Back to Journals » Journal of Asthma and Allergy » Volume 18
The Morphologic Characteristics of Meibomian Glands in Allergic Conjunctivitis-Related Dry Eye in Children
Authors Tang XJ, Chen L ![]() , Liu Q, Li Y
, Liu Q, Li Y
Received 20 April 2025
Accepted for publication 9 September 2025
Published 13 September 2025 Volume 2025:18 Pages 1269—1281
DOI https://doi.org/10.2147/JAA.S535595
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Luis Garcia-Marcos
Xiao-Jiao Tang,1– 4 Lin Chen,1– 4 Qing Liu,1– 4 Yong Li1– 4
1Department of Ophthalmology, Children’s Hospital of Chongqing Medical University, Chongqing, People’s Republic of China; 2National Clinical Research Center for Child Health and Disorders, Chongqing, People’s Republic of China; 3Ministry of Education Key Laboratory of Child Development and Disorders, Chongqing, People’s Republic of China; 4Chongqing Key Laboratory of Child Neurodevelopment and Cognitive Disorders, Chongqing, People’s Republic of China
Correspondence: Lin Chen, Department of Ophthalmology, Children’s Hospital of Chongqing Medical University, No. 136, Zhongshan 2nd Road, Yuzhong District, Chongqing, 400014, People’s Republic of China, Tel +8618623041022, Fax +86-23-63631759, Email [email protected]
Purpose: To investigate the morphological characteristics of the meibomian glands (MGs) in children with allergic conjunctivitis (AC)-related dry eye (DE).
Methods: Children with a clinical diagnosis of seasonal allergic conjunctivitis (SAC) and perennial allergic conjunctivitis (PAC) were recruited. Age- and sex-matched children without a history of allergy or dry eye were recruited as controls. All participants completed the 5-item Dry Eye Questionnaire (DEQ-5) and ocular surface examination, including assessment of the tear meniscus height (TMH), noninvasive tear breakup time (NIBUT), and morphology of the upper lower MGs by noncontact infrared meibography (Oculus Keratograph 5M). Receiver operating characteristic (ROC) curve analysis was performed to determine the predictive value of the morphological characteristics of the MGs for AC-related DE.
Results: Sixty-two children with AC (31 with DE and 31 without DE) and 33 healthy children were enrolled in the study. The mean age was 7.67 (ranging from 5– 13.5) years. More morphological changes were observed in the upper eyelids of AC children with DE than in healthy children. No morphological feature difference was found between AC children without DE and healthy children. ROC curve analysis showed that the morphological characteristics with good predictive value for DE were shortened upper eyelid MGs (AUC=0.72, P< 0.001) and hooked upper eyelid MGs (AUC=0.71, P< 0.001).
Conclusion: The grading of MG morphology according to the DREAM Study may be a valuable predictor for AC-related DE in children.
Keywords: allergic conjunctivitis, dry eye, children, meibomian glands, morphology
Introduction
Allergic conjunctivitis (AC) is a critical disease entity that significantly impacts the quality of life of children.1 Seasonal allergic conjunctivitis (SAC) and perennial allergic conjunctivitis (PAC) are the most common forms of AC. The main pathological mechanism of the two types is a type I hypersensitivity reaction, affecting at least 15–20% of the population.2,3 Our previous study showed that the incidence of dry eye based on breakup time (BUT) was up to 97.5% in young children with SAC and PAC.4 AC has been reported as a potential risk factor for dry eye (DE) by the TFOS DEWS II study.5 Early studies found that AC-related DE was associated with increased tear stability4 and variation in the tear film lipid layer.6,7 The TFOS DEWS II classified DE into two primary categories, aqueous deficient DE and evaporative DE.8 In clinical studies, evaporative DE is more common than aqueous deficient DE and is associated with tear instability and an abnormal tear film lipid layer.
Meibomian glands (MGs) are large sebaceous glands located in the tarsal plates of the eyelids. Their function is to synthesize and secrete lipids, which distribute to the ocular surface and constitute the main lipid component of the outer layer of the tear film, maintaining the stability and reducing the evaporation of the tear film.9 Meibomian gland dysfunction (MGD) is a leading cause of dry eye, especially evaporative dry eye.10 AC-related morphological changes in the MGs have been gradually confirmed. Liu et al11 found that the rate of MG distortion and dropout in patients with SAC was dramatically higher than that in normal controls. Arita et al12 reported that PAC was associated with increased meibomian gland duct distortion. MG alterations and dysfunction have been found in atopic keratoconjunctivitis (AKC) and vernal keratoconjunctivitis (VKC) patients.13,14 Therefore, MGD is recognized as a long-term complication of AC.5
The MG morphology is a sensitive indicator of the function of MGs.15 With the application of noninvasive and infrared imaging technology, MG morphology has become an important means of clinically evaluating MG function. The grading of the MG morphology has gradually improved from grades 0−316 and grades 0−417 based on the area of MG atrophy/loss to the grading standard for 13 specific features recommended by the Dry Eye Assessment and Management (DREAM) study.18 Although there is no uniform international grading standard, increasingly detailed MG morphology grading in clinical studies has made grading analysis for MG morphology a potential tool for predicting DE.
Recently, Ahrentschildt et al19 analysed the characteristics of the MGs based on the DREAM study and found some marginally predictive morphology metrics in contact lens wearers with dry eye diseases (DED). Although some studies have confirmed the morphological changes of the MGs of AC patients, the predictive value of the metrics of these characteristics for AC-related DE remain unclear. Studies on MG morphology in children with AC are rare. The purpose of this study was to grade the morphologic characteristics of the MGs based on the DREAM study morphology metrics and assess the predictive value of these morphologic characteristics in AC-related DE in children.
Materials and Methods
Subjects and Study Protocol
This prospective, case-control study was carried out at the Outpatient Department of Ophthalmology in the Children’s Hospital of Chongqing Medical University from 1 May 2022 to 30 December 2022 in Southwest China. This study was approved by the Ethics Committee of the Children’s Hospital of Chongqing Medical University, Chongqing, China (NO.2022–529). Informed consent was obtained from the parents or guardians of the children. All procedures were conducted in accordance with the principles of the Declaration of Helsinki.
SAC and PAC were clinically diagnosed based on the criteria of Chinese expert consensus, including subjective symptoms (ocular itching, lacrimation, hyperaemia, and foreign body sensation) and clinical signs (conjunctival hyperaemia, conjunctival oedema, and conjunctival follicles) assessed by slit lamp examination.20 The age range of the participants recruited was 5 to 14 years. This age bracket was selected because allergic conjunctivitis (AC) is especially prevalent in pediatric populations, and this specific range enabled us to focus on a group where the condition is most frequently observed in clinical settings. Additionally, children within this age range generally demonstrated sufficient compliance during clinical examinations, which ensured the reliability and accuracy of the data collected. The control group comprised 33 age- and sex-matched children undergoing physical examination without a history and any symptoms of allergies or ocular surface abnormalities. Patients were excluded from the study if they had any of the following: (1) systemic administration of anti-allergy drugs, glucocorticoids, immunosuppressants or topical ocular medication within 3 months; (2) a history of ocular trauma or ocular surgery; (3) active ocular infection; (4) diabetes, kidney disease or immune system diseases with the potential to confound the results of the study; and (5) poor cooperation with everting the lids, resulting in low-quality MG images. For participants enrolled in the study, data collection and eye examination were performed as shown in Supplemental Figure 1.
Questionnaire on Dry Eye
The 5-item Dry Eye Questionnaire (DEQ-5) was used to evaluate the symptoms and intensity of dry eye in the past month and is currently available and reliable for use in children.21 Each subject was asked to complete a DEQ-5 for assessment of the severity of dry eye symptoms.
Ocular Surface Examination
Patients sat in front of the device (Keratograph 5M, OCULUS, Germany), and the chin was rested on a chin strap. The lower TMH was measured in tear meniscus mode. The mean of three measurements was recorded. The NITBUT was also measured using the Keratograph 5M. The average NIBUT (NIBUT-avg) was calculated automatically by the software. DE was diagnosed if the child had a TMH of <0.2 mm or NITBUT of <10 seconds in the worst eye19 and a DEQ-5 score >6.
Infrared Meibography and Morphological Characteristic Grading
Infrared photography of the upper and lower MGs was performed using the Keratograph 5M. The morphologic characteristics were analysed according to the grading standard of the DREAM study,18 including distorted, tortuous, hooked, shortened, thickened, thinned, overlapping, ghost, and tadpoling MGs and MGs with abnormal gaps, fluffy areas, dropout, and no extension to the lid margin (Table 1).
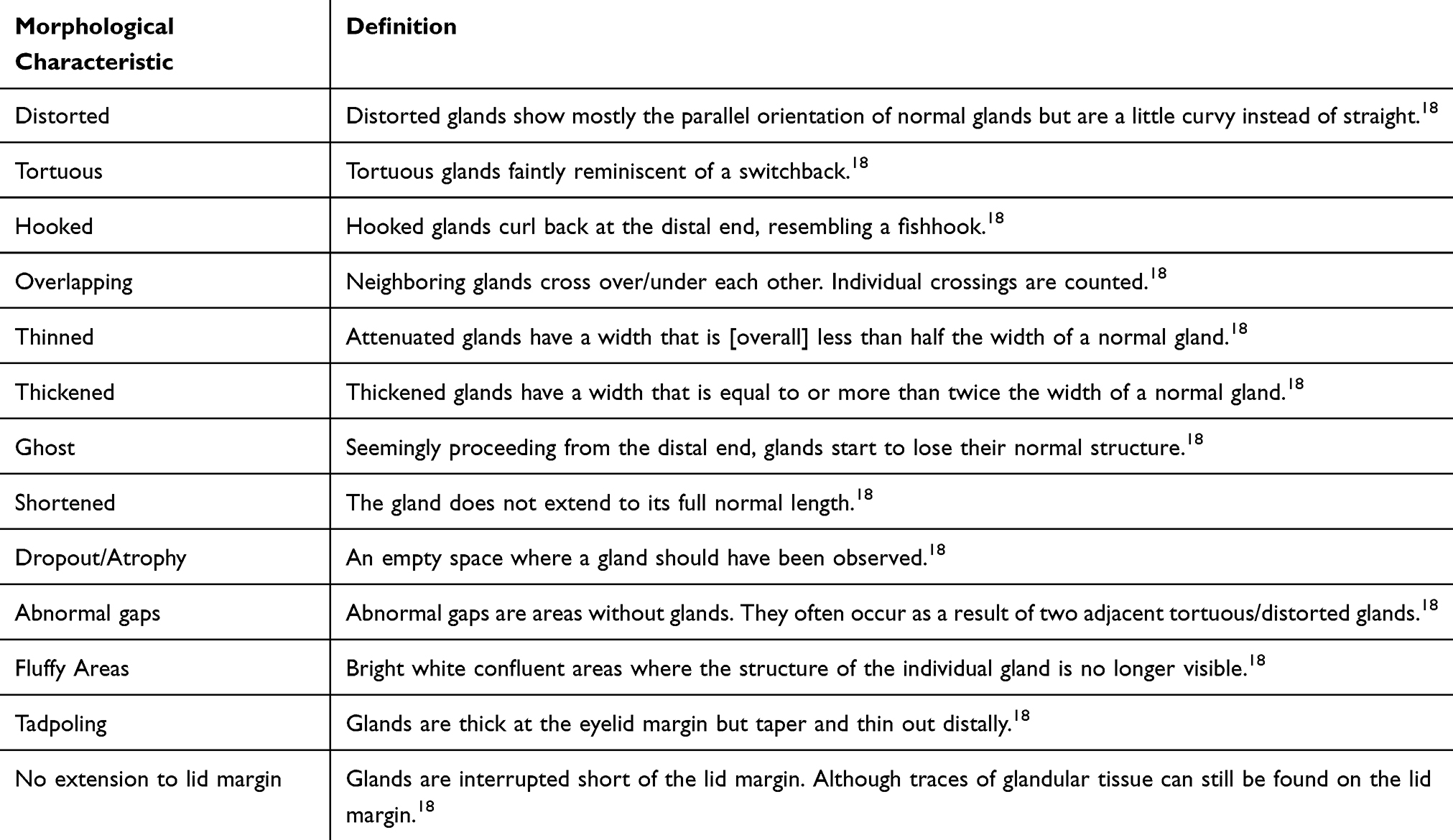 |
Table 1 Illustrations and Descriptions of Meibomian Gland Morphologic Characteristics Based on the DREAM Study |
Quality Control
Two readers received training in the assessment of the 13 morphological characteristics of MGs for 1 month. After the training, the readers were required to analyse the features of 20 images. Two weeks later, readers were required to grade the same 20 images to measure the interreader and grade-regrade consistency test. During the study, if the two readers were inconsistent in describing the features of the images, a third person (the study quality controller) joined in the evaluation and discussion. When two of them reached a consensus, the grading data were included in the final analysis.
Statistical Analysis
All the subjects received examinations of both eyes and the right eye was selected for analysis. Data were analysed by using SPSS version 22.0 software (SPSS, Inc., Chicago, IL). The interreader and intrareader consistency were evaluated using test-retest reliability. The intraclass correlation coefficient (ICC) was used to evaluate continuous variables. Cohen’s Kappa coefficient was used to evaluate the categorical variables. Values for continuous variables are given as the means and standard deviations (SD). Continuous data between the groups were compared using Student’s t test. The categorical variables were compared with the chi-square test. One-way ANOVA was used for comparisons among the three groups. Receiver operating characteristic (ROC) curve analysis was used to analyse the predictive value of the MG morphological characteristics for DE. The area under the curve (AUC) with 95% confidence interval (CI) was calculated for each morphological feature. P values less than 0.05 were considered statistically significant.
Results
A total of 62 children with AC and 33 healthy children were enrolled in the study. The mean age was 7.67±2.12 (ranging from 5–13.5) years. There were no significant differences in age or sex among the three groups (P>0.05). The clinical characteristics of the patients are shown in Table 2. The duration of AC with DE (Group A) was significantly longer than that of AC without DE (Group B) (6.77±1.03 vs 3.39±0.69 months, P<0.01). The DEQ-5 score of Group A was significantly higher than that of Group B (P<0.0001). The TMH and NIBUT were statistically different among the three groups (F=13.66, P<0.001 and F=3.11, P=0.049, respectively). Intrareader and interreader consistency assessment showed that the MG morphological features had good consistency (Supplemental Tables 1–3).
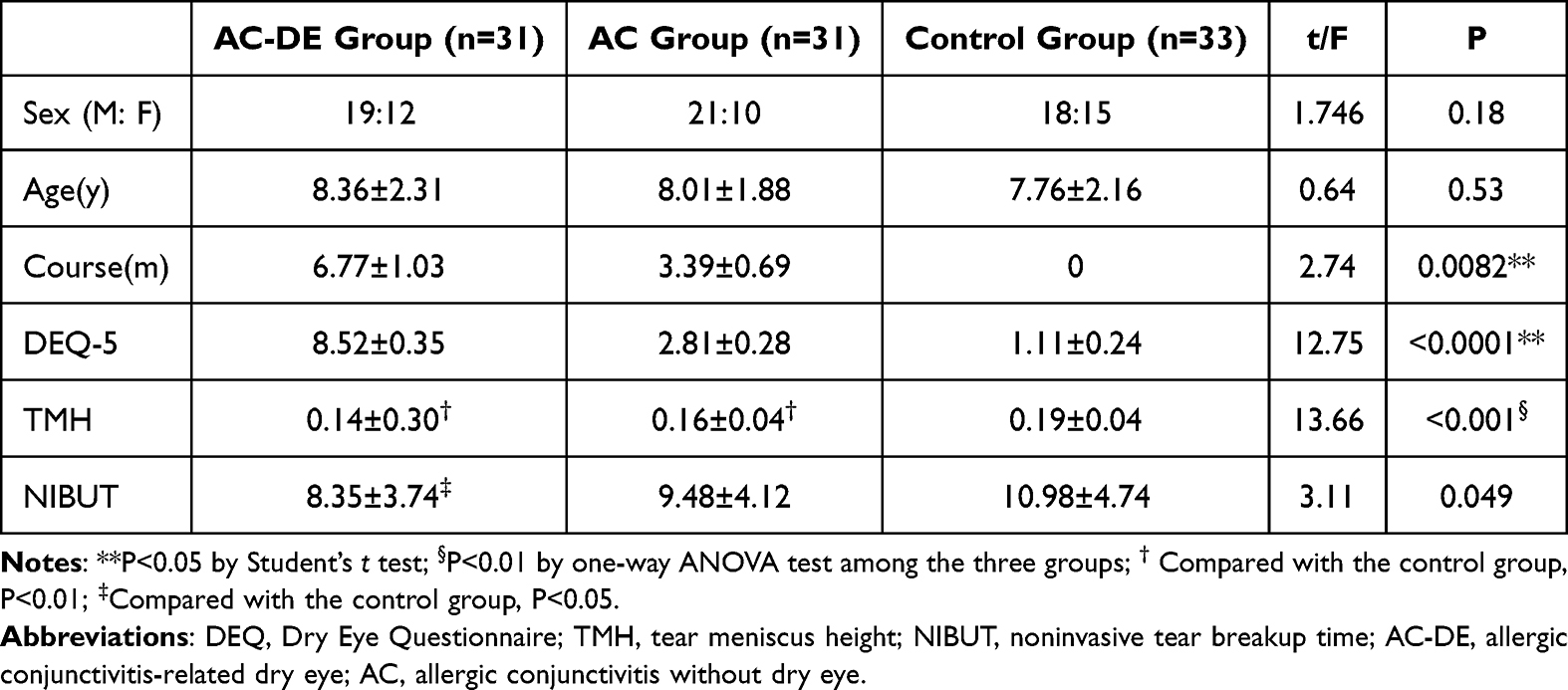 |
Table 2 Clinical Characteristics of the Subjects |
Table 3 shows the morphological characteristics of MG between AC children with and without DE. Among AC children, distorted lower eyelid MGs, hooked upper eyelid MGs, hooked mean upper plus lower eyelid MGs, overlapping lower eyelid MGs, abnormal gap in upper eyelid and in upper plus lower eyelid were more common in DE children than in non-DE children.
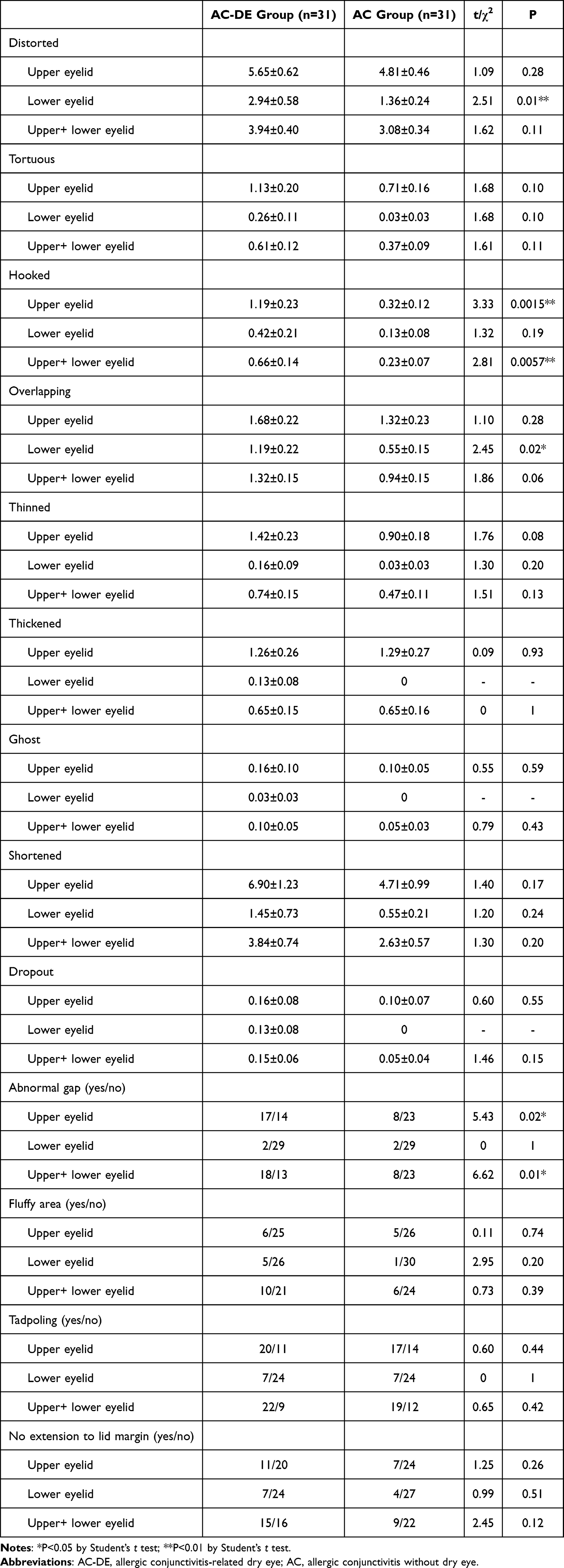 |
Table 3 Comparison of Morphological Characteristics of the Meibomian Glands Between Children in Allergic Conjunctivitis with and Without Dry Eye Groups |
Table 4 shows the morphological characteristics of MG between AC with DE and healthy children. Compared with the control group, the AC-related DE group more significantly demonstrated distorted upper eyelid MGs, distorted lower eyelid MGs, distorted mean upper plus lower eyelid MGs, tortuous upper eyelid MGs, tortuous mean upper plus lower eyelid MGs, hooked upper eyelid MGs, hooked mean upper plus lower eyelid MGs, overlapping lower eyelid MGs, overlapping mean upper plus lower eyelid MGs, thinned upper eyelid MGs, thinned mean upper plus lower eyelid MGs, shortened upper eyelid MGs and shortened mean upper plus lower eyelid MGs. Among categorical variables, morphological characteristics with significant differences among the groups included abnormal gap in upper eyelid and in upper plus lower eyelid, fluffy area in lower eyelid and in upper plus lower eyelid, tadpoling MGs in upper eyelid and in upper plus lower eyelid, and no extension to lid margin in upper eyelid and in upper plus lower eyelid.
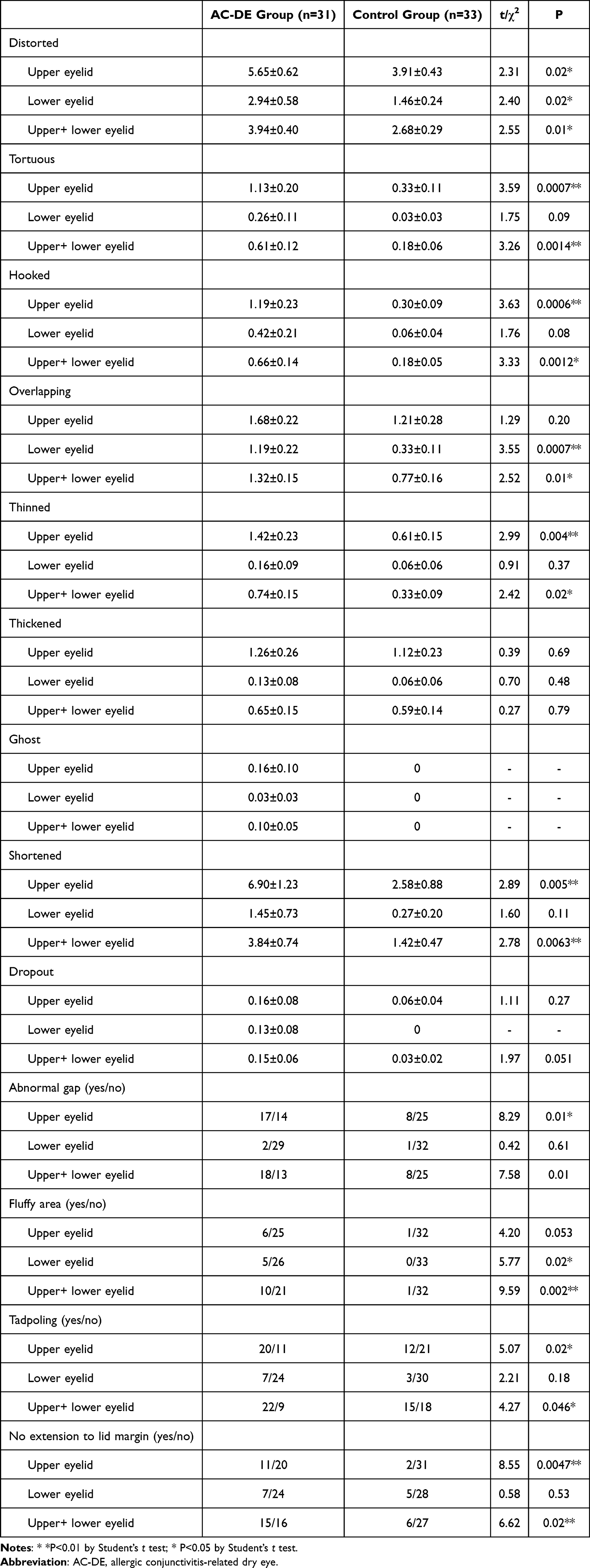 |
Table 4 Comparison of Morphological Characteristics of the Meibomian Glands Between Children with Allergic Conjunctivitis with Dry Eye and Healthy Children |
As shown in Table 5, no MG morphological characteristics in the upper or lower eyelid were found to be significantly different between the children with AC without DE and healthy children. The mean values of the morphological characteristics of the upper and lower eyelids were also not statistically significant compared with those of the control group.
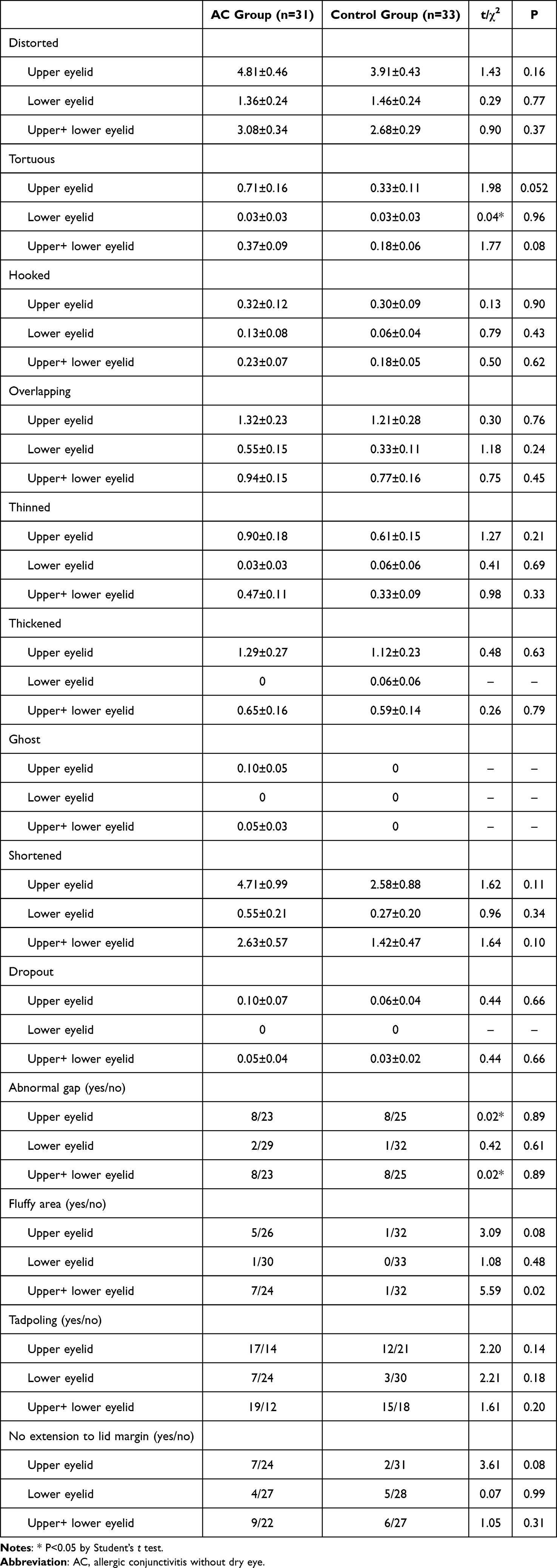 |
Table 5 Comparison of Morphological Characteristics of the Meibomian Glands Between Children with Allergic Conjunctivitis Without Dry Eye and Healthy Children |
ROC curve analysis of the MG morphology characteristics showed those with predictive value for DE in children with AC (Supplemental Table 4). Five morphological characteristics with predictive value were observed in the upper eyelid, including tortuous, hooked, thinned, shortened MGs and abnormal gap, with AUCs ranging from 0.65 to 0.72 (Figure 1A). In the lower eyelid, distorted (AUC=0.68, P<0.01) MGs and overlapping (AUC=0.69, P<0.01) MGs were predictive characteristics (Figure 1B). Combined analysis of the upper and lower eyelids revealed tortuous, hooked, overlapping and shortened MGs as predictive characteristics, but with AUCs ranging from 0.60 to 0.69 (Figure 1C). The morphological characteristics with the best predictive ability were tortuosity in the upper eyelid (AUC=0.71, P<0.001) and shortened shapes in the upper eyelid (AUC=0.72, P<0.001).
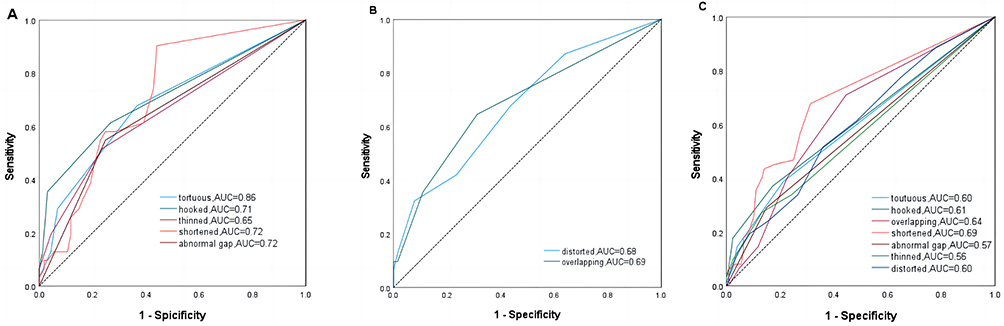 |
Figure 1 The Predictive Role of Statistically Significant Characteristics according to ROC Curve Analysis. (A) ROC curve analysis for the selected characteristics in the upper eyelid. (B) ROC curve analysis for the selected characteristics in the lower eyelid. (C) ROC curve analysis for the selected characteristics in the mean of the upper and lower eyelids. |
Discussion
AC is a critical disease affecting the quality of life of children,1 with progressively increasing incidence in developing countries.22 An unstable tear film, variation in the tear film lipid layer and a high tear evaporation rate in AC patients have been verified to be associated with DE.12,23 MG morphology has been proven to be associated with the function of the MGs.24 In this study, we observed the morphologic characteristics of the MGs based on the grading standard of the DREAM study in children with AC to investigate their predictive value for AC-related DE. Our results showed that the most highly predictive morphologic characteristics (AUC>0.70, P<0.01) of AC-related DE in children were shortened upper eyelid MGs and hooked upper eyelid MGs. However, no morphological feature differences were found between children with AC without DE and healthy children.
Abnormal MG morphological characteristics in AC patients have been described in the previous literature, including tortuousness, distortions and shortening.11,12,23 However, there is no uniform standard for evaluating the morphological characteristics of MGs. Recently, Daniel et al18 improved and detailed the grading of MG morphology and provided more evidence for studying the relationship between the characteristics of MGs and DE. However, there are few studies and reports on dry eye in children. In the current study, we found no significant difference in MG morphology between AC children without DE and normal controls. Our results showed that tortuous MGs in the upper eyelid and distorted MGs in the upper +lower eyelids were obviously more common in AC-DE children than in healthy children. Our findings agree with those of Arita et al12 who found increased MG duct distortion in PAC and contact lens-related allergic conjunctivitis (CLAC). Both distortions and tortuousness indicate curved changes in the straight morphology of MG and were associated with DE in patients with AC in this study. In addition, since the lower eyelid MG is shorter and thicker than that of the upper eyelid,25 it may be more likely to overlap when distortion or tortuousness is present,18 which may explain why distorted and tortuous MGs were more common in the upper eyelid but overlapping MGs were more common in the lower eyelid.
ROC curve analysis showed that the morphological characteristics with the best predictive value (AUC>0.70, P<0.01) for AC-related DE were shortened upper eyelid MGs and hooked upper eyelid MGs. Few previous studies have reported on shortened MG in children with AC, and more studies have focused on MG loss/atrophy6,11,26 and its associated meiboscore.12 A higher meiboscore in the upper and lower eyelids, especially in the upper eyelid was found in AC children, which is similar to the findings of the current study.6 The meiboscore is graded by the proportion of meibomian gland loss (MGL). Shortened MGs in the current study were defined as MGs that did not extend to their full normal length,18 that is, the terminal region of the shortened MG is equivalent to the region of MGL in two-dimensional images. The difference between the two terms is that the former is counted by shortened MG, while the latter is graded by the proportion of loss. Yang et al6 found that upper eyelid MGL was associated with smaller lipid layer thickness in paediatric patients with SAC and PAC. Decreased lipid layer thickness and blinking disorders in paediatric patients with AC may contribute to lipid layer deficiency. Xiao and et al26 found that MG length was a good predictor for MGD. These findings preliminarily explain why shortening has good predictive value for DE in AC children.
The hooked MG is distinguished from the distorted and tortuous MG, defined as curling back at the distal end, resembling a fishhook.18 The current study found that hooked upper MGs were a good predictor of AC-related DE in children. This morphological feature has rarely been reported in children in the previous literature. In China, Zhao et al described hooked MGs in children without symptoms of DE, but their role in predicting DE diagnosis has not been studied.27 In terms of appearance, the hook in a hooked MG is located at the end of the gland, which resembles a tortuous MG, sometimes with gland shortening. In other words, the hook may be a special morphology that combines tortuousness and shortening.
This is a preliminary study on the predictive value of MG morphological characteristics for AC-related DE in children, and there are some limitations. First, this study did not evaluate ocular surface indicators (such as ocular surface staining, TBUT, Schirmer test, tear film lipid layer, etc.) and MG secretions; therefore, the relationship between the observed MG morphology and changes in the ocular surface or/and tear film and its influence on the pathogenesis of AC-related DE cannot be explained. Second, the current study only enrolled children with SAC and PAC. Neither atopic keratoconjunctivitis (AKC) and vernal keratoconjunctivitis (VKC) populations nor adults and elderly individuals were enrolled in this study. The pathogenesis of AKC and VKC is not the same as that of SAC and PAC, involving instead a combined impact of both type I and type IV reactions. Ageing is a significant factor affecting MG morphology and function.28 Further study should be carried out to clarify the morphological characteristics of the MGs in these populations. Last, the sample size of this study is small and from a single centre, and a larger sample size and multicentre study will be conducted in the future to verify the accuracy and sensitivity of the predicted features.
Despite these limitations, in this study, we found that the MG morphology grading system of the DREAM study may be a valuable in predicting AC-related DE in children. Paediatric ophthalmologists should focus on shortened upper eyelid MGs and hooked upper eyelid MGs in children with AC. By incorporating early screening protocols, developing targeted interventions, and enhancing patient education, clinicians have the potential to substantially reduce the burden of DE in this vulnerable paediatric population.
Data Sharing Statement
The data is available on request from the corresponding author.
Ethical Approval
This study was approved by the Ethics Committee of the Children’s Hospital of Chongqing Medical University, Chongqing, China (NO.2022-529). Informed consent was obtained from the parents or guardians of the children. All procedures were conducted in accordance with the principles of the Declaration of Helsinki.
Acknowledgments
We are grateful to the parents and children for participating in the study. We are grateful to the staff at the Department of Ophthalmology, Children’s Hospital of Chongqing Medical University collected the clinical information (nonfinancial). This submission has not been published anywhere previously and that it is not simultaneously being considered for any other publication.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No financial support was received for this submission.
Disclosure
No financial or non-financial benefits have been received or will be received from any party related directly or indirectly to the subject of this article. None of the following authors have any proprietary interests or conflicts of interest related to this submission.
References
1. Zhang SY, Li J, Liu R, et al. Association of Allergic Conjunctivitis With Health-Related Quality of Life in Children and Their Parents. JAMA Ophthalmol. 2021;139(8):830–837. doi:10.1001/jamaophthalmol.2021.1708
2. La Rosa M, Lionetti E, Reibaldi M, et al. Allergic conjunctivitis: a comprehensive review of the literature. Ital J Pediatr. 2013;39(1):18. doi:10.1186/1824-7288-39-18
3. Miyazaki D, Fukagawa K, Okamoto S, et al. Epidemiological aspects of allergic conjunctivitis. Allergol Int. 2020;69(4):487–495. doi:10.1016/j.alit.2020.06.004
4. Chen L, Pi L, Fang J, Chen X, Ke N, Liu Q. High incidence of dry eye in young children with allergic conjunctivitis in Southwest China. Acta Ophthalmol. 2016;94(8):e727–e730. doi:10.1111/aos.13093
5. Stapleton F, Alves M, Bunya VY, et al. TFOS DEWS II Epidemiology Report. Ocul Surf. 2017;15(3):334–365. doi:10.1016/j.jtos.2017.05.003
6. Yang B, Wen K, Li J, et al. Quantitative evaluation of lipid layer thickness and blinking in children with allergic conjunctivitis. Graefes Arch Clin Exp Ophthalmol. 2021;259(9):2795–2805. doi:10.1007/s00417-021-05199-9
7. Suzuki S, Goto E, Dogru M, et al. Tear film lipid layer alterations in allergic conjunctivitis. Cornea. 2006;25(3):277–280. doi:10.1097/01.ico.0000178277.29010.bc
8. Craig JP, Nichols KK, Akpek EK, et al. TFOS DEWS II Definition and Classification Report. Ocul Surf. 2017;15(3):276–283. doi:10.1016/j.jtos.2017.05.008
9. Knop E, Knop N, Millar T, Obata H, Sullivan DA. The international workshop on meibomian gland dysfunction: report of the subcommittee on anatomy, physiology, and pathophysiology of the meibomian gland. Invest Ophthalmol Vis Sci. 2011;52(4):1938–1978. doi:10.1167/iovs.10-6997c
10. Nichols KK, Foulks GN, Bron AJ, et al. The international workshop on meibomian gland dysfunction: executive summary. Invest Ophthalmol Vis Sci. 2011;52(4):1922–1929. doi:10.1167/iovs.10-6997a
11. Liu L, Yang J, Ji W, Wang C. Assessment of Meibomian Gland (MD) Impairment Among Seasonal Allergic Conjunctivitis (SAC) Patients. Med Sci Monit. 2022;28:e935359. doi:10.12659/msm.935359
12. Arita R, Itoh K, Maeda S, et al. Meibomian gland duct distortion in patients with perennial allergic conjunctivitis. Cornea. 2010;29(8):858–860. doi:10.1097/ICO.0b013e3181ca3668
13. Ibrahim OM, Matsumoto Y, Dogru M, et al. In vivo confocal microscopy evaluation of meibomian gland dysfunction in atopic-keratoconjunctivitis patients. Ophthalmology. 2012;119(10):1961–1968. doi:10.1016/j.ophtha.2012.04.001
14. Wei Q, Le Q, Hong J, Xiang J, Wei A, Xu J. In vivo confocal microscopy of meibomian glands and palpebral conjunctiva in vernal keratoconjunctivitis. Indian J Ophthalmol. 2015;63(4):327–330. doi:10.4103/0301-4738.158073
15. Adil MY, Xiao J, Olafsson J, et al. Meibomian Gland Morphology Is a Sensitive Early Indicator of Meibomian Gland Dysfunction. Am J Ophthalmol. 2019;200:16–25. doi:10.1016/j.ajo.2018.12.006
16. Arita R, Itoh K, Inoue K, Amano S. Noncontact infrared meibography to document age-related changes of the meibomian glands in a normal population. Ophthalmology. 2008;115(5):911–915. doi:10.1016/j.ophtha.2007.06.031
17. Pult H, Riede-Pult B. Comparison of subjective grading and objective assessment in meibography. Cont Lens Anterior Eye. 2013;36(1):22–27. doi:10.1016/j.clae.2012.10.074
18. Daniel E, Maguire MG, Pistilli M, et al. Grading and baseline characteristics of meibomian glands in meibography images and their clinical associations in the Dry Eye Assessment and Management (DREAM) study. Ocul Surf. 2019;17(3):491–501. doi:10.1016/j.jtos.2019.04.003
19. von Ahrentschildt A, Hanenberg L, Robich ML, et al. Morphological characteristics of Meibomian Glands and their Influence on Dry Eye disease in contact lens wearers. Ocul Surf. 2022;24:93–99. doi:10.1016/j.jtos.2022.01.002
20. Sánchez-Hernández MC, Montero J, Rondon C, et al. Consensus document on allergic conjunctivitis (DECA). J Investig Allergol Clin Immunol. 2015;25(2):94–106.
21. Chidi-Egboka NC, Golebiowski B, Lee SY, Vi M, Jalbert I. Dry eye symptoms in children: can we reliably measure them? Ophthalmic Physiol Opt. 2021;41(1):105–115. doi:10.1111/opo.12762
22. Lu CW, Fu J, Liu XF, et al. Air pollution and meteorological conditions significantly contribute to the worsening of allergic conjunctivitis: a regional 20-city, 5-year study in Northeast China. Light Sci Appl. 2021;10(1):190. doi:10.1038/s41377-021-00630-6
23. Gu T, Zhao L, Liu Z, Zhao S, Nian H, Wei R. Evaluation of tear film and the morphological changes of meibomian glands in young Asian soft contact lens wearers and non-wearers. BMC Ophthalmol. 2020;20(1):84. doi:10.1186/s12886-020-1328-2
24. Kim HM, Eom Y, Song JS. The Relationship Between Morphology and Function of the Meibomian Glands. Eye Contact Lens. 2018;44(1):1–5. doi:10.1097/icl.0000000000000336
25. Ban Y, Shimazaki-den S, Tsubota K, Shimazaki J. Morphological evaluation of meibomian glands using noncontact infrared meibography. Ocul Surf. 2013;11(1):47–53. doi:10.1016/j.jtos.2012.09.005
26. Xiao J, Adil MY, Olafsson J, et al. Diagnostic Test Efficacy of Meibomian Gland Morphology and Function. Sci Rep. 2019;9(1):17345. doi:10.1038/s41598-019-54013-4
27. Zhao Y, Chen S, Wang S, et al. The significance of meibomian gland changes in asymptomatic children. Ocul Surf. 2018;16(3):301–305. doi:10.1016/j.jtos.2018.03.006
28. Den S, Shimizu K, Ikeda T, Tsubota K, Shimmura S, Shimazaki J. Association between meibomian gland changes and aging, sex, or tear function. Cornea. 2006;25(6):651–655. doi:10.1097/01.ico.0000227889.11500.6f
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.