Back to Journals » Psychology Research and Behavior Management » Volume 15
The Mediating Role of Social Support in the Relationship Between Psychological Capital and Depression Among Chinese Emergency Physicians
Received 10 February 2022
Accepted for publication 8 April 2022
Published 20 April 2022 Volume 2022:15 Pages 977—990
DOI https://doi.org/10.2147/PRBM.S360611
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Haibo Xu,1,2 Xin Liu,1,2 Ping Zeng3
1Center for Mental Health Education and Research, Xuzhou Medical University, Xuzhou, Jiangsu, People’s Republic of China; 2School of Management, Xuzhou Medical University, Xuzhou, Jiangsu, People’s Republic of China; 3School of Public Health, Xuzhou Medical University, Xuzhou, Jiangsu, People’s Republic of China
Correspondence: Haibo Xu, Email [email protected]
Purpose: Depression is common in medical practitioners across all stages of their careers, but few studies have explored positive factors for combatting depression in emergency physicians. This study aims to explore the association between psychological capital and depression among Chinese emergency physicians, along with the mediating role of social support in this relationship.
Methods: A cross-sectional survey was conducted at 33 grade III and class A general hospitals in 13 cities of Jiangsu Province, China. Emergency physicians participating in the study completed 568 questionnaires on psychological capital, social support, and depression. Regression analysis was applied to explore the relationship between psychological capital, social support, and depression, and to assess the mediating role of social support.
Results: The rate of potentially depressed physicians was determined as 18.5% among our study sample. Depression was negatively correlated with psychological capital (r = − 0.384, p < 0.01) and its four components of hope, self-efficacy, resiliency, and optimism, and negatively correlated with social support (r = − 0.299, p < 0.01). Depression was negatively affected by psychological capital (c = − 0.398, p < 0.001), or by both psychological capital (c′ = − 0.334, p < 0.001) and social support (b = − 0.171, p < 0.001), and social support was positively affected by psychological capital (a = 0.372, p < 0.001), leading to a mediation effect of − 0.064 and accounting for approximately 16.0% of the total effect of psychological capital on depression. Furthermore, social support exhibited a potent mediating role for emergency physicians with potential depressive disorder compared to those without depression.
Conclusion: Psychological capital not only can directly affect depression, but can also alleviate it by increasing social support. Hospitals should pay attention to the mental health status of emergency physicians, and psychological capital training and emotional support can be implemented to improve mental health.
Keywords: depressive symptoms, psychological capital, social support, influence mechanism, emergency physician
Introduction
Depression is a common neuropsychiatric disorder characterized by sadness, loss of interest or pleasure in life, feelings of tiredness, and poor concentration.1 More than 300 million people suffer from depression worldwide, equivalent to 4.4% of the world’s population.1 It is projected that by 2025, the prevalence of mental disorders in China will increase by approximately 10% to 36.9 million.2 In extreme cases, depression can lead to suicide, with the number of victims close to 0.8 million per annum.1 One might be shocked by this statistic, but what is the status quo for those who provide professional medical care and emergency assistance in regard to depression or suicidal tendencies?
“Put on your own oxygen mask before assisting others.” — Randy Pausch, The Last Lecture.
Depression and Suicidal Tendency in Medical Practitioners
Depression is as common in medical practitioners across all stages of their careers as in the general population,3,4 occurring much more frequently than with other professionals,5 with the morbidity of depression among medical practitioners estimated between 12.1% and 19.3%.6 More specifically, it was disclosed that the prevalence of depression among resident physicians was 28.8% and increased year by year;7 among residency trainees in general surgery, the prevalence of depression approached 40%,8 and approximately 61.7% of nurses presented with different degrees of depression in a study conducted in China.9 Another mental health survey of primary-care physicians in China showed that 31.7% suffered from depression.10 There have been few studies on depression among emergency physicians in China, and a new study shows that a total of 35.6% of emergency physicians suffered from depression among 15,243 national samples.11
Since the 1960s, many studies have confirmed that medical practitioners have a higher rate of suicide than other professionals, with depression as the leading risk factor.3 Critical risk factors for depression and suicidal attempt in physicians include work stress and burnout.4 Burnout affects 76% of resident physicians and around 70% of physicians.12 Furthermore, the problem of depression and suicidal tendency in physicians often leads to the remarkable (and tragic) distinction of having more successful suicides than the general population.13 It was reported that over 400 physicians took their own lives in the US each year, presumably related to increasing depression.6 In addition to suicide, the sudden death of physicians in China also poses a concern. Research has indicated that nearly 3 physicians died from sudden death every month in 2017.14 However, physicians per se do not often recognize the symptoms of depression, and they seek help even less often.5
In addition, physicians are frequently affected by the intensity of clinical practice, the higher risk of litigation, and the chronic fatigue of circadian rhythm disruption, all of which particularly predispose emergency physicians (EPs) to a high risk of depression,15 which is exacerbated by their arduous working conditions including significant psychological demands, lack of resources, and poor supports.16 In China, physicians also suffer from public distrust. Research has shown that between 2011 and 2016, the percentage of people who trusted their physicians fell from 83.4% to 64.2%.17 As public trust declines, the trend of violent events against physicians remains ongoing.18 All of these factors cause physicians to live under great psychological stress. Due to the low level of public awareness and stigma of depression,19 many physicians with depressive symptoms in China would be reluctant or embarrassed to seek professional medical care,20 different from the concern of western physicians about repercussions to their medical licensure.21 Rather, they might attempt to deal with substance abuse, depression, or suicidal thoughts alone,6 indicating the urgent need for additional professional supports for physicians with depression.4
Psychological Capital as a Positive Psychological Resource for Addressing Depression
Psychological capital (PsyCap) is defined as “a positive state of mind exhibited during the growth and development of an individual”, comprising four core components: self-efficacy, optimism, hope, and resiliency.22 As a beneficial resource, PsyCap was reported to be negatively associated with depression,23 and all four of its components positively related to the adaptive response to depression.24 Those physicians with high anxiety scores displayed the potential signs of developing depression,25 and PsyCap was demonstrated to be a protective factor for fighting against anxiety and depression.23,26
Social Support as a Positive Social Resource for Depression
In parallel, the ability of social support (SS) to serve as a crucial social factor with beneficial effects on human health has long been recognized27 and well documented for several decades now.27,28 People persist, cope, and thrive not as isolated individuals but as members of social groups.29 Therefore, most patients long to receive SS from their physicians, friends, and family.30 SS, as a “stress buffer”, can reduce anxiety symptoms31 and to a certain extent can alleviate an individual’s stress and improve individual physical and mental health.32 SS reportedly mediates, at least in part, the relationship between optimism and depression among women at risk for breast cancer33–35 and serves as a full mediator of the effects of HIV stigma on both depression and quality of life.36 Thus, we hypothesize that SS acts as a mediator in the relationship between PsyCap and depression for Chinese EPs.
In summary, a wealth of literature has validated the mediating role of SS in depression.37 However, due to the paucity of publications on the relationship between PsyCap, SS, and depression for physicians—especially regarding EPs—it is of great practical significance to explore the relationship between these factors for the sake of improving the health level and medical service quality of EPs in China. The present study aims to make such an effort and bridge this gap. We hypothesized that a) depression negatively relates to PsyCap and its four factors, as well as SS; and b) SS mediates the pathways of PsyCap and its major factors on depression.
Methods
Participants and Procedure
In July and August 2017, a cross-sectional survey was performed at 33 grade III and class A (top-level) general hospitals in 13 prefecture-level cities of Jiangsu Province in eastern China (see Figure 1). A randomized cluster sample was used to select qualified emergency departments from those hospitals, and an anonymous self-assessment questionnaire was distributed to all selected participants (emergency physicians).
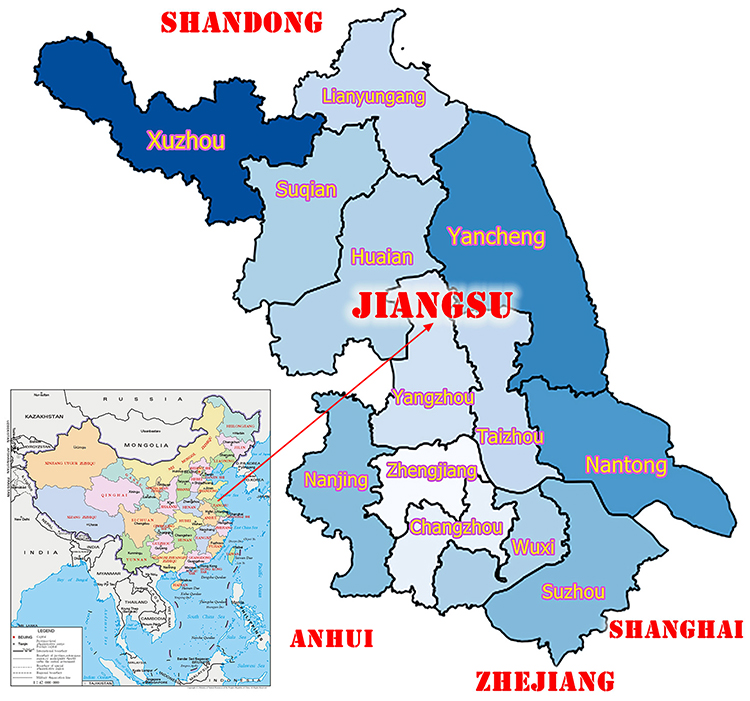 |
Figure 1 Administrative divisions of prefecture-level cities of Jiangsu Province, China. |
The inclusion criteria for participants included: first, being regular staff who are certified as emergency physicians and work in hospitals; second, having no cognitive impairment and being able to understand the questions on the questionnaire; and third, voluntarily participating in our survey and following the principle of informed consent.
Procedures and quality control included: 1) all investigators were trained to guarantee the standardization of the survey; 2) prior to the formal measurement, the investigators meticulously clarified the questionnaire profiles and conducted on-site questionnaire distribution, followed by an on-site request for the questionnaire completion and submittal to ensure the validity and the response rate; 3) the questionnaires with missing or incorrect items were screened to ensure the accuracy of statistical data, and cases with missing data were deleted; 4) during data entry, all the records were inputted and verified by two investigators for consistency.
Ethical Considerations
This study was reviewed and approved by the Ethics Committee of Xuzhou Medical University. All participants were informed about the purpose of this study, in accordance with the Declaration of Helsinki. The survey was conducted under the consent of the participants, and was also approved and assisted by the relevant hospital administrators. The participants were informed about 1) the purpose and procedures of the study, and 2) the privacy protection policy. The data collected will only be used for relevant research and will not be used for any other purposes that may violate personal privacy.
Measures
The general questionnaire comprised two sections. In the first part, the social demographic and other relevant features of the EPs, such as gender, age, educational background, work-years, professional post, current position-years, and hospital grade were anonymously self-reported and recorded. In the second part, the assessment and diagnostic instruments utilized in our survey consisted of three scales (Chinese versions), including the Symptom Checklist-90, Psychological Capital Questionnaire, and Social Support Rating Scale. All three scales were standardized, suitable for the Chinese population, and had high reliability and validity, as detailed below.
Symptom Checklist-90 (SCL-90)
The Symptom Checklist-90-Revised is a 90-item self-reported symptom inventory developed by Leonard R. Derogatis in the mid-1970s and widely employed to measure psychological status or screen for mental disorders.38 SCL-90 is scored with a Likert 5-point scale, with a higher score representing a more evident degree of depression. Both the overall SCL-90 scale (Cronbach’s α = 0.96) and the depression subscale (comprising 13 items, with Cronbach’s α = 0.82) have strong internal consistency.39 An average score of 2 points for the depression subscale was employed as the cut-off value to calculate the detection rate and to determine whether the respondents (ie, EPs) would likely exhibit depression.40 Of note, there is no significant difference in the detection rate (p > 0.05) compared with that yielded by the mean score of the scale norm, indicating that this cut-off value (ie, 2 points) can be directly applied. In this study, the total reliability of SCL-90 was 0.973 and the reliability of the depression subscale was 0.912.
Psychological Capital Questionnaire (PCQ-24)
PsyCap was measured via the Psychological Capital Questionnaire, which was developed by Luthans et al with a high internal consistency coefficient.22 The PCQ-24 consists of four dimensions (self-efficacy, hope, optimism, and resilience), with each dimension including six items. Each of the items is scored on a Likert 6-point scale, with 1 indicating potent disagreement and 6 indicating strong agreement. A higher score generally indicates a higher level of PsyCap and better mental health. In this study, the total reliability of the PCQ-24 scale was 0.933.
Social Support Rating Scale (SSRS)
The Social Support Rating Scale, designed by Xiao in 1986, was adopted to measure an individual’s social support within three dimensions: objective social support, subjective social support, and social support availability.41 Objective social support represents visible, or practical, support, as well as direct material support, along with the existence and participation of social networks and group relations. Subjective social support refers to an emotional experience in which the individual is respected, supported, and appreciated in society. Social support availability indicates the degree of individual acceptance and utilization of social support. There are 10 items in the SSRS, with each worth 1–4 points and a higher score representing a better general SS. In this study, the total reliability of SSRS was 0.886.
Statistical Analysis
Data Detection Method
The Harman’s single-factor test and variance inflation factor (VIF) test were employed to assess the common method bias (CMB) and the multicollinearity of variables. Most studies using the Harman’s single-factor test have adopted a single factor by which the variation to be interpreted cannot exceed 40% or 50%,42 while VIF of less than 10 often indicates the absence of multicollinearity.43
Descriptive Statistics
The socio-demographic characteristics were described with mean and standard deviation (SD) for continuous variables (eg, the score for depression, PsyCap, or SS) or rate (or proportion) for discrete variables (eg, gender or educational background). The independent samples t-test and one-way analysis of variance (ANOVA) were used to describe and compare the socio-demographic data (eg, gender, age, and working-years) and the distribution of the score of depression symptoms. The Bonferroni correction was performed for multiple testings when the results of variance analysis were significant. The Pearson and Spearman rank correlation analyses were used to describe the correlation among socio-demographic variables, depression, SS, and PsyCap (and its components).
Regression Analysis
Multiple-linear regression was applied to explore the relationship between depression, PsyCap, and SS; the mediation analyses were utilized to examine the mediating effect of SS on the pathway from PsyCap to depression (see Figure 2).44–47 In the mediation analysis, we employed the joint significance test method to evaluate the significance of the estimated mediation effect.48 In addition, c is the total effect; c′ is the direct effect of PsyCap on depression; a is the effect of PsyCap on SS; and b is the effect of SS on depression. The mediating effect can be calculated by the product of a and b (ie, a × b); and we have the following relationship in the linear mediation analysis: c = ab + c′. SPSS 22.0 was used for all data analysis. All significance tests were two-sided with a significance level of 0.05.
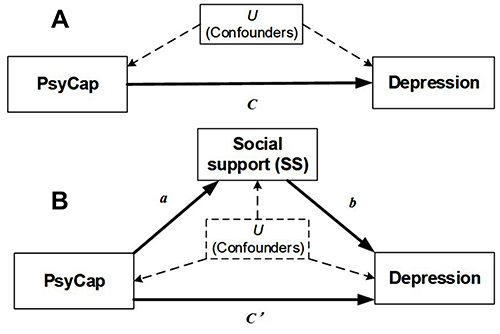 |
Figure 2 Conceptual and statistical diagram of the mediation analysis for the relationship between psychological capital (PsyCap), social support (SS) and depression. (A) Relationship between PsyCap and depression; (B) Relationship between PsyCap, SS and depression. Here, PsyCap serves as the exposure, SS as the mediator, depression as the outcome, and U the confounding factor. |
Results
Sample Description
A total of 593 EPs were recruited for this study, among whom 568 submitted valid questionnaires (total effective rate 95.8%), including 356 (62.7%) males and 212 (37.3%) females. The majority of participants (55.3%) were ages 26–35. Most (67.6%) of the participants had less than 10 years of working experience, and most (57.6%) had a master’s degree or higher level of education. Nearly half (47.9%) were residents or interns. Sample details are shown in Table 1.
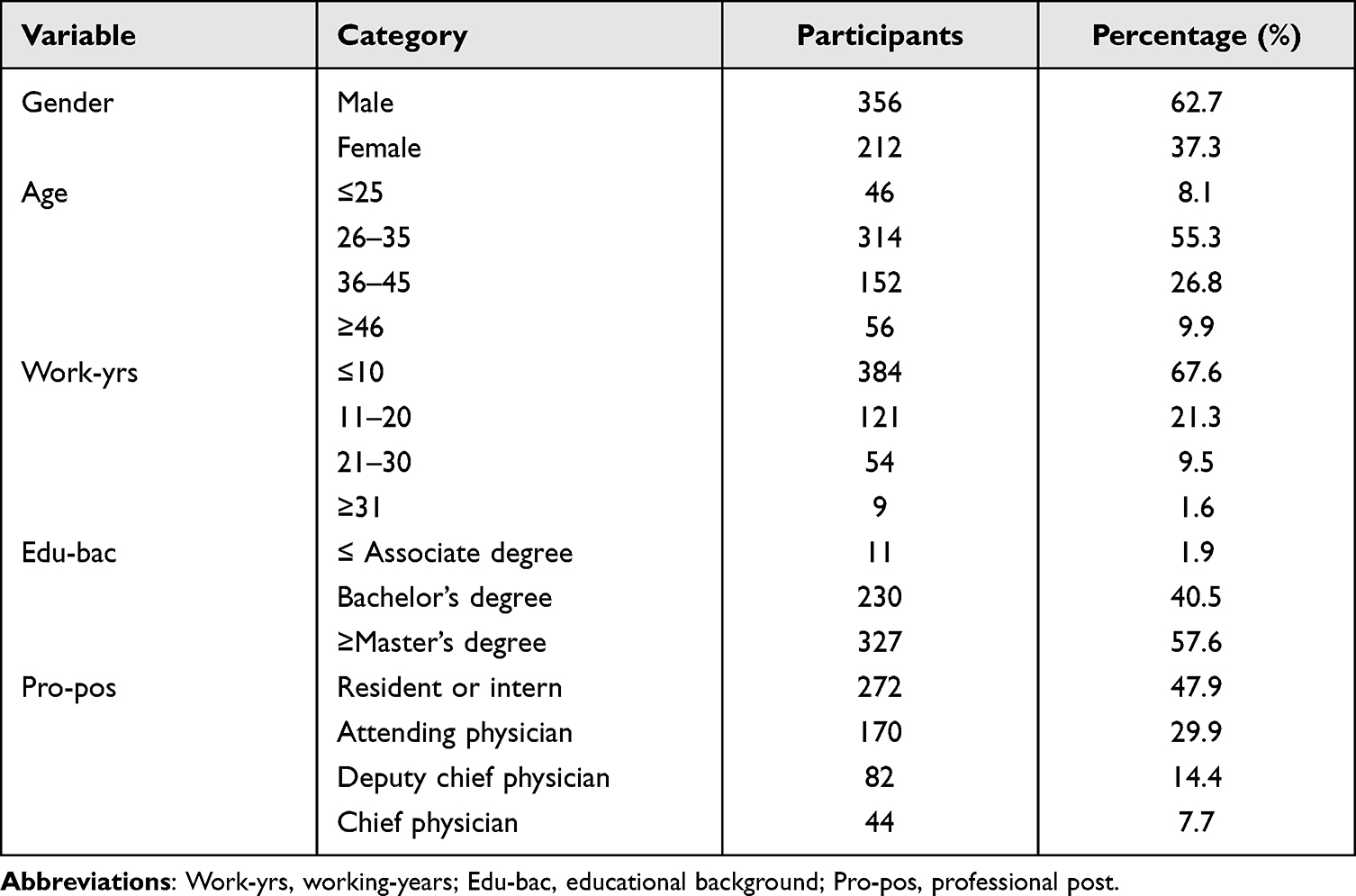 |
Table 1 Collation and Analysis of Participants’ Demographic Information |
The Harman’s single-factor test revealed that the proportion of the variance interpreted by the first factor was 35.0% and the estimated VIF ranged between 1.2 and 3.1, indicating modest evidence for the presence of CMB and multicollinearity in our data.
Degree of Depression
Table 2 shows that the average score of depression among overall EPs was 1.54 ± 0.55. There was a significant difference in depression among EPs with various working-years (p < 0.001). Specifically, the EPs with 11–20 working-years on average had the highest depression score. There was no evident difference in depression with respect to gender, age, educational background, and professional post. In addition, there were 105 EPs who had an average depression score of ≥ 2, resulting in an overall rate of depressive disorder (DepD) of 18.5% (= 105/568) and corresponding to an average DepD score of 2.45 (SD = 0.52). Among them, the detection rate of DepD was 23.1% (= 49/212) in females and much higher than that in males (15.7% = 56/356), and there were significant differences in the DepD among different educational backgrounds (p = 0.005). More specifically, the EPs with a master’s degree or above on average had the lowest depression scores.
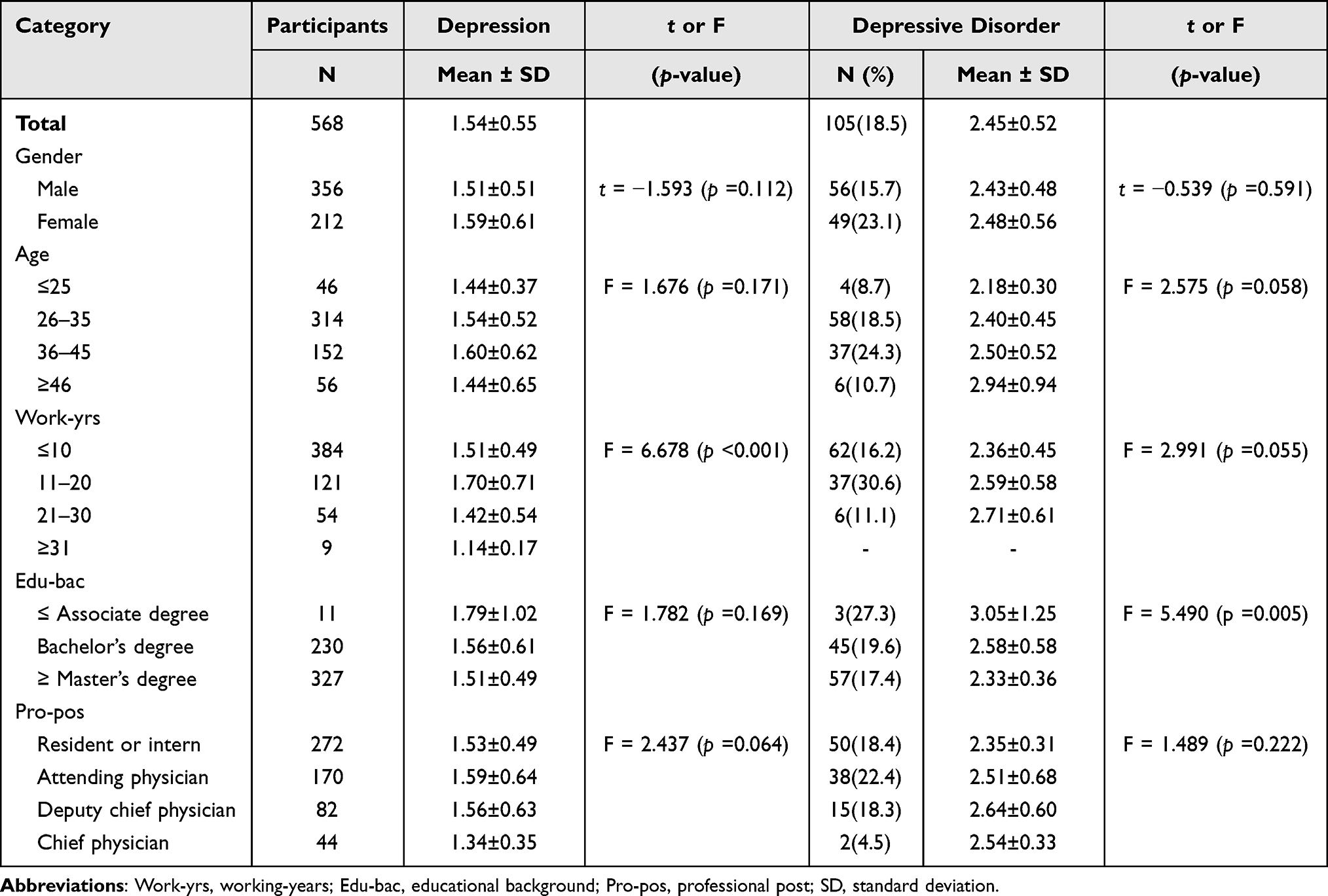 |
Table 2 Depression and Depressive Disorder Among Emergency Physicians |
PsyCap Level
No gender difference was observed in PsyCap among the EPs studied (p = 0.472), but there were substantial distinctions in the age level (p < 0.001), working-years (p = 0.009), and professional post (p < 0.001). Specifically, the EPs of age 46 or above, on average, had higher scores than those of age 35 or below. The difference in PsyCap score was only significant between the EPs with 10 working-years or below and those with working-years of 21 and 30. The EPs whose professional post was chief physician had higher scores than those who held the professional post of resident, intern, or attending physician (see Table 3).
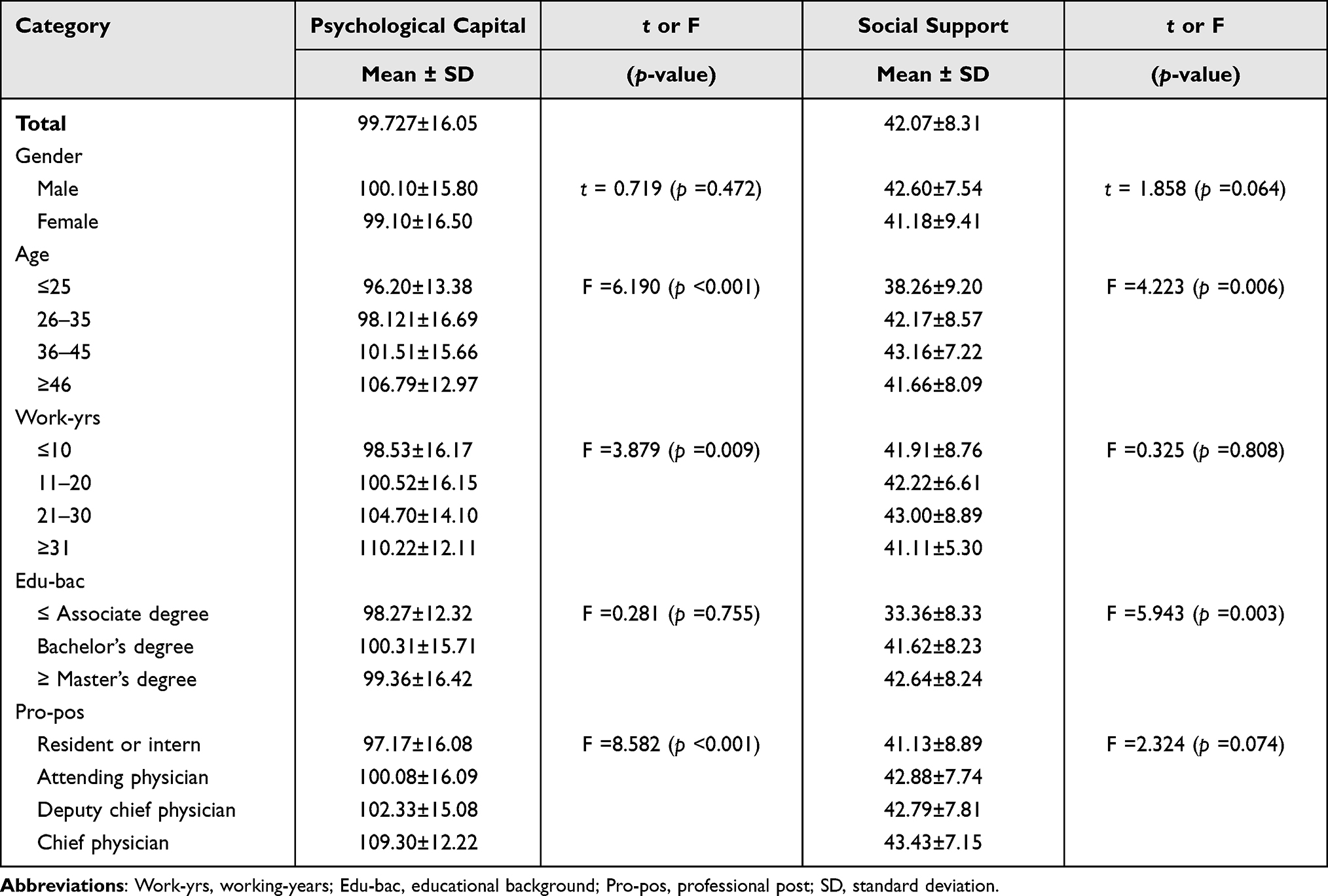 |
Table 3 Psychological Capital and Social Support Among Emergency Physicians |
Social Support
No difference in the SS score was observed in regard to gender, working-years, and professional post (p > 0.05), but there were significant differences in the SS score for age (p = 0.006) and educational background (p = 0.003). More specifically, the EPs below age 25 exhibited a lower SS score compared to others, except for those of age 46 or above. Further, the EPs with a master’s degree or above on average had the highest SS scores. In addition, the SS score typically increased with higher educational level as well as professional post (see Table 3).
Correlation Analysis
A non-significant correlation existed between the depression score and all the socio-demographic factors (Table 4), whereas depression was negatively related to PsyCap (r = −0.384, p < 0.01) and its four factors, including hope (r = −0.360), self-efficacy (r = −0.184), resiliency (r = −0.387), and optimism (r = −0.344), and was also negatively associated with SS (r = −0.299, p < 0.01). Furthermore, we identified a positive correlation between PsyCap and SS (r = 0.264, p < 0.01; Table 4).
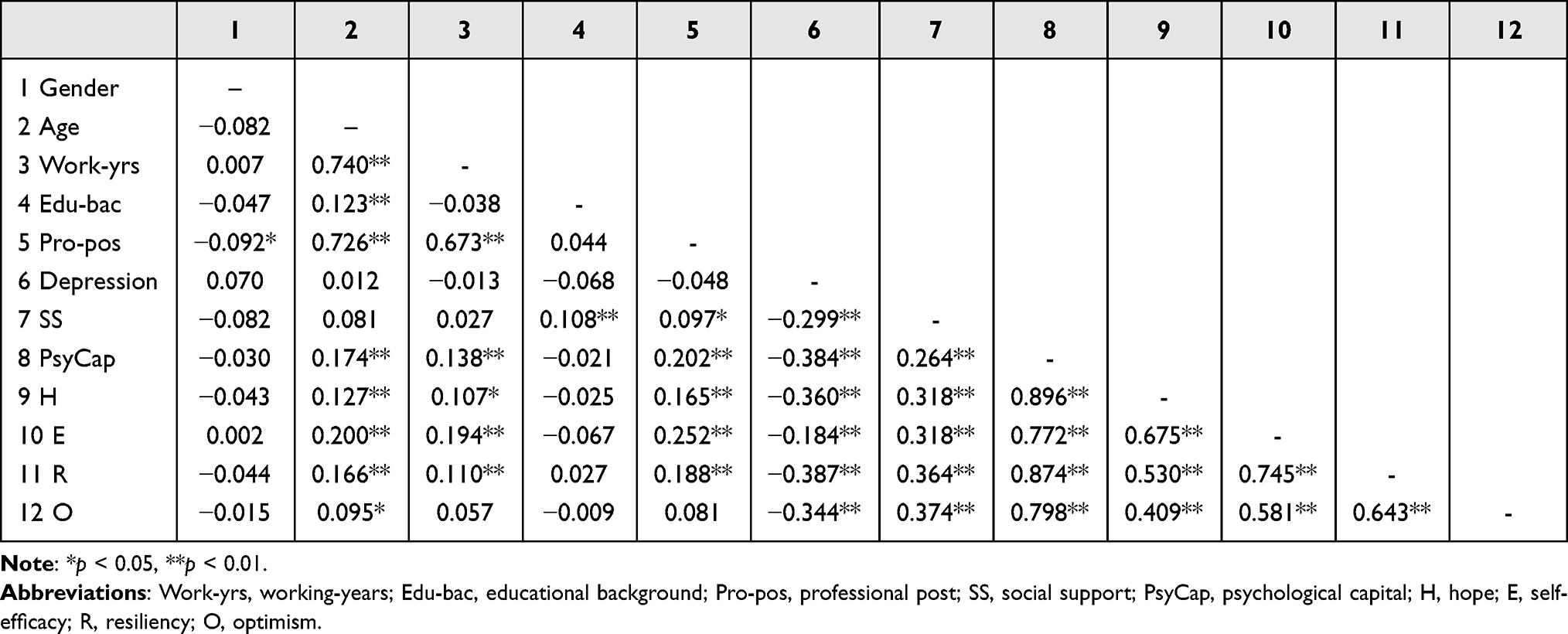 |
Table 4 Correlation Analysis of Socio-Demographic Factors and Variables |
Multiple Regression and Mediation Analyses
Regression analysis was conducted to explore whether PsyCap had an effect on depression and whether SS could mediate the effect of PsyCap (Figure 2). To achieve these goals, multiple models with standardized scores for PsyCap, SS, and depression were fitted (Table 5). M1 was employed to confirm the overall relationship between PsyCap and depression (ie, H0: c = 0), M2 was utilized to explore the relationship between PsyCap and SS (ie, H0: a = 0), and M3 was adopted to evaluate the association between SS and depression while adjusting for the direct effect of PsyCap (ie, H0: b = 0). As for the results of these models, we identified that: 1) depression was negatively affected by PsyCap (c = −0.398, p < 0.001), 2) SS was positively affected by PsyCap (a = 0.372, p < 0.001), and 3) depression was simultaneously negatively influenced by PsyCap (c′ = −0.334, p < 0.001) and SS (b = −0.171, p < 0.001). On the grounds of these findings, we conclude that SS plays an important mediating role in the path from PsyCap to depression, with a mediating effect of −0.064 (= −0.372 × 0.171), accounting for approximately 16.0% (= 0.064/0.398) of the total effect of PsyCap on depression.
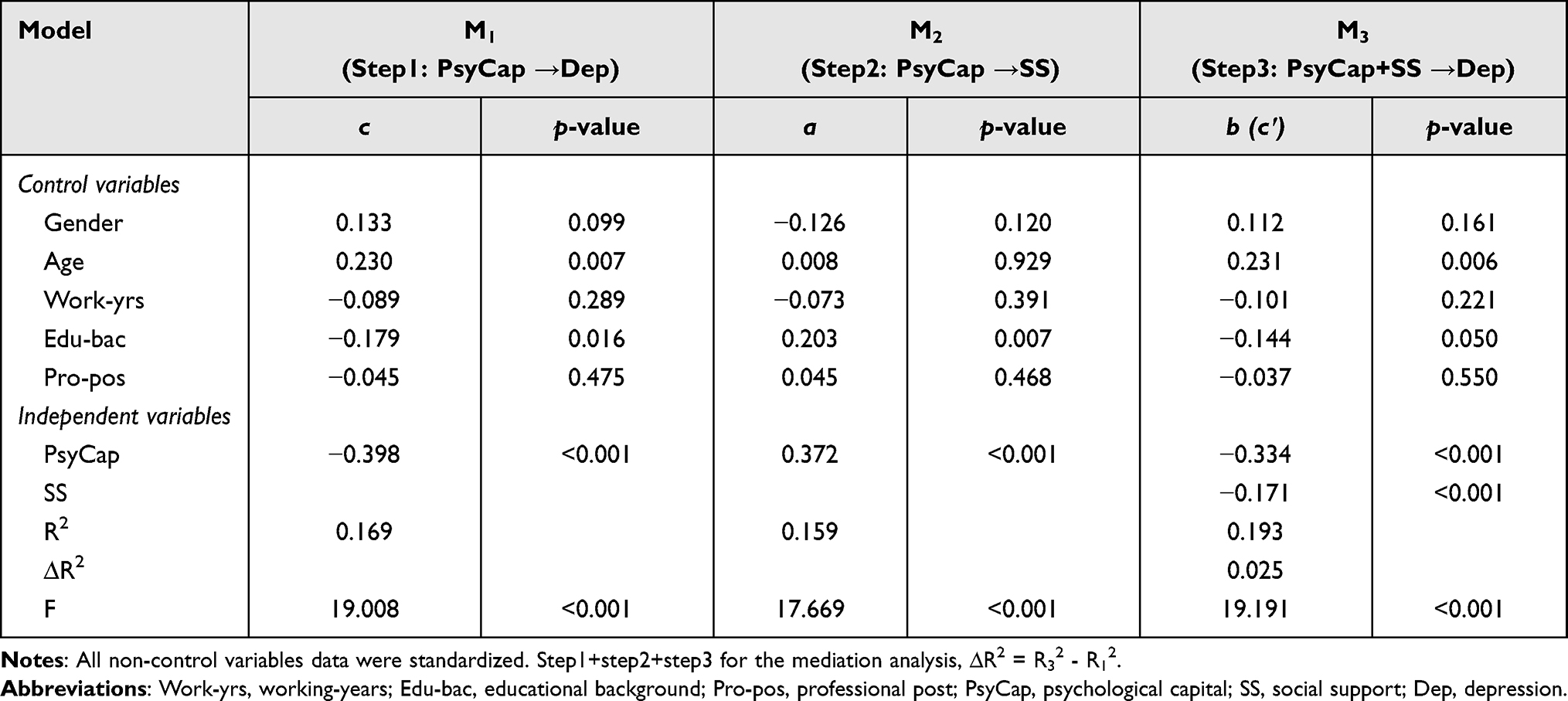 |
Table 5 Multiple Regression Analysis of PsyCap and SS on Depression |
Moreover, controlling for demographic variables, we further explored the relationship between PsyCap, SS, and depression in each of the four factors of PsyCap (Table 6). In the mediation analysis, we found that: 1) depression was negatively influenced by hope (c = −0.205, p = 0.002), resiliency (c = −0.209, p =0.001), and optimism (c = −0.141, p = 0.006) and positively affected by self-efficacy (c = 0.123, p = 0.018); 2) SS was only positively influenced by optimism (a = 0.266, p < 0.001); 3) depression was jointly influenced by hope, self-efficacy, resiliency, and SS, but not optimism. Therefore, we conclude that optimism has a direct negative effect on depression and further has an indirect effect on depression via the complete mediating role of SS (b = −0.181), contributing to a mediating effect of −0.048 (= −0.181 × 0.266) in all the EPs.
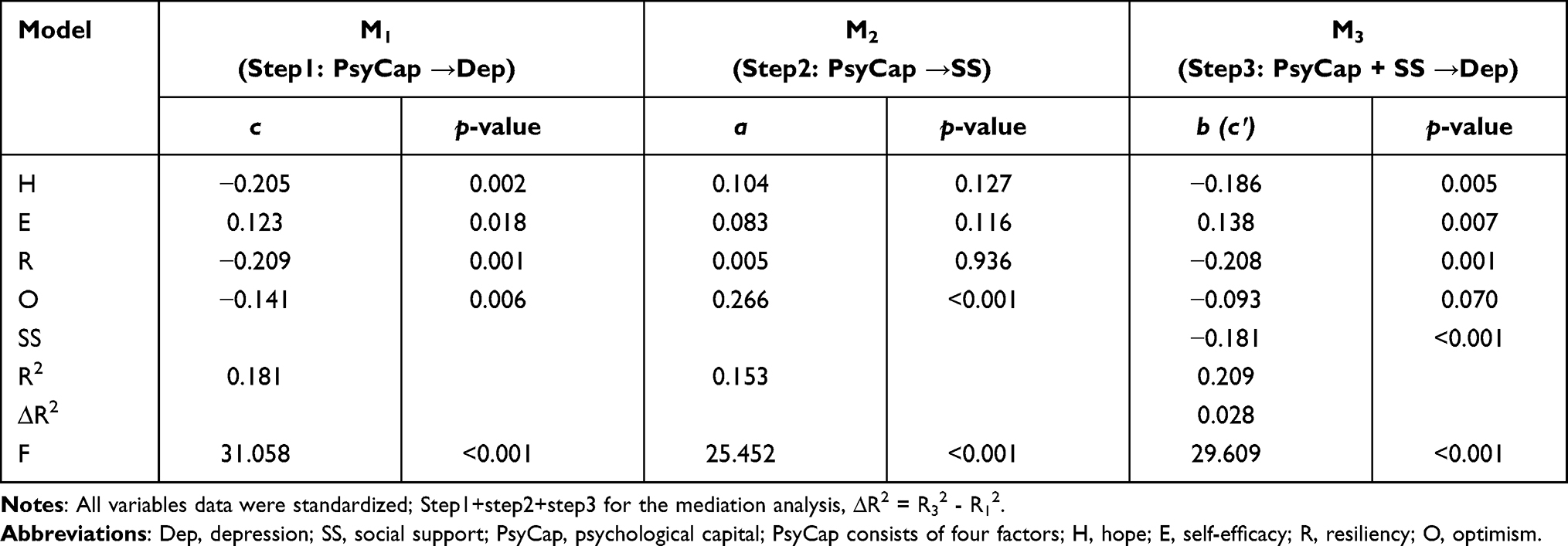 |
Table 6 Multiple Regression Analysis of PsyCap Factors and Social Support on Depression |
Furthermore, we implemented the same analytical procedures as above with a special group of 105 EPs who were evaluated for potential depressive disorder because they had an average depression score of greater than 2 (Table 6). For comparison, we also performed the same analyses for the remaining 463 EPs with an average depression score of less than 2 (Table 7). Herein, we identified some discrepancy in the results: 1) depression was negatively affected by resiliency and optimism, and positively affected by self-efficacy; nevertheless, compared with all EPs, the effect was stronger for EPs with potential depressive disorder (c = −0.444 vs −0.209, −0.267 vs −0.141, 0.233 vs 0.123, respectively); 2) in the subgroup of EPs without potential depressive disorder, depression was only negatively influenced by hope, whereas the effect was weaker than that obtained with all the EPs (c = −0.130 vs −0.205).
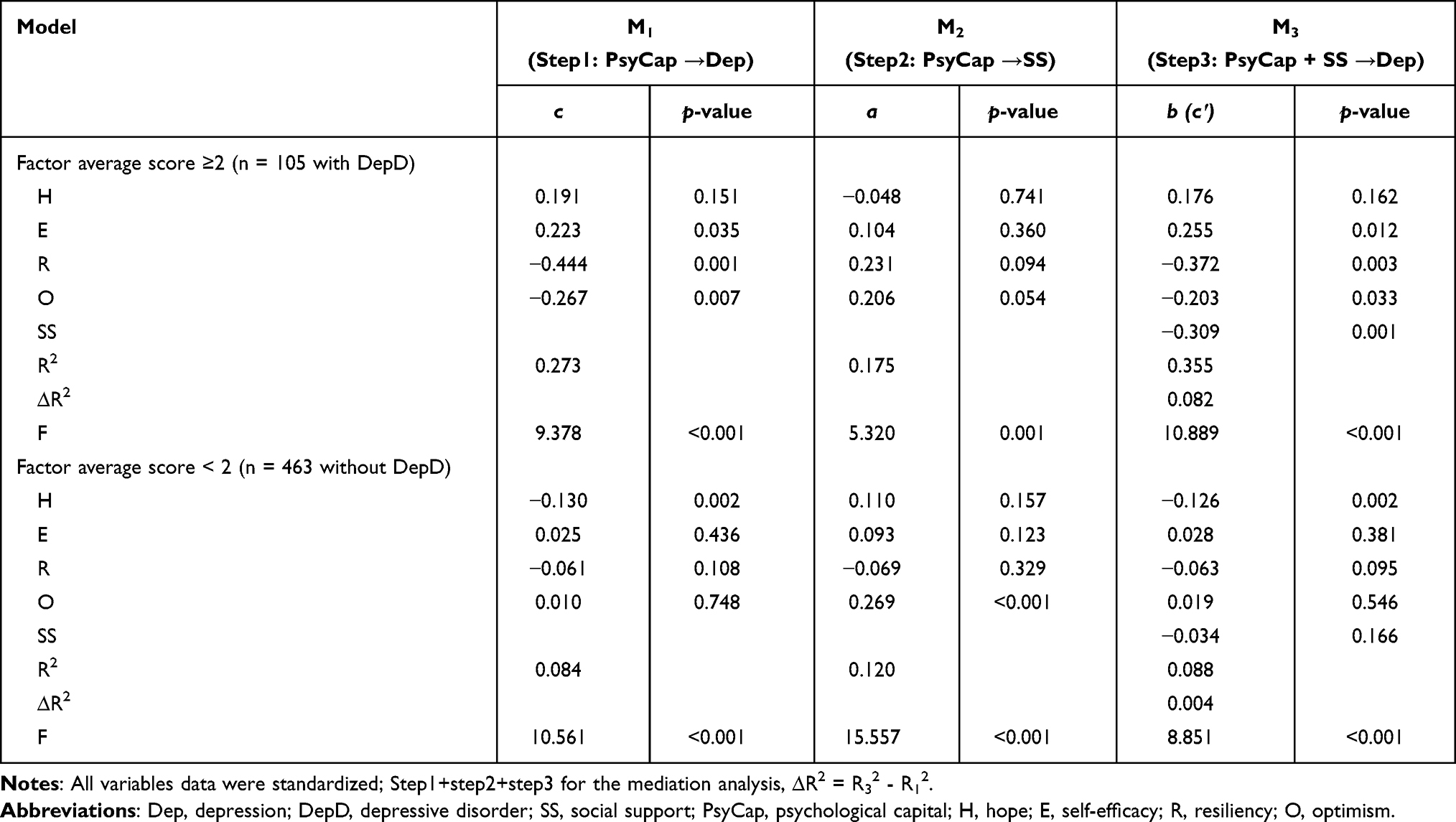 |
Table 7 Multiple Regression Analysis for Emergency Physicians with DepD and without DepD |
Discussion
To explore the relationship between PsyCap, SS, and depression in medical practitioners, our team conducted a survey investigating the status quo of depression among EPs. We identified that the average score of depression among EPs was generally higher compared with the results observed in prior studies by Jin, Wu, and Zhang;49 Tang et al;50 Chen and Li;51 Tong;41 and Liu et al,52 with respect to the application of SCL-90 in other Chinese populations, which may be a consequence of the diversity in occupations. A 24-hour shift responsibility system is routinely implemented in the emergency department of all the hospitals involved, and the EPs should always be fully prepared for emergency incidents to prompt medical response and care that spans a full 24 hours, which frequently subjects the EPs to patients or families who display negative emotions or behaviors, including those who are drunk, ornery, aggressive, or even violent. Therefore, the vast majority of EPs are in a state of high stress and overload for prolonged shift durations and often experience great psychological pressure every day, which is especially typical in the tertiary grade-A general hospitals in China.53 Importantly, Chinese society is collectivist. When EPs have problems, for the sake of group harmony, they tend to blame the problems on themselves and choose to fight against the pressure alone. Furthermore, the restriction of their working environment and monotony of their working procedures can predispose the EPs to deprivation in regard to social activity, lack of desire to engage in activities, and decline of interest in life, ultimately leading to disappointment, pessimism, despair, and depression as well as other possible negative emotions.
Moreover, our study estimated that approximately 18.5% of EPs suffer from potential depressive disorder, essentially consistent with previous findings (12.1–19.3%) in regard to physicians in the general population in the U.S.6 but different from the results of 28.8% of physicians in the earlier studies on resident physicians,7 indicating that the depression prevalence in EPs in tertiary grade-A general hospitals in Jiangsu is comparable to that found in their foreign counterparts, and that the depression status of residents in emergency departments is lower (better) than that in foreign countries, which could be attributable to the diverse levels of local economic development in those studies.
The depression scores differed in terms of EPs’ working-years, with significantly higher scores for those with 11–20 working-years. More than 10 years of working time caused doctors to reach the stage of physical and psychological fatigue, and 10 years is also a significant time span in Chinese culture. China’s professional title promotion system stipulates that physicians can submit applications every 5 years. After 10 years of service, doctors can seek promotion to the position of deputy chief physician, which requires difficult-to-attain scientific research and clinical experience. Thus, hospital authorities should pay more attention to these first-line physicians and provide more organizational support as well as humane care. For those EPs with several influencing factors of depressive disorder in particular, some corresponding intervention measures should be taken to prevent the tragedy of individual suicide. No significant difference in depression was observed in terms of gender, age, educational background, and professional post among EPs. This may be attributed to the nature of EPs’ work, since they all share an identical working environment and high workload and encounter a combination of complicated conditions while treating emergency patients each day. However, the detection rate of depression in female EPs was approximately 7.4% higher than that found in males, and those with lower education had higher depression scores, which also constitutes an important issue that hospital management must address.
The present study identified that PsyCap had a significant negative effect on depression and a positive effect on SS among participants, and that SS partially mediated and enhanced the effect of depression alleviated by PsyCap. As an internal positive psychological resource, this research found that PsyCap can effectively alleviate depressive symptoms, consistent with previous research.23,26 In addition, PsyCap can further combat depression by increasing social support. Physicians with higher levels of PsyCap are likely to be better able to cope with problems in work and life, and to perceive and take advantage of emotional or material support from leaders, colleagues, and family members. This indicates that the relevant departments of hospitals can develop and nurture physicians’ psychological capital effectively by means of group counseling and skill development.
In addition, our study showed that self-efficacy had a significant positive influence on depression in all participating EPs. This result is inconsistent with previous studies that explored the same association in surgery trainees and diabetics.54,55 We infer that the divergence in results may relate to the differences in hospital management in different countries. Chinese emergency physicians need a high level of self-efficacy to deal with various complex situations quickly every day, which will increase stress, thereby leading to depressive symptoms. Optimism can further influence depression by enhancing the overall mediating role of SS. These findings imply that EPs themselves can ease depressive symptoms via self-care that can reduce burnout risk,56 and by seeking support from others to boost their optimism when coping with problems.
Furthermore, we revealed the discriminating effect of PsyCap factors on depression among the two subgroups of EPs. Depression was negatively affected by resiliency and optimism in the EPs with depressive disorder. In facing work-family conflicts, EPs who have potential depressive disorder may lack understanding and support from their family.57 When they suffer stress, the EPs only rely on their own resiliency and optimism to relieve the stress. EPs without depressive disorder feel full of hope about their work and life because they can get support from family and colleagues. The EPs should strengthen communication with family in their daily life to relieve pressure, but two cultural norms pose a challenge in this regard. In the Chinese cultural background, high expectations from family and colleagues represent more responsibility. Traditionally in China, it is widely believed that doctors have a high-paying profession, which leads to high economic expectations from physicians’ family members. In addition, the physician in the family is often the first person they turn to when a family member becomes sick. At present, the majority of the population does not hold mental health-related knowledge, which has sometimes led physicians to have difficulty communicating with their families about mental health challenges they are experiencing, which further increases the pressure experienced by the physicians and the need for family support, leading to the emergence of depressive symptoms. We infer that EPs with low SS intend to cope with depression by themselves rather than seeking professional help. If it is not well handled, these EPs will likely develop depressive disorder. Hospital management should provide professional service for these EPs, such as regular psychological evaluations, appropriate group activities, and individual conversations between the supervisor and the physician to understand the physician’s current emotional state.
In conclusion, this study has demonstrated that PsyCap negatively affects EPs’ depressive symptoms, and social support mediates the relationship between PsyCap and depressive symptoms. Here, the prior condition allows us to unveil different states that cause individuals to act differently—a more dynamic conception of how third variables operate.58
Limitations and Prospects
This study also has some shortcomings, which provide directions for further research. First, despite our illustration of the association between PsyCap, SS, and depression, the time causality between these factors cannot be robustly determined and established due to the cross-sectional observational nature of our study. Second, the de facto association between SS and depression may be much more complex and complicated than the models that we fitted.37 For example, our study may be subject to power loss if the relationship between PsyCap, SS, and depression is nonlinear rather than linear as we assumed in our analysis. Due to the COVID-19 outbreak, many doctors in China went to the front lines to provide medical assistance in early 2020. Studies have shown that the health care workers who responded to the pandemic had lower levels of depression,59 and an extension of this study needs to take the pandemic into account. There is a reciprocal influence between individuals’ mental health and social relationships, and research has indicated that mental health can affect individuals’ social relationships.60 Future research could build upon this idea, which is not explored in the current study. In addition, we did not measure the severity of depression and specific family factors of the study subjects that related to depression, and we will fill in this gap in future studies. Third, the sample size for the sub-dataset of EPs with depressive disorder was not sufficiently large (n = 105), which could undermine our estimation (eg, greater standard error) in regard to mediating factors for depression. Thus, our results for EPs with depressive disorder need to be interpreted with caution, and larger sample sizes are required for solid inferences in the future. Fourth, our study only included EPs from tertiary grade-A general hospitals in Jiangsu Province—one of the most developed provinces at political, economic, and cultural levels, with a population of ~80.7 million and the second-largest GDP in China. Thus, further studies are required to authenticate whether our conclusion can be generalized to other medical practitioners in other grades of hospitals or in other Chinese provinces with profiles that differ from Jiangsu Province (see Figure 1).
Conclusion
The results show that the detection rate of depression among emergency physicians is high in China. Psychological capital not only alleviates depressive symptoms directly, but also negatively affects depression by increasing the social support of emergency physicians, the study found. The emergency physician, the family, and the hospital need to work together to ensure the mental health of the physician. Hospitals can conduct effective trainings on psychological capital development, and doctors themselves need to pay attention to the use of their own social support.
Data Sharing Statement
The original dataset used in this study is available from the corresponding author on request.
Acknowledgments
The authors would like to share appreciation for all the investigators, participants, and general hospitals involved and referenced in this study.
Funding
This research was funded by the Social Science Foundation of Jiangsu project (Project number 18GLD010) and the Collegiate Philosophy and Social Science Foundation of Jiangsu project (Project number 2018SJA0956), and was also associated with the Jiangsu Province National College Students Innovation and Entrepreneurship Program (Project number 201710313030).
Disclosure
The authors report no conflicts of interest in this work.
References
1. WHO. Licence: CC BY-NC-SA 3.0 IGO. Geneva: WHO; 2017.
2. Charlson FJ, Baxter AJ, Cheng HG, Shidhaye R, Whiteford HA. The burden of mental, neurological, and substance use disorders in China and India: a systematic analysis of community representative epidemiological studies. Lancet. 2016;388:376–389. doi:10.1016/S0140-6736(16)30590-6
3. Center C, Davis M, Detre T, et al. Confronting depression and suicide in physicians - a consensus statement. JAMA. 2003;289:3161–3166. doi:10.1001/jama.289.23.3161
4. Bailey E, Robinson J, McGorry P. Depression and suicide among medical practitioners in Australia. Intern Med J. 2018;48:254–258. doi:10.1111/imj.13717
5. Yates SW. Physician stress and burnout. Am J Med. 2020;133:160–164. doi:10.1016/j.amjmed.2019.08.034
6. Stehman CR, Testo Z, Gershaw RS, Kellogg AR. Burnout, drop out, suicide: physician loss in emergency medicine, part I. West J Emerg Med. 2019;20:485–494. doi:10.5811/westjem.2019.4.40970
7. Mata DA, Ramos MA, Bansal N, et al. Prevalence of depression and depressive symptoms among resident physicians: a systematic review and meta-analysis. JAMA. 2015;314:2373–2383. doi:10.1001/jama.2015.15845
8. Williford ML, Scarlet S, Meyers MO, et al. Multiple-institution comparison of resident and faculty perceptions of burnout and depression during surgical training. JAMA Surg. 2018;153:705–711. doi:10.1001/jamasurg.2018.0974
9. Gao Y-Q, Pan B-C, Sun W, Wu H, Wang J-N, Wang L. Depressive symptoms among Chinese nurses: prevalence and the associated factors. J Adv Nurs. 2012;68:1166–1175. doi:10.1111/j.1365-2648.2011.05832.x
10. Shen LL, Lao LM, Jiang SF, et al. A survey of anxiety and depression symptoms among primary-care physicians in China. Int J Psychiatry Med. 2012;44(3):257–270. doi:10.2190/PM.44.3.f
11. Chen Y, Shen X, Feng J, et al. Prevalence and predictors of depression among emergency physicians: a national cross-sectional study. BMC Psychiatry. 2022;22(1):69. doi:10.1186/s12888-022-03687-8
12. Hart D, Paetow G, Zarzar R. Does implementation of a corporate wellness initiative improve burnout? West J Emerg Med. 2019;20:138–144. doi:10.5811/westjem.2018.10.39677
13. Kuhn CM, Flanagan EM. Self-care as a professional imperative: physician burnout, depression, and suicide. Can J Anesth. 2017;64:158–168. doi:10.1007/s12630-016-0781-0
14. Gao L, Xiao X, Che G, et al. Sudden death of physicians in China: a red alert. Popul Health Manag. 2019;22(3):191–192. doi:10.1089/pop.2018.0090
15. Boutou A, Pitsiou G, Sourla E, Kioumis I. Burnout syndrome among emergency medicine physicians: an update on its prevalence and risk factors. Eur Rev Med Pharmaco. 2019;23:9058–9065.
16. Bragard I, Dupuis G, Fleet R. Quality of work life, burnout, and stress in emergency department physicians: a qualitative review. Eur J Emerg Med. 2015;22:227–234. doi:10.1097/MEJ.0000000000000194
17. Zhao D, Zhang Z. Changes in public trust in physicians: empirical evidence from China. Front Med. 2019;13(4):504–510. doi:10.1007/s11684-018-0666-4
18. Si Y. When to end the continuing violence against physicians in China. J Public Health. 2021;43(1):e129–e130. doi:10.1093/pubmed/fdaa116
19. Yang F, Yang BX, Stone TE, et al. Stigma towards depression in a community-based sample in China. Compr Psychiatry. 2020;97:152152. doi:10.1016/j.comppsych.2019.152152
20. Wang Y, Liu L, Xu H. Alarm bells ring: suicide among Chinese physicians: a STROBE compliant study. Medicine. 2017;96(32):e7790. doi:10.1097/MD.0000000000007790
21. Dyrbye LN, West CP, Sinsky CA, Goeders LE, Satele DV, Shanafelt TD. Medical licensure questions and physician reluctance to seek care for mental health conditions. Mayo Clin Proc. 2017;92:1486–1493. doi:10.1016/j.mayocp.2017.06.020
22. Luthans F, Youssef C, Avolio B. Psychological Capital. Oxford University Press; 2007.
23. Shen X, Yang YL, Wang Y, Liu L, Wang S, Wang L. The association between occupational stress and depressive symptoms and the mediating role of psychological capital among Chinese university teachers: a cross-sectional study. Bmc Psychiatry. 2014;1:14, 329.
24. Bakker DJ, Lyons ST, Conlon PD. An exploration of the relationship between psychological capital and depression among first-year doctor of veterinary medicine students. J Vet Med Educ. 2017;44:50–62. doi:10.3138/jvme.0116-006R
25. Erdur B, Ergin A, Turkcuer I, Parlak I, Ergin N, Boz B. A study of depression and anxiety among doctors working in emergency units in Denizli, Turkey. Emerg Med J. 2006;23:759–763. doi:10.1136/emj.2006.035071
26. Liao ML, Fang F, Liu GX, Zhang YX, Deng CQ, Zhang XQ. Influencing factors and correlation of anxiety, psychological stress sources, and psychological capital among women pregnant with a second child in Guangdong and Shandong Province. J Affect Disord. 2020;264:115–122. doi:10.1016/j.jad.2019.11.148
27. Ditzen B, Heinrichs M. Psychobiology of social support: the social dimension of stress buffering. Restor Neurol Neurosci. 2014;32:149–162. doi:10.3233/RNN-139008
28. Cobb S. Presidential address-1976. Social support as a moderator of life stress. Psychosom Med. 1976;38:300–314. doi:10.1097/00006842-197609000-00003
29. Cameron JE, Voth J, Jaglal SB, Guilcher SJT, Hawker G, Salbach NM. “In this together”: social identification predicts health outcomes (via self-efficacy) in a chronic disease self-management program. Soc Sci Med. 2018;208:172–179. doi:10.1016/j.socscimed.2018.03.007
30. Finck C, Barradas S, Zenger M, Hinz A. Quality of life in breast cancer patients: associations with optimism and social support. Int J Clin Health Psychol. 2018;18:27–34. doi:10.1016/j.ijchp.2017.11.002
31. Wu M, Yao WQ, Wang L, et al. The mediating role of psychological capital in the relationship between social support and anxiety symptoms among people living with HIV/AIDS. Chron Pathematol J. 2013;14:489–491. In Chinese.
32. Shang Z, Liang Q, Song S, Li M, Zhao W, Liu X. Analysis of social support status of emergency doctors with different working years. Continuing Med Educ. 2019;33:5–6. In Chinese.
33. Melissa J, Garner B, McGregor A, Karly M, Murphy A, Albano D. Optimism and depression: a new look at social support as a mediator among women at risk for breast cancer. Psycho Oncol. 2015;24:1708–1713. doi:10.1002/pon.3782
34. Trunzo J, Pinto J, Bernardine M. Social support as a mediator of optimism and distress in breast cancer survivors. J Consult Clin Psych. 2003;71:805–811. doi:10.1037/0022-006X.71.4.805
35. Zhang H, Zhao Q, Cao P, Ren G. Resilience and quality of life: exploring the mediator role of social support in patients with breast cancer. Med Sci Monit. 2017;23:5969–5979. doi:10.12659/MSM.907730
36. Rao D, Chen WT, Pearson CR, et al. Social support mediates the relationship between HIV stigma and depression/quality of life among people living with HIV in Beijing, China. Int J STD AIDS. 2012;23:481–484. doi:10.1258/ijsa.2009.009428
37. Ren P, Qin X, Zhang Y, Zhang R. Is social support a cause or consequence of depression? A longitudinal study of adolescents. Front Psychol. 2018;9:1634. doi:10.3389/fpsyg.2018.01634
38. Schmitz N, Hartkamp N, Kiuse J, Franke GH, Reister G, Tress W. The symptom check-list-90-R (SCL-90-R): a German validation study. Qual Life Res. 2000;9:185–193. doi:10.1023/A:1008931926181
39. Bonicatto S, Dew MA, Soria JJ, Seghezzo ME. Validity and reliability of symptom checklist ‘90 (SCL90) in an Argentine population sample. Soc Psych Psych Epid. 1997;32:332–338. doi:10.1007/BF00805438
40. Tong H. A research of twenty years’ vicissitude: SCL-90 and its norm. Psychol Sci. 2010;33:
41. Xiao S. Theoretical basis and research application of social support rating scale. J Clin Psych Med. 1994;04:98–100. in Chinese.
42. Deng W, Li X, Chen B, Luo K, Zeng X. Analysis on application of common methods bias test to psychological studies during recent five years in China. J Jiangxi Normal Univ. 2018;42:447–453. In Chinese.
43. O’brien RM. A caution regarding rules of thumb for variance inflation factors. Qual Quant. 2007;41:673–690. doi:10.1007/s11135-006-9018-6
44. Mackinnon DP. Introduction to statistical mediation analysis. Introd Probab Stat Eng Sci. 2008;36:1–8.
45. VanderWeele T. Explanation in Causal inference: Methods for Mediation and Interaction. New York, NY: Oxford University Press; 2015.
46. Imai K, Keele L, Tingley D. A general approach to causal mediation analysis. Psychol Methods. 2010;15:309. doi:10.1037/a0020761
47. Hicks R, Tingley D. Causal mediation analysis. Stata J. 2011;11:605–609. doi:10.1177/1536867X1201100407
48. Dai JY, Stanford JL, LeBlanc M. A multiple-testing procedure for high-dimensional mediation hypotheses. J Am Stat Assoc. 2020;1–39. doi:10.1080/01621459.2020.1811100
49. Jin H, Wu W, Zhang M. Preliminary analysis of SCL-90 assessment results of Chinese normal people. Chin J Nervous Ment Dis. 1986;12:260–263. In Chinese.
50. Tang Q, Cheng Z, Yuan A, Deng Y. The use and reanalysis of SCL-90 in China. Chin J Clin Psychol. 1999;07:19–23. In Chinese.
51. Chen S, Li L. Re-testing reliability, validity and norm applicability of SCL-90. Chin J Nervous Ment Dis. 2003;29:323–327. In Chinese.
52. Liu Y, Wu S, Li Y, Shao F, Su J, Liu X. A survey of mental symptoms of Chinese population based on SCL-90. Chin Ment Health J. 2018;32:437–441. In Chinese.
53. Liu Q, Xie X-L, Liu R, Chen E-Z, Yang Z. Shift scheduling method for physicians in emergency department with time-varying demand. Industr Eng Manag. 2015;20:122–129. In Chinese.
54. Janko Matthew R, Smeds Matthew R. Burnout, depression, perceived stress, and self-efficacy in vascular surgery trainees. J Vasc Surg. 2019;69:1233–1242. doi:10.1016/j.jvs.2018.07.034
55. Cassidy D, Karuthan C. Depression, distress and self-efficacy: the impact on diabetes self-care practices. PLoS One. 2017;12:1–16.
56. Hotchkiss JT. Mindful self-care and secondary traumatic stress mediate a relationship between compassion satisfaction and burnout risk among hospice care professionals. Am J Hosp Palliat Care. 2018;35(8):1099–1108. doi:10.1177/1049909118756657
57. Wang Y, Liu L, Wang J, et al. Work‐family conflict and burnout among Chinese doctors: the mediating role of psychological capital. J Occup Health. 2012;54:232–240. doi:10.1539/joh.11-0243-OA
58. Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. J Pers Soc Psychol. 1986;51:1173–1182. doi:10.1037/0022-3514.51.6.1173
59. Liu Y, Chen H, Zhang N, et al. Anxiety and depression symptoms of medical staff under COVID-19 epidemic in China. J Affect Disord. 2021;278:144–148. doi:10.1016/j.jad.2020.09.004
60. Lamblin M, Murawski C, Whittle S, et al. Social connectedness, mental health and the adolescent brain. Neurosci Biobehav Rev. 2017;80:57–68. doi:10.1016/j.neubiorev.2017.05.010
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.