-related macular degeneration. Br J Ophthalmol. 2015;99(2):220–226. doi:10.1136/bjophthalmol-2014-305327
2. Pieramici DJ, Wang PW, Ding B, Gune S. Visual and anatomic outcomes in patients with diabetic macular edema with limited initial anatomic response to ranibizumab in RIDE and RISE. Ophthalmology. 2016;123(6):1345–1350. doi:10.1016/j.ophtha.2016.02.007
3. Prunte C, Fajnkuchen F, Mahmood S, et al. Ranibizumab 0.5 mg treat-and-extend regimen for diabetic macular oedema: the RETAIN study. Br J Ophthalmol. 2016;100(6):787–795. doi:10.1136/bjophthalmol-2015-307249
4. Brown DM, Campochiaro PA, Bhisitkul RB, et al. Sustained benefits from ranibizumab for macular edema following branch retinal vein occlusion: 12-month outcomes of a Phase III study. Ophthalmology. 2011;118(8):1594–1602. doi:10.1016/j.ophtha.2011.02.022
5. Campochiaro PA, Brown DM, Awh CC, et al. Sustained benefits from ranibizumab for macular edema following central retinal vein occlusion: twelve-month outcomes of a phase III study. Ophthalmology. 2011;118(10):2041–2049. doi:10.1016/j.ophtha.2011.02.038
6. Nguyen AX, Gervasio KA, Wu AY. Differences in SARS-CoV-2 recommendations from major ophthalmology societies worldwide. BMJ Open Ophthalmology. 2020;5:e000525. doi:10.1136/bmjophth-2020-000525
7. Lai THT, Tang EWH, Chau SKY, Fung KSC, Li KKW. Stepping up infection control measures in ophthalmology during the novel coronavirus outbreak: an experience from Hong Kong. Graefes Arch Clin Exp Ophthalmol. 2020;258(5):1049–1055. doi:10.1007/s00417-020-04641-8
8. Hu VH, Watts E, Burton M, et al. Protecting yourself and your patients from COVID-19 in eye care. Community Eye Health. 2020;33(108):S1–S6.
9. Chu DK, Akl EA, Duda S, et al. Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: a systematic review and meta-analysis. Lancet. 2020;395(10242):1973–1987. doi:10.1016/S0140-6736(20)31142-9
10. Korobelnik JF, Loewenstein A, Eldem B, et al. Guidance for anti-VEGF intravitreal injections during the COVID-19 pandemic. Graefes Arch Clin Exp Ophthalmol. 2020;258(6):1149–1156. doi:10.1007/s00417-020-04703-x
11. Li JPO, Shantha J, et al. Preparedness among Ophthalmologists: during and Beyond the COVID-19 pandemic. Ophthalmology. 2020;127(5):569–572. doi:10.1016/j.ophtha.2020.03.037
12. Pei X, Jiao X, Lu D, Qi D, Huang S, Li Z. How to face COVID-19 in ophthalmology practice. Med Hypothesis Discov Innov Ophthalmol. 2020;9(3):164–171.
13. Schmidt-Erfurth U, Garcia-Arumi J, Gerendas BS, et al. Guidelines for the management of retinal vein occlusion by the European Society of Retina Specialists (EURETINA). Ophthalmologica. 2019;242(3):123–162. doi:10.1159/000502041
14. Seah IYJ, Anderson DE, Kang AEZ, et al. Assessing viral shedding and infectivity of tears in coronavirus disease 2019 (COVID-19) patients. Ophthalmology. 2020;127(7):977–979. doi:10.1016/j.ophtha.2020.03.026
15. Peng Y, Zhou YH. Is novel coronavirus disease (COVID-19) transmitted through conjunctiva? J Med Virol. 2020;92(9):1408–1409. doi:10.1002/jmv.25753
16. Larsen M, Waldstein SM, Boscia F, et al. Individualized ranibizumab regimen driven by stabilization criteria for central retinal vein occlusion: twelve-month results of the CRYSTAL study. Ophthalmology. 2016;123(5):1101–1111. doi:10.1016/j.ophtha.2016.01.011
17. Tadayoni R, Waldstein SM, Boscia F, et al. Sustained benefits of ranibizumab with or without laser in branch retinal vein occlusion: 24-month results of the BRIGHTER study. [published correction appears in Ophthalmology. 2018 Mar;125(3):463]. Ophthalmology. 2017;124(12):1778–1787. doi:10.1016/j.ophtha.2017.06.027
18. Rosenfeld PJ, Brown DM, Heier JS, et al. Ranibizumab for neovascular age-related macular degeneration. N Engl J Med. 2006;355:1419–1431. doi:10.1056/NEJMoa054481
19. Wecker T, Grundel B, Reichl S, et al. Anti-VEGF injection frequency correlates with visual acuity outcomes in pro re nata neovascular AMD treatment. Sci Rep. 2019;9:3301. doi:10.1038/s41598-019-38934-8
20. Ashraf M, Souka A, Adelman R. Predicting outcomes to anti-vascular endothelial growth factor (VEGF) therapy in diabetic macular oedema: a review of the literature. Br J Ophthalmol. 2016;100(12):1596–1604. doi:10.1136/bjophthalmol-2016-308388
21. Schmidt-Erfurth U, Garcia-Arumi J, Bandello F, et al. Guidelines for the management of diabetic macular edema by the European Society of Retina Specialists (EURETINA). Ophthalmologica. 2017;237(4):185–222. doi:10.1159/000458539
22. Koshy ZR, Dickie D. Aerosol generation from high speed ophthalmic instrumentation and the risk of contamination from SARS COVID19. Eye. 2020. doi:10.1038/s41433-020-1000-3
23. Zhou Y, Duan C, Zeng Y, et al. Ocular findings and proportion with conjunctival SARS-COV-2 in COVID-19 Patients. Ophthalmology. 2020;127(7):982–983. doi:10.1016/j.ophtha.2020.04.028
24. Patel R, Babady E, Theel ES, et al. Report from the American Society for Microbiology COVID-19 International Summit, 23 March 2020: value of Diagnostic Testing for SARS-CoV-2/COVID-19. mBio. 2020;11(2):e00722–00720. doi:10.1128/mBio.00722-20
25. Al-Muharraqi MA. Testing recommendation for COVID-19 (SARS-CoV-2) in patients planned for surgery - continuing the service and ‘suppressing’ the pandemic. Br J Oral Maxillofac Surg. 2020;58(5):503–505. doi:10.1016/j.bjoms.2020.04.014
26. Carmo A, Pereira-Vaz J, Mota V, et al. Clearance and persistence of SARS-CoV-2 RNA in patients with COVID-19. J Med Virol. 2020:1–5. doi:10.1002/jmv.26103.
27. Li R, Pei S, Chen B, et al. Substantial undocumented infection facilitates the rapid dissemination of novel coronavirus (SARS-CoV-2). Science. 2020;368(6490):489–493. doi:10.1126/science.abb3221
28. Gharebaghi R, Desuatels J, Moshirfar M, Parvizi M, Daryabari SH, Heidary F. COVID-19: preliminary clinical guidelines for ophthalmology practices. Med Hypothesis Discov Innov Ophthalmol. 2020;9(2):149–158.
29. Parrish RK
30. Green A. Li Wenliang. Lancet. 2020;395(10225):682. doi:10.1016/S0140-6736(20)30382-2
31. Liu Y, Yan L-M, Wan L, et al. Viral dynamics in mild and severe cases of COVID-19. Lancet Infect Dis. 2020;20(6):656–657. doi:10.1016/S1473-3099(20)30232-2
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.