Back to Journals » Clinical Ophthalmology » Volume 20
The Efficacy and Safety of Nanoparticle-Based Clobetasol Propionate in Managing the Inflammation and Pain in Post-Operative Cataract Patients: A Systematic Review and Meta-Analysis
Authors Alamoudi A ![]() , Aldahlawi AK
, Aldahlawi AK ![]() , Almufarriji N
, Almufarriji N ![]() , Alsudais AS, Alharbi BJ, Alomari BKA, Alghamdi AM, Alshehri OA, Aldayel AA
, Alsudais AS, Alharbi BJ, Alomari BKA, Alghamdi AM, Alshehri OA, Aldayel AA
Received 2 May 2025
Accepted for publication 14 November 2025
Published 6 January 2026 Volume 2026:20 535477
DOI https://doi.org/10.2147/OPTH.S535477
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Bharat Gurnani
Anas Alamoudi,1 Abdulaziz Khalid Aldahlawi,2 Naif Almufarriji,1 Ali Saleh Alsudais,3,4 Bandar J Alharbi,5 Basil Khalid A Alomari,3,4 Amer M Alghamdi,6 Omar A Alshehri,1,7 Ahmed Abdullah Aldayel7
1Department of Ophthalmology, Jeddah Eye Hospital, Jeddah, Saudi Arabia; 2Department of Emergency, King Faisal Complex Hospital, Taif, Saudi Arabia; 3College of Medicine, King Saud bin Abdulaziz University for Health Sciences, Jeddah, Saudi Arabia; 4King Abdullah International Medical Research Center, Jeddah, Saudi Arabia; 5Ophthalmology Department, Hera General Hospital, Makkah, Saudi Arabia; 6Department of Ophthalmology, College of Medicine, King Saud University, Riyadh, Saudi Arabia; 7Anterior Segment Department, King Khaled Eye Specialist Hospital, Riyadh, Saudi Arabia
Correspondence: Anas Alamoudi, Department of Ophthalmology, Jeddah Eye Hospital, Jeddah, Saudi Arabia, Email [email protected]
Background: Nanotechnology-based drug delivery systems are emerging as promising solutions for ocular diseases by improving bioavailability and therapeutic effectiveness. This systematic review and meta-analysis evaluated the efficacy and safety of nanoparticle-based clobetasol propionate (CP) in managing inflammation and pain following cataract surgery.
Methods: A comprehensive search across multiple databases identified five randomized controlled trials (RCTs) with a total of 1306 participants. Outcomes measured were anterior chamber cell (ACC) grade, anterior chamber flare (ACF) grade, ocular pain scores, and adverse events. Meta-analysis was conducted using RevMan 5.4.1.
Results: Meta-analysis demonstrated significant efficacy of CP in achieving an ACC grade of zero at both 8 days (RR = 2.30, 95% CI [1.81, 2.92], p < 0.00001) and 15 days (RR = 3.06, 95% CI [2.29, 4.09], p < 0.00001), and in reducing ACF grades (RR = 1.87 at day 8; RR = 2.30 at day 15, both p < 0.0001). Pain reduction was significantly superior in the CP group at both intervals (RR = 1.73 day 8; RR = 1.77 day 15, both p < 0.00001). The safety profile of CP showed a marginal trend toward fewer adverse events compared to placebo, but without statistical significance (RR = 0.50, 95% CI [0.24, 1.04], p = 0.06).
Conclusion: In summary, nanoparticle-based clobetasol propionate is an effective and well-tolerated drug for managing postoperative inflammation and pain in cataract patients.
Keywords: nanotechnology, clobetasol propionate, cataract surgery, inflammation, meta-analysis
Introduction
Nanotechnology-based drug delivery systems are emerging as promising alternatives to conventional ocular drug delivery methods for treating anterior segment eye diseases, including cataracts, glaucoma, dry eye syndrome, and inflammatory diseases, among others.1 The use of nanotechnology in ocular drug delivery offers several advantages, such as improved bioavailability, overcoming barriers, enhanced drug penetration, reduced dosing frequency, lower toxicity and side effects, and long shelf life.1,2 The complex drug delivery barrier in the eye, which includes the corneal and conjunctival barriers, reduces the bioavailability of many drugs, resulting in poor therapeutic effects.3 Nanotechnology-based delivery systems can overcome these barriers, thereby enhancing the effectiveness of treatment. Several nano formulations of drugs are currently under clinical trials or have already been approved for use in ophthalmology in preclinical and clinical trials.4 These advanced delivery systems offer improved drug bioavailability, targeted drug delivery, and reduced side effects, making them a promising alternative to conventional ocular drug delivery methods.3 As research and development continue, it is expected that more innovative nanotechnology-based ocular drug delivery systems will be developed to improve the treatment of anterior segment eye diseases.
Post-operative inflammation and pain are common concerns in cataract surgery. Inflammation can result from the breakdown of the blood-aqueous barrier, leading to an inflammatory state, which is usually well-controlled with topical steroid tapers and NSAIDs.5 Clobetasol propionate is a synthetic corticosteroid, which is a potent anti-inflammatory, antipruritic, and vasoconstrictive agent that has been suggested for the management of inflammation and pain in post-operative cataract patients.6 Studies have shown that clobetasol propionate ophthalmic nanoemulsion, 0.05%, may be safe, effective, and well-tolerated in reducing inflammation and pain associated with cataract surgery.7 The nanoemulsion is formulated to improve the bioavailability and effectiveness of the drug while minimizing potential side effects. This systematic review and meta-analysis aimed to comprehensively describe the efficacy and safety of nanoparticle-based clobetasol propionate in managing inflammation and pain in post-operative cataract patients.
Materials and Methods
Methods
This systematic review and meta-analysis adhered to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines and the Cochrane Handbook for Systematic Reviews of Interventions to ensure methodological rigor and transparency.8,9 Before data collection, the study protocol was prospectively registered on PROSPERO (CRD42023464582).
Eligibility Criteria
Randomized controlled trials (RCTs) were included if they evaluated nanoparticle-based clobetasol propionate formulations for managing postoperative outcomes in adults (≥18 years) undergoing cataract surgery, with eligible comparators including placebo, vehicle control, or non-intervention (standard care). Studies were required to report quantitative measures of predefined efficacy and safety endpoints.
The primary endpoints were postoperative ocular inflammation severity, measured by anterior chamber cell grade. Postoperative pain intensity assessed using validated pain scales including the Visual Analog Scale. Secondary endpoints included: safety outcomes comprising intraocular pressure (IOP) changes from baseline, incidence and severity of adverse events (both local and systemic), and treatment-related complications.
Studies published in any language were eligible for inclusion, with non-English articles translated as needed. Exclusion criteria comprised: non-randomized study designs (observational studies, case series, case reports); grey literature including conference abstracts, editorials, commentaries, and letters; studies with duplicate or overlapping patient populations; studies involving pediatric populations (age < 18 years) or non-cataract surgical procedures; and studies with inaccessible full-text manuscripts despite author contact attempts.
Information Sources and Search Strategy
A comprehensive search was conducted in Clinicaltrials.gov, EMBASE, PubMed, and the Directory of Open Access Journals from inception to February 1, 2025. Search terms combined keywords related to cataract surgery (eg, “cataract” “phacoemulsification”) and clobetasol (eg, “clobetasol propionate”). Manual searches of Google Scholar, reference lists of included studies, and other clinical trial registries (CENTRAL, WHO ICTRP) supplemented database results.
Screening and Data Extraction
Two independent reviewers screened titles/abstracts using Rayyan software,10 followed by full-text assessment of potentially eligible studies. Discrepancies were resolved through discussion or consultation with a third reviewer. Data extraction utilized a standardized Excel sheet to capture study characteristics (author, year, design, country), participant demographics, intervention details, and outcomes. Missing data were requested from the corresponding authors.
Statistical Analysis and Quality Assessment
Analyses were performed using Review Manager (RevMan 5.4). Primary outcomes included mean differences (MD) in inflammation scores and pain reduction pooled using inverse-variance with 95% confidence intervals (CI). Heterogeneity was evaluated via Cochran’s Q-test and I2 statistics, with I2 > 50% or p < 0.10 prompting random-effects models; otherwise, fixed-effects models were applied. For studies reporting pre- and post-treatment means without change scores, standard deviations were imputed using a correlation coefficient of 0.5, as per Cochrane’s recommendations. Subgroup analyses explored the days of assessment 8 and 15 days. A p-value <0.05 denoted statistical significance. Publication bias was not assessed due to a limited number of studies and included studies not being published articles themselves.
Our outcomes included the risk of Anterior chamber cell (ACC) grade of zero, Anterior chamber flare (ACF) grade of zero, percentage of pain scores of zero indicative no ocular pain and any adverse events. The number of cells in the anterior chamber of the eye are counted and graded for each number of cells in a 1 mm × 1 mm area. ACC Grade 0 = 0 cells, ACC grade 1 = 1–5 cells, ACC grade 2 = 6–15 cells, ACC grade 3 = 16–30 cells, ACC grade 4 = >30 cells in studies. The degree of turbidity (flare) in the anterior chamber of the eye is quantified on a five-point (0–4) anterior chamber flare grade scale (0 = none; 4 = Intense). We aimed to assess ACC or ACF grades of zero as indicative of reduced inflammation.
The quality of the included studies was assessed using the risk of bias 2 tool (RoB-2) by Cochrane.11 This tool assesses studies’ quality based on five domains (1) randomization, (2) deviations from intended interventions, (3) missing outcome data, (4) measurement of the outcome, and (5) selection of the reported result to categorize studies into low, some concerns and high risk of bias. In addition, the overall quality of evidence and the strength of recommendations for each outcome were assessed using the GRADE framework. This method takes into account aspects such as risk of bias, inconsistency, indirectness, imprecision, and publication bias, and it categorizes confidence in the estimates into four levels: high, moderate, low, or very low.12
Results
Selection Process and Characteristics of the Included Studies
Out of initially 1361 retrieved records, we identified 147 duplicates that were removed by Endnote software. Following that, 1214 reports underwent abstract screening; of them, only 5 trials were eligible for full-text screening and eventually included in our study (see Figure 1).
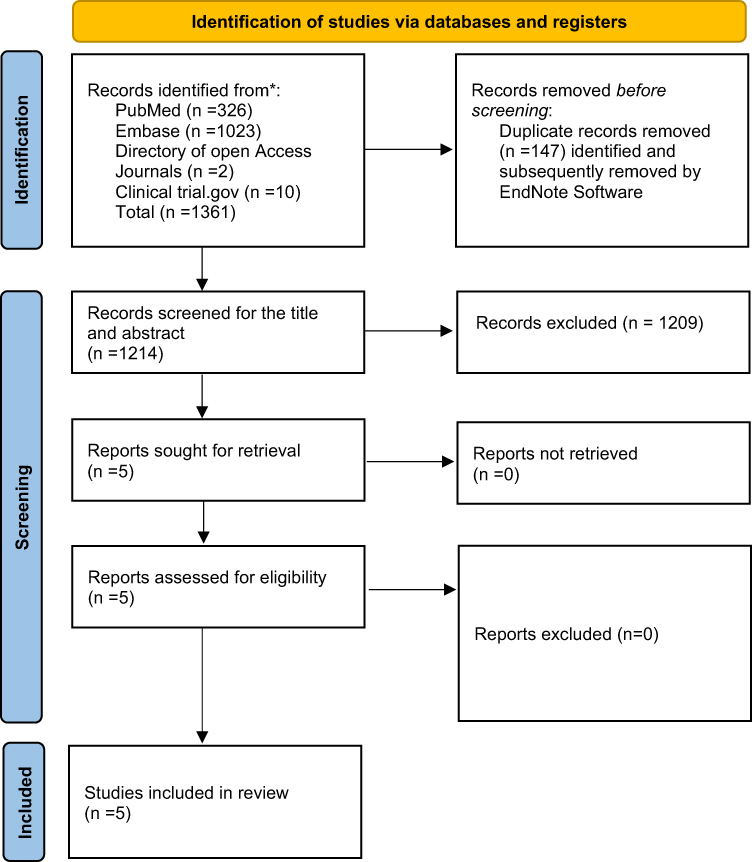 |
Figure 1 PRISMA flow diagram of the selection process. Notes: PRISMA figure adapted from Page MJ, McKenzie JE, Bossuyt PM et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. Creative Commons.8 |
The systematic review includes five double blinded RCTs (NCT04246801, NCT04249076, NCT04810962, NCT04739709, NCT04089735) that evaluated the efficacy of clobetasol propionate 0.05% versus placebo in patients undergoing cataract surgery. All of the five included trials were unpublished trials registered in clincaltrails.gov. The trials varied in follow-up duration from as early as Day 4 to as late as Day 22, with most assessments occurring around Day 8 and Day 15. Sample sizes for the clobetasol groups ranged from 66 to 185 patients, while placebo groups included between 66 and 197 patients, with a total sample size of 1306 participants. Across studies, the patient populations were comparable, with a mean age consistently in the high 60s (approximately 67–68 years) and a relatively balanced gender distribution. For further details, see Table 1. The risk of bias assessment revealed that 3 studies had an overall low risk of bias, while 2 studies had some concerns regarding their risk of bias deriving from the measurement of outcomes (Figure 2).
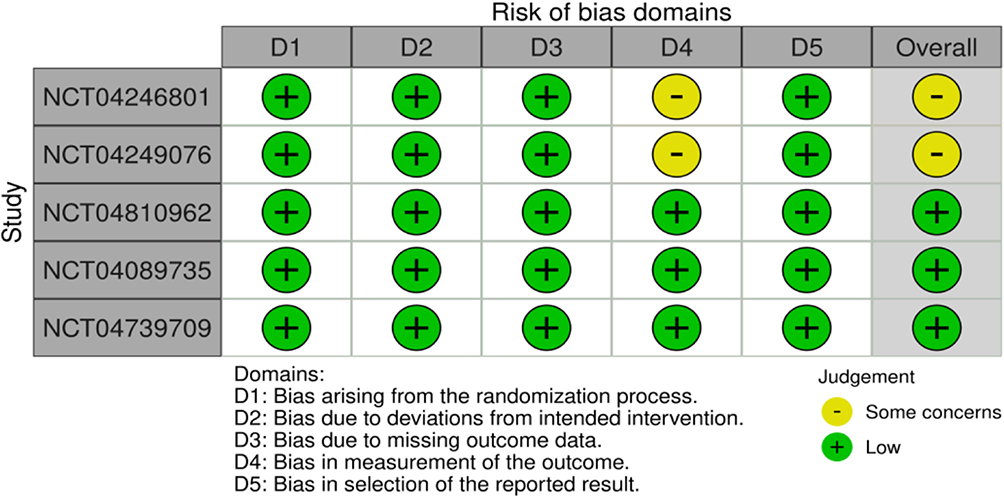 |
Figure 2 Risk of bias assessment using RoB-2. |
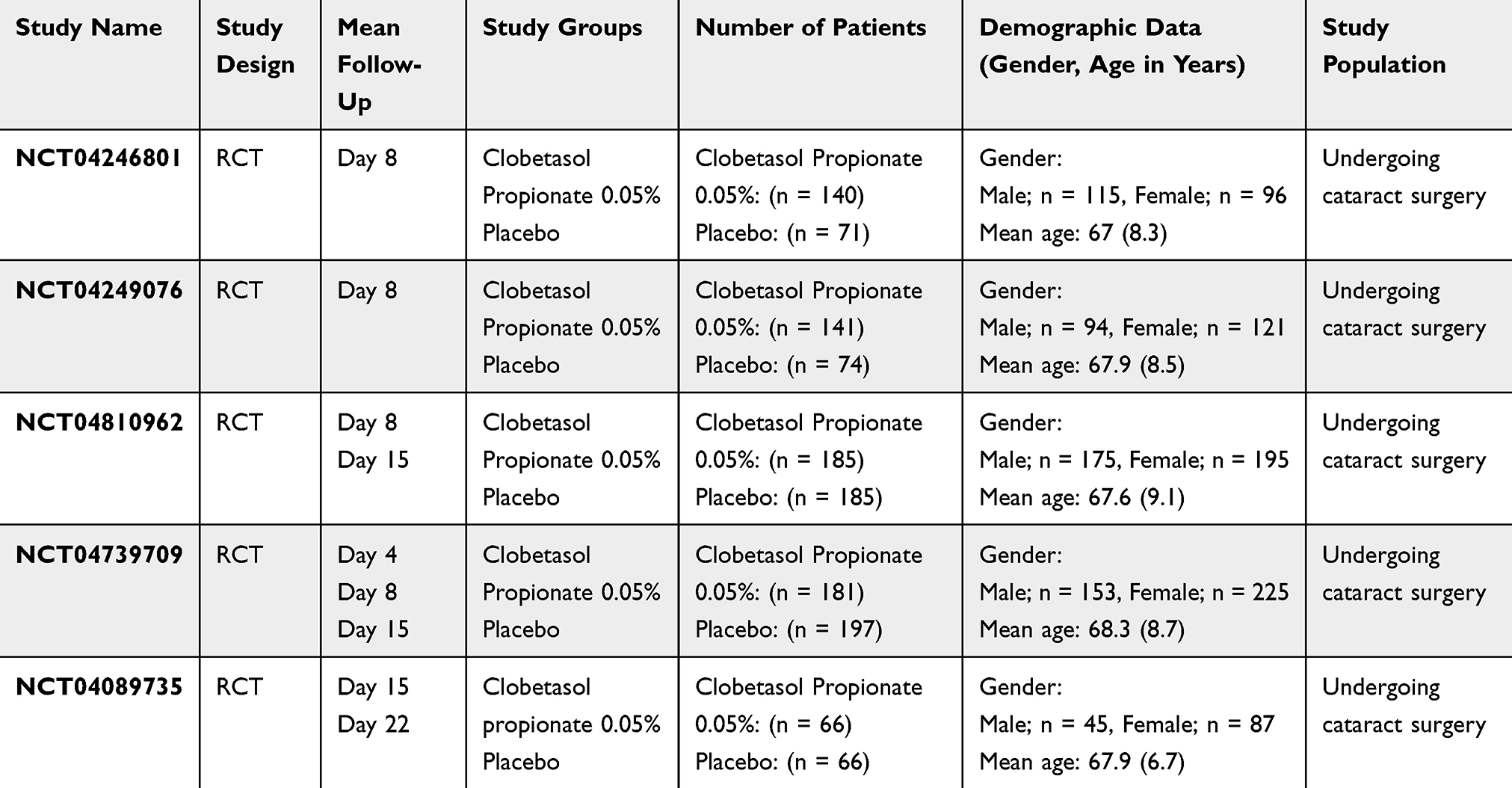 |
Table 1 Characteristics of Included Trials |
Meta-Analysis of Anterior Chamber Cells Grade (ACC)
Four RCTs reported ACC grade 0 on POD 8 and three RCTs on POD 15 as an outcome. At 8 days after surgery, the Clobetasol Propionate (CP) group showed better efficacy than the Vehicle group (RR = 2.30, 95% CI [1.81, 2.92], P = <0.00001, I2 = 0%). Similarly, at 15 days, the CP group showed good efficacy compared to Vehicle (RR = 3.06, 95% CI [2.29, 4.09], P = <0.00001, I2 = 36%). The test of subgroup differences was not significant (P = 0.13) (Figure 3).
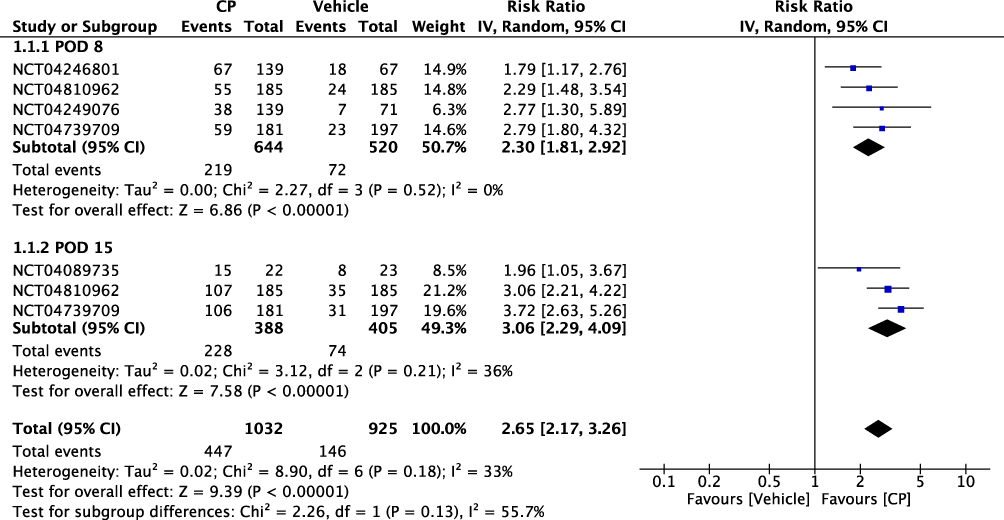 |
Figure 3 Forest Plot of Anterior Chamber Cells (ACC). |
Meta-Analysis of Anterior Chamber Flare Grade
Two RCTs reported ACF grade as an outcome with 748 participants. Both days 8 (RR = 1.87, 95% CI [1.57, 2.23], P = <0.00001, I2 = 49%) and 15 (RR = 2.30, 95% CI [1.75, 2.46], P = <0.0001, I2 = 75%) showed significant improvement of ACF in the CP group compared to the control group and there was no significant difference between them (P = 0.21) (Figure 4).
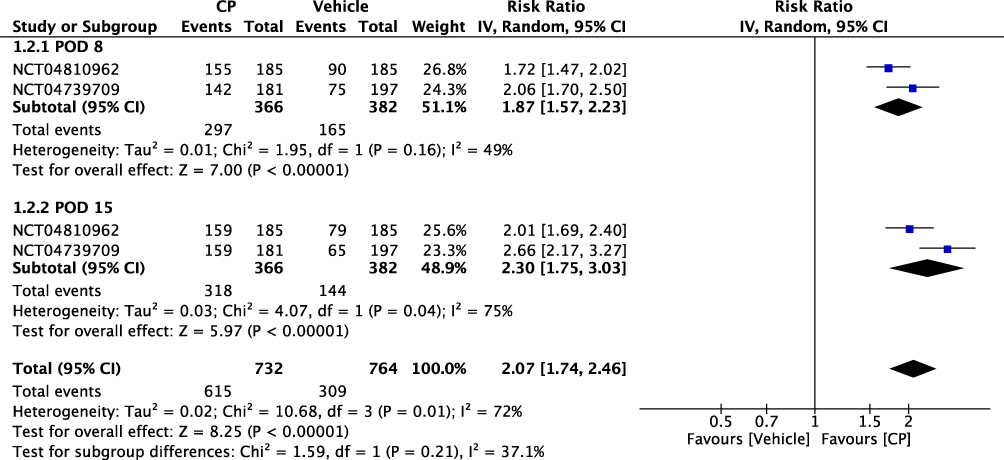 |
Figure 4 Forest Plot of Anterior Chamber Flare (ACF). |
Meta-Analysis of Pain Scores Grade
Five RCTs reported a percentage of participants with an ocular pain score of “0” on POD 8 and three RCTs on POD 15. On POD 8, CP showed significant improvement in levels of pain (RR = 1.73, 95% CI [1.39, 2.15], P = <0.00001, I2 = 70%) compared to the vehicle group, and on POD 15 (RR = 1.77, 95% CI [1.41, 2.21], P = <0.00001, I2 = 74%). The test of subgroup differences showed no significant difference (P = 0.89) (Figure 5).
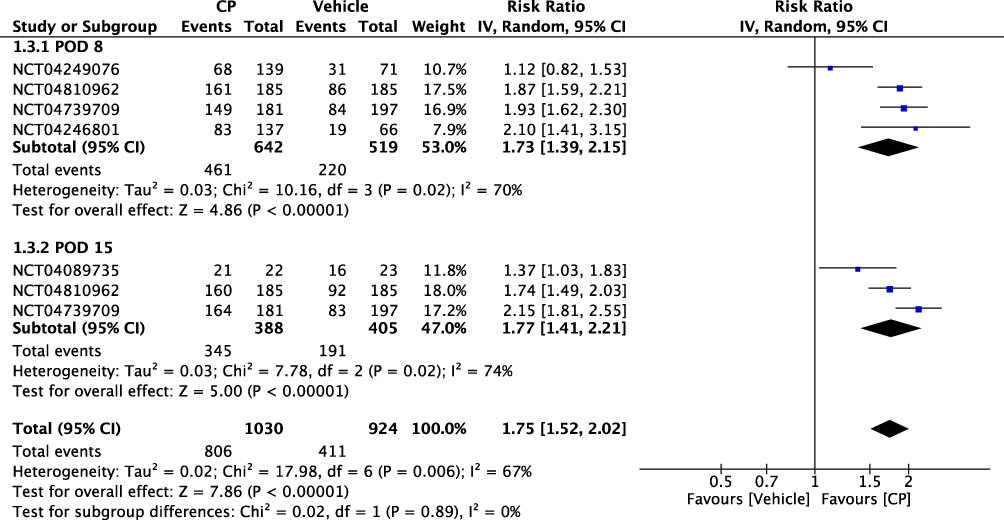 |
Figure 5 Forest Plot of Pain Scores. |
Meta-Analysis of Adverse Effects
Five RCTs reported adverse events, with a total of 1218 patients. Compared to the placebo group, the CP group had no significant adverse events (RR = 0.50, 95% CI [0.24, 1.04], P = 0.06, I2 = 61%) with a marginal trend of fewer adverse events than the control group (Figure 6).
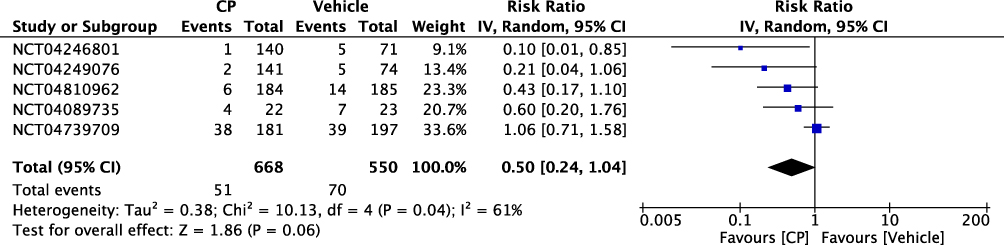 |
Figure 6 Forest plot of adverse events. |
Certainty of Outcomes Using GRADE
The certainty of evidence was evaluated using the GRADE framework. The certainty of evidence for ACC and ACF outcomes was assessed as very low due to significant concerns about the risk of bias and inconsistency across studies. The certainty regarding pain outcomes was low, primarily due to serious inconsistency and risk of bias concerns. The certainty assessment for adverse events could not be conclusively rated due to insufficient available data and methodological variability, see Table 2.
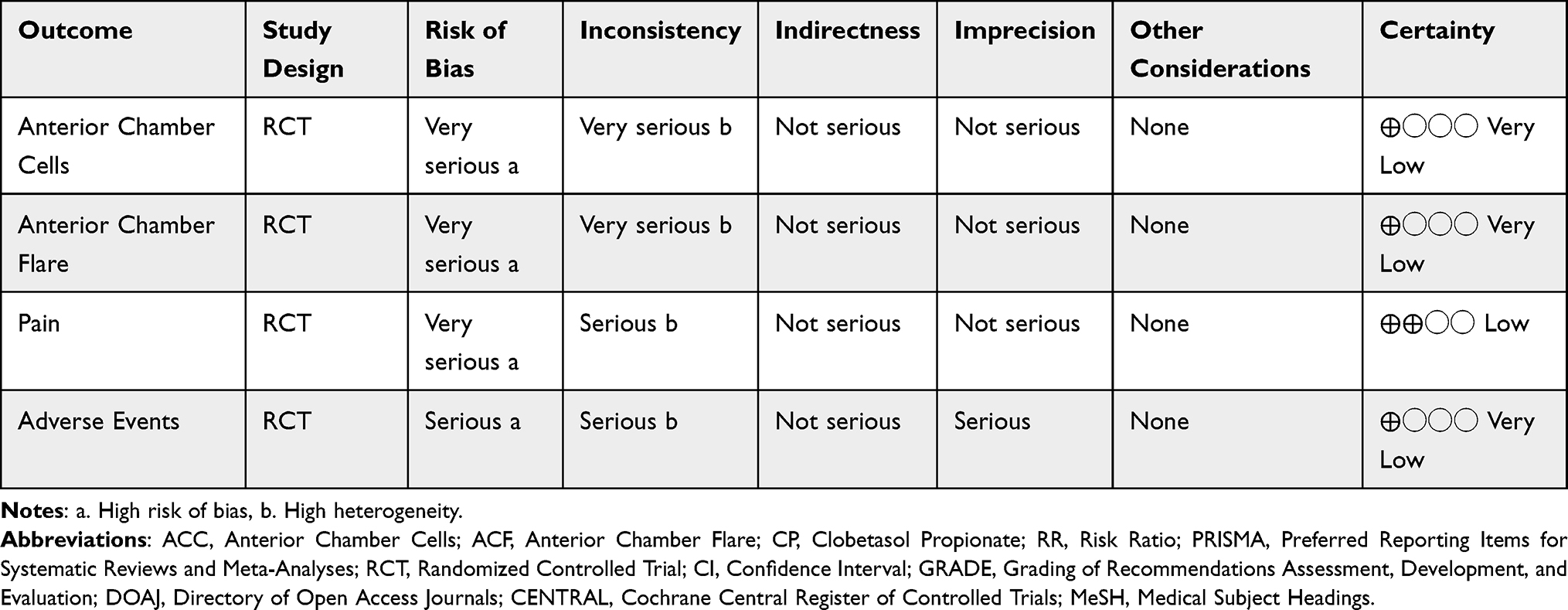 |
Table 2 Certainty Assessment Table Using GRADE |
Discussion
This is the first systematic review and meta-analysis summarizing the available evidence on nanoparticle-based CP in managing inflammation and pain post-cataract surgery. The pooled analyses from five RCTs involving around 1306 participants indicate that CP significantly improves the resolution of ACC and ACF at both 8-day and 15-day postoperative intervals compared to placebo, indicating improved inflammation post-operatively. Additionally, CP showed considerable efficacy in reducing ocular pain scores significantly at these same intervals. The safety profile of nanoparticle-based CP was promising, indicating fewer adverse events than the placebo group, although this difference was not statistically significant. The enhanced effectiveness of CP aligns with the theoretical benefits of nanoparticle-based drug delivery, such as increased bioavailability, improved drug penetration through ocular barriers, and sustained drug release.13
The commonest side effects of cataract surgeries are pain and inflammation causing uveitis, secondary glaucoma, and macular edema, which are still concerning even after the development of minimally invasive procedures.14 The current management strategies of post-cataract operations inflammation include the use of non-steroidal anti-inflammatory drugs (NSAIDs) (Bromfenac, Diclofenac, Ketorolac, etc.) and steroids (prednisolone, dexamethasone, fluorometholone) with inconsistent evidence and no conclusive guidelines.15 A combination of both NSAIDs and steroids is usually used and advised to prevent post-operative inflammation.5,15 The topical administration of steroids as a suspension remains the most common route for anterior segment ocular drug delivery due to its simplicity, convenience, and non-invasive nature. However, its efficacy is significantly constrained by the ocular barriers, including rapid tear clearance, nasolacrimal drainage, and the multi-layered corneal structure.16 Tear film rapidly removes drugs from the ocular surface, significantly reducing bioavailability. Nanoparticle-based formulations address these issues by enhancing corneal penetration, prolonging drug retention, and overcoming rapid clearance by tears, leading to improved bioavailability and clinical efficacy.17 Clobetasol propionate in its recent formulation as an ophthalmic nanoemulsion 0.05% was recently approved by the FDA for treating pain and inflammation post-ocular surgeries. It is originally one of the most potent topical steroids usually preserved for severe cases of atopic dermatitis, psoriasis, and other skin conditions.6 It is now available in a regimen of twice daily for 14 days without tapering for post-ocular surgeries inflammation, and it is the first new steroid formulation for post-ocular surgeries in over 15 years. Although its FDA approval was based on clinical trials, this is the first meta-analysis to pool evidence from all its clinical trials.
Considerable statistical heterogeneity was observed across the included studies, particularly in the assessment timings and outcome measurements. Although we did not conduct a sensitivity analysis due to a limited number of studies, concerns can be mitigated by the fact that most of the studies’ individual findings supported the efficacy of CP. Another critical aspect of this review is the evaluation of minimal clinically important differences (MCIDs) for inflammation and pain outcomes. Although statistically significant, the clinical relevance of these findings warrants careful consideration. The choice of outcomes in this review reflects commonly accepted clinical practice standards for evaluating postoperative inflammation and pain in cataract surgery. ACC and ACF grades are widely adopted markers due to their objective measurability and direct correlation with clinical inflammatory status.18 However, measurement of these outcomes through Slit-lamp (which was reported in most studies) can be subjective, limited by Interobserver variability while other objective techniques like Laser flare and cell photometry, Anterior segment fluorophotometry, and optical coherence tomography provide more objective measurements.18 Pain scores similarly represent crucial patient-centered outcomes, reflecting the subjective burden of postoperative recovery. Additionally, the concentration on dichotomizing the outcomes and concentrating on zero grades warrants further caution. However, while these outcomes are clinically relevant, additional patient-centered outcomes such as quality of life, patient satisfaction, and return-to-daily activities warrant inclusion in future studies. Expanding outcome assessments to incorporate these parameters could provide more comprehensive insights into the broader impacts of nanoparticle-based CP treatment.
Several limitations should be considered when interpreting the findings of this systematic review and meta-analysis. Firstly, the inclusion of unpublished clinical trials introduces potential publication bias, limiting the generalizability and robustness of the results. The absence of peer-reviewed published data restricts the confidence in their results. However, we conducted a comprehensive search through all possible databases and found no other published studies. Cochrane and other researchers recommend the analysis of unpublished results and grey literature to avoid publication bias.19,20 Secondly, variability in follow-up durations across the included studies may affect the comparability and interpretation of outcomes. We conducted a subgroup analysis whenever possible and found no difference between different time points. Heterogeneity in study designs and measurement methodologies among the included trials can introduce inconsistencies, affecting the reliability and external validity of pooled results. We chose to conduct all analyses with a random effect model a prior to account for any possible heterogeneity and have the most conservative outcomes. Furthermore, the limited number of included studies prevented comprehensive subgroup and sensitivity analyses.
Despite these limitations, this first systematic review and meta-analysis has several notable strengths. The rigorous methodology, adhering to PRISMA guidelines and the Cochrane Handbook, ensures transparency and replicability. The inclusion of RCTs exclusively strengthens the internal validity of meta-analysis, as RCTs minimize biases associated with observational study designs. Additionally, this systematic review addresses a clinically relevant question regarding postoperative inflammation and pain management—areas critical to patient satisfaction and surgical outcomes in cataract procedures. Another significant strength is the comprehensive database search strategy, encompassing multiple major databases and clinical trial registries, complemented by manual searches. This extensive approach ensures the identification of relevant studies and reduces the likelihood of missing important trials. Finally, assessing the quality of evidence through the GRADE framework provides clinicians and policymakers with transparent information regarding the confidence in and applicability of the findings, facilitating evidence-based clinical practice.
Future research should address these limitations by conducting well-designed, peer-reviewed, and published RCTs with larger sample sizes and standardized assessment methods. Longitudinal studies with extended follow-up periods are necessary to evaluate long-term safety profiles comprehensively and identify potential delayed adverse events. Standardization of outcome measures, particularly inflammation and pain assessment scales, would enhance the comparability and reliability of future meta-analyses. Moreover, further subgroup analyses investigating patient demographics (such as age, gender, ethnicity, and baseline ocular conditions) and procedural differences are recommended to identify populations that may derive greater benefits or face higher risks from nanoparticle-based CP treatments. Enhanced transparency in trial registration and result reporting in clinical trial databases will also help mitigate publication bias and improve the validity of future systematic reviews. Lastly, comparing this recently FDA-approved drug to other regimens of drugs may be beneficial for clinical decision making.
Conclusion
Nanoparticle-based clobetasol propionate significantly reduced inflammation and pain after cataract surgery, providing substantial therapeutic advantages compared to conventional treatments. Its promising safety profile supports its clinical adoption as a valuable postoperative care option, potentially enhancing patient recovery and comfort. However, the current evidence is limited by the small number of trials and the non-peer reviewed nature of the included trials. Further trials comparing CP to other regimens for post-cataract surgery are needed for better clinical decision making.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Onugwu AL, Nwagwu CS, Onugwu OS, et al. Nanotechnology based drug delivery systems for the treatment of anterior segment eye diseases. J Control Release. 2023;354:465–10. doi:10.1016/j.jconrel.2023.01.018
2. Vaneev A, Tikhomirova V, Chesnokova N, et al. Nanotechnology for topical drug delivery to the anterior segment of the eye. Int J Mol Sci. 2021;22(22):12368. doi:10.3390/ijms222212368
3. Zhang J, Jiao J, Niu M, et al. Ten years of knowledge of nano-carrier based drug delivery systems in ophthalmology: current evidence, challenges, and future prospective. Int J Nanomed. 2021;16:6497–6530. doi:10.2147/IJN.S329831
4. Khiev D, Mohamed ZA, Vichare R, et al. Emerging nano-formulations and nanomedicines applications for ocular drug delivery. Nanomater Basel Switz. 2021;11(1):173. doi:10.3390/nano11010173
5. Grzybowski A, Sidaraite A, Zemaitiene R. Management of inflammation after the cataract surgery. Curr Opin Ophthalmol. 2023;34(1):9–20. doi:10.1097/ICU.0000000000000912
6. Schwartz GF, Korenfeld MS, Silverstein SM, Potvin R, Walters TR. Efficacy and safety of clobetasol propionate ophthalmic nanoemulsion in reducing inflammation and pain after cataract surgery. Invest Ophthalmol Vis Sci. 2023;64(8):2744. doi:10.1167/iovs.64.8.2744
7. Azhar SD, Shahid N, Sadiq A, Khan AW, Sultan Dar M, Fadlalla Ahmed TK. Clobetasol propionate for post-cataract surgery pain and inflammation. Ann Med Surg. 2024;86(11):6395–6398. doi:10.1097/MS9.0000000000002619
8. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021:
9. Higgins J, Thomas J, Chandler J, et al. Cochrane handbook for systematic reviews of interventions.
10. Valizadeh A, Moassefi M, Nakhostin-Ansari A, et al. Abstract screening using the automated tool Rayyan: results of effectiveness in three diagnostic test accuracy systematic reviews. BMC Med Res Methodol. 2022;22(1):160. doi:10.1186/s12874-022-01631-8
11. De Cassai A, Schramel FMNH, van Dartel M, et al. The RoB 2 tool provides clearer guidance on how to evaluate the risk of bias in each domain and how to rate the overall risk of bias, making it a valuable tool for researchers conducting systematic reviews and meta-analyses. BMC Med Res Methodol. 2023;23(1):1–12. doi:10.1186/s12874-023-02000-0
12. Alonso-Coello P, Schünemann HJ, Moberg J, et al. GRADE Evidence to Decision frameworks: a systematic and transparent approach to making well-informed healthcare choices. BMJ. 2020;370:m3334. doi:10.1136/bmj.m3334
13. Patra JK, Das G, Fraceto LF, et al. Nano based drug delivery systems: recent developments and future prospects. J Nanobiotechnology. 2018;16(1):71. doi:10.1186/s12951-018-0392-8
14. Terveen D, Berdahl J, Dhariwal M, Meng Q. Real-world cataract surgery complications and secondary interventions incidence rates: an analysis of US medicare claims database. J Ophthalmol. 2022;2022:8653476. PMID: 35433042; PMCID: PMC9007656. doi:10.1155/2022/8653476
15. Haddad JE, Sabbakh NA, Macaron MM, et al. NSAIDs and corticosteroids for the postoperative management of age-related cataract surgery: a systematic review and meta-analysis. Am J Ophthalmol. 2024;260:1–13. Epub 2023 Oct 4. PMID: 37797866.doi:10.1016/j.ajo.2023.09.027
16. Agarwal P, Rupenthal ID. Non-aqueous formulations in topical ocular drug delivery – a paradigm shift? Adv Drug Deliv Rev. 2023;198:114867. doi:10.1016/j.addr.2023.114867
17. Baig MS, Karade SK, Ahmad A, et al. Lipid-based nanoparticles: innovations in ocular drug delivery. Front Mol Biosci. 2024;11:1421959. PMID: 39355534; PMCID: PMC11442363. doi:10.3389/fmolb.2024.1421959
18. Oo HH, Mohan M, Song W, et al. Anterior chamber inflammation grading methods: a critical review. Surv Ophthalmol. 2024;69(2):253–264. doi:10.1016/j.survophthal.2023.10.005
19. Golder S, Loke YK, Bland M. Unpublished data can be of value in systematic reviews of adverse effects: methodological overview. J Clin Epidemiol. 2010;63:10 1071–1081. doi:10.1016/j.jclinepi.2010.02.009
20. Greiner B, Corcoran A, Wheeler D. Clinical trial registry searches are under-utilized in systematic reviews from critical care journals: A bibliometric analysis. Journal of Critical Care. 2021;63: 175–178. doi: 10.1016/j.jcrc.2020.09.010
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.