Back to Journals » Clinical Ophthalmology » Volume 20
The Final Millimeter: A Single-Center Retrospective Analysis of an Integrated Pneumatic Microinjection System for Subretinal Gene Therapy
Authors Almeida DRP, Mahajan VB ![]()
Received 28 January 2026
Accepted for publication 30 April 2026
Published 21 May 2026 Volume 2026:20 595568
DOI https://doi.org/10.2147/OPTH.S595568
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Yousef Fouad
David RP Almeida,1,2 Vinit B Mahajan3
1Erie Retina Research, Erie, PA, USA; 2The Centers for Advanced Surgical Exploration (Casex), Erie, PA, USA; 3Molecular Surgery Laboratory, Byers Eye Institute, Stanford University, Palo Alto, CA, USA
Correspondence: David RP Almeida, Erie Retina Research, 2005 West 8th Street, Erie, PA, 16505, USA, Email [email protected]
Introduction
The transition from chronic disease management to curative genetic intervention represents a seismic shift in ophthalmology. However, the delivery mechanism for these therapies — manual subretinal injection — remains a significant bottleneck. The procedure demands that surgeons operate at the limits of physiological stability, where the margin of error (retinal thickness ~250 µm) is roughly equivalent to the amplitude of physiological hand tremor (~100 µm).1 Manual injection is further complicated by stiction (static friction) within the syringe, which can cause uncontrolled pressure spikes and lead to retinal pigment epithelium (RPE) damage, vector reflux, or iatrogenic retinal tears.2,3
Beyond clinical morbidity, the variability of manual subretinal injection carries an underappreciated economic dimension: a single complication that compromises therapeutic dosing can incur facility costs that exceed the marginal revenue of the index procedure.2 Quantifying the workflow and economic impact of standardized delivery platforms is therefore central to evaluating their broader adoption.4 To address these mechanical limitations, we evaluated the real-world clinical impact of the EVA INICIO™ Microinjection System (DORC International, Zuidland, Netherlands), an integrated pneumatic platform designed to standardize the final step of gene therapy delivery.
Methods
We conducted a retrospective analysis of 19 consecutive cases of subretinal vector-based therapy performed by a single surgeon (D.A.) using the EVA INICIO system between 1 October 2023 and 1 March 2024. These 19 cases represent the first 19 consecutive eyes treated with the INICIO system at our center; no cases were selected from a larger pool. The system replaces the assistant-driven manual syringe with foot-pedal-controlled, automated pneumatic injection (16 ± 1 psi) integrated directly into the EVA NEXUS™ vitrectomy console, with vector delivery actuated through DORC disposable subretinal injection cannulas.
Inclusion criteria for both the INICIO and historical manual cohorts were identical: all consecutive patients undergoing subretinal vector-based therapy by the senior surgeon (D.A.) within the respective study windows. No additional clinical or anatomical exclusions were applied to either group. Indications across both cohorts comprised inherited retinal dystrophies and other vector-amenable retinal pathologies; specific therapies included voretigene neparvovec for biallelic RPE65 mutation–associated retinal dystrophy and additional investigational AAV-mediated vectors administered under clinical trial or expanded access protocols.5 The historical manual cohort (n=18) underwent subretinal injection via a standard tuberculin syringe connected to a subretinal cannula, with vector delivery actuated by a second operator under verbal coordination from the surgeon, between January 2022 and September 2023.
Standard surgical steps — conjunctival peritomy, 25-gauge trocar placement, core vitrectomy, and posterior vitreous detachment induction — were performed identically in both cohorts. The procedures diverged at the moment of subretinal injection: in the manual cohort, an assistant manually depressed the syringe plunger under verbal coordination from the surgeon; in the INICIO cohort, the surgeon initiated foot-pedal-controlled pneumatic injection without a second operator.
Primary outcome metrics included total operating time (defined as time from first trocar insertion to completion of scleral wound closure), first-attempt subretinal bleb success rate, and the incidence of intraoperative or postoperative adverse events including retinal tears, hemorrhage, vector reflux, endophthalmitis, persistent hypotony, and ocular hypertension. Adverse events were prospectively recorded during surgery and at all postoperative visits per institutional protocol — Day 1, Week 1, Month 1, Month 3, and Month 6 examinations. Minimum follow-up duration was six months in both cohorts.
To support an unbiased safety assessment, all 19 INICIO surgical videos were independently reviewed by a second masked vitreoretinal surgeon (V.B.M)., who confirmed cannula stability, controlled rate of bleb formation, retinal integrity at and around the injection site, and absence of device-related adverse events. Mean operating times between cohorts were compared using an independent samples t-test (IBM SPSS Statistics version 30) after confirming assumptions of normality and homogeneity of variance; a p-value of <0.05 was considered statistically significant. Other outcomes are reported descriptively as means, standard deviations, and percentages.
Results
The introduction of the integrated pneumatic system was associated with a substantial reduction in total case duration. Mean operating time decreased from 42 minutes 45 seconds in the historical manual cohort to 27 minutes 9 seconds in the INICIO cohort, representing a 37% reduction (p<0.0001) (Figure 1). This 15-minute reduction per case has direct economic implications: at standard operating room costs of $60–$100 per minute, this translates to approximately $1,200 in direct OR savings per procedure.
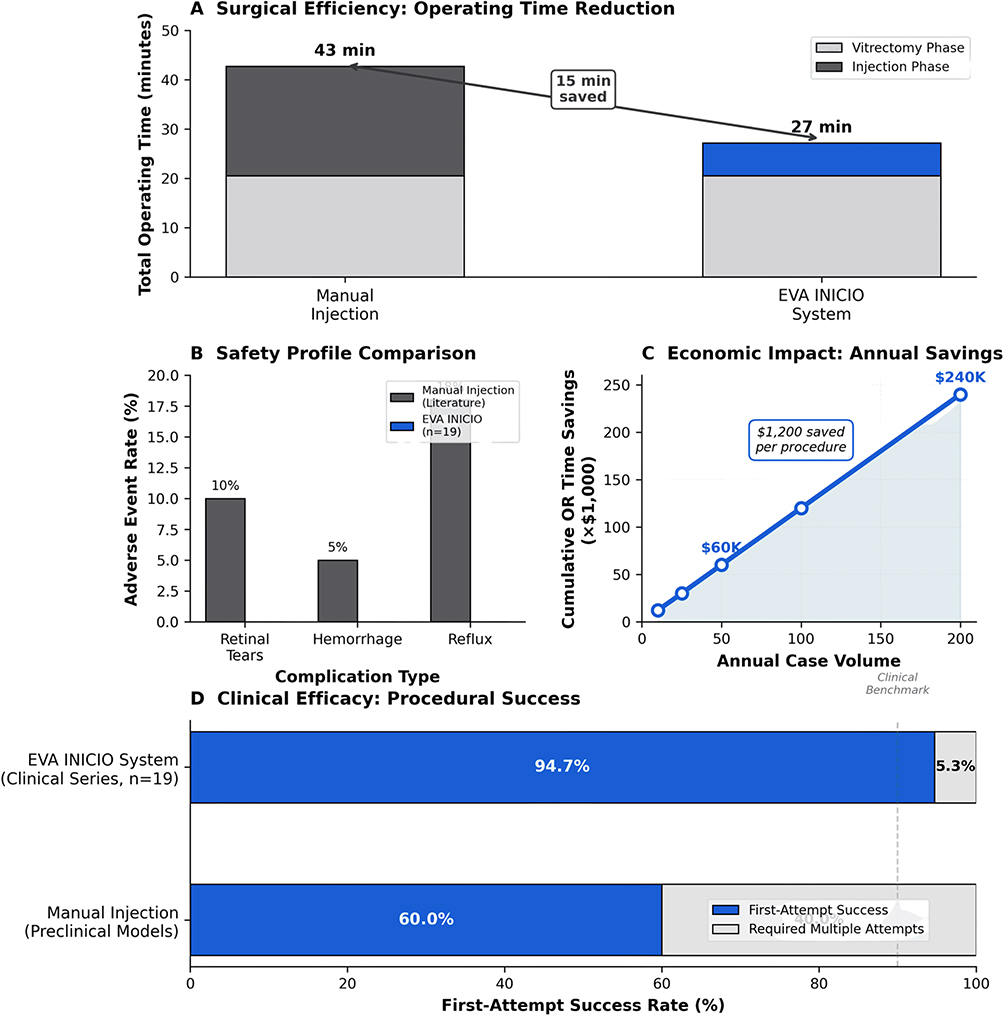 |
Figure 1 Clinical Impact of the EVA INICIO Microinjection System in Subretinal Gene Therapy. (A) Surgical Efficiency. Stacked bar chart comparing total operating time between the historical manual cohort (n=18) and the EVA INICIO cohort (n=19). The vitrectomy phase (light gray) was performed identically in both cohorts. The injection phase (dark gray for manual; blue for INICIO) accounts for the observed 15-minute reduction in mean operating time, from 42 minutes 45 seconds to 27 minutes 9 seconds (37% reduction, p<0.0001 by independent samples t-test). (B) Safety Profile. Bar chart comparing adverse event rates between manual subretinal injection (literature benchmark) and the present EVA INICIO cohort (n=19). Reported literature rates of retinal tears (≈10%), intraoperative hemorrhage (≈5%), and clinically significant vector reflux (≈15%) are contrasted with the absence (0%) of these events in the INICIO cohort over a minimum six-month follow-up window. No instances of endophthalmitis, persistent hypotony, or ocular hypertension were observed. Independent masked video review of all 19 INICIO cases by a second vitreoretinal surgeon (V.B.M.) corroborated appropriate handling of the delivery system and the absence of device-related adverse events. (C) Economic Impact. Illustrative projection of cumulative operating-room time savings as a function of annual case volume, derived from the observed 15-minute per-case reduction at standard operating-room costs of $60–$100 per minute (≈$1,200 in direct OR savings per procedure). Indicative cumulative savings reach approximately $60,000 at 50 cases and $240,000 at 200 cases annually. Projections assume linear scaling and are presented for illustrative purposes only; realized savings will vary by site cost structure, surgeon experience, and case mix. (D) Clinical Efficacy. Horizontal bar chart of first-attempt subretinal bleb success rates. In the present INICIO clinical series, 18 of 19 cases (94.7%) achieved successful bleb formation on the first attempt; the single second-attempt case required only minor cannula repositioning within the subretinal space, without removal of the cannula from the eye or complications. This is contrasted against a 60% first-attempt success rate reported in preclinical manual-injection models, providing a comparative benchmark for the technical reliability of the integrated pneumatic delivery system. Abbreviations: EVA INICIO, DORC EVA INICIO™ Microinjection System; OR, operating room; min, minutes; s, seconds. |
The system demonstrated high procedural reliability, achieving successful subretinal bleb formation on the first attempt in 18 of 19 cases (94.7%) (Figure 1). In the single case where the first attempt was not successful, the bleb was successfully created on a second attempt after minor repositioning of the cannula tip within the subretinal space, without removal from the eye and without complication.
Regarding safety, no intraoperative or postoperative adverse events — including retinal tears, hemorrhage, clinically significant vector reflux, endophthalmitis, persistent hypotony, or ocular hypertension — were observed in the 19 INICIO cases over the minimum six-month follow-up window. The historical manual cohort similarly demonstrated no adverse events over a comparable follow-up period, indicating that both delivery techniques can be performed safely in experienced hands. Independent masked video review of all 19 INICIO cases by V.B.M. corroborated the absence of device-related adverse events and confirmed appropriate handling of the delivery system, including stability of the cannula during injection and a controlled rate of bleb formation.
Discussion
The principal finding of this preliminary series is that an integrated pneumatic microinjection system was associated with a 37% reduction in operating time for subretinal vector-based therapy, with maintained safety relative to the surgeon’s historical manual baseline and a high first-attempt bleb success rate. While safety appears comparable between platforms in this experienced-surgeon setting, the consistency and predictability of pneumatic delivery may carry particular value as gene therapy expands beyond ultra-specialized centers.
Mechanistically, the EVA INICIO system replaces the high-stiction interface of a manual hand-driven syringe with a closed-loop pneumatic regulator integrated into the vitrectomy console. Foot-pedal activation delivers a pre-calibrated 16 ± 1 psi to the injection cannula via a regulated pressure circuit, eliminating the static-friction breakaway force that produces the uncontrolled fluid jets characteristic of manual systems. The result is a smooth, repeatable flow profile that is independent of operator hand strength or assistant technique — properties that may translate, in principle, into the consistent bleb formation and absence of RPE injury observed here.
Recent in-human work by De Clerck et al demonstrated feasibility of subretinal injection through attached retina using a robotic comanipulation platform, complementing the present findings on automated pneumatic delivery.6 Together, these emerging platforms point to a broader trend toward standardization of the final delivery step in retinal gene therapy, addressing variability from different angles — robotic motion control on one hand, and pneumatic pressure regulation on the other.
The economic dimension warrants brief comment. At standard operating room costs of $60–$100 per minute, the observed 15-minute reduction translates to approximately $1,200 in direct OR savings per procedure.7 This figure represents a per-case calculation only; we have intentionally avoided extrapolation to higher annual case volumes given the absence of supporting data on whether time savings scale linearly across surgeons or sites.
Selection considerations for the platform include posterior vitreous detachment status, target lesion accessibility, absence of significant subretinal fibrosis or tractional membranes that could preclude smooth bleb propagation, and adequate vitreous-base shaving to permit a stable subretinal cannula approach. The system’s automated pressure profile may be particularly advantageous in cases with thin or atrophic retina, where manual stiction-driven pressure spikes pose the greatest risk. Furthermore, the absence of any intra-cohort performance gradient across the first 19 consecutive INICIO cases suggests that the system’s standardized pressure profile may reduce the dependence of outcomes on accumulated case experience, with potential implications for adoption beyond ultra-specialized centers.
Study Limitations
This study has several limitations. The sample size of 19 cases, while demonstrating proof of concept, limits the statistical power to detect rare adverse events. The single-surgeon, single-center design may limit generalizability across different practice settings and levels of surgeon experience. Use of a historical, non-concurrent control cohort introduces potential confounding from evolving surgical practice over time, and structured demographic data collection differed between cohorts in this retrospective design, precluding formal demographic comparison. Longer-term follow-up data are needed to assess durability of therapeutic efficacy and late-presenting complications. Larger prospective multicenter studies with concurrent controls and extended follow-up are warranted to validate these findings and establish the platform’s performance across a broader range of surgeons, patient populations, and vector types.
Conclusion
In this single-center retrospective series, the EVA INICIO system was associated with substantially reduced operative time and a favorable safety profile in subretinal gene therapy delivery, with safety comparable to the surgeon’s historical manual baseline. By standardizing pressure control and reducing dependence on assistant-driven manual injection, this platform may improve procedural reliability and broaden access to gene therapy beyond ultra-specialized academic centers. Larger prospective multicenter studies are required to confirm these findings and to define optimal patient selection.
Data Sharing Statement
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request, subject to institutional privacy policies.
Ethics Statement
This manuscript is a Research Letter presenting a retrospective analysis of clinical outcomes and does not constitute a prospective interventional trial. The study was conducted in accordance with the Declaration of Helsinki. As the data analyzed were retrospective and fully de-identified, the Research Ethics Committee of Erie Retina Research (Erie, Pennsylvania, USA) reviewed the protocol and determined that the work is exempt from formal IRB oversight and that informed consent was not required.
Disclosure
David R.P. Almeida has served as a consultant/advisor and received research support/grants from Dutch Ophthalmics (DORC), the manufacturer of the EVA INICIO™ Microinjection System evaluated in this study. The funder had no role in the design of the study, in the collection, analysis, or interpretation of data, in the writing of the manuscript, or in the decision to publish the results. Vinit B. Mahajan declares no conflicts of interest related to this work.
References
1. Elble RJ. Characteristics of physiologic tremor in young and elderly adults. Clin Neurophysiol. 2003;114(4):624–5. doi:10.1016/s1388-2457(03)00006-3
2. Peng Y, Tang L, Zhou Y. Subretinal injection: a review on the technique and its associated complications. Ophthalmol Ther. 2023.
3. Ehlers JP, Petkovsek DS, Yuan A, et al. Intrasurgical assessment of subretinal tPA injection for submacular hemorrhage in the PIONEER study utilizing intraoperative OCT. Ophthalmic Surg Lasers Imaging Retina. 2015;46(3):327–332. doi:10.3928/23258160-20150323-05
4. American Society of Retina Specialists. The Economics of Emergency Retinal Surgery and Declining Access to Care; 2025.
5. Maguire AM, Russell S, Wellman JA, et al. Efficacy, safety, and durability of voretigene neparvovec-rzyl in RPE65 mutation-associated inherited retinal dystrophy. Ophthalmology. 2019;126(9):1273–1285. doi:10.1016/j.ophtha.2019.06.017
6. De Clerck I, Schoovaerts M, Polidoro M, Ourak M, Poorten EV, Stalmans P. In-human feasibility and safety of subretinal drug injection through attached retina using a robotic comanipulation system. Retina. 2025. doi:10.1097/IAE.0000000000004745
7. Ciulla TA, Williams DF. Opportunity costs of vitreoretinal surgical referrals at a tertiary care center. Invest Ophthalmol Vis Sci. 2023.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.