Back to Journals » Patient Preference and Adherence » Volume 19
The Mediating Effects of Self-Acceptance and Self-Evaluation on Mindfulness and Benefit -Finding in a Sample of Chinese Systemic Lupus Erythematous Patients
Authors Xu F, Tong X, Niu Y, Lin Q, Yao A ![]() , Yang F, Li L
, Yang F, Li L
Received 4 April 2025
Accepted for publication 4 July 2025
Published 21 July 2025 Volume 2025:19 Pages 2129—2146
DOI https://doi.org/10.2147/PPA.S529674
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Fei Xu,1,* Xu Tong,2,* Yanping Niu,3 Qin Lin,3 Anling Yao,1 Feng Yang,4 Ling Li3
1School of Nursing, Zhejiang Chinese Medical University, Hangzhou, Zhejiang, People’s Republic of China; 2School of Nursing, Bozhou College, Bozhou, Anhui, People’s Republic of China; 3School of Nursing, Zhejiang Shuren University, Hangzhou, Zhejiang, People’s Republic of China; 4Tongxiang First People’s Hospital, Tongxiang, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ling Li, School of Nursing, Zhejiang Shuren University, Hangzhou, People’s Republic of China, Email [email protected]
Purpose: This study investigated the relationship between mindfulness, self-acceptance and benefit-finding in SLE patients. Through structural equation models, we examined the mediating role of self-acceptance and self-evaluation between mindfulness and benefit-finding.
Patients and Methods: We used a convenient sampling method to investigate the demographics characteristics, mindfulness, self-acceptance, and benefit-finding of 319 SLE patients who were admitted to the rheumatology and immunology departments of tertiary, and Grade-A hospitals from December 2019 to December 2020.
Results: Educational Levels, age, presence of other diseases besides SLE, medical expense payment method can affect mindfulness, and benefit-finding in SLE patients (p< 0.05), monthly salary can also influence mindfulness (p< 0.05), marital status also have impact on benefit-finding (p< 0.05). Educational Levels, age and monthly salary can affect the self-acceptance of SLE patients (p< 0.05). Mindfulness is positively correlated with the benefit-finding and has a significant positive impact on it (r=0.379, p< 0.01). Mindfulness is positively correlated with self-acceptance, and self-evaluation (r = 0.124 and 0.130, p < 0.05), which are positively correlated with the benefit-finding (r = 0.256 and 0.255, p < 0.05) in turn. Self-acceptance, and self-evaluation played a partially mediating role in the relationship between mindfulness, and the benefit-finding in SLE patients, with the mediating effect accounting for 7.95% (The path coefficient was 0.0391, p < 0.01), and 7.74% of the total effect (The path coefficient was 0.0384, p < 0.01), respectively.
Conclusion: Mindfulness, self-acceptance, and benefit-finding in SLE patients are influenced by various sociodemographic factors. Self-acceptance and self-evaluation can mediate the relationship between mindfulness and benefit-finding in SLE patients. Clinical caregivers should pay more attention to improving patients’ levels of mindfulness and their self-acceptance of the disease, and guide patients in cognitive reappraisal, so that they can benefit from the struggle with the disease.
Keywords: systemic lupus erythematosus, SLE, mindfulness, self-acceptance, benefit-finding, mediation role
Introduction
Systemic lupus erythematosus (SLE) is a chronic autoimmune inflammatory connective tissue disease, which can affect joints, kidneys, skin, mucous membranes, and blood vessel walls. Common symptoms include fatigue, fever, arthralgia, myalgia, weight loss, rash, oral ulcers, thrombocytopenia, and leukopenia.1,2 The severity of SLE varies between mild and severe. Women experience significantly worse outcomes in lupus symptoms, cognition, and fertility, and experience worse functioning in the domains of physical function and pain-vitality.3 Currently, the treatment of SLE mainly includes general treatment, and drug therapy, with the latter being widely used. Long-term drug use brings economic, mental, and physiological burdens due to side effects, and both disease progression and drug therapy impact patients’ emotions negatively. Approximately 54.5% of SLE patients suffer from depression, while 61.5% suffer from anxiety, with the severity of these conditions positively correlated with disease activity, which greatly affect their quality of life.4 Interactions between depression, anxiety, and SLE can lead to an increased incidence of suicidal ideation, poor treatment adherence, and increased dysfunction.5,6 SLE is regarded as a stress-related disease, with stress conditions often worsening symptoms.7 Some studies suggest that depressive symptoms, and health-related quality of life (HRQoL) in patients with rheumatic diseases can be improved by antidepressants and psychotherapy. Therefore, targeted interventions should be carried out for depressive symptoms in patients with SLE.8
Over the past 20 years, positive psychology has advocated for a positive attitude towards disease, and researchers have begun to consider the positive benefits of trauma, such as improvements in quality of life, post-traumatic growth, social support, and well-being.9 This is especially relevant for long-term, chronic, and recurrent diseases like SLE. The involvement of multiple organs in SLE patients has a profound impact on their health-related quality of life and mental health.10,11 In particular, disease activity, severity of fatigue, psychological morbidity, and body image in SLE are correlated with quality of life (QoL).12 Positive psychology encompasses mindfulness, self-acceptance, resilience, benefit-finding, and post-traumatic growth, etc. The Monitoring and Acceptance Theory predicts that removing acceptance skills training from mindfulness interventions (acceptance is an emotion regulation skill) will weaken its protective effect against stress-related diseases.13 Mindfulness training has also been proven to be beneficial to patients with multiple sclerosis by encouraging self-acceptance of the presence of emotions such as worry.14 It can also benefit patients with inflammatory bowel disease by fostering disease acceptance and self-compassion.15 However, no such studies have been conducted on SLE patients.
Theoretical Analysis and Model Hypothesis
According to the “Mindful Coping Model”, individuals first undergo primary and secondary evaluations when faced with stressor stimuli. They then use mindfulness to redirect attention, achieving positive reappraisal, which increases positive emotions and reduces stress.16 As a positive coping style, and emotion regulation strategy, self-acceptance includes self-evaluation, and the resulting self-experience and attitude,17 which encompass both psychological and physical attributes. For example, individuals who have a positive self-evaluation of their bodies possess an accurate self-awareness.18,19 Individuals with higher levels of self-acceptance are more likely to adopt positive coping styles.20 Therefore, it can be speculated that self-acceptance, and self-evaluation (two dimensions of the SAQ) may help patients reduce stress and negative emotions, and facilitate benefit-finding in SLE patients according to the Mindful Coping Model, but the specific mechanism is not very clear.
Relationship Between Mindfulness, and Benefit-Finding
Mindfulness is a psychological state that involves focusing one’s attention on the present moment and accepting the thoughts and feelings that arise, rather than immediately reacting to or judging them.21 Benefit-finding refers to the positive changes in self-perception that result from highly stressful experiences, usually achieved through cognitive reappraisal. This change can reduce the inherent threats associated with negative events, allowing individuals to recover or alter their views of themselves, others, and the world.22 Mindfulness, and benefit-finding are interconnected. Evidence shows that mindfulness training can alleviate the burden of stress-related illnesses.23 Mindfulness-based interventions (MBIs) can enhance accurate symptom assessment, reduce symptoms of chronic diseases, and improve disease management, and health outcomes.24 One study found that through the practice of yoga, practitioners can influence their personal resources such as mindfulness or self-compassion, thereby gaining benefits.25
Relationship Between Mindfulness, and Self-Acceptance
Self-acceptance reflects the degree to which individuals accept themselves, embracing all their characteristics, both good and bad, with a positive attitude.26 It encompasses two dimensions: self-acceptance (SAQ-SA), and self-evaluation (SAQ-SE), forming the foundation of self-esteem. Both self-evaluation and self-acceptance are dominated and restricted by the ideal self. However, self-evaluation cannot be completely equated with self-acceptance. For example, a person with low self-evaluation can still be self-accepting, while a person with high self-evaluation can also be self-unaccepting. When self-acceptance is lacking, a sense of inferiority will emerge psychologically, leading to feelings of low self-esteem.27 Studies have shown that mindfulness is highly correlated with self-acceptance. Mindfulness practice is associated with increased awareness, and self-acceptance.28,29 It involves being aware of emotional experiences with an attitude of acceptance, and non-judgment.30 Several studies have identified cognitive reappraisal as a mediator between mindfulness and depression, with a positive correlation of 0.294 between mindfulness and reappraisal.31 Mindfulness promotes positive reappraisal through cognitive transformation, facilitating a shift of attention from negative to positive emotional stimuli, which is central to positive reappraisal.7
Relationship Between Self-Acceptance, and Benefit-Finding
Studies have found a positive correlation between self-acceptance, and positive coping styles.32 Research on breast cancer patients has shown that positive coping through cognitive-behavioral stress intervention can reduce depressive symptoms and enhance perceived benefits.33 This suggests that a patient’s self-acceptance is correlated with benefit-finding. Benefit-finding is described as a positive reappraisal process,34 where individuals experience greater benefits when they mobilize their potential coping, and problem-solving abilities, enhance self-confidence, and improve self-efficacy to produce positive change.35
The Mediating Role of SAQ-SA, and SAQ-SE
Self-acceptance plays a mediating role between mindfulness, and subjective well-being in college students.36,37 A study of empty-nest elderly in rural areas found that self-acceptance partially mediates the relationship between self-worth, and subjective well-being.38 Additionally, self-acceptance has been shown to partially mediate the relationship between mindfulness, and peace of mind.39 Cognitive reappraisal can influence self-evaluation, and Shi’s study suggests that this strategy can mediate the relationship between personality traits, and mental experience.40
Numerous studies have found correlations between these factors.28,41 The positive psychological effects of mindfulness have been confirmed by a wide range of studies. Mindfulness meditation,42 mindfulness-based stress reduction,17 and mindfulness-based cognitive therapy have been widely used in treating SLE.43 However, research on self-acceptance, and benefit-finding in SLE patients is limited. Only one study found that complex complications, CD4+/CD8+ levels, coping style, depression, social support, and poor sleep quality were associated with post-traumatic growth in adult SLE patients.44 After reviewing the theoretical, and empirical literature, the research question of this study is: What are the influencing factors of mindfulness, self-acceptance, and benefit-finding in SLE patients, and do SAQ-SA, and SAQ-SE mediate the relationship between mindfulness and benefit-finding? We propose the following research hypotheses:
H1: Mindfulness is associated with benefit-finding in SLE patients. H2: Mindfulness is associated with SAQ-SA in SLE patients. H3: Mindfulness is associated with SAQ-SE in SLE patients. H4: SAQ-SA is associated with benefit-finding in SLE patients. H5: SAQ-SE is associated with benefit-finding in SLE patients. H6: SAQ-SA mediates the relationship between mindfulness, and benefit-finding. H7: SAQ-SE mediates the relationship between mindfulness, and benefit-finding.
Figure 1 shows the hypothetical model.
 |
Figure 1 Hypothetical model. |
Participants and Methods
Research Participants
This study employs a cross-sectional research design, with the research team conducting a questionnaire survey in a tertiary hospital in Hangzhou. Data collection was carried out from December 2019 to December 2020. According to Structural Equation Modeling (SEM) guidelines, the minimum sample size should be 10 times the estimated number of paths in the model.45 Thus, the minimum sample size for this study was determined to be 160 cases. Considering a 10% rate of attrition, the appropriate sample size for this study was set at 180. A total of 352 SLE patients from five tertiary A-grade hospitals were selected using convenience sampling principles between December 2019 and December 2020. Inclusion criteria were as follows: patients had to meet the classification, and diagnostic criteria for SLE revised by the American College of Rheumatology (ACR) in 1997, have a disease duration between 0.5 and 5 years, possess normal cognitive function, and adequate language comprehension, be aged 18 years or older, and be able to provide informed consent. Exclusion criteria included patients with serious complications such as heart, brain, and kidney issues, inability to read or write in Chinese, and inability to complete assessments due to vision impairment, among others (Table 1).
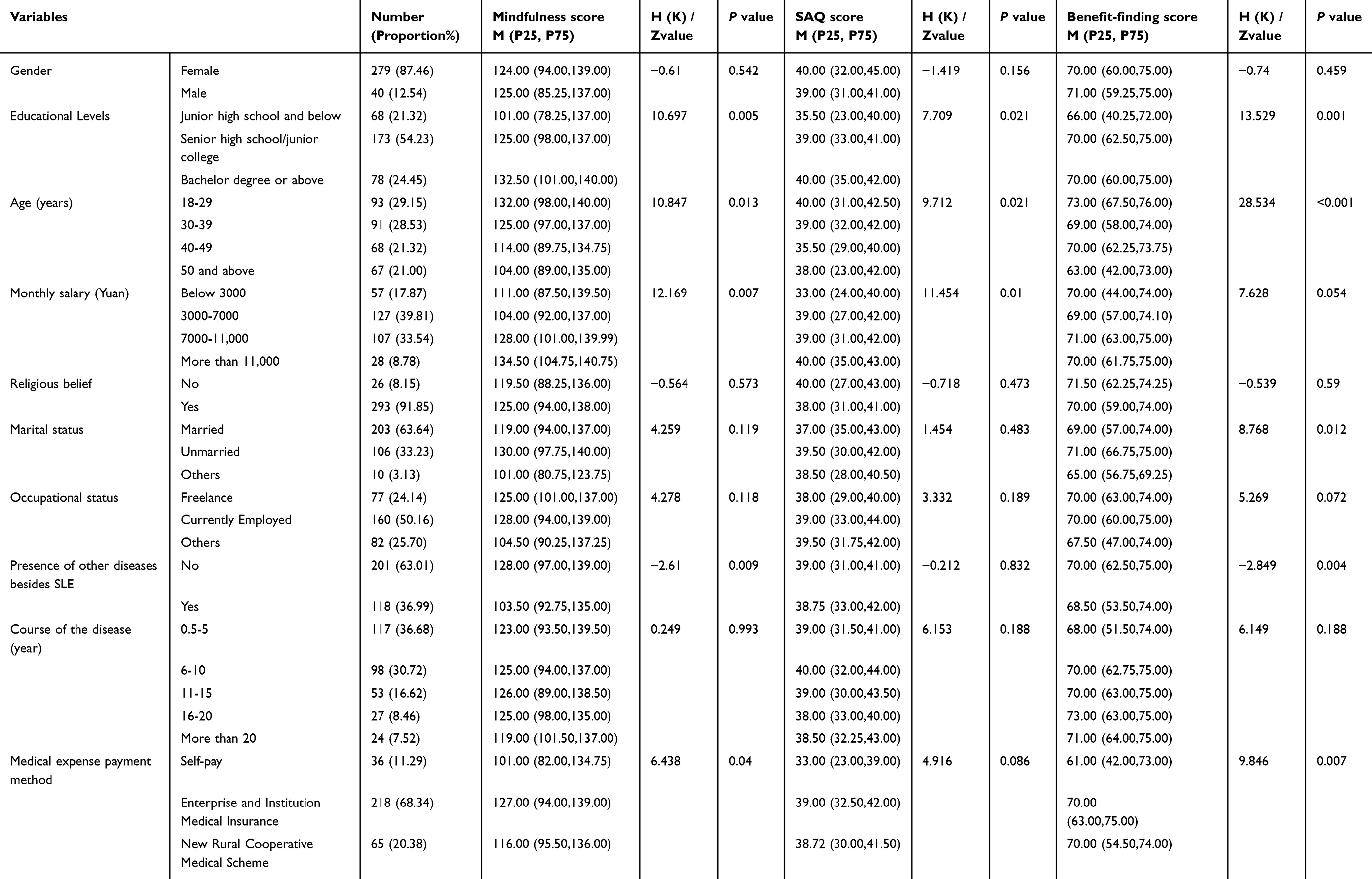 |
Table 1 Subgroup Analysis of Sociodemographic Factors on Mindfulness, SAQ, and Benefit-Finding (n=319) |
This study was approved by the Ethics Review Committee of the Institutional Review Board of the Institutional Review Board (IRB) of Zhejiang Shu Ren University (NO:20200105). Participation was voluntary, anonymity was guaranteed. Informed consent was provided by all participants prior to participating in the survey.
Data Collection
Initially, the research team underwent training for data collection between December 2019, and December 2020. The primary researcher conducted surveys at one hospital, while the research team, assisted by fellow nurses, distributed questionnaires at other hospitals. A total of 352 questionnaires were personally distributed at hospital outpatient clinics or wards. Unified guidelines were employed to explain the research objectives and important principles to the participants, emphasizing the anonymity, and confidentiality of data collection and usage. It took approximately 15 to 20 minutes to complete the questionnaire. All questionnaires were filled out independently by the patients, and collected after completeness checks by the research team members. Since each questionnaire was checked for completeness of completion by the research team members, there were no missing values in the questionnaire responses. After excluding 33 invalid questionnaires that exhibited the same response or adherence to specific patterns, 319 valid questionnaires were obtained, resulting in an effective rate of 90.63%. To ensure data accuracy, two individuals independently entered the data while a third checked for discrepancies. Additionally, an associate professor with extensive statistical experience was invited to oversee data processing, ensuring the accuracy, and rigor of statistical analysis.
Measurements
General Information Questionnaire
We developed a demographic questionnaire to assess the characteristics of the participants. Considering the impact of general demographic factors such as gender and age on the disease, as well as the influence of monthly salary, occupational status, medical expense payment method, and educational levels on the economic situation of chronic diseases and the awareness of disease knowledge, presence of other diseases besides SLE, course of the disease on the damage of chronic diseases, and the marital status and religious beliefs in the social and spiritual support for patients, covering gender, educational levels, age, monthly salary, religious beliefs, marital status, occupational status, presence of other diseases besides SLE, course of the disease, and medical expense payment method.
Five-Facet Mindfulness Questionnaire (FFMQ)
This scale, originally developed by Baer et al46 underwent Chinese revision by Deng et al47 in 2011 and was utilized in this study. It encompasses 5 dimensions: describing, observing, non-reactivity, non-judgment, and acting with awareness. The Likert 5-level scoring method was employed, ranging from “not consistent at all” to “fully consistent with”, measured on a 1–5 scale. The scale comprises 39 questions, including 20 positively scored items, and 19 reverse-scored items. Total scores were found to be positively correlated with levels of mindfulness. In the original validation study, the scale demonstrated high internal consistency with a Cronbach’s α of 0.917. In this study, the Cronbach’s α coefficient was 0.914 Supplementary materials.
The Self-Acceptance Questionnaire (SAQ)
The Self-Acceptance Questionnaire, developed by Cong Zhong, and Gao Wenfeng,27 encompasses two dimensions: self-evaluation (SAQ-SE), and self-acceptance (SAQ-SA) Supplementary materials. The scale comprises 16 items, with each dimension containing 8 items. A Likert 4-level scoring method was utilized, where responses ranging from “very identical” to “very opposite” were scored as 4, 3, 2, and 1 point, respectively. The cumulative score of the 8 items for SAQ-SE, and SAQ-SA respectively represented the scores for each factor, while the total scale score was the sum of these two factors, ranging from 16 to 64. A higher total score indicates a higher level of self-acceptance among subjects. The scale demonstrated good reliability and validity. The internal consistency coefficients for SAQ-SA, and SAQ-SE were 0.9344, and 0.9124, respectively. The scale also exhibited satisfactory retest reliability with a coefficient of 0.7653. In this study, the Cronbach’s alpha coefficient was 0.702.
The Benefit-Finding Scale for Adults (BFS-A)
This scale, adapted by Weaver et al,48 comprises 6 dimensions, and 22 items, covering acceptance, personal growth, social relations, family relations, health behaviors, and worldview. Each item is rated on a 5-point scale, ranging from 1 (not at all) to 5 (very much). The total score, ranging from 22 to 110, is calculated as the sum of all items, with higher scores indicating greater Benefit-finding (BF) status. Its Chinese version, translated by Liu,49 demonstrated high reliability with a Cronbach’s coefficient alpha of 0.95. In this study, the Cronbach’s alpha coefficient was 0.856 Supplementary materials.
Data Analysis
We conducted statistical analysis using SPSS 25.0 software. Initially, data were assessed for normal distribution or not. Normally distributed measurement data were described using the mean (x¯), and standard deviation (s), while frequency or component ratios were used for count data. For non-normally distributed data, statistical description was provided using the median, and interquartile range. The Mann–Whitney U-test, and Kruskal–Wallis H-test were employed to analyze the related factors of socio-demographic characteristics with mindfulness, self-acceptance, and benefit-finding. Spearman correlation analysis was then utilized to examine the correlations between mindfulness, SAQ, and benefit-finding. When the residuals of the test variables did not adhere to a normal distribution, Box-Cox transformation was applied to the data. Additionally, Harman’s single factor test was conducted to mitigate common methodological biases. Prior to testing for mediation effects, the measurement model underwent confirmatory factor analysis. Using AMOS 24.0, we constructed a Structural Equation Model to explore the mediating effect of SAQ-SA, and SAQ-SE between mindfulness, and benefit-finding. The bias-corrected bootstrap method was employed to assess the significance of mediating effects, while obtaining robust standard errors, and confidence intervals for parameter estimation. Statistically significant results were determined if the confidence interval did not include zero.50
Results
Subgroup Analysis of Socio-Demographic Factors on Mindfulness, SAQ, and Benefit-Finding
The majority of subjects were female (279, 87.46%), with a predominant educational level of high school/technical secondary school (173, 54.23%). The distribution of patients across different age groups was similar, with slightly more than 127 individuals (39.81%) earning a monthly salary of 3000–7000 yuan. The majority of patients reported having a religious belief (293, 91.85%), while a relatively high proportion were married (203, 63.64%). Most subjects were currently employed (160, 50.16%), and a minority reported having other diseases besides SLE (63.01%). Approximately 117 patients (36.68%) had a disease duration ranging from 0.5 to 5 years, and 218 patients (68.34%) utilized enterprise and institution medical insurance as their payment method. Significant differences in mindfulness among SLE patients were observed based on educational levels, age, monthly salary, presence of other diseases besides SLE, and medical expense payment method (P < 0.05). Similarly, educational levels, age, and monthly salary exhibited significant differences in the Self-Acceptance Questionnaire (SAQ) among SLE patients (P < 0.05). Notably, significant differences in benefit-finding were observed among SLE patients based on educational levels, age, marital status, presence of other diseases besides SLE, and medical expense payment method (P < 0.05). Subgroup analysis of sociodemographic factors on mindfulness, SAQ, and benefit-finding is presented in Table 1.
Correlation Between Mindfulness, SAQ, and Benefit-Finding
Mindfulness, and the self-acceptance (SAQ) demonstrated a significant positive correlation (r = 0.120, P < 0.05). Specifically, all dimensions of mindfulness were positively related to SAQ-SA (r = 0.067–0.149). Notably, the differences in describing, and non-reactivity were statistically significant (P < 0.05). Additionally, these dimensions showed positive correlations with SAQ-SE (r = 0.097–0.142), with observing, describing, and non-reactivity exhibiting significant differences (P < 0.05). Benefit-finding was significantly, and positively associated with SAQ (r = 0.301, P < 0.01). SAQ-SA was positively correlated with all dimensions of benefit-finding (r = 0.075–0.304). Similarly, SAQ-SE demonstrated positive correlations with all dimensions of benefit-finding (r = 0.136–0.262, P < 0.05). Furthermore, mindfulness exhibited a significant positive association with benefit-finding (r = 0.383, P < 0.01). Each dimension of mindfulness was positively correlated with each dimension of benefit-finding (r = 0.126–0.403, P < 0.05). For detailed information, please refer to Table 2.
 |
Table 2 Correlation Analysis of Mindfulness, SAQ, and Benefit-Finding in SLE Patients |
Testing for Mediation Effect of SAQ-SA and SAQ-SE
Common Method Deviation Test
To mitigate potential common methodological biases inherent in self-reported data,51 we conducted the Harman single factor test prior to data analysis. Exploratory factor analysis was performed on the questions pertaining to mindfulness, self-acceptance, and benefit-finding. Results revealed that after rotation, the eigenvalues of 12 factors exceeded 1, with the explanatory rate of the first common factor being 23.647%. This value significantly falls below the critical threshold of 40%. Consequently, there is no notable indication of significant common methodological bias in this study.52
Measurement Model Check
Before conducting the mediation effect test, the measurement model underwent confirmatory factor analysis. This study incorporated three potential variables: mindfulness (comprising observing, describing, acting with awareness, non-judgment, and non-reactivity), self-acceptance (SAQ) including SAQ-SA, and SAQ-SE, and benefit-finding (encompassing acceptance, family relations, worldview, personal growth, social relations, and health behaviors). The results of the confirmatory factor analysis indicated a good fit for the model, with χ²(62) = 141.912, CFI (Comparative Fit Index) = 0.966, TLI (Tucker-Lewis Index) = 0.957, SRMR (Standardized Root Mean Square Residual) = 0.037, RMSEA (Root Mean Square Error of Approximation) = 0.064. Moreover, the 90% confidence intervals for RMSEA fell within the range [0.532, 0.750], suggesting satisfactory model fit. Additionally, Table 3 revealed that the standardized load of each index was significant for the corresponding factors (P < 0.001). Furthermore, the Average Variance Extracted (AVE) value exceeded 0.50, and the Composite Reliability (CR) value exceeded 0.70, indicating good data aggregation validity.
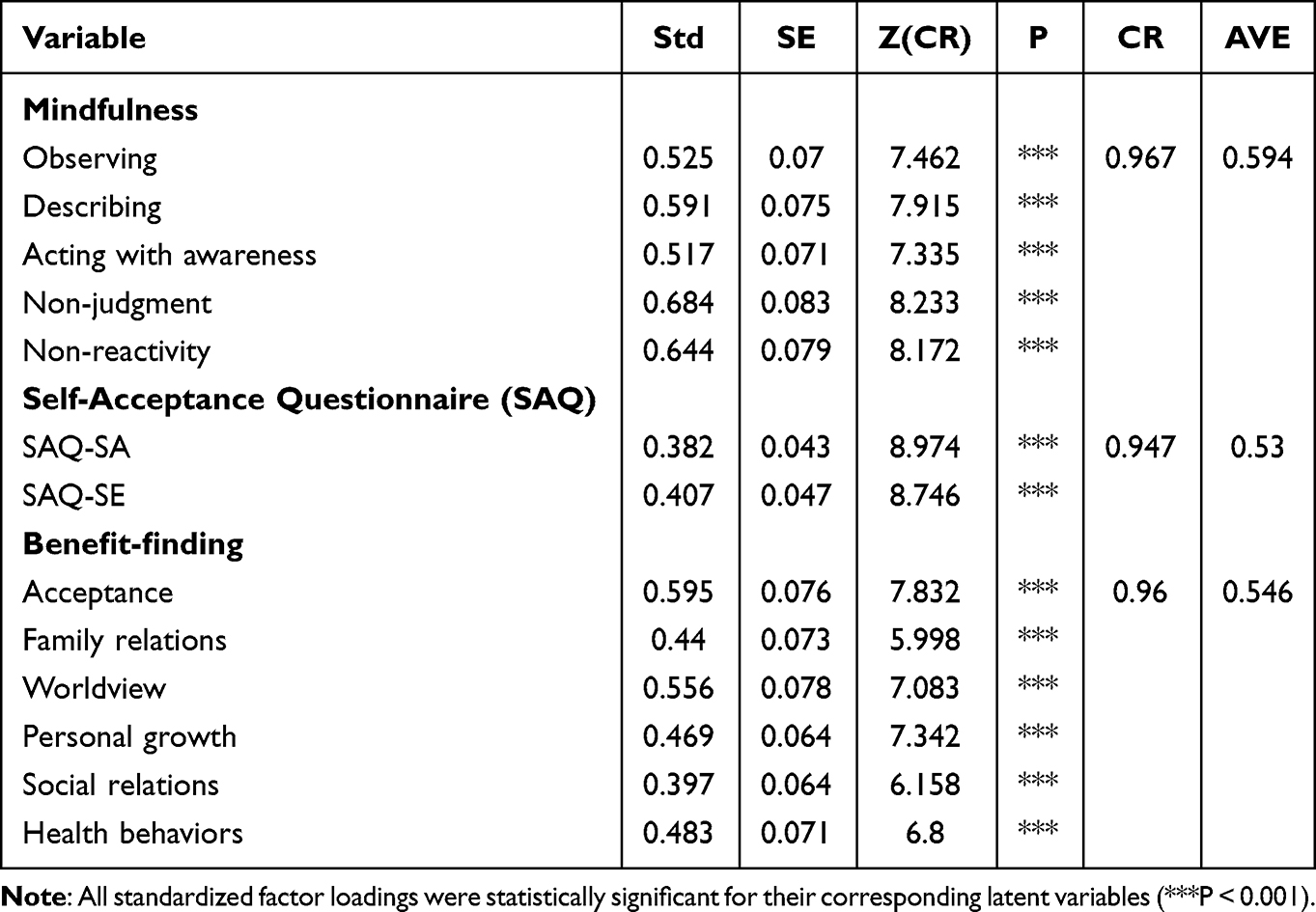 |
Table 3 Factor Loading Coefficient Table |
Mediating Effect Test
After controlling for gender, educational levels, age, monthly salary, religious belief, marital status, occupational status, presence of other diseases besides SLE, course of the disease, and medical expense payment method in the Structural Equation Model (SEM), the parameters were estimated using the variance maximum likelihood method, and bootstrap testing was employed to examine the mediating effect. A SEM model was constructed with mindfulness (comprising five latent variables: observing, describing, acting with awareness, non-judgment, and non-reactivity) as the independent variable, benefit-finding (comprising six latent variables: acceptance, family relations, worldview, personal growth, social relations, and health behaviors) as the dependent variable, and self-acceptance (comprising two latent variables: SQA-SA, and SQA-SE) as the mediating variable. The final model is illustrated in Figure 2, with all fitting indexes meeting statistical requirements, indicating good model fit (Table 4). Parameter values obtained from the final model fitting and the average values of parameters obtained during the bootstrap process are presented in Table 5 and Table 6. Hypotheses H1-H7 were confirmed as follows: (1) Mindfulness directly, and positively predicts benefit-finding, with a standardized estimate of the path coefficient at 0.414 (t = 7.043, P < 0.01). (2) SAQ-SA is a direct positive predictor of benefit-finding, with a standardized estimate of the path coefficient at 0.233 (t = 4.119, P < 0.01), and SQA-SE also directly predicts benefit-finding positively, with a standardized estimate of the path coefficient at 0.162 (t = 2.833, P < 0.01). (3) Mindfulness is a direct positive predictor of SAQ-SA, with a standardized path coefficient of 0.170 (t = 2.918, P < 0.01), and mindfulness also directly predicts SAQ-SE positively, with a standardized path coefficient of 0.238 (t = 4.118, P < 0.01). (4) Mindfulness influences benefit-finding through SAQ-SA, and SAQ-SE, with standardized estimation of the indirect influence path coefficient at 0.0391, and 0.0384, respectively. The mediation effect accounts for 7.95%, and 7.74% of the total effect, respectively. The partial mediating effect of SAQ-SA is slightly stronger than that of SAQ-SE, as detailed in Table 6.
 |
Table 4 Structural Equation Model Fitting Index (n = 319) |
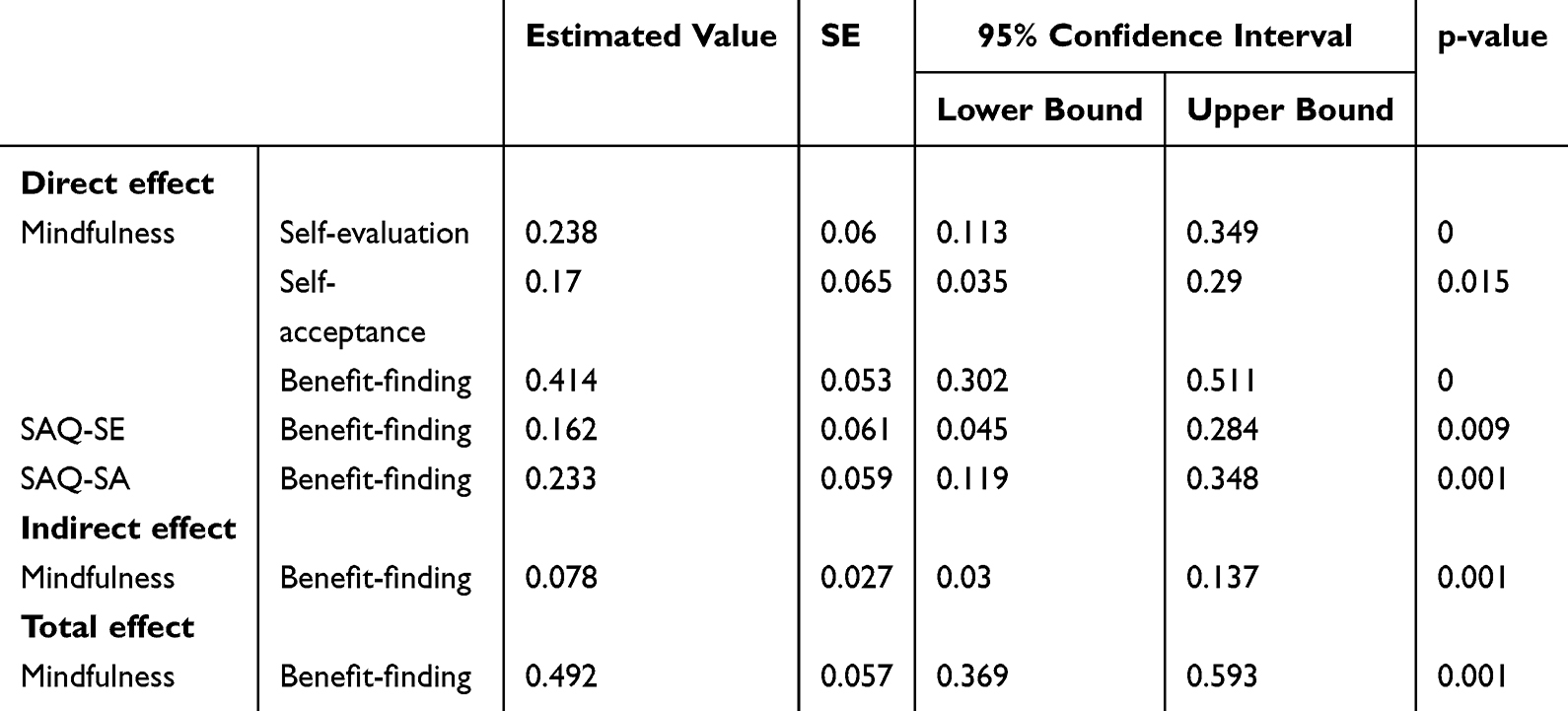 |
Table 5 Coefficient Decomposition of Mindfulness, SAQ-SA, SAQ-SE, and Benefit-Finding Effect Model in SLE Patients (n=319) |
 |
Table 6 Path Coefficient Estimates, Standard Errors, 95% Confidence Intervals, and Effect Proportions for Each Path |
 |
Figure 2 Model of the mediating effect of SAQ-SA, SAQ-SE on mindfulness, and the benefit-finding of SLE patients. |
Discussion
This study aims to investigate the factors influencing mindfulness, self-acceptance, and benefit-finding in SLE patients at tertiary hospitals in East China. Additionally, it seeks to construct a mediating model involving SAQ-SA, and SAQ-SE between mindfulness, and benefit-finding in SLE patients.
Subgroup Analysis of Socio-Demographic Factors on Mindfulness, SAQ, and Benefit-Finding
Significant differences were observed in the mindfulness among SLE patients with varying educational levels, ages, monthly salaries, presence of other diseases besides SLE, and medical expense payment method in this study. Patients with higher educational levels exhibited greater cognition of SLE, a more comprehensive understanding of the disease, and a higher level of mindfulness, echoing findings from Camilleri’s study.53 Contrary to previous research indicating a positive correlation between age, and mindfulness,54 our study found higher mindfulness levels among younger patients. This finding may be attributed to the physical decline experienced by elderly patients, and the chronic suffering associated with SLE, which may make older individuals more susceptible to sub-syndromes of depression compared to other age groups.55 Regarding the presence of other diseases besides SLE, patients with multiple co-morbidities exhibited lower mindfulness compared to those without additional ailments. The co-occurrence of hypertension, diabetes, coronary heart disease, and other underlying conditions can lead to significant physiological strain, and exacerbate negative emotions.56 The complexity of managing multiple diseases, including adhering to various medication regimens, may also contribute to decreased mindfulness among SLE patients. Furthermore, our study revealed that SLE patients with higher monthly salaries, and enterprise and institution medical insurance demonstrated relatively higher mindfulness, consistent with findings by Bränström.57 Patients with better financial means often have access to superior medical insurance coverage, reducing financial stress during treatment. This financial stability enables them to afford non-insurance medications, explore alternative treatment modalities, and dedicate adequate time, and energy towards coping with, overcoming, and self-managing their condition, thus exhibiting higher mindfulness.
Educational levels, age, and monthly salaries were identified as influential factors on the SAQ among SLE patients in this study. SLE patients with higher educational levels exhibited elevated SAQ, consistent with findings by Xia.58 Research indicates that individuals with lower educational attainment may struggle to comprehend treatment plans, fail to seek timely assistance, and exhibit reduced treatment adherence.59 Consequently, their disease prognosis worsens, contributing to negative emotions, and diminished self-acceptance. Elderly patients tended to report lower SAQ, echoing findings from Xia’s study.58 Specifically, SLE patients aged 40–49 years demonstrated the lowest SAQ in our study. Patients in this age bracket often shoulder substantial responsibilities in both their careers, and families, frequent hospital visits disrupt their professional, and familial roles. Additionally, the physiological changes associated with aging, coupled with prolonged, and high-dose steroid therapy, can lead to physical manifestations like moon face, alopecia, and buffalo hump, causing significant psychological distress.60 These factors collectively contribute to diminished self-evaluation, and self-acceptance. Furthermore, higher monthly incomes were associated with elevated SAQ, aligning with Zhu’s findings that students from affluent backgrounds,61 and supportive family environments exhibit better self-acceptance, and mental well-being. Conversely, patients with lower incomes bear a heavier financial burden due to disease treatment, leading to feelings of inferiority, and an inability to achieve normal levels of self-acceptance.
Significant discrepancies in benefit-finding were observed among SLE patients with varying educational levels, ages, marital statuses, presence of other diseases besides SLE, and medical expense payment method in this study. Undergraduate patients exhibited higher benefit-finding compared to other groups, aligning with Liu’s findings.62 Patients with higher educational levels typically possess greater treatment-seeking abilities, a deeper understanding of disease-related information, and stronger self-management skills, leading to heightened benefit-finding experiences. Younger patients also reported higher benefit-finding, consistent with Heusler’s study.63 This could be attributed to the greater receptivity of younger patients, and their ability to perceive the positive aspects of their situation, thereby experiencing more benefits. Conversely, elder patients, burdened by physiological decline, disease severity, and economic constraints, may experience feelings of guilt, and diminished confidence in recovery during treatment,64 resulting in relatively fewer perceived benefits. Surprisingly, unmarried patients exhibited higher benefit-finding compared to their married counterparts, contrary to the expectation that married patients would benefit more due to family support. However, Saxena et al reported that the overall QoL scores of unmarried individuals were higher than those of married individuals.65 Moreover, a study reported that marital status can affect mental health status, with married individuals having higher levels of anxiety than unmarried individuals.66 In this study, it is considered as unmarried patients, typically younger, and more receptive to new information, may possess stronger self-management abilities without the familial, and childcare responsibilities that married patients face, contributing to their heightened benefit-finding experiences. A higher sense of mastery, or the perceived control over what happens in one’s personal life, is associated with better physical and mental health in other chronic diseases.67 Some studies have also suggested a positive correlation between patients’ benefit-finding, and family functioning,68 but marital status may not influence benefit-finding if patients receive adequate family, and social support. Patients with comorbidities reported lower benefit-finding compared to those without comorbidities, likely due to the increased disease severity, multiple treatments, and recurrent episodes associated with comorbid conditions.69,70 Comorbidities amplify physical, psychological, and economic burdens, making it more challenging for patients to fulfill their social roles, and thereby diminishing their perceived benefits. Patients covered by enterprise and institution medical insurance or enrolled in the New Rural Cooperative Medical Scheme exhibited higher benefit-finding than those with self-paid medical expenses, consistent with Lin’s research.71 Self-pay medical expenses impose significant financial strain on patients, and their families, hindering their ability to derive benefit from their experiences.
Correlation Between Mindfulness, SAQ, and Benefit-Finding
This study has unveiled a positive relationship between mindfulness, and benefit-finding in SLE patients. Those with heightened mindfulness exhibit a more positive self-perception, possess superior self-regulation, and emotional coping mechanisms to navigate adversity, and trauma, and demonstrate stronger adaptability, and interpersonal skills, leading to an enhanced quality of life, and overall well-being.72,73 Mindfulness interventions could improve symptoms of depression, anxiety, perceived stress, and quality of life, with lasting effects extending up to six months.74 Moreover, this study uncovered a positive correlation between mindfulness, and self-acceptance in SLE patients, aligning with findings indicating that individuals with higher levels of trait mindfulness tend to harbor higher core self-evaluations, and are more inclined to accept themselves non-critically.75 Mindfulness training operates by mitigating self-critical attitudes, nurturing non-judgmental present-centered awareness, and fostering self-acceptance, and self-compassion.76
Furthermore, the observation, description, and non-reactivity dimensions of mindfulness were found to be positively associated with self-acceptance. The existence of a positive correlation between mindfulness, and self-evaluation (SAQ-SE) in SLE patients was confirmed in this study. The Mindful Coping Model posits that mindful individuals tend to centralize their stress assessments, perceive experiences with broader attention, and engage in flexible cognition, thereby enhancing cognitive reappraisal.77 Consequently, individuals with heightened mindfulness are better equipped to adopt positive coping strategies, such as self-acceptance, and self-evaluation (including cognitive reappraisal), attentional switching (distraction), or attentional expansion, to regulate emotions, and buffer stress. Research has indicated that the core processes of mindfulness (description, and non-reactivity to experiences) are particularly pertinent to acceptance, and reappraisal as emotional regulation strategies, yielding positive outcomes.78 Hence, it is recommended that clinical practitioners focus on patients’ capacity to observe, describe, and react non-reactively in future mindfulness training sessions to enhance patients’ self-acceptance, facilitate cognitive restructuring, alleviate negative emotions, alleviate clinical symptoms, and promote mental well-being.
In this study, self-acceptance (SAQ-SA) exhibited a positive correlation with benefit-finding, and its various dimensions. Ou et al found that patients who received Acceptance and Commitment Therapy (ACT) were better able to perceive benefits, detach themselves from problems, observe, learn, and overcome difficulties.79 It can also help cancer patients accept negative changes related to their illness, and encourage them to recognize the benefits brought by their condition, thereby improving their quality of life.80 Moreover, self-evaluation (SAQ-SE) was positively associated with benefit-finding in this study. Individuals often engage in cognitive reappraisal when confronted with stressful events during illness, a process that not only generates negative emotions but also explores the positive significance of the disease.81 Positive reappraisal represents a coping mechanism, and adaptive process that reframes stressful events as benign, valuable, or beneficial.16
The Mediating Role of Self-Acceptance, and Self-Evaluation Between Mindfulness, and Benefit-Finding in SLE Patients
The findings of this study underscore the role of SAQ-SA among SLE patients, revealing its partial mediating effect in the relationship between mindfulness, and benefit-finding, with the mediation effect accounting for 7.95% of the total effect. This aligns with prior research indicating self-acceptance mediate mindfulness, and subjective well-being among college students. It was found that there is a positive correlation between perceived benefits, and subjective well-being.82 Consequently, SAQ-SA emerges as a pivotal mechanism through which mindfulness can enhance the benefit-finding of SLE patients, with higher levels of mindfulness correlating with improved SAQ-SA, and greater benefit-finding, ultimately leading to better health outcomes, and reduced levels of perceived stress.83
Furthermore, this study revealed that self-evaluation (SAQ-SE) among SLE patients also plays a partial mediating role between mindfulness, and benefit-finding, accounting for 7.74% of the total effect. This mirrors findings from research on chronic pelvic pain, which demonstrated that mindfulness interventions can enhance cognitive processes such as positive cognitive reappraisal, and strengthen emotion regulation skills to mitigate stress, and mental-emotional dysfunction.84 Patients with elevated mindfulness can not only directly experience positive effects on their perception of illness benefits but can also indirectly enhance such perceptions by bolstering their SAQ-SA, and SAQ-SE. Thus, clinical practitioners are encouraged to monitor patients’ physical, and mental states, enhance their mindfulness levels, mitigate negative emotions through positive cognitive restructuring, bolster self-acceptance, implement cognitive reappraisal techniques, and thereby ameliorate the psychosomatic symptoms experienced by SLE patients.
Implications
Theoretical contributions of this study include: (1) Exploring the enhancing effects of mindfulness, and self-acceptance on the benefit-finding of patients through the lens of the Mindfulness Coping Model and delving into its mechanism in depth. (2) Establishing a theoretical framework of SAQ-SA, and SAQ-SE mediating benefit-finding, providing novel insights for a comprehensive analysis of the pathways shaping benefit-finding. Practical implications derived from the study are as follows: (1) Identification of key influencing factors, and target populations for interventions aimed at enhancing mindfulness, self-acceptance, and benefit-finding among SLE patients. (2) Highlighting the significant predictive power of mindfulness on individual benefit-finding, suggesting that appropriate mindfulness interventions can foster a positive outlook on living with the disease, and encourage patients to actively engage in treatment. (3) Recognition of the mediating effects of SAQ-SA, and SAQ-SE underscores the importance of nursing care workers in addressing SLE patients’ coping strategies, focusing on fostering self-acceptance, and reappraisal of adverse stress to alleviate mood disturbances, reduce stress levels, and enhance overall quality of life. Based on the study’s findings, it is found that improving mindfulness is an important means to improve the benefit-finding of SLE patients. Nursing workers can try to apply several mindfulness-based psychotherapy methods to SLE patients, such as Cognitive-Behavioral Therapy (CBT), Mindfulness-based stress reduction (MBSR), and ACT, etc. The benefit-finding of SLE patients can be improved by the following methods: (1) Cognitive therapy, such as group cognitive behavior theory,85 mindfulness-based stress reduction (MBSR).86 (2) Problem-solving or skill training. problem-solving therap,87 coping skills training.88 (3) Narrative therapy: writing, and expression therapy,89 Mandala painting.90 (4)Exercise therapy: muscle relaxation,91 yoga.92 (5) Other therapies: peer support,93 Internet information support,94 resourcefulness intervention,95 etc. Current studies have shown that the methods to improve self-acceptance are limited, and one study found that improving mindfulness can affect their views of themselves, and others.96 Storytelling may be a way to improve self-acceptance.97 Yoga therapy may increase the acceptance of depression.98 Self-acctance has a self-adaptive function, which can be expressed through the constant reduction of the tendency to stress, thus ensuring inner balance, and peace,99 which is an important method to improve the patients’ mental health. Further research should focus on finding effective ways to improve SLE patient’s self-acceptance.
Conclusion
This study explored the influencing factors of mindfulness, self-acceptance, and benefit-finding among systemic lupus erythematosus (SLE) patients treated in a tertiary hospital in eastern China, including education levels, age, presence of other diseases besides SLE, medical expense payment method, monthly salary, and marital status. Additionally, this study confirmed the partial mediating effects of the SAQ-SA and SAQ-SE between mindfulness and benefit-finding, validating the Mindfulness Coping Model. Health professionals should enhance health education and psychological support for patients, highlighting their potential and cultivating mindfulness. Moreover, interventions should focus on improving patients’ self-acceptance and cognitive reappraisal, ultimately enhancing their ability to find benefits in their disease experience. The findings of this study are enlightening for nursing professionals caring for SLE patients and other chronic disease patients. Future research directions could focus on improving the empirical effects of SAQ-SA and SAQ-SE between mindfulness and benefit-finding in SLE patients.
Study Limitations
There are several limitations of this study that need to be acknowledged. First, the use of convenience sampling may limit the representativeness of the sample and introduce potential sampling bias, thereby affecting the generalizability of the study results. Additionally, the cross-sectional design of this study limits the ability to determine causal relationships between variables. Second, the study was conducted only in five tertiary hospitals in the eastern region, which may affect the external validity of the study results and limit the applicability of the findings to other regions with different socioeconomic and demographic characteristics. Moreover, reliance on self-reported questionnaires may introduce the possibility of response bias. Lastly, the lack of empirical evidence from intervention studies highlights the need for future research to investigate the effectiveness of interventions aimed at improving benefit-finding in SLE patients. Despite these limitations, the strength of this study lies in identifying key populations for positive psychological interventions among SLE patients in eastern China. Specifically, individuals with lower educational levels, older age, multiple comorbidities, and self-payment for medical expenses exhibited lower benefit-finding. This underscores the importance of strengthening nursing assessments and interventions targeted at these key populations to improve their benefit-finding, particularly in terms of the SAQ-SA and SAQ-SE. Future research should delve deeper into the factors influencing benefit-finding in SLE patients and evaluate the impact of intervention studies on improving patient outcomes.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
This study adheres to the ethical principles outlined in the Declaration of Helsinki and was reviewed and approved by the Ethics Committee of Zhejiang Shuren University (Approval No. 20200105) to ensure compliance with ethical standards.
Acknowledgment
Tong is the co-first author. The authors thank all the participants and research assistants involved with this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was not supported by any funding source.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Ballester P, Cerdá B, Arcusa R, et al. Effect of ginger on inflammatory diseases. Molecules. 2022;27(21):7223. doi:10.3390/molecules27217223
2. Bhattarai M, Sharma NK, Paudel S, et al. Systemic lupus erythematosus associated with erythema multiforme: a rare case report of Rowell’s syndrome. Clinical Case Reports. 2024;12(4):e8677. doi:10.1002/ccr3.8677
3. Jolly M, Sequeira W, Block JA, et al. Sex differences in quality of life in patients with systemic Lupus Erythematosus. Arthritis Care Res. 2019;71(12):1647–1652. doi:10.1002/acr.23588
4. Liao J, Kang J, Li F, et al. A cross-sectional study on the association of anxiety and depression with the disease activity of systemic lupus erythematosus. BMC Psychiatry. 2022;22(1):591. doi:10.1186/s12888-022-04236-z
5. Du X, Chen H, Zhuang Y, Zhao Q, Shen B. Medication adherence in Chinese patients with systemic Lupus Erythematosus. J Clin Rheumatol. 2020;26(3):94–98. doi:10.1097/RHU.0000000000000952
6. Jordan J, Thompson NJ, Dunlop-Thomas C, Lim SS, Drenkard C. Relationships among organ damage, social support, and depression in African American women with systemic lupus erythematosus. Lupus. 2019;28(2:253–260. doi:10.1177/0961203318815573.
7. Taub R, Horesh D, Rubin N, et al. Mindfulness-based stress reduction for systemic Lupus Erythematosus: a mixed-methods pilot rand-omized controlled trial of an adapted protocol. J Clin Med. 2021;10(19):4450. doi:10.3390/jcm10194450
8. Dietz B, Katz P, Dall’Era M, et al. Major depression and adverse patient-reported outcomes in systemic lupus erythematosus: results from a prospective longitudinal cohort. Arthritis Care Res. 2021;73(1):48–54. doi:10.1002/acr.24398
9. Li RH, Peng HL, Yeh MH, Lou J. Psychological well-being increment as post-traumatic growth in women with breast cancer: a controlled comparison design using propensity score matching. Healthcare. 2022;10(8):1388. doi:10.3390/healthcare10081388
10. Li S, Ding H, Qi Z, et al. Serum metabolic fingerprints characterize systemic lupus erythematosus. Adv Sci. 2024;11(2):2304610. doi:10.1002/advs.202304610
11. Tayyab Z, Khan H, Saeed S, et al. Undiagnosed depression and its effects on patients with systemic lupus erythematosus. Cureus. 2024;16(1):e53064. doi:10.7759/cureus.53064
12. Pereira MG, Duarte S, Ferraz A, Santos M, Fontes L. Quality of life in patients with systemic lupus erythematosus: the mediator role of psychological morbidity and disease activity. Psychol Health Med. 2020;25(10):1247–1257. doi:10.1080/13548506.2020.1728350
13. Chin B, Lindsay EK, Greco CM, et al. Psychological mechanisms driving stress resilience in mindfulness training: a randomized controlled trial. Health Psychol. 2019;38(8):759. doi:10.1037/hea0000763
14. Sauder T, Hansen S, Bauswein C, et al. Mindfulness training during brief periods of hospitalization in multiple sclerosis (ms): beneficial alterations in fatigue and the mediating role of depression. BMC Neurol. 2021;21:1–15. doi:10.1186/s12883-021-02390-7
15. Forbes L, Johnson SK. Online mindfulness intervention for inflammatory bowel disease: adherence and efficacy. Front Psychol. 2022;12:709899. doi:10.3389/fpsyg.2021.709899
16. Garland E, Gaylord S, Park J. The role of mindfulness in positive reappraisal. Explore. 2009;5(1):37–44. doi:10.1016/j.explore.2008.10.001
17. Li S, Zhang X, Luo C, et al. The mediating role of self-acceptance in the relationship between loneliness and subjective well-being among the elderly in nursing home: a cross-sectional study. Medicine. 2021;100(40):e27364. doi:10.1097/MD.0000000000027364
18. Meireles JFF, Neves CM, Morgado FFR, et al. Development and psychometric properties of the self-acceptance scales for pregnant and postpartum women. Perceptual and Motor Skills. 2021;128(1):258–282. doi:10.1177/0031512520973518
19. Li C, Lyu S, Yan J, et al. The effect of gender in binge eating behavior in Chinese culture: the serial mediation model of body dissatisfaction and self-acceptance. Front Psychol. 2023;14:1285272. doi:10.3389/fpsyg.2023.1285272
20. Jing CFW, Feng J. The relationship between coping-style and self-acceptance among 239 female addicts. Chin J Social Med. 2014;3:190–192. doi:10.3969/j.issn.1673-5625.2014.03.016
21. Kabat-Zinn J. Full Catastrophe Living: The Program of the Stress Reduction Clinic at the University of Massachusetts Medical Center. New York: Delta; 1990.
22. Affleck G, Tennen H. Construing benefits from adversity: adaptational significance and di-spositional underpinnings. J Pers. 1996;64(4):899–922. doi:10.1111/j.1467-6494.1996.tb00948.x
23. Greeson JM, Chin GR. Mindfulness and physical disease: a concise review. Curr Opin Psychol. 2019;28:204–210. doi:10.1016/j.copsyc.2018.12.014
24. Tian L, Zhang Y, Li L, Wu Y, Li Y. The efficacy of mindfulness-based interventions for patients with COPD: a systematic review and meta-analysis protocol. BMJ Open. 2019;9(5):e026061. doi:10.1136/bmjopen-2018-026061
25. Kishida M, Mogle J, Elavsky S. The daily influences of yoga on relational outcomes off of the mat. Int J Yoga. 2019;12(2):103–113. doi:10.4103/ijoy.IJOY_46_18
26. Cai Z, Gui Y, Wang D, Yang H, Mao P, Wang Z. Body image dissatisfaction and impul-se buying: a moderated mediation model. Front Psychol. 2021;12:653559. doi:10.3389/fpsyg.2021.653559
27. Cong ZGW. Development of SELF-ACCEPTANCE QUESTIONNAIRE and its reliability and validity test. Chin Behav Med Sci. 1999;8(1):20–22.
28. Hanley AW, Garland EL. Clarity of mind: structural equation modeling of associations between dispositional mindfulness, self-concept clarity and psychological well-being. Pers Individ Dif. 2017;106:334–339. doi:10.1016/j.paid.2016.10.028
29. Sadooghiasl A, Ghalenow HR, Mahinfar K, Hashemi SS. Effectiveness of mindfulness-based stress reduction program in improving mental well-being of patients with COVID-19: a randomized controlled trial. Indian J Crit Care Med. 2022;26(4):439–445. doi:10.5005/jp-journals-10071-24164
30. Mazaheri M. Difficulties in emotion regulation and mindfulness in psychological and so-matic symptoms of functional gastrointestinal disorders. Iran J Psychiatry Behav Sci. 2015;9(4):e954. doi:10.17795/ijpbs-954
31. Parmentier FBR, García-Toro M, García-Campayo J, Yañez AM, Andrés P, Gili M. Mindf-ulness and Symptoms of Depression and Anxiety in the General Population: The Mediating Roles of Worry, Rumination, Reappraisal and Suppression. Front Psychol. 2019;10:506. doi:10.3389/fpsyg.2019.00506
32. Han D, Li S, Li X, Jiang F. An analysis of coping style and self-acceptance of master’s deg-ree students in a medical university. Chin J Health Psychol. 2016;24:1477–1480. doi:10.13342/j.cnki.cjhp.2016.10.011
33. Campo RA, Wu LM, Austin J, Valdimarsdottir H, Rini C. Personal resilience resources pr-edict post-stem cell transplant cancer survivors’ psychological outcomes through reductions in depressive symptoms and meaning-making. J Psychosoc Oncol. 2017;35(6):666–687. doi:10.1080/07347332.2017.1342306
34. Chiba R, Funakoshi A, Yamazaki Y, Miyamoto Y. The Benefit Finding Questionnaire (BFQ): scale development, validation, and its psychometric properties among people with mental illness. Healthcare. 2020;8(3):303. doi:10.3390/healthcare8030303
35. Chen Q, Xiao X, Zhang Y, Lin C. Analysis of the correlation between the level of posttraumatic growth and social support among caregivers of children with acute leukemia. Contrast Media Mol Imag. 2022;2022:7456284. doi:10.1155/2022/7456284
36. Huang X, Chen H, Li S. The relationship between assistance satisfaction and negative affect in long-term social assistance recipients in china: the moderating role of self-acceptance. Front Psychol. 2019;10:109. doi:10.3389/fpsyg.2019.00109
37. Xu W, Oei TP, Liu X, Wang X, Ding C. The moderating and mediating roles of self-acceptance and tolerance to others in the relationship between mindfulness and subjective well-being. J Health Psychol. 2016;21(7:1446–1456. doi:10.1177/1359105314555170.
38. Su H, Wang L, Li Y, Yu H, Zhang J. The mediating and moderating roles of self-accept-ance and self-reported health in the relationship between self-worth and subjective well-be-ing among elderly Chinese rural empty-nester: an observational study. Medicine. 2019;98(28):e16149. doi:10.1097/MD.0000000000016149
39. Xu W, Rodriguez MA, Zhang Q, Liu X. The mediating effect of self-acceptance in the relationship between mindfulness and peace of mind. Mindfulness. 2014;6:797–802. doi:10.1007/s12671-014-0319-x
40. Shi J, Yao Y, Zhan C, Mao Z, Yin F, Zhao X. The relationship between big five personality traits and psychotic experience in a large non-clinical youth sample: the mediating role of emotion regulation. Front Psychiatry. 2018;9:648. doi:10.3389/fpsyt.2018.00648
41. Shallcross AJ, Willroth EC, Fisher A, et al. Relapse/recurrence prevention in major depressive disorder: 26-month follow-up of mindfulness-based cognitive therapy versus an active control. Behav Ther. 2018;49(5):836–849. doi:10.1016/j.beth.2018.02.001
42. Porter N, Jason LA. Mindfulness Meditation Interventions for Long COVID: biobehavioral Gene Expression and Neuroimmune Functioning. Neuropsychiatr Dis Treat. 2022;18:2599–2626. doi:10.2147/NDT.S379653
43. Solati K, Mousavi M, Kheiri S, et al. The effectiveness of mindfulness-based cognitive therapy on psychological symptoms and quality of life in systemic lupus erythematosus patients: a randomized controlled trial. Oman Med Journal. 2017;32(5):378. doi:10.5001/omj.2017.73
44. Xu R, Yan Q, Xu Z, Long X, Yin R. Post-traumatic growth in adult patients with systemic lupus erythematosus: a cross-sectional study in China. Rheumatol Int. 2023;43(6):1077–1085. doi:10.1007/s00296-022-05233-x
45. Tarka P. An overview of structural equation modeling: its beginnings, historical development, usefulness and controversies in the social sciences. Qual Quant. 2018;52(1):313–354. doi:10.1007/s11135-017-0469-8
46. Baer RA. Mindfulness training as a clinical intervention: a conceptual and empirical review. Clin Psychol Sci Pract. 2003;10(2):125. doi:10.1093/clipsy.bpg015
47. Deng Y-Q, Liu X-H, Rodriguez MA, Xia C-Y. The five-facet mindfulness questionnaire: psychom-etric properties of the Chinese version. Mindfulness. 2011;2:123–128. doi:10.1007/s12671-011-0050-9
48. Weaver KE, Llabre MM, Lechner SC, Penedo F, Antoni MH. Comparing unidimensional and multidimensional models of benefit finding in breast and prostate cancer. Qual Life Res. 2008;17(5):771–781. doi:10.1007/s11136-008-9348-z
49. Liu Z, Zhang LF, Gudenkauf L. Cross-cultural adaptation of the Benefit Finding Scale(BFS) in Chinese cancer patients. Chin J Nurs. 2015;50(5):561–566. doi:10.3761/j.issn.0254-1769.2015.05.010
50. Erceg-Hurn DM, Mirosevich VM. Modern robust statistical methods: an easy way to maximize the accuracy and power of your research. Am Psychol. 2008;63(7):591–601. doi:10.1037/0003-066X.63.7.591
51. Zhou H, Long L. Statistical remedies for common method biases. Adv Psychhol Sci. 2004;12(06):942.
52. Xiong HX, Zhang J, Ye BJ, et al. Common method variance effects and the models of statistical approaches for controlling it. Adv Psychhol Sci. 2012;20(5):757. doi:10.3724/SP.J.1042.2012.00757
53. Camilleri GM, Méjean C, Bellisle F, Hercberg S, Péneau S. Association between mindfulness and weight status in a general population from the nutrinet-santé study. PLoS One. 2015;10(6):e0127447. doi:10.1371/journal.pone.0127447
54. Gonzalez-Mendez R, Díaz M. Volunteers’ compassion fatigue, compassion satisfaction, and post-traumatic growth during the SARS-CoV-2 lockdown in Spain: self-compassion and s-elf-determination as predictors. PLoS One. 2021;16(9):e0256854. doi:10.1371/journal.pone.0256854
55. Gregg JJ, Fiske A, Gatz M. Physicians’ detection of late-life depression: the roles of d-ysphoria and cognitive impairment. Aging Mental Health. 2013;17(8):1030–1036. doi:10.1080/13607863.2013.805403
56. Zhao J, Shao X. Self-management oriented 5 a nursing mode combined with mindfulness decompression method in the application of the elderly with type 2 diabetes. Clin Res Pra. 2012;7(11):153–155. doi:10.19347/j.cnki.2096-1413.202211042
57. Bränström R, Duncan LG, Moskowitz JT. The association between dispositional mindfulness, psychological well‐being, and perceived health in a Swedish population‐based sample. Br J Health Psychol. 2011;16(2):300–316. doi:10.1348/135910710X501683
58. Xia Y, Wei QF. Status and influencing factors of self-acceptance in patients with urinary flow diversion abdominal wall stomy for bladder cancer. Chin Nus Res. 2021;35(19):3522–3525.
59. Di J, Rutherford S, Wu J, et al. Knowledge of cervical cancer screening among women across different socio-economic regions of China. PLoS One. 2015;10(12):e0144819. doi:10.1371/journal.pone.0144819
60. Gong L, Men XY, Liu H, Liu S. Influencing factors of psychological distress in patients with systemic lupus erythematosus. J Community Med. 2020;18(21):1445–1448. doi:10.19790/j.cnki.JCM.2020.21.04
61. Zhu H. Exploration and practice of the relationship between college students’ learning adaptation and mental health under the information‐based teaching environment of pote-ntial profile analysis. J Environ Public Health. 2023;2023(1):2256741. doi:10.1155/2023/2256741
62. Liu ZZ, Zhang LF, Shi SS, Cao YR. Influencing factors of benefit finding in cancer patients. Chin J Behav Med Brain Sci. 2017;26(1):41–45. doi:10.1016/j.apjon.2024.100584
63. Hensler MA, Katz ER, Wiener L, Berkow R, Madan-Swain A. Benefit finding in fathers of childhood cancer survivors: a retrospective pilot study. J Pediatr Oncol Nurs. 2013;30(3):161–168. doi:10.1177/1043454213487435
64. Sekine Y, Fujisawa T, Suzuki K, et al. Detection of chronic obstructive pulmonary disease in community-based annual lung cancer screening: chiba chronic obstructive pulmonary disease lung cancer screening study group. Respirology. 2014;19(1):98–104. doi:10.1111/resp.12179
65. Saxena S, Misra PJ, Vishwanath NS, et al. Quality of life and its correlates in Central India. Int J Res Dev Health. 2013;1(2):85–96.
66. Gao J, Zheng P, Jia Y, et al. Mental health problems and social media exposure during COVID-19 outbreak. PLoS One. 2020;15(4):e0231924. doi:10.1371/journal.pone.0231924
67. Webers C, Vanhoof L, Leue C, et al. Depression in ankylosing spondylitis and the role of disease-related and contextual factors: a cross-sectional study. Arthritis Res Ther. 2019;21:1–10. doi:10.1186/s13075-019-1995-7
68. Sun CY, Lin Z, Zhou MJ, et al. Inflammatory bowel disease disease benefit status and influence factors analysis. J Nurs. 2022;29(6):1–6.
69. Lechner SC, Carver CS, Antoni MH, Weaver KE, Phillips KM. Curvilinear associations between benefit finding and psychosocial adjustment to breast cancer. J Consult Clin Psy-chol. 2006;74(5):828–840. doi:10.1037/0022-006X.74.5.828
70. Gardner MH, Mrug S, Schwebel DC, Phipps S, Whelan K, Madan-Swain A. Demographic, medical, and psychosocial predictors of benefit finding among caregivers of childhood cancer survivors. Psychooncology. 2017;26(1):125–132. doi:10.1002/pon.4014
71. Lin L, Jiang XJ, Zhang CP. Stage of ovarian cancer chemotherapy patients benefit level and influencing factors of study. Mater Child Health Care Chin. 2019;34(21):4860–4863.
72. Wang Y, Zheng Z, Duan X, Li M, Li Y. The relationship between mindfulness and social adaptation among migrant children in China: the sequential mediating effect of self-e-steem and resilience. Int J Environ Res Public Health. 2022;19(23):16241. doi:10.3390/ijerph192316241
73. Shorey RC, Brasfield H, Anderson S, Stuart GL. The relation between trait mindfulness and early maladaptive schemas in men seeking substance use treatment. Mindfulness. 2015;6(2):348–355. doi:10.1007/s12671-013-0268-9
74. Carletto S, Tesio V, Borghi M, et al. The effectiveness of a body-affective mindfulness intervention for multiple sclerosis patients with depressive symptoms: a randomized controlled clinical trial. Front Psychol. 2017;8:2083. doi:10.3389/fpsyg.2017.02083
75. Li X, Ma L, Li Q. How mindfulness affects life satisfaction: based on the mindfulness-t-o-meaning theory. Front Psychol. 2022;13:887940. doi:10.3389/fpsyg.2022.887940
76. Antonova E, Amaratunga K, Wright B, Ettinger U, Kumari V. Schizotypy and mindfulness: magical thinking without suspiciousness characterizes mindfulness meditators. Schizophr Res Cogn. 2016;5:1–6. doi:10.1016/j.scog.2016.05.001
77. Chen M, Cheung RYM. Testing interdependent self-construal as a moderator between mindfulness, emotion regulation, and psychological health among emerging adults. Int J Environ Res Public Health. 2021;18(2):444. doi:10.3390/ijerph18020444
78. Cova F, Garcia F, Oyanadel C, Villagran L, Páez D, Inostroza C. Adaptive reflection on negative emotional experiences: convergences and divergence between the processing-m-ode theory and the theory of self-distancing reflection. Front Psychol. 2019;10:1943. doi:10.3389/fpsyg.2019.01943
79. Ou LC, Guo XP, Meng YZ. Effect of acceptance and commitment therapy on resilience and perceived benefits of illness in patients with breast cancer after surgery. Mod Clin Nurs. 2017;16(2):14–18.
80. Gong Y, Yan Y, Yang R, et al. Factors influencing death anxiety among Chinese patients with cancer: a cross-sectional study. BMJ Open. 2022;12(10):e064104. doi:10.1136/bmjopen-2022-064104
81. Helgeson VS, Zajdel M. Adjusting to Chronic Health Conditions. Annu Rev Psychol. 2017;68:545–571. doi:10.1146/annurev-psych-010416-044014
82. Chaves C, Vazquez C, Hervas G. Benefit finding and well-being in children with life thr-eatening illnesses: an integrative study. terapia psicolÓgica. 2013;31(1):59–68. doi:10.4067/s0718-48082013000100006
83. Serban DM, Serban CL, Ursoniu S, Putnoky S, Moleriu RD, Putnoky S. Mindful Eating Questionnaire: Validation And Reliability In Romanian Adults. Int J Environ Res Public Health. 2022;19(17):10517. doi:10.3390/ijerph191710517
84. Paiva S, Carneiro MM. Complementary and alternative medicine in the treatment of chronic pelvic pain in women: what is the evidence? Int Scholarly Res Notices. 2013;2013:469575. doi:10.1155/2013/469575
85. Chen BC, Li H, Lin R, et al. Mindfulness-based cognitive intervention for benefit finding in patients with permanent enterostomy. J Nurs Sci. 2022;37(11):66–70.
86. Shen MY, Zhou JH. Effects of mindfulness-based stress reduction on hormone level alexithymia and benefit finding in women with menopausal syndrome. Chin Remed Clin. 2018;18(11):2087–2089. doi:10.11655/zgywylc2018.11.109
87. Shi JQ, Li XL, Xue LN, Ye HZ. Effect of follow-up based on problem-solving therapy on benefit finding in young and middle-aged breast cancer patients undergoing postoperative chemotherapy. Chin Rural Health Service Admin. 2018;38(6):781–784. doi:10.3969/j.issn.1005-5916.2018.06.028
88. Porter LS, Keefe FJ, Garst J, et al. Caregiver-assisted coping skills training for lung cancer: r-esults of a randomized clinical trial. J Pain Symptom Manage. 2011;41(1):1–13. doi:10.1016/j.jpainsymman.2010.04.014
89. Gao J, Wang X, Sun LY, Wang SL. Expressive writing application in the diagnosis of th-yroid cancer patients for the first time study. J Nur Train. 2020;35(5):468–472. doi:10.16821/j.cnki.hsjx.2020.05.020
90. Zhou XG, Hu JE, He WB, et al. Mandala painting therapy effects on cancer patients’ family caregivers benefit found. J Nurs Sci. 2020;35(5):83–86.
91. Liu SF, Feng WN, Wang C, et al. Effects of resourcefulness intervention combined with progressive muscle relaxation training on resourcefulness, disease benefit perception and cancer-induced fatigue in patients with lung cancer radiotherapy. J Community Med. 2022;20(4):223–227.
92. Nugent NR, Brick L, Armey MF, Tyrka AR, Ridout KK, Uebelacker LA. Benefits of yoga on IL-6: findings from a randomized controlled trial of yoga for depression. Behav Med. 2021;47(1):21–30. doi:10.1080/08964289.2019.1604489
93. Zhao HY, Zhang YB, Ma YF, et al. Implementation experience of peer support on improving benefit finding in patients with breast cancer after surgery. J Nurs. 2017;24(14):76–78.
94. Chen MG, Li Y, Ma CH, et al. Effects of “Internet +” mindfulness-based stress reduction combined with aerobic exercise on anxiety, depression, and post-traumatic growth in youngfemale cancer patients. J Nurs Train. 2021;36(03):197–202. doi:10.16821/j.cnki.hsjx.2021.03.002
95. Yang Y, Song CX. Based on the theory of ingenuity, nursing intervention and nutritional status in patients with laryngeal cancer radiotherapy after disease benefit influence. Chin J Prac Nurs. 2020;36(23):6.
96. Litvak Hirsch T, Lazar A. The contribution of long-term mindfulness training on personal and professional coping for teachers living in a conflict zone: a qualitative perspective. Int J Environ Res Public Health. 2020;17(11):4096. doi:10.3390/ijerph17114096
97. Shafieyan S, Soleymani MR, Samouei R, Afshar M. Effect of storytelling on hopefulness in girl students. J Educ Health Promot. 2017;6:101. doi:10.4103/jehp.jehp_59_16
98. Uebelacker LA, Kraines M, Broughton MK, et al. Perceptions of hatha yoga amongst persistently depressed individuals enrolled in a trial of yoga for depression. Complement Ther Med. 2017;34:149–155. doi:10.1016/j.ctim.2017.06.008
99. Iorgulescu G. Low self-esteem in women with eating disorders and alcohol abuse as a psycho-social factor to be included in their psychotherapeutic approach. J Med Life. 2010;3(4):458–464.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.