Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 12
The NFκB Expression on Apical Dental Granuloma: An Immunohistochemistry Analysis
Authors Cilmiaty R, Pribadi N, Rukmo M, Surboyo MDC ![]()
Received 14 April 2020
Accepted for publication 16 July 2020
Published 5 August 2020 Volume 2020:12 Pages 313—318
DOI https://doi.org/10.2147/CCIDE.S256284
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Christopher E. Okunseri
Risya Cilmiaty,1 Nirawati Pribadi,2 Mandojo Rukmo,2 Meircurius Dwi Condro Surboyo3
1Department of Oral Disease, Faculty of Medicine, Universitas Sebelas Maret, Surakarta, Indonesia; 2Department of Conservative Dentistry, Faculty of Dental Medicine, Universitas Airlangga, Surabaya, Indonesia; 3Department of Oral Medicine, Faculty of Dental Medicine, Universitas Airlangga, Surabaya, Indonesia
Correspondence: Nirawati Pribadi
Department of Conservative Dentistry, Faculty of Dental Medicine, Universitas Airlangga. Jalan Prof. Dr. Moestopo 47x, Surabaya 60132, Indonesia
Tel +628123292481
Email [email protected]
Risya Cilmiaty
Department of Oral Disease. Faculty of Medicine, Universitas Sebelas Maret, Jalan Ir. Sutami No. 36A, Kenthingan, Surakarta 57126, Indonesia
Tel +6281227316161
Email [email protected]
Background: Endodontic treatment on dental caries with dental granuloma on the periapical has the potential to flare. The symptoms of acute flare in dental granuloma are strongly related to the activation of macrophages that produce pro-inflammatory cytokine through nuclear factor kappa B (NFκB). However, the role of NFκB in dental granuloma has not been widely explained.
Purpose: To compare NFκB expression in dental granuloma and dental nongranuloma in the periapical of dental caries.
Methods: The periapical lesion of dental granuloma and dental nongranuloma was obtained from patients with dental caries who were subjected to tooth extraction. The periapical lesion was confirmed by periapical radiography and then differentiated by histological and immunohistochemistry by analyzing the NFκB expression.
Results: Most dental granulomas were found in females (66.67%) between the ages 36 and 45 (61.11%). Dental granuloma showed higher NFκB expression compared to dental nongranuloma lesions in tooth caries (p=0.021).
Conclusion: The dental granuloma tissue of dental caries showed an increase in NFκB expression. Understanding the role of NFκB might provide additional insights into the process of periapical lesion development.
Keywords: dental granuloma, dental caries, NFκB expression, periapical lesion
Introduction
The dental caries that are not treated gradually will reach the pulp and cause inflammation. The process of pulp inflammation can cause periapical tissue abnormalities, such as dental granuloma. Dental granuloma is one of the periapical lesions characteristic in chronic inflammation caused by microorganisms present in the root canal as a consequence of dental caries.1 Dental granuloma present as periapical radiolucency in dental x-ray. The product of microorganisms results in root canals and periapical infection. This process attracts monocytes, macrophages, fibroblasts, and other cells in the immune system. The immune system will produce pro-inflammatory cytokines responsible for tissue destruction and degradation of extracellular matrix (ECM) components,2 which results in the resorption of periapical tissues.3
Bacteria enter the periapical tissue will be phagocyted and destroyed by histiocytes. The presence of bacteria triggers the development of histiocytes into macrophages (angry macrophage) and antigen-presenting cell (APC) which drives the formation of dental granuloma. On the other hand, histiocytes develop into phagocytes, so the nongranuloma will be formed.3
The resorption of periapical tissue is interpreted as bone resorption. The bone resorption process is modulated by proinflammatory cytokines in response to bacteria in the root canals and periapical infection such as interleukin 1β (IL-1β), interleukin 6 (IL-6), interferon γ (IFNγ), and tumor necrosis factor α (TNF-α).4 These pro-inflammatory cytokines are produced by macrophages when nuclear factor kappa B (NFκB) is activated.5
Based on histological analysis, dental granuloma comprises of granulation by inflammatory cells such as lymphocytes, plasma cells, macrophages, and mast cells. Macrophages are the main component in dental granuloma covered by a dense connective tissue capsule.6 When root canals are infected with bacteria, the macrophages will be activated and will function as phagocytes. Macrophages also serve as antigen-presenting cells; they process the antigen and present it to T-helper lymphocytes by major histocompatibility type II (MHC II).7 This process creates inflammation as in acute granuloma or acute flare of dental granuloma.8
A dental granuloma is a form of self-defense so that infection does not spread. It is characterized by an exudation of immune cells and is used as an intermediary for the production of inflammation such as cytokines. The inflammatory reaction is triggered by Th-1, Th-2, and Th-17 responses, and this polarization can be translated into the development of disease and bone resorption cytokines. In the pathogenesis process, an increase in proinflammatory cytokines will occur.
Patients and Methods
This research involved an analytic observational cross-sectional study conducted in the dental clinic at Dr Moewardi General Hospital, Surakarta, Central Java, from June 2008 until July 2009. To find out the exact diagnosis of dental granuloma, it is necessary to do a histopathological examination, so it is necessary to have a tooth extraction. The research protocol was approved by the ethics committee of the School of Medicine, Sebelas Maret University (E.C.106/XI/2008) and was performed in accordance with the principles of the Declaration of Helsinki.
Patient Criteria
Selected patients had to meet the following criteria and sign an informed consent form:
- Ages 17–57 years
- Did not have any systemic disease
- Did not consume antibiotics or immunosuppressants
- Level albumin ranges 3.5–5.2 mg/dl
- Hemoglobin range 2.3–15.0 g/dl.
Apical Lesion Determination
The apical lesion was determined and collected from the following criteria:
- Apical lesion on a permanent tooth with profundal caries, both maxillary and mandibular teeth.
- The apical lesion was confirmed with periapical radiography, then selected for dental granuloma and dental nongranuloma.
- The dental granuloma appeared radiolucent with a clear margin in the apical tooth.
- The dental nongranuloma was enlarged by apical periodontitis and the apical tooth appeared radiolucent.
- All profundal caries were indicated for extraction and the patient gave consent.
Hematoxylin-Eosin Staining
The apical lesion was separated from the tooth then immersed on buffer saline 10% (Merck). The histopathology confirmation of dental granuloma and dental nongranuloma was done by the following criteria:
- The dental granuloma lesion showed chronic inflammation consisting of granulation tissue; the wall was surrounded by fibrous tissue and showed the presence of macrophages, lymphocytes, plasma cells, giant cells, fibroblasts, and mast cells.
- The dental non granuloma lesion showed chronic inflammation without granulation tissue and showed the presence of macrophages, lymphocytes, plasma cells, fibroblasts, and mast cells.
NFκB Expression
The NFκB expression of the dental granuloma and dental nongranuloma was then analyzed by immunohistochemistry. The NFκB expression is counting based on the number of macrophages that give a positive reaction to anti-NFκB anti-body, which is calculated on the area of the incision of granuloma tissue. All sections were stained using the R&D HRP-DAB staining kit (Ultravision plus) according to the manufacturer’s instructions. The primary antibodies were monoclonal antibody NFκB (anti-human NFκB, Lab. Vision). Counterstaining was performed with hematoxylin. The negative controls were treated with phosphate-buffered saline rather than primary antibodies.
The images were analyzed by two evaluators in a blinded fashion. For each specimen, five random areas around the apical lesion were selected for pathologic assessment under 400x magnification. The average number in each group was taken as a result. At the end of the evaluation, discrepant cases were confirmed by a third pathologist.
Statistical Analysis
Statistical analyses were performed with independent t-tests to compare the NFκB expression using SPSS 20.0 software (SPSS Inc, Chicago, IL). The significance was assumed at P < 0.05.
Results
Patient Data
Table 1 presents the patients’ data, which included gender, age, and who had dental granuloma and nongranuloma. Most of the patients with dental granuloma were female (66.67%) between the ages 36–45 (61.11%). Dental nongranuloma was mostly found in males (61.11%) between the ages 36–45 (77.77%).
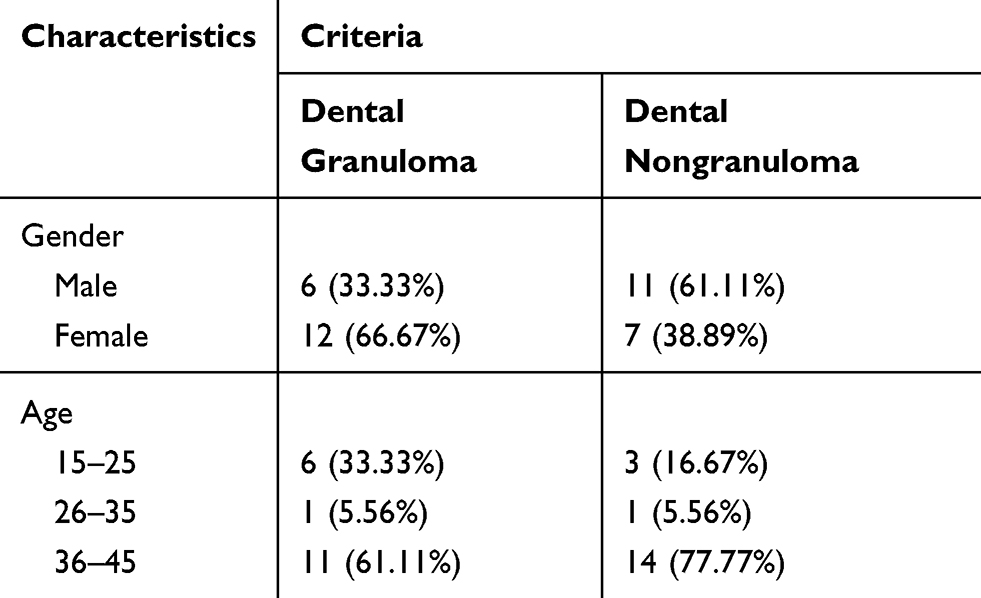 |
Table 1 Patient’s Demographics |
Lesion Specimens from Patients
Table 2 shows that most of the patients with dental granuloma were affected on their mandibular posterior teeth (71.22%) with 22.22% affected on their maxillary posterior teeth. Dental nongranuloma mostly affected mandibular posterior teeth (55.56%).
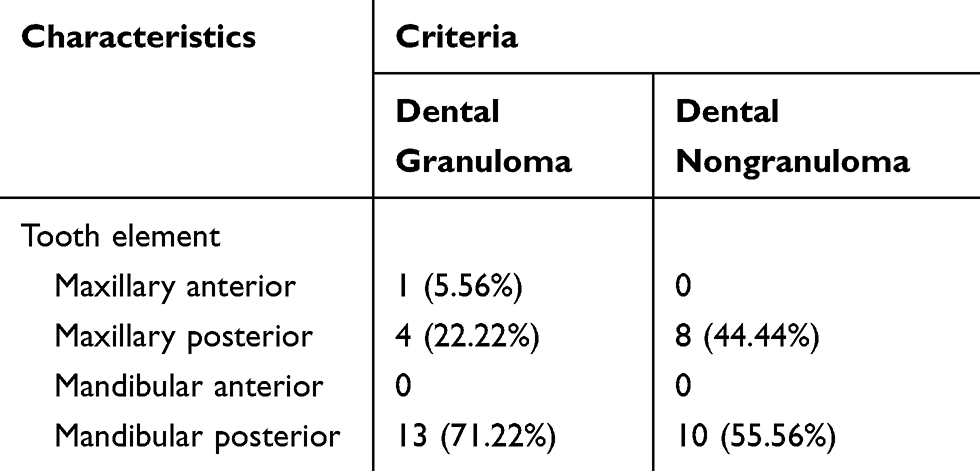 |
Table 2 The Origin of Dental and Dental Nongranuloma |
Periapical radiography confirmed that all teeth enamel appeared radiolucent until the dentin in the pulp chamber, and indicated profundal caries. The dental granuloma appeared radiolucent with a clear margin in the apical tooth (Figure 1D and E). The dental nongranuloma appeared enlarged by apical periodontitis and radiolucent in the apical tooth (Figure 1A–C).
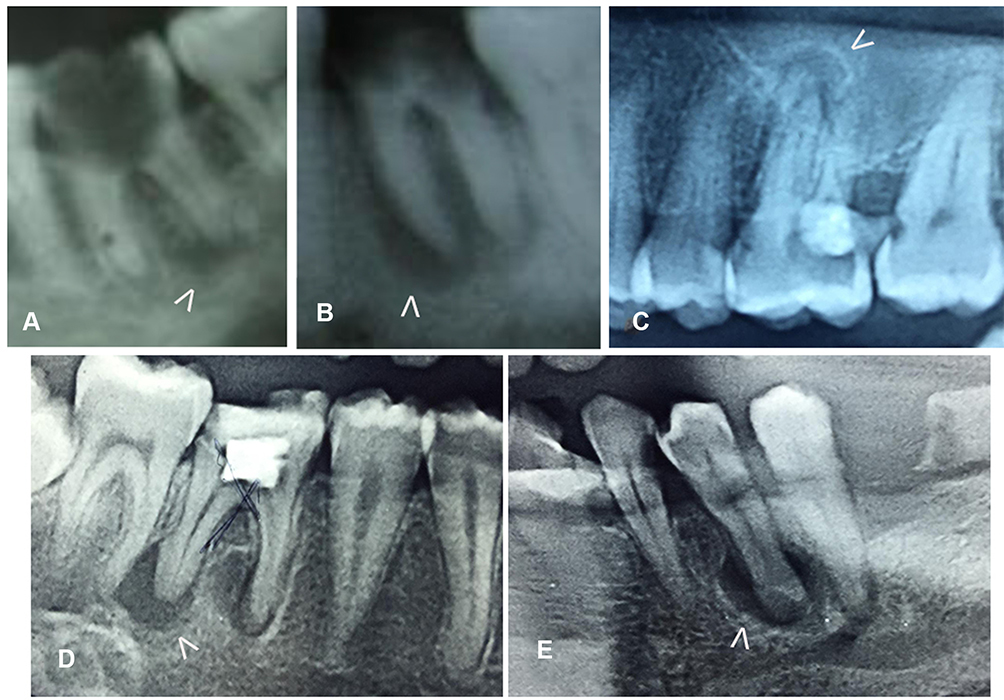 |
Figure 1 Periapical radiography for confirming the periapical lesion. (A–C) dental nongranuloma (white arrow); (D–E) dental granuloma (white arrow). |
Hematoxylin-Eosin Staining
Hematoxylin-eosin staining in both dental and dental nongranuloma is shown in Figure 2A and B. Dental granuloma lesions show granulation tissue with the presence of macrophages, lymphocytes, plasma cells, giant cells, fibroblasts, mast cells, and datia cells (Figure 2A). Dental nongranuloma lesions do not show granulation tissue but do have a presence of macrophages, lymphocytes, plasma cells, fibroblasts, and mast cells (Figure 2B).
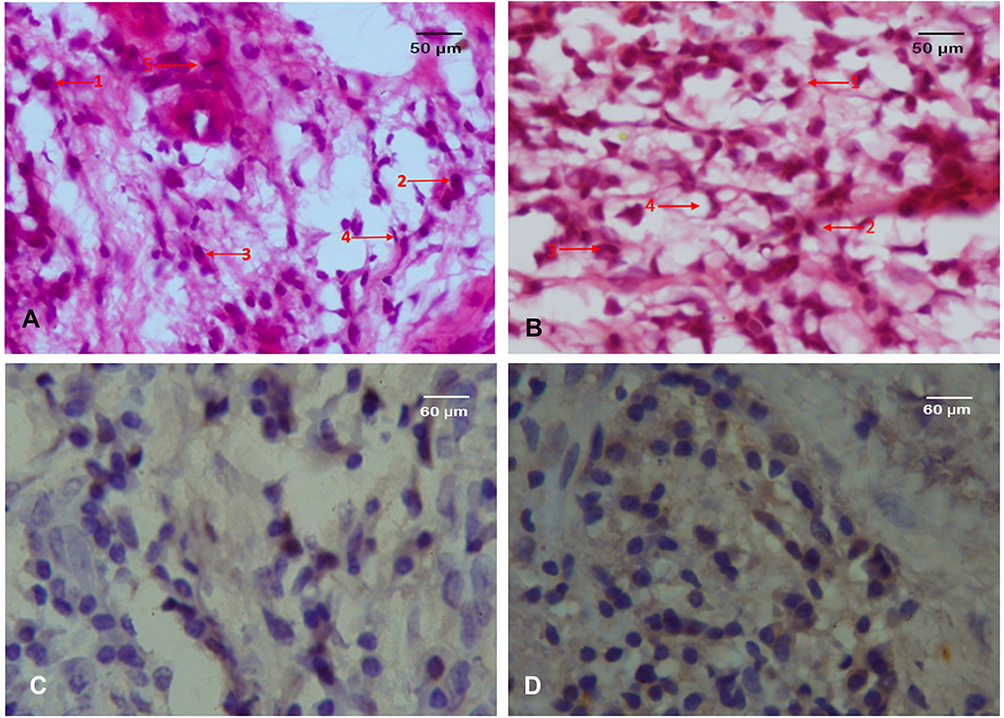 |
Figure 2 (A) Dental granuloma showing the appearance of a (1) datia cell, (2) lymphocytes, (3) macrophages, (4) fibroblasts, (5) plasma cells. (B) Dental nongranuloma showing the appearance of (1) macrophages, (2) lymphocytes, (3) plasma cells, (4) fibroblasts. (C) Immunohistochemistry of NFκB expression on dental granuloma. (D) Immunohistochemistry of NFκB expression on dental nongranuloma. Magnification at 400x. |
NFκB Expression
Immunohistochemistry analysis of the dental granuloma lesions shows a higher NFκB expression compared to dental nongranuloma lesions (p=0.021) (Figure 3). Immunohistochemistry also showed that not all cells in the dental and dental nongranuloma expressed NFκB (Figure 2C and D).
 |
Figure 3 The NFκB expression on dental and dental nongranuloma. |
Discussion
The distribution of granuloma was dominant in females (66.67%) compared to males (33.33%). In terms of the distribution of ages, dental granuloma was mostly found in the 36–45 age bracket (61.11%). This result contradicts a previous study by Omoregie et al, who found that dental granuloma was mostly found in males between 21 and 30 years old.9
Bacterial infections in dental pulp usually cause irreversible pulpitis and pulpal necrosis. The interaction between bacterial infection and the immune system in dental pulp results in the release of numerous mediators through the root canal system and initiates reactions in apical tissues that result in the formation of apical lesions.10 Dental granuloma is the apical lesion resulting from pulp necrosis and consists of a granulomatous tissue with inflammatory cells, fibroblasts, and a well-developed fibrous capsule. In this histological analysis of dental granuloma, we found the presence of macrophages, lymphocytes, plasma cells, giant cells, fibroblasts, and mast cells. This result is similar to that of Omoregie et al, who found the main dominant cell in the early stages of granuloma was infiltrated by macrophages, foamy cytoplasm, with or without neutrophils, and a few lymphocytes.9
The condition of irreversible pulpitis or pulpal necrosis along with dental granuloma will increase the rate of acute flare if the pulp and root canals are inadequately disinfected.11 One study demonstrated the highest distribution of bacteria and bacteria biofilm in the entire root canal system in irreversible pulpitis or pulpal necrosis with dental granuloma. Bacterial biofilm was detected in 81.2% of the cementum, 65.6% at the apical surface and 79.2% in the dental granuloma itself. Endodontic failure is mainly due to an infected root canal system that acts as a reservoir for bacteria and antigens that evoke and maintain apical periodontitis,12 acute granuloma or an acute flare of dental granuloma.13
Macrophages are important inflammatory cells in the development of dental granuloma and acute granuloma. The presence of bacteria triggers the development of histiocytes into macrophages. This process produces HSP60, which triggers the apoptosis of CD4 lymphocytes (TH2 cells); this causes the balance to shift towards CD8 lymphocytes (TH1 cells) and this is reflected by increased IFNy-producing cells. IFNy-producing cells are increased by the induction of IL-12, which triggers the formation of granuloma.14 As the main component in granuloma with lymphocytes, macrophages are activated by bacteria in the root canal system. This will then activate antigen-presenting cells to sensitive T-lymphocytes to release proinflammatory cytokines such as IL-1β, IL-6, IL-11, IL-17, and TNF-α, by stimulating the up-regulation of NFκB receptors on macrophages.15,16 This research confirmed that the NFκB expression is higher in granuloma compared to nongranuloma.
Other cells found in dental granuloma are the mast cell, which is associated with bone tissue destruction and the growth of granulomas. Many of the cytokines produced by activated mast cells, such as IL-1, IL-6, and TNF-α in particular, have been shown to increase local osteolytic activity.17
The research on the mechanism of periapical lesions formation in humans using real time-PCR showed that when compared with healthy periodontal ligaments, the expression of RANKL (Receptor Activator of Factor Kappa β Ligand) in periapical granulomas is higher, especially in lesions with a diameter of less than 5 mm.18 This condition explains the role of RANKL in the regulation of the expansion of periapical lesions at an early stage. Kawashima et al (2007) explained that the optimal expression of RANKL in the third week of the formation of periapical lesions and decreased stably from the fourth week, followed by periapical bone damage.19
The results of this study indicate that dental granulomas have high NFκB expression and their main components are macrophages, lymphocytes, and mast cells so the possibility of recurrence after endodontic therapy is also very high. From this perspective, adequate endodontic treatment of pulpitis irreversible or pulp necrosis with dental granuloma is needed so that it does not trigger the activation of NFκB to produce proinflammatory cytokines such as IL-1β, IL-6, and TNF-α.
Studies investigating the presence of NFκB expression in granuloma periapical are limited. Therefore, the objective of this study is to compare the NFκB expression between dental granuloma and nongranuloma in an apical lesion. The data should contribute to a better understanding of the role of NFκB in the immunopathogenesis of acute granuloma or acute flare of periapical granuloma after endodontic treatment. If the pathogenesis can be explained, it will be easier to carry out therapy, namely by suppressing the expression of NFκB. For future therapeutic solutions in endodontic treatment, we can use ingredients whose purpose is to suppress NFκB expression (as an immunomodulator).
Conclusion
The dental granuloma tissue in dental caries shows there is an increase of NFκB expression. Understanding the role of the NFκB might provide additional insights into the process of periapical lesion development.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Marçal JRB, Samuel RO, Fernandes D, et al. T-helper cell type 17/regulatory T-cell immunoregulatory balance in human radicular cysts and periapical granulomas. J Endod. 2010;36(6):995–999. doi:10.1016/j.joen.2010.03.020
2. de Paula-silva FWG, D’Silva NJ, da Silva LAB, Kapila YL. High matrix metalloproteinase activity is a hallmark of periapical granulomas. J Endod. 2009;35(9):1234–1242. doi:10.1016/j.joen.2009.06.008
3. Correa CP, García LB, Del Río EP, Caballero AD. Correlation of clinical, radiographic and histological diagnoses of apical dental lesions. Rev Odontológica Mex. 2017;21(1):e21–8. doi:10.1016/j.rodmex.2017.02.007
4. De Carvalho Fraga CA, Alves LR, De Sousa AA, et al. Th1 and Th2-like protein balance in human inflammatory radicular cysts and periapical granulomas. J Endod. 2013;39(4):453–455. doi:10.1016/j.joen.2012.11.054
5. Álvares PR, de Arruda JAA, Oliveira Silva LV, et al. Immunohistochemical analysis of cyclooxygenase-2 and tumor necrosis factor alpha in periapical lesions. J Endod. 2018;44(12):1783–1787. doi:10.1016/j.joen.2018.09.002
6. Awinashe MV, Wanjari SP, Parwani RN. Presence and location of bacteria in human periapical pathosis: a histopathological study. J Pierre Fauchard Acad. 2013;27(1):9–13. doi:10.1016/j.jpfa.2013.01.004
7. Graunaite I, Lodiene G, Maciulskiene V. Pathogenesis of apical periodontitis: a literature review. J Oral Maxillofac Res. 2011;2(4):1–15. doi:10.5037/jomr.2011.2401
8. Metzger Z. Macrophages in periapical lesions. Endod Dent Traumatol. 2000;16:1–8. doi:10.1034/j.1600-9657.2000.016001001.x
9. Omoregie FO, Ojo MA, Saheeb BDO, Odukoya O. Periapical granuloma associated with extracted teeth. Niger J Clin Pract. 2011;14(3):293–296. doi:10.4103/1119-3077.86770
10. De Sá AR, Garcia Santos Pimenta FJ, Dutra WO, Gomez RS. Immunolocalization of interleukin 4, interleukin 6, and lymphotoxin α in dental granulomas. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003;96(3):356–360. doi:10.1016/S1079-2104(03)00067-2
11. Arango DV, Manotas JR, Caballero AD. Apicoectomy and retrograde filling as periapical granuloma treatment. A case report. Rev Fac Odontol. 2016;28(1):203–209.
12. Garlet GP, Horwat R, Ray HL, et al. Expression analysis of wound healing genes in human periapical granulomas of progressive and stable nature. J Endod. 2012;38(2):185–190. doi:10.1016/j.joen.2011.09.011
13. Ribeiro FC, Pinheiro TN, Consolaro A. Bacterial distribution in teeth with pulp necrosis and apical granuloma. Int J Exp Dent Sci. 2013;2(2):86–91. doi:10.5005/jp-journals-10029-1047
14. Cilmiaty R, Rukmo M. The role of Hsp0, CD-8 and IFN-γ in immunopathobiogenesis of periapical granuloma in dental caries. Dent J (Majalah Kedokt Gigi). 2014;47(1):7–12. doi:10.20473/j.djmkg.v47.i1.p7-12
15. Bănică AC, Popescu SM, Mercuţ V, et al. Histological and immunohistochemical study on the apical granuloma. Rom J Morphol Embryol. 2018;59(3):811–817.
16. Ajuz NC, Antunes H, Mendonça TA, Pires FR, Siqueira JF, Armada L. Immunoexpression of interleukin 17 in apical periodontitis lesions. J Endod. 2014;40(9):1400–1403. doi:10.1016/j.joen.2014.03.024
17. Sethi N, Savan SR, Mahendrakumar PH, et al. Immunoregulatory role of mast cells in apical granulomas and periapical cysts-an immunohistochemical study. OHDM. 2015;14(2):70–74.
18. Menezes R, Garlet TP, Letra A, et al. Differential patterns of receptor activator of nuclear factor kappa B ligand/osteoprotegerin expression in human periapical granulomas: possible association with progressive or stable nature of the lesions. J Endod. 2008;34(8):932–938. doi:10.1016/j.joen.2008.05.002
19. Kawashima N, Suzuki N, Yang G, et al. Kinetics of RANKL, RANK and OPG expressions in experimentally induced rat periapical lesions. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;103(5):707–711. doi:10.1016/j.tripleo.2006.11.036
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.