Back to Journals » International Journal of Nephrology and Renovascular Disease » Volume 9
The number of patients with severe encapsulating peritoneal sclerosis is decreasing in a large referral center in Germany
Authors Kitterer D, Braun N, Alscher MD ![]() , Segerer S, Latus J
, Segerer S, Latus J
Received 29 March 2016
Accepted for publication 6 May 2016
Published 5 August 2016 Volume 2016:9 Pages 183—186
DOI https://doi.org/10.2147/IJNRD.S108529
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Pravin Singhal
Daniel Kitterer,1 Niko Braun,2 M Dominik Alscher,1 Stephan Segerer,3,* Joerg Latus1,*
1Division of General Medicine and Nephrology, Department of Internal Medicine, Robert-Bosch-Hospital, Stuttgart, Germany; 2Nephrology Center Stuttgart, Stuttgart, Germany, 3Division of Nephrology, University Hospital, Zurich, Switzerland
*These authors contributed equally to this work
Background: Encapsulating peritoneal sclerosis (EPS) is the most severe complication associated with long-term peritoneal dialysis (PD). Previous studies noticed a sharp decline in new patients with severe EPS. We investigated the number of severe EPS patients in our large referral center over almost 20 years.
Methods: All late-stage EPS patients who underwent major surgery due to extensive symptoms caused by bowel obstruction (vomiting, abdominal pain, and weight loss) between March 1997 and end of December 2015 in our hospital were included in the present study. An index was calculated between the number of patients with severe EPS and the implanted PD catheters in our center.
Results: Between 1979 and 2015, a total of 745 PD catheters were implanted in our center, with a steady increase in the numbers between 2003 and 2015. First patient with severe EPS was treated in 1998, then a rise in the number of patients with EPS was present in 2005. The number of patients with EPS peaked in the period of 2010–2012 (15 patients within 3 years). Afterward, both the absolute numbers and the index between the number of patients with severe EPS and the implanted catheters demonstrated a prominent reduction in the next 3-year period from 2013 to 2015.
Conclusion: Our data support the hypothesis that there seems to be a decrease of late-stage EPS incidence over the last years, but data about milder or asymptomatic patients are lacking. This should be kept in mind while giving the patients information about different renal replacement therapies at start of dialysis.
Keywords: encapsulating peritoneal sclerosis, EPS surgery, decrease of EPS incidence
Introduction
Encapsulating peritoneal sclerosis (EPS) is the most severe complication associated with long-term peritoneal dialysis (PD). This life-threatening disease caused significant uncertainty in the PD community and still reflects the “sword of Damocles” hanging over long-term PD users. The overall rate of occurrence has been described in the range of 0.7%–3.3%, being mainly associated with the time on PD.1
Unfortunately, the mortality is still high (ranging from 19% to 55%), especially in the first year after diagnosis.2,3 In the last 2 decades, a significant number of studies have been performed on the clinical and pathophysiological aspects, but many questions remain unanswered. It is important to note that mild or asymptomatic disease manifestations might commonly be missed.4 Recently, the NEXT-PD Study from Japan showed that a multidisciplinary approach reduced the risk of the development of EPS (overall incidence was only 1%).5 We were involved in a large number of basic and clinical science studies and the initiation of the European registry for EPS as the Robert Bosch Hospital remains one of the largest referral centers for EPS patients in Europe.3 While designing future studies during the last 2 years, we noticed a sharp decline in new patients with severe EPS. Therefore, in this manuscript, we asked the question whether the current numbers reflected this clinical impression.
Patients and methods
The present study included all late-stage EPS patients who underwent major surgery due to extensive symptoms caused by bowel obstruction (vomiting, abdominal pain, weight loss, sepsis) between March 1997 and December 2015 in our hospital. For the diagnosis of EPS, we used clinical criteria stated by Nakamoto,6 radiological criteria by Vlijm et al,7 and histological criteria by Braun et al8 and Honda et al.9 An index was calculated between the number of patients with severe EPS and the implanted PD catheters in our center.
The study was approved by the local ethics committee in Germany (Eberhard-Karls University Tuebingen, Germany). All patients gave written informed consent before participating in the study.
Results
Between 1979 and 2015, a total of 745 PD catheters were implanted in our center, with a steady increase in the numbers between 2003 and 2015 (Figure 1A). This was used as an indication of the overall development of the size of the PD program. Since 1979, a total of 34 patients required major surgery due to a late-stage EPS with severe signs of bowel obstruction over the whole study period. All patients suffered from abdominal pain or vomiting prior to surgery. Additionally, weight loss was noted in almost all patients. computed tomography scans were performed in all patients and supported the diagnosis of EPS. Histopathological analyses of the peritoneal biopsies of all patients were done and the evaluation was consistent with the diagnosis of EPS in all patients.
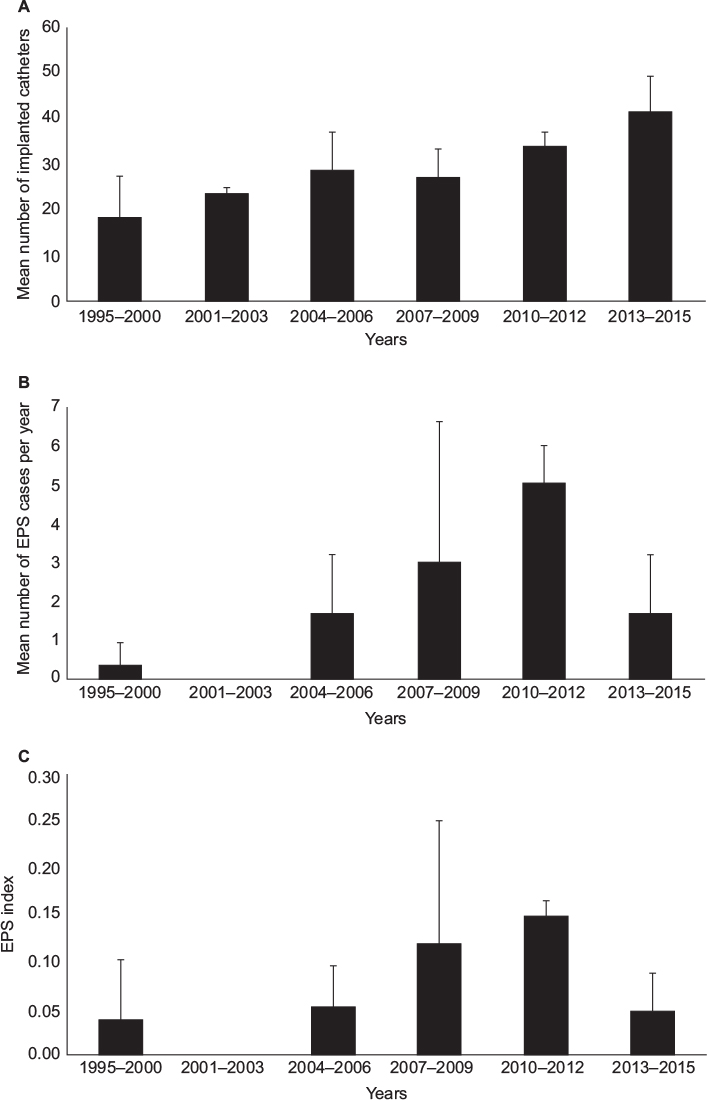 | Figure 1 Number of implanted PD catheters and number of EPS patients over the years. Notes: (A) The mean number of PD catheters implanted in 3-year period (P<0.05). (B) Mean number of patients with EPS in 3-year period (P<0.05). (C) EPS index illustrates the number of patients with EPS divided by the number of PD catheters implanted (P<0.05). Abbreviations: EPS, encapsulating peritoneal sclerosis; PD, peritoneal dialysis. |
A single patient with EPS was treated in 1998, then a rise in the number of patients with EPS was detectable starting in 2005. The number of patients with EPS peaked in the period of 2010–2012 (15 patients within 3 years) (Figure 1B). Interestingly, both the absolute numbers and the index between the number of patients with severe EPS and the implanted catheters demonstrated a prominent reduction in the next 3-year period from 2013 to 2015 (only five patients underwent major surgery in this period) (Figure 1C).
Discussion
While planning studies on EPS, we noticed that the number of patients with EPS diagnosis seemed to be low as compared with the earlier years. To the best of our knowledge, this is the second study illustrating a decline in the number of patients suffering from EPS. A study from Spain reported that the incidence of EPS declined during three decades of experience (5.6%, 3.9%, and 0.3%).5,10 Our data are the first from Germany illustrating a prominent reduction since 2012.
The use of biocompatible solutions, identification of EPS-prone patients with subsequent start of tamoxifen treatment, and planned stop of PD after, for example, 8 years has been supposed to minimize EPS incidence.5,10 It is noteworthy that we are a referral center for EPS and often patients with late-stage disease were transferred to our center. Our data support the hypothesis that there seems to be a clinically relevant decrease of late-stage EPS incidence over the last years. It is still not possible to diagnose early forms; therefore, data about milder or asymptomatic patients are lacking. Early and disproportionate reduction in osmotic conductance during the course of PD might serve as an independent predictor of EPS in the future and might help the clinicians to identify patients at higher risk for developing EPS.
A note of caution needs to be added. Although the decrease illustrated in our population is the first for almost a decade (and is consistent with the data from Spain), we cannot exclude an oscillation of the incidence. As a variety of potential factors (eg, handling of the PD materials, antiseptic, number and type of infections) have changed over time, it is of course impossible to establish a causal relationship with the use of more biocompatible dialysates.
It might still be an important piece of information for the informed patient that this is an important and severe complication seems to decrease in recent years.
Acknowledgments
Daniel Kitterer and Joerg Latus were supported by the Robert-Bosch Foundation (Stuttgart, Germany). Stephan Segerer is supported by grants by Fundação Pesquisa e Desenvolvimento Humanitario and the Else Kröner-Fresenius Stiftung.
Disclosure
The authors report no conflicts of interest in this work.
References
Brown MC, Simpson K, Kerssens JJ, Mactier RA. Encapsulating peritoneal sclerosis in the new millennium: a national cohort study. Clin J Am Soc Nephrol. 2009;4(7):1222–1229. | ||
Kawanishi H, Kawaguchi Y, Fukui H, et al. Encapsulating peritoneal sclerosis in Japan: a prospective, controlled, multicenter study. Am J Kidney Dis. 2004;44(4):729–737. | ||
Latus J, Ulmer C, Fritz P, et al. Encapsulating peritoneal sclerosis: a rare, serious but potentially curable complication of peritoneal dialysis-experience of a referral centre in Germany. Nephrol Dial Transplant. 2013;28(4):1021–1030. | ||
Nitsch D, Davenport A. Designing epidemiology studies to determine the incidence and prevalence of encapsulating peritoneal sclerosis (EPS). Perit Dial Int. 2015;35(7):678–682. | ||
Nakayama M, Miyazaki M, Honda K, et al. Encapsulating peritoneal sclerosis in the era of a multi-disciplinary approach based on biocompatible solutions: the NEXT-PD study. Perit Dial Int. 2014;34(7):766–774. | ||
Nakamoto H. Encapsulating peritoneal sclerosis – a clinician’s approach to diagnosis and medical treatment. Perit Dial Int. 2005;25(Suppl 4):S30–S38. | ||
Vlijm A, Stoker J, Bipat S, et al. Computed tomographic findings characteristic for encapsulating peritoneal sclerosis: a case-control study. Perit Dial Int. 2009;29(5):517–522. | ||
Braun N, Fritz P, Ulmer C, et al. Histological criteria for encapsulating peritoneal sclerosis – a standardized approach. PLoS One. 2012;7(11):e48647. | ||
Honda K, Nitta K, Horita S, et al. Histologic criteria for diagnosing encapsulating peritoneal sclerosis in continuous ambulatory peritoneal dialysis patients. Adv Perit Dial. 2003;19:169–175. | ||
De Sousa-Amorim E, Del Peso G, Bajo MA, et al. Can EPS development be avoided with early interventions? The potential role of tamoxifen – a single-center study. Perit Dial Int. 2014;34(6):582–593. | ||
Morelle J, Sow A, Hautem N, et al. Interstitial fibrosis restricts osmotic water transport in encapsulating peritoneal sclerosis. J Am Soc Nephrol. 2015;26(10):2521–2533. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.