Back to Journals » Drug Design, Development and Therapy » Volume 19
The Effect of Pericapsular Nerve Group Block with Liposomal Bupivacaine on Postoperative Rebound Pain in Older Hip Fracture Patients: A Randomized Controlled Trial
Authors Wang Q ![]() , Wang J, Liu Y, Dai Z, Wang Y, Xia X, Li Y
, Wang J, Liu Y, Dai Z, Wang Y, Xia X, Li Y
Received 27 August 2025
Accepted for publication 2 December 2025
Published 5 December 2025 Volume 2025:19 Pages 10811—10820
DOI https://doi.org/10.2147/DDDT.S562733
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Anastasios Lymperopoulos
Qiang Wang,1,* Jiyuan Wang,2,* Yujia Liu,1 Zhen Dai,1 Yan Wang,1 Xiaoqiong Xia,1 Yuanhai Li2
1Anesthesiology Department, The Fourth Affiliated Hospital of Anhui Medical University, ChaoHu, Hefei, People’s Republic of China; 2Anesthesiology Department, The First Affiliated Hospital of Anhui Medical University, Hefei, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaoqiong Xia, Anesthesiology Department, The Fourth Affiliated Hospital of Anhui Medical University, ChaoHu, Hefei, Anhui Province, 238000, People’s Republic of China, Tel +8613966386669, Email [email protected] Yuanhai Li, Anesthesiology Department, the First Affiliated Hospital of AnHui Medical University, Hefei, 230000, People’s Republic of China, Tel +8613505697561, Email [email protected]
Objective: This study aims to investigate and discuss the effect of pericapsular nerve group (PENG) block with liposomal bupivacaine (LB) on postoperative rebound pain following hip fracture in older adults.
Patients and Methods: Ninety patients scheduled for hip fracture surgery were randomized into three groups: LB (liposomal bupivacaine, 30 mL), R (0.375% ropivacaine, 30 mL), and C (saline, 30 mL). MAP and HR were recorded at T1 (pre-induction), T2 (post-intervention), and T3 (skin incision). NRS scores were evaluated at 12– 72 h postoperatively, along with rebound pain, quadriceps function, analgesic consumption, and adverse reactions.
Results: The incidence of rebound pain was significantly lower in the LB and R groups than in the C group (p < 0.05). The AUC of NRS scores over 72 hours was significantly lower in the LB group (2.053 ± 1.258) than in the R (3.600 ± 2.087) and C (4.880 ± 2.739) groups (p < 0.0001). Hemodynamic analysis revealed significant differences in HR between T2 and T3 in all groups (LB: 77.10 ± 11.28 vs 73.77 ± 8.47; R: 79.57 ± 8.05 vs 74.00 ± 8.13; C: 80.50 ± 8.71 vs 84.13 ± 8.07; p < 0.05). MAP in the LB group differed significantly from Group C across the three time points (p < 0.05). There were no significant differences between the groups in adverse events.
Conclusion: LB PENG blockade reduces rebound pain incidence post-nerve block in elderly hip fracture patients, decreases PCA demand, preserves quadriceps function, and enhances satisfaction.
Keywords: rebound pain after nerve block, PENG block, liposomal bupivacaine, hip fracture
Introduction
Hip fracture1 is common in older adults worldwide. With an aging population, the prevalence of this condition is steadily increasing. In addition, high morbidity and mortality associated with it profoundly impact patients’ quality of life and impose a substantial burden on families and society.2 First proposed in 2018, the pericapsular nerve group (PENG) block technique3 is based on the anatomy of hip joint innervation, targeting an articular branch of the femoral nerve to the hip and the obturator nerve, which can quickly and effectively block pain signals from the innervated areas described above.4 Although nerve blocks can reduce patient pain during the early postoperative period, nerve block rebound pain5 may cause physical and mental distress, potentially compromising the therapeutic efficacy of peripheral nerve blocks. Rebound pain was operationally defined as an increase in the Numerical Rating Scale (NRS) score from ≤3 during an effective nerve block to ≥7 following block resolution, occurring within 24 hours after the procedure. While continuous catheterization and local anesthetic adjuvants are used clinically to avert rebound pain after nerve blocks, the effectiveness of ultra-long-acting local anesthetics for this purpose, specifically within the PENG block scenario, has not been established. Current evidence6 suggests that prolonging the duration of nerve block may reduce rebound pain, highlighting the significance of exploring the use of long-acting local anesthetics. Liposomal bupivacaine7 is a novel, long-acting local anesthetic agent. It utilizes the DepoFoam multivesicular liposome technology to encapsulate bupivacaine. Following injection, the vesicles gradually disintegrate, enabling a slow, sustained release of the drug while maintaining the structural integrity of the liposomes. Since vesicles exhibit variable disintegration times, this formulation consistently delivers both safe and effective therapeutic drug concentrations, which provides long-acting analgesia. However, the formulation’s effects on rebound pain after PENG block remain unclear. This study is the first to systematically evaluate the impact of LB on rebound pain following PENG block in elderly Chinese patients with hip fractures.
Methods
Ethical Approval and Study Design
The comprehensive research question explored in this study underwent rigorous ethical review and evaluation. The study was approved by the Ethics Committee of the Fourth Affiliated Hospital of Anhui Medical University (No. KYXM-202409-002) and registered under the identifier ChiCTR2400091793 in the China Clinical Trial Center following the oversight procedure. The study was conducted and reported in accordance with the Consolidated Standards of Reporting Trials (CONSORT) guidelines and the ethical principles of the Declaration of Helsinki. Written informed consent was obtained by signature from patients or their legal representatives.
Participants
This study enrolled patients undergoing elective hip arthroplasty at Anhui Medical University’s Fourth Affiliated Hospital between December 2024 and August 2025. Patients aged ≥ 65 years, with a BMI of 18.5–30kg/m2, and ASA grade II–III were enrolled irrespective of gender. The surgical procedures included hip arthroplasty and femoral neck internal fixation.
Exclusion criteria included: severe hematologic disease or coagulation abnormality, contraindication to general anesthesia, simultaneous surgery of both limbs, history of allergy to local anesthetics, peripheral neurological disease, impaired communication, cognitive dysfunction, need for a nerve block for severe or compound trauma, moderate or severe pain in the PACU (NRS score ≥ 7), referral to the ICU after surgery, infection of the puncture site, serious adverse events during surgery, and early withdrawal from the procedure for non-study-related reasons.
Randomization and Sample SizeEligible participants were allocated in a 1:1:1 ratio using the random number table method. The allocation sequence was generated by an independent anesthesiologist using the SPSS software, who also sealed the group assignments in sequentially numbered, identical, opaque envelopes. When the eligible patients were in the preoperative area, one external coordinator not involved in the study opened the envelopes and communicated the allocation. Patients were randomized to three groups (n=30 each). Group LB (experimental; received Liposomal Bupivacaine), group R (active control; received Ropivacaine), and group C(negative control).
The sample size was calculated using the PASS15 software. The incidence of rebound pain in the 12–24 h postoperative period was used as the main index, and according to the pre-test results and related references,8 its incidence rate was 10% in the LB group, and 43% in the C group. A two-sided test was used with a significance level α = 0.025, 1-β = 0.90. A sample size of 30 patients per group was determined, accounting for a 10% attrition rate.
Perioperative Procedures
In the preoperative area, anesthesia was prepared and vital signs were routinely monitored, specifically blood pressure (BP), heart rate (HR), pulse oximetry (SpO2), and electrocardiogram (ECG). Patients’ BIS values were recorded using a BIS monitor. Radial artery cannulation was carried out under local anesthesia. In Group LB, a PENG block was performed with 266 mg (20 mL) of liposomal bupivacaine dissolved in 0.9% saline to a total volume of 30 mL (Jiangsu Hengrui Co., Ltd., National Drug Registration No. H20223899, China), and a lateral femoral cutaneous nerve block was performed with 0.375% ropivacaine (5 mL), both before the induction of general anesthesia. In Group R, 30 mL of 0.375% ropivacaine and 5 mL of 0.375% ropivacaine were injected at the same site to achieve a lateral femoral cutaneous nerve block prior to induction. In Group C, 30 mL of 0.9% saline was injected at the same site, along with 5 mL of 0.375% ropivacaine for a lateral femoral cutaneous nerve block prior to induction. All operations were performed by the same experienced anesthesiologist. After placing the patient in the supine position, a low-frequency convex array probe was used. After routine disinfection of the skin, the probe was placed at the junction of the middle and lateral thirds of the line between the anterior inferior iliac spine and the perineum, aligned with the pubic branch, identifying the iliopubic ramus, femoral artery, femoral vein, iliopsoas muscle, and pubic bone. The needle was inserted in-plane, with the tip placed on the myofascial plane posterior to the psoas major tendon and on the surface of the iliopubic ramus. Hydrodissection was performed after negative blood aspiration, and 30 mL of bupivacaine liposome was injected until upward movement of the psoas major tendon was observed (see Figure 1). We positioned a convex ultrasound probe below the anterior superior iliac spine to locate the lateral femoral cutaneous nerve over the tensor fasciae latae. The needle was inserted in-plane, and 5 mL of 0.375% ropivacaine was injected after negative aspiration. The PENG-blocked area was assessed using an alcohol swab. The PENG was considered effective if the patient’s sensation diminished or disappeared; otherwise, it was classified as ineffective, and the group was excluded. A single experienced anesthesiologist performed all nerve blocks. This investigator was blinded to patient group allocation throughout the study. The laryngeal mask airway was inserted immediately after intravenous induction. After induction, etomidate 0.2–0.6 mg/kg or remazolam 0.1–0.3 mg/kg, sufentanil 0.2–0.5 µg/kg, and/or cis-atracurium 0.15–0.2 mg/kg were administered. After placement, the laryngeal mask airway was connected to mechanical ventilation. The laryngeal mask was connected to mechanical ventilation (respiratory rate of 10–12 breaths per minute, tidal volume of 8–10 mL/kg, fresh gas flow rate of 2.0 L per minute, an inspiratory-to-expiratory ratio of 1:2), with end-tidal carbon dioxide (EtCO2) maintained at 35–45 mmHg. During the procedure, cis-atracurium ammonium (2 mg) was administered to maintain neuromuscular relaxation. Anesthesia was maintained with a plasma concentration of propofol ranging from 1.5–3.0 g/mL, concurrently with remifentanil concentrations ranging from 1.0–3.0 ng/mL. Target concentration was rapidly adjusted to the patient’s physiologic response to maintain mean arterial pressure (MAP) and heart rate (HR) within ±20% of baseline values, and to maintain the bispectral index (BIS) value between 40 and 60. After surgery, the patient was transferred to the post-anesthesia care unit (PACU) for observation. Once the patient regained consciousness and resumed spontaneous respiration without complications, their vital signs stabilized, and the Steward score was > 4 points, the laryngeal mask was removed, and the patient was transferred back to the general ward. The postoperative patient-controlled intravenous analgesia (PCIA) formulation consisted of sufentanil at 3ug/kg diluted with saline to a total volume of 150 mL, with no background infusion, a self-controlled analgesic dose of 2 mL, and a lock time of 20 minutes. Patients were instructed to record pain intensity every 4 hours and to press the self-controlled analgesic pump when the pain became intolerable. If the NRS score remained ≥ 7 in the ward, 30 mg of ketorolac tromethamine was administered intravenously to optimize postoperative analgesia.
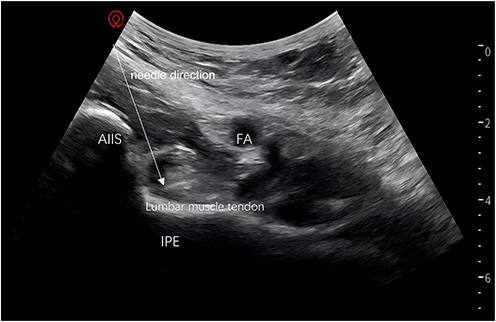 |
Figure 1 Anterior inferior iliac spine (AIIS). The iliopubic ramus (IPE). Femoral artery (FA). |

Outcome Measures
Primary Outcomes
- NRS scores were assessed at 12, 24, 48, and 72 hours postoperatively and the AUC of NRS scores was assessed at 72 hours postoperatively. The highest NRS score minus the lowest PACU pain score within 24 hours was recorded.5 Rebound pain was diagnosed if the patient’s pain changed from mild (NRS ≤ 3) in the PACU to severe pain (NRS ≥ 7) within 24 hours.
- Incidence of rebound pain.
Secondary Outcome Measures
- Mean arterial pressure (MAP) and heart rate (HR) of patients undergoing PENG block were recorded at predefined time points: 10 minutes before incision (T1), 10 minutes after the intervention (T2), and upon skin incision (T3).
- NRS scores at rest and during exercise (passive leg elevation 15°) 20 minutes after the block, and the number of analgesic pump presses after the operation.
- The quadriceps muscle function following the operation.
- Incidence of nausea and vomiting, dizziness, and other adverse events.
Statistical Methods
The SPSS 26 software was employed for data analysis. Data normality was checked with the Shapiro–Wilk test, while variance homogeneity was tested with Levene’s test. Data following a normal distribution are expressed as mean ± standard deviation (SD). Non-normally distributed variables are summarized as median (interquartile range, IQR), with intergroup differences analyzed using the Kruskal–Wallis H-test. The repeated measures analysis of variance was applied to analyze repeated measures data across three categories. The Bonferroni correction was applied post hoc. Chi-square testing evaluated group differences in categorical variables, expressed as counts (n) and percentages (%). Significant results (p < 0.05) revealed notable disparities between the groups.
Results
Characteristics of the Patients
One hundred seventeen subjects were initially enrolled in this study. Ninety patients were ultimately enrolled. Postoperative ICU admission was required for eight patients, ten were diagnosed with an infection at the nerve block puncture site, and nine exhibited coagulation abnormalities (Figure 2).
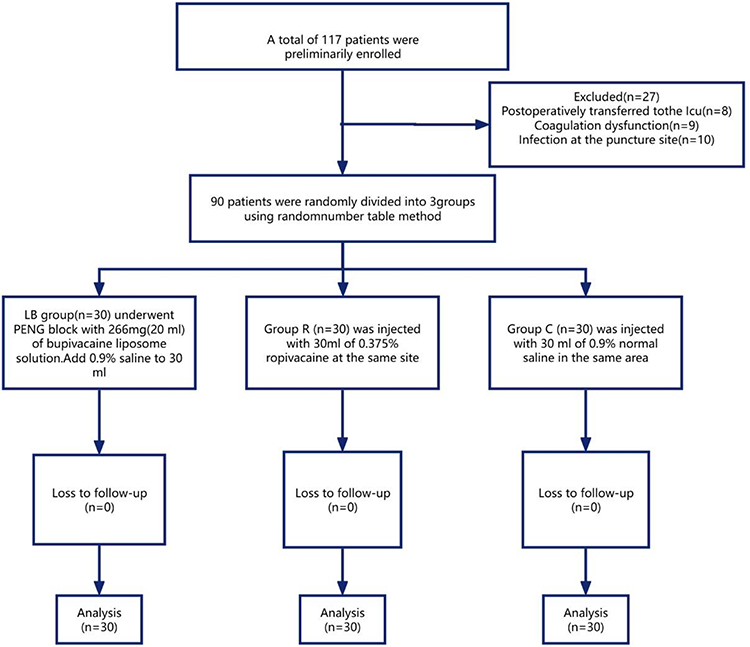 |
Figure 2 CONSORT diagram of patient recruitment. |
The age, gender, ASA classification, type of surgery, BMI, and duration of surgery of patients in the three groups were not statistically different from those in Group LB (p > 0.05; Table 1).
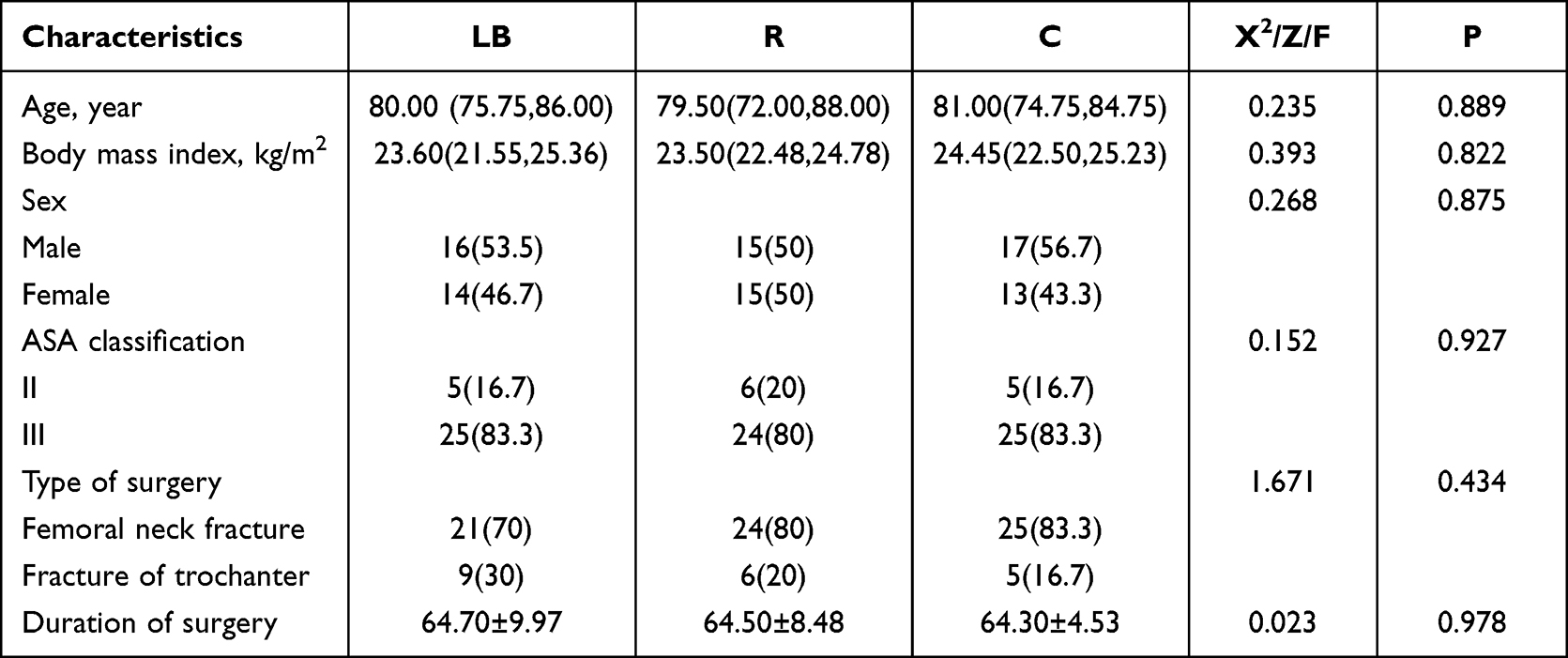 |
Table 1 Comparison of General Conditions of Patients in Group LB, Group R, and Group C |
The NRS scores at 12, 24, and 48 hours after surgery in the LB group were significantly lower than those in groups R and C. This difference reached statistical significance (p < 0.05; Table 2).
 |
Table 2 Comparison of NRS Scores (Points) at Multiple Time Points in the Three Groups ( |

Note: A: Compared with group C, P < 0.05; a: Compared with 12 hours post-surgery, P < 0.05; b: Compared with 48 hours post-surgery, P < 0.05; c: In the LB group, compared with 12 hours post-surgery, P < 0.05; d: Compared with 72 hours post-surgery, P < 0.05; e: In the R group, compared with 12 hours post-surgery, P < 0.05; f: Compared with 72 hours post-surgery, P < 0.05; g: In the C group, compared with 72 hours post-surgery, P < 0.05 (Table 2).
* Interactions between r-groups and time were analyzed using pairwise comparisons with Bonferroni correction.
The AUC of NRS scores in the LB group was significantly lower than the AUC of NRS scores (p < 0.001) in the R group and C group (2.053 ± 1.258 vs 3.600 ± 2.087 vs 4.880 ± 2.739, p < 0.01). Calculated based on the trapezoidal rule. ****indicates statistical differences between the two groups (P < 0.0001) (Figure 3).
 |
Figure 3 AUC area under the NRS curve at different time points. ****indicates statistical differences between the two groups (P<0.0001). |
The graph depicts the NRS scores collected over the 72-hour postoperative period, with the horizontal axis representing time intervals and the vertical axis representing pain intensity, and calculated based on the trapezoidal rule. Compared with the T1 time point, there were statistically significant differences in HR and MAP between different groups (P < 0.05). Compared with the C group, there were statistically significant differences in MAP at different time points in the LB group (P < 0.05).
Note: a: Compared with the T1 time point, there was a statistically significant difference in HR at the T2 and T3 time points.
b: Compared with the T2 time point, there was a statistically significant difference in MAP at the T2 and T3 time points.
c: Compared with C, there was a statistically significant difference in MAP between different time points in the LB group.
* Interactions between the groups and time were analyzed using pairwise comparisons with Bonferroni correction (Table S1).
In the LB group, NRS scores were 1.5 (1.0, 2.0) at rest and 2.0 (2.0, 3.0) during exercise.
In the R group, NRS scores were 2.0 (1.75, 2.0) at rest and 3.0 (2.0, 3.0) during exercise.
In the C group, NRS scores were 4.0 (3.0, 5.0) at rest and 7.0 (6.0, 7.25) during exercise.
There was a difference between the overall distribution, with a statistical difference between the C, LB, and the R groups (p < 0.01). There was no statistical difference between Groups LB and R (p = 0.114, not statistically significant (p > 0.05).
Note: a and b denote comparison with Group C (p < 0.01) (Table 2).
* Interactions between the groups and time were analyzed using a pair-wise comparison with Bonferroni correction.
The LB group demonstrated significantly fewer analgesic pump presses than the C group, with a parallel reduction in Group R versus Group C (both p < 0.05; Table S2).
There were no significant differences in dizziness and vomiting incidence between the groups (p > 0.05), whereas rebound pain incidence varied significantly across treatment groups (p = 0.017; Table 3).
 |
Table 3 Comparison of the Incidence of Adverse Reactions and Rebound Pain Among the Three Groups (n, %) |
There were no statistically significant differences in the patient’s muscle strength between the three groups at 24h and 72h postoperatively. A subset of patients from the group R had decreased muscle strength within 12 hours postoperatively (Z=12.170, P = 0.002), as shown in Table S2, based on pairwise comparisons with Bonferroni correction.
Discussion
Hip fracture in older adults, frequently accompanied by a femoral neck fracture and intertrochanteric femoral fracture, is a common orthopedic condition with significant morbidity and mortality.9 The management of these patients is further complicated by multiple comorbidities, posing challenges for anesthesiologists during the perioperative period. The enhanced recovery after surgery (ERAS) concept10 focuses on evidence-based perioperative interventions to accelerate recovery. A nerve block is a common procedure of multimodal analgesia in geriatric hip fracture surgery.11 Anesthesiologists prefer the PENG block due to its clinical safety profile regarding the quadriceps muscle function during the postoperative period.12 As evidenced by one study, the PENG block combined with the block of the lateral femoral cutaneous nerve (LFCN) could promote early bed mobilization and ambulation after surgery,13 thus improving overall prognosis. While nerve blocks significantly reduce postoperative pain, patients frequently report rebound pain once the block effect wears off, affecting the patient’s prognosis. The incidence of peripheral nerve block (RP) has been reported to range from 35% to 41%,14 and in some cases may be as high as 52%.15,16 Rebound pain after a nerve block not only dramatically decreases patient comfort, increases the administration of analgesic medications, including opioids, counteracting the benefit of the nerve block to the patient. Moreover, it also seriously impedes postoperative recovery, bringing a heavy burden on the whole family and society.17
In this study, consistent with previous studies, the incidence of rebound pain reached 10% in the LB group and 43% in the C group. This suggests that liposomal bupivacaine in PENG block can reduce the incidence of rebound pain in hip fracture patients. Among patients who received PENG block with ropivacaine, the incidence of rebound pain was lower in the LB group, likely due to the longer duration of analgesia provided by liposomal bupivacaine compared to ropivacaine. Also in this study, in the LB group, one vial of liposomal bupivacaine was reconstituted in normal saline to a final volume of 30 mL for injection, which exceeds the conventional volume of 20 mL. This larger volume of LB may have a potential effect on postoperative muscle strength and contribute to the decrease in quadriceps muscle strength at 12 hours postoperatively.18 Conversely, in the LB group, the recovery of strength was minimally affected by the release of liposomal bupivacaine, likely owing to its uniform and gradual release. This finding is consistent with previous studies. The rationale for selecting 30 mL as the control group was to explore whether a larger volume of local anesthetic could prolong the duration of action and thus reduce the rebound pain following a nerve block.
Liposomal bupivacaine (LB) was approved for marketing by the State Drug Administration of China on November 30, 2022, becoming the first liposomal form of long-acting extended-release local anesthetic to be approved in China.19 Currently, the duration of action of available local anesthetics is less than 12 hours, whereas LB can produce 72 hours of analgesia with a single dose injection. Additionally, its unique long-acting sustained-release effect can be used as an important component of multimodal analgesia.20 Previous studies have shown that rebound pain after a nerve block mostly occurs between 12 and 24 hours after the nerve block, and, theoretically, LB provides analgesia that spans the duration of rebound pain that follows a nerve block, inhibiting the sensation of rebound pain. In this experiment, rebound pain was reduced by 30% in the LB group compared with the C group, which was associated with a markedly improved prognosis for the patients. During the 12-hour postoperative period, patients in the LB group exhibited significantly less dizziness and vomiting than those in the C group, along with fewer presses of the analgesic pump. Higher incidence of postoperative nausea and vomiting in the LB group compared with the C group may be attributed to the side effects associated with increased use of opioids for analgesia in the C group after the operation. It is worth noting that in the LB group, the muscle strength returned to baseline levels at 12 and 24 hours after operation,21 and a certain analgesic effect may be prolonged in the group. This effect may be due to the uninterrupted and uniform release of bupivacaine from the vesicles in the LB group, which provided patients with continuous pain relief without compromising quadriceps function. Prof. Michael22 claims that LB can reduce pain scores after arthroplasty, which is consistent with the present study. In this study, NRS scores at different time points in the LB group decreased to varying degrees compared to the R and C groups. However, the difference between the R and C groups was larger than the NRS scores observed in the R group during the first 48 hours and continued to narrow after 48 hours, which may be related to the pharmacokinetic characteristics of LB.23 LB exhibits a bimodal release profile, dose-related properties, acting immediately after administration, subsequently demonstrating a second-phase release and reaching a peak between 12 and 24 hours post-administration, followed by a plateau phase.
There are some limitations to this study. In studies involving comparisons among the three groups, using sample size calculation methods designed for two groups is inaccurate. We have revised the paper to clearly position the work as an exploratory study. Consequently, future definitive studies are needed to estimate larger sample sizes based on this effect size. Specifically, this is a single-center study with a small sample size. Therefore, further expansion of the sample size is needed in the future to reinforce the validity of the protocol. The test protocol used in this study is mostly a rating scale developed based on the subjective feelings of patients, which may lead to unreliable results. Consequently, in the future, more objective data should be used in the analysis to minimize the impact of such errors on the results.
Conclusion
In summary, compared to traditional ropivacaine, the liposomal bupivacaine-based PENG block is superior in reducing the incidence of rebound pain. It reduces the number of postoperative analgesic pump presses and decreases opioid use, without impairing quadriceps muscle function, thereby accelerating patient postoperative recovery.
Data Sharing Statement
Data available upon reasonable request from the corresponding author, Xiaoqiong Xia.
Acknowledgments
We are grateful to all participants, data providers, and contributing authors.
Funding
Clinical Medicine Discipline Construction Project of Anhui Medical University (No. 2021lcxk040).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Vail EA, Feng R, Sieber F, et al. Long-term outcomes with spinal versus general anesthesia for hip fracture surgery: a randomized trial. Anesthesiology. 2024;140:375–386. doi:10.1097/ALN.0000000000004807
2. Guay J, Kopp S. Peripheral nerve blocks for Hip fractures in adults. Cochrane Database Syst Rev. 2020;11:Cd001159.
3. Girón-Arango L, Peng PWH, Chin KJ, et al. Pericapsular Nerve Group (PENG) block for hip fracture. Reg Anesth Pain Med. 2018;43:859–863.
4. Lin DY, Morrison C, Brown B, et al. Pericapsular nerve group (PENG) block provides improved short-term analgesia compared with the femoral nerve block in Hip fracture surgery: a single-center double-blinded randomized comparative trial. Reg Anesth Pain Med. 2021;46:398–403. doi:10.1136/rapm-2020-102315
5. Barry GS, Bailey JG, Sardinha J, et al. Factors associated with rebound pain after peripheral nerve block for ambulatory surgery. Br J Anaesth. 2021;126:862–871. doi:10.1016/j.bja.2020.10.035
6. Yin W, Luo D, Mi H, et al. Rebound pain after peripheral nerve block: a review. Drugs. 2025;85:991–1002. doi:10.1007/s40265-025-02196-8
7. Quaye A, McAllister B, Garcia JR, et al. A prospective, randomized trial of liposomal bupivacaine compared to conventional bupivacaine on pain control and postoperative opioid use in adults receiving adductor canal blocks for total knee arthroplasty. Arthroplasty. 2024;6:6. doi:10.1186/s42836-023-00226-y
8. Singla P, Ye Y, Elkassabany NM, et al. ‘Pain as regional anaesthesia wears off’ or ‘rebound pain’: what’s in a name? Anaesthesia. 2025;80:607–611. doi:10.1111/anae.16583
9. Andrade PP, Lombardi RA, Marques IR, et al. Pericapsular Nerve Group (PENG) block versus fascia iliaca compartment (FI) block for hip surgery: a systematic review and meta-analysis of randomized controlled trials. Braz J Anesthesiol. 2023;73:794–809. doi:10.1016/j.bjane.2023.07.007
10. Chen L, He W, Liu X, et al. Application of opioid-free general anesthesia for gynecological laparoscopic surgery under ERAS protocol: a non-inferiority randomized controlled trial. BMC Anesthesiol. 2023;23:34. doi:10.1186/s12871-023-01994-5
11. Kim CH, Yang JY, Min CH, et al. The effect of regional nerve block on perioperative delirium in Hip fracture surgery for the elderly: a systematic review and meta-analysis of randomized controlled trials. Orthop Traumatol Surg Res. 2022;108:103151. doi:10.1016/j.otsr.2021.103151
12. Mosaffa F, Taheri M, Manafi Rasi A, et al. Comparison of pericapsular nerve group (PENG) block with fascia iliaca compartment block (FICB) for pain control in hip fractures: a double-blind prospective randomized controlled clinical trial. Orthop Traumatol Surg Res. 2022;108:103135. doi:10.1016/j.otsr.2021.103135
13. Liang L, Zhang C, Dai W, et al. Comparison between pericapsular nerve group (PENG) block with lateral femoral cutaneous nerve block and supra-inguinal fascia iliaca compartment block (S-FICB) for total hip arthroplasty: a randomized controlled trial. J Anesth. 2023;37:503–510. doi:10.1007/s00540-023-03192-6
14. Singh NP, Makkar JK, Chawla JK, et al. Prophylactic dexamethasone for rebound pain after peripheral nerve block in adult surgical patients: systematic review, meta-analysis, and trial sequential analysis of randomised controlled trials. Br J Anaesth. 2024;132:1112–1121. doi:10.1016/j.bja.2023.09.022
15. Fallon F, Ramly MS, Moorthy A. Rebound pain after regional anaesthesia. Medicina. 2025;61:790. doi:10.3390/medicina61050790
16. Woo JH, Lee HJ, Oh HW, et al. Perineural dexamethasone reduces rebound pain after ropivacaine single injection interscalene block for arthroscopic shoulder surgery: a randomized controlled trial. Reg Anesth Pain Med. 2021;46:965–970. doi:10.1136/rapm-2021-102795
17. Touil N, Pavlopoulou A, Barbier O, et al. Evaluation of intraoperative ketamine on the prevention of severe rebound pain upon cessation of peripheral nerve block: a prospective randomised, double-blind, placebo-controlled study. Br J Anaesth. 2022;128:734–741. doi:10.1016/j.bja.2021.11.043
18. Girón-Arango L, Peng P. Pericapsular nerve group (PENG) block: what have we learned in the last 5 years? Reg Anesth Pain Med. 2025;50:402–409. doi:10.1136/rapm-2024-105427
19. Hussain N, Speer J, Abdallah FW. Analgesic effectiveness of liposomal bupivacaine versus plain local anesthetics for abdominal fascial plane blocks: a systematic review and meta-analysis of randomized trials. Anesthesiology. 2024;140:906–919. doi:10.1097/ALN.0000000000004932
20. Kim DH, Liu J, Beathe JC, et al. Interscalene brachial plexus block with liposomal bupivacaine versus standard bupivacaine with perineural dexamethasone: a noninferiority trial. Anesthesiology. 2022;136:434–447. doi:10.1097/ALN.0000000000004111
21. Chan TCW, Wong JSH, Wang F, et al. Addition of liposomal bupivacaine to standard bupivacaine versus standard bupivacaine alone in the supraclavicular brachial plexus block: a randomized controlled trial. Anesthesiology. 2024;141:732–744. doi:10.1097/ALN.0000000000005035
22. Mont MA, Beaver WB, Dysart SH, et al. Local infiltration analgesia with liposomal bupivacaine improves pain scores and reduces opioid use after total knee arthroplasty: results of a randomized controlled trial. J Arthroplasty. 2018;33:90–96. doi:10.1016/j.arth.2017.07.024
23. Hamilton TW, Knight R, Stokes JR, et al. Efficacy of liposomal bupivacaine and bupivacaine hydrochloride vs bupivacaine hydrochloride alone as a periarticular anesthetic for patients undergoing knee replacement: a randomized clinical trial. JAMA Surg. 2022;157:481–489. doi:10.1001/jamasurg.2022.0713
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.