Back to Journals » Drug Design, Development and Therapy » Volume 20
The Optimal Effective Concentration of Spinal Anesthesia for Interlaminar Endoscopic Lumbar Discectomy: An Approach Based on the Biased Coin Design
Authors Zhang L ![]() , Zhang Y, Li P
, Zhang Y, Li P ![]() , Hu B
, Hu B ![]() , Liu G, Zhu M
, Liu G, Zhu M ![]() , Yuan L, Xu Y
, Yuan L, Xu Y
Received 24 December 2025
Accepted for publication 14 April 2026
Published 18 April 2026 Volume 2026:20 591332
DOI https://doi.org/10.2147/DDDT.S591332
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Anastasios Lymperopoulos
Long Zhang,1,2,* Yu Zhang,1,2,* Ping Li,3 Bingwei Hu,4 Guanyi Liu,2,5 Miao Zhu,1,2 Liyong Yuan,1,2 Yaqing Xu1,2
1Department of Anesthesiology, Ningbo No.6 Hospital, Ningbo, Zhejiang, People’s Republic of China; 2Ningbo Clinical Research Center for Orthopedics, Sports Medicine & Rehabilitation, Ningbo, Zhejiang, People’s Republic of China; 3Department of Anesthesiology, Ningbo Medical Center Lihuili Hospital, Ningbo, Zhejiang, People’s Republic of China; 4Department of Anesthesiology, Tongde Hospital of Zhejiang Province, Hangzhou, Zhejiang, People’s Republic of China; 5Spine Surgery Center, Ningbo No.6 Hospital, Ningbo, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yaqing Xu, Department of Anesthesiology, Ningbo No.6 Hospital, No. 1059 Zhongshan East Road, Ningbo, Zhejiang, 315040, People’s Republic of China, Email [email protected]
Purpose: To determine the optimal spinal anesthesia concentration for interlaminar endoscopic lumbar discectomy (IELD), in order to deliver precise and individualized anesthesia for this procedure.
Methods: Fifty-four patients scheduled for IELD were randomized via a biased coin design to receive spinal anesthesia with different ropivacaine doses. The initial dose was 7.5 mg/3 mL. If the patient reported a negative outcome, the subsequent dose was increased by 0.75 mg. If a positive outcome was reported, subsequent dose remained unchanged (89% probability) or was decreased by 0.75 mg (11% probability). At least 45 positive outcomes were needed to estimate the MEC90. Outcome measures: onset and duration of surgical analgesia, postoperative pain scores, urinary retention incidence, end-of-surgery modified Bromage score, and patient satisfaction.
Results: The isotonic regression estimated the MEC90 of ropivacaine for spinal anesthesia in IELD at 9.474 mg/3 mL (95% CI: 8.242– 10.088); Probit regression yielded MEC90 = 9.480 mg/3 mL (95% CI: 8.806– 10.154), MEC95 = 9.932 mg/3 mL (95% CI: 8.957– 10.907), and MEC99 = 10.779 mg/3 mL (95% CI: 9.122– 12.436). Analgesia onset was 5.0 min (IQR: 5.0– 7.0), lasting 100.0 min (IQR: 90.0– 110.0). Postoperative pain scores (VAS, cm) at 2, 6, 12, and 24 hours were 2.0 (1.0– 3.0), 2.0 (2.0– 2.0), 2.0 (2.0– 3.0), and 2.0 (2.0– 2.0), respectively. Bromage score at surgery end was 4.5 (IQR: 3.0– 5.0). Mild urinary retention occurred in 4 patients (7.4%); no other complications were observed. Patient satisfaction: excellent (53.7%), good (20.4%), fair (13.0%), poor (5.6%), very poor (7.4%). Ropivacaine concentration was negatively correlated with analgesia onset time (r = − 0.228, P = 0.049) and Bromage score (r = − 0.235, P = 0.044), but not associated with analgesia duration (r = 0.105, P = 0.224).
Conclusion: The MEC90 of ropivacaine for spinal anesthesia in IELD was 9.474 mg/3 mL, the clinically recommended dose was 9.5 to 10.5 mg/3 mL.
Plain Language Summary: Interlaminar Endoscopic Lumbar Discectomy (IELD) is a minimally invasive procedure for lumbar disc herniation; however, the optimal dosing of spinal anesthesia remains unclear. Using a biased-coin up-and-down sequential design, this study determined the effective intrathecal ropivacaine concentrations for IELD. The MEC90 was 9.47 mg/3 mL. Sensory blockade onset occurred at approximately 5 minutes (range: 5– 7 min); duration was approximately 100 minutes (90– 110 min). Postoperative VAS scores remained stable at approximately 2 cm over 24 hours. At the end of surgery, the median Bromage score was 4.5 (range: 3– 5), indicating moderate motor blockade. Four patients (7%) experienced mild urinary retention; no other adverse events occurred. Patient satisfaction was as follows: 54% rated the anesthesia “excellent”, 20% “good”, 13% “fair”, and 13% “poor” or “very poor”. Higher ropivacaine concentrations shortened the onset time and increased the degree of motor blockade (reflected by higher Bromage scores) but did not prolong the duration of sensory blockade. These findings support evidence-based ropivacaine dosing for spinal anesthesia in IELD, thereby improving safety, efficacy, and clinical decision-making.
Keywords: spinal anesthesia, interlaminar endoscopic lumbar discectomy, biased coin design, optimal effective concentration, anesthesia success rate
Introduction
Interlaminar endoscopic lumbar discectomy (IELD) serves as a crucial procedure for the treatment of lumbar disc herniation, owing to its minimally invasive characteristics, rapid recovery, minimal blood loss, and shorter hospital stay.1,2
Current empirical evidence indicates that spinal anesthesia confers substantial advantages over other methods in IELD, encompassing superior intraoperative efficacy, heightened patient comfort, fewer postoperative cardiopulmonary complications, and reduced healthcare expenditures.3–5 Compared with local anesthesia, spinal anesthesia can provide more perfect analgesic effect, avoid the surgical stimulation and discomfort that patients may feel in the awake state, and also create more stable surgical conditions for the surgeon.3–6 Compared with general anesthesia, spinal anesthesia can significantly reduce the risk associated with airway management and minimize the interference of anesthetics on the physiological functions of patients, particularly for elderly patients with underlying diseases or individuals with a higher ASA grade.6,7
However, the determination of the optimal local anesthetic dose for spinal anesthesia in IELD still remains a critical clinical challenge.8 These multifaceted challenges underscore the critical necessity of developing a comprehensive anesthetic strategy that effectively balances the precise demands of the surgical procedure with the imperative for swift and complete functional recovery in patients. Inadequate dosing may lead to insufficient analgesia, which in turn can cause intraoperative pain, patient discomfort, and potential surgical complications. On the other hand, excessive dosing can elevate the risk of adverse events such as prolonged motor blockade, urinary retention, and delayed recovery.5,9
The utilization of low-concentration spinal anesthesia has been increasingly recognized as a superior approach, as it is associated with a significant reduction in both intraoperative and postoperative complications. More importantly, this method actively promotes and accelerates the overall process of postoperative recovery, enabling patients to regain functionality more rapidly and comfortably.8,10
Ropivacaine, a long-acting amide local anesthetic with a favorable safety profile and less motor blockade than bupivacaine, has gained widespread use in spinal anesthesia.11–13 Nevertheless, high-quality evidence on the minimum effective concentration (MEC) of ropivacaine—particularly the MEC90 (ie, the concentration producing effective anesthesia in 90% of patients)—remains scarce, especially for patients with IELD. This knowledge gap hinders anesthesiologists’ ability to select optimal doses that balance efficacy and safety in this specific surgical population.
Biased coin design up-and-down sequential method is a valuable tool in this context. It allows for a systematic and efficient way to determine the optimal concentration of local anesthetics.14,15 By using this method, we can precisely titrate the ropivacaine concentration based on the patient’s response.
Therefore, the present study was designed to determine the MEC90 of intrathecal ropivacaine for spinal anesthesia in patients undergoing IELD by using a biased coin up-and-down sequential design, with the aim of providing evidence-based guidance for clinical practice.
Materials and Methods
This study utilized a biased coin design up-and-down method to determine the optimal effective concentration of ropivacaine for spinal anesthesia in patients undergoing IELD. Ethical approval was obtained from the Ethics Committee of Ningbo No. 6 Hospital on March 11, 2024, with the reference number 2024–02 (K). Subsequently, the study was registered on April 9, 2024, in the Chinese Clinical Trial Registry (www.chictr.org.cn) under the registration number ChiCTR2400082845.
Patient Enrollment
Eligible patients were adult individuals who were scheduled for IELD due to lumbar disc herniation from May 1, 2024, to August 31, 2025. The inclusion criteria were that patients required IELD surgery for lumbar disc herniation at the L4/5 and/or L5/S1 segments, American Society of Anesthesiologists (ASA) physical status classification of grade I–III, an age range of 18 to 65 years, and a body mass index (BMI) ranging from 18.5 to 30 kg/m2. Each participating patient was required to comprehensively understand the content, purpose, and risks of the trial and voluntarily sign the informed consent form.
The exclusion criteria included patients with allergies to local anesthetic agents or contraindications to spinal anesthesia, individuals with intellectual disabilities or communication impairments, those with a history of psychiatric disorders, and participants who had been enrolled in other clinical trials. In the event that a patient voluntarily requests withdrawal from the study during the trial, is lost to follow-up, or experiences severe complications, they was excluded from the study.
Outcomes
The primary outcome measure was the analgesic response after spinal anesthesia, assessed using the visual analog scale (VASpain) score. The positive outcome was VASpain = 0, and the negative outcome was VASpain ≥ 1. Secondary outcomes included the onset time of pain block (defined as the time interval from the end of drug injection to the absence of pain during needle puncture in the surgical area, measured every two minutes after drug administration) and its duration (defined as the absence of pain during needle puncture in the surgical area until the patient starts to feel pain at the puncture site), postoperative pain scores, the incidence of urinary retention (defined as postoperative functional inability to urinate or difficulty in urination, excluding organic changes), and patient satisfaction. In addition, record the patient’s baseline information, such as gender, age, BMI, ASA classification, operation time, and lumbar segment.
At the conclusion of the surgery, the motor block status was assessed in accordance with the modified Bromage scale: a score of 1 signified complete motor block; a score of 2 denoted that only the joints below the ankle were capable of movement; a score of 3 indicated that only the knee joint could be moved; a score of 4 meant that the leg could be lifted but not held in that position; a score of 5 signified that the leg could be lifted and maintained for over 10 seconds; and a score of 6 indicated no motor block whatsoever.16,17
Patient satisfaction scores were gathered 24 hours post-surgery using a 5-point scale, where 1 represented very poor, 2 represented poor, 3 represented fair, 4 represented good, and 5 represented excellent.
Sequential Method for Biased Coins
Based on clinical experience and previous literature, the first patient was given a dose of 7.5 mg ropivacaine, and the volume was maintained at 3 mL.10 When the patient had a negative outcome (VAS ≥ 1), the dose of ropivacaine for the subsequent patient was increased by 0.75 mg until the first patient with a positive outcome was identified. Starting from the first patient with a positive outcome (VAS = 0), if the previous patient had a negative outcome, the dose of ropivacaine for this patient was increased by 0.75 mg. Conversely, if the previous patient had a positive outcome, the concentration of ropivacaine for this patient was randomly adjusted through a biased coin toss. There was an 11% probability of a 0.75 mg decrease and an 89% probability of remaining unchanged. A minimum of 45 positive outcome was necessary to estimate the MEC90.14,15,18
Randomization and Blinding
A computer generated a random sequence of 44 numbers marked with −1 or 0, with probabilities of 11% and 89% respectively. Here, −1 denoted a reduction of one unit in the dose of ropivacaine, while 0 signified that the dose of ropivacaine for the subsequent patient remained unchanged. The sequence was concealed via the envelope method. When a positive result is encountered, open the envelope to determine whether the dose for the next patient should be maintained or reduced. In the event that a patient withdrew from the study, the data of this patient was removed, and the dose of the drug for the next patient remained unchanged. All ropivacaine solutions utilized were prepared by an individual not involved in the study, and the labels were hidden. Neither the anesthesiologists nor the observers were aware of the concentration of the drug employed.
Spinal Anesthesia
The patient was placed in a lateral flexed position with the operating table level. After routine disinfection and draping, the L3/4 intervertebral space was identified as the puncture site, and a small amount of 1% lidocaine was injected at the puncture site for local infiltration anesthesia. The puncture needle was slowly inserted into the subarachnoid space via a median approach. After confirming cerebrospinal fluid outflow, needle advancement was halted, and 3 mL of isotonic ropivacaine hydrochloride solution (Naropin®, Sweden, AstraZeneca AB) prepared with normal saline was slowly injected into the head end at a rate of 1 mL/10s. Following injection completion, the patient remained in a supine position for 15 minutes until the anesthesia level stabilized and ensure that the sensory block plane covers the surgical area, after which the position was adjusted to a surgical-ready position.
IELD
The patient was placed on the operating table and positioned in the prone position. Before the operation, precise imaging localization was performed using a C-arm X-ray machine to determine the needle insertion point. Under X-ray fluoroscopy guidance, a 23-gauge guide needle was inserted near the lateral boundary of the intervertebral foramen. Subsequently, a 0.8 mm diameter guide wire was used to replace the guide needle, and a dilator was used to open the paraspinal muscles to establish a working channel. Fluoroscopy was used to confirm that the working channel was accurately located at the lateral edge of the interlaminar opening. A spinal endoscopy system (Joimax Inc., Irvine, California, USA) was used to perform an incision at the junction of the ligamentum flavum and the facet joint, exposing the lateral edge of the nerve root, and directly observing and removing the protruding part of the intervertebral disc. After nerve root decompression and hemostasis were completed, the endoscope and working channel were safely removed.
Rescue Analgesia
For any moment during the operation when the patient experiences moderate to severe pain (VAS > 3), local injection of lidocaine for rescue analgesia was administered first. The pain degree was assessed every 5 minutes. If the VAS remains above 3, sufentanil 5 μg was added. If the pain is still not relieved after five minutes, another 5 μg of sufentanil was given. If the analgesic effect is still unsatisfactory, general anesthesia was changed to after obtaining the patient’s consent.
Statistics
Statistical analysis was performed using SPSS software (version 26.0), GraphPad Prism software (version 8.0.1), and R for Windows software (version 4.3.2). The Shapiro–Wilk test was initially applied to assess the normality of continuous data. For normally distributed measurement data, results were described as mean ± standard deviation (Mean ± SD); for non-normally distributed measurement data, median (M) and interquartile range (IQR) were used for representation. Count data were presented as frequencies and percentages (%). The MEC90 and 95% confidence interval (CI) of the drug were calculated using isotonic regression and validated with Probit regression.14 Spearman’s rank correlation analysis was adopted to explore the relationship between variables, and a one-tailed test was conducted.
Results
Fifty-nine patients were assessed for eligibility. Three patients were excluded due to contraindications to spinal anesthesia, and one patient was excluded due to communication impairments. Then, fifty-five patients were enrolled in this study, and one patient was lost to follow-up due to a second surgery. Finally, fifty-four patients, aged 47.5 ± 11.3 years, were analyzed in this study (Figure 1). The patients’ height was 1.66 ± 0.08 m, their weight was 66.54 ± 11.35 kg, and their BMI was 24.06 ± 2.98 kg/m2. There were 32 males (59.3%) and 22 females (40.7%). Twenty-one patients (38.9%) were classified as ASA grade I, 20 patients (37.0%) as grade II, and 13 patients (24.1%) as grade III. The distribution of ropivacaine doses used for patients at various ASA grades is shown in Figure 2. The operation time was 61.6 (45.0, 81.3) min. There were 14 cases (25.9%) where the surgical segment was at L4/L5, 23 cases (42.6%) at L5/S1, and 17 cases (31.5%) involving both segments (Table 1).
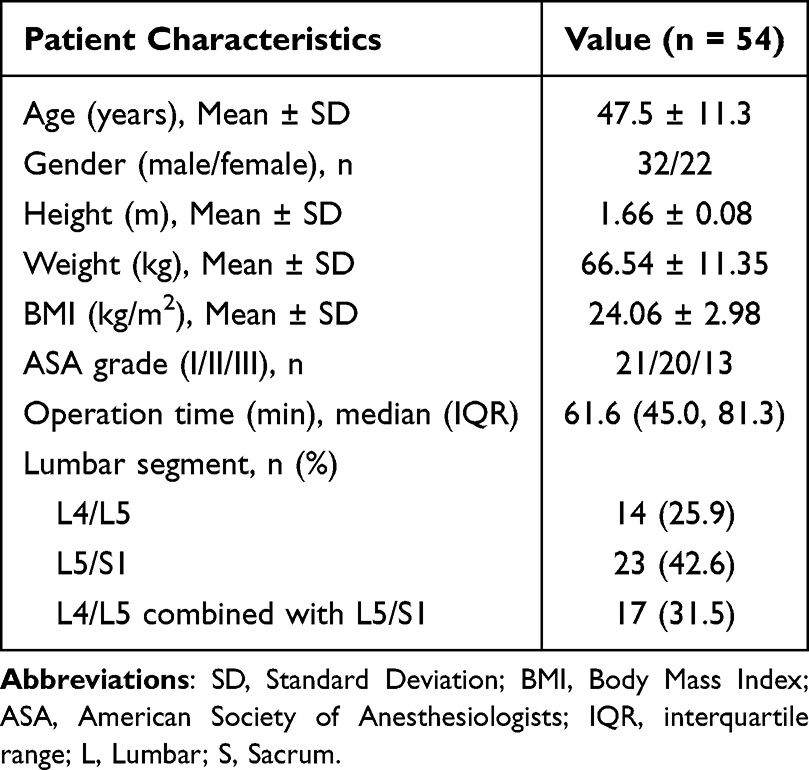 |
Table 1 Demographic Characteristics |
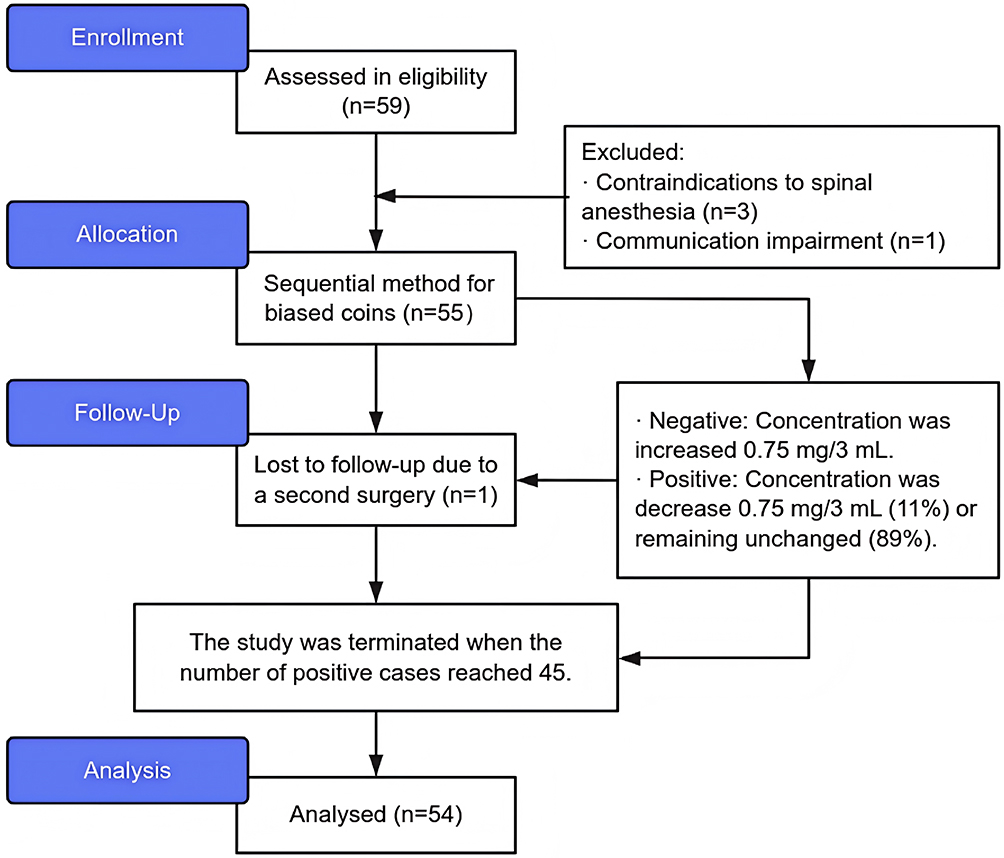 |
Figure 1 Research flowchart. |
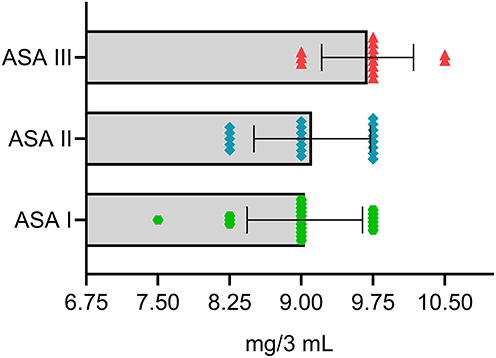 |
Figure 2 The distribution of ropivacaine doses used for patients at various ASA grades. Abbreviation: ASA, American Society of Anesthesiologists. |
The isotonic regression results indicated that the MEC90 of ropivacaine for spinal anesthesia in IELD was 9.474 mg/3 mL (0.318%), and the 95% CI was 8.242 mg/3 mL (0.275%) to 10.088 mg/3 mL (0.336%) (Figure 3). The Probit regression results indicated that the MEC90 was 9.480 mg/3 mL (95% CI: 8.806–10.154), the MEC95 was 9.932 mg/3 mL (95% CI: 8.957–10. 907), and the MEC99 was 10.779 mg/3 mL (95% CI: 9.122–12.436) (Figure 4).
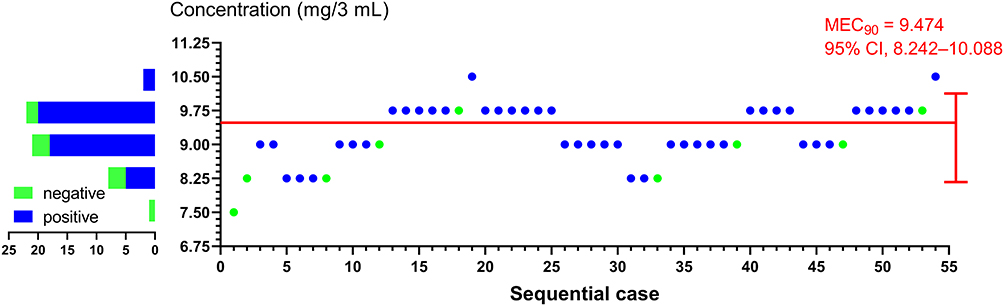 |
Figure 3 Sequential data for the complete BCD are presented to the right of the ordinate. Negative cases are indicated by green dots (●), positive cases by blue dots (●), and an estimate of MEC90 and 95% CI is represented by a red line (━). The bar chart on the left depicts the number of usage cases and their distribution at each concentration. Abbreviations: MEC, minimal effective concentration; CI, confidence interval. |
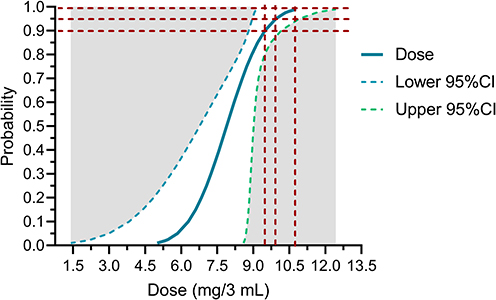 |
Figure 4 Dose-response curve based on Probit regression results. The red dashed lines correspond to MEC90, MEC95, and MEC99, respectively. Abbreviations: MEC, minimal effective concentration; CI, confidence interval. |
The onset time of pain block was 5.0 (5.0, 7.0) min, and its duration was 100.0 (90.0, 110.0) min. The postoperative pain scores at 2 hours, 6 hours, 12 hours, and 24 hours were 2.0 (1.0, 3.0) cm, 2.0 (2.0, 2.0) cm, 2.0 (2.0, 3.0) cm, and 2.0 (2.0, 2.0) cm, respectively. The Bromage score at the end of the surgery was 4.5 (3.0, 5.0). Four patients (7.4%) experienced mild urinary retention, and no other discomfort or complications were found in any of the patients. Twenty-nine patients (53.7%) were very satisfied, 11 patients (20.4%) were satisfied, 7 patients (13.0%) thought the anesthetic effect was average, 3 patients (5.6%) considered the anesthetic effect poor, and 4 patients (7.4%) expressed extreme dissatisfaction with the anesthetic effect (Table 2). All nine negative cases underwent further management and successfully completed the surgery. Among these cases, three patients required only one additional local anesthesia, five patients received a combination of local anesthesia and intravenous analgesics, and one patient was ultimately converted to general anesthesia.
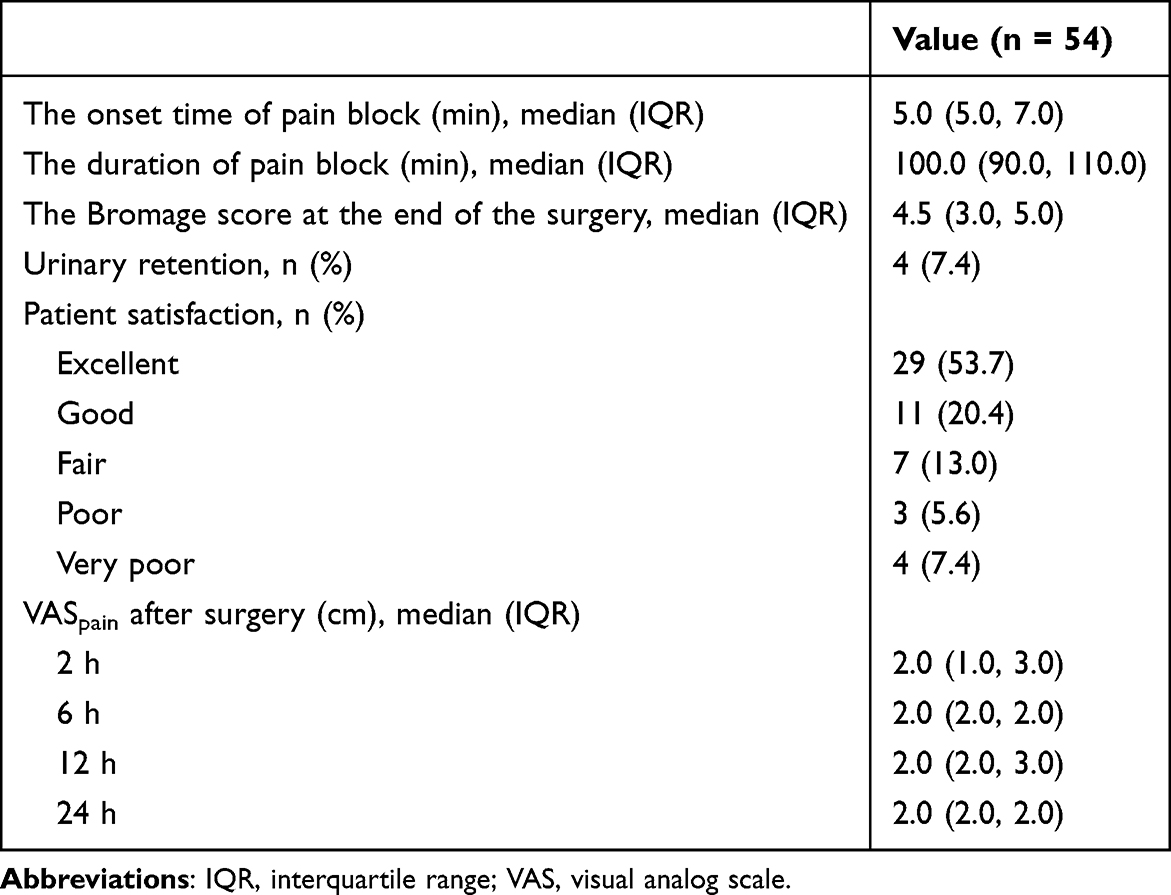 |
Table 2 Clinical Outcomes |
The results of the correlation analysis demonstrated that the concentration of ropivacaine was significantly negatively correlated with the onset time of analgesia (r = −0.228, P = 0.049), and positively correlated with the duration of the analgesic effect; however, this correlation was not significant (r = 0.105, P = 0.224). Moreover, it was also significantly negatively correlated with the Bromage score at the end of the surgery (r = −0.235, P = 0.044) (Figure 5).
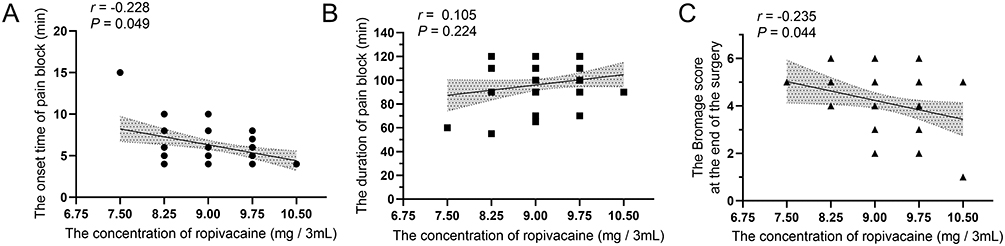 |
Figure 5 Correlations between ropivacaine concentration and analgesic block characteristics. Scatter plots showing the relationship of ropivacaine concentration (mg/3 mL) with (A) the onset time of pain block, (B) the duration of pain block, and (C) the Bromage score at the end of surgery. A linear regression line with a 95% confidence interval (gray shading) is displayed in each panel. |
Discussion
This study investigates a clinical trial utilizing a biased coin design to determine the optimal concentration of ropivacaine for spinal anesthesia in patients undergoing IELD. This study finally showed that the MEC90 of ropivacaine for spinal anesthesia in IELD was 9.474 mg/3 mL (0.318%), and the 95% CI was 8.242 mg/3 mL (0.275%) to 10.088 mg/3 mL (0.336%). This study also utilized Probit regression to validate the experimental results. The outcomes indicated that the MEC90 was 9.480 mg/3 mL (95% CI: 8.806–10.154), the MEC95 was 9.932 mg/3 mL (95% CI: 8.957–10. 907), and the MEC99 was 10.779 mg/3 mL (95% CI: 9.122–12.436). The similarity between the two sets of results further corroborated the reliability of the research findings.
The choice of ropivacaine, a long-acting amino amide local anesthetic, was deliberate, given its favorable safety profile and lower potential for cardiotoxicity compared to other agents.11,12 Its use in spinal anesthesia has been shown to produce reliable sensory and motor blockade with a predictable duration, making it an ideal candidate for dose-response studies in the context of IELD procedures.11–13
In this study, the positive indicator was set as a VAS score of 0, which is a relatively strict criterion and differs from other studies.14 By adopting this strict standard, the application effect of ropivacaine in spinal anesthesia can be evaluated more precisely, reducing the error caused by individual subjective pain perception differences. Compared with other studies that use relatively loose standards, the results of this study have higher reliability and persuasiveness. More importantly, the primary advantage of spinal anesthesia compared to local anesthesia lies in its distinct and powerful analgesic effect.5 Weakening this effect would strip it of its crucial clinical value.
The clinical implications of the findings are significant. From a clinical application perspective, the determined MEC offer clear reference benchmarks for clinicians when selecting ropivacaine for IELD spinal anesthesia. In actual clinical practice, physicians can flexibly adjust the drug concentration within this reference range according to the patient’s specific circumstances, such as age, physical state, and surgical complexity, to attain the optimal anesthetic effect.19 For instance, in the case of patients with good physical tolerance and high complexity surgeries, the drug concentration can be appropriately increased to approach MEC95 or even MEC99. This ensures that the patient experiences no pain and has good muscle relaxation during the surgery. On the other hand, for patients who are physically frail and have poor drug tolerance, a concentration close to MEC90 can be selected to guarantee the anesthetic effect while minimizing the risk of adverse drug reactions.8 Therefore, considering pharmacological principles, clinical practice, and the convenience of drug formulation, the recommended clinical dose of ropivacaine in this study is 9.5 to 10.5 mg/3 mL.
It is noteworthy that, in addition to the type and dosage of local anesthetic agents, the specific gravity (density) of the drug and the injection speed are also critical factors influencing the diffusion range of the drug in interstitial tissues, distribution uniformity, and the stability of final anesthetic efficacy.20,21 During the experimental design phase, this study deliberately adopted standardized drug concentration ratio protocols and implemented strictly uniform slow injection speeds throughout all procedural steps, aiming to minimize systematic biases introduced by these variables and ensure the intrinsic comparability of research data and the reliability of conclusions. However, in the complex and dynamic clinical practice environment, due to individual anatomical variations among patients, differences in operator techniques, and site-specific characteristics, healthcare professionals must exercise heightened attention and meticulous consideration toward these factors—namely, the specific gravity properties of the drug and injection push rates—during clinical application. These factors directly and significantly impact the onset time of anesthesia, the completeness of block formation, and potential complication risks, ultimately determining the safety and efficacy of clinical anesthesia.
In addition, certain factors may also influence the research results regarding drug dosage. Apart from the well-known factors like age and obesity, the specification of the puncture needle is also an influencing factor. Research indicates that for spinal anesthesia during cesarean section, the minimum effective dose of ropivacaine required when using a real-time UG 26 spinal needle is significantly higher than that of a 24-gauge needle. This might be because the diameter of the spinal needle significantly impacts the diffusion rate of ropivacaine in the spinal canal.22 Meanwhile, despite the absence of direct evidence, it remains challenging to exclude the possibility that the puncture approach (eg, the midline approach or the paramedian approach) exerts an influence on the research results. Moreover, height could also serve as an independent influencing factor. Research findings have demonstrated that, in the context of spinal anesthesia for cesarean section, the ED50 of ropivacaine rises in tandem with the increase in the subjects’ height, suggesting that height may partially determine the dosage.23 Finally, the combined use of intravenous analgesics (eg, opioid analgesics) may also influence the dosage of ropivacaine in spinal anesthesia, and this effect is generally advantageous.24,25
Compared with other studies, the effective concentration of ropivacaine for IELD spinal anesthesia determined in this study falls within a reasonable and reference-worthy range.10,26 The effective concentrations obtained in previous studies might have fluctuated because of differences in surgical methods, sample sizes, research methods, or patient groups.
Previous related studies have demonstrated that 10 mg of ropivacaine for spinal anesthesia can attain satisfactory anesthetic effects during hemorrhoidectomy and exerts a relatively minor influence on postoperative urinary retention.26 Another study determined that when ropivacaine spinal anesthesia was applied in anorectal surgery, its MEC90 was only 0.248% (3.732 mg, 95% CI: 0.150%–0.300%), and the MEC99 was 0.293% (4.439 mg, 95% CI: 0.250%–0.300%).27 The dosage of ropivacaine in that study (rather than the concentration) was significantly lower than the results of this study. This clearly demonstrates that different surgeries have distinct requirements for the block effect. The required block range for anorectal surgery is relatively narrow, and only local anesthesia is necessary. In contrast, IELD surgery may involve a broader range of tissues and nerves and has more rigorous requirements for the range and depth of anesthesia. Therefore, a higher concentration of ropivacaine is required to achieve the ideal anesthetic effect. Additionally, the duration of the surgery is also a crucial factor. Anorectal surgery typically takes less time, whereas IELD surgery may necessitate longer-term maintenance of anesthesia, and a higher drug concentration facilitates maintaining a stable anesthetic state over a longer period.
Studies have demonstrated that when low-density ropivacaine is employed for unilateral spinal anesthesia in elderly patients undergoing hip replacement surgery, the median effective dose (ED50) and 95% effective dose (ED95) are 11.13 mg (95% CI: 10.85–11.42 mg) and 13.30 mg (95% CI: 12.04–13.65 mg), respectively. Unilateral spinal anesthesia can confine the block level to the surgical side, induce less physiological disturbance to the patient, maintain more stable perioperative hemodynamics, and lead to relatively fewer complications.10 This research result is consistent with the findings of this study. However, it is necessary to emphasize the influence of drug concentration and administration method on the research result.28
This study also concentrated on the onset and duration of pain block, postoperative pain scores, lower-extremity movement at the end of surgery, the incidence of urinary retention, and patient satisfaction. These indicators comprehensively mirror the influence of the anesthesia effect on the postoperative recovery of patients. The correlation analysis results further explained the relationship between the ropivacaine concentration and important indicators. The significant negative correlation between the ropivacaine concentration and the onset time of analgesia suggests that a higher concentration of ropivacaine can lead to a faster onset of pain relief. The non-significant positive correlation with the duration of the analgesic effect implies that while there may be a tendency for a longer-lasting effect with higher concentrations, other factors may also play important roles. This is basically consistent with the previous research viewpoints.29
This study also discovered that there was a negative correlation between the concentration of ropivacaine used in spinal anesthesia and the Bromage score at the end of the surgery. This finding suggests that the lower the concentration of ropivacaine, the less influence it exerts on motor function.13 This is also fundamentally consistent with previous research viewpoints. Reducing motor blockage is conducive to the early recovery of limb movement in patients after surgery and reduces the incidence of complications.13 More importantly, the risk of accidental nerve contact is relatively high during IELD surgery. Maximally preserving motor function is conducive to the timely detection of nerve damage. Once the patient perceives abnormal motor responses during the surgery, it can promptly alert the surgeon to adjust the surgery, thereby preventing further nerve damage. This is crucial for ensuring the patient’s surgical safety and the post-operative recovery of nerve function.14
In addition, this study analyzed the incidence of urinary retention and patient satisfaction. The incidence of urinary retention in this study was relatively low, which could be attributed to the relatively minor impact of the lower concentration of ropivacaine on bladder function. A higher drug concentration may increase the risk of urinary retention, possibly because of the excessive inhibition of the nerves controlling the bladder.30 Meanwhile, it was also found that the occurrence of urinary retention was dependent on population characteristics, with elderly men still facing a higher risk. Urinary retention not only causes discomfort to patients but also increases the risk of complications such as urinary tract infections.26 Therefore, this group of individuals still merits more attention.
In terms of patient satisfaction, although more than half of the patients were very satisfied or satisfied with the anesthetic effect, there was still a proportion of patients who were not satisfied. This may be related to individual differences in pain perception, the anesthetic effect, and other factors.3,31 Future research could focus on ways to further improve patient satisfaction, such as optimizing the anesthetic protocol, better preoperative communication, and individualized anesthetic plans.
In addition, no other severe anesthesia-related complications were observed during the study. Despite the relatively higher ropivacaine concentration distribution in ASA III patients, the procedure still demonstrated good safety. Overall, this study contributes to the growing body of evidence supporting the use of enhanced recovery after surgery (ERAS) pathways in neurosurgical practice. By refining anesthesia protocols specifically for endoscopic spinal surgery, we pave the way for the development of standardized ERAS protocols that can be widely adopted and implemented, ultimately leading to better patient experiences and outcomes.32
This study also presents certain limitations. The sample size is relatively small, and the source population is limited, which might impact the generalizability of the research findings. Future studies ought to conduct large-scale multi-center clinical trials to further validate the outcomes of this study. Moreover, this study solely concentrated on the concentration of ropivacaine and did not carry out in-depth investigations into other factors that could influence the anesthetic effect, such as drug compatibility and injection techniques. Future research can further enlarge the sample size and incorporate more patients of diverse ages and physical states to enhance the universality of the research results. It is also feasible to compare the application effects of different anesthetic drugs or approaches in ILDE surgery to offer more choices and references for clinical practice. Simultaneously, in-depth research on the relationship between ropivacaine concentration and individual patient factors (such as genes and metabolism) to formulate personalized anesthetic plans were a crucial direction for improving anesthetic quality and patient prognosis.
Conclusion
The MEC90 of ropivacaine for spinal anesthesia in IELD was 9.474 mg/3 mL. The clinically recommended dose was 9.5 to 10.5 mg/3 mL.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article. The datasets used and/or analyzed during the current study are also available from the author (Dr. Long Zhang, [email protected]) upon reasonable request.
Ethics Approval and Informed Consent
The study was approved by the Ethics Committee of Ningbo No. 6 Hospital on March 11, 2024, with the reference number 2024-02 (K), and was performed in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants. Subsequently, the study was registered on April 9, 2024, in the Chinese Clinical Trial Registry (www.chictr.org.cn) under the registration number ChiCTR2400082845.
Consent for Publication
Written informed consent was obtained from all patients, their legally authorized representatives, or their guardians for the publication of this report.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was financially supported by the Science and Technology Project for Agricultural and Social Development in Yinzhou District (No. 2024AS036), Ningbo Clinical Research Center for Orthopedics, Sports Medicine & Rehabilitation (2024L004), and Zhejiang Provincial Medical and Health Science and Technology Project (No. 2025HY0880, 2025HY1076, and 2025HY1078).
Disclosure
Long Zhang and Yu Zhang are co-first authors for this study. All authors declare that the implementation of this study, data analysis, or interpretation of the results have no economic or non-economic associations that could be construed as conflicts of interest.
References
1. Pan M, Li Q, Li S, et al. Percutaneous endoscopic lumbar discectomy: indications and complications. Pain Physician. 2020;23(1):49–12.
2. Ahn Y. Endoscopic spine discectomy: indications and outcomes. Int Orthop. 2019;43(4):909–916. doi:10.1007/s00264-018-04283-w
3. Vural C, Yorukoglu D. Comparison of patient satisfaction and cost in spinal and general anesthesia for lumbar disc surgery. Turk Neurosurg. 2014;24(3):380–384. doi:10.5137/1019-5149.JTN.8575-13.0
4. Liu G, Zhao J, Yuan L, et al. Spinal anesthesia for L5-S1 interlaminar endoscopic lumbar discectomy: a retrospective study[J]. BMC Musculoskelet Disord. 2023;24(1):818. doi:10.1186/s12891-023-06956-z
5. Liu G, Zhang J, Zhang L, et al. Comparison of spinal anesthesia and local anesthesia in percutaneous interlaminar endoscopic lumbar discectomy for L5/S1 disc herniation: a retrospective cohort study. BMC Musculoskelet Disord. 2024;25(1):774. doi:10.1186/s12891-024-07898-w
6. Ye XF, Wang S, Wu AM, et al. Comparison of the effects of general and local anesthesia in lumbar interlaminar endoscopic surgery. Ann Palliat Med. 2020;9(3):1103–1108. doi:10.21037/apm-20-623
7. Mooney J, Laskay N, Erickson N, et al. General vs local anesthesia for percutaneous endoscopic lumbar discectomy (peld): a systematic review and meta-analysis. Global Spine J. 2023;13(6):1671–1688. doi:10.1177/21925682221147868
8. Wang Y, Zha H, Fang X, et al. Dose selection of ropivacaine for spinal anesthesia in elderly patients with hip fracture: an up-down sequential allocation study. Clin Interv Aging. 2022;17:1217–1226. doi:10.2147/CIA.S371219
9. Critchley LA. Hypotension, subarachnoid block and the elderly patient. Anaesthesia. 1996;51(12):1139–1143. doi:10.1111/j.1365-2044.1996.tb15051.x
10. Lin C, Xian WL, Xu J, et al. ED50 and ED95 of hypobaric ropivacaine during unilateral spinal anesthesia in older patients undergoing Hip replacement surgery. Front Med Lausanne. 2025;12:1571574. doi:10.3389/fmed.2025.1571574
11. Casati A, Santorsola R, Cerchierini E, et al. Ropivacaine[J]. Minerva Anestesiol. 2001;67(9 Suppl 1):15–19.
12. Zink W, Graf BM. Benefit-risk assessment of ropivacaine in the management of postoperative pain[J]. Drug Saf. 2004;27(14):1093–1114. doi:10.2165/00002018-200427140-00003
13. Zheng T, Ye P, Wu W, et al. Minimum local anesthetic dose of ropivacaine in real-time ultrasound-guided intraspinal anesthesia for lower extremity surgery: a randomized controlled trial. Ann Transl Med. 2020;8(14):861. doi:10.21037/atm-20-3805
14. Hu B, Li L, Wang H, et al. Determining the minimum effective concentration of ropivacaine in epidural anesthesia for tolerable pain in transforaminal percutaneous endoscopic lumbar discectomy to avoid nerve injury: a double-blind study using a biased-coin design. Drug Des Devel Ther. 2022;16:315–323. doi:10.2147/DDDT.S334605
15. Li P, Yang Z, Zhang L, et al. Minimum effective concentration of ropivacaine for ultrasound-guided RISS block in VATS: a biased coin design approach. Drug Des Devel Ther. 2025;19:4151–4161. doi:10.2147/DDDT.S520427
16. Wang J, Xia F, Wang LY, et al. Effect of epidural volume extension using low-dose sufentanil combined with low-concentration ropivacaine on visceral pain during cesarean sections: a randomized trial. Pain Physician. 2024;27(10):E1065–E1071.
17. Breen TW, Shapiro T, Glass B, et al. Epidural anesthesia for labor in an ambulatory patient. Anesth Analg. 1993;77(5):919–924. doi:10.1213/00000539-199311000-00008
18. Sotthisopha T, Elgueta MF, Samerchua A, et al. Minimum effective volume of lidocaine for ultrasound-guided costoclavicular block. Reg Anesth Pain Med. 2017;42(5):571–574. doi:10.1097/AAP.0000000000000629
19. Sun S, Yin Q, Shen J, et al. The 90% minimum effective volume and concentration of lidocaine for ultrasound-guided stellate ganglion blocks in adults: a biased-coin design, up-and-down sequential allocation trial. Korean J Anesthesiol. 2025;78(5):471–481. doi:10.4097/kja.24607
20. Qiao W, Liu L, Zhang X, et al. Heavy gravity combined with light gravity local anesthetic in subarachnoid anesthesia for cesarean section did not reduce the incidence of intraoperative hypotension in maternal women: a prospective cohort study. BMC Anesthesiol. 2025;25(1):22. doi:10.1186/s12871-025-02895-5
21. Sakura S. Factors influencing the level of spinal anesthesia: (I). Characteristics of anesthetic solutions. Masui. 2000;49(1):18–25.
22. Zheng C, Fan H, Ye P, et al. Minimum local anesthetic dose of ropivacaine in cesarean section for real-time ultrasound-guided spinal anesthesia using 24-gauge versus 26-gauge needles based on fluid simulation technology: a randomized controlled trial. Drug Des Devel Ther. 2024;18:4401–4412. doi:10.2147/DDDT.S476710
23. Yu X, Zhang F. The effect of parturient height on the median effective dose of intrathecally administered ropivacaine. Ann Saudi Med. 2016;36(5):328–333. doi:10.5144/0256-4947.2016.328
24. Yue L, Zhang F, Mu G, et al. Effectiveness and safety of intrathecal morphine for percutaneous endoscopic lumbar discectomy under low-dose ropivacaine: a prospective, randomized, double-blind clinical trial[J]. Spine J. 2023;23(7):954–961. doi:10.1016/j.spinee.2023.03.001
25. Li M, Xie G, Chu L, et al. Efficacy of low-dose hypobaric anesthetics in spinal anesthesia for cesarean delivery: systematic review and meta-analysis. J Matern Fetal Neonatal Med. 2025;38(1):2519655. doi:10.1080/14767058.2025.2519655
26. Wang LL, Kang M, Duan LX, et al. Effect of single spinal anesthesia with two doses ropivacaine on urinary retention after hemorrhoidectomy in male patients. Front Surg. 2022;9:1077575. doi:10.3389/fsurg.2022.1077575
27. Chen L, Dong X, Chen J, et al. Determining the optimal ropivacaine concentration for spinal anaesthesia during day surgery for anorectal procedures: a dose-finding study. Sci Rep. 2025;15(1):40520. doi:10.1038/s41598-025-24272-5
28. Paliwal N, Kokate MV, Deshpande NA, et al. Spinal anaesthesia using hypobaric drugs: a review of current evidence. Cureus. 2024;16(3):e56069. doi:10.7759/cureus.56069
29. Wahedi W, Nolte H, Klein P. Ropivacaine for spinal anesthesia. A dose-finding study. Anaesthesist. 1996;45(8):737–744. doi:10.1007/s001010050306
30. Altschul D, Kobets A, Nakhla J, et al. Postoperative urinary retention in patients undergoing elective spinal surgery. J Neurosurg Spine. 2017;26(2):229–234. doi:10.3171/2016.8.SPINE151371
31. Neuman MD, Ellenberg SS, Carson JL, et al. Pain, analgesic use, and patient satisfaction with spinal versus general anesthesia for hip fracture surgery. Ann Intern Med. 2023;176(1):eL220367. doi:10.7326/L22-0367
32. Li F, Yu W, Zhou H, et al. Construction and development of an enhanced recovery after surgery program for the surgical management of patients with spinal metastasis: a modified delphi study. Orthop Surg. 2025;17(3):939–952. doi:10.1111/os.14375
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.