Back to Journals » Clinical Ophthalmology » Volume 13
The frequency of non-pathologically thin corneas in young healthy adults
Authors Rashdan H, Shah M, Robertson DM ![]()
Received 27 September 2018
Accepted for publication 16 January 2019
Published 9 July 2019 Volume 2019:13 Pages 1123—1135
DOI https://doi.org/10.2147/OPTH.S188935
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Hannah Rashdan, Manali Shah, Danielle M Robertson
Department of Ophthalmology, UT Southwestern Medical Center, Dallas, TX, USA
Purpose: Measurement of normal corneal thickness and corneal epithelial thickness is important in keratorefractive surgery, glaucoma, following extended contact lens wear, and in patients with corneal disease. Clinically, a central corneal thickness less than 500 μm is considered to be moderately-to-extremely thin. The purpose of this study was to compare biological differences in patients with clinically thin compared to normal corneal thickness values in healthy young adults using Fourier domain optical coherence tomography.
Patients and methods: In total, 168 eyes from 84 patients aged 19–38 years were scanned using an Avanti optical coherence tomographer. To eliminate circadian effects on corneal thickness, all patients were scanned within a 4-hour window. Corneal thickness was measured across the central 6 mm of the cornea. Total central corneal thickness, corneal epithelial thickness, and corneal stromal thickness were compared between males and females and tested for correlations with age, use of systemic hormones, degree of myopia, and corneal curvature.
Results: The average central corneal thickness for males and females was 540.5±32.0 μm and 525.2±33.0 μm, respectively (P=0.020). Thirty-eight eyes had corneal thickness measurements below 500 μm; 12% (6 eyes) from males and 28% (16 eyes) from females (P=0.008). All women with corneas below 500 μm were bilaterally thin. This finding differed for men. Corneal thinning was not associated with age, use of systemic hormones, or degree of myopia. Females had steeper keratometry (K) readings (P=0.01 for flat K, P=0.002 for steep K) than males. No differences in layer offset values between normal thickness corneas and thin corneas were evident, suggesting that the reduced thickness was not pathological.
Conclusion: The results of this study indicate that a subpopulation of healthy young adults have non-pathologically thin corneas, well below 500 μm; and that these thinner corneas are more frequent in females. This underscores the importance of accurate corneal thickness measurements prior to keratorefractive surgery and when evaluating intraocular pressure in glaucoma.
Keywords: cornea, epithelial, stroma, thickness, OCT
Introduction
The cornea is an avascular, transparent tissue that accounts for approximately 60% of the refractive power of the eye. The anterior portion of the cornea is composed of a stratified, multi-layered epithelium, which has been shown to thin in multiple disease states, during extended contact lens wear and during aging.1–9 Accurate measurement of central epithelial and stromal corneal thickness is important, not only for patients undergoing keratorefractive procedures, such as photorefractive keratectomy and LASIK, but also in the assessment and diagnosis of glaucoma, for monitoring pathological changes in the ectatic cornea, and for assessing alterations in corneal biology and physiology in response to systemic disease.9–13 Numerous studies have investigated the relationship between biological parameters, including age, sex and racial differences, degree of myopia, and hormonal influences in relation to total corneal and epithelial thickness.14–23 The results of these studies have varied, and no clear consensus among different research groups exists.
Currently, multiple instruments are available for measuring total corneal and/or epithelial and stromal thickness. These include tandem scanning in vivo confocal microscopy through focusing, ultrasound pachymetry, slit scan pachymetry, Scheimpflug imaging, non-contact specular microscopy, and anterior segment optical coherence tomography (OCT).11,24–37 Similar to Scheimpflug imaging, slit scanning pachymetry, and non-contact specular microscopy, OCT is non-invasive and does not require applanation of the cornea.11,14,32,38 OCT was first used to measure the cornea in 1994. Now, OCT is used in many clinics for corneal and anterior segment imaging.38,39 Different types of anterior segment OCT have been developed. These include time domain and spectral/Fourier domain OCT.40,41 Unlike time domain OCT, spectral/Fourier domain OCT permits rapid image acquisition and allows for the precise measurement of 3-dimensional volumes across a specific region in the cornea.
Galgauskas et al42 reported on central corneal thickness in 1,650 Caucasians. In their study, they classified central corneal thickness ranging from 524–564 µm as average. Thinner central corneas were then classified based on severity: 510–524 µm (mild thinning), 489–510 µm (moderate thinning), and less than 489 µm (extreme thinning). For keratorefractive candidates, a central corneal thickness value below 500 µm is typically an exclusionary criteria for surgery. Our clinical observations suggest that there is a population of patients that present to the clinic with normally thin corneas that fall within the moderate-to-extreme range with no other signs of pathology, and that these patients tend to be female. The frequency of perspective candidates presenting with these normally thin corneas is unknown. Measurement of total corneal, epithelial, and stromal thickness using Fourier domain OCT has been reported to demonstrate high repeatability in normal, diseased, and post-surgical corneas.11,41 In the present study, we measured total central corneal, stromal, and epithelial thickness in healthy young adults across the central 6 mm of the cornea using the XR Avanti Fourier domain OCT. We then evaluated differences in corneal thickness as a function of key biological parameters, including age, sex, corneal curvature, and refractive error.
Materials and methods
This is a cross-sectional study to evaluate central corneal epithelial and stromal thickness across the central 6 mm in a population of normal, healthy adults. This study cohort was part of a larger, prospective, ongoing national clinical trial (NCT 02347631). All procedures were approved by the Institutional Review Board at the University of Texas Southwestern Medical Center and adhered to the Declaration of Helsinki. All patients signed informed consent prior to inclusion in the study.
A total of 168 healthy eyes from 84 adults were evaluated in this study. All patients were non-pregnant adults between 18 and 38 years of age and free of any existing ocular or systemic pathology. For inclusion in this study, each patient was required to have a refractive error below six diopters of myopia for the sphere power and less than one diopter of cylinder. All patients were correctable to 20/20 with spectacles. Patients had no prior history of ocular surgery and were either non-contact lens wearers or had not worn contact lenses for a minimum of 30 days prior to examination. None of the patients were currently using any topical ophthalmic medications. A basic slit lamp biomicroscopic examination was performed to rule out any anterior segment pathology. Schirmers testing without anesthesia and corneal staining using sodium fluorescein were used to rule out any clinically significant dry eye. All measurements were performed between the hours of 8 AM and 12 PM to control for diurnal fluctuations in corneal thickness. Spectacle correction was determined for all patients by manifest refraction. Keratometry values were determined using a Nidek Auto Ref/Keratometer (Fremont, CA, USA).
Corneal epithelial and stromal thickness mapping
Corneas were scanned using the Avanti Optical Coherence Tomographer (OCT) with the Cornea Advance module (Optovue, Fremont, CA, USA). Patients were scanned using the pachymetry map and total corneal power feature. Eight radial measurements were obtained with the beam centered within the pupil. Each cornea was scanned twice. Analysis of total corneal, epithelial, and stromal thickness measurements were performed automatically across the central 6 mm cornea using the manufacturer provided commercial software. This included the central 2 mm of the cornea, a 2–5 mm annulus, and a 5–6 mm annulus in the paracentral cornea. Thickness changes were evaluated for the horizontal, vertical, and diagonal meridians. In addition to thickness values, the following default layer offset values were automatically calculated by the Avanti software for total corneal thickness within the 2–5 mm region: difference between superior nasal and inferior temporal thickness (SN-IT), difference between the superior and inferior regions (S-I), minimum thickness (Min), difference between the minimum and median thickness (Min-Median), and difference between the minimum and maximum thickness (Min–Max). For the corneal epithelium, thickness values within the 2–5 mm region were computed for the superior quadrant (S), the inferior quadrant (I), minimum thickness (MIN), maximum thickness (MAX), standard deviation (SD), and the difference between the minimum and maximum thickness values (Min–Max). Individual eyes were independently evaluated, thus both eyes were not required to be thin for inclusion in the dataset.
Statistical analysis
Statistical analysis was performed using SigmaPlot 11.0 (Systat Software, Inc., San Jose, CA, USA). All data are expressed as mean±SD or mean standard error, as indicated. To determine variability, the coefficient of variation was determined by taking the ratio of the standard deviation to the mean. Normality and equal variance testing were performed using the Shapiro Wilk Normality Test and Kolmogorov-Smirnov Equal Variance Test. To assess differences in numerical data between two groups, such as age or thickness values, atwo-tailed Student's t-test or Mann-Whitney Rank Sum test was used, where appropriate. To determine differences in proportions such as sex, race, and ethnicity, a chi-square or Fisher’s exact test was used. To compare differences in thickness values between males and females in different quadrants, a two-way ANOVA with appropriate post-hoc multiple comparison test was used. Significance was set at P<0.05.
Results
One hundred and sixty-eight eyes from 84 participants were evaluated. Participant demographics are detailed in Table 1. Fifty-eight participants (69%) were female and 26 (31%) male. The mean age of all participants was 26.9±4.7 years (range=19–38). The male cohort had a mean age of 25.9±3.8 years. This was not significantly different from the female group, that had a mean age of 27.4±5.0 years (P=0.214, Mann-Whitney Rank Sum test). Approximately half of the study population was Caucasian (52%), 36% were Asian, and the remaining 12% were African American. The mean sphere power based on the manifest refraction for all patients was 3.31±1.59 diopters. The mean cylinder was 0.57±0.28 diopters. There were no differences in the sphere or cylinder component between males and females. Differences in keratometry values were present, however, with females exhibiting steeper keratometry (K) values than males (P=0.010 and P=0.002 for flat and steep K’s, respectively; Mann-Whitney Rank Sum test).
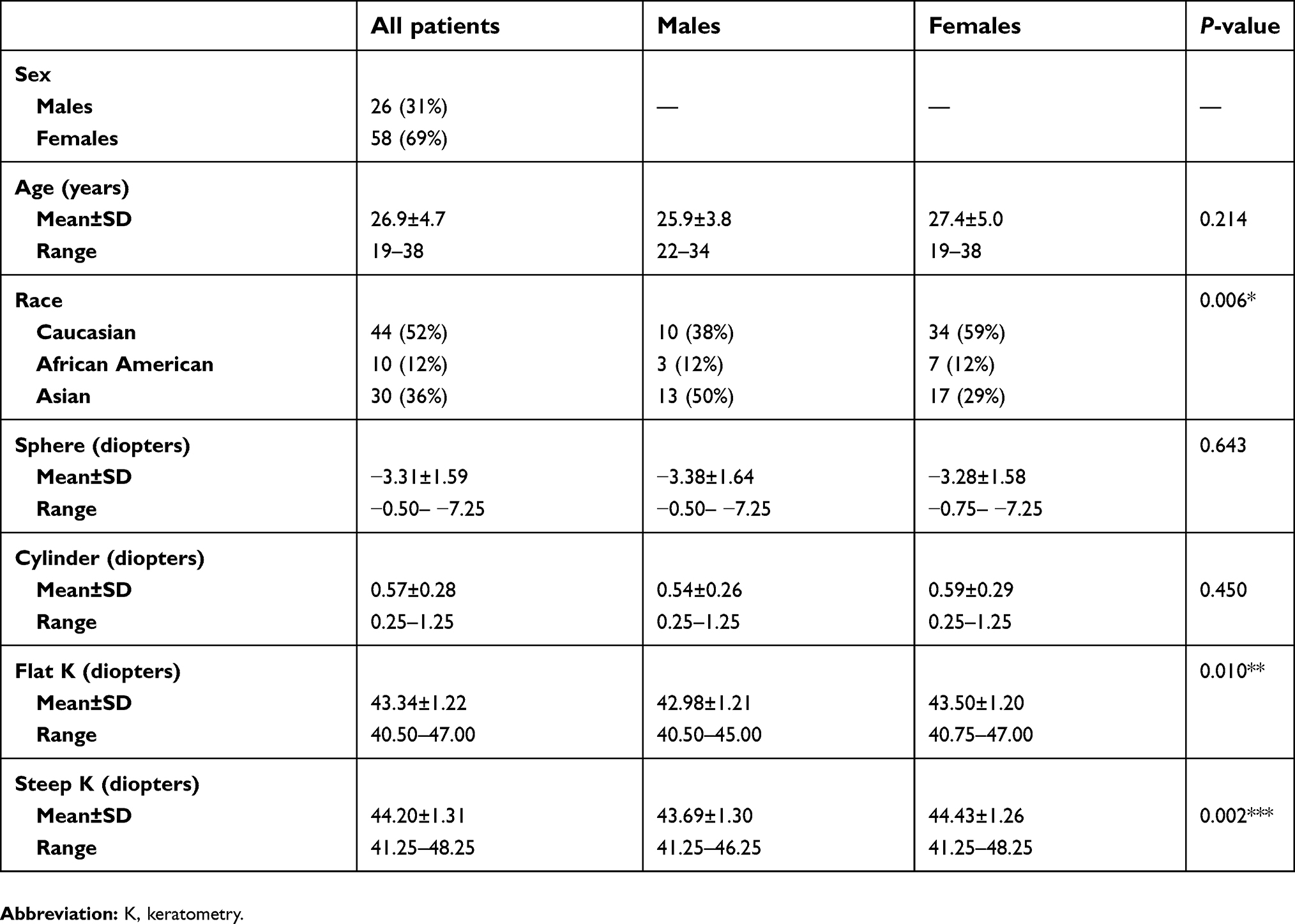 |
Table 1 Patient demographics |
Mean central corneal thickness within the central 2 mm for all participants was 529.7±32.8 μm (Table 2). Central corneal thickness values ranged from 465 μm to 611 μm. Mean central corneal epithelial thickness was 54.3±2.8 μm (range=48–64 μm) and mean stromal thickness was 475.4±31.9 μm (range=412–550 μm). As detailed in Table 2, there were no statistical differences in central corneal thickness (P=0.998, t-test), epithelial thickness (P=0.798, Mann-Whitney Rank Sum test), or stromal thickness (P=0.977, t-test) between right and left eyes.
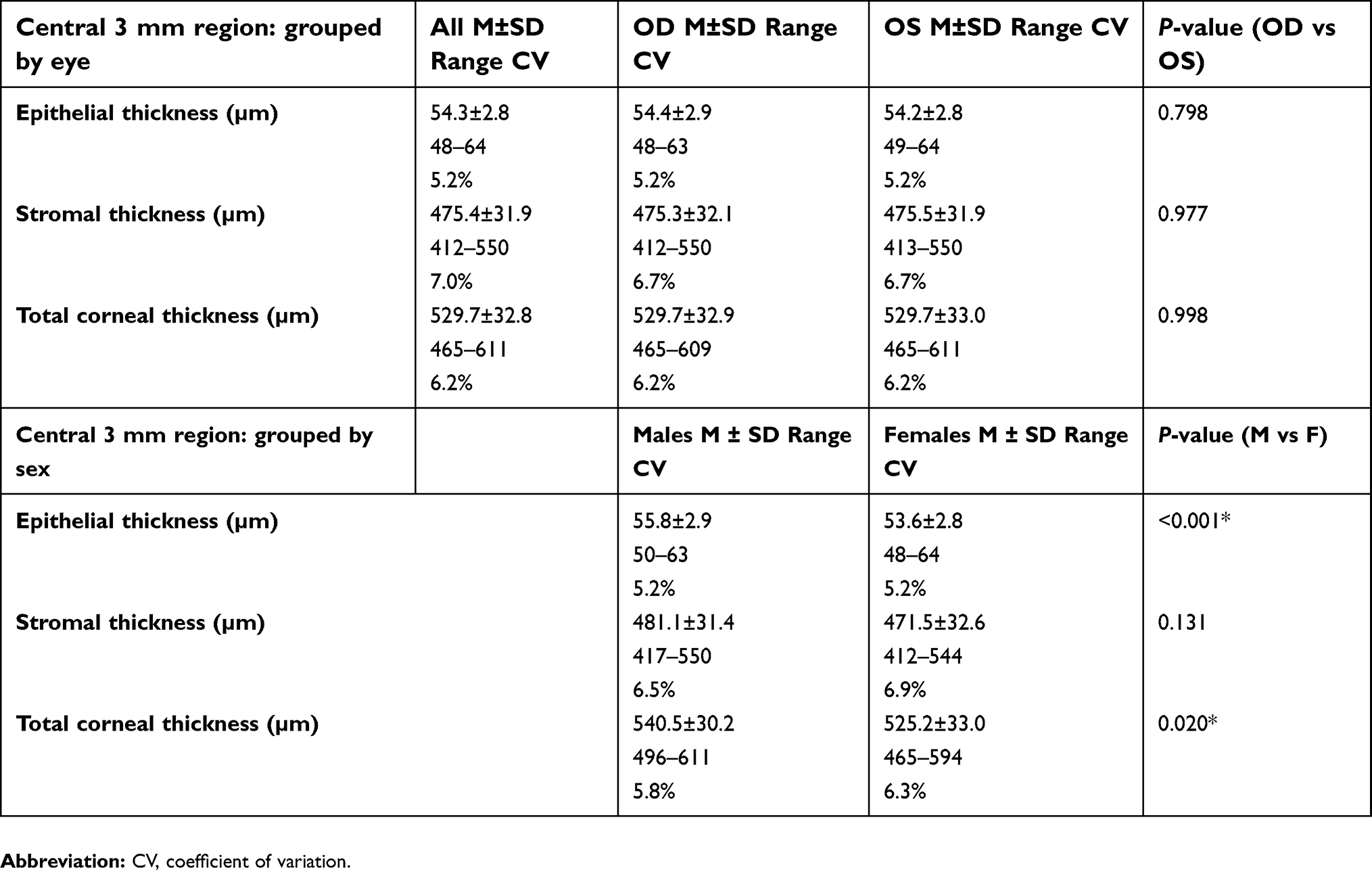 |
Table 2 Central corneal epithelial and stromal thickness |
Comparison of central corneal thickness values between males and females was statistically significant, with females having a thinner cornea (Table 2, 540.5±30.2 µm vs 525.2±33.0 µm, for males vs females, respectively; P=0.020, Mann-Whitney Rank Sum test). The corneal epithelium was also slightly thinner for females (53.6±2.8 μm for females vs 55.8±2.9 μm for males; P<0.001, Mann-Whitney Rank Sum test). While stromal thickness tended to be thinner in females than males, this finding was not significant (P=0.131, t-test). There was no significant correlation between central corneal thickness and age (R=0.0054, P=0.945, Pearson’s correlation coefficient). Similarly, there was no correlation between central corneal thickness and the spherical equivalent refractive error (R=−0.0433, P=0.579, Pearson’s correlation coefficient). While African Americans tended to have a lower mean central corneal thickness (515.4±31.8 µm) compared to Asians (531.5±37.3 µm) and Caucasians (529.9±30.2 µm), this finding was not significant (P=0.152, one-way ANOVA). Interestingly, mean keratometry readings were mildly inversely correlated with corneal thickness (R=−0.24, P=0.002, Pearson’s correlation coefficient). This is consistent with our finding of thinner central corneal thickness and steeper K values in females.
Comparison of regional differences in corneal epithelial thickness demonstrated that, in the 5 mm zone, the corneal epithelium was thickest inferiorly and inferior nasally (Figure 1A, P<0.001, two-way ANOVA). Epithelial thickness was further increased in the 6 mm circular zone inferiorly (56.1±3.2 μm) compared to the 5 mm circular zone (55.3±3.0 μm, P<0.001, two-way ANOVA). The epithelium was thinnest in the superior and superior temporal regions in both the 5 mm and 6 mm zones compared to all other regions (P<0.001, two-way ANOVA). In contrast to corneal epithelial thickness, stromal thickness was thickest superiorly and thinnest inferior temporally (Figure 1B, P<0.001, two-way ANOVA). Stromal thickness was uniformly increased across all regions in the 6 mm circular zone compared to the 5 mm circular zone (P<0.001, two-way ANOVA).
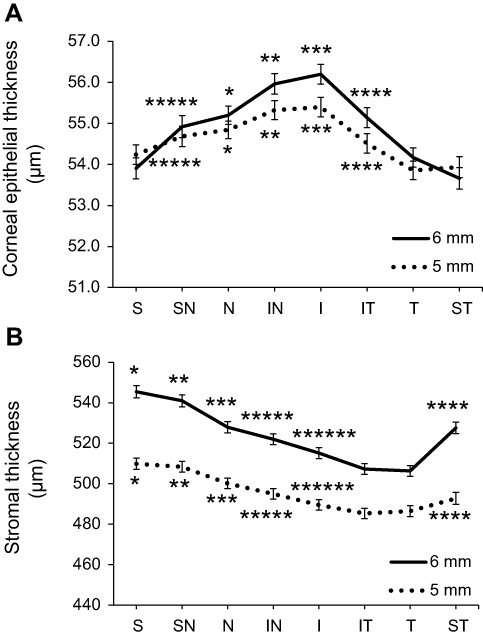 |
Figure 1 Epithelial and stromal thickness within 2–5 mm zone (5 mm) and the 5–6 mm zone (6 mm) measured across all eight regions. (A) In both the 5 mm and 6 mm corneal zones, the corneal epithelium was thickest inferiorly and inferior nasally and thinnest superiorly (*P<0.001 for N compared to ST, S, and T; **P<0.05 for IN compared to ST, S, T, SN, IT, and N; ***P<0.05 for I compared to ST, S, T, SN, IT, N, and IN; ****P>0.05 for IT compared to ST, S, and T; *****P<0.05 for SN compared to ST, S, and T; One-way ANOVA, Student-Newman-Keuls post hoc multiple comparison test). Epithelial thickness values at all regions were significantly different between the 5 mm and 6 mm zones (P=0.009). (B) Unlike the corneal epithelium, corneal stromal thickness was thickest superiorly and thinnest in the inferior temporal region (*P<0.001 for S compared to all other regions except SN; **P<0.001 for SN compared to all other regions; ***P<0.001 for N compared to IT, T, and I; ****P<0.001 for ST compared to IT, T, and I; *****P<0.05 for IN compared to IT, T, and I; and ******P<0.05 for I compared to IT and T; One-way ANOVA, Student-Newman-Keuls post hoc multiple comparison test). Overall stromal thickness was uniformly thinner within the 5 mm zone compared to the 6 mm zone (P<0.001). Data presented as mean±standard error. Abbreviations: I, inferior; IN, inferior nasal; IT, inferior temporal; N, nasal; S, superior; SN, superior nasal; ST, superior temporal; T, temporal. |
As expected, comparison of right and left eyes revealed no differences in epithelial or stromal thickness in any of the regions tested (Tables S1 and S2). The co-efficient of variation ranged from 5.3%–7.3%. The mean coefficient of variation was slightly increased for stromal measurements compared to epithelial measurements (P<0.001, t-test). Evaluation of epithelial thickness between males and females demonstrated a consistent 2–3 μm decrease across all corneal regions assessed, with females having a significantly thinner corneal epithelium than males (P<0.001, Figures 2A and C, two-way ANOVA, Student-Newman-Keuls post hoc multiple comparison test, and Table 2, Mann-Whitney Rank Sum test). Similarly, stromal thickness was thinner for females compared to males in the 5 and 6 mm annular regions (P<0.001, Figures 2B and D, two-way ANOVA, Student-Newman-Keuls post-hoc multiple comparison test). The effect of sex on stromal thickness in the central 2 mm region was not significant, although it showed a trend towards stromal thinning in females (P=0.131, Table 2, t-test).
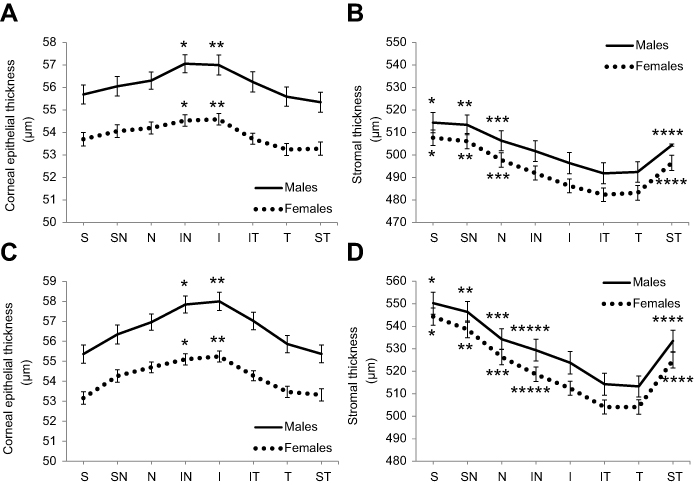 |
Figure 2 Corneal epithelial and stromal thickness in males vs females. (A) Epithelial thickness within the 5 mm zone was significantly thicker in the inferior and inferior nasal region (*P<0.05 for IN compared to ST, T, and S; **P<0.05 for I compared to ST, T, and S; Two-way ANOVA, Student-Newman-Keuls post hoc multiple comparison test). Across all regions, the epithelium was thicker for males compared to females (P<0.001). (B) Stromal thickness within the 5 mm zone was thickest superiorly (*P<0.05 for S compared to IT, T, I, IN, and ST; **P<0.05 for SN compared to IT, T, I, and IN; ***P<0.05 for N compared to IT, T, and I; ****P<0.05 for ST compared to IT and T; Two-way ANOVA, Student-Newman-Keuls post hoc multiple comparison test). Stromal thickness was greater in males than females in all regions (P<0.001). (C) In the 6 mm zone, the epithelium was also thickest in the inferior and inferior nasal region (*P<0.05 for IN compared to ST, T, and S; **P<0.05 for I compared to ST, T, and S; Two-way ANOVA, Student-Newman-Keuls post hoc multiple comparison test). Similar to the 5 mm zone, the epithelium was thicker for males than females across all regions (P<0.001). (D) Stromal thickness within the 6 mm zone was also thicker superiorly, with a greater difference between the superior and inferior stroma (*P<0.001 for S compared to all other regions except SN; **P<0.05 for SN compared to all other regions; ***P<0.05 for N compared to all other regions except T, IT, and I; ****P<0.05 for ST compared to T, IT, and I; *****P<0.05 for IN compared to T and IT; Two-way ANOVA, Student-Newman-Keuls post hoc multiple comparison test). Again, males had a greater stromal thickness than females across all regions (P<0.001). Data presented as mean±standard error. Abbreviations: I, inferior; IN, inferior nasal; IT, inferior temporal; N, nasal; S, superior; SN, superior nasal; ST, superior temporal; T, temporal. |
A histogram showing the distribution of corneal thickness values across males and females is shown in Figure 3. Data for males and females are normalized to the number of patients in each group. Interestingly, 23% of participants (38 of 168 eyes) had clinically thin corneas, defined by a total central corneal thickness value of less than 500 μm; 28% of females (32 eyes) examined had thin corneas, whereas only 12% of males (6 eyes) were clinically thin (P<0.001, chi-square test). In this study cohort, all females with a central corneal thickness value of less than 500 μm showed bilaterally thin corneas; whereas two males presented with a unilaterally thin cornea with mean thickness values approaching 500 μm. To rule out any effects of prolonged daily soft contact lens wear on central corneal thickness, measurements for clinically thin corneas (<500 µm) were subdivided into non-lens wearers and established wearers. Central corneal thickness for non-wearers was 483.1±10.3 µm (n=15 eyes) and 484.2±10.2 µm (n=23 eyes) for established wearers (P=0.611, Mann-Whitney Rank sum test).
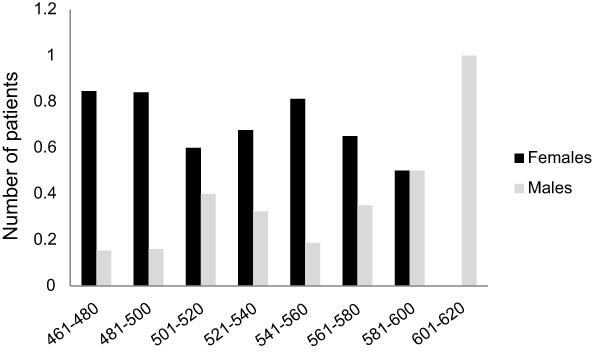 |
Figure 3 Distribution of central corneal thickness across all subjects. Data is plotted as the normalized number of males and females per total number in each group. |
Analysis of the metrics for identifying a pathologically thin cornea or form fruste keratoconic is shown in Table 3. The mean layer offset thickness value superior to inferior (S-1) measurement was 19.1±12.0 µm for all subjects and dropped to 16.9±11.9 µm in subjects with corneal thickness below 500 µm. A value greater than 45 would be suspicious for keratoconus. Similarly, the minimum corneal thickness value was 522.8±32.9 µm for all subjects and 478.1±12.3 µm for thin corneas, and the minimum to maximum value ranged from −63.2±13.5 µm for all subjects to −60.4±12.2 µm for thin corneas, all well within the normal value range.
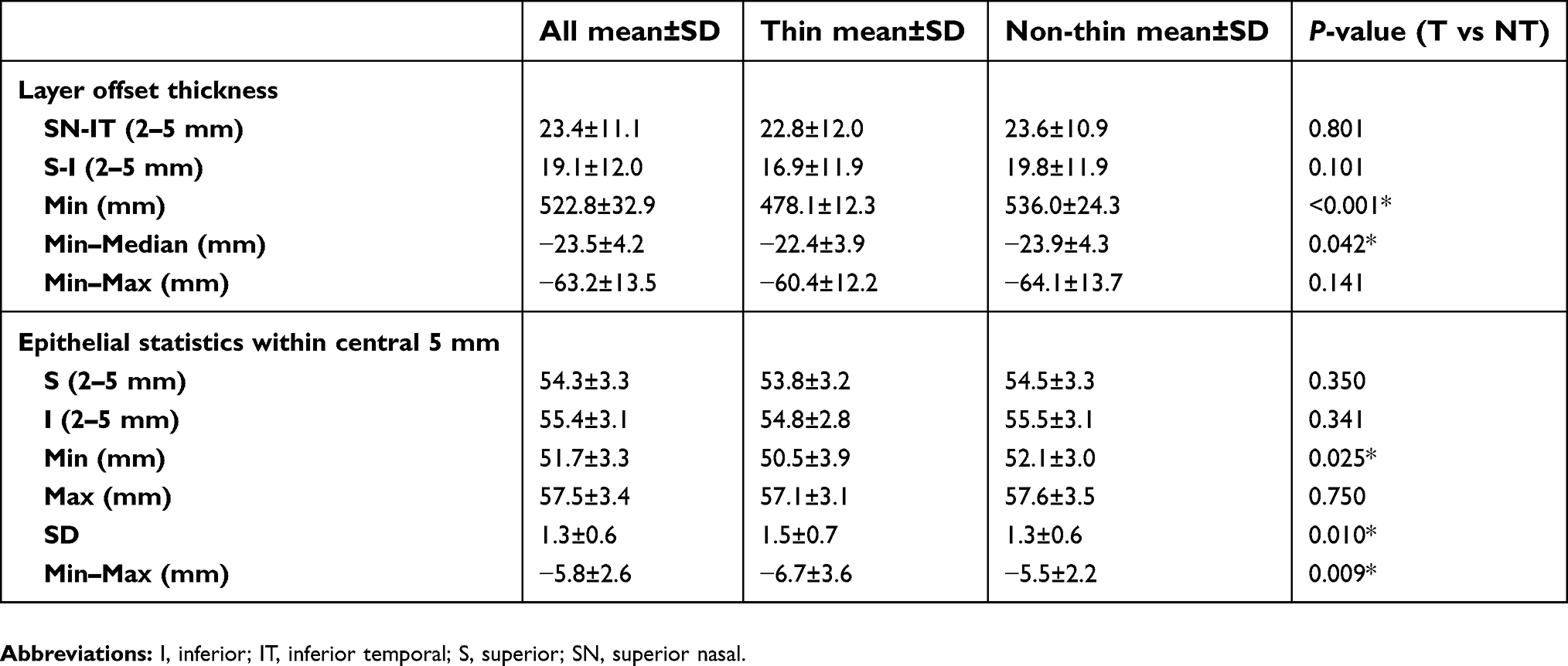 |
Table 3 Corneal epithelial and layer offset values for thin vs non-thin corneas |
Discussion
In the present study, epithelial, stromal, and total corneal thickness values were measured across the 6 mm central cornea. For all three parameters, thickness was significantly thinner in females compared to males. This finding is in agreement with previous studies reporting that central corneal thickness was higher in males.21,43,44 However, other studies have yielded conflicting results. In their paper evaluating 500 eyes from 250 subjects, Hassan et al45 reported a mean central corneal thickness value of 529.5±33.6 µm and 524.1±33.3 µm, for males and females, respectively. Sanchis-Gimeno et al46 also measured central corneal thickness in 100 eyes of 100 subjects. Using the Orbscan II, they also reported no thickness differences between males and females. In fact, the range of central corneal thickness values for males was 405–601 µm and 480–606 µm for females. Using spectral domain OCT, Samy et al20 evaluated corneal thickness in 240 eyes from 120 subjects split evenly between males and females. In that study, corneal thickness did decrease with age, but was unaffected by sex. Differences between the current and former study designs that may account for the sex disparity in central corneal thickness include the wide age range used in many studies. For example, in their report, Galgauskas et al42 found that, while corneal thickness was impacted by age, with thicker corneas present in younger subjects, the age affect was greater on males than females. Likewise, Samy et al20 and Sanchis-Gimeno et al46 both had extended age ranges from 18–80 years of age and 19–54 years of age, respectively. Unlike these latter studies, Hassan et al45 restricted their age range to 40–44 years of age and concluded that male central corneal thickness was slightly thinner than females.
In the present study, we restricted our age range to 18–38 years, thus our cohort consisted of healthy young adults. After controlling for age, we were able to detect a sex difference in central corneal thickness. Unlike other studies, we also accounted for use of systemic hormones, which may likely contribute to changes in both corneal biomechanics and thickness, and diurnal changes by imaging all subjects within the morning hours. One limitation to the current study, however, is the lack of male participants enrolled compared to females. Here we reported a cohort that was composed of 31% males and 69% females. This unequal gender distribution is common in contact lens studies. While the distribution in the number of patients of each sex was slightly skewed, variance in corneal thickness between each group was equal and the sample size was sufficient for good statistical power.
Prior studies have shown that corneal thickness using Fourier/Spectral Domain OCT results in thinner measurements than other methodologies. In a study by Vollmer et al,47 they reported that measurements with spectral domain OCT were, on average, 12 µm thinner. In agreement with a more recent report, Erdur et al48 reported mean thickness measurements also using spectral domain OCT compared to other methodologies, and found a decrease in means of 9 µm. Our measured central corneal thickness in the present study was 529.75±32.8 µm. After accounting for the 10–15 µm reduction in corneal thickness that has been reported when using this technology, these values are well within the reported ranges for corneal thickness values.
The important finding in this study is not the overall thinner cornea in females, but the interesting finding that there is an increase in the proportion of clinically thin, non-pathological corneas in females compared to males. A total of 38 eyes examined in our study had central corneal thickness values below 500 µm. When split into subgroups, four eyes from three different males had corneas ranging in thickness from 481–500 µm; compared to 21 eyes from 42 females. Going even thinner, in the 461–480 µm subgroup, 11 eyes from 22 females had thin corneas compared to two eyes from one male. None of the subjects with a normal thin cornea had undergone any type of ocular surgery, including keratorefractive procedures, and all patients had not worn contact lenses for a period of at least 1 month prior to measurement.
For those patients that were contact lens wearers, 100% were habitual or occasional daily soft lens wearers. There were no rigid lens wearers enrolled in this study. In contrast to extended soft lens wearers, daily wear of soft contact lenses does not normally alter corneal epithelial thickness.2 However, even during extended wear, corneal epithelial thickness shows the largest drop during the first month of wear, but this recovers to near baseline values over 12 months of wear. Any residual reduction in corneal epithelial thickness has been shown to recover in full approximately 1 month following cessation of contact lens wear.49 Consistent with this, subsequent evaluation of contact lens wearing history in our subjects with thin corneas revealed no differences in central corneal thickness between non-lens and established wearers. Hormonal contraceptive use was also not associated with the thinner corneas. In agreement with published findings, African Americans tended to have a lower central corneal thickness value.50,51 This was not significant in our study, indicating that a larger cohort is needed to tease out the effects of race.
The mean flat and steep keratometry values were 43.3±1.2 D and 44.2±1.3 D for all subjects. Keratometry values were slightly but significantly steeper for women compared to men, suggesting a potential relationship between corneal curvature and thickness. This finding is in agreement with work by Mimouni et al52 that found that thinner central corneal thickness values were associated with an increase in mean keratometry readings. Reinstein et al53 also investigated the relationship between central corneal epithelial thickness and curvature, both at the epithelial vertex and within the central 3 mm zone. In that study, there was no association between corneal epithelial thickness and age. Similarly, another group evaluated the relationship between keratometry and central corneal thickness in subjects with Marfan syndrome. They found that both corneal thickness and keratometry values were lower in test subjects compared to controls, which argues against our current data.54 Collectively, the relationship between corneal curvature and central corneal thickness is unclear. Further study is needed to establish the relationship between these two parameters.
In addition to central corneal thickness, regional differences in corneal epithelial and stromal thicknesses were also evident. In general, the corneal epithelium is thicker inferiorly and inferior-nasally, with the thinnest region located superiorly and superior-temporally. Consistent with this vertical shift in epithelial thickness, the inferior epithelium was thicker in the 6 mm zone compared to the 5 mm zone. This vertical change in corneal epithelial thickness is in agreement with previously reported work.28,53 We speculate that the observed thinning of the superior corneal epithelium is due to the tension and pressure forces from the superior eyelid. In contrast to the epithelium, the stroma was thickest superiorly and thinnest temporally and inferior-temporally. Regional changes within the 5 mm and 6 mm zones were also noted. This measured difference in zones was maintained across all quadrants.
Sex-based differences were also noted between epithelial and stromal thickness for both males and females within each quadrant and zone. On average, the corneal epithelium in males was approximately 2–3 μm thicker than females, regardless of location. Likewise, stromal thickness tended to be thicker in males compared to females. The underlying basis for this sex difference in corneal sublayer thickness is unknown. Interestingly, studies evaluating skin thickness have shown that males have thicker skin than females, regardless of age.55,56 Different mechanisms have been suggested, including the loss of collagen. Skin thickness, like corneal thickness, has been shown to decrease in subjects in their mid-forties.55 Thus, while an age-specific effect on corneal thickness was not detected in the present study, this is most likely due to the narrow age range evaluated and exclusion of subjects over 38 years of age. The tight exclusion criteria for age would have also eliminated post-menopausal women from analysis.
Conclusion
There is a sub-population of healthy young adults that have clinically thin corneas. In addition, sex-based differences in central corneal thickness measurements indicate that approximately one-fourth of females have clinically thin corneas. The role of female sex hormones as a potential underlying etiology for driving this shift in thickness is not well established, but we speculate likely plays a contributory role. Of note, sex hormones have been associated with corneal ectasia in subjects with known pathology.57 How these hormones regulate corneal thickness during normal development compared to pathological thinning is an important direction for further study. Central corneal thickness has become increasingly important in the measurement of intraocular pressure in glaucoma and in determining suitability of candidates for keratorefractive surgery. Moreover, the recent push by the National Institutes of Health to examine sex as a biological variable further underscores the need to investigate these differences. Future studies are needed to characterize factors that mediate corneal thickness changes over time and to identify select patient groups who may be more prone to normal, non-pathological thinning.
Data sharing availability
The questions below were taken from Taichman et al.58
- Will individual participant data be available?Yes
- What data in particular will be shared?The specific individual, de-identified participant data that was used for analysis and reporting of results in the present manuscript (including text, tables, and figures).
- What other documents will be available?Study protocol, statistical analysis plan, and the code used for analysis.
- When will data be available?Immediately following publication and ending 36 months following article publication.
- With whom will data be available?Any researchers who submit a valid proposal to the corresponding author/principal investigator of this study.
- For what type of analyses?To achieve aims in the outlined proposal.
- By what mechanism will data be made available?All research proposal requests should be directed to [email protected]. To gain access, data requestors will be required to sign a data access agreement.
Disclosure
Dr Danielle M Robertson reports grants from Alcon Laboratories for colleting data as part of a larger study. The data presented does not relate to any of Alcon's products. Grants from Alcon Laboratories were for an investigator-designed research study. Alcon had no input in the study design or analysis/interpretation of any of the data. The authors report no other conflicts of interest in this work.
References
1. Cavanagh HD, Ladage PM, Li SL, et al. Effects of daily and overnight wear of a novel hyper oxygen-transmissible soft contact lens on bacterial binding and corneal epithelium. Ophthalmology. 2002;109:1957–1969.
2. Ladage PM, Yamamoto K, Ren DH, et al. Effects of rigid and soft contact lens daily wear on corneal epithelium, tear lactate dehydrogenase, and bacterial binding to exfoliated epithelial cells. Ophthalmology. 2001;108:1279–1288.
3. Hashemi H, Asgari S, Emamian MH, Mehravaran S, Fotouhi A. Five year changes in central and peripheral corneal thickness: the shahroud eye cohort study. Cont Lens Anterior Eye. 2016;39(5):331–335. doi:10.1016/j.clae.2016.05.004
4. Rosenberg ME, Tervo TM, Immonen IJ, Muller LJ, Gronhagen-Riska C, Vesaluoma MH. Corneal structure and sensitivity in type 1 diabetes mellitus. Invest Ophthalmol Vis Sci. 2000;41(10):2915–2921.
5. Deinema LA, Vingrys AJ, Chinnery HR, Downie LE. Optical coherence tomography reveals changes to corneal reflectivity and thickness in individuals with tear hyperosmolarity. Transl Vis Sci Technol. 2017;6(3):6. doi:10.1167/tvst.6.3.6
6. Villani E, Galimberti D, Viola F, Mapelli C, Ratiglia R. The cornea in Sjogren’s syndrome: an in vivo confocal study. Invest Ophthalmol Vis Sci. 2007;48(5):2017–2022. doi:10.1167/iovs.06-1129
7. Pircher N, Schwarzhans F, Holzer S, et al. Distinguishing keratoconic eyes and healthy eyes using ultrahigh-resolution optical coherence tomography-based corneal epithelium thickness mapping. Am J Ophthalmol. 2018;189:47–54. doi:10.1016/j.ajo.2018.02.006
8. Li Y, Tan O, Brass R, Weiss JL, Huang D. Corneal epithelial thickness mapping by Fourier-domain optical coherence tomography in normal and keratoconic eyes. Ophthalmology. 2012;119(12):2425–2433. doi:10.1016/j.ophtha.2012.06.023
9. Li Y, Meisler DM, Tang M, et al. Keratoconus diagnosis with optical coherence tomography pachymetry mapping. Ophthalmology. 2008;115(12):2159–2166. doi:10.1016/j.ophtha.2008.08.004
10. Sng CC, Ang M, Barton K. Central corneal thickness in glaucoma. Curr Opin Ophthalmol. 2017;28(2):120–126. doi:10.1097/ICU.0000000000000335
11. Temstet C, Sandali O, Bouheraoua N, et al. Corneal epithelial thickness mapping using Fourier-domain optical coherence tomography for detection of form fruste keratoconus. J Cataract Refract Surg. 2015;41(4):812–820. doi:10.1016/j.jcrs.2014.06.043
12. Li Y, Netto MV, Shekhar R, Krueger RR, Huang D. A longitudinal study of LASIK flap and stromal thickness with high-speed optical coherence tomography. Ophthalmology. 2007;114(6):1124–1132. doi:10.1016/j.ophtha.2006.09.031
13. Fogagnolo P, Rossetti L, Mazzolani F, Orzalesi N. Circadian variations in central corneal thickness and intraocular pressure in patients with glaucoma. Br J Ophthalmol. 2006;90(1):24–28. doi:10.1136/bjo.2005.079285
14. Hashmani N, Hashmani S, Saad CM. Wide corneal epithelial mapping using an optical coherence tomography. Invest Ophthalmol Vis Sci. 2018;59(3):1652–1658. doi:10.1167/iovs.17-23717
15. Inomata T, Mashaghi A, Hong J, Nakao T, Dana R. Scaling and maintenance of corneal thickness during aging. PLoS One. 2017;12(10):e0185694. doi:10.1371/journal.pone.0185694
16. Yang Y, Hong J, Deng SX, Xu J. Age-related changes in human corneal epithelial thickness measured with anterior segment optical coherence tomography. Invest Ophthalmol Vis Sci. 2014;55(8):5032–5038. doi:10.1167/iovs.13-13831
17. Batawi H, Lollett IV, Maliakal C, et al. A comparative study of central corneal epithelial, stromal, and total thickness in males with and without primary open-angle glaucoma. Cornea. 2018;37(6):712–719. doi:10.1097/ICO.0000000000001575
18. Kim BJ, Ryu IH, Lee JH, Kim SW. Correlation of Sex and myopia with corneal epithelial and stromal thicknesses. Cornea. 2016;35(8):1078–1083. doi:10.1097/ICO.0000000000000850
19. Wang X, Dong J, Wu Q. Corneal thickness, epithelial thickness and axial length differences in normal and high myopia. BMC Ophthalmol. 2015;15:49. doi:10.1186/s12886-015-0039-6
20. Samy MM, Shaaban YM, Badran TAF. Age- and sex-related differences in corneal epithelial thickness measured with spectral domain anterior segment optical coherence tomography among Egyptians. Medicine. 2017;96(42):e8314. doi:10.1097/MD.0000000000008314
21. Kim BJ, Ryu IH, Kim SW. Age-related differences in corneal epithelial thickness measurements with anterior segment optical coherence tomography. Jpn J Ophthalmol. 2016;60(5):357–364. doi:10.1007/s10384-016-0457-x
22. Karaca Adiyeke S, Karaca I, Yildirim S, Adiyeke M, Uyar I, Ture G. Anterior segment findings in women with polycystic ovary syndrome. Turk J Ophthalmol. 2017;47(1):24–27. doi:10.4274/tjo.73659
23. Baser H, Cuhaci N, Topaloglu O, et al. Is there any association between primary hyperparathyroidism and ocular changes, such as central corneal thickness, retinal thickness, and intraocular pressure? Endocrine. 2016;51(3):545–550. doi:10.1007/s12020-015-0724-5
24. Prospero Ponce CM, Rocha KM, Smith SD, Krueger RR. Central and peripheral corneal thickness measured with optical coherence tomography, scheimpflug imaging, and ultrasound pachymetry in normal, keratoconus-suspect, and post-laser in situ keratomileusis eyes. J Cataract Refract Surg. 2009;35(6):1055–1062. doi:10.1016/j.jcrs.2009.01.022
25. Guilbert E, Saad A, Grise-Dulac A, Gatinel D. Corneal thickness, curvature, and elevation readings in normal corneas: combined placido-scheimpflug system versus combined placido-scanning-slit system. J Cataract Refract Surg. 2012;38(7):1198–1206. doi:10.1016/j.jcrs.2012.01.033
26. Gonzalez-Perez J, Queiruga Pineiro J, Sanchez Garcia A, Gonzalez Meijome JM. Comparison of central corneal thickness measured by standard ultrasound pachymetry, corneal topography, tono-pachymetry and anterior segment optical coherence tomography. Curr Eye Res. 2018 Jul;43(7):866–872.
27. Li HF, Petroll WM, Moller-Pedersen T, Maurer JK, Cavanagh HD, Jester JV. Epithelial and corneal thickness measurements by in vivo confocal microscopy through focusing (CMTF). Curr Eye Res. 1997;16(3):214–221.
28. Reinstein DZ, Archer TJ, Gobbe M, Silverman RH, Coleman DJ. Stromal thickness in the normal cornea: three-dimensional display with artemis very high-frequency digital ultrasound. J Refractive Surg. 2009;25(9):776–786. doi:10.3928/1081597X-20090813-04
29. Ruiz-Mesa R, Abengozar-Vela A, Ruiz-Santos M. Comparison of a new scheimpflug imaging combined with partial coherence interferometry biometer and a low-coherence reflectometry biometer. J Cataract Refract Surg. 2017;43(11):1406–1412. doi:10.1016/j.jcrs.2017.08.016
30. Maldonado MJ, Ruiz-Oblitas L, Munuera JM, Aliseda D, Garcia-Layana A, Moreno-Montanes J. Optical coherence tomography evaluation of the corneal cap and stromal bed features after laser in situ keratomileusis for high myopia and astigmatism. Ophthalmology. 2000;107(1):81–87. discussion 88.
31. Moller-Pedersen T, Vogel M, Li HF, Petroll WM, Cavanagh HD, Jester JV. Quantification of stromal thinning, epithelial thickness, and corneal haze after photorefractive keratectomy using in vivo confocal microscopy. Ophthalmology. 1997;104(3):360–368.
32. Li Y, Shekhar R, Huang D. Corneal pachymetry mapping with high-speed optical coherence tomography. Ophthalmology. 2006;113(5):792–799.e792. doi:10.1016/j.ophtha.2006.01.048
33. Cheng AC, Rao SK, Lau S, Leung CK, Lam DS. Central corneal thickness measurements by ultrasound, orbscan II, and visante OCT after LASIK for myopia. J Refractive Surg. 2008;24(4):361–365. doi:10.3928/1081597X-20080401-08
34. Mohamed S, Lee GK, Rao SK, et al. Repeatability and reproducibility of pachymetric mapping with Visante anterior segment-optical coherence tomography. Invest Ophthalmol Vis Sci. 2007;48(12):5499–5504. doi:10.1167/iovs.07-0591
35. Francoz M, Karamoko I, Baudouin C, Labbe A. Ocular surface epithelial thickness evaluation with spectral-domain optical coherence tomography. Invest Ophthalmol Vis Sci. 2011;52(12):9116–9123. doi:10.1167/iovs.11-7988
36. Rio-Cristobal A, Martin R. Corneal assessment technologies: current status. Surv Ophthalmol. 2014;59(6):599–614. doi:10.1016/j.survophthal.2014.05.001
37. Lee YW, Choi CY, Yoon GY. Comparison of dual rotating scheimpflug-placido, swept-source optical coherence tomography, and Placido-scanning-slit systems. J Cataract Refract Surg. 2015;41(5):1018–1029. doi:10.1016/j.jcrs.2014.08.040
38. Izatt JA, Hee MR, Swanson EA, et al. Micrometer-scale resolution imaging of the anterior eye in vivo with optical coherence tomography. Arch Ophthalmol. 1994;112(12):1584–1589.
39. Lim SH. Clinical applications of anterior segment optical coherence tomography. J Ophthalmol. 2015;2015:605729. doi:10.1155/2015/605729
40. Ang M, Baskaran M, Werkmeister RM, et al. Anterior segment optical coherence tomography. Prog Retin Eye Res. 2018. doi:10.1016/j.preteyeres.2018.04.002
41. Prakash G, Agarwal A, Jacob S, Kumar DA, Agarwal A, Banerjee R. Comparison of fourier-domain and time-domain optical coherence tomography for assessment of corneal thickness and intersession repeatability. Am J Ophthalmol. 2009;148(2):282–290.e282. doi:10.1016/j.ajo.2009.03.012
42. Galgauskas S, Juodkaite G, Tutkuviene J. Age-related changes in central corneal thickness in normal eyes among the adult Lithuanian population. Clin Interv Aging. 2014;9:1145–1151. doi:10.2147/CIA.S61790
43. Rush SW, Matulich J, Biskup J, Cofoid P, Rush RB. Corneal epithelial thickness measured by manual electronic caliper spectral domain optical coherence tomography: distributions and demographic correlations in preoperative refractive surgery patients. Asia Pac J Ophthalmol. 2016;5(2):147–150. doi:10.1097/APO.0000000000000166
44. Vijaya L, George R, Arvind H, et al. Central corneal thickness in adult south indians: the chennai glaucoma study. Ophthalmology. 2010;117(4):700–704. doi:10.1016/j.ophtha.2009.09.025
45. Ul Hassan M, Ur Rehman A, Abbas M, Fawad U, Bhatti N, Daud A. Relationship between central corneal thickness and intraocular pressure in selected Pakistani population. Pak J Ophthalmol. 2010;26(2):79–82.
46. Sanchis-Gimeno JA, Alonso L, Rahhal SM, Martinez-Soriano F. Gender differences in corneal thickness values. Eur J Anat. 2004;8(2):67–70.
47. Vollmer L, Sowka J, Pizzimenti J, Yu X. Central corneal thickness measurements obtained with anterior segment spectral domain optical coherence tomography compared to ultrasound pachymetry in healthy subjects. Optometry. 2012;83(5):167–172.
48. Erdur SK, Demirci G, Dikkaya F, Kocabora MS, Ozsutcu M. Comparison of central corneal thickness with ultrasound pachymetry, noncontact specular microscopy and spectral domain optical coherence tomography. Semin Ophthalmol. 2018;33(6):782–787. doi:10.1080/08820538.2018.1448091
49. Holden BA, Sweeney DF, Vannas A, Nilsson KT, Efron N. Effects of long-term extended contact lens wear on the human cornea. Invest Ophthalmol Vis Sci. 1985;26(11):1489–1501.
50. Aghaian E, Choe JE, Lin S, Stamper RL. Central corneal thickness of Caucasians, Chinese, Hispanics, Filipinos, African Americans, and Japanese in a glaucoma clinic. Ophthalmology. 2004;111(12):2211–2219. doi:10.1016/j.ophtha.2004.06.013
51. La Rosa FA, Gross RL, Orengo-Nania S. Central corneal thickness of Caucasians and African Americans in glaucomatous and nonglaucomatous populations. Arch Ophthalmol. 2001;119(1):23–27.
52. Mimouni M, Flores V, Shapira Y, et al. Correlation between central corneal thickness and myopia. Int Ophthalmol. 2018; 38(6): 2547–2551.
53. Reinstein DZ, Archer TJ, Gobbe M, Silverman RH, Coleman DJ. Epithelial thickness in the normal cornea: three-dimensional display with artemis very high-frequency digital ultrasound. J Refractive Surg. 2008;24(6):571–581. doi:10.3928/1081597X-20080601-05
54. Heur M, Costin B, Crowe S, et al. The value of keratometry and central corneal thickness measurements in the clinical diagnosis of marfan syndrome. Am J Ophthalmol. 2008;145(6):997–1001. doi:10.1016/j.ajo.2008.01.028
55. Giacomoni PU, Mammone T, Teri M. Gender-linked differences in human skin. J Dermatol Sci. 2009;55(3):144–149. doi:10.1016/j.jdermsci.2009.06.001
56. Sandby-Moller J, Poulsen T, Wulf HC. Epidermal thickness at different body sites: relationship to age, gender, pigmentation, blood content, skin type and smoking habits. Acta Derm Venereol. 2003;83(6):410–413. doi:10.1080/00015550310015419
57. McKay TB, Hjortdal J, Sejersen H, Asara JM, Wu J, Karamichos D. Endocrine and metabolic pathways linked to keratoconus: implications for the role of hormones in the stromal microenvironment. Sci Rep. 2016;6:25534. doi:10.1038/srep25534
58. Taichman et al. Data Sharing Statements for Clinical Trials – A Requirement of the International Committee of Medical Journal Editors. N Engl J Med. 2017;376:2277–2279.
Supplementary materials
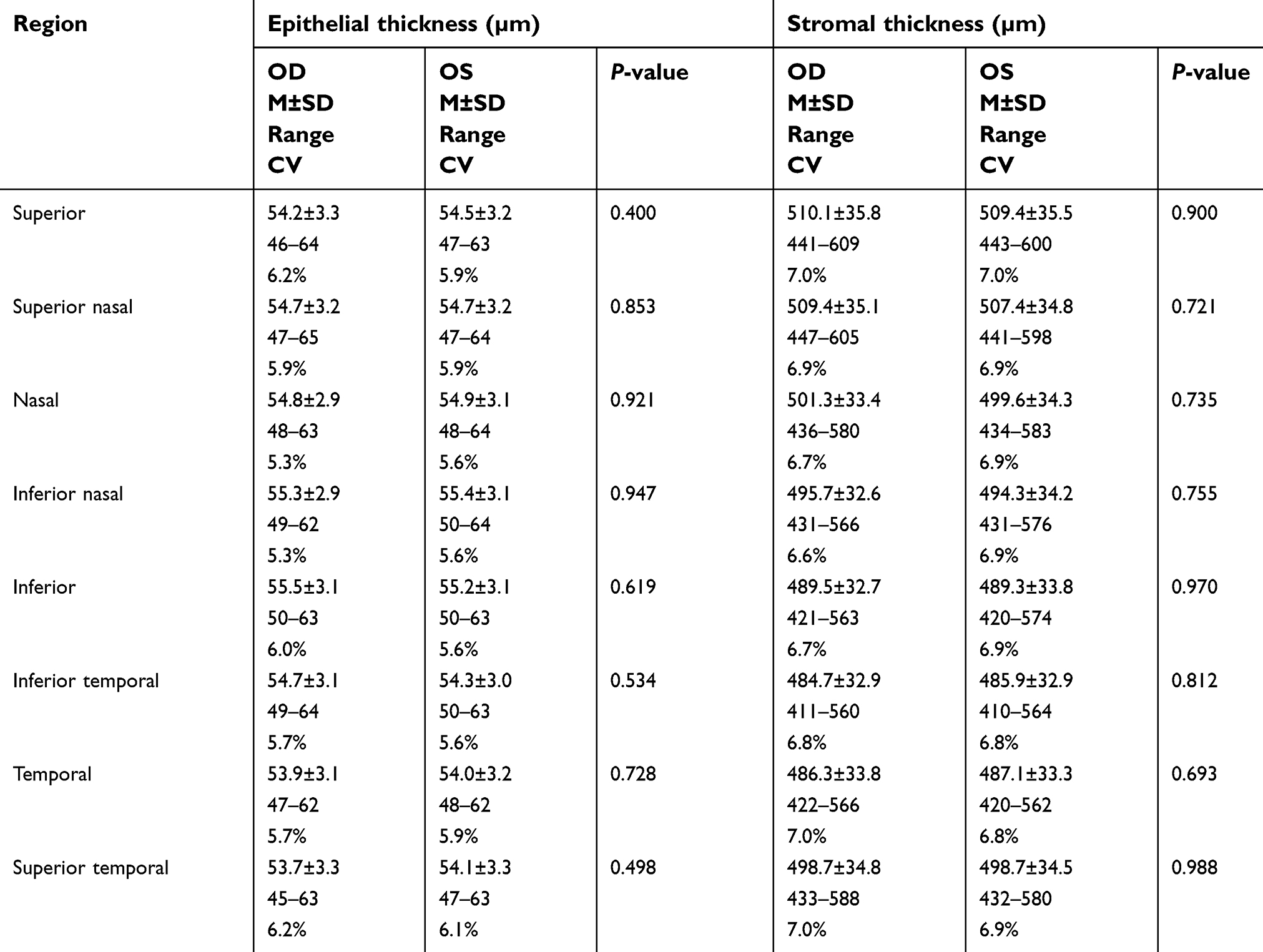 |
Table S1 Comparison of OD vs OS for all geographic regions within the 5 mm zone |
 |
Table S2 Comparison of OD vs OS for all geographic regions within the 6 mm zone |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.