Back to Journals » Risk Management and Healthcare Policy » Volume 14
The Effect of Peer Education on Decision-Making, Smoking-Promoting Factors, Self-Efficacy, Addiction, and Behavior Change in the Process of Quitting Smoking of Young People
Received 9 September 2020
Accepted for publication 28 January 2021
Published 5 March 2021 Volume 2021:14 Pages 925—945
DOI https://doi.org/10.2147/RMHP.S280393
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Marco Carotenuto
Ozgul Orsal,1 Ayse Ergun2
1Eskisehir Osmangazi University, Faculty of Economics and Administrative Sciences, Department of Business/Department of Management and Organization, Eskisehir, Turkey; 2Marmara University Faculty of Health Sciences Department of Nursing, Istanbul, Turkey
Correspondence: Ozgul Orsal
Faculty of Economics and Administrative Sciences, Department of Business/Department of Management and Organization, Eskisehir Osmangazi University, Eskisehir, Turkey
Email [email protected]
Purpose: The study aims to examine the effect of peer education on the decision to quit smoking, factors that encourage smoking, self-efficacy, addiction, and behavior change in students who apply to the Youth Friendly Center to quit smoking.
Participants and Methods: This research is a Randomized Controlled Trials study. The experimental group consisted of students who were enrolled in the peer education course (n=759). The control group has consisted of students (n=1095) who did not enroll in this course.
Results: Participants in the experimental group to quit smoking, more than the control group (p> 0,01). The addiction level of the participants in the experimental group, less than the participants in the control group (p> 0,01). According to the scores of the participants in the control group of the participants in the experimental group, the factors that trigger smoking, and the benefit sub-dimension scores in the Decision Balance Scale were low. Loss sub-dimension scores, which show the losses from the harms of smoking, increased significantly in the Self-Efficacy Scale, Behavior Change Process Scale, and Decision Balance Scale (p> 0,01).
Conclusion: Peer educators trained by the researcher and her team in the Youth Friendly Center Smoking Quit Program have an important effect in supporting/improving the cognitive and behavioral change processes of university students in smoking quit compared to those who do not receive an education. 94% success of the smoking quit program; Students’ voluntary application to receive professional support, students’ voluntary attendance of the treatment program for 6 months, strong communication and feedback, effective and functional professional counseling, and social support depend on strengthening the program with peer education. Especially with peer education, the development of leadership and role model characteristics made the smoking quit program preferred by students.
Keywords: health promotion and risk management, youth-peer education, smoking quit, randomized controlled trial, university student, youth studies, cognitive/behavioral processes
Introduction
The WHO defines smoking addiction as regular smoking within at least one month, having withdrawal symptoms when quitting, inability to quit despite the harms, and unsuccessful smoking quit attempts.1 Nicotine is the most important addictive ingredient in cigarettes. Nicotine easily crosses the blood-brain barrier, stimulating acetylcholine receptors in the ventral tegmental area promoting the release of dopamine oscillation which relaxes the person. This reward system creates the need to smoke again, and 50% of those who try to smoke develop an addiction.1–3 In the United States, about one in 13 Americans age 17 and older have smoked.4 According to Young with Turkey Statistics Institute releases 2017 statistics, the incidence of smoking between the ages of 15–24, 28.2% for males and 7.8% for women. In the WHO 2018 report, the prevalence of smoking among young people; 20.6% boys, 26.6% girls in Italy; 18% boys, 20% girls in France; 6% boys, 8% girls in England; 5% boys, 3% girls in Norway.1 According to the WHO 2018 report attempts to quit smoking; in young people between the ages of 13 and 15 decreased in 20 of the 108 countries from 1999 to 2016, did not change in 43 countries, and increased in 18 countries.1 According to the Turkey Global Adult Tobacco Survey 2012, attempts to quit smoking in young people between the ages of 15 and 24 decreased from 52.3% in 2008 to 40.2% in 2012.5
Despite quitting programs and political regulations, the prevalence of young smokers is still high today and the decrease in quitting rates indicates the need for continued studies on this issue. WHO’s a tobacco-free initiative program, the abbreviated MPOWER (Monitor/Protect/Offer/Warn/Enforce/Raise), provided tools to evaluate the effectiveness of the programs to reduce the frequency and number of daily smoking and increase the rate of quit smoking. WHO emphasizes that these tools should be implemented in the field and successful examples are needed.1
The university period has been defined as a period in life in which negative-positive health behaviors can be acquired. It is emphasized that young people in this period should be protected from risky behaviors and should be educated to gain healthy behavior changes.1 University student can gain healthy behavioral changes by reaching the right education method, right place/environment, right person/peer.4–6 Therefore, youth-friendly units that carry out health-promoting practices are of great importance to optimize the health of university students, who have a significant population.6,7 To optimize the health of students, who will be carried out in youth-friendly units that undertake the school health of universities, there is a need for health-promoting programs (for example, smoking quit, gaining health-enhancing behavioral changes).6,7 Health education and counseling in programs have an important place in popularizing smoking prevention and quitting strategies. These programs held at the university provide leadership, coordination, program management, and guidance in the development of strategies in the field of school health.6,7 While performing these roles, effective interpersonal communication techniques, motivational interview techniques, and theoretical elements that explain the behavior of individuals are used. Theory and models used for behavior change; Social Learning Theory, Health Belief Model, Planned Behavior Theory, Health Promotion Model, and Transtheoretical Model -TTM. It is stated that motivational interviews with individuals based on TTM are effective in behavior change and facilitate behavioral change.8,9
Existing studies in the literature to change the problematic health behaviors of young people regarding smoking quit are descriptive and short-term.10–14 In the studies conducted, four smoking quit programs for young people are mentioned. These are counseling techniques, nicotine patch therapy, counseling, and technology (internetandtelephoneandcomputer) supported programs. Despite these programs, among university students risky smoking still on the agenda protects. Because quitting smoking and changing behavior requires a long process, follow-up, and support. Especially the university period, when risky behaviors and smoking rates are high, should be considered. Because of the university, individuals have to live in cities far from their families. Interaction with peers is more common in the city they go to because of the university. Therefore, peer education is important in youth smoking prevention and quit programs. There is a need for youth-friendly health units with experts who know how to work with peers. Although there are studies in the literature on smoking specifically to different age groups; There are no experimental studies on smoking quit decisions, factors that encourage smoking, social peer support, self-efficacy, addiction, and behavioral change specific to university students with long-term follow-up and support. This study was conducted to eliminate all these deficiencies in the literature.
Objective
The study aims to examine the effect of peer education on smoking quit decisions, factors that encourage smoking, self-efficacy, addiction, and behavior change in students who apply to the Youth Friendly Center-YFC to quit smoking.
Our Research Questions
- What are the factors affecting the decision of students to quit smoking with and without peer education?
- Do students in groups with and without peer education affect quitting smoking and, reducing nicotine addictions (Fagerstrom)?
- Do students in groups with and without peer education affect quitting smoking, increasing their self-efficacy, and smoking-promoting factors?
- Do students in groups with and without peer education have an impact on the losses and benefit scores of decisions to quit smoking?
- Does it affect smoking to quit, cognitive, and behavioral change process scores of students in groups who have peer education and who do not have peer education?
Methods
Study Design and Participants
This study is a “Randomized Controlled Trials” study on university students (n=1.854) who applied to YFC for “quitting smoking” between June 2008 and June 2018. Before starting the “smoking quit program” applied in YFC, the program and its applications were explained to the applicants. Before the first counseling was given, each student voluntarily stated that they wanted to quit smoking within 30 days. Also, a commitment was made stating that they are willing to come to the next consultancy, change their behavior, and adapt to treatment by making the plans and applications determined in the counseling. A total of 40 students, 30 students with three months to graduation, and 10 students who did not want to make a contract were not included in the treatment program (Figure 1). See participant flow chart in Figure 1.
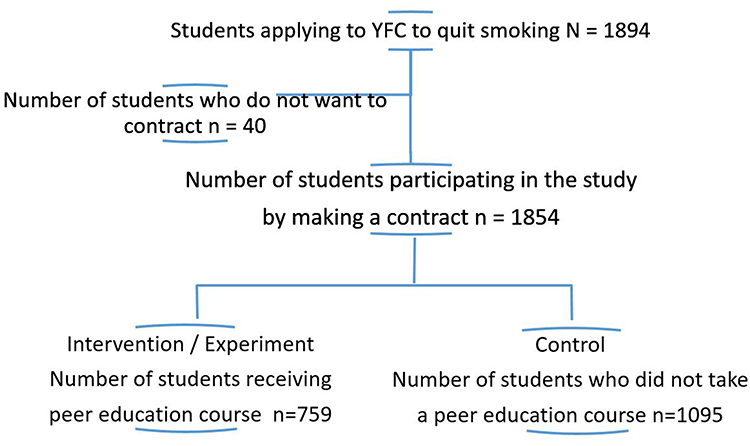 |
Figure 1 Participant flowchart. |
Power analysis of our sample size was performed by G-Power. It was determined that there were 1854 participants with standard power equal to 95%, effect size 0.3, and alpha sample size 0.05. Participants were students who applied to quit smoking (n=1854). The experimental group consists of students (n=759) enrolled in the peer education course. The control group consists of students (n=1095) who did not enroll in this course (Figure 1).
YFC
The Youth Friendly Center (YFC) has been providing school-based primary health services (preventive, treatment, rehabilitation) to university students since 2003. YFC, in school-based primary health care services; conducts necessary intervention programs to protect the health, prevent risk factors that damage health, and gain healthy lifestyle behaviors. One of these programs is the smoking quit program. The theoretical framework of the program was developed by the researcher. Two approaches were used in the theoretical framework of the program. First; Smoking Quit Methods General Approach from Non-Drug Therapies to Smoking Quit Therapies Stepped Treatment Method (5A); Ask, Advise, Assess, Assist, Arrange.1,15 The second is; It is the Transtheoretical Model (TTM) developed by Prochaska and DiClemente in 1982.9
The program includes professional counseling, training (peer education and peer tutor training), and Social support practices (peer and professional) based on these two approaches. Programs for all these health promotion practices were coordinated by the researcher. Except for the first interview in the smoking quit program, each student was followed up every 20 days for a total of 6 months, with eight follow-ups. Each student filled in all relevant scale questionnaires to measure cognitive and behavioral changes in eight follow-up periods. Besides, professional in-depth consultancy service was provided face-to-face after filling the relevant registration forms with information on whether the practices given in the previous consultancy were carried out or not. According to the needs determined in the counseling processes, social support programs specific to each student was given continuous support for six months. Study design flowchart sees Figure 2.
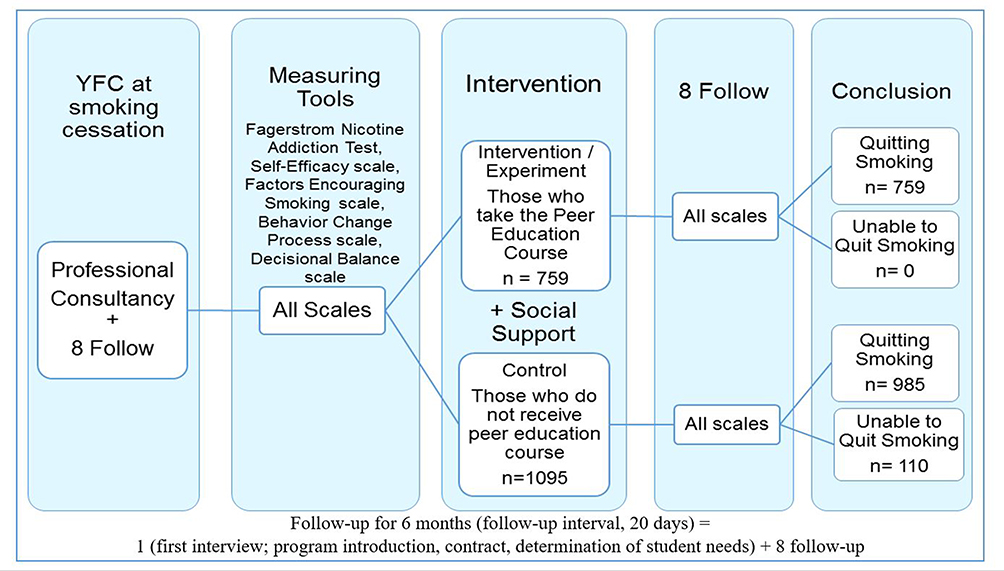 |
Figure 2 Study design flowchart. |
When the students faced obstacles in quitting smoking, they made use of the YFC coordinated social support activities by calling YFC by phone. Each student attended the social peer support program a minimum of 5 and a maximum of 40 times (Figure 3A and B).
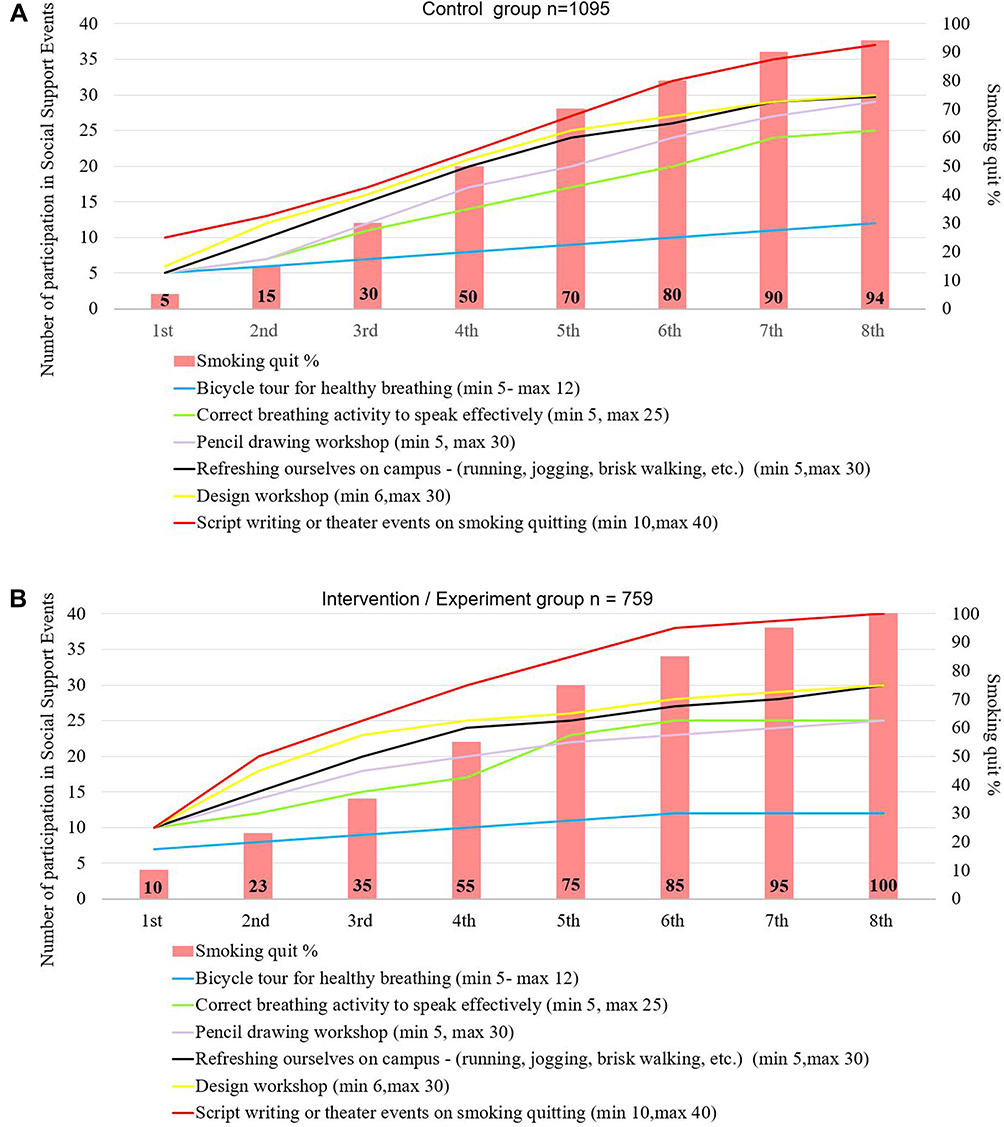 |
Figure 3 The students’ in the experimental and control groups according to eight follow-up results Numbers of participation in social support events’ and smoking quit of rate. |
Education, among the students who applied to YFC to quit smoking, those who wanted to receive peer education, were selected by the deanships in their faculty who meet the peer education criteria.
Professional Consultancy;
- Self-knowledge and self-efficacy were strengthened to gain alternative planning behavior when smoking was desired. Alternative Plan Cards (time, mood/mood, place, what he does instead of smoking) were used when smoking was requested after the counseling.
- At least 4 of the smoking quit strategies chosen by each student were determined. The necessary professional consultancy was given. Social peer support specific to the student was provided when it was difficult to act.
- Behavior change plans were created. The most important reasons and goals for wanting to quit smoking were determined. Plans to be made to achieve their goals were drawn up. He was encouraged to act. After the consultancy, plan cards (special activities, time, place, the realization of the plan) were used to achieve the goals in practice.
- The people who will help each student in the behavior change process and how they will help were determined. After the counseling, in practice, with the “social support system and peer support”, people who will help during behavior change and help techniques were determined. Whether the application was made or not, the success status was followed and the necessary support was provided.
- Each student was given counseling on possible obstacles to behavior change and coping techniques.
- In each professional consultancy given for six months, the results of all plans and applications were reviewed and the necessary consultancy was provided.
Intervention/Experiment
The intervention group includes peer education and practices in small closed groups of 16 people by the researcher and her team to increase the use of health services and health-promoting behaviors of young people who smoke. The intervention group consists of students who apply to YFC to quit smoking, want peer education, meet the peer education criteria, selected by the deans of the faculty.
Peer education has two stages. The first is peer education, the second is peer trainer training. 40% theoretical and 60% interactive techniques were used in the training. Among the 1854 students who applied to quit smoking, 759 volunteers, selected according to peer education criteria, received peer education. For the peer trainer training program, which is the second training; 259 people, 759 of whom completed the peer education, were trained according to the peer trainer training criteria. According to the smoking quit program after the training, each student completed 8 applications. Peer education; Peer Education is an education that lasts a week (7days) between 8.30–17.30 every day. Peer trainer training; Peer Trainer Training is a training that lasts two weeks (14days) every day between 8.30–17.30.
Randomization 1 with “Play to the Winner” to Avoid Selection Bias: Peer Education Receiving Criteria
To have completed the application form to voluntarily receive peer education. School grade point average; Being over 2 according to the 4 system, wanting to quit smoking. Having worked as a volunteer in a non-governmental organization before. To have social skills in which he is strong; For example; Play an instrument; making cartoon drawings; have theatrical talent; to have design skills; writing a script, etc. Having a reference to having effective speaking skills and leadership skills approved by his professors in the field.
Randomization 2 with “Play to the Winner” to Avoid Selection Bias: Peer Trainer Training Receiving Criteria
Having completed a week of peer education and voluntarily completed the peer trainer training application form. Completing at least 5 of the social support programs related to the subject after the training. To know a foreign language. Receiving at least 5 positive feedback (stating the rationale for the events experienced in the subjects such as effective communication skills, having the right information, problem-solving skills, etc.) by the participants of the social and peer support program.
Education Topics
The harms of cigarette/tobacco use and exposure to second-hand cigarettes, ways of protection. Legal regulations and penalties for the use of cigarettes and tobacco products. Coping methods with cigarette/tobacco use; Being able to say “No” to cigarette and tobacco derivatives. Gaining health-enhancing behaviors; “Why Smokeless Environments”. Creating a campus free from cigarettes and tobacco products and practices that raise awareness about their harm. Breathing exercises for correct breathing and diction in 8 steps with the diaphragm technique. Strengthening leadership, effective speaking, and teamwork skills; The ability to demonstrate exemplary behavior to students in need and to direct them to professional units that offer smoking quit services.
Training Output
Producing slogan, to make a poster brochure, writing and playing role plays, organizing creative awareness activities for groups who smoke or taking part in organized events, to be able to plan and carry out group work on the subject. According to the post-training smoking quit program, each student completed 8 applications.
Social Support
The obstacles and alternative solutions that every student may encounter in the smoking quit process are social support applications made by evaluating the cards they offer. This program was coordinated and directed by the researcher. All programs were held at least twice each month for six months. All programs were planned and implemented in line with the sustainable development goals, the third substance, healthy individuals, and healthy life recommendations. The programs applied are as follows (Figure 3A and B)
- Bicycle tour to breathe healthily: Coordinated bicycles were provided free of charge by the municipality. Groups were formed with students in the smoking quit program who were interested in this social support program. Volunteer peer trainers who are professional cycling were chosen as the group leaders. The practice has been completed successfully.
- Correct breathing activity to speak effectively (smooth sound management with breathing techniques): 2 teachers and a physical environment were provided from the provincial public education center. Groups were formed with students in the smoking quit program who were interested in this social support program. In the program, breathing exercises for correct breathing and diction were taught with the diaphragm technique.
- Pencil drawing workshop: In the program, two teachers from the municipality, pencil drawing experts, supported the program. Groups were formed with students in the smoking quit program who were interested in this social support program. Volunteer peer educators who had talented pencil drawing work in middle school and high school periods led the groups.
- Refreshing ourselves on campus (running, jogging, brisk walking, etc.): Groups were formed with students in the smoking quit program who were interested in this social support program. The peer educators selected for this group led the groups.
- Design workshop: “Come on, design with us, and show your creativity” (Cigarette themed poster, bookmark, brochure design). Two teachers, who are experts in cigarette-themed posters, bookmarks, and brochure design, supported the program. Groups were formed with students in the smoking quit program who were interested in this social support program.
- Scriptwriting or theater events on smoking quitting: Two teachers specializing in scriptwriting or theater activities supported the program. Groups were formed with students in the smoking quit program who were interested in this social support program.
Definitions
Smoking Quit Methods Non-Drug Therapies General Approach to Smoking Quit Therapies Stepped Treatment Method (5A)1,15,16
In the guideline published by the US Ministry of Health in 2014,16 the things to be done in approaching a smoking patient were collected under the title of “5A”. These strategies are; 1A=Ask; Identify the use of tobacco at each visit of all patients and record them with their vital signs. In this query, to predict the degree of addiction and to adjust the treatment dose, it is questioned how long he has smoked, the number of cigarettes he smokes per day when he smokes his first cigarette after getting up in the morning. Other than cigarettes, nicotine-containing substances (hookah, e-cigarette, etc.) and exposure to passive smoking should also be questioned. Difficulties such as nicotine withdrawal syndrome in smoking quit should be revealed. Environmental triggers such as drinking coffee, drinking alcohol, smoking at home, being in a smoking environment should also be questioned. Smokers should be alert to these triggers and develop individual activities such as talking to a friend, phone calls and breathing exercises to fight.
2A=Advise; It is the recommendation to Quitting Smoking. The quit message should be clear, strong, encouraging, and individualized.
3A=Assess; Evaluate your willingness to attempt to quit smoking and your nicotine addiction level. The duration of the smoking behavior and the amount they drink should be questioned and nicotine addiction should be evaluated. Sample; For those who drink; “Do you want to try to quit smoking in a month?”
4A=Assist-Support; Supporting and assisting the quit attempt. Suggestions for solving problems, social support, pharmacotherapy if there are no contraindications, and additional informative material should be provided.
5A=Arrange; To watch in the period after quitting. Those who quit smoking should be called for control at regular intervals and try to prevent them from starting to smoke again. If the person smokes more than 10 cigarettes a day, smokes his first cigarette within 30 minutes after waking up in the morning, and gives information that he feels physical deprivation during his quit attempts even though the number of cigarettes smoked is low, it can be considered sufficient to start pharmacotherapy. Primary care methods are seven. Five of these are nicotine-containing treatment methods (nicotine gum, nicotine inhaler, nicotine lozenge, nicotine nasal spray, and nicotine patch) while the other two (bupropion and varenicline) are nicotine-free treatments.
Transtheoretical Model (TTM); was developed by Prochaska and DiClemente in 1982. TTM is a conscious behavior change process model that focuses on the individual’s own decisions.9 First, the model used in smoking quit programs identified common points that reveal how individuals change their negative behaviors.9 In this model, Velicer, and Prochaska define change as a gradual, continuous, and dynamic structure.9 In traditional behavioral approaches, while change is considered as a sharp and direct result, the model focuses on helping individuals make a willful behavioral change and understanding the change process. TTM evaluates the correct evaluation of the results, the measurement of progress, and the effectiveness of the initiatives. Briefly, the Model includes the stages of Cognitive and Behavioral change.
Cognitive Processes
Increasing Awareness; It is to raise awareness about the causes, consequences, and solutions of problem behavior with initiatives such as feedback, training, conference, media. Emotional Arousal; It is the process that occurs when an individual experiences fear and very strong sadness about his problematic behavior. Reevaluating the Environment; It is the process by which an individual evaluates how his habits affect his physical and social environment. Social Liberation (Environmental Opportunities); It is the process of increasing awareness of social opportunities and alternative behaviors provided to individuals in society. Self-Reevaluation; It is the process of evaluating oneself by associating with a special cognitive and emotionally healthy or unhealthy habit. Desires desired to come true; It indicates the regret of the individual for starting unhealthy behavior and the desire for change.
Behavioral Processes
Presence of Helping Relations (Supporting), is the process that includes relationships that provide trust and support an individual for healthy behavioral changes. Stimulus Control (Reconstruction), is controlling the stimuli or choosing healthier alternatives instead of them to reduce the risk of restarting problematic behaviors. Opposing Running (Substitution), includes learning and using healthier behaviors that can be substituted for unhealthy behavior. Strengthening (Rewarding), includes the use of empowerment, rewarding initiatives for the individual to express himself positively. Agreement with itself (Individual Liberation), it is the belief of the individual in implementing his/her decisions to change, make decisions, and act with the belief of change. Change Levels (Dependent Variable Dimension), self-efficacy/incentive factors scales, and decision making scales constitute the last part of the Transtheoretical Model. These scales are sensitive measures against developments and continuity in the change process.9,17–20
Motivational Interviewing
It is a method developed for 30-minute interviews to involve individuals who are resistant to the change process.20 Motivation is a product of the interaction between people, it expresses a situation, not a feature. As an internal feature that varies according to personal characteristics and time and is affected by external factors, it reflects the state of being established in the individual to change.17,20 Motivational interviewing is to help people recognize and resolve contradictions, understand their problems, and take action. It is a useful method especially for people who have conflicts for change. The contradiction is the difference between two perceptions, and the degree of this difference affects the change positively or negatively, the greater the contradiction, the greater the significance of the change.17,20 How long the motivational interview lasts varies according to the study. In studies, it has been observed that individuals with motivational interviews are generally followed for periods ranging from a few months to a few years. It is stated that the interviews can be continued by phone after a meeting with the interviewees.17,20 Basic principles of Motivational Interviewing; the empathic approach is to reveal contradictions, fight resistance, support self-sufficiency (self-confidence). A motivational interview consists of two stages. Stage One is establishing the motivation for behavior change. It is focused on the importance and trust (competence). Stage Two is the strengthening of commitment to change. It involves being aware of readiness, increasing belief in change, and adhering to the change plan to complete the change.17,20
The Dependent Variable
Smoking Quit, Fagerstrom Nicotine Addiction Test, Self-Efficacy Scale, Smoking-Promoting Factors, Behavior Change Process Scale, and Decisional Balance Scale.
The Independent Variable
Effect of peer trainers, Socio-demographic characteristics.
Measurements
In our study, Socio-demographic characteristics, Fagerstrom Nicotine Addiction Test, Self-Efficacy Scale, Smoking-Promoting Factors, Behavior Change Process Scale, and Decisional Balance Scale were used.
Socio-Demographic Characteristics
The questions prepared by the researcher by scanning the literature are as follows; gender, age, the number of cigarettes smoked daily, how long have you been smoking? Have you ever tried to quit smoking? Smoking status of the mother, smoking status of the father, smoking status of friends, is there anyone smoking at your current home/dormitory, the status of studying youth-peer (Y-PEER) education. In this study, “smoking Quit” is defined as not smoking at all until the next professional consultancy (follow-up).
Fagerstrom Nicotine Addiction Test – FNAT
The assessment of nicotine addiction was performed with the FNAT developed in 1990 by Fagerstrom et al.9 Uysal et al assessed the Turkish validity in 2004.21 The test is six questions and the scores are in the range of 0–10. As scores increase, the level of dependency increases. There are five levels: non- addiction, low, moderate, high, and severe addiction. FNAT’s Cronbach alpha coefficient reported by Uysal et al,21 was 0.56, while in our study it was 0.85.
Self-Efficacy Scale – SES
Based on Bandura’s self-sufficiency theory, Velicer and colleagues developed this scale in 1990.17 Erol and Erdogan assessed the Turkish validity in 2007.10 High scores from the SES indicate the ability of the individual to stop smoking even in stimulating situations. SES has eight 5-point Likert items. The scores are in the range of 8–40. Anatchkova et al,22 reported the Cronbach alpha coefficient of the scale was 0.90, while our study found 0.85.
Smoking-Promoting Factors – SPF
Pallonen23 developed and Plummer19 determined school-based approaches. Anatchkova adapted it to adolescents in 2007.22 Erol and Erdogan assessed the Turkish validity in 2007.10 Obtaining a high score on the scale indicates a lack of ability to stop smoking in situations that make you want to smoke. SPF has eight 5-point Likert items. The scores are in the range of 8–40. The Cronbach alpha coefficient of the original scale was 0.90. In our study, the Cronbach alpha coefficient of the scale was 0.90.
Decisional Balance Scale – S-DBS
Velicer and his colleagues developed S-DBS in 1985.24 Plummer et al determined school-based approaches.19 Anatchkova et al adapted it to adolescents in 2007.22 Erol and Erdogan assessed the Turkish validity in 2007.10 It is a 5-point Likert assessment with 12 items. The scores are in the range of 12–60. It has two sub-dimensions: benefit and loss. Anatchkova’s Cronbach alpha coefficient was 0.94 and its sub-dimensions were 0.79–0.89. In our study, the Cronbach alpha coefficient for the loss sub-dimension was 0.92 and for the benefit, sub-dimension was 0.93.
Behavior Change Process Scale – BCPS
Prochaska developed the BCPS in 1988 for adults9 and Pallonen adapted it for adolescents in 1998.23 Erol and Erdogan assessed the reliability and validity of the scale in Turkish.10 BCPS is a 5-point Likert type assessment with 22 items containing cognitive and behavioral sub-dimensions. Cognitive processes are the factors associated with the individual’s emotions, values, and awareness. Behavioral processes show what behaviors the individual chooses as they move towards change. The scores range from 22 to 110. Higher scores on the BCPS indicate the probability of behavioral change success. The Cronbach alpha coefficient of the scale is reported as 0.849 and 0.83,10 while in our study it was 0.95.
Data Assessment
As a result of the analysis, the significance value of (p) for the peer education in the intervention/experiment group and the no peer education in the control group, according to the Test of Normality results, is p=, 000. This value is below the 0.05 significance level. Therefore, it can be said that the scores of All Scales (p; 0.000) do not have a normal distribution. Therefore, Mann–Whitney U-tests were used for intergroup comparison as they did not meet the assumptions of parametric tests. Analysis of variance (2x3ANOVA) was used for repeated measures used three or more times in the experimental and control groups in measuring the dependent continuous variable (all scales, smoking quit status). Also, the p-value in the Greenhouse and Geisser, Huynh, and Feldt corrections was examined. Since the sphericity assumption was not provided, p was lower than 0.05, the value p and F values in our analysis were examined. The Effect Size (partial eta-squared) is explained by the time variable.
Bonferroni method was used to prevent a type-I error that could interfere with the measurement process while paired comparisons were made with the Mann–Whitney U-test. In our study, using the Bonferroni method, a significant difference was evaluated between all scale measurements of the students according to eight follow-ups in multiple comparisons among eight tests, using the Bonferroni method, a significant difference was evaluated between all scale measurements of the students according to eight follow-ups in multiple comparisons among eight tests. In two-way ANOVA in repeated measurements, the Hypothesis is Degrees of Freedom=7, error Degrees of Freedom=1854.
Ethics
This study was approved by the Marmara University Faculty of Medicine Non-Invasive Clinical Research Ethics Committee with the number “M University-495”. Institutional approval was obtained from Eskisehir Osmangazi University Rectorate, Eskisehir Osmangazi University Health, Application, and Research Hospital. All participants were informed about the study and their verbal and written consents in accordance with the Declaration of Helsinki were obtained.
Results
Most (94.5%) of the students who formed the study group were male and the average age was 18.87±0.73 years old. Students smoked an average of 41.82±5.36 cigarettes per day for an average of 4.7±0.81 years. Although some (6.4%) of the students said they had never tried to quit smoking before, 36.7% said they had tried twice. Of the smokers, 42.6% of mothers, 97.0% of fathers, and 98.2% of friends also smoked. With YFC support, 94.1% of the students quit smoking. In the analysis of the data, qualitatively stated (quit smoking and did not quit smoking) gender, parents’ smoking status, etc. whether the difference between observed and expected frequencies is significant was evaluated by Chi-square analysis (Table 1). With peer education of the university student, the smoking quit sensitivity is 100%, and the specificity is 43.5%, and the likelihood is LR+=2.35. In men, 20-year-olds, those who smoked 50–60 cigarettes per day, smoked more than 6 years, had not tried to quit before, whose mother, father, and friends were smokers, who smoked at home/dormitory, and did not have peer support had significantly lower smoking quit rates (p<0.001; Table 1).
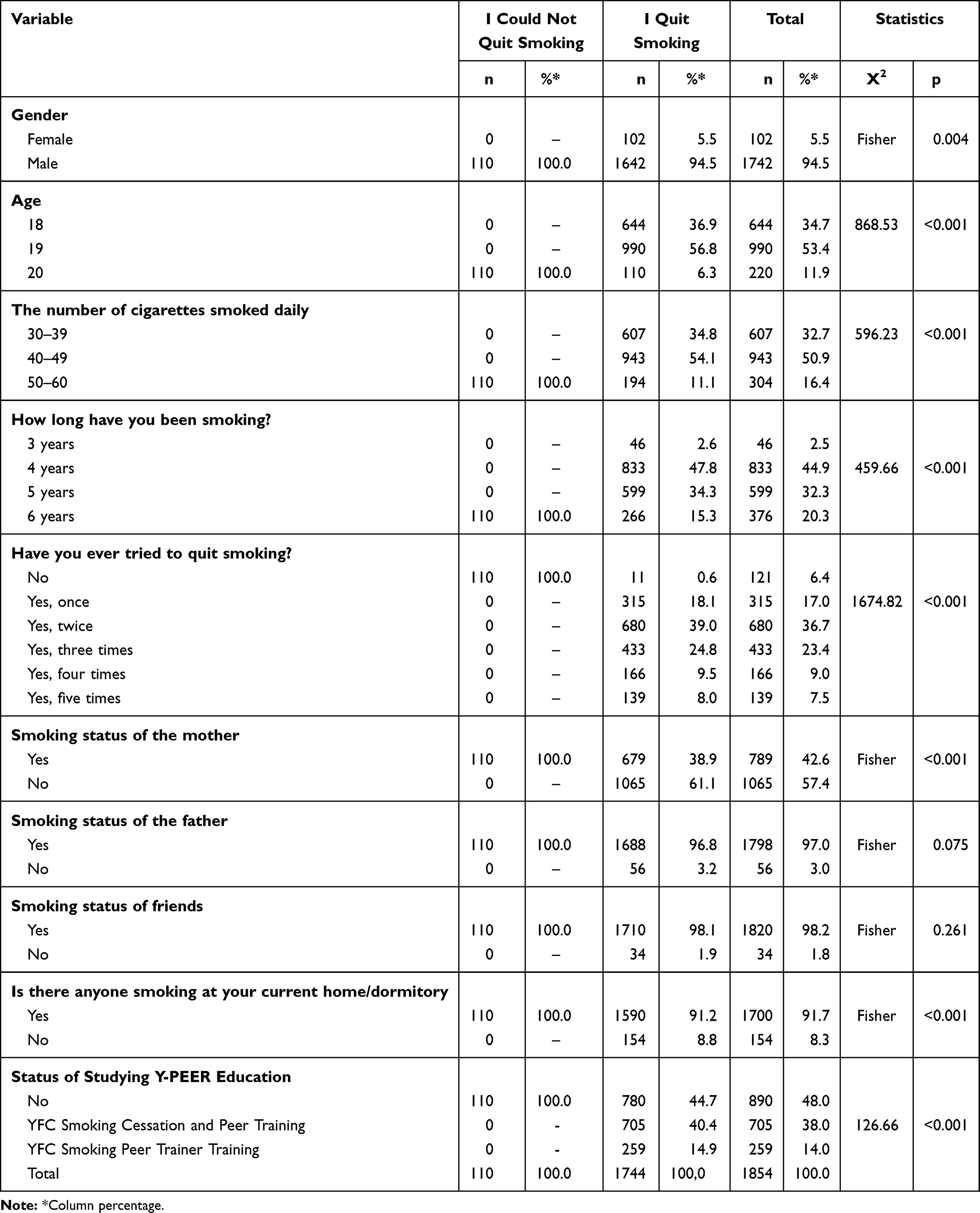 |
Table 1 Smoking Quit According to Sociodemographic Variables |
When Table 2 is examined, in the experimental and control group, the dependent continuous variable (Fagerstrom, Self-efficiency, Smoking-Promoting factors, Smoking Decision Balance Scale; Losses & Benefit and Behavior Change Process Scale; cognitive and processes) because it has been measured eight times, analysis of variance was used in repeated measures. As a result of the analysis, the significance value of (p) for the peer education in the intervention/experiment group and the no peer education in the control group, according to the Test of Normality results, is p=, 000. This value is less than the 0.05 significance level. Therefore, it can be said that the scores of All Scales (p; 0.000) do not have a normal distribution. Therefore, Mann–Whitney U-tests were used for intergroup comparison as they did not meet the assumptions of parametric tests. Analysis of variance (2x3ANOVA) was used for repeated measures used three or more times in the experimental and control groups in measuring the dependent continuous variable (all scales, smoking quit status). Besides, the p-value in the Greenhouse and Geisser, Huynh, and Feldt corrections was examined. Since the sphericity assumption was not provided, p was lower than 0.05, the value p and F values in our analysis were examined. Bonferroni method was used to prevent Type-I error that could interfere with the measurement process while paired comparisons were made with the Mann Whitney U-test. In our study, using the Bonferroni method, a significant difference was evaluated between all scale measurements of the students according to eight follow-ups in multiple comparisons among eight tests. In two-way ANOVA in repeated measurements, the Hypothesis is Degrees of Freedom=7, error Degrees of Freedom=1854.
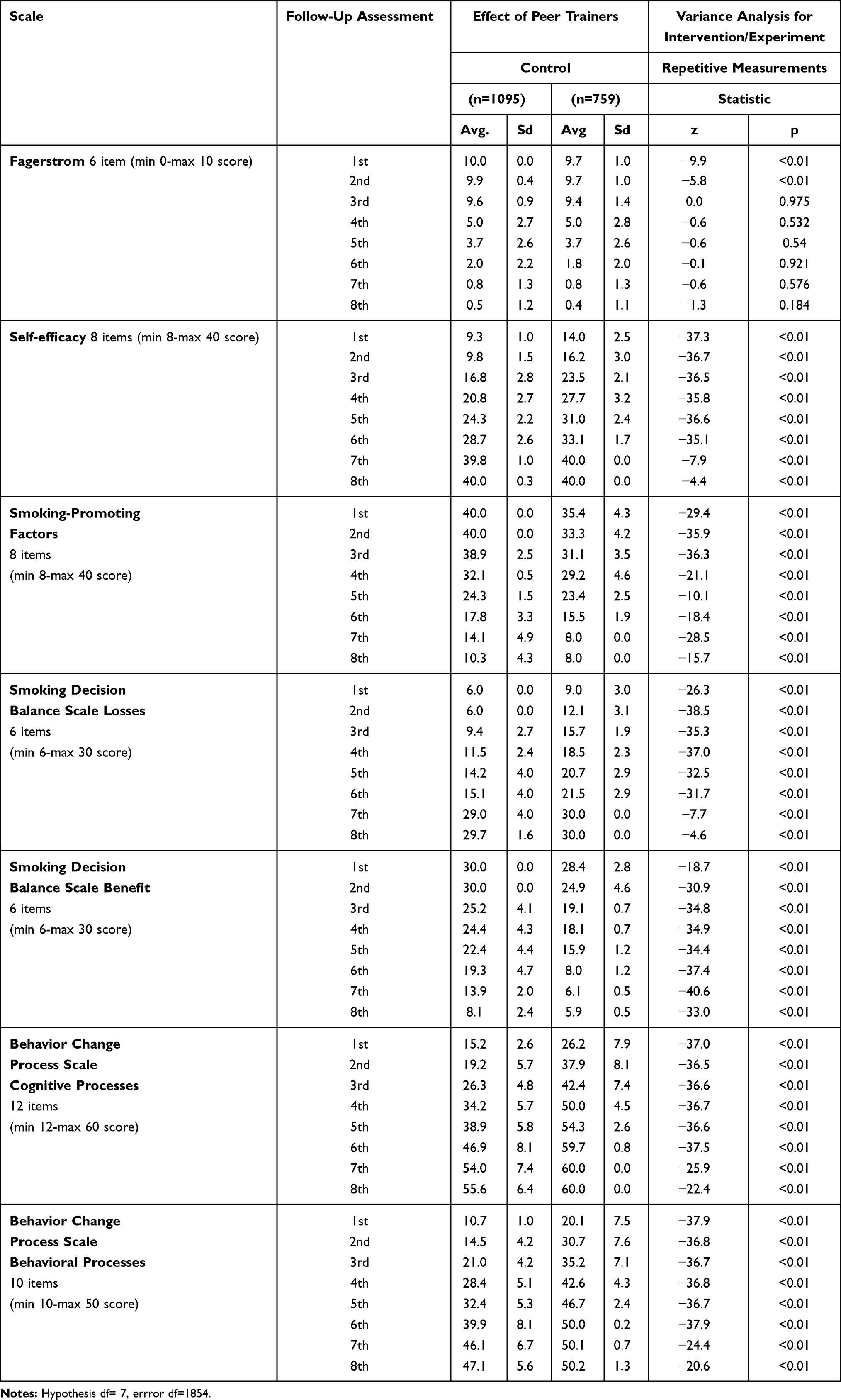 |
Table 2 Comparison of Fagerstrom, Self-Efficacy, Smoking-Promoting Factors, Decisional Balance Scale (S-DBS), Benefit, S-DBS-Losses, and Behavior Change Process Scale (BCPS) Mean Scores According to the Effect of Peer Trainers. Hypothesis df= 7, Error df=1854 |
According to the Fagerstrom nicotine addiction test, almost all students in the control and experimental groups had very high scores at the first follow-up. After the fourth follow-up, significant decreases were observed in the scores of the students in the control and experimental groups. Particularly, the decrease in the scores of the students in the intervention group was higher than the control group. At the seventh and eighth follow-up, 94% of the students did not have nicotine addiction and quit smoking (p<0.001) (Figure 4).
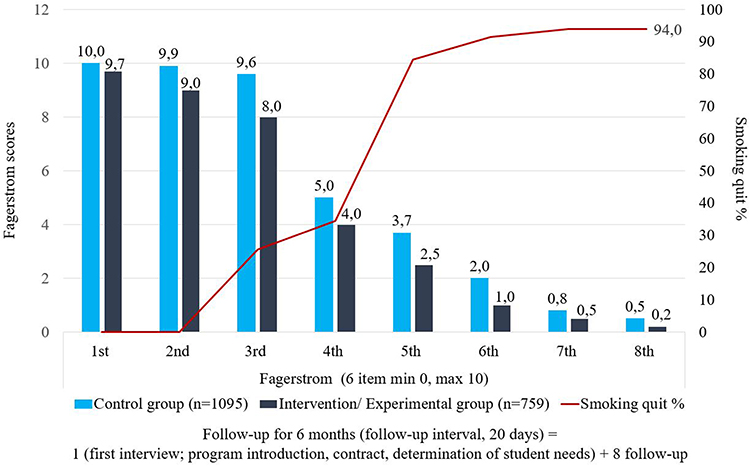 |
Figure 4 The students’ in the experimental and control groups according to eight follow-up results from Fagerstrom Nicotine Addiction Test scores and smoking quit rate. |
University students stated that peer educators affected reducing and quitting smoking. The results in the Fagerstrom addiction test are similar. Especially, Fagerstrom addiction test scores (avg 9.7) of students, who stated that peer educators affected were significantly lower in the first two follow-ups than those who stated that peer educators had no influence (avg 10.0–9.9). (p<0.001) (Table 2).
The mean scores of the students in the intervention and control groups of the self-efficacy scores from eight follow-ups are shown in Figure 5.
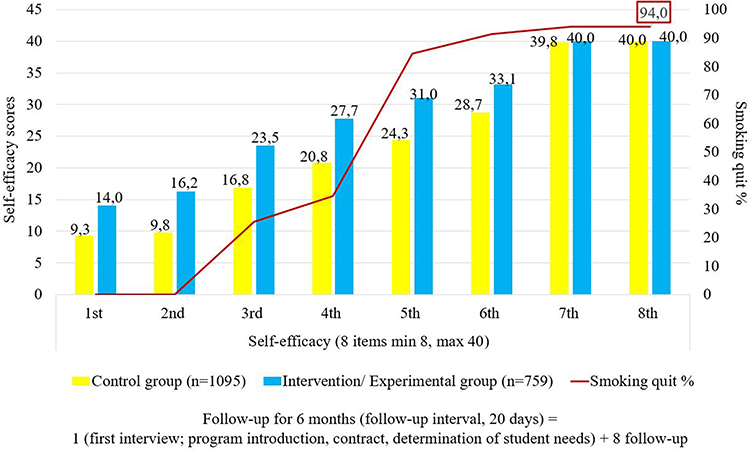 |
Figure 5 The students’ in the experimental and control groups according to eight follow-up results from self-efficacy scores and smoking quit of rate. |
The self-efficacy scores of the students in the intervention group were higher than the students in the control group in all follow-ups. These results are also statistically significant (Figure 5) (F=38,234.684, p<0.001).
The SES scores of the students who started the peer trainers were helpful were significantly higher in all the follow-ups than those who stated that the peer trainers did not affect. (p<0.001) (Table 2).
The scores obtained by the students in the intervention and control groups for the Smoking-Promoting Factors scores in eight follow-ups are shown in Figure 6.
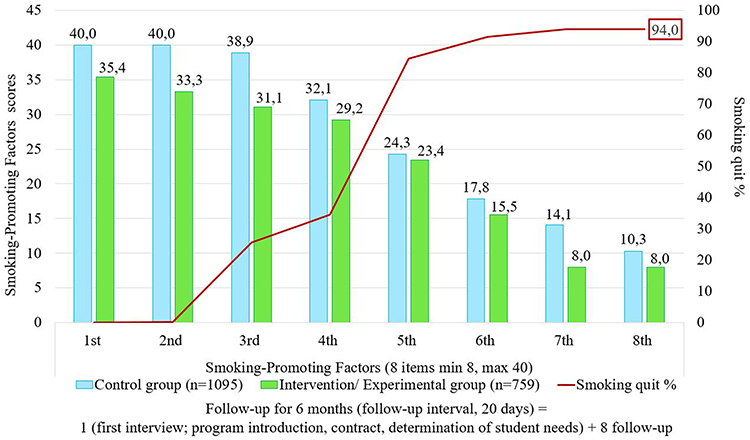 |
Figure 6 The students’ in the experimental and control groups according to eight follow-up results smoking-promoting factors scores and smoking quit of rate. |
According to the Smoking-Promoting Factors scores, almost all of the students in the control and experimental groups got very high scores in the first follow-up. After the fifth follow-up, significant decreases were observed in the scores of the students in the control and experimental groups. Especially, the decrease in the scores of the students in the intervention group is higher than the control group. At the eighth follow-up, the students’ Smoking-Promoting Factors scores were 8 in the intervention group and 10.3 in the control group, and 94% quit smoking. (F=11,177.557, p<0.001) (Figure 6).
Smoking-Promoting Factors scores of the students who stated that peer trainers affected were statistically lower in all follow-ups than those who stated that peer trainers did not affect (p<0.001) (Table 2).
The scores obtained by the students in the intervention and control groups for the Decision Balance Scale losses and benefit scores in eight follow-ups are shown in Figure 7A and B.
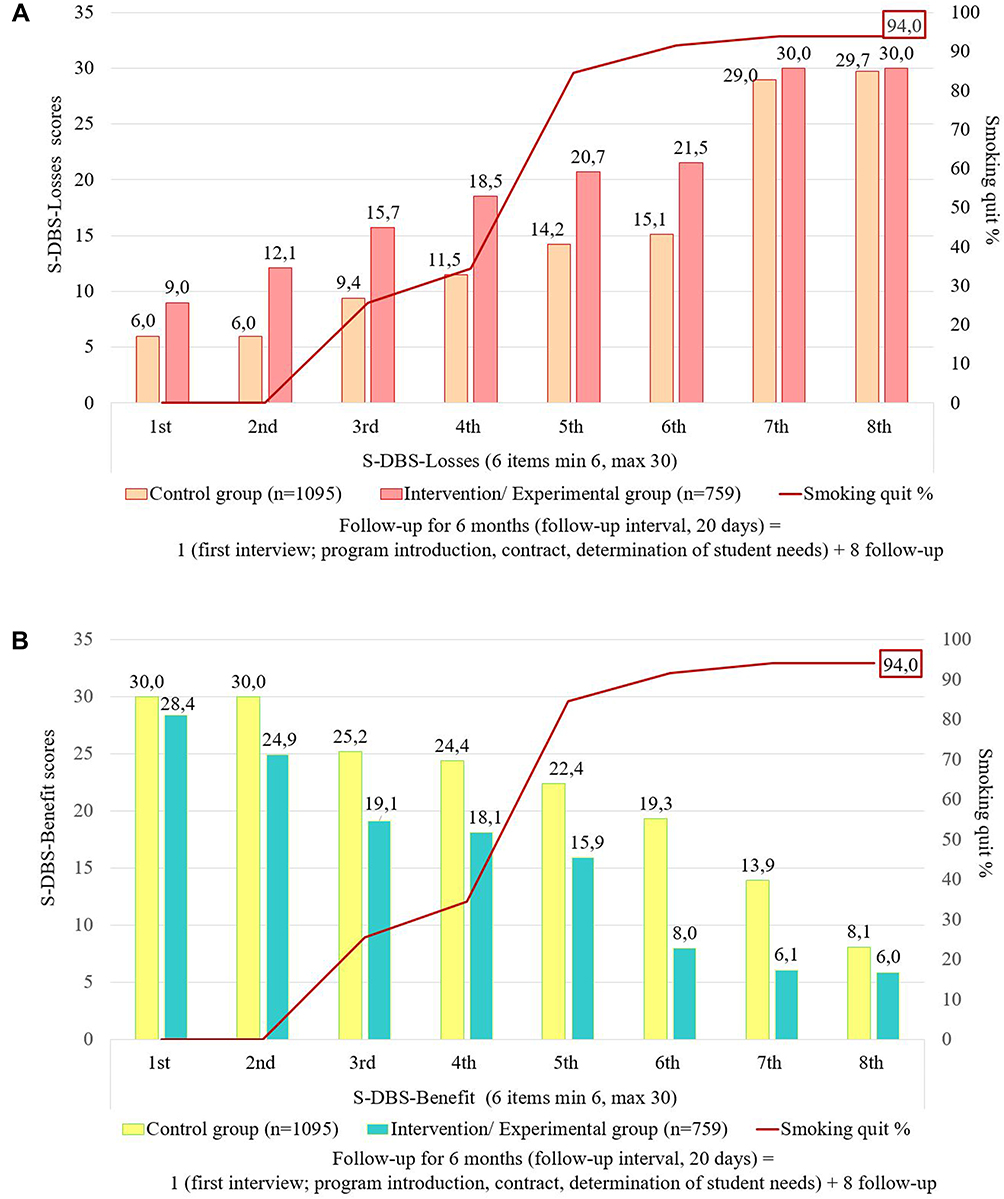 |
Figure 7 The students’ in the experimental and control groups according to eight follow-up results Decision Balance Scale losses and benefit scores and smoking quit of rate. |
According to the loss scores of the Decision Balance Scale, almost all of the students in the control and experimental groups received low min 6 and 9 points at the first follow-up. After the fifth follow-up, significant increases were observed in the scores of the students in the control and experimental groups. Especially, the increase in the scores of the students in the intervention group is higher than the control group. At the seventh and eighth follow-up, the Decision Balance Scale ‘losses scores were the highest max 30 for the students in the intervention group and 29.0 and 29.7 for the students in the control group (Figure 7).
According to the benefit scores of the Decision Balance Scale, almost all of the students in the control and experimental groups got the max score of 30.0–28.4 in the first follow-up. After the sixth follow-up, significant decreases were observed in the scores of the students in the control and experimental groups. Especially, the decrease in the scores of the students in the intervention group is higher than the control group. At the seventh and eighth follow-up, Decision Balance Scale benefit scores, while the min score for students in the intervention group was 6, it was 8.1 for the students in the control group (Figure 7A and B). Benefit scores on follow-up decreased significantly and loss scores increased. This result is statistically significant (p <0.001).
S-DBS benefit scores of students who stated that peer educators affected were significantly lower than those who stated peer educators did not influence all follow-up assessments, whereas the S-DBS-loss scores were higher (p<0.001) (Table 2).
The students’ in the experimental and control groups according to eight follow-up results Behavıor Change Process Scale cognitive and behavioral processes scores in eight follow-ups showed in Figure 8A and B.
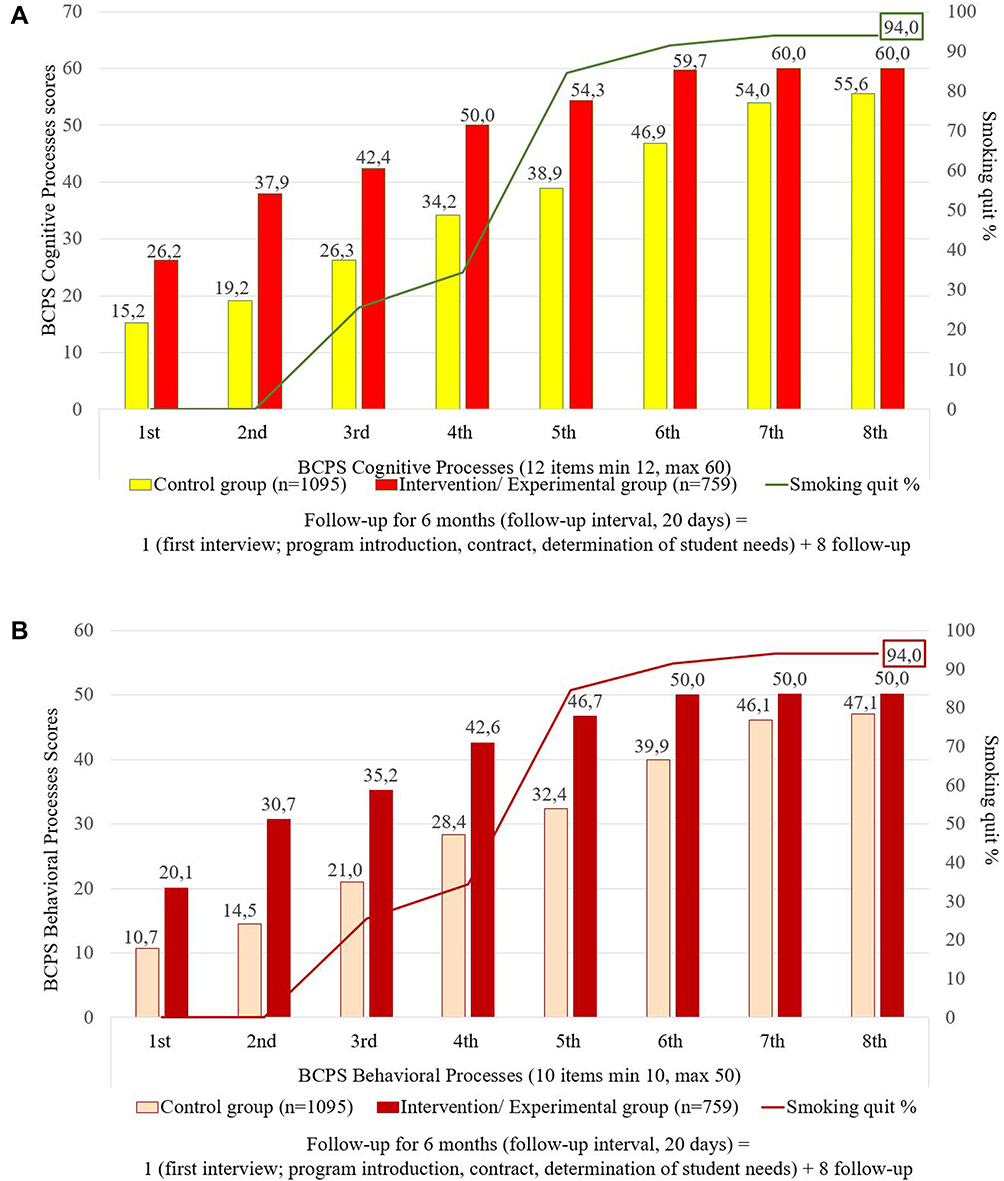 |
Figure 8 The students’ in the experimental and control groups according to eight follow-up results from Behavıor Change Process Scale cognitive processes and behavioral processes scores and smoking quit rate. |
According to the Behavıor Change Process Scale cognitive processes and behavioral processes test scores, almost all students in the control and experimental groups had very low scores at the first follow-up. After the fourth follow-up, a significant increase was observed in the scores of the students in the control and experimental groups. Particularly, the increase in the scores of the students in the intervention group was higher than the control group. According to the eight follow-up results of the students in the experimental group, the cognitive process scores of the Behavior Change Process Scale were higher than the control group, and they got a maximum of 60 points from the sixth and subsequent monitoring (Figure 8A and B). According to the eight follow-up results of the students in the experimental group, the behavioral process scores of the Behavior Change Process Scale were higher than the control group, and they got a maximum of 50 points from the sixth and subsequent monitoring (Figure 8A and B). This result is statistically significant (p<0.001). The BCPS scores of the students who stated that peer educators were beneficial were significantly higher in all follow-ups than those who stated that peer educators had no influence (p<0.001) (Table 2).
Discussion
What are the Factors Affecting the Decision of Students to Quit Smoking with and without Peer Education?
When we look at the gender of the students who applied to quit smoking, the number of men is higher. Similarly, in many countries around the world, men have a higher number of smoking than women. In this study, the smoking quit frequency of students participating in the smoking quit program in the Youth Friendly Center was found to be 94.1% after eight follow-ups. The frequency of smoking quit in young people varies between 15% and 80%.3,9,25,26 While several studies are showing the short term impact of smoking quit programs in young people,21 there are limited studies with long term follow-up.3,26 Long-term 5–16 follow-ups are more effective than short term 2–4 follow-ups.26 In this study, the high rate of smoking quit shows that the program implemented by YFC is effective. It is thought that providing peer training with a team of experts in the use of peer education, professional consultancy, and eight follow-ups of the program at 20-day intervals increase the effectiveness. Peer education in young people increases self-awareness, self-confidence, and knowledge of the risk factors concerning their health. Peer education is an effective method that promotes positive decision making and changes in risk-taking behaviors in all age groups.27–29
Similarly, in our study, peer educated students compared to non-peer educated students, FNAT, SPF, and S-DBS benefit subscale scores decreased significantly and SES, BCPS, and S-DBS-loss subscale scores increased significantly. One of the strengths of our study is that it is unique to university students between the ages of 18–20. University students in this age group, who mostly study in provinces far from their families, show a higher frequency of risky behavior. Indeed, in the literature, parents who smoke and teenagers who smoke26 had higher smoking addiction rates than parents who did not smoke.3,30 At the same time, the partner and friends’ circle affects smoking rates.3,26,30 Similarly, in our study, almost all of the students who smoked were smoking with their family, friends, and people around them. Smoking quit was lower in students with these variables (Table 1).
This result shows that students should be supportive of family and friends in smoking quit programs. Each individual is expected to communicate with the individuals around him, especially his peers, about the harms of smoking and the quit.3,26,28 In our study, all students who received peer education quit smoking. In line with this result, it is recommended to focus on peer education in smoking quit programs for young people.
According to the analysis results in our study, the factors that affect the smoking of university students are as follows; in men, 20-year-olds, those who smoked 50–60 cigarettes per day, smoked more than 6 years, had not tried to quit before, whose mother, father, and friends were smokers, who smoked at home/dormitory and did not have peer support had significantly lower smoking quit rates (Table 1). The reason for this may be that students who smoke more than 50 cigarettes experience more intense physiological withdrawal symptoms than those who smoke 30–49. The reason for this situation may be due to the cumulative effect of the addiction level of the students who have been smoking for more than 6 years. It may be recommended that smokers of 50 or more be supported by treatment centers where medical support is given more intensively, such as addiction clinics.
Do Students in Groups with and without Peer Education Affect Quitting Smoking and, Reducing Nicotine Addiction (Fagerstrom)?
Although the prevalence of smoking has decreased in the literature, it states that heavy nicotine addiction has increased.2,31,32 In our study, the students’ nicotine addiction (Fagerstrom) was high. This result is similar to the results of smoking quit outpatient clinic in the literature.20,31,33 The number of cigarettes smoked daily is one of the most important variables in determining nicotine addiction. Studies indicate that smoking reduction increases smoking quit rates.31 Similarly, in our study, 30–49 cigarette/day smoking students had a higher rate of smoking quit than 50–60 cigarette/day smokers did (Table 1). In the literature, it is reported that students’ nicotine addiction decreases after peer education.27 According to the results of the study, the students in the peer education group, according to students without peer education in eight follow-ups it has a significant effect on quitting smoking, and reduction of nicotine addiction (Fagerstrom) (Figure 4). Especially, Fagerstrom addiction test scores (avg 9.7) of students, who stated that peer educators affected were significantly lower in the first two follow-ups than those who stated that peer educators had no influence (avg 10.0–9.9). (p<0.001) (Table 2). This result shows the importance of peer support, especially in the early stages of smoking quit.
Do Students in Groups with and without Peer Education Affect Quitting Smoking, Increasing Their Self-Efficacy, and Smoking-Promoting Factors?
Self-Efficacy and Smoking-Promoting Factors
As self-efficacy increases, the perception of incentives decreases.9,22,32 Students’ self-efficacy increased as individuals progressed through behavior change stages. Reduced exposure to stimulating factors provides control over smoking behaviors with a final goal to quit smoking. It is known that young people with low self-efficacy are less motivated to quit smoking because they cannot change their cognitive perceptions and habits.32,34 Similarly, in our study, as follow up increased, students gradually obtained decreasing points from the SPF and increasing scores from the SES (Table 2; Figures 5 and 6).
It is thought that the students whose self-efficacy increases with peer education constantly exchange information, thus ensuring continuity of education. They form positive role models and encourage social learning with their friends.27–29,35 Similarly, in our study, the students in the peer education group according to students without peer education, in eight follow-up sessions, it has a significant effect on quitting smoking, increasing their self-efficacy and reducing smoking-promoting factors (Table 2; Figures 5 and 6). In one study, short-term and non-continuous peer education programs did not affect the smoking behavior of young people.33
Do Students in Groups with and without Peer Education Have an Impact on the Losses and Benefit Scores of Decisions to Quit Smoking?
Decisional Balance Scale
According to the Transtheoretical Model, as individuals progress in behavior change stages (non-thinking, thinking, preparation, movement, and sustaining), they are expected to increase their decision-making scores in the loss sub-dimension and decrease scores in the benefit sub-dimension.18–20,35–37 Similarly, in our study, compared to students without peer education, the peer education group had a significant effect on quitting smoking and decreasing S-DBS Benefit scores, and increasing S-DBS Loss scores in eight follow-ups (Table 2; Figure 7A and B). These results show that the effects of counseling, training, and empowerment practices vary according to the theoretical model structure and support progress.
Does It Affect Smoking to Quit, Cognitive, and Behavioral Change Process Scores of Students in Groups Who Have Peer Education and Who Do Not Have Peer Education? Behavior Change Process
The most successful behavioral changes occur in individuals who have experienced a relapse to the old behavior an average of three to four times and transition between stages.35,38,39 Similarly, in our study 23.4% of the students had tried quitting smoking 3 times, and 16.5% tried 4–5 times. Students who had tried to quit smoking gave up smoking at a higher rate than students who had not tried.
BCPS scores peak during the smoking quit phase and continue at the same level during the continuation phase.23,25,35,38 Similarly, in our study BCPS cognitive and behavioral process scores of smoking quit students increased. However, in some studies focused on a computer program, peer, and face to face training, these scores did not relate to the smoking quit rate.33,36,37 Change in individuals occurs through the use of cognitive methods such as awareness, sensory arousal, and reassessment of the environment.35,36,38 Similarly, in our study, compared to students without peer education, the peer education group had a significant effect on quitting smoking and increasing BCPS-cognitive process sub-dimension scores in eight follow-ups (Table 2; Figure 8A).
Individuals acting for change are expected to use behavioral methods (social emancipation, opposing conditioning, strengthening, control of stimuli, and supportive relationships).20,35,38 Similarly, in our study, compared to students without peer education, the peer education group had a significant effect on quitting smoking and increasing BCPS behavioral process sub-dimension scores in eight follow-ups (Table 2; Figure 8B). According to the service delivery (counseling, education, social support, etc.) at YFC, it can have a significant impact on the progress and smoking quit of the student through the initiatives it applies. More distinctly than in the literature, there was an increase in the scores of both cognitive and behavioral processes in smoking quit.37 It was emphasized by all students participating in the smoking quit program that there were complete trust and satisfaction throughout the process. The most important factors that provide full trust and satisfaction are; to be Youth Friendly Center that they can reach (inside the campus), having expert staff, professional counseling, peer education, social support, etc. it was specified as having a holistic program that includes interventions.
Conclusion and Suggestions
Risky behaviors are common among university students. That’s why the university period is so important. In the literature, in this example, no study was found, on average 18years old, who smoked 35 or more per day and examined the effects of their peers on healthy development. It is used to prevent risk factors as part of interventions to promote healthy behavior for young people, as well as improving school-based primary health care. Peer-Educators trained by the YFC has a significant effect on supporting/enhancing the cognitive and behavioral change process in university students’ quitting smoking. These practices increased the self-efficacy of smokers and 94% of students quit smoking. Our research results are thought to contribute to WHO and researchers working in this field.
Acknowledgments
The authors would like to thank all individuals who participated in this study.
Disclosure
The authors declare no conflicts of interest.
References
1. Word Health Organization WHO. Global report on trends in prevalence of tobacco smoking 2000–2025. 978-92-4-151417-0. World Health Organization WHO. 2017 Report on the Global Tobacco Epidemic, Youth. 2018.
2. Pérez-Ríos M, Santiago-Pérez MI, Alonso B, Malvar A, Hervada X, Leon J. Fagerstrom test for nicotine dependence vs. heavy smoking index in a general population survey. BMC Public Health. 2009;9:1–5. doi:10.1186/1471-2458-9-493
3. Chinwong D, Mookmanee N, Chongpornchai J, Chinwong SA. Comparison of gender differences in smoking behaviors, intention to quit, and nicotine dependence among Thai University Students. J Addict. 2018;8081670. doi:10.1155/2018/8081670
4. Delgado-Lobete L, Montes-Montes R, Vila-Paz A, et al. Individual and environmental factors associated with tobacco smoking, alcohol abuse and illegal drug consumption in university students: a mediating analysis. Int J Environ Res Public Health. 2020;17(9):3019. doi:10.3390/ijerph17093019
5. United States Substance Abuse and Mental Health Services Administration. National survey on drug use and health: detailed tables external icon. Substance Abuse Mental Health Data Archive. 2018.
6. Macedo TTS, Sheets D, Figueredo WN, Eickemberg M, Teixeira JRB, Mussi FC. Lifestyle risk behaviors of university students: a bibliometric analysis. Research, Society Development. 2020;9(10):e1699108624. doi:10.33448/rsd-v9i10.8624
7. Dietz P, Reichel JL, Edelmann D, et al. A systematic umbrella review on the epidemiology of modifiable health influencing factors and on health promoting interventions among university students. Front Public Health. 2020;8:137. doi:10.3389/fpubh.2020.00137
8. Cheung E, Romero T, Crespi CM, et al. Undergraduate support for university smoke-free and vape-free campus policies and student engagement: a quasi-experimental intervention. J Am College Health. 2020;1–9. doi:10.1080/07448481.2020.1782920
9. Prochaska JO, Velicer WF, Diclemente CC, Fava JL. Measuring processes of change: applications to the quit of smoking. J Consult Clin Psychol. 1988;56(4):520–528. doi:10.1037/0022-006X.56.4.520
10. Erol S, Erdoğan S. Using the trans theoretic model to improve and change health behaviors. J Atatürk Univ School Nursing. 2007;10(2):86–94.
11. White JS, Toussaint S, Thrul J, Bontemps-Jones J, Abroms L, Westmaas JL. Peer mentoring and automated text messages for smoking quit: a randomized pilot trial. Nicotine Tobacco Res. 2020;22(3):371–380. doi:10.1093/ntr/ntz047
12. Cheung YTD, Chan CHH, Ho KS, et al. Protocol: effectiveness of nicotine replacement therapy sample at outdoor smoking hotspots for initiating quit attempts and use of smoking quit services: a protocol for a cluster randomized controlled trial. BMJ Open. 2020;10(4):e036339. doi:10.1136/bmjopen-2019-036339
13. Garrison KA, Pal P, O’Malley SS, et al. Craving to quit: a randomized controlled trial of smartphone app–based mindfulness training for smoking quit. Nicotine Tobacco Res. 2020;22(3):324–331. doi:10.1093/ntr/nty126
14. Bendtsen M. Heterogeneous treatment effects of a text messaging smoking quit intervention among university students. PLoS One. 2020;15(3):e0229637. doi:10.1371/journal.pone.0229637
15. TC. Ministry of Health. Turkey Global Adult Tobacco Survey 2012. Ministry of Health Publications; 2014.
16. US Department of Health and Human Services. A Report of the Surgeon General; the Health Consequences of Smoking-50 Years of Progress. Atlanta: US Department of Health and Human Services; 2014.
17. Velicer W, DiClemente C, Rossi J, Prochachaska J. Relapse situation and self-efficacy; An integrative model. Addict Behav. 1990;15:283–311. doi:10.1016/0306-4603(90)90070E
18. Alvermann DE, Unrav NJ, Ruddell RB. Theoretical Models and Processes of Reading.
19. Plummer B, Velicer W, Redding C, et al. Stage of change, decisional balance, and temptations for smoking: measurement and validation in a large, school-based population of adolescents. Addict Behav. 2001;26:551–571. doi:10.1016/S0306-4603(00)00144-1
20. Prochaska J, Norcross JC. Systems of Psychotherapy; a Transtheoretical Analysis. Oxford University Press.; 2018.
21. Uysal M, Kadakal F, Karsidag C, Bayram N, Uysal O, Yilmaz V. Fagerstrom test for nicotine dependence: reliability in a Turkish sample and factor analysis. Tuberk Toraks. 2004;52:115–121.
22. Anatchkova M, Redding C, Rossi J. Development and validation of trans theoretical model measures for Bulgarian adolescent non-smokers. Subst Use Misuse. 2007;42:23–41. doi:10.1080/10826080601094140
23. Pallonen U, Prochaska J, Velicer W, Prokhorov A, Smith N. Stages of acquisition and quit for adolescent smoking: an empirical integration. Addict Behav. 1998a;23(3):303–324. doi:10.1016/S0306-4603(97)00074-9
24. Velicer W, DiClemente CC, Prochaska OJ, Brandenburg N. Decisional balance measure for assessing and predicting smoking status. J Pers Soc Psychol. 1985;48(5):1279–1289. doi:10.1037/0022-3514.48.5.1279
25. Kleinjan M, Brug J, Van-den Eijnden RJ, Vermulst AA, Van Zundert RM, Engels RC. Associations between the transtheoretical processes of change, nicotine dependence, and adolescent smokers’ transition through the stages of change. Addiction. 2008;103:331–338. doi:10.1111/j.1360-0443.2007.02068.x
26. Martínez TJ, Peñuela EM. Prevalencia y factores asociados al consumo de cigarrillo tradicional, en adolescentes escolarizados; Prevalence of smoking among Colombian adolescents. Rev Med Chil. 2017;145(3):309–318. doi:10.4067/S0034-98872017000300004
27. Glynn G, Macfarlane A, Kelly M, Cantillon P, Murphy W. Helping each other to learn-a process evaluation of peer-assisted learning. BMC Med Educ. 2006;6(18):1–21
28. Bilgic N, Günay T. Evaluation of the effectiveness of peer education on smoking behavior among high school students. Saudi Med J. 2018;39(1):74–80. doi:10.15537/smj.2018.1.21774
29. Akkus D, Eker F, Karaca A, Kapısız Ö, Acıkgöz F. High School youth peer education program. An effective model to prevent substance abuse happen? J Psy Nurs. 2016;7:34–44. doi:10.5505/phd.2016.59489
30. Creamer M, Loukas A, Clendennen S, et al. Longitudinal predictors of cigarette use among students from 24 Texas colleges. J Am College Health. 2018;1–8. doi:10.1080/07448481.2018.1431907
31. Saglam L. Investigation of the results of smoking quit clinic and the factors associated with success. Turk J Med Sci. 2012;42(3):515–522. doi:10.3906/sag-1101-1452
32. Tarı SK, Avcı D, Mercan Y. Smoking addiction among university students and the willingness and self-efficacy to quit smoking. Clin Exp Health Sci. 2018;8:36–43. doi:10.5152/clinexphealthsci.2017.420
33. Yaslı G. Effectiveness of peer education program on smoking protection in youth. Turkey J Public Health. 2012;10(2):59–67. doi:10.20518/tjph.173065
34. VanZundert R, Ferguson S, Shiffman S, Engels R. Dynamic effects of self-efficacy on smoking lapses and relapse among adolescents. Health Psychol. 2010;29(3):246–254. doi:10.1037/a0018812
35. Alexandra H, Helena W. The HANS KAI Project: a community-based approach to improving health and well-being through peer support. Health Promot Chronic Dis Prev Can. 2018;38(3):135–146. doi:10.24095/hpcdp.38.3.04
36. Aveyard P, Sherratt E, Almond J, et al. The change-in-stage and updated smoking status results from a cluster-randomized trial of smoking prevention and quit using the transtheoretical model among British adolescents. Prev Med. 2001;33(4):313–324. doi:10.1006/pmed.2001.0889
37. Erol S, Balci A, Sisman F. Effect of transtheoretical model-based smoking quit program on high school students. J Nutr Health Sci. 2018;5(3):301.
38. Jarlstrup NS, Juel K, Pisinger CH, Grønbæk M, Holm S, Andersen S. International approaches to tobacco use quit programs and policy in adolescents and young adults: Denmark. Current Addiction Rep. 2018;5:42–53. doi:10.1007/s40429-018-0187-x
39. Resen HM. Impact of parents and peers smoking on tobacco consumption behavior of university students. Asian Pac J Cancer Prev. 2018;19(3):677–681. doi:10.22034/APJCP.2018.19.3.677
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.