Back to Journals » Substance Abuse and Rehabilitation » Volume 17
The Effect of Smartphone-Delivered Approach Bias Modification Training on Relapse Among Patients Leaving Residential Alcohol Treatment: A Randomised Controlled Trial
Authors Garfield JBB ![]() , Whelan D
, Whelan D ![]() , Piercy H, Hopwood M, Maloney M
, Piercy H, Hopwood M, Maloney M ![]() , Mahasuar R, Roxburgh AD
, Mahasuar R, Roxburgh AD ![]() , Lubman DI
, Lubman DI ![]() , Manning V
, Manning V ![]()
Received 9 March 2026
Accepted for publication 30 April 2026
Published 16 June 2026 Volume 2026:17 607994
DOI https://doi.org/10.2147/SAR.S607994
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rajendra Badgaiyan
Joshua BB Garfield,1,2 Danielle Whelan,1,2 Hugh Piercy,1,2 Malcolm Hopwood,3,4 Michael Maloney,5 Rajnarayan Mahasuar,6 Ariel D Roxburgh,1,2,7 Dan I Lubman,1,2 Victoria Manning1,2
1Monash Addiction Research Centre, Eastern Health Clinical School, Monash University, Melbourne, VIC, Australia; 2Turning Point, Eastern Health, Melbourne, VIC, Australia; 3Department of Psychiatry, University of Melbourne, Melbourne, VIC, Australia; 4Ramsay Clinic Albert Road, Ramsay Health, Melbourne, VIC, Australia; 5The Melbourne Clinic, Healthscope, Melbourne, VIC, Australia; 6Wyndham Clinic Private Hospital, Melbourne, VIC, Australia; 7Arrow Health, Melbourne, VIC, Australia
Correspondence: Joshua BB Garfield, Monash Addiction Research Centre, Eastern Health Clinical School, Monash University, Turning Point, 110 Church Street, Richmond, VIC, 3121, Australia, Tel +61 3 8413 8711, Email [email protected]
Purpose: Approach bias modification (ApBM), a cognitive training intervention that reduces “alcohol approach bias” (impulses to approach alcohol-related stimuli), reduces post-treatment relapse rates when delivered during residential alcohol use disorder (AUD) treatment. However, few residential treatment services provide ApBM to their clients. Smartphone app-delivered ApBM may circumvent barriers to implementation within services by allowing clients to self-administer ApBM after discharge instead. This double-blind RCT tested whether providing a personalised ApBM smartphone app to people discharging from residential AUD treatment increased alcohol abstinence rates.
Participants and Methods: Participants were recruited while attending residential AUD treatment programs. 171 participants were sent app download instructions following discharge, of whom 134 installed it (61 receiving the ApBM version; 73 sham-training controls), providing only 39% power for primary outcome analysis. App notifications reminded participants to complete training tasks each week for 4 weeks. Alcohol use and other secondary outcomes were measured post-intervention and at 1-month, 3-month, and 6-month follow-ups. The primary outcome was past-month abstinence from alcohol at the 3-month follow-up.
Results: Abstinence rates at 3-month follow-up were 55% [95% CI: 40%, 70%] in controls and 52% [95% CI: 36%, 67%] in ApBM participants. This difference was non-significant (contrast: − 3% [95% CI: − 25%, 18%], p = 0.758). All secondary outcomes analyses also found non-significant effects of group. Exploratory post-hoc analyses suggested that duration of residential treatment and number of ApBM sessions completed may moderate ApBM’s effects on abstinence.
Conclusion: Findings did not support the efficacy of post-discharge, personalised, app-delivered ApBM for relapse prevention in residential AUD treatment clients. These findings should be treated with caution due to this trial’s low statistical power. Exploratory analyses suggest that future trials may be more likely to find evidence of efficacy for this approach if they focus on clients with shorter admissions and deliver a more sustained, structured ApBM intervention.
Keywords: alcohol, alcohol use disorder, approach bias modification, cognitive bias modification, rehabilitation, inpatient treatment
Introduction
Alcohol use contributes to more than 2.6 million deaths annually and accounts for 4.7% of the global burden of disease.1 An estimated 400 million people are living with alcohol use disorder (AUD).1 In Australia, alcohol was the most common primary drug of concern among clients accessing publicly funded addiction rehabilitation services in 2023–24, accounting for 43% of publicly funded rehabilitation episodes.2 Although residential rehabilitation is among the most resource-intensive treatment approaches for AUD, over half of clients relapse within one year of discharge.3–5 This underscores the importance of providing evidence-informed relapse prevention support during the vulnerable period of transition from residential care back into the community.
Vulnerability to relapse is related to multiple demographic, clinical, treatment-related, and structural variables. Australian studies suggest that post-treatment engagement with social welfare and allied health services (eg., mental health, housing, and family counselling services) and attendance at mutual aid groups (eg., Alcoholics Anonymous, SMART Recovery) may be protective against relapse,6 while higher alcohol craving at the end of treatment predicts higher risk of relapse.7 A large Danish treatment outcome study suggested that younger age and history of psychiatric illness also predicted relapse.8
Vulnerability to relapse is also influenced by strongly ingrained “cognitive biases” that develop with repeated heavy drinking. These include “attention bias” (the tendency for alcohol-associated stimuli to capture attention) and “approach bias” (the automatic action tendency to approach alcohol-related stimuli).9 Visual, auditory, olfactory, and contextual/social stimuli associated with alcohol, such as advertisements, pubs, bottle shops, and alcoholic beverages themselves, are so ubiquitous in Australian society that, in many contexts, they are unavoidable. Therefore, biased cognitive processing of these stimuli poses a serious challenge for people making the transition from protective residential treatment settings, where they are sheltered from these cues, to community settings where they are bombarded by reminders of alcohol use.
Cognitive bias modification interventions have been developed to reduce these biases, with “approach bias modification” (ApBM) showing the most consistent effects in treatment-seeking populations. ApBM involves training individuals to repeatedly make avoidance responses to alcohol-related images and approach responses to non-alcohol-related images. When delivered during residential treatment, ApBM typically involves a computerised task in which participants use a joystick to “push” alcohol images “away”; and “pull” non-alcohol images “closer”. Over time, individuals learn to “avoid” alcohol-related cues more automatically, with several studies showing reductions in approach bias, or development of an alcohol avoidance bias, among people undergoing AUD treatment following ApBM training.10–14
Multiple randomised controlled trials (RCTs) have shown that delivering ApBM during residential AUD treatment can reduce post-treatment relapse risk.3,10,13–18 However, despite there now being an international expert consensus recommending implementation of ApBM for AUD treatment,19,20 very few treatment services have done so internationally. Organisational, resource, and training barriers likely contribute to its limited service-level implementation. While overcoming these barriers is an important research direction, exploring alternative modalities of ApBM that do not rely on in-service implementation is also warranted.
Delivering ApBM via a smartphone app would allow individuals to access ApBM after leaving residential treatment, including at times and in contexts when they are at most risk of relapse, such as during acute cravings. To date, only a small number of studies have examined alcohol ApBM apps, and most have recruited general community samples, rather than people undergoing treatment. In a factorial RCT, Crane et al21 tested apps which either included or omitted ApBM (alongside other intervention modules) among people drinking heavily. Although initial analyses suggested that versions of the app that included both ApBM and normative feedback modules reduced weekly alcohol consumption more than versions that lacked this combination, later re-analysis in a larger sample found no significant effects.22 Peerenboom et al23 found that participants who completed a session of app-based ApBM showed reduced cue-induced alcohol craving the following day, and reduced AUD severity after 1 week, compared to controls. However, their app delivered only a single, unusually long ApBM session, which is not an approach likely to be implemented widely. Laurens et al24 piloted an ApBM smartphone app in a community sample of individuals who wanted to reduce their drinking, encouraging them to complete two ApBM sessions per week over three weeks. Participants reported reductions in weekly alcohol consumption over this 3-week period, with further declines at 3-month follow-up. However, the lack of a control group in this study limits causal conclusions.
Laurens et al also reported qualitative data, including participants’ criticisms of the lack of personalisation of beverage images used in the app’s ApBM training task, and of the task’s repetitiveness, suggesting that game-like features could improve engagement.24 Personalisation of training stimuli may improve ApBM’s efficacy too, because approach bias is thought to develop through repeated associative conditioning experiences,25 and individuals with AUD typically consume a limited range of alcoholic beverages. Hence, using generic alcohol stimulus sets that may include images of beverages an individual rarely or never consumes, may limit ApBM’s efficacy. In addition, most alcohol ApBM studies train participants to approach non-alcoholic beverages. Using positive images representing personally meaningful goals and healthy sources of pleasure (eg., friends, family, pets, exercise) may be more engaging, and, as suggested by our recent qualitative studies of personalised ApBM,26,27 also reinforces motivations towards adaptive behaviours, potentially enhancing the therapeutic impact of ApBM. Indeed, we have recently trialled a personalised approach to ApBM in a small sample of people undergoing inpatient treatment for methamphetamine use disorder, with promising preliminary results.28
Following this reasoning, we developed “SWiPE”, the first personalised, gamified ApBM smartphone app.29 Our open-label feasibility study of SWiPE, in a community sample of individuals drinking at hazardous levels (Alcohol Use Disorder Identification Test (AUDIT) score of at least 8), observed reductions in alcohol use, craving, and dependence severity after 4 weeks of using the app.30 However, since this study lacked a control group, it is unclear whether these outcomes were attributable to ApBM.
Building on these findings, we tested this personalised ApBM app (renamed “AAT-App”, which stands for “Alcohol Avoidance Training App”, to preserve blinding, following publicity that SWiPE received) in two recently published RCTs. In one RCT, AAT-App was delivered as an adjunctive intervention to people receiving outpatient AUD treatment,31 while the other RCT tested it in people aged over 55 years recruited from the general community and drinking at hazardous levels.32 Participants in both RCTs were randomised to receive either personalised, gamified ApBM or a sham-training control version of the app. Participants were prompted to use the app for four weeks. While significant differences between groups were not observed for the primary outcome (past-week alcohol consumption at the end of the 4-week intervention) in either trial, both trials detected differences between groups in weekly alcohol consumption at secondary endpoints. In the outpatient trial, ApBM participants reduced their alcohol consumption, relative to baseline levels, significantly more than controls at the final follow-up (3 months after the end of the 4-week intervention); while in the trial of people aged over 55, participants who received ApBM consumed less alcohol than controls during the second week of the intervention. The present trial was the third RCT of AAT-App and aimed to test its efficacy as a relapse-prevention tool for people discharging from residential AUD treatment.
Materials and Methods
Study Design and Setting
We conducted a multi-site, double-blind, randomised, parallel-group controlled superiority trial. Participants were recruited while receiving residential treatment for AUD from 5 addiction treatment services in Victoria, Australia. Four services were private psychiatric hospitals offering inpatient addiction withdrawal and rehabilitation programs that typically ranged from 1 to 3 months duration. One was a service run by a public hospital organisation that offered a (typically 3–4 week) withdrawal and stabilisation program. One of the private services was located in a small regional town, while all other services were in the Melbourne metropolitan region.
Participants were recruited between November 28, 2022 and November 11, 2024 and were randomised to receive the ApBM or sham-training control version of AAT-App. Participants activated the app between November 30, 2022 and December 17, 2024, and the final follow-up data collection occurred on July 11, 2025. The study was approved by the Eastern Health Human Research Ethics Committee (HREC; project number 87504), Monash University HREC (project number: 35421), and The Melbourne Clinic REC (project number: 351). Eastern Health HREC review ensured the study complied with Australia’s National Statement on Ethical Conduct in Human Research 2007 (Updated 2018),33 which complies with the Helsinki Declaration. The study was prospectively registered on the Australian New Zealand Clinical Trials Registry (project ID: ACTRN12622001245785).
Participants
One-hundred-thirty-four participants installed the app. Inclusion criteria were: Aged ≥18 years; owned an Apple or Android smartphone with an Australian phone number; smartphone operating system updated within the past year; currently receiving residential treatment for AUD at the time of recruitment; ≥4 DSM-5 symptoms of AUD present within the past 6 months; and sufficient English literacy to use the app and complete questionnaires. Patients were excluded if they were planning to transfer to another residential treatment facility following discharge; or if their treating clinician considered them too cognitively or psychiatrically impaired to provide informed consent or safely participate.
The initial sample size target was 300. The a priori power calculation assumed a 45% abstinence rate in controls (based on previous research),3,10,14 and assumed a 17% increase (ie., 62% abstinence rate) in the ApBM group, based on the effect size we observed in per protocol analysis of 2-week outcomes in a previous ApBM trial.13 This suggested that 300 participants would provide 82% power. A later re-analysis of power based on a more conservative 13% increase in abstinence rate observed in intention-to-treat 3-month follow-up analyses in the previous trial15 indicated that 300 participants would provide only 68% power. Hence, we decided to aim to recruit a larger sample if time and recruitment rates allowed. However, due to lower-than expected recruitment rates, only 134 participants had installed the app when recruitment ended due to funding limitations. A post-hoc power analysis, based on the control group’s abstinence rate at the 3-month follow-up in this trial, found that this sample size provided only 39% power to detect the expected 13% increase in abstinence rate in the ApBM group.
Measures
Demographic Characteristics
A survey hosted on Qualtrics Plus assessed participants’ age, gender, race, whether English was their first language, highest level of education, employment status, and postcode of residence.
Alcohol Consumption
Quantity of alcohol consumed on each of the 28 days immediately preceding admission to the residential treatment service was assessed at baseline using an in-person timeline follow-back (TLFB) interview.34 These data were used to derive past-month and past-week measures of baseline alcohol use, including total number of standard drinks (defined in Australia as 10 grams alcohol), total drinking days (days on which any alcohol was consumed); and total number of heavy drinking days (HDDs: days on which 5 or more standard drinks were consumed). Five standard drinks was chosen as the definition of an HDD based on the Australian National Health and Medical Research Council (NHMRC) guidelines, which recommend limiting intake to no more than four standard drinks on any day to minimise risk of alcohol-related harm.35
During the 4-week intervention period, the app automatically prompted participants each week (ie., 7, 14, 21, and 28 days after they installed the app) to report the number of standard drinks consumed on each of the past 7 days. Examples of how many standard drinks commonly consumed beverages typically contained were displayed in the app to assist participants with estimating consumption. The final week’s report was used to calculate past-week standard drinks, drinking days and HDDs at the end of the intervention period. At the 1-month and 3-month post-intervention follow-ups, the app prompted participants to complete the same assessment of past-week alcohol use, and also to estimate the total number of drinking days in the past 28 days. Past-month drinking days data were used to categorise participants as abstinent (0 drinking days) vs. non-abstinent (1–28 drinking days) for the purpose of primary outcome analysis. At the 6-month follow-up, a researcher administered a TLFB by phone covering the past 28 days.
AUD Severity
The current AUD module of the Structured Clinical Interview for DSM-5 Disorders–Research Version (SCID–5–RV)36 was used to confirm eligibility at baseline and to assess whether participants met criteria for current AUD at 6-month follow-up. Questions were modified to refer to the past six months (rather than the past year) to allow assessment of equivalent non-overlapping periods at each time. The Alcohol Use Disorders Identification Test (AUDIT)37 and The Severity of Dependence Scale (SDS)38 were also used as secondary outcomes and are described further in the Supplement (see Supplementary Methods).
App Acceptability
At the end of the 4-week intervention period, participants rated each of the following 6 statements using 5-point Likert scales ranging from “strongly agree” to “strongly disagree”: “The app helped me reduce my alcohol use”, “The app increased my alcohol consumption”, “The app helped reduce my cravings for alcohol”, “The app increased my cravings for alcohol”, “The app helped increase my interest in healthy activities and positive goals”, and “The app helped increase my engagement in healthy activities and pursuing positive goals”.
Blinding Success
At the end of the 6-month follow-up interview, participants were reminded that they had been randomly assigned to either a version of the app that delivered “brain training that was designed to change automatic reactions to alcohol images” or a version where “the training task was not designed to change these automatic reactions to alcohol” and were asked to guess which version they received.
Other Secondary Outcomes
Other secondary outcome measures are described in more detail in the Supplement (see Supplementary Methods). These include the Craving Experience Questionnaire Frequency scale (CEQ-F);39 items from the Australian Treatment Outcomes Profile (ATOP)40 assessing psychological health, physical health, and overall quality of life; the Depression Anxiety Stress Scales (DASS-21);41 The Snaith-Hamilton Pleasure Scale (SHAPS);42 and an assessment of readmission to substance use withdrawal or rehabilitation treatment, or any alcohol-related emergency department or inpatient hospital admissions, during the post-discharge follow-up period.
Intervention
ApBM
After activating the ApBM version of the app, participants viewed a short video explaining the concept of “alcohol cognitive bias”. They were then prompted to select 6 alcohol-related images that represent the drinks they most frequently consumed. A library of 67 alcohol-related images, representing a broad range of alcoholic beverages commonly consumed in Australia, was provided in the app, but participants could also select from their own photographs of alcohol (if they had images of alcohol stored on their phone) or take new photographs (eg., to include a specific drink type/brand not already in the app’s image library). Participants were then prompted to select 6 images that “represent your goals and motivations”. Again, participants could either select from a library of 68 images representing a range of healthy activities or sources of pleasure, or positive goals (eg., people socialising; financial success; employment; exercise, sports, and recreational activities; healthy foods; pets; travel and holidays), or use photographs from their own phone. If participants used their own photographs, instructions reminded them to select positive images that did not contain depictions of alcohol.
The alcohol and positive image libraries provided in the app were based on similar image libraries used in the previous SWiPE app.30 These image libraries were developed following a focus group, comprising people with lived experience of undergoing treatment for AUD, which we convened to help us select appropriate sets of alcohol-related and positive images for use in our AUD research program. The SWiPE image libraries were further refined following consultation with people with lived experience of trying to quit or reduce heavy drinking, who tested an early version of SWiPE. The content of the image libraries used in AAT-App was further informed by qualitative feedback from SWiPE trial participants.26
After selecting their 12 training images, participants were presented with ApBM task instructions. Images were displayed inside a white rectangular “frame” which was either in landscape or portrait orientation. Participants were instructed to “approach” images presented in landscape frames by swiping downwards (ie., towards themselves). This caused the image to expand, to simulate the experience of “pulling” the image “closer”. Participants were instructed to “avoid” images in portrait frames by swiping upwards (ie., away from themself). This caused the image to shrink and disappear, simulating the experience of “flicking” the image “away”. If participants swiped in the incorrect direction, a red “X” was displayed.
Participants completed 10 practise trials before proceeding to their first ApBM session. Each session comprised 156 trials (13 presentations of each of the 12 images), and typically took 3–5 minutes to complete. For each alcohol image, 12 of the 13 presentations were framed in portrait orientation, and hence required an “avoidance” response, and one was in landscape orientation. For each positive image, 12 of the 13 presentations were framed in landscape orientation (requiring an “approach” response), while one was framed in portrait orientation. Thus, participants were supposed to avoid 92% of alcohol images and approach 92% of positive images. This was intended to help participants practice “over-riding” their alcohol approach impulses and train an automatic “avoidance” response to alcohol instead, while reinforcing “approach” responses to positive stimuli.
To increase engagement and encourage accurate responding, the task was gamified with a scoring system that awarded points for correct responses (with faster responses gaining more points) and deducted points for incorrect responses. Scores were displayed at the top of the screen as participants performed the task, and upon task completion, the final score was displayed. On the second, and subsequent, sessions, participants’ final score for that session was shown alongside their previous personal best score, so they could compare their performance. Further details of task parameters are available in the protocol attached to the trial registration.43
App notifications reminded participants to complete two training sessions each week for 4 weeks (ie., they were encouraged to complete at least 8 sessions in total). Participants could complete more than 2 sessions in a week if they wanted and could continue using the app after the first 4 weeks (but no longer received notifications to do so). After the first session, participants had the option of whether or not to review the task instructions and complete practise trials prior to training sessions.
Sham Training
Participants who activated the control version of the app were first presented with a text explanation that the app was “designed to target their alcohol use and awareness” and would involve completing one training task at the end of each week and answering questions about their alcohol consumption. Participants were then presented with task instructions, which were identical to those in the ApBM condition, and completed 10 practice trials prior to their first sham training session. Each sham training session involved presentation of 20 alcohol and 20 neutral (eg., stationary, kitchenware) images. Images were not personalised (ie., the same 40 images were used for all participants in the sham-training control group). Each image was presented twice, once with a landscape frame and once with a portrait frame, for a total of 80 image presentations per session. Hence, participants were supposed to swipe 50% of alcohol images and 50% of neutral images away; and swipe 50% of each category towards themselves. By requiring an equal number of approach and avoidance responses to each image category, the sham training was intended to neither reduce nor increase approach bias. Following completion of their first session, participants were instructed that they would be notified to complete additional “brain-training” tasks at the end of each of the following 4 weeks. They could not complete additional sessions.
Randomisation
The app developers provided two lists of app access codes, one comprising codes which activated the ApBM version, and the other comprising codes which activated the control version of AAT-App. A research manager who was not involved in recruitment, data collection, or analysis combined these into 5 randomised lists of codes (one list for each recruitment site), based on site-stratified randomisation sequences computer-generated by the research manager using a 1:1 allocation ratio and variable block sizes. The versions of the randomised code lists provided to researchers involved in recruitment did not include information regarding which codes activated which condition to ensure blinding of research staff involved in recruitment and data collection. When participants discharged from residential treatment, blinded researchers accessed the code list for the participant’s treatment site and sent them the first unused activation code from the list. Versions of the lists that identified which codes activated each condition were protected with a password that was not shared with staff involved in recruitment and data collection until all data collection was complete.
Procedure
Clinicians at participating residential treatment services were informed of eligibility criteria and asked to inform potentially eligible clients about the study. If a client was interested, a researcher met with them to explain the research and obtain written informed consent. If a client consented, the researcher administered a battery of measures to confirm eligibility and collect baseline data. Measures administered at each timepoint are summarised in Table 1. At baseline, demographic questions, SCID-5-RV AUD module, AUDIT, and TLFB were interviewer-administered; and SDS, CEQ-F, ATOP items, DASS-21, and SHAPS were self-administered.
When a participant discharged from residential treatment, researchers sent them an app download link and access code by SMS. If they did not activate the app within 1 day, researchers attempted to remind participants up to 5 times over the following days by phone, SMS, and email.
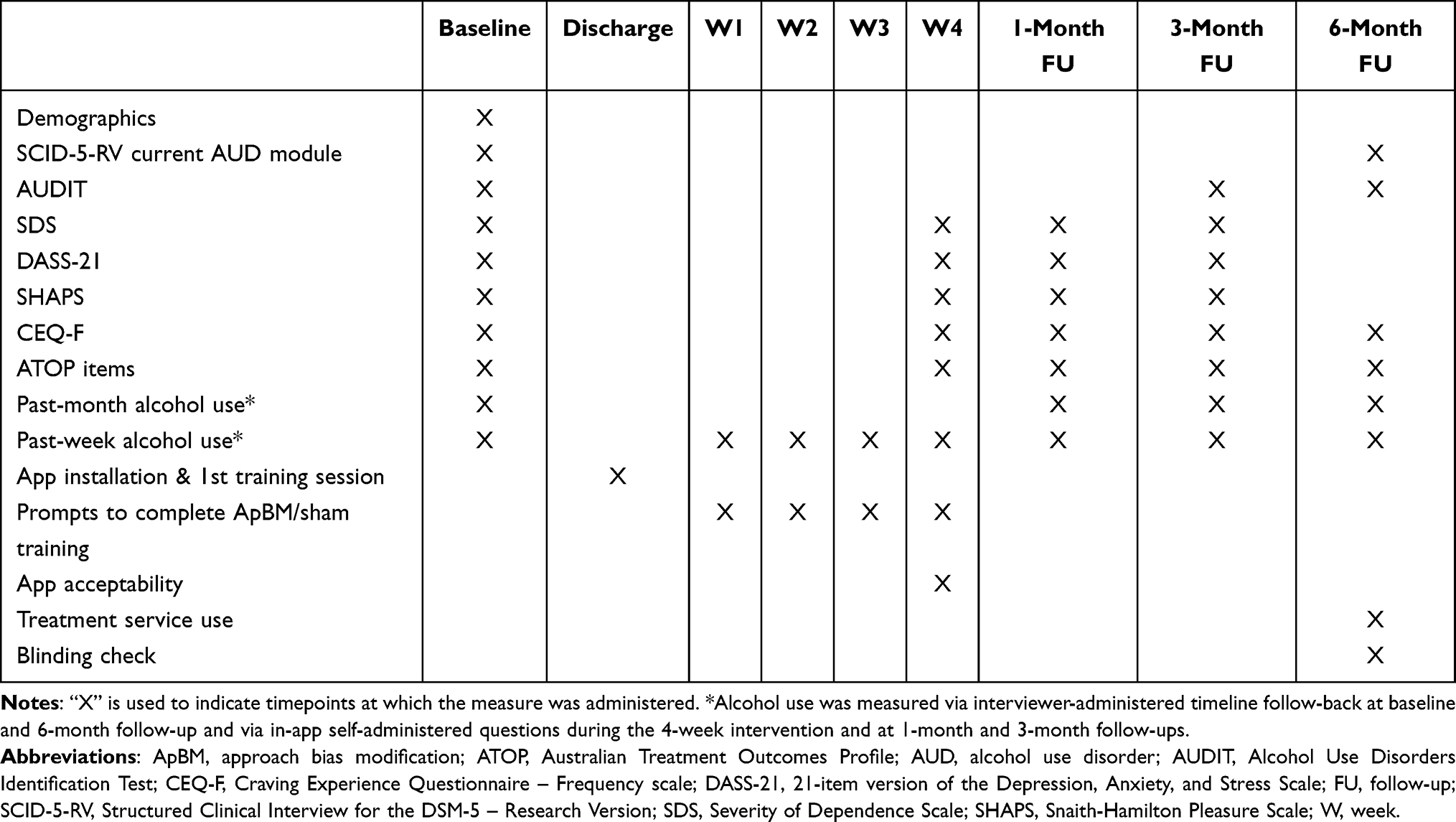 |
Table 1 Schedule of Measures and Tasks |
After completing their week 4 alcohol use questions, participants were prompted to follow a link to the post-intervention Qualtrics survey (see Table 1). Participants received a $20 (Australian dollars) supermarket gift voucher for completing this survey. Access to post-intervention assessments expired after 1 week (ie., they could only be completed 28–35 days after app activation).
Twenty-eight days after the end of the intervention period (ie., 56 days post-activation), an app notification prompted participants to complete 1-month follow-up alcohol use questions in the app, after which they followed a link to a Qualtrics survey (see Table 1). The same process occurred 84 days after the end of the intervention period (for the 3-month follow-up). Participants received $20 vouchers for completing each of these follow-ups. Access to the 1-month follow-up expired 14 days after the due date, and after 28 days for the 3-month follow-up. Researchers attempted to contact participants up to 5 times during these intervals to remind them to complete follow-ups if they did not complete them on the day they were due.
At least 168 days after the end of the intervention, researchers contacted participants to complete the 6-month follow-up phone interview (see Table 1). There was an 8-week allowable interval for 6-month follow-up completion (ie., 168–224 days after the end of the intervention period). Participants received a $30 voucher for completing the 6-month follow-up.
Data Analysis
Statistical significance was ascertained using α = 0.05. Any participants who commenced at least 1 session of ApBM (if in the ApBM condition) or sham-training (if in the control condition) were included in the analysis set. Analyses were conducted using Stata 19.
Primary Outcome
The primary outcome, past-month abstinence, was analysed over the 3 post-intervention follow-ups using a mixed-effects logistic regression model which tested the fixed effects of group (ApBM vs. sham); time (1-month, 3-month, and 6-month follow-up; entered as a categorical variable with 1-month follow-up as the reference timepoint); and group × time interaction effects to test whether the size of between-group differences varied across timepoints. Levels were included for participant and for recruitment site (to allow for possible non-independence of data from participants from the same site). Planned contrasts between groups’ estimated marginal proportions abstinent were conducted for the primary outcome endpoint (3-month) and the secondary outcomes (1-month and 6-month). The primary analysis was conducted with no imputation of missing outcomes, while a supplementary sensitivity analysis imputed outcomes by assuming that participants lost to follow-up were not abstinent.
Secondary Outcomes
Acceptability ratings were explored using descriptive statistics, particularly proportions of participants endorsing each response option, with Pearson’s chi-squared tests conducted to compare these response distributions between groups. Pearson’s chi-squared test was used to compare the proportion of each group who believed they received the active training intervention. Statistical analyses used to analyse other secondary outcomes are described in the Supplement (see Supplementary Methods).
Post-Hoc Exploratory Analyses
Due to variance in duration of residential treatment, time taken to install the app after discharge, and number of ApBM sessions completed, we conducted post-hoc exploratory analyses to examine whether these factors may have influenced effects of ApBM on past-month abstinence rates. These were conducted for the purpose of guiding the design of, and generating hypotheses for, future research. For duration of residential treatment, this involved repeating the mixed-effects logistic regression models described above with the additional inclusion of the fixed effect of residential treatment duration (in days, entered as a continuous variable) and its 2-way and 3-way interactions with group and timepoint. This was conducted twice, using both non-imputed and imputed abstinence outcome data.
The association between number of ApBM sessions completed and abstinence rates at follow-ups was explored at each follow-up separately using mixed-effects logistic regression testing the effect of number of sessions on abstinence, with site included as a level. Only participants in the ApBM group were included in these models, since differences between groups in the number of sessions the app allowed them to complete would otherwise confound analyses. Moreover, since increased number of sessions significantly predicted follow-up completion, these analyses used only non-imputed outcomes, since assuming non-abstinence in those lost to follow-up could otherwise inflate associations between number of sessions and abstinence. Finally, we repeated the primary analyses of past-month abstinence excluding participants who did not activate the app within 1 week after discharge.
Results
Figure 1 shows the number of clients who were referred, screened, randomised, activated the app, and completed follow-ups. Table 2 presents the baseline demographic characteristics of the sample and Table 3 presents the baseline clinical and treatment characteristics. Typical of AUD treatment samples, participants’ mean age was in the mid-40s. There were similar numbers of male and female participants, and the sample predominantly comprised White, native-English speakers recruited from private treatment services. Approximately half had completed university degrees. Participants had consumed alcohol on a mean of 22 of the 28 days before they commenced residential treatment, and their mean consumption was more than 10 times higher than the 10 standard drink-per-week limit suggested by Australia’s NHMRC to minimise long-term risk of alcohol-related disease.35 Approximately half of participants used nicotine daily and approximately a quarter had used illicit drugs in the month prior to their admission. A large majority of participants said their goal was complete abstinence from alcohol.
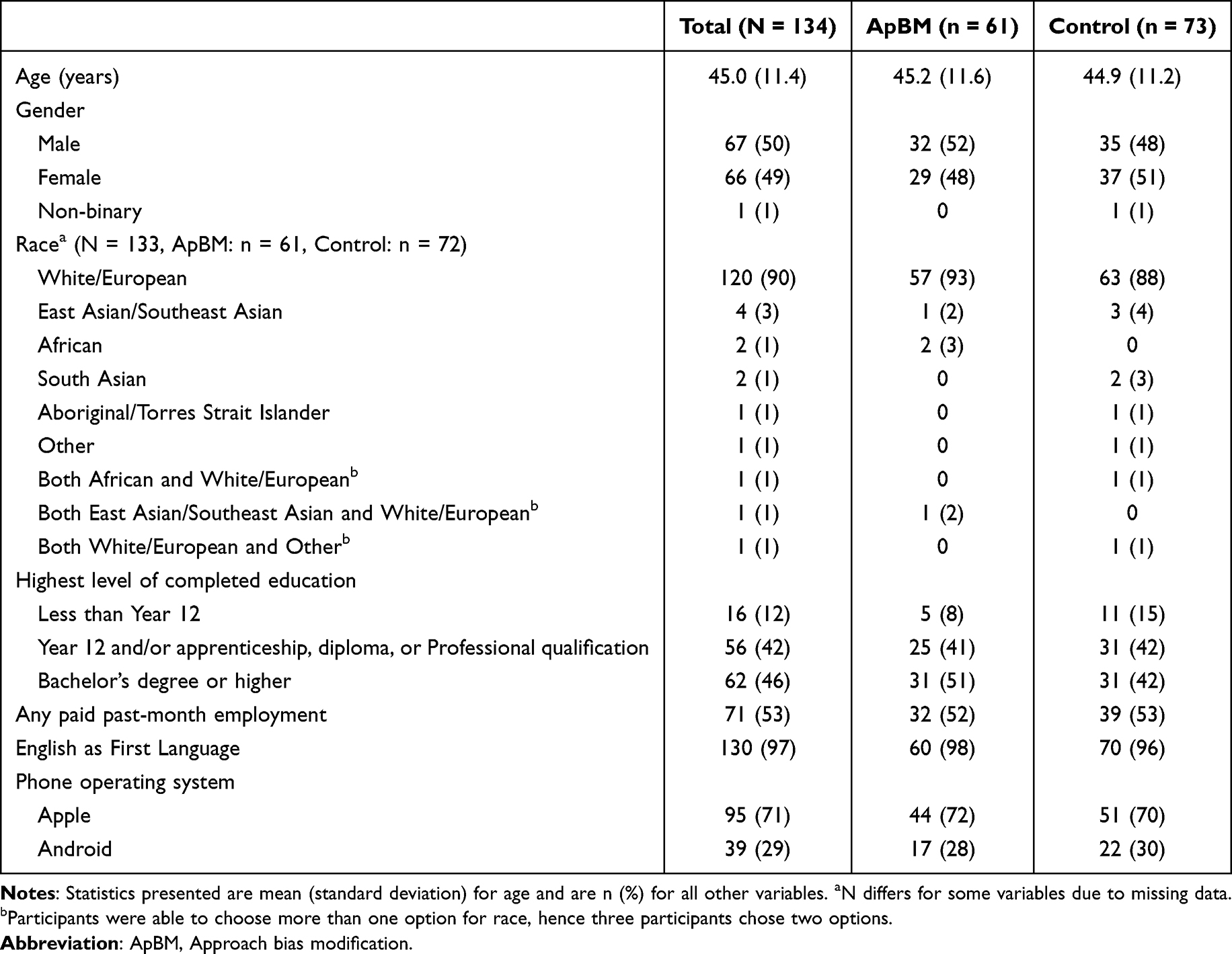 |
Table 2 Baseline Demographic Characteristics of Participants Who Activated the App |
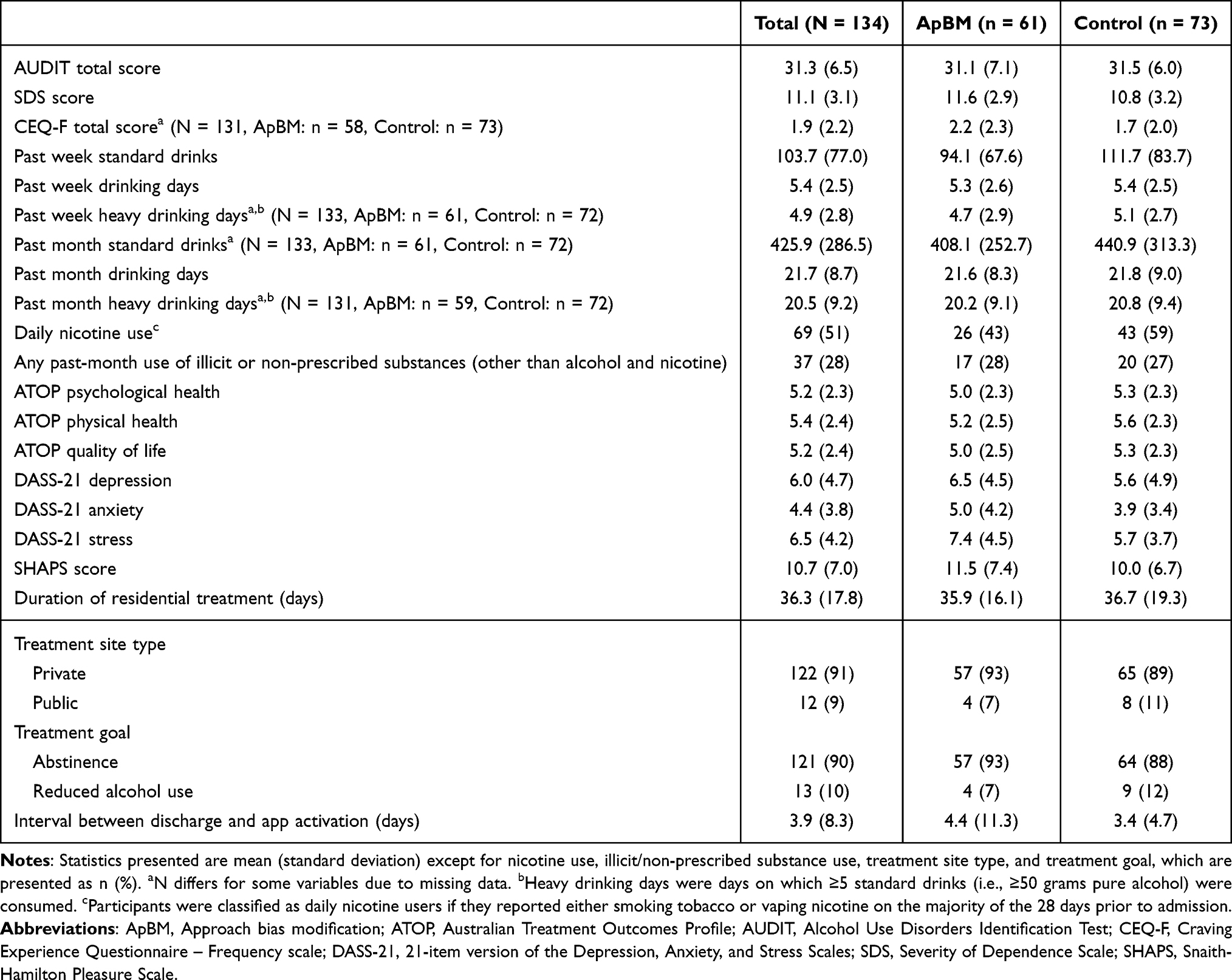 |
Table 3 Baseline Clinical Characteristics of Participants Who Activated the App |
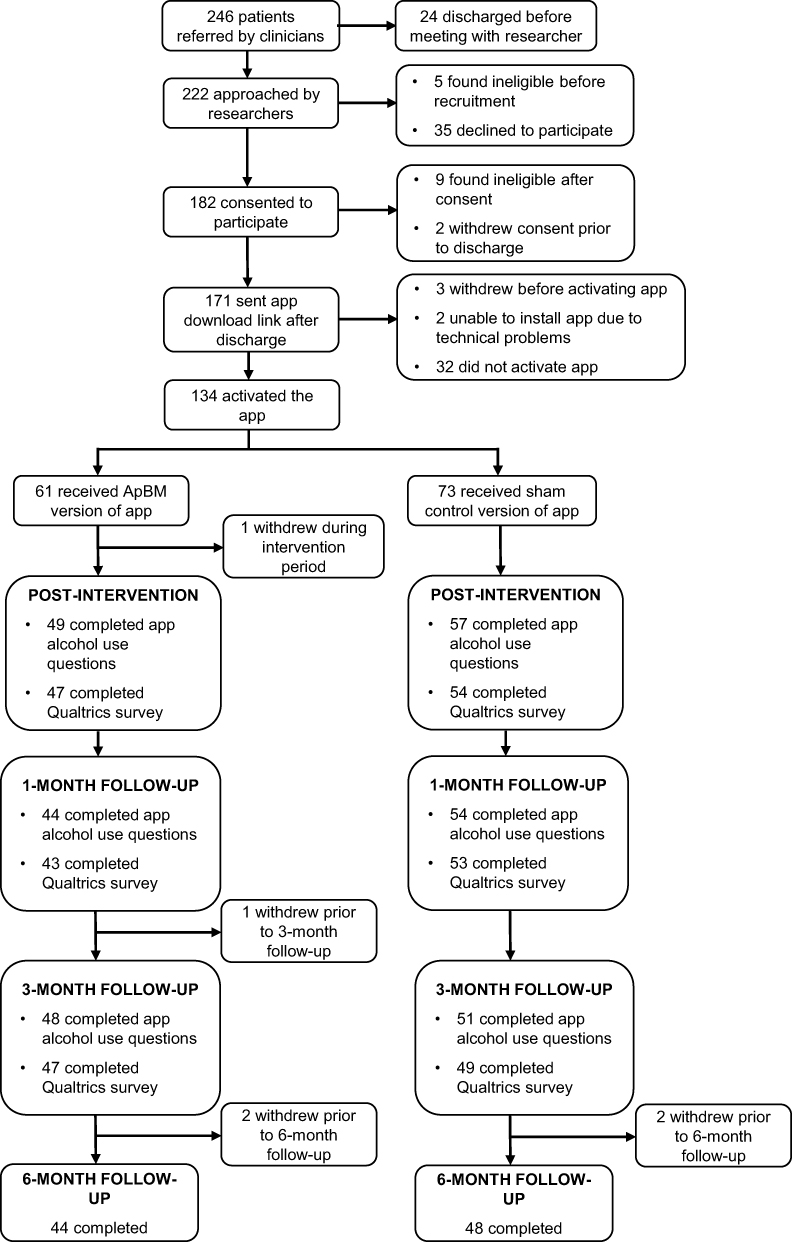 |
Figure 1 CONSORT flow diagram. |
Duration of the residential treatment episode from which participants were recruited ranged from 9 to 103 days. Following discharge, participants took between 0 and 87 days to activate the app, although 89% activated the app within a week of discharging. Participants in the ApBM condition completed a mean of 7.3 sessions of ApBM during the first 4 weeks after installing the app (range: 1–16), or 8.0 in total (range 1–17) if additional sessions completed after the first 4 weeks are counted. Participants in the control group completed a mean of 2.9 sham training sessions (range 1–5) during the 4-week intervention period or 3.9 (range 1–7) overall.
Primary Outcome
Figure 2 shows proportions of participants reporting past-month abstinence at each follow-up. Results of the mixed-effects logistic regression analysis of past-month abstinence across the 1-month, 3-month, and 6-month follow-ups are shown in Table 4. There were no significant effects of group or interactions between group and time. The significant main effect of time in the contrast between the 6-month and 1-month follow-up indicates that abstinence rates decreased between these two follow-ups. Consistent with the overall model, planned between-group contrasts for the primary outcome (3-month follow-up) found no significant effect. The observed-data analysis suggested that controls’ abstinence rate was 55% [95% CI: 40%, 70%], while in the ApBM group it was 52% [95% CI: 36%, 67%] (contrast: −3% [95% CI: −25%, 18%], p = 0.758). The analysis that assumed non-abstinence for participants lost to follow-up suggested a 34% [95% CI: 25%, 44%] abstinence rate in controls and 36% [95% CI: 26%, 47%] in the ApBM group (contrast: 2% [95% CI: −12%, 17%], p = 0.746). Contrasts between groups at the secondary endpoints also found non-significant effects at both the 1-month follow-up (Observed data: p = 0.701; imputed: p = 0.985) and 6-month follow-up (Observed data: p = 0.991; imputed: p = 0.661).
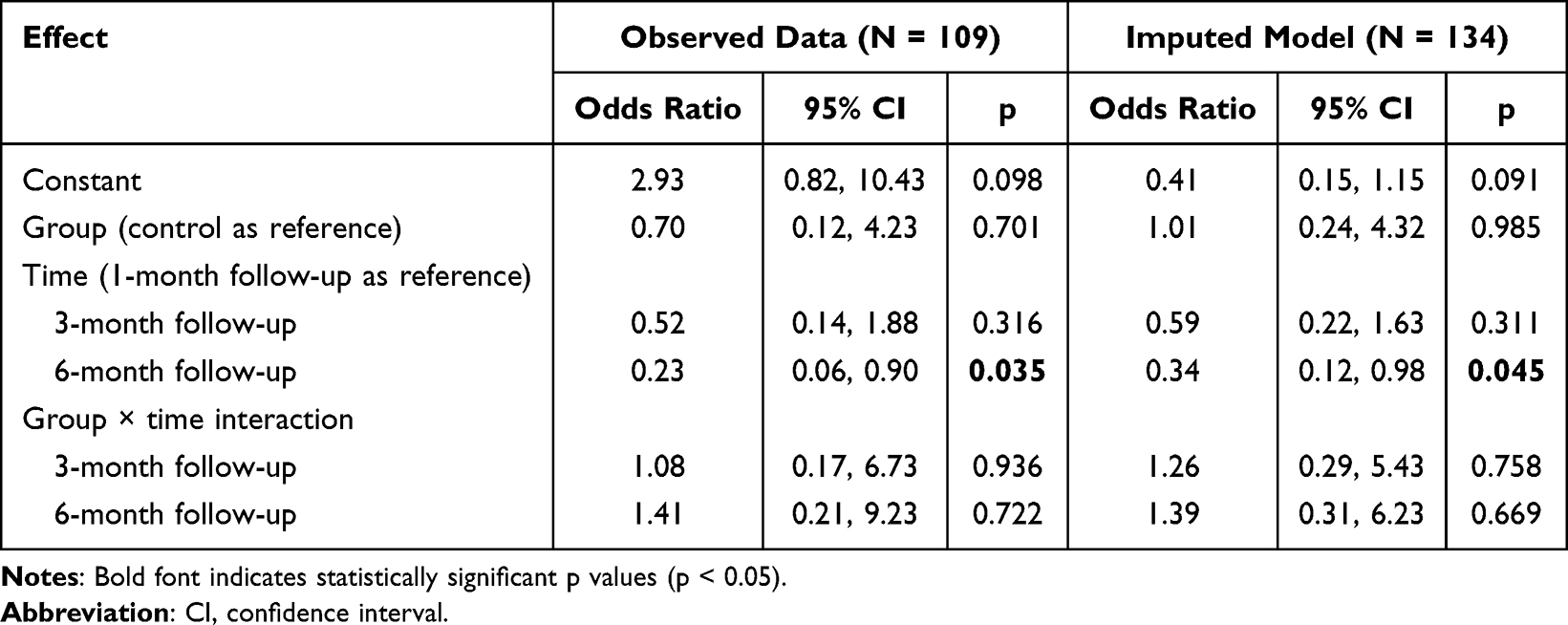 |
Table 4 Results of Mixed-Effects Logistic Regression Analysis of Past-Month Abstinence at Follow-Ups |
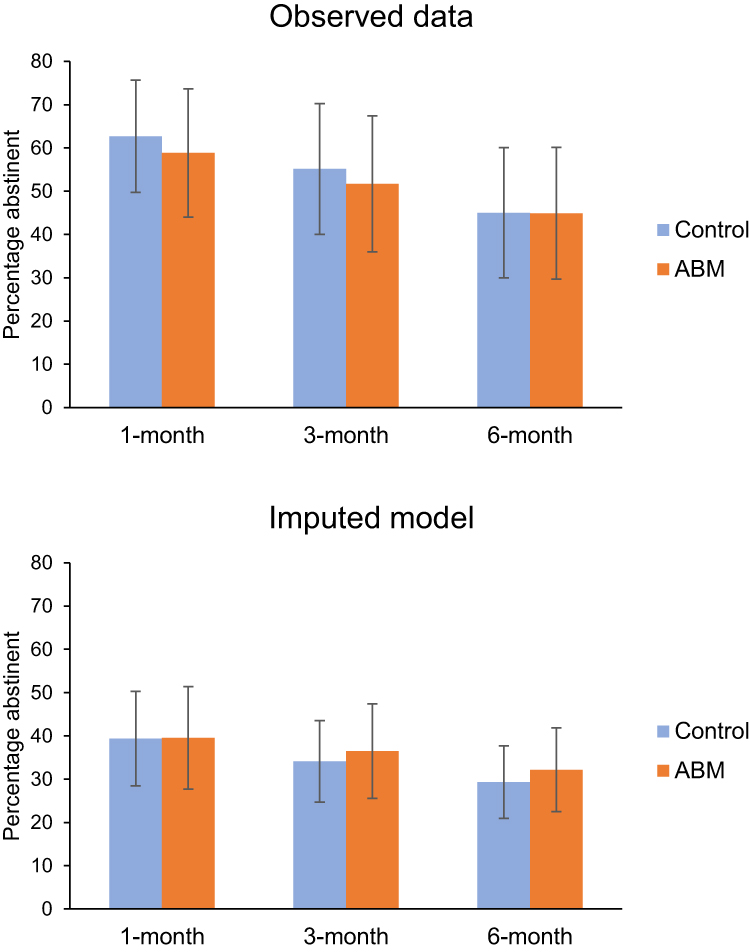 |
Figure 2 Predicted marginal percentages from mixed-effects logistic regression model of proportions of participants reporting past-month abstinence from alcohol at each follow-up. The top panel shows results from the model only using observed data, while the bottom panel shows results based on the assumption that participants lost to follow-up were not abstinent. Error bars show 95% confidence intervals. |
Secondary Clinical Outcomes
Supplementary Material describes results of mixed-effects models for past-week drinking days (Supplementary Table S1), past-week HDDs (Supplementary Table S2), past-week standard drinks (Supplementary Table S3), AUDIT scores (Supplementary Table S4), SDS scores (Supplementary Table S5), CEQ-F scores (Supplementary Table S6), ATOP psychological health (Supplementary Table S7), ATOP physical health (Supplementary Table S8), ATOP quality of life (Supplementary Table S9), DASS-21 depression (Supplementary Table S10), DASS-21 anxiety (Supplementary Table S11), DASS-21 stress (Supplementary Table S12), and SHAPS (Supplementary Table S13). None of these analyses suggested that ApBM affected outcomes. There was also no significant difference between groups in survival analysis of time until return to subsequent substance use withdrawal or rehabilitation or alcohol-related emergency department or hospital inpatient admission.
Participant Ratings of the App
Figure 3 shows the proportions of participants endorsing each response option for the six app rating items (and numerical data used to construct Figure 3 are provided in Supplementary Table S14). When asked if the app had positive effects (helping reduce alcohol use or cravings; or increasing interest or engagement in healthy activities and positive goals), the most common response was “unsure”, with few participants strongly agreeing or disagreeing. When asked if the app had harmful effects (causing participants to drink or crave alcohol more), most participants disagreed, with only four participants (8%) in the ApBM group feeling it had increased cravings, and no participants feeling it increased their alcohol use. Pearson’s chi-squared tests did not detect significant differences between groups in distributions of responses (all ps > 0.076).
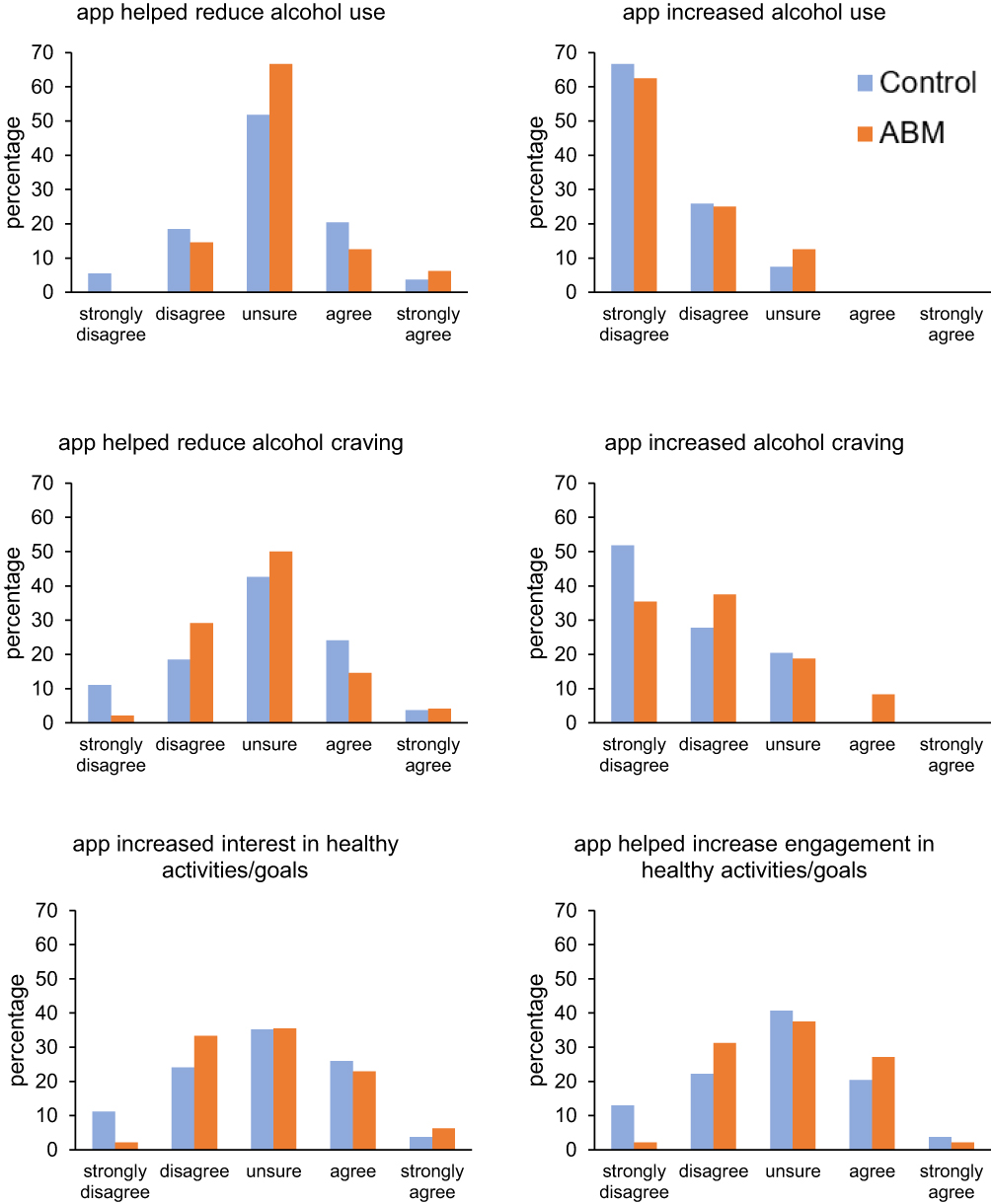 |
Figure 3 Percentages of participants endorsing each response option for the six ratings of the app. |
Assessment of Blinding Success
Forty-seven controls and 44 ApBM participants completed the allocation guessing item at their 6-month follow-up. Of these participants, 21 controls (45%) and 26 ApBM participants (59%) guessed they received an active intervention (χ2(1) = 1.89, p = 0.169).
Post-Hoc Exploratory Analyses of Past-month Abstinence
Does Duration of Residential Treatment Episode Moderate ApBM’s Effect on Abstinence?
Given the wide range in duration of the residential treatment episode participants underwent prior to accessing the app (9–103 days), we repeated the analyses of past-month abstinence to test whether duration of residential treatment moderated the size of ApBM’s effect on abstinence. These models are shown in Table 5. Both the observed data and imputed models indicated main effects of residential treatment duration, suggesting that longer residential treatment predicted higher odds of abstinence. We noted that the group × duration interaction approached significance in the observed data analysis (p = 0.081) and was significant in the imputed analyses (p = 0.045). To visualise the significant interaction in the imputed analysis, we trichotomised treatment durations to create short (9–28 days, n = 50), medium (29–36 days, n = 43), and long (37–103 days, n = 41) categories and generated estimated proportions abstinent for each duration category in each group at each follow-up (see Figure 4). Figure 4 suggests that this moderation effect arises from a tendency for ApBM participants to have higher abstinence rates than controls among participants with shorter residential treatment durations, which is lost, or even reversed, in those with longer treatment durations.
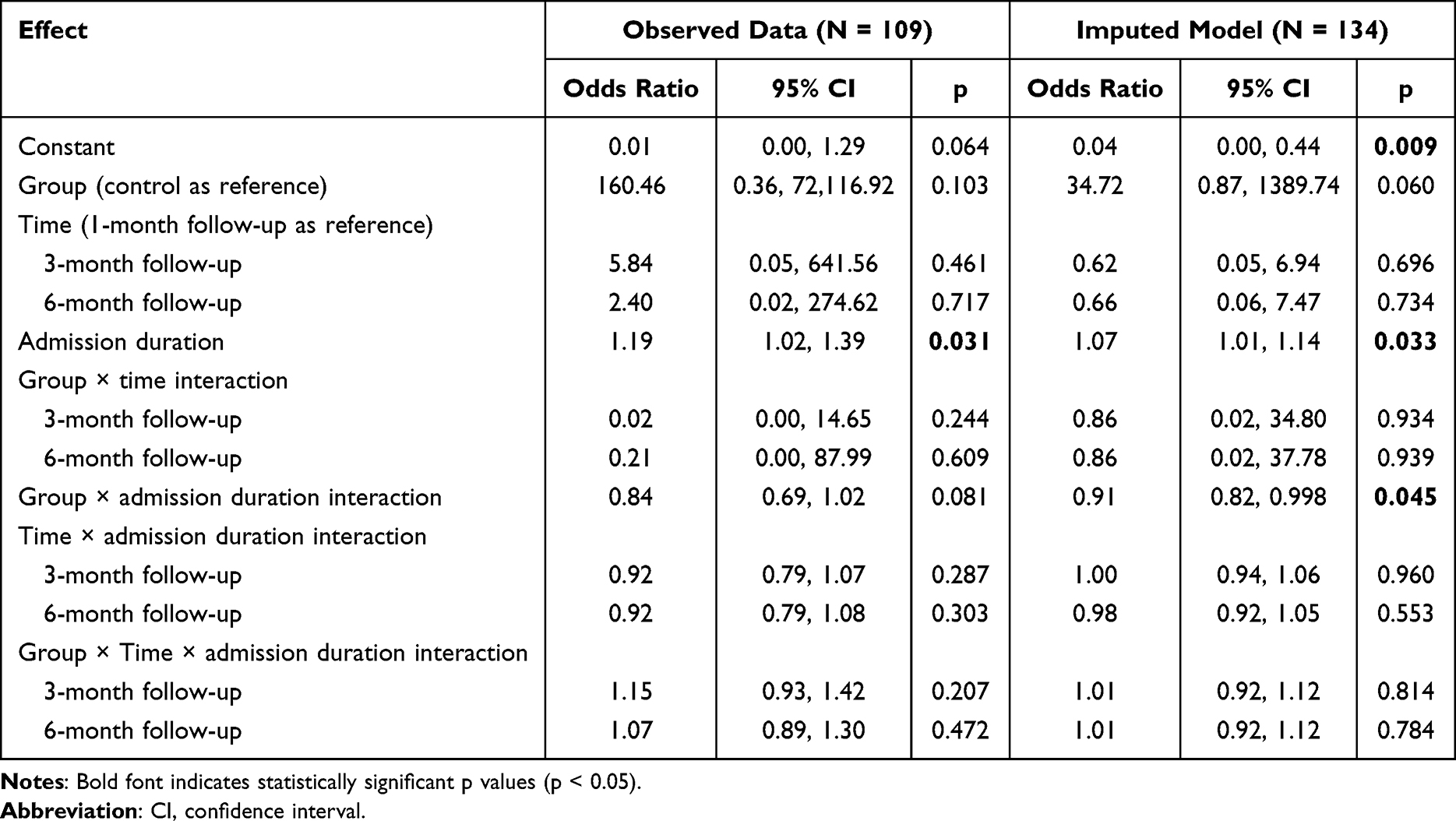 |
Table 5 Results of Mixed-Effects Logistic Regression Analysis of Past-Month Abstinence at Follow-Ups, Including Duration of Residential Treatment as a Moderator |
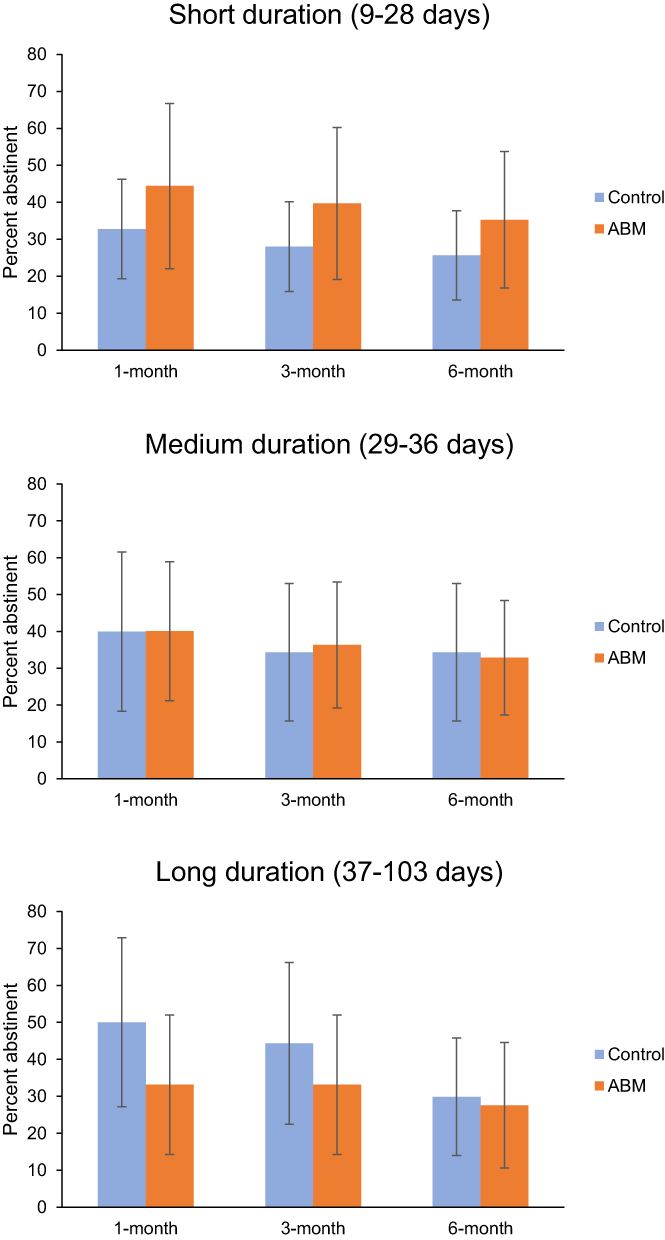 |
Figure 4 Predicted past-month abstinence rates (based on imputed outcomes) at follow-ups in participants whose index residential treatment admission was 9–28 days (top; n = 50), 29–36 days (middle; n = 43), or 37–103 days (bottom; n = 41). Error bars show 95% confidence intervals. |
Association Between Number of ApBM Sessions Completed and Odds of Abstinence
Within the ApBM group participants who completed the 1-month follow-up, each additional session of ApBM completed during the first 28 days after installing the app predicted a 25% increase in odds of past-month abstinence at the 1-month follow-up (ie., OR = 1.25 [95% CI: 1.03, 1.52], p = 0.021). However, this association became non-significant at the 3-month (OR = 1.13 [95% CI: 0.97, 1.32], p = 0.127) and 6-month follow-up (OR = 1.04 [95% CI: 0.90, 1.20], p = 0.618).
Abstinence Outcomes in Participants Who Installed the App Within 1 Week of Discharge
The app was intended, in this trial, to be installed soon after discharge from residential treatment to be tested as a relapse-prevention tool. However, 11% of participants (n = 15) took more than a week after discharge to install the app, with the delay between discharge and installation ranging up to 87 days. Hence, to test the app’s performance in conditions closer to its intended use, we repeated the primary analysis excluding participants who installed the app more than 7 days after discharge. However, these analyses did not show any evidence for differences between groups (see Supplementary Table S15).
Discussion
Analysis of our primary outcome found no significant effect of providing a personalised ApBM smartphone app to people recently discharged from residential AUD treatment on abstinence rates at the 3-month post-intervention follow-up. Nor did past-month abstinence rate differ between groups at either of the secondary timepoints at which it was measured (1 month or 6 months after the end of the 4-week ApBM app intervention). Other psychological and clinical variables also showed no significant effects of ApBM.
Findings did, however, support the effectiveness of the residential treatment programs from which participants were recruited – it is remarkable that, as noted in the Supplement, almost half of participants no longer met DSM-5 criteria for AUD at the 6-month follow-up, given participants’ AUD severity at baseline. Analyses of secondary outcomes related to quantity and frequency of alcohol consumption and presence and severity of AUD suggested substantial average improvements following rehabilitation treatment (see Supplement for details). However, the magnitude of these changes did not differ significantly between groups. Hence, these outcomes are likely related to benefits of engaging in residential treatment, along with non-specific effects, eg., of participants’ motivation, rather than their use of the ApBM app.
Our lack of any findings supporting efficacy contrasts with findings from multiple previous RCTs where ApBM was delivered during residential treatment (using computers and joysticks, rather than a smartphone app), which found that rate of relapse was reduced (typically by approximately 10%) at follow-up intervals ranging from 2 weeks to 1 year.3,10,13–18 It also contrasts with the two other RCTs of the same app (AAT-App) used in the present study which, despite not finding significant effects at either trials’ primary outcome (week 4), both found that the ApBM group reduced drinking more than sham controls at a secondary endpoint (after 2 weeks in older adults who were drinking at hazardous levels;32 at 3-month follow-up in AUD outpatients).31 However, as is typical of people accessing residential treatment, this trial’s sample tended to have more severe AUD than participants in the other two RCTs of AAT-App. Given this high severity, participants may have required a more structured, prolonged, or intensive ApBM intervention to derive benefits. Previous trials that delivered ApBM during residential treatment, with sessions administered on-site by treatment or research staff in a therapeutic context that reinforced recovery motivations, could ensure that most participants completed the number and frequency of sessions consistent with their protocol. The less-structured, unsupervised app-based delivery in the present trial relied on participants, who had already exited residential treatment, to remember to complete sessions in response to app prompts, resulting in substantial variance in the actual number of sessions completed. Indeed, exploratory post-hoc analyses found that participants who completed more ApBM sessions were more likely to report abstinence at the 1-month follow-up. While this post-hoc analysis cannot be interpreted as confirming causality, it does suggest the hypothesis that a more intensive schedule of ApBM sessions could yield positive effects in this setting in future research.
The interval between discharge and app installation also varied between participants. Since not all participants installed the app immediately upon discharge, it is possible that this also resulted in some participants only installing the app after a first lapse to alcohol use, undermining the intention for the app to be used as a relapse-prevention measure. Future trials could address this by having treatment service staff facilitate app installation as part of the discharge process.
The exploratory post-hoc finding that duration of residential treatment moderated the association between ApBM and abstinence suggests that future studies may be more likely to detect a positive effect of post-discharge smartphone ApBM if they focus on people who received briefer periods of residential treatment (eg., withdrawal treatment only). Briefer periods of residential treatment may be less effective at preparing clients to resist impulses to consume alcohol, hence leaving a vulnerability that post-discharge ApBM helps ameliorate. Clients who remain in residential treatment for longer periods undergo more sustained psychotherapeutic interventions and interaction with other clients, which emphasise the negative consequences of alcohol use, and further reinforce clients’ recovery-oriented motivations. According to some theoretical models, ApBM’s efficacy (when effective) is driven by the formation of negative and avoidance-related inferential evaluations of alcohol.44 However, if these have already been substantially reinforced by prolonged residential treatment, a relatively minimal program of smartphone ApBM may not have as much additional benefit.
Participants’ subjective ratings of the app’s effects supported the safety of the intervention. Despite the training tasks involving exposure to alcohol-related stimuli, participants did not feel that it exacerbated alcohol use, and only a small number of participants felt that ApBM increased craving. Despite differences between the ApBM and sham training schedules, the two groups appeared to have similar subjective perceptions of the app’s effects (Figure 3). Moreover, when blinding was assessed at 6-month follow-up, approximately half of each group believed they received an active intervention. Hence, it is unlikely that outcomes were substantially influenced by differences between groups in expectancy effects.
Several limitations affected these analyses. Our sample size was substantially smaller than the planned target, meaning the study had only 39% power to detect an effect size similar to what we previously observed using computer/joystick-delivered ApBM during withdrawal treatment.15 At the time we applied for funding, we overestimated the likely recruitment rate. In part, this was due to recruitment commencing while COVID-19 pandemic-related restrictions or changes in practice were still in effect at services, causing delays in commencing recruitment at some services, temporary suspensions of recruitment at some services which experienced COVID-19 outbreaks, and generally slower recruitment than anticipated. Hence, our originally intended study timeline, which was based on an ambitious estimate of likely recruitment rate, allowed insufficient time to recruit a sample that would have provided adequate statistical power. We therefore suggest that researchers planning future studies in similar settings use very conservative a priori estimates of recruitment rates.
Our reliance on self-reported alcohol consumption, where recall errors or social desirability bias may introduce inaccuracies, may have further impacted precision of our analyses. Post-intervention app ratings may have been affected by attrition bias, eg., if participants with less positive experiences using the app were more likely to disengage and therefore not complete post-intervention measures. Finally, demographic characteristics of the sample (eg., 90% White, 97% with English as their first language) may limit generalisability of our findings, eg., to other national or cultural contexts. Moreover, participants were predominantly recruited from private treatment services and were required to own a working, recently updated smartphone. These factors may have led to under-representation of more socio-economically disadvantaged people, further limiting generalisability.
In summary, this study suggested that providing personalised smartphone-delivered ApBM to clients following discharge from residential alcohol rehabilitation treatment was safe and acceptable, although this conclusion may be influenced by attrition bias. However, outcomes provided no significant evidence for smartphone ApBM’s clinical efficacy in this population and context. Nonetheless, exploratory analyses suggested the possibility of better efficacy for patients with shorter treatment durations, though this underpowered analysis would require replication in a fully powered study. Additionally, people who engaged in more ApBM sessions had higher rates of abstinence, although we note that correlational analysis does not infer causality. Future research could examine whether residential treatment outcomes could be bolstered by a more structured and/or intensive delivery of smartphone ApBM; whether this intervention could be more effective in shorter-duration residential treatment settings; or whether an ApBM app could have additive effects if delivered following computer-based ApBM during residential treatment.
Data Sharing Statement
Due to conditions of ethical approval, we do not intend to make the dataset accessible to the general public. However, researchers interested in accessing deidentified individual participant data may contact the chief investigator, Professor Victoria Manning ([email protected]) with a proposal explaining their intended analyses. Granting access to other researchers to use deidentified data will require completion of data sharing agreements between Monash University and the researchers seeking to access the data. Data will be retained for 7 years after the completion of reporting of trial outcomes but may be unavailable after that point.
Acknowledgments
The authors thank Samuel K. Liu, Josephine C. B. Paxie, Mietta C. L. Bell, Thomas McCullagh, and Natasha Izwan for their contributions to participant recruitment, data collection, and data cleaning. We also thank staff at the participating services (including Eastern Health, The Melbourne Clinic, Ramsay Clinic Albert Road, Arrow Health, and Wyndham Clinic Private Hospital) who assisted with project set-up, referring clients, and facilitating recruitment, including: Aine Finnan, Angela Komiti, Anthony Hew, Ayodya Walpola Lokuge, Bonnie Jones, Breanna Blair, Brogan Douglas, Elizabeth Mwaura, Ferghal Armstrong, Gillian Benington, Goke Okedara, Helen Looby, Jolie Tse, Kon Mrnjaus, Laoise Redmond, Mananya “Fern” Kaewborisut, Mary Quick, Melanie Hurley, Nadine Hartnett, Nathan Dowling, Pia O’Leary, Rebecca Wardan, Tina Garlick, Trudy Trice, Vicky Phan, and Wendy Davis. We acknowledge ANT Development Studios for developing the app, and we thank Monash University eSolutions staff, including Faisha Surjatin and Paul McIntosh, for providing additional technical support to maintain app functioning during the trial. We thank Ellie McSheedy and Ian Logan for their assistance with project administration and data management. We acknowledge Anthony Barnett’s role in helping to obtain funding. This work was supported by Helix at Monash University and by using the Monash University managed Qualtrics Plus platform. Finally, we thank the participants for their time and data.
Funding
This project was funded by a grant from HCF Research Foundation. HCF Research Foundation played no role in study design or in the collection, management, analysis, interpretation, or publication of data.
Disclosure
In addition to salary support for Dr Joshua Garfield and Hugh Piercy from the HCF Research Foundation grant which funded this study, the authors report non-financial support from Ramsay Clinic Albert Road, The Melbourne Clinic, Arrow Health, Eastern Health, and Wyndham Clinic Private Hospital during the conduct of the study. All authors declare that they have no conflicts of interests relevant to this work.
References
1. World Health Organization. Global status report on alcohol and health and treatment of substance use disorders. Geneva: World Health Organization; 2024.
2. AIHW. Alcohol and other drug treatment services in Australia annual report: Australian Institute of Health and Welfare. 2025. Available from: https://www.aihw.gov.au/reports/alcohol-other-drug-treatment-services/alcohol-other-drug-treatment-services-australia/contents/about.
3. Rinck M, Wiers RW, Becker ES, Lindenmeyer J. Relapse prevention in abstinent alcoholics by cognitive bias modification: clinical effects of combining approach bias modification and attention bias modification. J Consulting Clin Psychol. 2018;86(12):1005–20. doi:10.1037/ccp0000321
4. Staiger PK, Liknaitzky P, Lake AJ, Gruenert S. Longitudinal Substance Use and Biopsychosocial Outcomes Following Therapeutic Community Treatment for Substance Dependence. J Clin Med. 2020;9(1):118. doi:10.3390/jcm9010118
5. Vanderplasschen WOI, Colpaert KAG, Broekaert EKM. Determinants of relapse and re-admission among alcohol abusers after intensive residential treatment. Arch Public Health. 2010;67(4):194. doi:10.1186/0778-7367-67-4-194
6. Manning V, Garfield JBB, Best D, et al. Substance use outcomes following treatment: findings from the Australian Patient Pathways Study. Aust N Z J Psychiatry. 2017;51(2):177–189. doi:10.1177/0004867415625815
7. Garfield JBB, Piccoli LR, Whelan D, et al. The effect of approach bias modification during alcohol withdrawal treatment on craving, and its relationship to post-treatment alcohol use in a randomised controlled trial. Drug Alcohol Depend. 2022;239:109621. doi:10.1016/j.drugalcdep.2022.109621
8. Hansen EM, Mejldal A, Nielsen AS. Predictors of Readmission Following Outpatient Treatment for Alcohol Use Disorder. Alcohol Alcohol. 2020;55(3):291–298. doi:10.1093/alcalc/agaa018
9. Wiers RW, Gladwin TE, Hofmann W, Salemink E, Ridderinkhof KR. Cognitive Bias Modification and Cognitive Control Training in Addiction and Related Psychopathology: mechanisms, Clinical Perspectives, and Ways Forward. Clin Psychol Sci. 2013;1(2):192–212. doi:10.1177/2167702612466547
10. Eberl C, Wiers RW, Pawelczack S, Rinck M, Becker ES, Lindenmeyer J. Approach bias modification in alcohol dependence: do clinical effects replicate and for whom does it work best? Developmental Cognitive Neurosci. 2013;4:38–51. doi:10.1016/j.dcn.2012.11.002
11. Laurens MC, Postel MG, Brusse-Keizer M, et al. Augmenting outpatient alcohol treatment as usual with online approach bias modification training: a double-blind randomized controlled trial. Addict Behav. 2023;142:107630. doi:10.1016/j.addbeh.2023.107630
12. Loijen A, Rinck M, Walvoort SJW, Kessels RPC, Becker ES, Egger JIM. Modification of Automatic Alcohol-Approach Tendencies in Alcohol-Dependent Patients with Mild or Major Neurocognitive Disorder. Alcohol Clin Exp Res. 2018;42(1):153–161. doi:10.1111/acer.13529
13. Manning V, Garfield JBB, Staiger PK, et al. Effect of Cognitive Bias Modification on Early Relapse Among Adults Undergoing Inpatient Alcohol Withdrawal Treatment: a Randomized Clinical Trial. JAMA Psychiatry. 2021;78(2):133–140. doi:10.1001/jamapsychiatry.2020.3446
14. Wiers RW, Eberl C, Rinck M, Becker ES, Lindenmeyer J. Retraining Automatic Action Tendencies Changes Alcoholic Patients’ Approach Bias for Alcohol and Improves Treatment Outcome. Psychol Sci. 2011;22(4):490–497. doi:10.1177/0956797611400615
15. Manning V, Garfield JBB, Reynolds J, et al. Alcohol use in the year following approach bias modification during inpatient withdrawal: secondary outcomes from a double-blind, multi-site randomized controlled trial. Addiction. 2022;117(11):2837–2846. doi:10.1111/add.15989
16. Manning V, Staiger PK, Hall K, et al. Cognitive Bias Modification Training During Inpatient Alcohol Detoxification Reduces Early Relapse: a Randomized Controlled Trial. Alcohol Clin Exp Res. 2016;40(9):2011–2019. doi:10.1111/acer.13163
17. Salemink E, Rinck M, Becker E, Wiers RW, Lindenmeyer J. Does comorbid anxiety or depression moderate effects of approach bias modification in the treatment of alcohol use disorders? Psychol Addict Behav. 2022;36(5):547–554. doi:10.1037/adb0000642
18. Schenkel EJ, Rinck M, Wiers RW, et al. Implementing Approach-Bias Modification as Add-On to Varieties of Clinical Treatment for Alcohol Use Disorders: results of a Multicenter RCT. Eur Addict Res. 2024;30(2):94–102. doi:10.1159/000537811
19. Verdejo-Garcia A, Rezapour T, Giddens E, et al. Cognitive training and remediation interventions for substance use disorders: a Delphi consensus study. Addiction. 2023;118(5):935–951. doi:10.1111/add.16109
20. Vrijsen JN, Grafton B, Koster EHW, et al. Towards implementation of cognitive bias modification in mental health care: state of the science, best practices, and ways forward. Behaviour Research Ther. 2024;179:104557. doi:10.1016/j.brat.2024.104557
21. Crane D, Garnett C, Michie S, West R, Brown J. A smartphone app to reduce excessive alcohol consumption: identifying the effectiveness of intervention components in a factorial randomised control trial. Sci Rep. 2018;8(1):4384. doi:10.1038/s41598-018-22420-8
22. Garnett C, Michie S, West R, Brown J. Updating the evidence on the effectiveness of the alcohol reduction app, Drink Less: using Bayes factors to analyse trial datasets supplemented with extended recruitment. F1000Research. 2019;8(114):114. doi:10.12688/f1000research.17952.2
23. Peerenboom N, Guzman NV, Kvamme T, Ritou V, Casero V, Voon V. Developing digital interventions for a post-Covid world: a smartphone-based approach-avoidance training to reduce alcohol craving. Scandinavian J Psychol. 2024;65(2):264–274. doi:10.1111/sjop.12974
24. Laurens MC, Pieterse ME, Brusse-Keizer M, et al. Alcohol Avoidance Training as a Mobile App for Problem Drinkers: longitudinal Feasibility Study. JMIR mHealth Health. 2020;8(4):e16217. doi:10.2196/16217
25. Stacy AW, Wiers RW. Implicit cognition and addiction: a tool for explaining paradoxical behavior. Annu Rev Clin Psychol. 2010;6(1):551–575. doi:10.1146/annurev.clinpsy.121208.131444
26. Bolt GL, Piercy H, Barnett A, Manning V. ‘A circuit breaker’ – interrupting the alcohol autopilot: a qualitative exploration of participants’ experiences of a personalised mHealth approach bias modification intervention for alcohol use. Addict Behav Rep. 2022;16:100471. doi:10.1016/j.abrep.2022.100471
27. Manning V, Bell MCL, Garfield JBB, et al. “A tool in a toolbox”: patient engagement with a gamified and personalised approach bias modification app to reduce harmful alcohol consumption – a qualitative study. Addiction Sci Clin Pract. 2026;21(1):22. doi:10.1186/s13722-026-00646-6
28. Manning V, Whelan D, Piercy H, et al. Approach With Caution: a Pilot Randomised Controlled Trial of Approach Bias Modification for People Undergoing Residential Treatment for Methamphetamine Use Disorder. Drug Alcohol Rev. 2026;45(4):e70151. doi:10.1111/dar.70151
29. Manning V, Piercy H, Garfield JBB, Lubman DI. Personalized Approach Bias Modification Smartphone App (“SWIPE”) to Reduce Alcohol Use Among People Drinking at Hazardous or Harmful Levels: protocol for an Open-Label Feasibility Study. JMIR Res Protoc. 2020;9(8):e21278. doi:10.2196/21278
30. Manning V, Piercy H, Garfield JBB, Clark SG, Andrabi MN, Lubman DI. A Personalized Approach Bias Modification Smartphone App (“SWiPE”) to Reduce Alcohol Use: open-Label Feasibility, Acceptability, and Preliminary Effectiveness Study. JMIR mHealth Health. 2021;9(12):e31353. doi:10.2196/31353
31. Garfield JBB, Rowland B, Liu SK, et al. Efficacy of a personalised alcohol approach bias modification smartphone app in people accessing outpatient alcohol use disorder treatment: a randomised controlled trial. Addiction. 2026;121(1):82–93. doi:10.1111/add.70184
32. Bolt GL, Rowland B, Piercy H, Bradshaw J, Lubman DI, Manning V. AAT-App+: a double-blind, pilot randomised controlled trial of a novel personalised smartphone intervention to reduce hazardous and harmful alcohol consumption among middle–older adults. Addict Behav. 2026;173:108560. doi:10.1016/j.addbeh.2025.108560
33. National Health and Medical Research Council, Australian Research Council, Universities Australia. National Statement on Ethical Conduct in Human Research 2007 (Updated 2018); 2018.
34. Sobell LC, Sobell MB. Timeline Followback User’s Guide: A Calendar Method for Assessing Alcohol and Drug Use. Toronto: Addiction Research Foundation; 1996.
35. National Health and Medical Research Council. Australian Guidelines to Reduce Health Risks From Drinking Alcohol. Canberra: National Health and Medical Research Council; 2020. Available from: https://www.nhmrc.gov.au/health-advice/alcohol.
36. First MB, Williams JBW, Karg RS, Spitzer RL. User’s Guide for the Structured Clinical Interview for DSM-5 Disorders, Research Version (SCID-5-RV). Arlington, Virginia: American Psychiatric Association; 2015.
37. Saunders JB, Aasland OG, Babor TF, de la Fuente JR, Grant M. Development of the Alcohol Use Disorders Identification Test (AUDIT): WHO Collaborative Project on Early Detection of Persons with Harmful Alcohol Consumption--II. Addiction. 1993;88(6):791–804. doi:10.1111/j.1360-0443.1993.tb02093.x
38. Gossop M, Darke S, Griffiths P, et al. The Severity of Dependence Scale (SDS): psychometric properties of the SDS in English and Australian samples of heroin, cocaine and amphetamine users. Addiction. 1995;90(5):607–614. doi:10.1046/j.1360-0443.1995.9056072.x
39. May J, Andrade J, Kavanagh DJ, et al. The Craving Experience Questionnaire: a brief, theory-based measure of consummatory desire and craving. Addiction. 2014;109(5):728–735. doi:10.1111/add.12472
40. Ryan A, Holmes J, Hunt V, et al. Validation and implementation of the Australian Treatment Outcomes Profile in specialist drug and alcohol settings. Drug Alcohol Rev. 2014;33(1):33–42. doi:10.1111/dar.12083
41. Antony MM, Bieling PJ, Cox BJ, Enns MW, Swinson RP. Psychometric properties of the 42-item and 21-item versions of the Depression Anxiety Stress Scales in clinical groups and a community sample. Psychological Assessment. 1998;10(2):176–181. doi:10.1037/1040-3590.10.2.176
42. Snaith RP, Hamilton M, Morley S, Humayan A, Hargreaves D, Trigwell P. A Scale for the Assessment of Hedonic Tone the Snaith–Hamilton Pleasure Scale. Br J Psychiatry. 1995;167(1):99–103. doi:10.1192/bjp.167.1.99
43. Garfield JBB, Whelan D, Piercy H, Barnett A, Manning V. AAT-App Rehabilitation Trial: the effect of smartphone-delivered cognitive training on relapse and treatment re-admission among patients leaving residential alcohol treatment: Australian New Zealand Clinical Trials Registry (ANZCTR). 2022. Available from: https://anzctr.org.au/Trial/Registration/TrialReview.aspx?ACTRN=12622001245785.
44. Van Dessel P, Hughes S, De Houwer J. How Do Actions Influence Attitudes? An Inferential Account of the Impact of Action Performance on Stimulus Evaluation. Personality Soc Psychol Rev. 2019;23(3):267–284. doi:10.1177/1088868318795730
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Alcohol Misuse, Marital Functioning and Marital Instability: An Evidence-Based Review on Intimate Partner Violence, Marital Satisfaction and Divorce
Kulak JA, Heavey SC, Marsack LF, Leonard KE
Substance Abuse and Rehabilitation 2025, 16:39-53
Published Date: 12 February 2025
Needs and Challenges to Improve Rehabilitative Care for Parents with Substance Use Disorder - A Qualitative Study from the Expert’s Perspective
Hoffmann L, Stullich A, Stephan J, Gehrmann J, Richter M
Substance Abuse and Rehabilitation 2025, 16:271-282
Published Date: 17 October 2025