Back to Journals » Journal of Experimental Pharmacology » Volume 11
The Effect of Sertraline on Hemodynamic Parameters and Nitric Oxide Production in Isolated Rat Hearts Subjected to Ischemia and Reperfusion
Authors Grotthus B ![]() , Szeląg A
, Szeląg A ![]()
Received 18 March 2019
Accepted for publication 10 October 2019
Published 23 December 2019 Volume 2019:11 Pages 149—158
DOI https://doi.org/10.2147/JEP.S209085
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Bal Lokeshwar
Bartosz Grotthus, Adam Szeląg
Department of Pharmacology, Wroclaw Medical University, Wroclaw, Poland
Correspondence: Bartosz Grotthus
Department of Pharmacology, Wroclaw Medical University, Ul. Jana Mikulicza-Radeckiego 2, Wrocław 50-345, Poland
Tel +48 71 784 14 40
Fax +48 71 784 14 38
Email [email protected]
Purpose: The aim of the study was to investigate the effect of sertraline on the rat heart during ischemia and reperfusion and to determine its effect on NO production.
Materials and methods: The study was performed on isolated rat hearts. Hearts from three groups were perfused with sertraline at three different concentrations and subjected to global ischemia and reperfusion. Hearts from the other three groups were perfused with the same concentrations of sertraline but without the ischemia/reperfusion process. Two control groups were perfused with the Krebs-Henseleit solution only with and without ischemia/reperfusion process. Coronary flow (CF), heart rate (HR), left ventricular developed pressure (LVDP) and maximum rate of rise of left ventricular pressure (dP/dt max) were measured. Perfusate effluent was collected to determine creatine phosphokinase (CPK) and nitrate plus nitrite (NOx) levels.
Results: In non-ischemic groups, sertraline at the concentration of 10 μmol/L exerts a strong vasodilatory effect on CF, and after a short positive inotropic effect, it exerts a strong inotropic and chronotropic negative effect on isolated rat hearts and causes a direct damage to cardiomyocytes. At the concentration of 1 μmol/L, sertraline exerts an increasing negative inotropic effect. There were no hemodynamic differences between any of groups of hearts subjected to reperfusion. Sertraline had no effect on the nitric oxide concentration in coronary effluent neither in rat hearts subjected to ischemia/reperfusion nor in non-ischemic conditions.
Conclusion: Sertraline at dose 10 μmol/L exerts a strong vasodilatory effect on coronary flow, and after a short positive inotropic effect, it exerts a strong negative effect on isolated rat hearts, causing a direct damage to cardiomyocytes. Sertraline had no effect on the nitric oxide concentration in coronary effluent.
Keywords: heart, ischemia, perfusion, sertraline, nitric oxide
Introduction
The class of drugs most commonly used for the treatment of people suffering from concurrent depression and ischemic heart disease are selective serotonin reuptake inhibitors (SSRIs).1,2 Those drugs are considered to be safer for the heart compared to tricyclic antidepressive drugs, and the results of some retrospective studies suggest that they may even exert a cardioprotective effect.3,4 On the other hand, there are also reports of possible side effects of SSRIs. Therefore, they may have some adverse effects on the heart.5–7
The exact mechanism of how these drugs may act on the heart remains unknown. Serotonin (5-hydroxytryptamine; 5-HT) is a neurohormonal substance demonstrating a direct impact on some cardiovascular functions. The antiplatelet effect of SSRIs is suggested,4,8 along with other mechanisms, including the effect of SSRIs on the immune system9 or on the autonomic nervous system.10,11 A direct effect of this class of drugs on coronary blood vessels is also considered.12
Nitric oxide (NO) is a strong vasodilator, able to restore a normal perfusion of ischemic tissues. NO plays protective roles in the ischemic heart via several mechanisms. Several ex vivo studies demonstrated that increasing NO levels, either by applying NO donors, NO-dependent vasodilators, L-arginine supplementation, angiotensin-converting enzyme inhibitors, or others, functionally protects the heart from acute ischemia/reperfusion injury and/or infarct size development.13 But the role of NO in reperfusion is a more complex one. Generation of free oxygen radicals is increased during reperfusion, depending on duration and severity of the preceding ischemia; thus, with more severe and prolonged ischemia, free radical generation during the subsequent reperfusion is enhanced,14 leading to the increased formation of peroxynitrite (ONOO−). It is now understood that many of toxic actions of NO are not directly due to NO itself, but are mediated via production of ONOO−, the reaction product of NO with O2−. Formation of ONOO− has been shown to contribute to several cardiovascular pathologies including the ischemia/reperfusion injury. High concentrations of peroxynitrite are thought to oxidize thiols or thioethers, to nitrate tyrosine residues, to nitrate and oxidize guanosine, to degrade carbohydrates, to initiate lipid peroxidation, and to cleave DNA.15
Data on the effect of SSRIs on nitric oxide metabolism in humans are contradictory. In the first study on that problem, Finkel et al suggested that paroxetine is an inhibitor of endothelial nitric oxide synthase (eNOS). The authors demonstrated that in patients with ischemic heart disease treated for depression, paroxetine caused a gradual decrease in the plasma concentration of nitric oxide metabolites (NOx).16 However, clinical trials conducted later demonstrated some completely different results. Lara et al found that following the 8-week paroxetine treatment of healthy volunteers, their plasma concentration of NOx increased by about 40% and returned to baseline after discontinuation of the treatment.17 Chrapko et al18 examined depressed patients and noticed some reduced plasma levels of NOx and a reduced activity of platelet NOS, compared to healthy volunteers. Eight weeks after the initiation of paroxetine treatment in patients with depression, the authors noticed an increase of NOx concentration to approximately 300% of the baseline value, and just to 40% in the control group. In the experiment conducted by Ikenouchi-Sugita et al, who compared effects of milnacipran (a selective serotonin and norepinephrine reuptake inhibitor) and paroxetine on the plasma NOx concentration in patients with depression, the authors demonstrated that paroxetine did not lead to any changes, and milnacipran caused a significant increase of the plasma NOx level.19 Thus, data from clinical studies are contradictory and do not allow a clear identification of whether and how could SSRIs affect the metabolism of nitric oxide.
Since data regarding the effect of SSRIs on the metabolism of nitric oxide do not allow a clear identification of whether and how do those drugs possibly affect the metabolism of NO, we tried to identify the effect of sertraline on isolated rat heart and nitric oxide production in non-ischemic and ischemic/reperfusion hearts.
Materials and Methods
The experiment was performed in accordance with NIH Guide for the Care and Use of Laboratory Animals and was approved by the 1st Local Ethics Committee on the Animal Research of the Institute of Immunology and Experimental Therapy Polish Academy of Sciences in Wroclaw. Permission number 53/2006.
Fifty-six male Buffalo rats (body weight 280–355 g) were anesthetized intraperitoneally (i.p.) with pentobarbital sodium (Biovet, Poland) 50 mg/kg. Each heart was excised, and the aorta was rapidly (within maximum 30 s) cannulated and perfused with the Krebs-Henseleit solution (NaCl 118.5 mmol/L; NaHCO3 25 mmol/L; KCl 4.75 mmol/L; CaCl2 1.41 mmol/L; MgSO4 × 7 H2O 1.19 mmol/L; KH2PO4 1.18 mmol/L; glucose 5.5 mmol/L) (all compounds purchased in Chempur, Poland) gassed with carbogen (95% O2, 5% CO2).
Perfusion was performed according to the Langendorff method20 using the S Series Isolated Working Heart Apparatus (ADInstruments GmbH, Germany). Every element of the apparatus was water coated with distilled running water warmed to maintain a temperature of the perfusate in all its parts during the entire study at 37ºC. All hemodynamic data were continuously collected (sample frequency 1kHz), processed and simultaneously shown on a computer monitor using LabChart® Pro v.6.1.3 software (AdInstruments GmbH, Germany).
Each heart was contained in a small water-coated chamber to maintain the physiological temperature. Perfusion was performed under constant pressure achieved by pumping the Krebs-Henseleit solution to the level of 95 cm above the heart (70 mmHg) pressure. Coronary flow (CF) was measured with a Doppler ultrasonic gauge placed just before the cardiac cannula. A fluid-filled latex balloon was inserted into the left ventricle. It was inflated to achieve the pressure of 10 mmHg during diastole of the heart and connected to a pressure transducer to measure the heart rate (HR), the left ventricular-developed pressure (LVDP), and the maximum rate of rise of left ventricular pressure (dPdt max). Measurements were started within 15 mins of the heart stabilization period and were referred to as baseline value (time 0 – start of the experiment). Hemodynamic data are shown in graphs in 5-min intervals.
Rats were divided randomly into eight groups (n=7). All hearts were subjected to 1-hr perfusion by one of two designed protocols:
- Four non-ischemic groups of hearts were subjected to 60 min long non-ischemic perfusion – the control group perfused with the Krebs-Henseleit solution, and three other groups with sertraline (Sigma-Aldrich, St. Louis, Missouri, USA) added to the perfusate between the 10th and the 50th minute after start of the experiment, at three concentrations: 0.1µmol/L, 1µmol/l, and 10µmol/L, respectively.
- Four ischemic/reperfusion groups of hearts – the control group was perfused with the Krebs-Henseleit solution, and three other groups with sertraline added to the perfusate at three concentrations: 0.1µmol/L, 1µmol/L, 10µmol/L, respectively, between the 10th and the 50th minute after the start of the experiment. Those groups were also subjected to twenty-minute ischemia, between the 20th and the 40th minute of the experiment. Ischemia was achieved by stopping the flow of fluid and lasted for 20 mins. Reperfusion was achieved by the restoration of the flow of the perfusate.
Hemodynamic Data
Values of each hemodynamic parameter were presented as a percentage change relative to the baseline value at the start of the experiment (100%) in order to facilitate the presentation of changes of those parameters. Baseline absolute values at experiment start ± SEM are shown in Table 1.
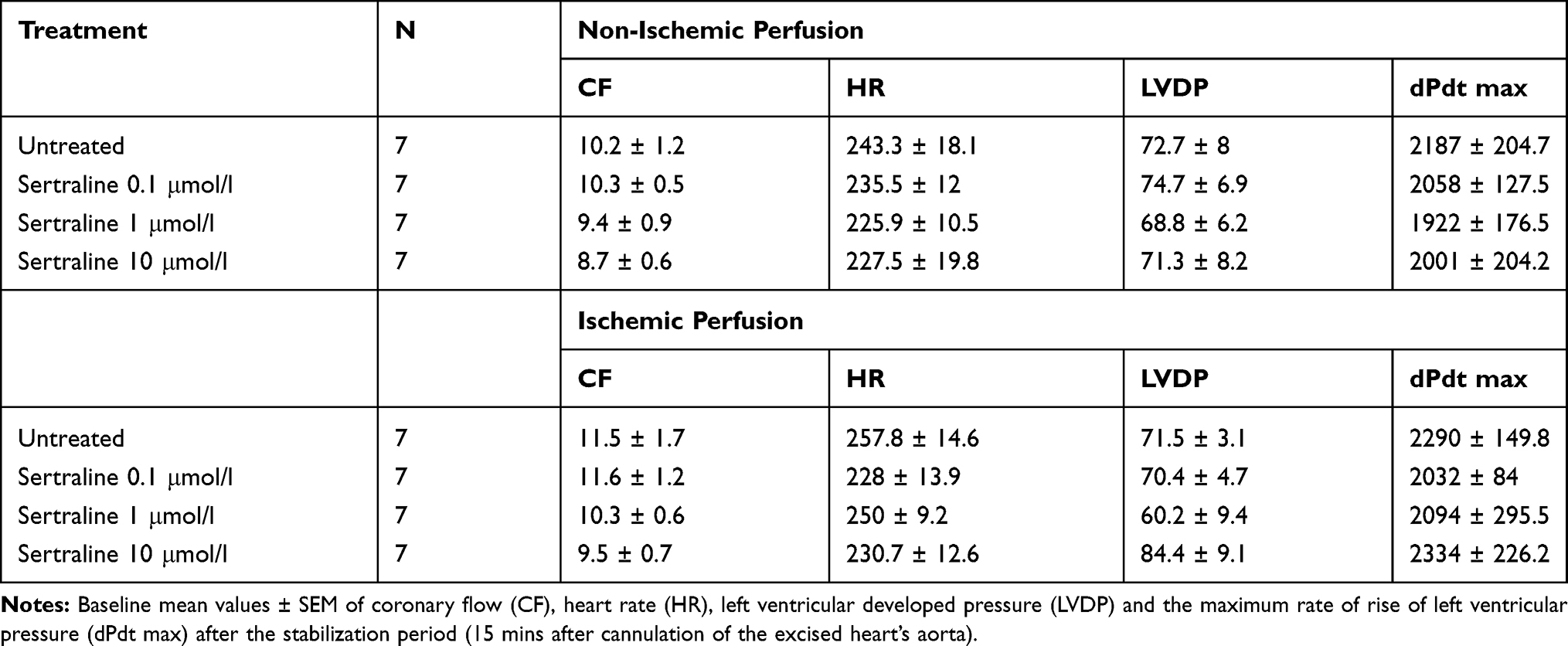 |
Table 1 Baseline Values of Hemodynamic Parameters of Isolated Hearts After Stabilization Period |
Biochemical Parameters
The total nitric oxide (NO) outflow in the effluent was collected in the 5th minute after the start of the experiment (baseline value); in the 15th minute of the experiment (after the start of the treatment) and in the 40th minute of the experiment (after reperfusion). NO formation was examined by the measurement of NOx (stable NO metabolites – nitrite and nitrate). The method used was a colorimetric determination using the commercial Total NO/Nitrite/Nitrate Assay (R&D Systems, UK). That assay determines nitric oxide concentrations based on the enzymatic conversion of nitrate to nitrite by nitrate reductase. The reaction is followed by a colorimetric detection of nitrite as an azo dye product of the Griess Reaction. The Griess reaction is based on a two-step diazotization reaction in which acidified NO2- produces a nitrosating agent, that reacts with sulfanilic acid to produce the diazonium ion. The ion is then coupled with N-(1-naphthyl)ethylenediamine to form the chromophoric azo-derivative, absorbing light at 540–570 nm.
Creatine phosphokinase (CPK) is an enzyme expressed by various tissues and cell types. It is assayed in blood tests as a marker of damage of CPK-rich tissue such as in myocardial infarction. CPK was repeatedly measured every 10 mins, from the 10th minute of experiment, using the Enzyline Kit CK NAC (Biomorieux, FranceIn the creatine kinase assay protocol, creatine kinase (CK) converts creatine into phosphocreatine and ADP. The phosphocreatine and ADP then react with the CK enzyme mix to form an intermediate, which reduces a colorless probe to a colored product with strong absorbance at λ= 450 nm.
Statistical Analysis
All values presented in graphs and tables are expressed as mean ± SEM Significant differences between groups were calculated using two-way analysis of variance (ANOVA) followed by the Dunnett’s post hoc test. Differences between groups were considered significant if the p value was <0.05. All calculations were performed using GraphPad® Prism v. 5.04 software.
Results
Nonischemic Perfusion
Hemodynamic Data
All hemodynamic data in both non-ischemic and ischemic/reperfusion groups were acquired every 5 mins (Figure 1).
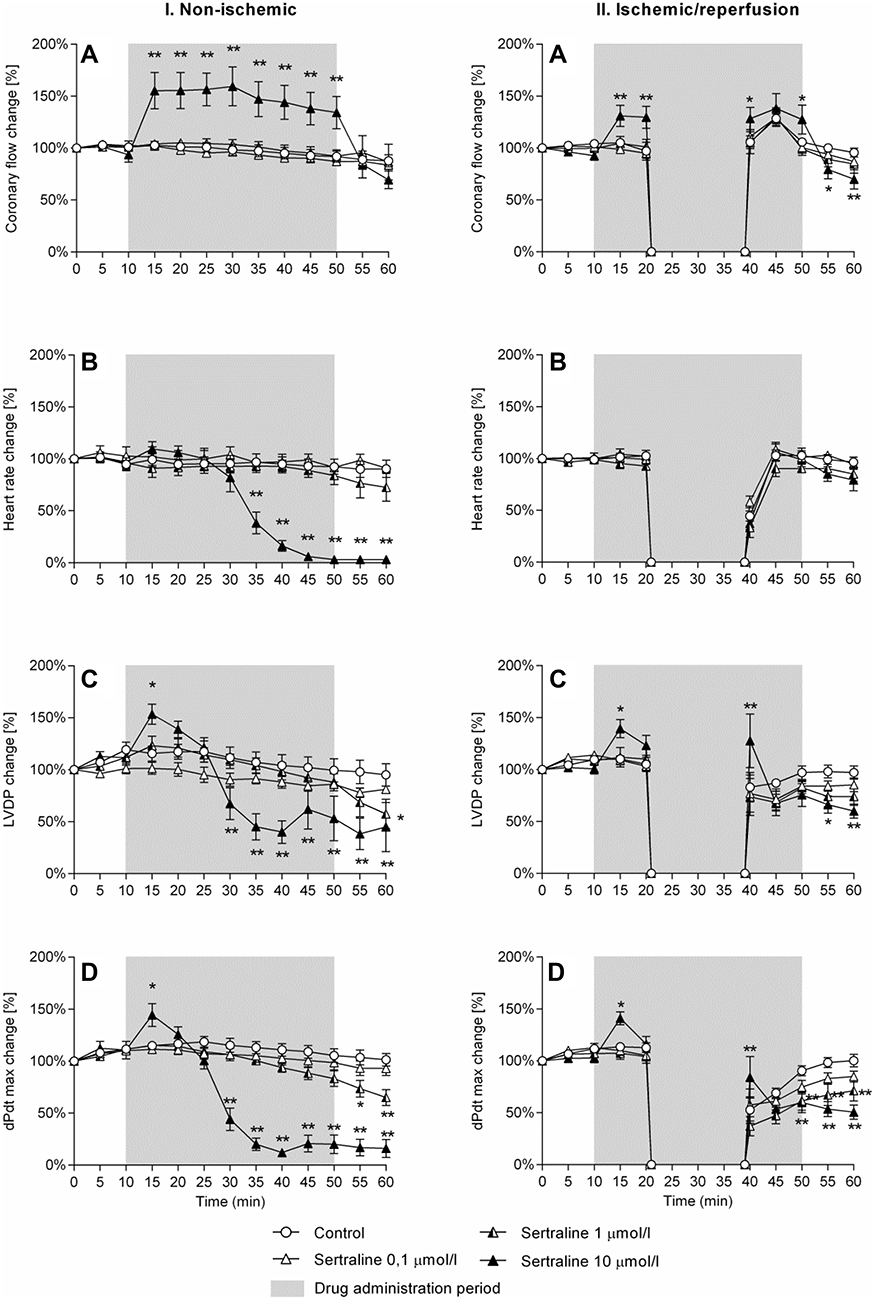 |
Figure 1 Effect of sertraline on changes of hemodynamic parameters in isolated rat heart. Changes of coronary flow (CF), heart rate (HR), left ventricular developed pressure (LVDP) and maximum rate of rise of left ventricular pressure (dPdt max) in isolated rat heart perfused in non-ischemic condition or subjected to 20-min ischemia and 20-min reperfusion. Values are means ± SEM of seven experiments. *p ≤ 0.05, **p ≤ 0.01 vs control group.` |
The most pronounced changes of hemodynamic parameters in non-ischemic hearts were observed in the group treated with sertraline at the concentration of 10 μmol/L (Figure 1 I.A). Five minutes after the drug administration CF increased to about 150% of the baseline value and declined quickly to the baseline value after discontinuation of sertraline. That confirms the strong coronary vasodilatory effect of sertraline at the concentration of 10 μmol/L.
Shortly after administration, 10 μmol/L sertraline caused also an increase of the left ventricle developed pressure (LDVP) to about 150% of the baseline value and rise of the left ventricular pressure (dP/dt max) (Figure 1. I.D) to approximately 144% of the baseline value at the maximum rate. However, that positive inotropic effect was short and lasted merely 5 mins after the start of the drug administration. Several minutes later, both parameters began to decrease rapidly, 30 mins after the start of the drug administration reaching statistically significant lower values in comparison to the control group. In the group of hearts receiving 1 μmol/L sertraline the positive inotropic effect did not occur, but a slight decline of LDVP and dP/dt max was observed, reaching statistically significant lower values in comparison to the control group in five to ten minutes before the end of the perfusion.
After 20 mins of 10 μmol/L sertraline administration, the average heart rate (HR) (Figure 1. I.B) declined gradually, and after 35 mins from the start of the experiment the mean HR of hearts in that group was reaching significantly lower values in comparison to the baseline (40%); in the next 10 min those values were close to 0% in comparison to baseline values.
Biochemical Analysis
In contrast to other groups, CPK activity in the 10 μmol/L sertraline group without ischemia/reperfusion increased slowly and at the time point of 30 mins it was significantly higher (p ≤ 0.05) compared to the control group. That indicates a direct damaging effect of 10 μmol/L sertraline on heart cells (Figure 2A).
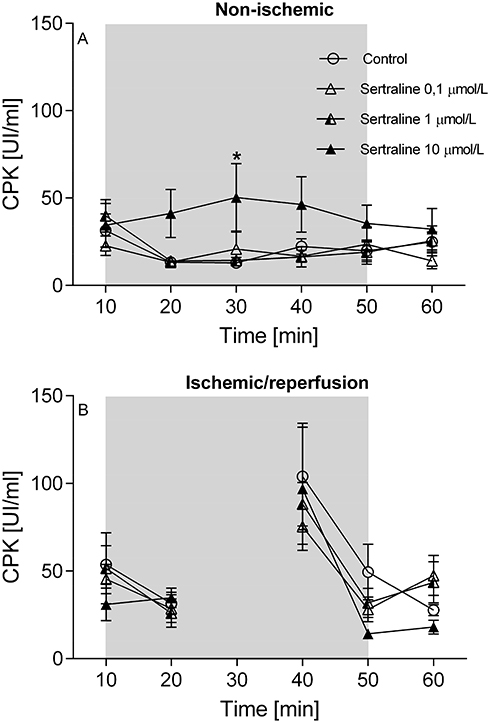 |
Figure 2 Effect of sertraline on creatine phosphokinase (CPK) outflow (UI/mL). Creatine phosphokinase (CPK) outflow in isolated rat heart perfused in non-ischemic condition or subjected to 20-min ischemia and 20-min reperfusion. Values are means ± SEM of seven experiments. *p ≤ 0.05; vs the control group. |
There was no difference between any of the non-ischemic group regarding the NO outflow, which means sertraline at any given concentration does not affect NO production in isolated perfused rat heart at any time point measured (Table 2).
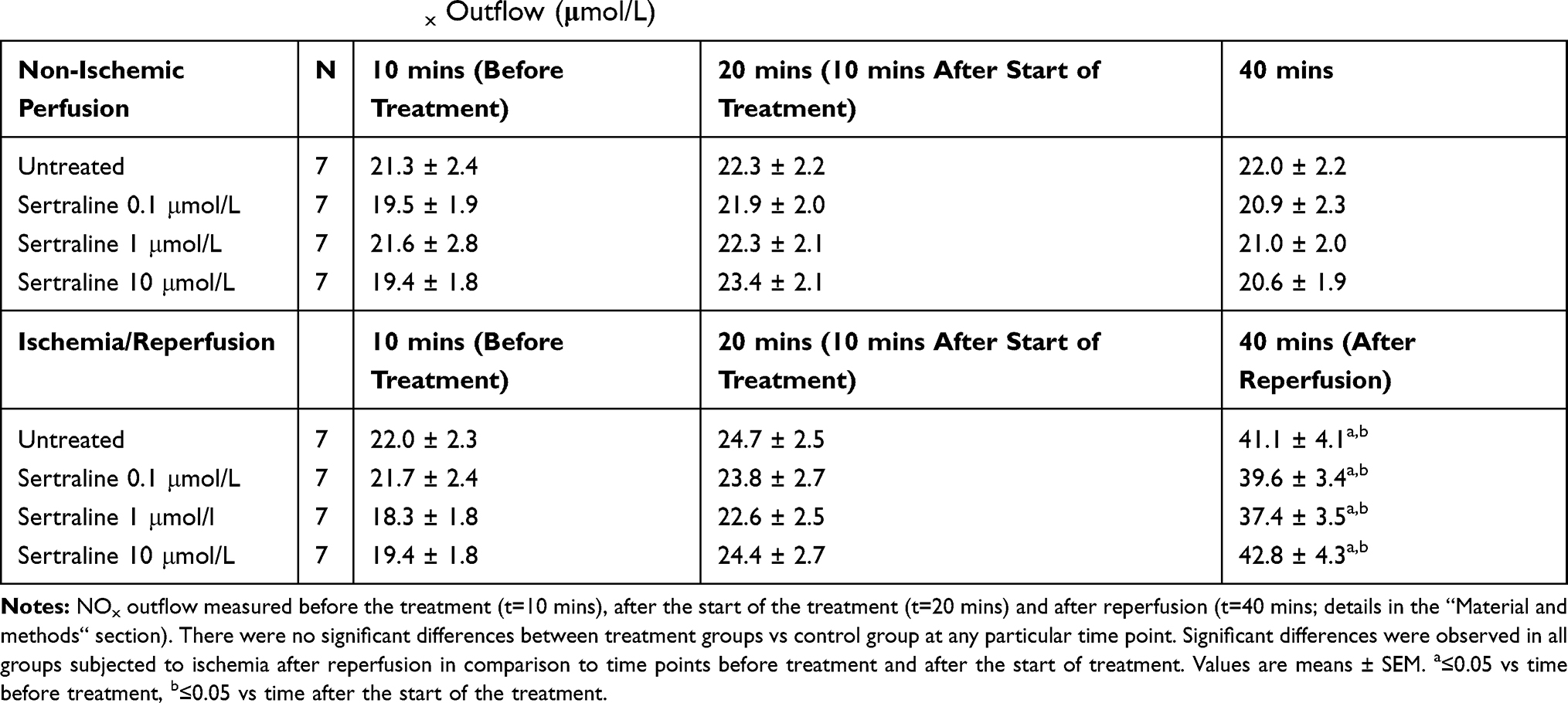 |
Table 2 Effect of Sertraline on NOx Outflow (μmol/L) |
Ischemia/Reperfusion
Hemodynamic Data
Before ischemia, hemodynamic parameters after administration of 10 μmol/L sertraline were very similar to the non-ischemic group – a statistically significant rise in CF, LVDP and dPdt was observed in the 5th minute after the drug administration (Figure 1 I.A, I.B, I.D)
After reperfusion, outcomes observed in each of the ischemic groups were different. In the 40th minute, the 10 μmol/L group showed significantly higher values of CF, LVDP and dP/dt max in comparison to the control group. However, those parameters decreased quickly and at the end of the experiment, they reached significantly lower values in comparison to the control group. In the group of 1 μmol/L sertraline, significantly lower values were observed only for the dP/dt max value in the time point of 10 mins before the end of the experiment, in comparison to the control group.
Biochemical Analysis
During ischemia, NO from both enzymatic and non-enzymatic sources is accumulated in tissues.21 Therefore, our data demonstrated a great increase of NOx production after the reperfusion in comparison to baseline values (10th minute) and values measured after the start of the treatment (20th minute). However, a comparison between groups with ischemia/reperfusion at the reperfusion time point (40th minute) did not demonstrate any difference in comparison to the control group (Table 2).
A similar situation was observed for CPK. There were no differences between ischemia/reperfusion groups in terms of CPK, both before ischemia and after reperfusion, in comparison to the control group. An initial increase of CPK after the reperfusion in all groups was a result of damage of muscle cells during ischemia. A comparison between groups with ischemia/reperfusion after the time of reperfusion did not show any differences between groups (Figure 2B).
Discussion
In their study, Gaur et al demonstrated the neuroprotective effect of sertraline on ischemic rat brain cells and suggested that it was associated with the influence of the substance on the metabolism of nitric oxide. In their study, sertraline reduced the oxidative stress caused by increased concentrations of potentially neurotoxic nitric oxide metabolites. Moreover, administration of L-arginine, being a substrate for nitric oxide synthase, abolished the protective effect of sertraline, and administration of L-NAME (a nitric oxide synthase inhibitor) increased its protective effect on ischemic brain cells. However, the detailed mechanism of that association remains unknown.22 It is possible that there is an indirect relationship between drugs selectively inhibiting the reuptake of serotonin and nitric oxide synthesis in brain cells, but there is no experimental study demonstrating the existence of a similar relationship relative to the blood vessels or heart muscle. Data regarding the effect of SSRIs on the metabolism of nitric oxide in humans are contradictory and do not allow clear identification of whether and how do SSRIs possibly affect NO metabolism. The results of our study demonstrate that sertraline does not significantly affect the metabolism of nitric oxide in the isolated rat heart. That means that the strong vasodilative effect of the highest applied dose of sertraline is not related with NO.
The effect of SSRIs on blood vessels has been studied in numerous animal models. Majority of these experiments indicated that their vasodilative effect.23–25 The mechanism of that effect of SSRIs is probably not related to serotonin reuptake inhibition, but results from their another property – the blocking effect on the voltage-dependent L-type calcium channels (inhibition of intracellular calcium current) or the effect on another signal path related to calcium ions, leading to relaxation of vascular smooth muscles and to vasodilation.26 Those additional effects of SSRIs may indicate a potentially beneficial mechanism in ischemic heart disease. The fact that the vasodilative action of those drugs has also been observed in vessels without endothelial cells and in series of experiments that showed a direct relaxant effect of SSRIs on smooth muscle cells of other organs in rats speaks in favor of that hypothesis.27,28 However, the strong vasodilative effect of the highest applied doses of sertraline observed in our experiment occurs for concentrations ranging between 10 and 100-times over the therapeutic level of the drug in patients’ plasma.29 At the concentration of 10 μmol/L, the coronary flow increased to 150% of the baseline value, but at the same concentration, sertraline caused a very strong damage to myocardial cells, resulting in a significant reduction of heart’s contractility.
A negative effect of serotonin reuptake inhibitors on the cardiac contraction of isolated heart has been demonstrated in some studies.30–33 Authors of papers describing the negative inotropic effect of SSRIs on parameters of the isolated myocardium suggested that it is mainly related to blocking channels of L-type calcium by those drugs. This is partially contradictory with the results of our research that demonstrated a short positive inotropic effect of 10 µmol/L sertraline on the myocardium. A transient increase of myocardial contraction observed in our study could be associated with the so-called Gregg phenomenon.34 It states that the increase in coronary perfusion leads to an increase in contractile force and the consumption of oxygen by the myocardium.35 In our experiment, the increase of systolic myocardial function was observed exactly at the same time as a very large increase in CF. The mechanism responsible for the Gregg’s effect is not fully understood, but probably it is related to the so-called, circumferential stress (hoop stress) exerted by extended coronary arteries on the muscle cell membrane, that could lead to opening of ion stretch activated channels (SAC) and consequently to an increase in the force of contraction of cardiac muscle cells.36 That phenomenon, however, does not fully explain the transient positive inotropic action of sertraline observed in our study. Dijkman et al demonstrated that the increase in contractile force in the Gregg effect is associated mainly with an increase in perfusion pressure, while the increased flow causes only an increased oxygen consumption by the myocardium.37,38 In the present study, the perfusion pressure of 70 mmHg remained constant during the whole experiment. That phenomenon does not also explain the fact that in our study the positive inotropic effect was very short-lasting, and within several minutes the contractile activity of the heart treated with 10 µmol/L sertraline decreased almost to zero, and a direct toxic effect of the drug was confirmed by high values of CPK.
On the other hand, Tatsuya Muto et al demonstrated some beneficial effects of fluvoxamine (another SSRI) on the contractile force of perfused guinea-pig heart during ischemia/reperfusion in the Langendorff model. They studied the effect of fluvoxamine on the increase of mitochondrial Ca2+ ([Ca2+]m) level. Beneficial effects of fluvoxamine on LVDP were shown in hearts pretreated with the drug at a dose of 0.5 μmol/L and it lasted for as long as over 40 mins after reperfusion, in comparison to the control group. Elevated [Ca2+]m levels after the fluvoxamine treatment were significantly suppressed compared to the control group. The authors suggest that fluvoxamine may prevent the opening of mitochondrial permeability transition pore (MPTP), and thus preserve mitochondrial function and exert beneficial effects on LVDP of the heart after reperfusion.39
The above-mentioned studies of effects of various SSRIs on perfused isolated animal heart report different results concerning heart contractile force. That difference may be explained in many ways. Experiments often used different protocols – the time of ischemia/reperfusion, hemodynamic data measurement, biochemical analysis and others. Various SSRIs have a similar property of inhibiting the reuptake of serotonin, but different chemical structure. Another explanation of that inconsistency could be different concentrations of drugs used – that is particularly evident in our study, where the concentration of 10 micromoles per liter of sertraline results in dramatic changes in hemodynamic and toxic effects on the myocardiac cell. Differences apparent in other studies regarding the effects of SSRIs on the isolated animal heart may be also due to species differences. In some electrophysiological studies on the cells of isolated animal hearts resulting data were different depending on species used. In their study concerning the effect of fluoxetine on the action potential of cells derived from the papillary muscles of the heart, Pacher et al demonstrated that the myocardium of rat reacted differently in comparison to the heart muscle of guinea pig and rabbit.30 Fluoxetine led to shortening of repolarization of cardiac muscle cells in these animals, but had no effect on the time of repolarization of myocytes in rats. Interestingly, only in rat muscle cells fluoxetine did cause a concentration-dependent decrease in contractile force before a total abolition at the concentration of 100 μmol/L. Electrophysiological dissimilarity of rat myocardial cells is also reflected in their ECG – in rats, a significant shortening of the QT interval may be observed.40,41 The difference between rat hearts and hearts of other rodent species may be a reason for different effects of various substances on cardiac conductivity.
In our study, no significant influence of sertraline on the synthesis of nitric oxide at various concentrations of sertraline was observed. It seems that observed effects of SSRIs on the isolated rat heart may be a result of other mechanisms, including the calcium pathway, as suggested by authors of other reports.
A detailed explanation of the exact toxic mechanism of high concentrations of sertraline on the heart muscle observed in our experiment undoubtedly requires further research, including other models and different animal species. The mechanism of action of SSRIs on ion channels of the myocardium cells and thus the strength and frequency of contraction may also be more complex. Numerous electrophysiological studies demonstrated that those drugs were able to block hERG potassium channels,42,43 as well as other types of potassium channels,44 and sodium channels,45 besides the block of calcium channels. Each of those mechanisms may lead to changes in cytoplasmic concentration of calcium or other ions, and consequently to changes in the cell action potential of myocardial contractions and strength. Further investigation of various cardiac effects of SSRIs may provide more information in that field.
Conclusion
Sertraline at dose 10 μmol/L exerts a strong vasodilatory effect on coronary flow, and after a short positive inotropic effect, it exerts a strong negative effect on isolated rat hearts, causing a direct damage to cardiomyocytes. Sertraline had no effect on the nitric oxide concentration in coronary effluent.
Acknowledgements
This work was supported by the Polish Committee for Scientific Research (KBN) under contract No. 1 P03B 059 27.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Paraskevaidis I, Parissis JT, Fountoulaki K, Filippatos G, Kremastinos D. Selective serotonin re-uptake inhibitors for the treatment of depression in coronary artery disease and chronic heart failure: evidence for pleiotropic effects. Cardiovasc Hematol Agents Med Chem. 2006;4:361–367. doi:10.2174/187152506784111454
2. Roose SP. Treatment of depression in patients with heart disease. Biol Psychiatry. 2003;54:262–268. doi:10.1016/S0006-3223(03)00320-2
3. Schlienger RG, Fischer LM, Jick H, Meier CR. Current use of selective serotonin reuptake inhibitors and risk of acute myocardial infarction. Drug Saf Int J Med Toxicol Drug Exp. 2004;27:1157–1165. doi:10.2165/00002018-200427140-00006
4. Serebruany VL, Glassman AH, Malinin AI, et al. Selective serotonin reuptake inhibitors yield additional antiplatelet protection in patients with congestive heart failure treated with antecedent aspirin. Eur J Heart Fail J Work Group Heart Fail Eur Soc Cardiol. 2003;5:517–521.
5. Isbister GK, Bowe SJ, Dawson A, Whyte IM. Relative toxicity of selective serotonin reuptake inhibitors (SSRIs) in overdose. J Toxicol Clin Toxicol. 2004;42:277–285. doi:10.1081/CLT-120037428
6. Pacher P, Kecskemeti V. Cardiovascular side effects of new antidepressants and antipsychotics: new drugs, old concerns? Curr Pharm Des. 2004;10:2463–2475. doi:10.2174/1381612043383872
7. Pacher P, Ungvari Z. Selective serotonin-reuptake inhibitor antidepressants increase the risk of falls and hip fractures in elderly people by inhibiting cardiovascular ion channels. Med Hypotheses. 2001;57:469–471. doi:10.1054/mehy.2001.1366
8. Serebruany VL, Gurbel PA, O’Connor CM. Platelet inhibition by sertraline and N-desmethylsertraline: a possible missing link between depression, coronary events, and mortality benefits of selective serotonin reuptake inhibitors. Pharmacol Res off J Ital Pharmacol Soc. 2001;43:453–462.
9. Musselman DL, Lawson DH, Gumnick JF, et al. Paroxetine for the prevention of depression induced by high-dose interferon alfa. N Engl J Med. 2001;344:961–966. doi:10.1056/NEJM200103293441303
10. Cohen H, Kotler M, Matar M, Kaplan Z. Normalization of heart rate variability in post-traumatic stress disorder patients following fluoxetine treatment: preliminary results. Isr Med Assoc J IMAJ. 2000;2:296–301.
11. Shores MM, Pascualy M, Lewis NL, Flatness D, Veith RC. Short-term sertraline treatment suppresses sympathetic nervous system activity in healthy human subjects. Psychoneuroendocrinology. 2001;26:433–439. doi:10.1016/S0306-4530(01)00002-6
12. van Melle JP, de Jonge P, van den Berg MP, Pot HJ, van Veldhuisen DJ. Treatment of depression in acute coronary syndromes with selective serotonin reuptake inhibitors. Drugs. 2006;66:2095–2107. doi:10.2165/00003495-200666160-00005
13. Ferdinandy P, Schulz R. Nitric oxide, superoxide, and peroxynitrite in myocardial ischaemia-reperfusion injury and preconditioning. Br J Pharmacol. 2003;138:532–543. doi:10.1038/sj.bjp.0705080
14. Bolli R, Jeroudi MS, Patel MS. et al. Direct evidence that oxygen-derived free radicals contribute to postischemic myocardial dysfunction in the intact dog. Proc Natl Acad Sci U S A. 1989;86:4695–4699. doi:10.1073/pnas.86.12.4695
15. Schulz R, Kelm M, Heusch G. Nitric oxide in myocardial ischemia/reperfusion injury. Cardiovasc Res. 2004;61:402–413. doi:10.1016/j.cardiores.2003.09.019
16. Finkel MS, Laghrissi-Thode F, Pollock BG, Rong J. Paroxetine is a novel nitric oxide synthase inhibitor. Psychopharmacol Bull. 1996;32:653–658.
17. Lara N, Archer SL, Baker GB, Le Mellédo J-M. Paroxetine-induced increase in metabolic end products of nitric oxide. J Clin Psychopharmacol. 2003;23:408–412. doi:10.1097/01.jcp.0000085416.08426.1d
18. Chrapko W, Jurasz P, Radomski MW, et al. Alteration of decreased plasma NO metabolites and platelet NO synthase activity by paroxetine in depressed patients. Neuropsychopharmacol off Publ Am Coll Neuropsychopharmacol. 2006;31:1286–1293. doi:10.1038/sj.npp.1300961
19. Ikenouchi-Sugita A, Yoshimura R, Hori H, et al. Effects of antidepressants on plasma metabolites of nitric oxide in major depressive disorder: comparison between milnacipran and paroxetine. Prog Neuropsychopharmacol Biol Psychiatry. 2009;33:1451–1453.
20. Skrzypiec-Spring M, Grotthus B, Szelag A, Schulz R. Isolated heart perfusion according to Langendorff - still viable in the new millennium. J Pharmacol Toxicol Methods. 2007;55:113–126. doi:10.1016/j.vascn.2006.05.006
21. Andreadou I, IIiodromitis EK, Rassaf T, et al. The role of gasotransmitters NO, H2S and CO in myocardial ischaemia/reperfusion injury and cardioprotection by preconditioning, postconditioning and remote conditioning. Br J Pharmacol. 2015;172:1587–1606. doi:10.1111/bph.12811
22. Gaur V, Kumar A. Behavioral, biochemical and cellular correlates in the protective effect of sertraline against transient global ischemia induced behavioral despair: possible involvement of nitric oxide-cyclic guanosine monophosphate study pathway. Brain Res Bull. 2010;82:57–64. doi:10.1016/j.brainresbull.2010.01.010
23. Pacher P, Ungvari Z, Kecskemeti V, Koller A. Serotonin reuptake inhibitor, fluoxetine, dilates isolated skeletal muscle arterioles. Possible role of altered Ca2+ sensitivity. Br J Pharmacol. 1999;127:740–746. doi:10.1038/sj.bjp.0702571
24. Ungvari Z, Pacher P, Kecskeméti V, Koller A. Fluoxetine dilates isolated small cerebral arteries of rats and attenuates constrictions to serotonin, norepinephrine, and a voltage-dependent Ca(2+) channel opener. Stroke J Cereb Circ. 1999;30:1949–1954. doi:10.1161/01.STR.30.9.1949
25. Ungvari Z, Pacher P, Koller A. Serotonin reuptake inhibitor fluoxetine decreases arteriolar myogenic tone by reducing smooth muscle [Ca2+]i. J Cardiovasc Pharmacol. 2000;35:849–854. doi:10.1097/00005344-200006000-00004
26. Deák F, Lasztóczi B, Pacher P, et al. Inhibition of voltage-gated calcium channels by fluoxetine in rat hippocampal pyramidal cells. Neuropharmacology. 2000;39:1029–1036. doi:10.1016/S0028-3908(99)00206-3
27. Pacher P, Ungvari Z, Kecskeméti V, Friedmann T, Furst S. Serotonin reuptake inhibitors fluoxetine and citalopram relax intestinal smooth muscle. Can J Physiol Pharmacol. 2001;79:580–584. doi:10.1139/y01-030
28. Velasco A, Alamo C, Hervás J, Carvajal A. Effects of fluoxetine hydrochloride and fluvoxamine maleate on different preparations of isolated guinea pig and rat organ tissues. Gen Pharmacol. 1997;28:509–512. doi:10.1016/S0306-3623(96)00274-1
29. Boulton DW, Balch AH, Royzman K, et al. The pharmacokinetics of standard antidepressants with aripiprazole as adjunctive therapy: studies in healthy subjects and in patients with major depressive disorder. J Psychopharmacol. 2010;24:537–546. doi:10.1177/0269881108096522
30. Pacher P, Magyar J, Szigligeti P, et al. Electrophysiological effects of fluoxetine in mammalian cardiac tissues. Naunyn Schmiedebergs Arch Pharmacol. 2000;361:67–73. doi:10.1007/s002109900154
31. Pousti A, Malihi G, Naghibi B. Effect of citalopram on ouabain-induced arrhythmia in isolated guinea-pig atria. Hum Psychopharmacol. 2003;18:121–124. doi:10.1002/hup.446
32. Pousti A, Deemyad T, Brumand K, Bakhtiarian A. The effect of fluvoxamine on ouabain-induced arrhythmia in isolated guinea-pig atria. Pharmacol Res. 2005;52:151–153. doi:10.1016/j.phrs.2005.01.002
33. Pousti A, Bakhtiarian A, Najafi R, et al. Effect of sertraline on ouabain-induced arrhythmia in isolated guinea-pig atria. Depress Anxiety. 2009;26:E106–E110. doi:10.1002/da.20407
34. Gregg DE. Effect of coronary perfusion pressure or coronary flow on oxygen usage of the myocardium. Circ Res. 1963;1:497–500. doi:10.1161/01.RES.13.6.497
35. Opie LH. Coronary flow rate and perfusion pressure as determinants of mechanical function and oxidative metabolism of isolated perfused rat heart. J Physiol. 1965;180:529–541. doi:10.1113/jphysiol.1965.sp007715
36. Lamberts RR, Van Rijen MHP, Sipkema P, et al. Increased coronary perfusion augments cardiac contractility in the rat through stretch-activated ion channels. Am J Physiol Heart Circ Physiol. 2002;282:H1334–H1340. doi:10.1152/ajpheart.00327.2001
37. Dijkman MA, Heslinga JW, Sipkema P, Westerhof N. Perfusion-induced changes in cardiac O2 consumption and contractility are based on different mechanisms. Am J Physiol. 1996;271:H984–989. doi:10.1152/ajpheart.1996.271.3.H984
38. Dijkman MA, Heslinga JW, Sipkema P, Westerhof N. Perfusion-induced changes in cardiac contractility and oxygen consumption are not endothelium-dependent. Cardiovasc Res. 1997;33:593–600. doi:10.1016/S0008-6363(96)00260-X
39. Muto T, Usuda H, Yamamura A, et al. Protective effects of fluvoxamine against ischemia/reperfusion injury in isolated, perfused guinea-pig hearts. Biol Pharm Bull. 2014;37:731–739. doi:10.1248/bpb.b13-00552
40. McDermott JS, Salmen HJ, Cox BF, Gintant GA. Importance of species selection in arrythmogenic models of Q-T interval prolongation. Antimicrob Agents Chemother. 2002;46:938–939. doi:10.1128/AAC.46.3.938-939.2002
41. Suzuki J, Tsubone H, Sugano S. Studies on the positive T wave on ECG in the rat - based on the analysis for direct cardiac electrograms in the ventricle. Adv Anim Cardiol. 1993;26:24–32.
42. Thomas D, Gut B, Wendt-Nordahl G, Kiehn J. The antidepressant drug fluoxetine is an inhibitor of human ether-a-go-go-related gene (HERG) potassium channels. J Pharmacol Exp Ther. 2002;300:543–548. doi:10.1124/jpet.300.2.543
43. Witchel HJ, Pabbathi VK, Hofmann G, Paul AA, Hancox JC. Inhibitory actions of the selective serotonin re-uptake inhibitor citalopram on HERG and ventricular L-type calcium currents. FEBS Lett. 2002;512:59–66. doi:10.1016/S0014-5793(01)03320-8
44. Park KS, Kong ID, Park KC, Lee JW. Fluoxetine inhibits L-type Ca2+ and transient outward K+ currents in rat ventricular myocytes. Yonsei Med J. 1999;40:144–151. doi:10.3349/ymj.1999.40.2.144
45. Hahn SJ, Choi JS, Rhie DJ, et al. Inhibition by fluoxetine of voltage-activated ion channels in rat PC12 cells. Eur J Pharmacol. 1999;367:113–118. doi:10.1016/S0014-2999(98)00955-8
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.