Back to Journals » Therapeutics and Clinical Risk Management » Volume 14
The impact of a combined intervention program: an educational and clinical pharmacist’s intervention to improve prescribing pattern in hospitalized geriatric patients at King Abdulaziz Medical City in Riyadh, Saudi Arabia
Authors Najjar MF ![]() , Sulaiman SAS
, Sulaiman SAS ![]() , Al Jeraisy M
, Al Jeraisy M ![]() , Balubaid H
, Balubaid H
Received 19 November 2017
Accepted for publication 21 December 2017
Published 16 March 2018 Volume 2018:14 Pages 557—564
DOI https://doi.org/10.2147/TCRM.S157469
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Muath Fahmi Najjar,1,2 Syed Azhar Syed Sulaiman,2 Majed Al Jeraisy,1 Hashim Balubaid3
1King Abdullah International Medical Research Centre, King Saud bin Abdulaziz University for Health Science, College of Pharmacy, King Abdulaziz Medical City, Ministry of National Guard-Health Affairs, Riyadh, Saudi Arabia; 2Pharmaceutical Sciences School, Clinical Pharmacy Discipline, Universiti Sains Malaysia, Penang, Malaysia; 3King Abdullah International Medical Research Centre, King Saud bin Abdulaziz University for Health Science, College of Medicine, King Abdulaziz Medical City, Ministry of National Guard-Health Affairs, Riyadh, Saudi Arabia
Background: There is a difference between evidence-based guidelines for geriatric patients and clinical practice of physicians. Prescribing potentially inappropriate medications (PIMs) can be attributed to the fact that many physicians are not aware of PIMs usage.
Aim: The aim of this study was to assess the effectiveness of a combined intervention program comprising an educational and clinical pharmacist intervention to reduce the incidence of PIMs among hospitalized geriatric patients.
Methods: This was a prospective pre-test versus post-test design study. The screening tool of older persons’ prescriptions, 2nd version, and 2015 American Geriatric Society Beers’ criteria were used to assess the appropriateness of medications prescribed for geriatric inpatients. The study was carried out in the medical wards of the Department of Medicine at King Abdulaziz Medical City in Riyadh, Saudi Arabia.
Results: Four hundred geriatric patients were enrolled in the study: 200 in a pre-intervention group (control) and 200 in the intervention group. After the combined intervention, the incidence rate of PIMs decreased significantly from 61% to 29.5% (p<0.001). Out of 317 recommendations given by the clinical pharmacist, the physicians accepted a total of 196 (61.83%) recommendations. The most common PIMs to avoid regardless of diagnosis of geriatric patients before interventions were first-generation antihistamines (46%), sliding scale insulin (18.5%), antipsychotics (6.5%), benzodiazepines (9.5%), and antiarrhythmic drugs (15%).
Conclusion: Using a combined intervention program that comprises an educational intervention of updated evidence-based guidelines and clinical pharmacist intervention would add a significant value to improve prescribing patterns in hospitalized geriatric patients.
Keywords: education, inappropriate, medication, elderly, Beers criteria, STOPP criteria
Introduction
Geriatric patients’ health care is complex due to the physiological, pathological, and psychological changes that increase with advancing age. Both the pharmacokinetics and pharmacodynamics of most drugs can become altered in the geriatric population, and this may contribute to adverse health outcomes. Inappropriate prescribing for geriatric patients remains a serious and continuing challenge to the health care system in most developed and developing countries. Therefore, the assessment of prescribing for geriatric patients is crucial to identify potentially inappropriate prescribing.1 The term potentially inappropriate medications (PIMs) refer to high-risk medications used by the geriatric population. According to the 2015 American Geriatric Society (AGS) Beers criteria, appropriate prescribing by avoiding PIMs can improve geriatric care. PIMs, as listed in the Beers criteria, have been widely used by researchers over the past 25 years in geriatric patients as an interventional tool for health care providers to improve their prescribing patterns.2 Unfortunately, some PIMs that should be avoided in geriatric patients were not included in the AGS 2015 Beers’ criteria. Therefore, the screening tool of older persons’ prescriptions (STOPP) criteria were developed to address some of these concerns. The STOPP criteria are based on an up-to-date literature review and consensus validation among a European panel of experts.
The STOPP cites 80 medications to be avoided, including drug–disease interactions and drug–drug interactions (DDIs), because they either lack efficacy or pose an unnecessarily high risk to geriatric patients when other safer alternatives are available.3 The high prevalence rate of PIMs can be attributed to the fact that many physicians are not aware of PIMs problems. There is a need to improve physicians’ and pharmacists’ knowledge of drug therapy in geriatric patients to improve the performance of health care system and serve people using the system.4 Pharmaceutical care may offer a promising strategy to improve the prescribing practice of physicians. Pharmacist-initiated interventions consist of a comprehensive evaluation of patients’ medication profiles for achieving optimal treatment by avoiding inappropriate medication selection, inappropriate dose or dosage form, disease–drug interactions, and potential DDIs.5 Clinical pharmacists can play an important role in detecting PIMs and recommending appropriate use of alternative medications to avoid adverse outcomes of inappropriate prescribing among geriatric patients.6
A persistent lack of geriatric physicians and geriatric pharmacists is the major concern not only in Saudi Arabia but also in most of the developing and developed countries. This shortage may lead to several medical problems in prescribing among geriatric patients.7 Also, using single intervention aimed at physicians might be less effective in reducing PIMs.8 Combined intervention is more effective in minimizing PIMs prescribing among geriatric patients.9 There is an overuse of PIMs in geriatric patients in Saudi Arabia due to lack of knowledge on the part of the physicians and clinical pharmacists.10 Hence, the study hypothesized that educational and clinical pharmacists’ interventions will reduce the incidence rate of PIMs among hospitalized geriatric patients. The main objective of this study was to assess the effectiveness of combined educational and clinical pharmacists’ interventions on the incidence rate of PIMs among geriatric patients in the inpatient setting, based on the STOPP and Beers criteria.
Methods
Our study adopted an interventional methodology pre-test versus post-test design to evaluate the efficacy of a combined intervention to prevent PIMs use among hospitalized geriatric patients. The intervention in the current study consisted of two components: an educational and a clinical pharmacist intervention. This study was approved under protocol number SP 14/152 by the Institutional Review Board of King Abdulaziz Medical City (KAMC). Only physicians who agreed to sign the consent for participation in the study were enrolled in the study. Informed consent from patients was waived by the institutional review board. For the second phase, the informed consent of patients has been waived since the objective of this study was to minimize the risk of prescribing PIMs among geriatric patients. It is a routine clinical practice of clinical pharmacist to provide physicians their recommendations based on evidence-based guidelines. Also, there was no communication with patients and no follow-up visits were required once the patients were discharged. Anonymous data have been collected from the patients by the clinical research coordinator. The main outcome of this study was the change in the incidence rate of PIMs, as measured in the pre-intervention and the intervention groups. Based on the literature, the average of incidence rate of PIMs was 50% and the researchers were hoping to be able to decrease this to half after the combined intervention.2,11 Using an alpha of 0.05 and a power of 80%, the estimated number of geriatric inpatients to be included was 384. A random sample of 400 hospitalized geriatric patients who met the inclusion criteria was enrolled to serve as a pre-intervention group (200 patients) and an interventional group (200 patients). The pre-intervention phase was carried out to gather and review baseline data about the current prescribing pattern of PIMs for geriatric inpatients. In the pre-intervention phase, a prospective audit was performed on data obtained from the Hospital Information System at KAMC to identify PIMs among geriatric inpatients.
The second phase was an educational program consisting of one-hour, weekly educational lectures for one month in the Department of Medicine. The educational sessions are part of the continuing medical education (CME) program accredited by the Saudi Committee of Health Sciences to help health care practitioners to update their knowledge in the form of educational grand rounds. It is a weekly grand round lectures carried out by the head of geriatric medicine and two clinical pharmacists. Lectures involved the updated lists of STOPP and Beers criteria. The handbook designed for the study was distributed to the physicians at the end of the seminars. The third phase was the collaboration between clinical pharmacists and the prescribers who aimed to utilize the STOPP and Beers criteria to optimize prescribing among hospitalized geriatric patients. The clinical pharmacists offered all possible interventions that might prevent PIM prescribing; the interventions included auditing of the physicians orders and providing feedback and recommendations during medical rounds, reminders, and discussions with physicians. The interventions and recommendations were made by three clinical pharmacists working in the medical wards in KAMC hospital. The clinical pharmacists were trained before starting the current phase using the updated 2015 AGS Beers and 2014 STOPP criteria. The daily responsibilities of the clinical pharmacists started with screening the hospitalized geriatric patients by means of the hospital information electronic system to identify patients who met the inclusion criteria. Geriatric patients who were 65 years old and above and admitted to the medical wards for more than 24 hours were enrolled in the study except those admitted for elective surgery. Then, patients were identified who were receiving PIMs based on the STOPP and Beers criteria. Finally, the pharmacists recommended appropriate and safe medications, medications dosage adjustment, or withdrawal of PIMs that were better avoided in geriatric inpatients. The study was conducted from January 2015 to July 2016. To facilitate the clinical pharmacists’ interventions, the authors of the study developed a pocket-sized handbook, “Handbook of PIMs Use Among Geriatric Patients®”, as an intervention tool based on the updated guidelines on prescribing appropriate medications in hospitalized geriatric patients. This tool was tailored to the drugs available in the formulary of KAMC Hospital. The purpose of the handbook was to save physicians’ time during clinical ward rounds and to improve their prescribing decisions. The study’s investigator compiled the data of PIMs based on STOPP and Beers criteria only.
Results
Four hundred geriatric patients were enrolled in the study: 200 in a pre-intervention group (control) and 200 in the intervention group. After the combined intervention, the incidence rate of PIMs decreased significantly from 61% to 29.5% (p<0.001). In general, all sociodemographic characteristics of geriatric patients, such as age, ethnicity, weight, smoking and alcohol consumption and family caregiver, did not significantly influence the PIMs rate before and after the clinical pharmacists’ intervention. Similarly, there was no significant difference with respect to Charlson age-comorbidity index, frailty, activities of daily living, and polymorbidity (≥4 diseases) before the baseline of the study. The highest percentage of chronic diseases observed was hypertension, diabetes mellitus, ischemic heart disease, heart failure, stroke, and chronic renal failure (Table 1). The total number of medications prescribed among the 400 hospitalized geriatric patients was 2,842 medications. The average number of prescribed medications received by the patients before the combined intervention was 7.16±3.2, with a range of 1–18 and a median of seven drugs, while the average number of the prescribed medications at post-intervention was 5.45±2.80, with a range of 1–12 and a median of five drugs. The prevalence rates of polypharmacy (concurrent use of five or more different prescription medications) during hospitalization and at discharge significantly decreased in the intervention group (p-value <0.001), whereas the prevalence rates of polypharmacy between two groups at the time of admission was not significant (p-value =0.472). The prescribers accepted 176 (89.8%) interventions as recommended and 20 (10.2%) with some modification. The most commonly accepted interventions were 96 (48.9%) to change PIMs among geriatric inpatients to safe alternatives. The majority of the recommendations were to stop PIMs as listed in Beers criteria (31; 15.8%), followed by to decrease dose (25; 12.7%), to stop STOPP criteria (21; 10.7%), to stop drug duplications (14; 7.1%), and to stop DDIs (9; 4.6%). Most of the clinical pharmacists’ recommendations were accepted by the staff physicians (32.7%) followed by consultants (24.5%). Neurologists accepted 49 (25.0%) and gastroenterologists accepted 36 (18.4%) of the recommendations provided by clinical pharmacists. The most common PIM medication classes to avoid based on Beers criteria, regardless of the diagnosis of geriatric patients before interventions, were antihistamines, diuretics, beta blockers, calcium channel blockers, angiotensin converting enzyme inhibitors, sliding scale insulins (SSIs), oral hypoglycemic agents, anticoagulants, analgesics, and benzodiazepines and antidepressants (Table 2). With regard to the PIMs and/or medication classes to be avoided in geriatric patients with a particular disease or syndrome, patients with heart failure and receiving non-steroidal anti-inflammatory drugs (NSAIDs), cyclooxygenase 2 (COX-2) inhibitors or calcium channel blockers were the higher incidence rate (Table 3). Table 4 includes the non-anti-infective PIMs that should be avoided or have their dosage reduced to varying levels of kidney function in geriatric inpatients (n=400) as per Beers criteria at pre-intervention and intervention groups. Of the 200 geriatric patients in the pre-intervention group, 110 (55%) received PIMs as listed in STOPP criteria and the incidence rate decreased to 31% patients after the combined intervention (p-value <0.05). Of the 110 hospitalized geriatric patients, 81 patients (40.5%) in our study were taking ≥2 PIMs. Table 5 shows the list of PIM incidence rates based on STOPP criteria before and after the combined intervention.
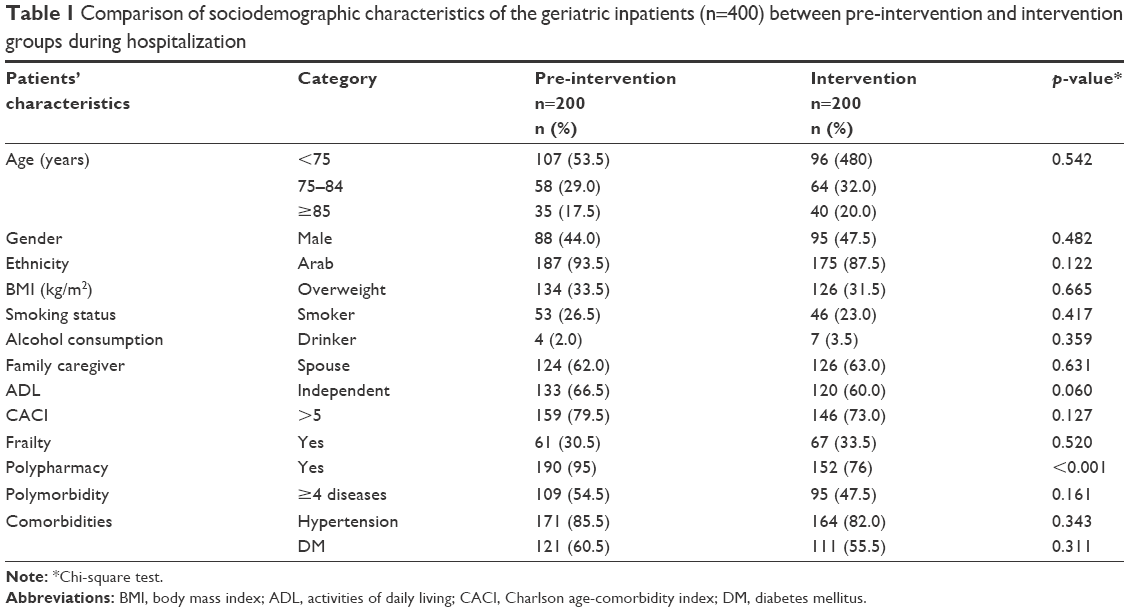 | Table 1 Comparison of sociodemographic characteristics of the geriatric inpatients (n=400) between pre-intervention and intervention groups during hospitalization |
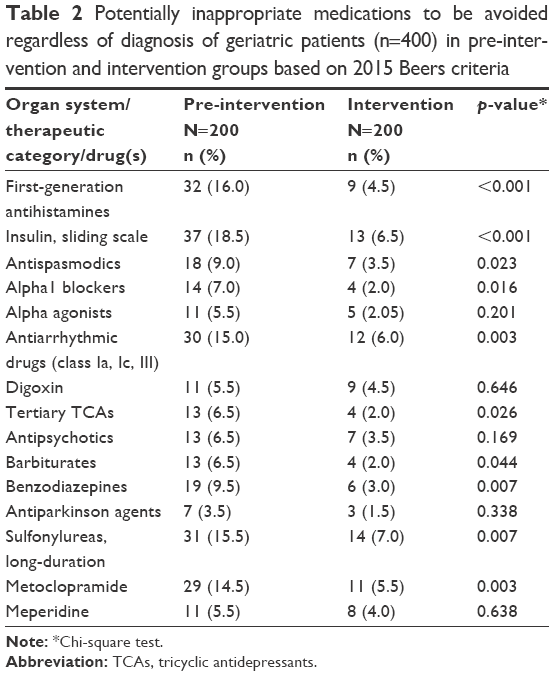 | Table 2 Potentially inappropriate medications to be avoided regardless of diagnosis of geriatric patients (n=400) in pre-intervention and intervention groups based on 2015 Beers criteria |
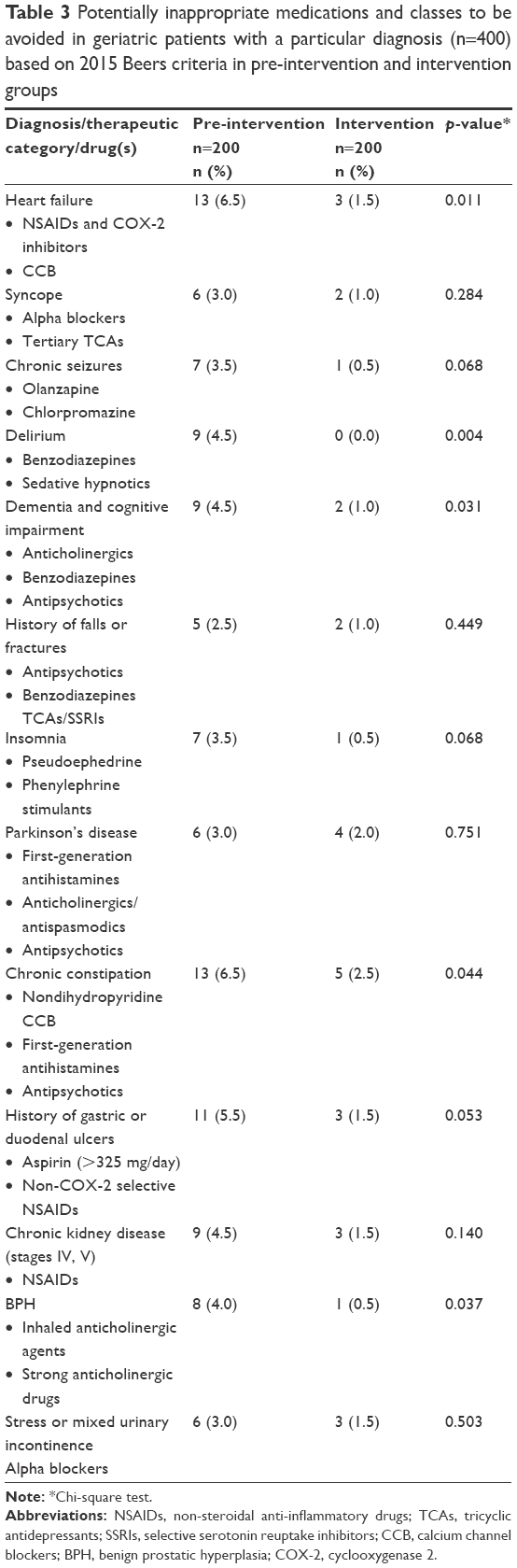 | Table 3 Potentially inappropriate medications and classes to be avoided in geriatric patients with a particular diagnosis (n=400) based on 2015 Beers criteria in pre-intervention and intervention groups |
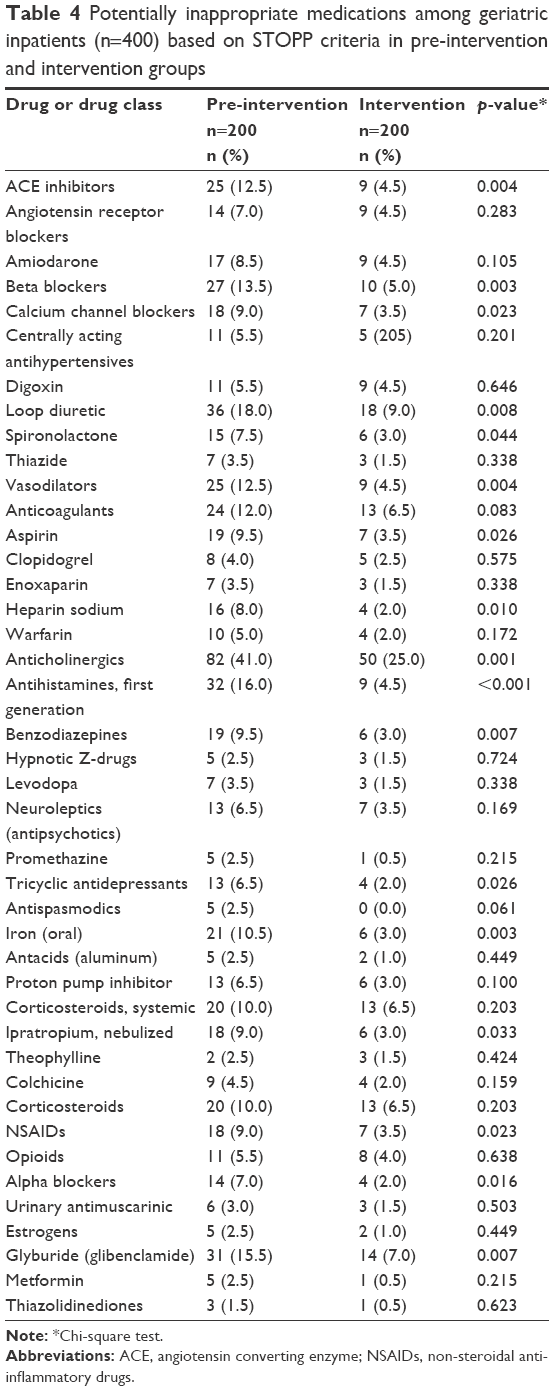 | Table 4 Potentially inappropriate medications among geriatric inpatients (n=400) based on STOPP criteria in pre-intervention and intervention groups |
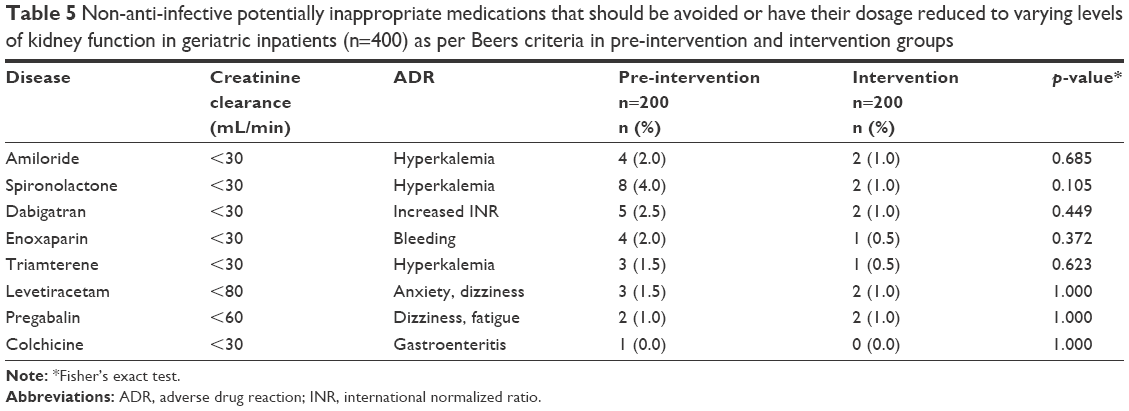 | Table 5 Non-anti-infective potentially inappropriate medications that should be avoided or have their dosage reduced to varying levels of kidney function in geriatric inpatients (n=400) as per Beers criteria in pre-intervention and intervention groups |
Discussion
Geriatric pharmacotherapy is becoming more complex and has not been well investigated. Health care professionals, including physicians, receive insufficient education in geriatric pharmacotherapy during their residency programs.4 Physicians’ knowledge has a significant impact on the prescription of appropriate medications for geriatric inpatients. There is little published research regarding prescribing patterns for hospitalized geriatric patients in the medical wards setting worldwide, and in Saudi Arabia locally. The role of the physicians is becoming more challenging as they encounter both polymorbidity and polypharmacy among geriatric patients. In the current study, we found a significant relationship between PIMs and polymorbidity (p<0.001) before the combined intervention. As most of the patients in our sample were suffering from polymorbidity, these high percentages of polypharmacy (95%) before the combined intervention among geriatric inpatients are expected. The percentage significantly decreased to 76% (p-value <0.05) in the intervention group. Clinical drug therapy becomes more complicated, especially for geriatric patients with multiple diseases (polymorbidity) and multiple medications (polypharmacy). In Saudi Arabia, polypharmacy was extremely high (89.1%) in outpatients attending a tertiary care centre.12 We found differences between the evidence-based guidelines for geriatric patients and the clinical practice of the study’s physicians in the pre-interventional phase. Most of the hospital physicians are unaware of the inappropriate use of medications in hospitalized geriatric patients.4 Hence, many previous studies have recommended the STOPP and Beers criteria in order to avoid PIMs among the geriatric population.13
To optimize physicians’ appropriate prescribing, there were educational and administrative interventions, or pharmacists’ interventions.13 Most studies in the literature recommend using multiple interventional approaches to avoid prescribing PIMs, for instance, educational programs or computerized alert systems on prescribed medications for geriatric patients. Thus, we conducted educational sessions, with a focus on clinical geriatric pharmacology, to improve geriatric pharmacotherapeutics; a clinical pharmacist intervention was applied simultaneously. Physicians’ decision making has been found to be affected by CME, while administrative interventions focus on effective approaches to avoid inappropriate prescribing practices. In the US, evidence-based pharmaceutical judgment helps to educate physicians about updated pharmacogeriatric guidelines.14 To acquire knowledge of geriatric pharmacotherapy, integration between theoretical knowledge and clinical practice is needed. The clinical pharmacist provided physicians with an evidence-based pharmaceutical care plan to recommend de-prescription of PIMs and give safe alternatives. In consistent with previous findings, the incidence rate of PIMs decreased significantly from 61% to 29.5% (p<0.001).15 Out of the 317 recommendations given by the clinical pharmacist, the physicians accepted a total of 196 (61.83%). The incidence rate of PIMs in our analysis was higher than that reported by earlier studies in other countries, which found that the incidence rate of PIMs ranged from 3.5% in France to 46% in Canada.16,17
There are several reasons behind the high incidence rate, and polypharmacy was the major risk factor of prescribing PIMs. Variable rate intravenous insulin infusion, which was previously known as SSI, was a very common PIM to avoid, based on the 2015 AGS Beers guidelines. About 37 (18.5%) of hospitalized geriatric patients received SSI at baseline, but the rate was reduced significantly to 13 (6.5%) in the intervention group (p<0.001). This finding is similar to the results reported in a previous study in India, in which 31 (15.5%) of geriatric inpatients were on SSI.18 Unfortunately, SSI is still widely used, despite evidence-based guidelines. We found a low adaptation to consensus recommendations, including the Beers criteria, showing an abuse of the SSI regimen as a single hypoglycemic treatment. These results are in line with other studies. First-generation antihistamines (eg, chlorpheniramine) were the commonly used PIMs among geriatric inpatients in our hospital. The incidence rate of first-generation antihistamine was reduced significantly from 32 (16.0%) before the interventions to 9 (4.5%) in the intervention group. In another study in Saudi Arabia, about 7.1% of geriatric patients were on chlorpheniramine.6 The AGS 2015 Beers criteria contain a strong recommendation to avoid the use of benzodiazepines and also noted that shorter-acting are no safer than long-acting benzodiazepines. The incidence rate of benzodiazepines in our results (9.5%) was lower than that found in several studies in the literature. In Korea, about 42.5% of geriatric patients take benzodiazepines.19 The reason for this reported by the authors was the high prevalence of delirium, dementia, and cognitive impairment of geriatric patients in their sample. Similar to our findings, about 10.8% of geriatric patients in the community setting of British Columbia, Canada received benzodiazepines.20 Potentially inappropriate antipsychotics continue to be prescribed, despite no clear evidence-based indication and poor outcomes in geriatric patients.21 We found that 13 (6.5%) of our patients received conventional and atypical antipsychotics at baseline. In India, 2.2% of hospitalized geriatric patients were on antipsychotics.22 Similarly, only 1% of geriatric inpatients received an atypical antipsychotic before admission and 12% were discharged from the hospital on an atypical antipsychotic.23 Potentially inappropriate psychotropic prescription in geriatric patients has become an important concern in developed countries antipsychotics (11.0%).24 The second group of the Beers criteria is the medications to be avoided with specific diseases or syndromes. We found that the most common practice of prescribing PIMs for hospitalized geriatric patients diagnosed with heart failure involved NSAIDs and COX-2 inhibitors. About 13 (6.5%) of the geriatric patients diagnosed with congestive heart failure were on the NSAIDs diltiazem, verapamil, pioglitazone, and rosiglitazone. This incidence rate is consistent with a study conducted in India, which showed that 12.5% of geriatric patients who were admitted to a tertiary care hospital in India were on PIMs.25 In contrast, our study showed a higher result than that found in a study conducted in the US, in which only 3.7% of geriatric patients with heart failure were on the NSAIDs and COX-2 inhibitors diltiazem, verapamil, pioglitazone, or rosiglitazone.26 The reason for our high incidence might be the high rate of cardiovascular diseases; in particular, congestive heart failure was higher among geriatric patients in our sample. It is inappropriate to compare the incidence rates between the present study and previous studies because of the differences in various factors, such as different settings (ie, sample size, location, and duration of study), assessment parameters, and health care systems. Clinical drug therapy should be safe, effective, and appropriate for geriatric patients. In many previous studies, PIMs prescribing among geriatric patients following the STOPP criteria ranged from 21.4% in primary care settings to 49.5% in nursing home facilities.27 Although there is agreement between the STOPP and Beers criteria in most of the recommendations, it is important to note the differences. The reasons for these may be due to the different prescribing patterns and the quality of medicine-based evidence between the US and Europe. Not all US medications are available in Europe and, therefore, Beers’ criteria are ineffective and need new criteria to apply in the European countries. Also, several medications in Europe that have a high risk of adverse drug reactions in geriatric patients are not included in the Beers’ criteria, which suggests that Beers criteria may be inadequate in their inclusion of medications linked to the common adverse drug reactions identified in geriatric patients.28 The main difference between the Beers and STOPP criteria is the safe alternative treatment options of the STOPP criteria.1 According to the STOPP criteria, PIMs are identified in 35%–77% of geriatric inpatients worldwide.8 In contrast, a retrospective cohort study found that about 27.6% of the geriatric patients admitted to 80 health care organizations in the US were on STOPP criteria medications.27 Tricyclic antidepressants are listed in both the STOPP and Beers criteria as a class of medications that can lead to serious adverse events including falls and/or dementia and/or cognitive impairment. According to the STOPP criteria, using NSAIDs with hypertension is considered as a drug–disease interaction and potentially inappropriate prescribing practice, while the Beers 2015 criteria do not mention this. Furthermore, the use of long-acting benzodiazepines is considered by both STOPP and Beers criteria as a PIM, and to be avoided regardless of the diagnosis, whereas that of short- and intermediate-acting benzodiazepines are regarded as PIMs in the Beers criteria only. Another difference is that the effect of first-generation antihistamines in causing falls is considered as a drug–disease interaction by the STOPP but not by the Beers criteria.
Conclusion
The combined intervention program comprising an educational intervention of updated evidence-based guidelines and clinical pharmacist intervention that targeted hospital physicians achieved a synergistic effect in avoiding PIMs among geriatric inpatients. Using the combined intervention would add a significant value to improve prescribing patterns in hospitalized geriatric patients.
Acknowledgments
This research was funded by the King Abdullah International Medical Research Center (KAIMRC). We would like to thank the School of Pharmaceutical Sciences at Universiti Sains Malaysia (USM), King Saud bin Abdulaziz University for Health Sciences (KSAU-HS) and King Abdullah International Medical Research Center (KAIMRC) for providing with facility to conduct this study.
Disclosure
The authors report no conflicts of interest in this work.
References
Hill-Taylor B, Walsh KA, Stewart S, Hayden J, Byrne S, Sketris IS. Effectiveness of the STOPP/START (Screening Tool of Older Persons’ potentially inappropriate Prescriptions/Screening Tool to Alert doctors to the Right Treatment) criteria: systematic review and meta-analysis of randomized controlled studies. J Clin Pharm Ther. 2016;41(2):158–169. | ||
Price SD, Holman CDJ, Sanfilippo FM, Emery JD. Association between potentially inappropriate medications from the Beers criteria and the risk of unplanned hospitalization in elderly patients. Ann Pharmacother. 2014;48(1):6–16. | ||
O’Mahony D, O’Sullivan D, Byrne S, O’Connor MN, Ryan C, Gallagher P. STOPP/START criteria for potentially inappropriate prescribing in older people: version 2. Age Ageing. 2014;44(2):213–218. | ||
Heininger-Rothbucher D, Bischinger S, Ulmer H, Pechlaner C, Speer G, Wiedermann CJ. Incidence and risk of potential adverse drug interactions in the emergency room. Resuscitation. 2001;49(3):283–288. | ||
Carson GL, Crosby K, Huxall GR, Brahm NC. Acceptance rates for pharmacist-initiated interventions in long-term care facilities. Pharm Pract. 2013;4(4):135. | ||
Bregnhoj L, Thirstrup S, Kristensen MB, Bjerrum L, Sonne J. Combined intervention programme reduces inappropriate prescribing in elderly patients exposed to polypharmacy in primary care. Eur J Clin Pharmacol. 2009;65(2):199–207. | ||
Fisher JM, Hunt K, Garside MJ. Geriatrics for juniors: tomorrow’s geriatricians or another lost tribe? J Royal Coll Physicians Edinb. 2014;44(2):106–110. | ||
Ramaswamy R, Maio V, Diamond JJ, et al. Potentially inappropriate prescribing in elderly: assessing doctor knowledge, confidence and barriers. J Eval Clin Pract. 2011;17(6):1153–1159. | ||
Petrovic M, Somers A, Onder G. Optimization of geriatric pharmacotherapy: role of multifaceted cooperation in the hospital setting. Drugs Aging. 2016;33(3):179–188. | ||
Al-Omar HA, Al-Sultan MS, Abu-Auda HS. Prescribing of potentially inappropriate medications among the elderly population in an ambulatory care setting in a Saudi military hospital: trend and cost. Geriatr Gerontol Int. 2013;13(3):616–621. | ||
Steinman MA, Seth Landefeld C, Rosenthal GE, Berthenthal D, Sen S, Kaboli PJ. Polypharmacy and prescribing quality in older people. J Am Geriatr Soc. 2006;54(10):1516–1523. | ||
Salih SB, Yousuf M, Durihim H, Almodaimegh H, Tamim H. Prevalence and associated factors of polypharmacy among adult Saudi medical outpatients at a tertiary care center. J Family Community Med. 2013;20(3):162–167. | ||
Clyne B, Fitzgerald C, Quinlan A, et al. Interventions to address potentially inappropriate prescribing in community-dwelling older adults: a systematic review of randomized controlled trials. J Am Geriatr Soc. 2016;64(6):1210–1222. | ||
Fick D, Semla T, Beizer J, et al. American Geriatrics Society updated Beers criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2012;60(4):616–631. | ||
Al Shemeili S, Stewart D. Use of the Drug Burden Index to identify and reduce potentially inappropriate prescribing of anticholinergic and sedative agents in elderly patients in institutionalized care: a systematic review protocol. JBI Database Syst Rev Implement Rep. 2014;12(4):48–59. | ||
Laroche ML, Charmes JP, Nouaille Y, Picard N, Merle L. Is inappropriate medication use a major cause of adverse drug reactions in the elderly? Br J Clin Pharmacol. 2007;63(2):177–186. | ||
Slaney H, MacAulay S, Irvine-Meek J, Murray J. Application of the beers criteria to alternate level of care patients in hospital inpatient units. Can J Hosp Pharm. 2015;68(3):218–225. | ||
Danisha P, Dilip C, Mohan PL, Shinu C, Parambil JC, Sajid M. Identification and evaluation of potentially inappropriate medications (PIMs) in hospitalized geriatric patients using Beers criteria. J Basic Clin Physiol Pharmacol. 2015;26(4):403–410. | ||
Nam YS, Han JS, Kim JY, Bae WK, Lee K. Prescription of potentially inappropriate medication in Korean older adults based on 2012 Beers criteria: a cross-sectional population based study. BMC Geriatr. 2016;16:118. | ||
Morgan SG, Weymann D, Pratt B, et al. Sex differences in the risk of receiving potentially inappropriate prescriptions among older adults. Age Ageing. 2016;45(4):535–542. | ||
Berryman SN, Jennings J, Ragsdale S, Lofton T, Huff DC, Rooker JS. Beers criteria for potentially inappropriate medication use in older adults. Medsurg Nurs. 2012;21(3):129–132; quiz 133. | ||
Sahana DA, Pai K, Rajeshwari S, Ullal SD, Rathnakar UP, Jaykumar SJ. Pattern of psychotropic drug usage in psychiatric illnesses among elderly. J Med Use Dev Ctries. 2010;2(1):3–10. | ||
Morandi A, Vasilevskis E, Pandharipande PP, et al. Inappropriate medication prescriptions in elderly adults surviving an intensive care unit hospitalization. J Am Geriatr Soc. 2013;61(7):1128–1134. | ||
Fond G, Fajula C, Dassa D, Brunel L, Lançon C, Boyer L. Potentially inappropriate psychotropic prescription at discharge is associated with lower functioning in the elderly psychiatric inpatients. A cross-sectional study. Psychopharmacology. 2016;233(13):2549–2558. | ||
Jhaveri BN, Patel TK, Barvaliya MJ, Tripathi C. Utilization of potentially inappropriate medications in elderly patients in a tertiary care teaching hospital in India. Perspect Clin Res. 2014;5(4):184–189. | ||
Lindblad CI, Hanlon JT, Gross CR, et al. Clinically important drug-disease interactions and their prevalence in older adults. Clin Ther. 2006;28(8):1133–1143. | ||
O’Sullivan DP, O’Mahony D, Parsons C, et al. A prevalence study of potentially inappropriate prescribing in Irish long-term care residents. Drugs Aging. 2013;30(1):39–49. | ||
Brown JD, Hutchison LC, Li C, Painter JT, Martin BC. Predictive Validity of the Beers and Screening Tool of Older Persons’ Potentially Inappropriate Prescriptions (STOPP) criteria to detect adverse drug events, hospitalizations, and emergency department visits in the United States. J Am Geriatr Soc. 2016;64(1):22–30. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.