Back to Journals » Substance Abuse and Rehabilitation » Volume 17
The Musical Reassociation Model (MRM): A Stage-Based Framework for Managing Music-Related Cues and Reclaiming Musical Agency in Substance Use Disorder Recovery
Authors Bensimon M ![]()
Received 13 March 2026
Accepted for publication 17 June 2026
Published 9 July 2026 Volume 2026:17 609154
DOI https://doi.org/10.2147/SAR.S609154
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rajendra Badgaiyan
Moshe Bensimon
Department of Criminology, Bar-Ilan University, Ramat Gan, Israel
Correspondence: Moshe Bensimon, Department of Criminology, Bar-Ilan University, Max and Anna Webb St, Ramat Gan, 5290002, Israel, Tel +972545301545, Email [email protected]
Abstract: Music plays a central role in identity, emotion regulation, and everyday functioning, yet in the context of substance use disorders, it may also become conditioned through repeated pairing with intoxication and later function as a cue for craving, urges to use, or emotional destabilization. Existing literature has recognized both the risks and therapeutic potential of music in recovery but has offered limited stage-sensitive guidance for clinical decision-making. This article introduces the Musical Reassociation Model (MRM), a stage-based conceptual framework that maps how the relationship between music and substance use evolves across addiction and recovery. The model describes five distinct phases: (1) the synergy phase, characterized by mutual enhancement between music and substance use; (2) acoustic erasure, marking the collapse or distortion of music’s aesthetic and self-regulatory function; (3) stabilization through avoidance or substitution; (4) active tolerance through graded exposure, musical agency, and reassociation; and finally (5) integration, in which music is reclaimed as a recovery resource. Across these stages, the MRM reframes music not only as a trigger to be managed but as a dynamic domain of identity, self-regulation, and agency. The model highlights a key clinical distinction between short-term stabilization strategies based on environmental control and later-stage interventions aimed at building durable agency in the presence of problematic music cues. It also introduces the construct of Aesthetic Recovery Capital to describe the musical, social, and interpretive resources that support reintegration in the aesthetic domain. By integrating cue reactivity, identity reconstruction, recovery-oriented theory, and recovery capital, the MRM provides a theoretically grounded account of how music shifts from a substance-linked vulnerability to an integrated recovery resource. The article concludes by discussing clinical implications and illustrative vignettes, while outlining directions for future research, such as validating stage boundaries, examining digital listening environments, and developing stage-matched therapeutic interventions.
Keywords: aesthetic recovery capital, substance use disorder, music cues, relapse vulnerability, musical agency, recovery-oriented rehabilitation
Introduction: Background and Clinical Rationale
Music plays a central role in everyday life and in the construction of meaning, coherence, and selfhood. It contributes to perceived quality of life and serves as an actively selected resource for mood and emotion regulation.1,2 DeNora3 conceptualized music as a Technology Of The Self through which individuals shape emotional trajectories and sustain preferred self-states across contexts. Complementing this perspective, research in aesthetics and identity suggests that aesthetic preferences can function as identity anchors shaping both self-experience and social recognition. From this perspective, the Aesthetic Self may be understood as a dimension of personal identity in which aesthetic tastes, especially in music, are experienced as central to who one is and to the continuity of self.4 Work in personality and music psychology likewise shows that musical preferences reflect relatively stable individual differences and predict personality across both controlled listening tasks and ecologically valid digital behavior, although most evidence to date is based on Western musical materials and samples.5,6 This cultural qualification is relevant to the account of musical agency developed below, since agency may be experienced not only as individual self-directed listening but also as a relational and communal capacity shaped through shared musical participation.7,8
Yet, the same qualities that make music a powerful resource for regulation and identity may also render it susceptible to maladaptive learning in the context of substance use. When music is repeatedly paired with intoxication in places such as rave parties, nightclubs, and electronic dance music festivals where music and drug use are often co-occur,9,10 it may become a conditioned element of substance use routines.11,12 Qualitative research indicates that individuals often select particular music to intensify intoxication and shape desired emotional states during substance use.12,13 Through repeated pairing, specific tracks may become tightly associated with use and later elicit cue like responses during recovery. A plausible neurobiological basis for this coupling comes from evidence that pleasurable music listening elicits endogenous dopamine release in the striatal system, with the caudate more involved in anticipation and the nucleus accumbens more involved in peak emotional experience.14 In addiction contexts, repeated pairing may therefore embed music within a broader cue ecology in which auditory material, listening contexts, and autobiographical memories acquire predictive value for substance related reward.
Scholars have long recognized that music can assume problematic roles in vulnerable contexts, although the terminology has varied. North and Hargreaves15 used the term Problem Music to describe music associated with psychosocial vulnerability and maladaptive outcomes. In addiction-oriented scholarship, Horesh16 introduced the concept of Dangerous Music to emphasize music that can function as an environmental cue for craving and relapse. Lozon and Bensimon17 later proposed the broader framework of music misuse, situating music related harm within a wider constellation of maladaptive personal and collective roles. Taken together, this conceptual trajectory suggests that musical risk is not inherent to specific genres. Rather, it emerges from person specific learning histories in which sound becomes linked with reward, autobiographical memory, and substance use practices. More recent work has accordingly used the term Problematic Music to refer to music conditioned through prior substance use experiences that may evoke vivid imagery, emotional destabilization, or craving during recovery.13,18
In residential treatment centers, responses to music related risk may reflect two contrasting orientations toward patients’ leisure listening: some settings view music as a potentially beneficial resource for emotion regulation and recovery related functioning,11,18 whereas others emphasize caution regarding music associated with past substance use because it may function as a conditioned cue for craving and thus carry relapse related risk.18,19 This contrast reflects a broader clinical dilemma within recovery settings, wherein music may function simultaneously as a trigger and as a resource for emotional regulation, identity reconstruction, and social reconnection. The dilemma becomes particularly pronounced in the digital era, as streaming platforms increasingly structure music exposure through interface design, recommendation systems, and autoplay features.20 Algorithms may unexpectedly surface autobiographically linked tracks,21 exposing individuals in treatment to music associated with prior substance use that may cue craving, urges to use, or emotional distress.11,19,22 Because music now accompanies listeners across both private and public environments through digitally mediated platforms, exposure to such cues is often less controllable than many other contextual triggers, particularly in early recovery, given the ubiquitous nature of contemporary listening.21
Despite growing recognition that music can function both as a conditioned cue and as a recovery resource, the literature offers limited stage-sensitive guidance for clinical decision making. Existing research shows that music may evoke craving and other emotionally salient responses in treatment populations,11,19 yet current frameworks rarely specify when avoidance is protective, when repertoire substitution is adaptive, and when structured exposure and reassociation become appropriate therapeutic goals. A recovery-oriented perspective conceptualizes recovery not only as symptom reduction or abstinence maintenance but also as the reconstruction of a meaningful, hopeful, and self-directed life, as reflected in the CHIME framework: connectedness, hope, identity, meaning, and empowerment.23,24 This framework is relevant here because it shifts the clinical focus from symptom control alone toward the psychosocial reconstruction of selfhood, agency, belonging, and meaning, domains in which music can play a central rehabilitative role. In the addiction field, this perspective is complemented by social identity accounts of recovery, which conceptualize recovery as a socially mediated transition from substance-use-linked identities and networks toward recovery-oriented identities, relationships, and meaningful activities.25 Applied to music-related rehabilitation, this perspective suggests that problematic music cues are not merely stimuli to be extinguished, but may also become materials through which identity, agency, belonging, and meaning are rebuilt. The present article addresses this gap by introducing the Musical Reassociation Model (MRM). The MRM is a stage-based, clinically actionable framework for understanding how the relationship between music and substance use may evolve across addiction and recovery. Its central claim is that sustainable rehabilitation requires more than reduction of cue reactivity. It requires aesthetic repair. This process entails progression from short-term stabilization through the development of tolerance and deliberate reassociation skills and ultimately toward the reclamation of music as a stable recovery resource. Building on the foundational theoretical construct of recovery capital,26 defined as the sum of personal and social resources available to initiate and sustain recovery, the model introduces the construct of aesthetic recovery capital. Here, aesthetic recovery capital refers to the accumulation of musical, social, and interpretive resources that enable individuals to reintegrate music into their lives in ways that support self-regulation, identity continuity, prosocial belonging, and the reconstruction of meaning in recovery.
The Musical Reassociation Model
The Musical Reassociation Model (MRM) is a clinically actionable, stage-based conceptual framework for managing music-related cues in substance use disorder (SUD) rehabilitation. SUD refers to a clinically significant pattern of substance use characterized by varying combinations of impaired control, craving, continued use despite harm, tolerance, withdrawal, and impairment or distress.27 Although the model primarily addresses listening-based encounters with recorded or digitally mediated music, it is not limited to passive listening. The same stage logic may also apply to music-making, performance, or participatory musicking when these forms of engagement are linked to substance use cues or become resources for recovery. Grounded in prior theory and qualitative evidence,11–13,18,19,22 the MRM is intended to organize existing evidence and generate testable propositions, rather than to function as a comprehensive theory of addiction. The model consists of five stages describing a clinically plausible trajectory in which music can shift from an enhancer of intoxication to cue-linked vulnerability, then to an avoided trigger, then to a tolerated stimulus, and finally to a reintegrated identity and community resource. This sequence was designed by synthesizing prior qualitative and theoretical work according to the changing clinical function of music across addiction and recovery. Existing studies describe music as mutually enhancing intoxication during active use. As addiction becomes dominant, music may later lose its earlier function as a meaningful, pleasure-enhancing, and self-regulatory resource and become distorted into a cue-linked source of vulnerability. In treatment and recovery, this altered relationship with music may then be managed through awareness, avoidance, substitution, tolerance building, and recovery-oriented reassociation.12,13,18,22
The five stages therefore reflect five clinically distinct functions of music rather than a fixed five-step protocol: enhancement of intoxication, collapse or distortion of aesthetic meaning, short-term stabilization through avoidance or substitution, active tolerance through regulated exposure and reassociation, and long-term integration as a recovery-supportive identity and social resource. This level of differentiation is clinically important because Stage 3 and Stage 4 involve different therapeutic tasks. Stage 3 uses alternative music to reduce immediate relapse-related risk, whereas Stage 4 involves deliberate re-engagement with problematic music under regulated conditions. If these tasks were collapsed into one stage, clinicians might introduce exposure before sufficient stabilization has been achieved or prolong avoidance after the client is ready for tolerance-building work. Conversely, adding more stages would risk making the model less clinically usable by creating artificial distinctions between closely related variations of the same task, thereby making stage identification less clear without adding meaningful clinical guidance.
Rather than rigid steps, the stages delineate clinically meaningful states and transition targets. While the MRM describes a progressive movement toward integration, the trajectory is often non-linear and may include periods of temporary regression. However, the model posits that the psychological gains and coping mechanisms developed during the process are cumulative. Even in the event of a setback, the prior experience of active engagement with music functions as a protective foundation, potentially shortening the duration of regressions and facilitating a more rapid return to a stable, integrated state. Detailed clinical applications of the MRM stages are presented below. Figure 1 summarizes the five stages of the MRM and the progressive transformation of music from a cue-linked vulnerability into a recovery resource.
 |
Figure 1 The Musical Reassociation Model (MRM): A 5-Phase Framework for Aesthetic Recovery. Notes: The figure illustrates a stage-based but non-linear developmental process in which music may shift from synergy with substance use (Stage 1), to acoustic erasure and the collapse or distortion of aesthetic and self-regulatory function (Stage 2), to stabilization through avoidance or substitution (Stage 3), to active tolerance, musical agency, and deliberate reassociation (Stage 4), and finally to aesthetic continuity and integration (Stage 5). Temporary returns to earlier stages may occur under conditions of stress or setback. Across the process, Aesthetic Recovery Capital accumulates and supports the recovery of musical agency, identity continuity, and meaning reconstruction in recovery. This image was generated and visually refined using Google Gemini 1.5 Pro via Imagen 3. |
Stage 1. The Mutual Enhancing Effect: The Synergy Phase
Stage 1 describes a mutual enhancing relationship in which music and substances intensify one another, creating a learned coupling experienced as functional and desirable during active use. Within the MRM, this pattern is conceptualized as the synergy phase. It builds on what Lozon and Bensimon12 term the mutual enhancing effect, that is, the reciprocal use of music to intensify drug effects and of drugs to amplify musical experience. Empirical work further suggests that music can modulate affect and craving in treatment contexts, particularly when specific songs are linked to prior substance use experiences and function as conditioned cues.11 This aligns with a systematic synthesis indicating that music can induce substance craving, supporting the plausibility of music as a conditioned component of cue reactivity across substances and settings.19 From a neurobiological perspective, repeated pairing may recruit reward learning mechanisms. Over time, musical features and listening contexts may acquire predictive value, become integrated into associative memory, and later reactivate drug-linked networks during abstinence.19,28
This consolidation of drug-linked associations alters the individual’s psychological relationship with music. A defining feature of Stage 1 is the gradual loss of aesthetic autonomy, defined here as the capacity to engage with music as a self-directed and intrinsically meaningful experience. As musical engagement becomes increasingly subordinated to instrumental goals such as drug seeking or craving regulation, it becomes progressively less likely to function as a reflection of personal taste, emotion, or identity. This shift undermines the role of music as a technology of the self,3 transforming an expressive medium into a conditioned environmental cue. As addiction progresses, music becomes valued less for its aesthetic qualities and more for its utility in amplifying intoxication, priming consumption, or regulating internal states in ways that support substance use routines. This shift is consistent with addiction-oriented studies emphasizing the need to differentiate beneficial from harmful engagement with popular music in the lives of substance users.16,18 Mechanistically, this stage may involve increasing reliance on reward and salience systems that assign motivational significance to cues. This may reduce top-down control over listening choices, so that music selection is driven less by reflective preference and more by cue value and anticipated drug-related effects, making music part of a broader cue repertoire.
Stage 2. Acoustic Erasure: The Cessation Phase
This stage describes acoustic erasure, a state in which music may lose perceived relevance as addiction becomes severe. According to Freimuth’s29 developmental model of addiction, this phase marks the transition into the fully addicted phase, in which addiction becomes the prime motivator guiding behavior and increasingly displaces other sources of interest, meaning, and reward. At this stage, the individual may continue using even after achieving the desired effect, reflecting the growing dominance of addiction over other sources of motivation. Consistent with this shift, addictive behavior in its later stages involves a subjective loss of control over initiation and cessation. This behavior is further characterized as increasingly automatic and less controllable, partly because immediate gratification becomes more salient than delayed adverse effects and awareness of triggers is reduced.30 Qualitative accounts of music use during peak severity describe a trajectory in which music, initially experienced in Stage 1 as a potent enhancer, eventually becomes irrelevant or entirely absent as the pharmacological state comes to dominate the individual’s experience.12
The MRM interprets this acoustic erasure as a severity linked collapse of the aesthetic domain. Within the MRM, this progression is associated with a narrowing of rewards and reduced sensitivity to non-drug reinforcers such as music. Crucially, acoustic erasure represents a tipping point in the psychological economy of the individual: as psychological resources are depleted by the demands of maintaining addiction, music undergoes a functional transformation. Within this logic, acoustic erasure may be understood not only as reduced engagement with music, but as a disruption of the Aesthetic Self, that is, of a domain of identity in which musical meaning and self-continuity are closely linked.4 It shifts from being a companion on the journey to becoming a distressing reminder of the individual’s deterioration. Importantly, acoustic erasure does not necessarily imply the literal disappearance of music. In some cases, this shift may involve the near absence of music from everyday life, whereas in others, music may remain present but lose its synergistic or pleasure-enhancing function and instead become a ruminative mirror of distress, shame, or perceived decline. To manage the cognitive dissonance and the pain of this perceived decline, the individual may erase music from their environment or remain caught in repetitive, distress-linked listening that no longer supports aesthetic autonomy.
The clinical significance of acoustic erasure is strengthened by identity focused scholarship, which suggests that aesthetic engagement forms part of how individuals experience continuity of self. If aesthetic engagement is central to perceived identity, then the collapse of music’s personal meaning constitutes an erosion of a primary identity resource rather than a neutral change in leisure behavior.4 The loss of such an identity anchor may also contribute to experiences of isolation and existential distress, a pattern that resonates with the qualitative themes of solitude and despair identified in recent research on severe substance use.12 In some cases, acoustic erasure may overlap with anhedonic processes, insofar as reduced engagement with music may reflect a broader decrease in responsiveness to naturally rewarding activities relative to the drug.30 Acoustic erasure thus marks not only reduced engagement with music but also diminished narrative continuity and growing disconnection from emotionally meaningful experience, as music ceases to function as a self-directed technology of the self3 and becomes bound up with withdrawal and estrangement.
Stage 3. Stabilization: The Protective Avoidance and Substitution Phase
This stage describes early sobriety coping strategies aimed at stabilizing abstinence in the presence of problematic music cues. One common pathway is protective avoidance, whereby individuals identify music associated with past use as a risk cue and deliberately exclude it in order to reduce acute craving risk. In some cases, this includes complete abstinence from personally salient repertoires tightly linked to prior substance use.13 This pattern is echoed in work using the Musical Presentation technique, an identity-focused group intervention in which participants present personally meaningful music and receive group feedback.31 In a study with formerly incarcerated individuals coping with SUD, this structured intervention was used to explore identity, emotional responses, personal resources, and potential music-related risks in recovery, and participants described refraining from problematic music as a deliberate protective choice after structured reflection.18
A second common strategy in this stage is alternative repertoire substitution, whereby individuals replace problematic music with safer genres, artists, or listening contexts that are less strongly conditioned to past substance use. In treatment settings, this may involve intentionally constructing new playlists, shifting toward unfamiliar repertoire, or turning to music associated with calm, structure, and recovery-oriented routines. Qualitative and intervention focused work suggests that coping in this phase may involve not only identifying and avoiding problematic music, but also actively developing safer musical alternatives that reduce cue density while preserving access to music as a resource for emotion regulation.18,22
Taken together, complete exclusion and substitution with alternative music are often clinically appropriate for short-term stabilization, particularly when coping resources are limited. Their limitation, however, is structural rather than motivational. Because music exposure cannot be fully controlled in everyday life, these strategies may reduce immediate risk without building the skills needed for inevitable encounters. This limitation is amplified in contemporary digital listening environments, where streaming platforms can unpredictably resurface autobiographically linked tracks through recommendation systems and autoplay features, increasing cue density precisely when individuals are relying on environmental control. The risk is especially pronounced when individuals rely on substitution without progressing toward tolerance (Stage 4), given that problematic music cannot be completely avoided outside treatment and that the development of tolerance appears crucial for rehabilitation.22 This dynamic reinforces the rationale for treating Stage 3 as time-limited stabilization and for explicitly preparing clients for subsequent skill-based coping responses that preserve agency during cue exposure.
Stage 4. Active Tolerance: The Desensitization and Reassociation Phase
This stage marks the transition from protective forms of agency, such as avoidance and repertoire substitution, to agency in the presence of problematic music cues. In the context of the MRM, musical agency refers to the shift from being a reactive subject to music cues to becoming an active, self-directed musical agent who can choose, regulate, and reinterpret musical encounters, whether through listening, music-making, or other forms of musical participation. This involves three core capacities: intentionality, or the ability to choose music in accordance with current recovery needs; regulation, or the ability to manage physiological arousal during exposure; and interpretive power, or the ability to assign new and protective meanings to musical material previously associated with substance use. Active tolerance refers to the capacity to encounter problematic music without relinquishing control, a capacity developed through intentional and supported practice rather than passive habituation. In qualitative research on rehabilitated individuals, a Tolerant Group was identified, characterized by the ability to develop resilience by re-associating problematic music with new, sobriety-based meanings.13 Within the MRM, this process is understood as the deliberate attachment of new meaning to an old sound within a structured clinical setting. These newly formed links may be understood as recovery associations: associations that connect formerly problematic music with sobriety, agency, self-regulation, and recovery-oriented identity rather than with substance use. In group music therapy, formerly problematic music may be re-experienced as a positive reminder of recovery commitments and as a warning signal that supports abstinence, thereby transforming the functional meaning of the cue while tolerance skills are being developed.13 Techniques such as the Musical Presentation technique, described above in relation to Stage 3, provide a concrete pathway for this work by bringing harmful music into a secure therapeutic space in which clients can reflect on its meaning and develop awareness and coping responses,18 rather than relying solely on avoidance, which may leave them without the tolerance skills needed outside treatment.22
Mechanistically, Stage 4 can be conceptualized as graded musical exposure paired with real-time regulation and meaning oriented processing, alongside repeated non-drug experiences of the same music within a new interpersonal frame. This phase also requires careful clinical judgment, as not every negative response to music is necessarily harmful. Drawing on the distinction between negative and harmful effects, the therapeutic task in this phase is to distinguish tolerable and potentially productive distress from responses that exceed the individual’s capacity for regulation and undermine safety or engagement.32 In this sense, the controlled exposure involved in Stage 4 may be understood as a form of Optimal Frustration, in which tolerable and contained distress supports the development of new regulatory capacities.33 Drawing on learning-based accounts of cue exposure,34 repeated and controlled contact with problematic music cues without drug reinforcement, when paired with coping practice, may weaken conditioned cue reactivity and strengthen self-efficacy.
Stage 5. Aesthetic Continuity: The Integration Phase
This stage represents a relatively stable late recovery state in which formerly problematic music is no longer primarily experienced as an external threat requiring management, but as an integrated part of the person’s rehabilitated identity and ongoing life narrative. Whereas Stage 4 focuses on the active therapeutic work of reassociation within a guided setting, Stage 5 reflects the consolidation of these changes into a more enduring form of aesthetic continuity. In this phase, music is no longer principally framed by the drug or by the treatment context. Instead, it is re-embedded within the person’s Aesthetic Self, allowing past and present to be linked without compromising sobriety. Music is thus reclaimed not merely as a stimulus to be tolerated, but as a stable resource for identity continuity, self-regulation, and everyday meaning.
The identity significance of this stage is supported by work suggesting that aesthetic tastes and engagements are experienced as central to perceived identity and diachronic continuity.4 The conceptualization of music as a technology of the self similarly supports the idea that music can be actively used to construct and sustain rehabilitated self-states across contexts.3 Within the MRM, Stage 5 therefore marks a shift from defensive management toward a more stable form of identity-based integration.
This integration is not only personal but also social. Recovery often involves movement away from substance-using networks toward recovery-oriented relationships, groups, and communities whose norms support abstinence and long-term rehabilitation.25 Qualitative findings further suggest that formerly problematic music may acquire new, sobriety-based meanings within these recovery-oriented social contexts.13 This process is often facilitated by prosocial musicking ie, the active participation in musical pathways that foster belonging, social resilience, and shared recovery values. The communal dimension of this process is particularly important for understanding musical agency in collectivist settings: agency may be co-constructed rather than residing only in the individual listener’s capacity to choose and regulate music. In such settings, recovery-supportive groups may provide the norms, containment, permission, and interpretive frames that make safe musical re-engagement possible.7,8 Such changes may reconnect music with social belonging and recovery-supportive forms of meaning, thereby countering the profound isolation associated with the more severe stages of addiction and facilitating a transition from aesthetic alienation to social integration.
To account for variation in movement from tolerance to continuity, the model draws on the recovery capital framework. Recovery capital refers to the breadth of internal and external resources available to initiate and sustain recovery and has been conceptualized in terms of human, social, physical, and cultural capital.26 Building on this framework, the MRM introduces Aesthetic Recovery capital as the set of resources that support reintegration in the aesthetic domain. Here, aesthetic recovery capital refers to the accumulated musical, social, and interpretive resources that support the reclamation of music as a recovery resource. This extension is informed by qualitative findings suggesting that music-related recovery processes can be understood through the lens of recovery capital in relation to music-based rehabilitation.18 In this formulation, human capital includes regulation skills and self-knowledge regarding problematic and safe repertoires. Social capital includes supportive recovery-linked relationships and group-based contexts. Physical capital includes access to stable substance-free listening environments and opportunities for participation. Cultural capital includes shifts in musical meanings and norms associated with movement away from addiction and toward recovery. Together, these resources support not only cue management but also the reconstruction of meaning, coherence, and belonging in recovery. For some individuals, this process may also include a spiritual dimension, as spirituality has been identified as a potential resource in recovery processes more broadly.35–37 Within the MRM, however, spirituality is not treated as a universal or required component, but as one possible expression of meaning-oriented reintegration in the aesthetic domain.
Finally, Stage 5 clarifies the non-linear character of the MRM. Because aesthetic recovery capital is cumulative, the skills and reassociations developed in earlier stages remain available even during setback, enabling a more resilient return to integration. In this sense, reclaimed music is no longer merely something to be managed or tolerated, but becomes an enduring resource through which identity continuity, meaning, and social belonging can be sustained over time. To facilitate the clinical application of the MRM, Table 1 provides operational definitions for the core constructs developed across the five stages.
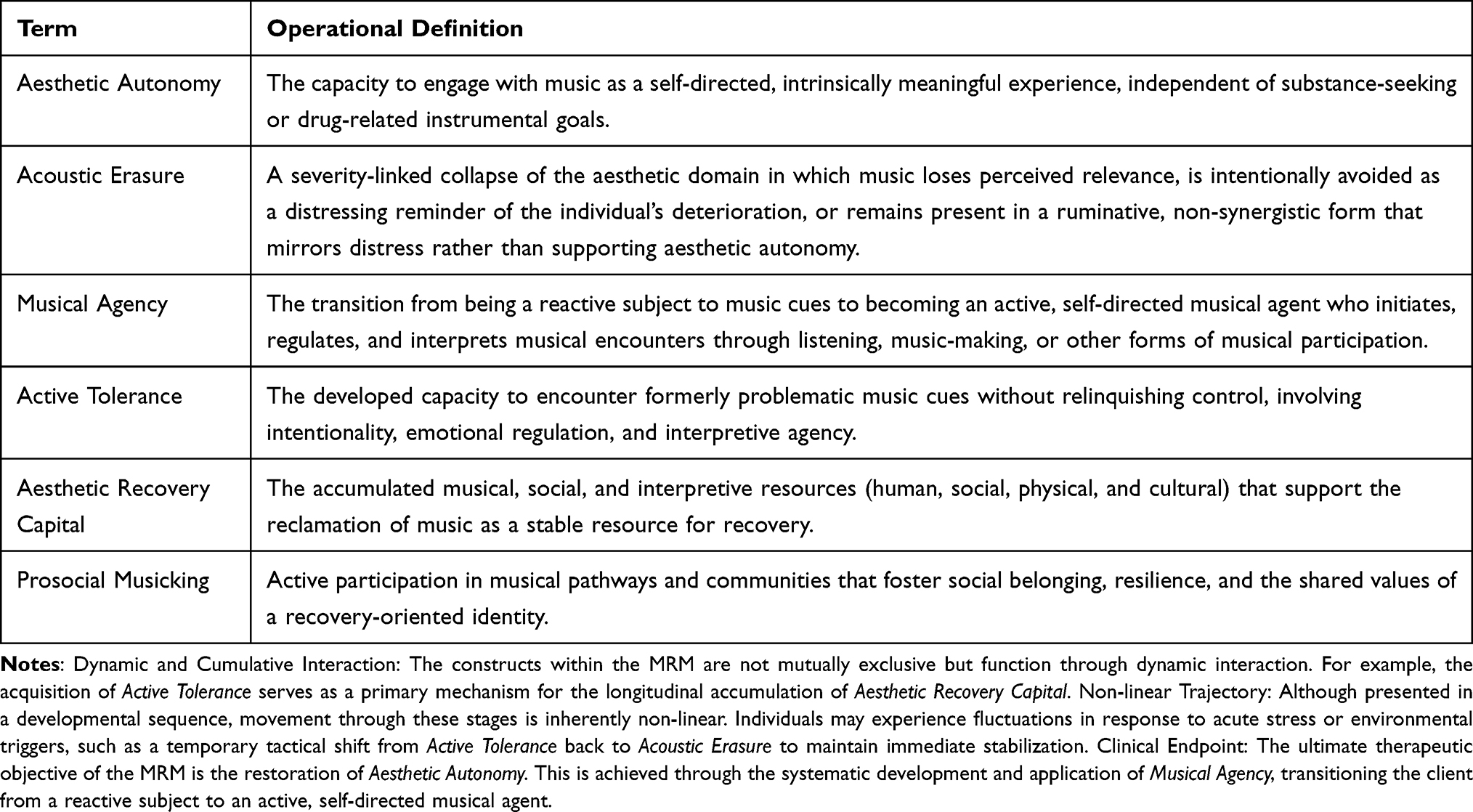 |
Table 1 Core Constructs of the Musical Reassociation Model (MRM) |
From Trigger to Resource: Illustrative Clinical Vignettes
The following vignettes are illustrative clinical examples intended to operationalize the developmental logic of the MRM across stages. Rather than serving as case reports drawn from a specific dataset, they are composite clinical illustrations designed to show how music may shift from a substance-linked enhancer to a conditioned cue, to an avoided trigger, and ultimately to a reintegrated recovery resource. Their purpose is to clarify how stage-based assessment and intervention might be applied in practice while preserving the person-specific relationship between particular substances, musical repertoires, and recovery trajectories. To reduce theoretical repetition and increase clinical transparency, the vignettes include concrete details about listening context, music selection, salient musical and autobiographical features, therapist prompts, client responses, and intervention strategies, drawing selectively on reporting principles for music-based interventions.38
Vignette A: Reassigning Meaning through Controlled Reassociation
This vignette follows a 34-year-old client who used music as a deliberate catalyst during cocaine use. He described a clear Stage 1 synergy in which specific high-tempo electronic tracks were not merely background stimulation but functioned as active amplifiers of intoxication. He recalled that the rhythmic drive of the music intensified the physiological rush of cocaine and made the euphoric state feel more immediate and complete. In his experience, the music operated as part of the consumption ritual itself.
This phase was followed by a Stage 2 period of acoustic erasure during the height of addiction. As cocaine use became more compulsive, the music that had once amplified the high began to feel hollow, emotionally flat, or absent from awareness altogether. In Stage 3, during early recovery, the client adopted alternative repertoire substitution by intentionally building safer playlists of acoustic music. This strategy preserved access to music as an emotion regulation resource, yet craving still emerged when the original drug-linked electronic tracks resurfaced unexpectedly in public spaces or through social sharing.
In one session, the client selected a short excerpt from a high-tempo electronic track that he had repeatedly used while preparing cocaine. Because the clinical aim was controlled exposure rather than musical performance, the therapist used the client’s recorded track, played through speakers in the therapy room at a moderate volume, with the client retaining permission to pause playback. The therapist asked him to identify what made the excerpt risky. He pointed to the repetitive bass line, the accelerating build-up before the drop, and the memory of arranging cocaine on the table while the track was playing. After twenty seconds of listening through speakers in the therapy room, he reported tightness in his chest, a “rush in the legs,” and a brief image of calling former drug-using friends. The therapist paused the playback and asked: “What is the music asking you to do right now, and what do you want to choose instead?” The client replied: “It is pulling me back to the ritual, but I want to pause it, slow down for a moment, and put on something safer instead of following the urge.”
To address this, the therapist collaboratively developed a cue hierarchy based on both musical features and the intensity of autobiographical associations. At the lower end of the hierarchy were unfamiliar acoustic tracks and electronic tracks with similar tempo but no direct link to cocaine use. Intermediate items included brief introductions from formerly used tracks before the drop or peak section. The highest-risk items were longer excerpts from the original playlist, especially sections with a repetitive bass line, accelerating build-up, and strong memories of preparing cocaine. Exposure sessions were time-limited and paired with regulation strategies such as noticing the urge without acting on it, slowing breathing, and grounding attention in the room. The client also practiced stopping playback as a deliberate act of agency rather than as evidence of failure. At times, however, exposure remained difficult. When the client asked to stop the track or return temporarily to safer music, the therapist treated this not as regression but as a protective pause within the process of building tolerance.
Over repeated sessions, craving intensity decreased and self-efficacy increased, supporting movement toward Stage 4 active tolerance. The clinical aim then became deliberate reassociation: selected excerpts of the original electronic playlist were paired with prompts that reframed the music as a reminder of survival and recovery commitments rather than intoxication. The therapist selected excerpts that the client could tolerate without leaving the session or becoming overwhelmed, and each listening trial was followed by a brief reflection on what the sound now represented in recovery. For example, after listening to the opening build-up of one track without acting on the urge, the therapist asked: “What does this track now show you about what you have survived?” The client replied: “It used to mean the start of using. Now it reminds me that I can feel the pull and still choose recovery.” By transforming the music from a catalyst for use into a symbolic anchor for resilience, the client successfully integrated these tracks into his aesthetic recovery capital, utilizing his newly developed human capital (regulation skills) to maintain stability. As the client moved into Stage 5, the playlist was no longer experienced as a threat but as part of a recovered sense of self. For example, when a similar electronic track came on during a car ride with a sober friend, the client kept listening without changing the song and experienced it primarily through the recovery associations formed during treatment, rather than through the earlier cocaine-use ritual. Music became a stable reminder of endurance and an enduring component of his aesthetic recovery capital.
Vignette B: Navigating Digital Environments and Protective Agency
This vignette follows a 27-year-old client whose substance use was closely tied to music during LSD use. In Stage 1, psychedelic trance and progressive electronic music were experienced as integral to the altered state, intensifying immersion and shaping the subjective experience of the drug. He described these tracks as producing tightly fused sensory and autobiographical associations, so that music and intoxication were encoded as a single experiential field rather than as separate elements.
Unlike the client in Vignette A, this client did not report a period of acoustic erasure on entering treatment. Instead, he moved directly from Stage 1 vulnerability into a rigid Stage 3 pattern of protective avoidance, refusing to listen to any music in order to maintain early stabilization. Although this strategy initially reduced risk, it also increased social isolation and removed an important identity resource.
A treatment focus emerged when the client described opening a streaming application after a stressful day and being offered an automatically generated playlist containing psychedelic trance tracks from his period of LSD use. Rather than treating the platform as neutral background technology, the therapist asked the client to show how the recommendation appeared and what he usually did next. The client noticed that the playlist title, cover image, and first track were enough to produce anticipatory arousal before the music even began. Together, they disabled autoplay, separated recovery-oriented listening from older listening histories, and created a substance-free playlist that the client could access quickly when algorithmic cues appeared. Only after this digital safety plan was established did exposure work begin, starting with a moderately associated track selected by the client rather than with the highest-risk music. The exposure used recorded music from the client’s streaming platform, played under therapist supervision, with the client able to stop playback if arousal exceeded his window of tolerance. For this client, moderately associated tracks included psychedelic trance pieces from the same genre that were not linked to specific LSD-use episodes, whereas the highest-risk tracks were those tied to particular drug-use settings, visual imagery, or memories of altered-state immersion.
Exposure work then proceeded through planned listening while the client monitored bodily cues and remained within his window of tolerance.39 The therapist helped the client practice real-time regulation when an unexpected track surfaced, so that the physiological spike of cue exposure could be tolerated without escalating toward lapse. Specifically, the client learned to treat the arousal as an alarm rather than as a command to use, using it as a cue to ground himself, contact support, or shift to a recovery-oriented playlist. Under periods of stress, he temporarily returned to broader avoidance, but these setbacks were incorporated into treatment as opportunities to refine coping and strengthen agency.
In Stage 4, the resurfacing track was gradually redefined as a protective signal that prompted a recovery action, such as grounding or reaching out for support. Across repeated listening tasks and real-world encounters with similar music, the client moved toward Stage 5 integration. He no longer relied on broad avoidance of digital music environments, but navigated them with greater agency. This digital proficiency and interpretive flexibility significantly bolstered his aesthetic recovery capital, specifically his human and cultural capital. For example, when similar psychedelic trance tracks later appeared in a substance-free live music setting, the client stayed with peers who supported his recovery and experienced the music primarily through recovery associations formed during treatment rather than through the earlier LSD-use context. Formerly problematic psychedelic trance and progressive electronic tracks became embedded in a new narrative of resilience, and he reconnected with peers through substance-free live events and recovery-oriented music settings, strengthening the social embedding of this final stage.
Clinical and Systemic Implications
The Musical Reassociation Model (MRM) carries important implications for clinical practice and the broader ecosystem of addiction recovery. At the clinical level, the model suggests that music therapists and addiction counselors move beyond trigger identification alone and use the MRM as a stage-based framework for assessment and intervention planning. A key implication is the need to distinguish between avoidance or alternative repertoire substitution used for short-term stabilization in Stage 3 and structured exposure paired with regulation and reassociation work in Stage 4. In clinical terms, Stage 3 reduces immediate risk through environmental control, whereas Stage 4 builds durable agency for inevitable exposure.
Readiness to move from Stage 3 to Stage 4 should therefore be assessed clinically rather than assumed from the passage of time. Potential markers include the client’s ability to identify specific problematic repertoires and listening contexts, maintain recovery-oriented motivation while discussing these cues, use regulation strategies when mild music-related arousal emerges, return to baseline after limited exposure or imaginal discussion, and distinguish craving from broader emotional distress.11,19 Additional markers include the client’s capacity to collaborate in constructing a graded exposure hierarchy, stable engagement in treatment, access to recovery-supportive relationships, and willingness to stop, pause, or modify exposure as an intentional act of agency rather than as a sign of failure.34
Relapse prevention planning may therefore benefit from incorporating music as a routine assessment domain, including the identification of problematic repertoires and the preparation of contingency plans for accidental exposure. Within this framework, a temporary return from tolerance to avoidance under acute stress may be understood as a deliberate protective maneuver rather than a failure, provided it remains part of a planned trajectory back toward tolerance work. As recovery progresses, the clinical focus may shift from stabilization and safe repertoire building to graded exposure, reassociation, and ultimately to meaning reconstruction and narrative identity work in Stage 5. The Musical Presentation technique, described above in relation to Stage 3, provides one concrete example of identity-focused work that can support music-related risk awareness and recovery-oriented meaning reconstruction.18
At the systemic level, the MRM suggests a shift in how rehabilitation centers manage the soundscapes of recovery. Qualitative findings indicate that prohibitive policies or uniform music bans may foster anxiety without promoting longer-term tolerance, whereas music-therapy-supported environments may offer a pathway toward reclaiming agency over problematic music. This points to the value of multidisciplinary training in which staff across clinical roles are familiar with the stages of the MRM and their transition targets. It also suggests that aesthetic recovery capital may warrant consideration alongside other recovery resources in treatment planning and evaluation.
Finally, the MRM addresses the contemporary challenge of algorithmic delivery. For individuals in Stage 3, streaming platforms may unpredictably surface high-risk tracks through autoplay and recommendation systems. Practical harm-reduction steps, such as disabling autoplay, separating listening histories, and pre-constructing safe playlists, may therefore function as important relapse prevention skills. By treating digital environments as part of cue density rather than as a neutral background, algorithm management can become a meaningful form of aesthetic recovery capital, strengthening the individual’s capacity to navigate digitally mediated exposure in recovery. In this way, the digital sphere may shift from a source of threat to a structured practice ground for agency.
Discussion
The Musical Reassociation Model (MRM) contributes to the literature on addiction and music by reframing music not only as a conditioned cue associated with substance use, but also as a potential recovery resource whose meaning and function may evolve across the course of rehabilitation. Previous research has shown that music can operate as a conditioned stimulus capable of eliciting craving and urges to use.11,19 Neurobiological work further suggests that pleasurable music engages brain reward systems that overlap with those involved in drug reward processing.28 Against this background, the MRM advances a developmental framework that clarifies how the relationship between music and substance use may shift across stages of addiction and recovery. In particular, the model highlights the clinical importance of distinguishing between stabilization strategies based on avoidance and environmental control, and later-stage interventions that cultivate tolerance, regulation, and reassociation in the presence of problematic music cues.
The model also contributes to recovery-oriented theory by connecting cue management with identity reconstruction. In the MRM, acoustic erasure is conceptualized not merely as reduced musical engagement, but as a collapse of an identity-relevant resource. This interpretation is consistent with work suggesting that aesthetic taste and engagement are experienced as central to perceived identity and continuity.4 From this perspective, recovery in the musical domain involves more than symptom reduction. It also involves restoring a medium through which continuity of self, meaning, and belonging may be rebuilt. In this respect, the model aligns with the CHIME framework of personal recovery, which identifies connectedness, hope, identity, meaning, and empowerment as core recovery processes,24 because the MRM similarly treats recovery as a process of rebuilding agency, identity continuity, meaning, and social belonging through the musical domain. At the same time, the MRM extends these frameworks by offering a domain-specific account of how music-related cues may shift from risk factors to recovery resources across distinct stages.
A further contribution of the MRM is its explicit focus on musical agency, defined as the transition from being reactive to music cues to becoming an active, self-directed musical agent. This emphasis challenges the idea that recovery from music-related risk can be achieved through avoidance alone. Although protective avoidance may be necessary in early recovery, the model suggests that long-term rehabilitation may require the development of tolerance, regulation, and new forms of meaning in relation to previously problematic music. In this regard, the MRM is consistent with relapse-prevention approaches that emphasize building coping skills and self-efficacy for responding to high-risk situations, rather than relying solely on efforts to eliminate risk from the environment.40 It also helps explain why accidental or unavoidable encounters with music may become especially important clinical moments rather than mere threats to be eliminated.
The model further addresses the reality of relapse through its non-linear structure. Temporary returns from tolerance to avoidance are not treated as evidence of global failure, but as potentially adaptive forms of short-term stabilization under conditions of acute stress. This position is compatible with the broader relapse literature, including work on the Abstinence Violation Effect, which highlights the risk of construing setbacks as total collapse.41 It also resonates with motivational interviewing’s understanding of behavior change as iterative and recurrent rather than strictly linear.42 Within the MRM, this non-linearity is not peripheral but central: the accumulation of regulatory skills, reassociations, and aesthetic recovery capital means that setbacks need not erase prior gains but may instead be followed by a more rapid and resilient return to integration.
Finally, the MRM provides a conceptual framework through which music-related cues can be assessed and addressed across stages of rehabilitation. By linking cue reactivity, identity reconstruction, and musical agency, the model offers clinicians a structured way to understand how problematic music may shift from a trigger to a recovery resource over time.
Limitations, Future Research, and Conclusion
While the MRM provides a theoretically grounded and clinically actionable framework, it also has limitations that warrant empirical investigation. First, the model remains primarily conceptual and is grounded largely in qualitative evidence, highlighting the need for systematic empirical testing. Future research should examine whether the proposed stage boundaries can be identified reliably across individuals, substances, and treatment contexts, and whether movement between stages follows the developmental logic proposed here. Particular attention should be given to cultural variation, given that musical meanings, listening practices, and the role of music in identity may differ substantially across social and cultural settings.
A second limitation concerns the contemporary digital listening environment, which is likely to shape both cue exposure and recovery trajectories in ways that remain insufficiently understood. Future studies should investigate how variations in algorithmic delivery interact with established individual differences in musical preferences and their psychological correlations. Prior work has shown that musical preferences are associated with stable psychological and personality related differences.5,6 Within the MRM, such personal and technological factors may therefore prove to be important moderators of the model’s applicability and effectiveness. Research should also examine how digitally mediated exposure, including recommendation systems, autoplay, and platform specific listening histories, affects the transition from avoidance to tolerance and from tolerance to integration.
A third priority for future research is intervention testing. Clinical trials should evaluate whether stage-matched music interventions improve outcomes relative to restriction-only approaches, particularly with respect to craving, self-efficacy, relapse vulnerability, identity continuity, and recovery-oriented social engagement. This agenda is consistent with emerging trial protocols on music-based treatment for SUD populations, including a recent multinational randomized controlled trial protocol comparing active music groups, music listening groups, and treatment as usual on addiction severity, recovery, and related outcomes.43 However, future studies should also examine the MRM-specific question of whether matching music-based intervention strategies to recovery stage improves outcomes beyond general music participation. Future research may also translate the model’s clinical observations into stage-linked empirical propositions and measurable indicators. For example, Stages 1 and 3 may be operationalized through cue reactivity and avoidance patterns, whereas Stage 2 may involve both diminished music engagement and reduced responsiveness to non-drug rewards. The transition from Stage 3 to Stage 4 may depend on growing musical agency and the accumulation of aesthetic recovery capital, while the transition from Stage 4 to Stage 5 may be reflected in identity continuity, recovery-supportive meaning, and renewed participation in social forms of musical life. In this way, the MRM may support the development of measurable transition markers, including cue reactivity tasks, ecological momentary assessment of music exposure, and longitudinal indicators of musical agency, identity reconstruction, and aesthetic recovery capital.
In conclusion, the MRM offers a stage-based account of how music may shift across the course of addiction and recovery: from an enhancer of substance use to a conditioned cue, to an avoided trigger, to an object of active tolerance and reassociation, and ultimately to an integrated recovery resource. By bringing together cue reactivity, identity reconstruction, musical agency, and recovery capital, the MRM extends existing accounts of music in SUD beyond trigger management alone. Its central clinical claim is that sustainable rehabilitation may require not only reducing cue reactivity but also reclaiming music as a resource for self-regulation, continuity of self, and social belonging. In this sense, the MRM offers both a conceptual framework for future research and a practical roadmap for engaging directly with problematic music in treatment, not only as a risk to be managed, but as a domain through which recovery may be deepened and sustained.
Generative AI Disclosure and Declaration
The author declares that generative AI tools were utilized in the preparation of this manuscript. ChatGPT (OpenAI, GPT-5.5 Thinking) was used only for language and style editing, while Google Gemini (Google Gemini 1.5 Pro via Imagen 3) was used for assistance in the design and visual refinement of Figure 1. All scholarly judgments, including the conceptualization of the model, interpretation of the literature, and conclusions, were made independently by the author. The author takes full responsibility for the integrity of the whole content, including the accuracy of references and the final content of the manuscript and figure. Furthermore, the author confirms that the originality and accuracy of the content within Figure 1 have been verified. The author has reviewed the applicable terms of use for the AI tools used and confirms that, to the best of his knowledge, their use is suitable for publication. The author further confirms that he has the right to publish Figure 1, that no third-party copyrighted material was intentionally incorporated into the figure, and that any permissions required have been obtained. In compliance with the journal’s policy, all image versions and records of the prompts used have been retained and will be shared upon request.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Ruud E. Music and the quality of life. Nor Tidsskr Musikkter. 1997;6(2):86–14. doi:10.1080/08098139709477902
2. Saarikallio S, Erkkilä J. The role of music in adolescents’ mood regulation. Psychol Music. 2007;35(1):88–109. doi:10.1177/0305735607068889
3. DeNora T. Music in Everyday Life.
4. Fingerhut J, Gomez-Lavin J, Winklmayr C, Prinz JJ. The aesthetic self. The importance of aesthetic taste in music and art for our perceived identity. Front Psychol. 2021;11:577703. doi:10.3389/fpsyg.2020.577703
5. Nave G, Minxha J, Greenberg DM, Kosinski M, Stillwell D, Rentfrow J. Musical preferences predict personality: evidence from active listening and Facebook Likes. Psychol Sci. 2018;29(7):1145–1158. doi:10.1177/0956797618761659
6. Greenberg DM, Kosinski M, Stillwell DJ, Monteiro BL, Levitin DJ, Rentfrow PJ. The song is you: preferences for musical attribute dimensions reflect personality. Soc Psychol Personal Sci. 2016;7(6):597–605. doi:10.1177/1948550616641473
7. Ansdell G, DeNora T. Musical Pathways in Recovery: Community Music Therapy and Mental Wellbeing. Routledge; 2016.
8. Small C. Musicking: The Meanings of Performing and Listening. University Press of New England; 1998.
9. Palamar JJ, Le A. Prevalence of self-reported adverse effects associated with drug use among nightclub and festival attendees, 2019–2022. Drug Alcohol Depend Rep. 2023;7:100149. doi:10.1016/j.dadr.2023.100149
10. Milshteyn Y, Bensimon M. Exploring the subjective experience of rave party participants in Israel who consume psychedelic drugs: a qualitative inquiry. Harm Reduct J. 2023;20(1):176. doi:10.1186/s12954-023-00908-5
11. Dingle GA, Kelly PJ, Flynn LM, Baker FA. The influence of music on emotions and cravings in clients in addiction treatment: a study of two clinical samples. Arts Psychother. 2015;45:18–25. doi:10.1016/j.aip.2015.05.005
12. Lozon J, Bensimon M. The mutual enhancing effect of music and drugs and its eventual cessation in the lives of people coping with substance abuse: a qualitative inquiry. Curr Psychol. 2024;43(8):6995–7006. doi:10.1007/s12144-023-04839-z
13. Lozon J, Bensimon M. A qualitative inquiry on problematic music in the lives of rehabilitated substance abusers: from past-to-present. Int J Offender Ther Comparative Criminol. 2026;70(9):979–1015. doi:10.1177/0306624X2513917
14. Salimpoor VN, Benovoy M, Larcher K, Dagher A, Zatorre RJ. Anatomically distinct dopamine release during anticipation and experience of peak emotion to music. Nat Neurosci. 2011;14(2):257–262. doi:10.1038/nn.2726
15. North AC, Hargreaves DJ. Problem music and self-harming. Suicide Life Threat Behav. 2006;36(5):582–590. doi:10.1521/suli.2006.36.5.582
16. Horesh T. Music is my whole life” - the many meanings of music in addicts’ lives. Music Ther Today. 2006;7(2):297–317.
17. Lozon J, Bensimon M. Music misuse: a review of the personal and collective roles of “problem music. Aggress Violent Behav. 2014;19(3):207–218. doi:10.1016/j.avb.2014.04.003
18. Bensimon M. Beneficial and harmful music for substance use disorder clients: implementation of the musical presentation technique. Arts Psychother. 2024;87:102121. doi:10.1016/j.aip.2024.102121
19. Silverman MJ, Bourdaghs S, Abbazio J, Riegelman A. A systematic review of music-induced substance craving. Music Sci. 2023;27(1):137–175. doi:10.1177/10298649211030314
20. Maasø A, Spilker HS. The streaming paradox: untangling the hybrid gatekeeping mechanisms of music streaming. Pop Music Soc. 2022;45(3):300–316. doi:10.1080/03007766.2022.2026923
21. Pedersen RR. Datafication and the push for ubiquitous listening in music streaming. MedieKultur J Media Commun Res. 2020;36(69):071–089. doi:10.7146/mediekultur.v36i69.121216
22. Lozon J, Bensimon M. A qualitative inquiry into music consumption at drug treatment centers with and without music therapy sessions – challenges, dangers, and successes. J Subst Use Addict Treat. 2025;172:209641. doi:10.1016/j.josat.2025.209641
23. Anthony William A. Recovery from mental illness: the guiding vision of the mental health service system in the 1990s. Psychosoc Rehabil J. 1993;16(4):11–23.
24. Leamy M, Bird V, Boutillier CL, Williams J, Slade M. Conceptual framework for personal recovery in mental health: systematic review and narrative synthesis. Br J Psychiatry. 2011;199(6):445–452. doi:10.1192/bjp.bp.110.083733
25. Best D, Beckwith M, Haslam C, et al. Overcoming alcohol and other drug addiction as a process of social identity transition: the social identity model of recovery (SIMOR). Addict Res Theory. 2016;24(2):111–123. doi:10.3109/16066359.2015.1075980
26. Cloud W, Granfield R. Conceptualizing recovery capital: expansion of a theoretical construct. Subst Use Misuse. 2008;43(12–13):1971–1986. doi:10.1080/10826080802289762
27. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders.
28. Fachner J. Retraining of drug reward, music cues and state-dependent recall in music therapy. Music Med. 2017;9(1):8. doi:10.47513/mmd.v9i1.524
29. Freimuth M. Addicted?: Recognizing Destructive Behaviors Before It’s Too Late. Bloomsbury Publishing PLC; 2008.
30. Sussman S, Leventhal A, Bluthenthal RN, Freimuth M, Forster M, Ames SL. A framework for the specificity of addictions. Int J Environ Res Public Health. 2011;8(8):3399–3415. doi:10.3390/ijerph8083399
31. Bensimon M, Gilboa A. The music of my life: the impact of the musical presentation on the sense of purpose in life and on self-consciousness. Arts Psychother. 2010;37(3):172–178. doi:10.1016/j.aip.2010.03.002
32. Murakami B. The music therapy and harm model (MTHM). ECOS - Rev Científica Musicoter Discip Afines. 2021;6(1):003. doi:10.24215/27186199e003
33. Kohut H. How Does Analysis Cure? University of Chicago Press; 1984. doi:10.7208/chicago/9780226006147.001.0001
34. Loeber S, Croissant B, Heinz A, Mann K, Flor H. Cue exposure in the treatment of alcohol dependence: effects on drinking outcome, craving and self-efficacy. Br J Clin Psychol. 2006;45(4):515–529. doi:10.1348/014466505X82586
35. Flint T, Ronel N. From deprivation to capital - spirituality and spiritual yearning as recovery capital from PTSD. J Aggress Maltreatment Trauma. 2023;32(3):325–345. doi:10.1080/10926771.2022.2146557
36. Harrison K. The social potential of music for addiction recovery. Music Sci. 2019;2:2059204319842058. doi:10.1177/2059204319842058
37. Snodgrass S, Corcoran L, Jerry P. Spirituality in addiction recovery: a narrative review. J Relig Health. 2024;63(1):515–530. doi:10.1007/s10943-023-01854-z
38. Robb SL, Story KM, Harman E, et al. Reporting guidelines for music-based interventions checklist: explanation and elaboration guide. Front Psychol. 2025;16:1552659. doi:10.3389/fpsyg.2025.1552659
39. Siegel DJ. The Developing Mind: How Relationships and the Brain Interact to Shape Who We Are. Guilford Publications; 1999.
40. Marlatt AG, Donovan DM. Relapse Prevention: Maintenance Strategies in the Treatment of Addictive Behaviors. Guilford press; 2005.
41. Curry S, Marlatt GA, Gordon JR. Abstinence violation effect: validation of an attributional construct with smoking cessation. J Consult Clin Psychol. 1987;55(2):145–149. doi:10.1037/0022-006X.55.2.145
42. Miller WR, Rollnick S. Motivational Interviewing: Helping People Change.
43. Geretsegger M, Kirkeng Meling HM, Savinova A, et al. Fighting Addictions, improving Lives through COmprehensive drug rehabilitation with music (FALCO): protocol for an international randomised controlled trial. medRxiv. 2026. doi:10.1101/2026.02.19.26346573
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.