Back to Journals » Drug Design, Development and Therapy » Volume 19
The Effect of Methylene Blue on Sublingual Microcirculation in Patients with Septic Shock: A Randomized Controlled Trial
Authors Dong C, Zhu J, Ni H, Chen Y, Chen B, Zhang M, Cui K, Zhang S, Jiang Y ![]() , Xu Y
, Xu Y
Received 18 August 2025
Accepted for publication 12 December 2025
Published 26 December 2025 Volume 2025:19 Pages 11629—11640
DOI https://doi.org/10.2147/DDDT.S561592
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Cuicui Dong,1,* Jiaqi Zhu,1,* Hang Ni,1,* Yanfang Chen,1 Benjia Chen,1 Mengqin Zhang,1 Ke Cui,1 Sheng Zhang,1 Yongpo Jiang,2 Yinghe Xu1
1Department of Critical Care Medicine, Taizhou Hospital of Zhejiang Province, Wenzhou Medical University, Taizhou, Zhejiang, People’s Republic of China; 2Department of Intelligent Medical Imaging, Sensing and Non-Invasive Rapid Testing, Zhejiang Engineering Research Center, Taizhou, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yinghe Xu, Department of Critical Care Medicine, Taizhou Hospital of Zhejiang Province, Wenzhou Medical University, No. 150, Ximen Street, Taizhou, 317000, People’s Republic of China, Email [email protected] Yongpo Jiang, Department of Intelligent Medical Imaging, Sensing and Non-invasive Rapid Testing, Zhejiang Engineering Research Center, No. 150, Ximen Street, Taizhou, 317000, People’s Republic of China, Email [email protected]
Background: Methylene blue (MB) has been proposed as an adjunctive therapy in the early management of septic shock; however, its effects on microcirculatory function remain poorly understood. This study aimed to investigate whether MB infusion improves sublingual microcirculatory parameters in patients with septic shock.
Methods: In this single-center, randomized controlled trial, participants were allocated in a 1:1 ratio to either the MB group or the control group. The MB group received an intravenous bolus of 2 mg/kg MB over 15 minutes, followed by a continuous infusion of 1 mg/kg MB diluted in 500 mL of 0.9% saline via a central venous catheter for 12 hours. The control group received an equivalent volume of saline. The primary endpoint was the change in sublingual microcirculation parameters from baseline to 24 hours, assessed using a repeated-measures mixed-effects model. Secondary endpoints included 28-day organ support-free days and 28-day mortality.
Results: Among the 72 randomized participants, 70.8% (n=51) were male, with a mean age of 68.6± 13.5 years. Following MB treatment, the mean microvascular flow index (MFI) in the MB group was 2.78, compared to 2.51 in the control group. MMRM analysis demonstrated that MB significantly improved MFI (least squares mean difference [95% CI]: 0.21 [0.09, 0.33], P=0.001), with significant increases observed as early as 1 hour post-intervention (T1: 0.24 [0.06, 0.42], P=0.009), and this effect persisted up to 24 hours (T24: P=0.005). However, no significant differences were observed between the groups in 28-day mortality (25.0% [9/36] vs 41.7% [15/36], P=0.200) or organ support-free days (20.0 [1.0– 22.0] vs 16.0 [1.3– 22.0], P=0.910).
Conclusions: Although MB improved sublingual microcirculatory parameters, these improvements did not translate into benefits in organ function or survival outcomes.
Trial Registration: chictr.org.cn ChiCTR 2400081549.
Keywords: septic shock, methylene blue, sublingual microcirculation, vasoactive agents, organ dysfunction, prognosis
Background
Septic shock is defined as sepsis in patients who require vasopressors to maintain a mean arterial pressure (MAP) ≥65 mmHg despite adequate fluid resuscitation and have a blood lactate level >2 mmol/L.1 As a major global public health challenge, septic shock contributes to millions of deaths annually, with a mortality rate as high as 20%-50%,2 and limited progress has been made in its treatment. Microcirculatory dysfunction is one of the core mechanisms underlying the development and progression of septic shock, serving as a key driver of the pathological process and directly impacting organ function.3 It is primarily characterized by loss of vascular tone, fluid extravasation, and increased capillary permeability.4 Studies have shown that persistent microcirculatory impairment for more than 24 hours is an independent risk factor for predicting patient outcomes.5 Therefore, interventions targeting microcirculatory function not only hold promise as a central clinical strategy but also provide a critical therapeutic target for improving patient prognosis.
In septic shock, the significant activation of inducible nitric oxide synthase (iNOS) leads to excessive release of nitric oxide (NO), while inflammatory mediators impair endothelial function, triggering progressive relaxation of arteriolar smooth muscle and ultimately resulting in loss of vascular tone,6 characterized by refractory hypotension. For the management of shock, guidelines emphasize early fluid resuscitation as the cornerstone, combined with vasopressors to improve organ perfusion.7 However, patient responses to fluid resuscitation are often limited,8 making it difficult to effectively counteract vasoplegia, and the use of high-dose vasopressors may increase the risk of adverse effects.9 Therefore, the early adoption of a multimodal therapeutic strategy combining different vasopressors and optimizing endothelial reactivity has become an important direction in current clinical practice.10,11
Traditionally, methylene blue has been utilized as a salvage therapy in the late stages of septic shock, yet its efficacy remains limited, with only 50% of patients exhibiting a positive response.12 Its mechanism of action primarily targets inducible nitric oxide synthase (iNOS) and soluble guanylate cyclase (sGC). Studies have demonstrated that iNOS and sGC expression and activity peak during the early phase of sepsis, such as within 24 hours post-cecal ligation and puncture (CLP).13,14 Administration of methylene blue during this critical window effectively inhibits iNOS, reduces nitric oxide (NO) production, and ameliorates pathological vasodilation. Consequently, early use of methylene blue may serve as a viable second-line option in combination therapy. As a non-catecholamine vasopressor, methylene blue selectively inhibits iNOS and guanylate cyclase (GC) within vascular smooth muscle, thereby attenuating NO-dependent vasodilation.15 Additionally, it mitigates oxygen free radical damage and the release of inflammatory factors, thereby preserving the structural integrity of the microvascular endothelium and microcirculatory function.16 Clinical studies have demonstrated that methylene blue significantly improves sublingual microcirculatory function in patients with refractory shock following cardiac surgery, alleviates abnormal vasoconstriction, reduces the dosage of norepinephrine required, and effectively corrects hemodynamic decoupling.17 In animal experiments, methylene blue increased capillary density in the terminal ileum of septic shock rats, thereby enhancing tissue perfusion.18 Furthermore, early adjunctive use of methylene blue in septic shock patients reduces the requirement for vasopressors without significant adverse effects.19 Some case reports also indicate that continuous intravenous infusion of methylene blue can markedly improve hemodynamic status.20,21
Although existing evidence supports the therapeutic potential of methylene blue in septic shock, its clinical application remains controversial, particularly due to the lack of relevant clinical studies on its direct impact on the microcirculation of septic shock patients.In recent years, advancements in Sidestream Dark Field (SDF) imaging technology have provided a novel perspective for non-invasive bedside monitoring of sublingual microcirculation.22 The parameters derived from this technique can quantitatively reflect the perfusion status and hypoxia level of intestinal mucosal microcirculation in septic patients,23 supporting the use of sublingual microcirculation as a “bedside window” for microcirculatory dysfunction in sepsis, with significant clinical translational value.Therefore, We hypothesized that methylene blue could improve sublingual microcirculation and correct hemodynamic decoupling. To test this hypothesis, we designed a randomized controlled clinical trial to assess the microcirculatory status of patients with septic shock using handheld vital microscopes (HVMs) and to investigate the effects of methylene blue on their microcirculatory function.
Methods
Study Design and Setting
This study is a single-center, prospective, randomized controlled trial. Consecutive patients admitted to three adult intensive care units (ICUs) at Taizhou Enze Medical Center for septic shock between March 15, 2024, and November 27, 2024, were enrolled, with the final follow-up conducted on December 25, 2024. The study was approved by the Ethics Committee of Taizhou Hospital in Zhejiang Province (approval number: K23230850) and strictly adhered to the ethical standards of the 1964 Declaration of Helsinki and its subsequent amendments. The trial was registered at the Chinese Clinical Trial Registry on March 5, 2024 (Registration No.: ChiCTR 2400081549). Informed consent was obtained from the family members of all patients, given that all enrolled cases received tracheal intubation and thus lacked the capacity for civil conduct, rendering them unable to provide informed consent independently.
Patients
Inclusion Criteria
- Age ≥18 years;
- Meeting the diagnostic criteria for septic shock according to Sepsis-3: high suspicion or confirmed infection, requiring vasopressors to maintain a mean arterial pressure (MAP) ≥65 mmHg despite adequate fluid resuscitation, and a blood lactate concentration >2 mmol/L;
- Endotracheal intubation.
Exclusion Criteria
- Pregnant or lactating women;
- Recent use (within 4 weeks) of selective serotonin reuptake inhibitors;
- Allergy to methylene blue (phenothiazines or food dyes);
- Glucose-6-phosphate dehydrogenase deficiency;
- Factors severely interfering with sublingual microcirculation imaging (eg, maxillofacial surgery or mucosal bleeding injuries);
- Other types of shock.
Study Protocol
Following the provision of informed consent, patients were randomized in a 1:1 ratio to either the Methylene Blue (MB) group or the control group. Simple randomization was employed, with random numbers generated using SPSS statistical software version 27.0 (IBM Corp, Armonk, NY). The randomization procedure was executed by an independent statistician, and the results were sealed in envelopes. A researcher not involved in other aspects of the trial assigned interventions based on the randomization codes contained in the envelopes, according to the order of patient enrollment. Both patients and researchers remained blinded throughout the study period.Patients in the MB group received an intravenous bolus of 2 mg/kg methylene blue administered over 15 minutes, followed by a maintenance infusion of 1 mg/kg methylene blue diluted in 500 mL of 0.9% sodium chloride solution,24 delivered via a dedicated central venous catheter over 12 hours. Patients in the control group received an equivalent volume of 500 mL of 0.9% sodium chloride solution infused over the same 12-hour period.Under the supervision of the attending physician, the doses of vasoactive agents, including norepinephrine, epinephrine, and dopamine, were gradually reduced, ensuring that the mean arterial pressure (MAP) was maintained within the range of 70–90 mmHg.
Sublingual Microcirculatory Measurement Andanalysis
Sublingual microcirculation networks were visualized using a sidestream dark field (SDF) imaging device (Model V100, Guangzhou, China) at a 5× magnification. This technology relies on the absorption characteristics of hemoglobin at 530 nm, where freely flowing red blood cells appear as black moving objects against a gray background in superficial vessels during imaging. Specifically, image sequences were recorded from three different regions on each side of the sublingual frenulum, with each sequence lasting between 5 and 20 seconds. At each key time point (ie, baseline and 1 hour, 6 hours, 12 hours, and 24 hours after methylene blue injection), up to three segments were selected and assigned random identifiers. According to the Massey evaluation method,25 image quality is assessed across six dimensions: illumination, duration, focus, content, stability, and pressure. Each dimension is scored on a scale of 0 (optimal), 1 (suboptimal but acceptable), or 10 (unacceptable). Videos with a total score exceeding 10 are deemed unqualified and excluded from further analysis. All images were assessed and analyzed by independent researchers who remained blinded to patient information.
According to the published expert consensus,26 the parameters of interest included the microvascular flow index (MFI), total vessel density (TVD), perfused vessel density (PVD), and heterogeneity index (HI). Specifically, MFI was calculated by dividing the image into nine quadrants, assigning a score to each quadrant (no flow = 0, intermittent flow = 1, sluggish flow = 2, and normal flow = 3), and then averaging the scores. TVD was defined as the total length of small vessels (diameter <20 μm) divided by the image area. PVD was calculated as the length of perfused vessels divided by the image area. The proportion of perfused vessels (PPV) was defined as the length of perfused vessels divided by the total vessel length within the image. HI was derived by dividing the difference between the highest and lowest MFI by the mean MFI.
The study recorded information encompassing demographics, duration of mechanical ventilation, and laboratory data. Sublingual microcirculation changes were monitored at baseline and at 1 hour, 6 hours, 12 hours, and 24 hours post-intervention, while mean arterial pressure was continuously monitored over the 24-hour period. The use of vasopressors was also documented. Additionally, clinical efficacy of methylene blue was assessed by evaluating ICU length of stay, the number of days free from organ support within 28 days, the degree of organ dysfunction, and 28-day and 90-day mortality. During the study, particular attention was paid to changes in serum creatinine, bilirubin, aspartate/alanine aminotransferase, PaO2/FIO2 ratio, and methemoglobin levels following the intervention.
Sample Size
Due to the absence of relevant data in existing literature, a formal sample size calculation could not be performed. We therefore pragmatically determined a sample size of 36 patients per group for this study.
Statistical Analysis
Data analysis was performed using IBM SPSS software version 27.0. The normality of continuous variables was assessed using the Shapiro–Wilk test. Normally distributed variables were expressed as mean ± standard deviation, and comparisons between groups were conducted using independent samples t-tests. Non-normally distributed variables were expressed as median (interquartile range), and group comparisons were performed using the Mann–Whitney U-test. Categorical variables were presented as frequencies and percentages, and group comparisons were made using the χ2-test or Fisher’s exact test. A mixed-model repeated measures (MMRM) analysis was employed to evaluate group differences in sublingual microcirculation parameters from baseline to 24 hours, with the model constructed based on the restricted maximum likelihood (REML) method. Results were presented as adjusted least-squares means. Survival rates were estimated using the Kaplan-Meier method, and differences between groups were compared using the Log rank test. Considering death as a competing risk event, the Fine-Gray test was used to analyze the discontinuation of vasopressors. Subgroup analysis was conducted using the Cox proportional hazards model to assess the efficacy of methylene blue in different subgroups. A significance level of p < 0.05 was set for all tests.
Results
Participant Characteristics
Between March 15, 2024, and November 27, 2024, 284 patients were screened, and 72 met the inclusion criteria and were randomized (Figure 1). Males accounted for 70.8% (n = 51), with a mean age of 68.6 ± 13.5 years. Baseline characteristics, including sex, age, infection sources, and comorbidities, were similar between the groups (Table 1). At baseline, there were no statistically significant differences between the two groups in microcirculation parameters, organ function indices, disease severity scores, metabolic indicators, or mean arterial pressure. Additionally, no significant differences were observed between the groups in the cumulative fluid volume within 24 hours after enrollment (4117.3 ± 1820.4 vs 4210.6 ± 1749.1, P = 0.825) or the use of colloid solutions (31.0 [86.1%] vs 27.0 [75%], P = 0.372).
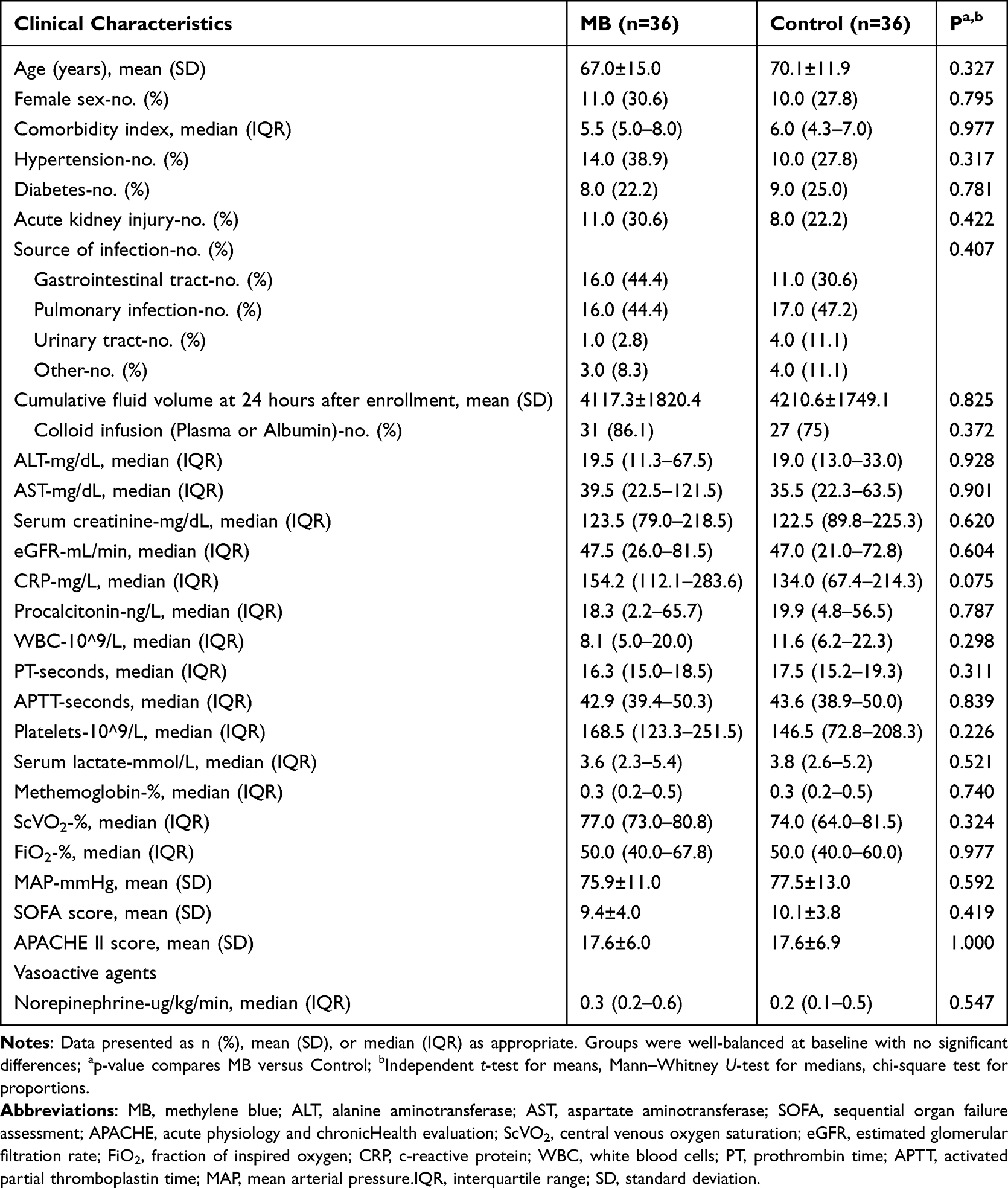 |
Table 1 Patients and Clinical Characteristics |
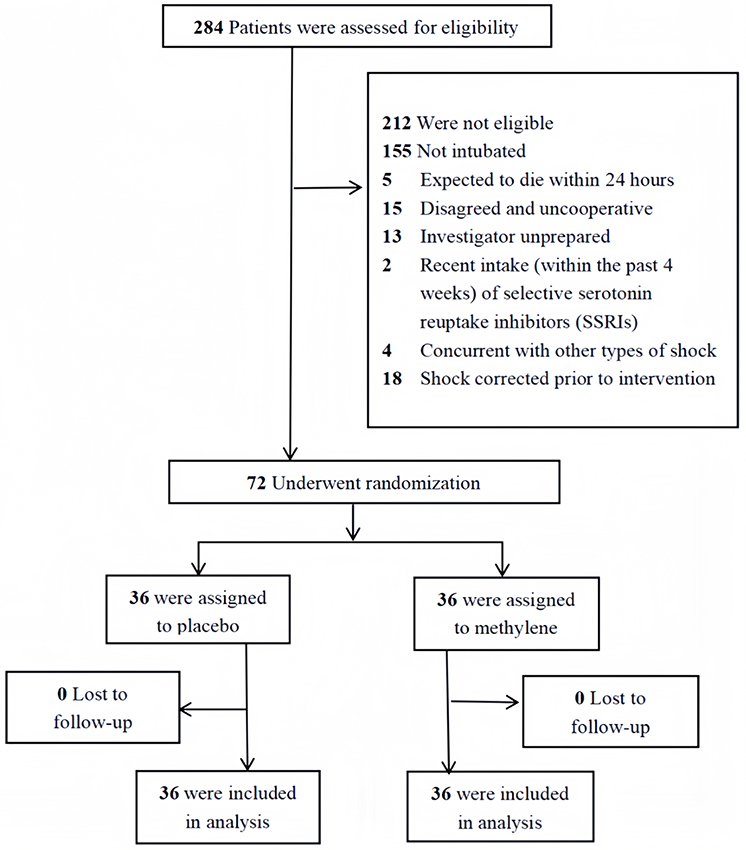 |
Figure 1 Flowchart of participants. Between March 15, 2024, and November 27, 2024, a total of 284 patients were screened, of whom 72 met the inclusion criteria and were randomized in a 1:1 ratio to the MB group (n=36) or the control group (n=36). The protocol completion rate was 100% in both groups. All 72 randomized patients completed the per-protocol analysis. |
Macrocirculation and Microcirculation
Following methylene blue treatment, the microvascular flow index (MFI) significantly improved (LSMD [95% CI]: 0.21 [0.09, 0.33], P = 0.001). At 1 hour post-intervention, MFI was already significantly higher in the treatment group compared to the control group (T1: LSMD [95% CI]: 0.24 [0.06, 0.42], P = 0.009), and this improvement trend persisted at 6 hours, 12 hours, and 24 hours post-intervention (Figure 2A). Additionally, other microcirculation parameters showed significant enhancements, including total vessel density (TVD) (LSMD [95% CI]: 3.04 [1.12, 4.96], P = 0.002), perfused vessel density (PVD) (LSMD [95% CI]: 1.87 [1.87, 6.46], P = 0.001), while the heterogeneity index (HI) was significantly reduced (LSMD [95% CI]: −0.185 [−0.30, −0.07], P = 0.003) (Figure 2B–D). Hemodynamically, mean arterial pressure (MAP) and norepinephrine (NE) dosage were continuously monitored for 24 hours before and after methylene blue administration, and the use of vasopressors within 28 days was recorded. Results showed no statistically significant differences in MAP (LSMD [95% CI]: −1.16 [−4.90, 2.58], P = 0.539) or NE dosage (LSMD [95% CI]: 0.02 [−0.18, 0.21], P = 0.890) between the methylene blue group and the control group (Supplementary Figure 1A and B). Notably, compared to baseline, the methylene blue group showed a significant reduction in NE dosage at 24 hours post-infusion (T24: LSMD [95% CI]: 0.17 [0.01, 0.34], P = 0.035). Furthermore, using death as a competing risk, Fine-Gray model analysis revealed no significant difference in the discontinuation rate of vasopressors between the two groups (HR = 0.93, [95% CI: 0.52 to 1.67]; P = 0.815) (Supplementary Figure 2).
 |
Figure 2 Changes in sublingual microcirculation indices in two groups over 24 hours. (A) Microvascular Flow Index (MFI): A significant difference in MFI was observed between the MB group and the control group (P=0.001). At 1 hour, 6 hours, 12 hours, and 24 hours, the MB group exhibited significantly higher MFI values compared to the control group (marked as **, *, **, **, respectively).(B) Heterogeneity Index (HI): There was a significant difference in HI between the MB group and the control group (P=0.003). At 12 hours, the MB group showed significantly lower HI values than the control group (marked as *). (C) Perfused Capillary Density (PCD): A significant difference in PCD was found between the MB group and the control group (P=0.001). At 1 hour, 6 hours, 12 hours, and 24 hours, the MB group demonstrated significantly higher PCD values compared to the control group (marked as *, **, **, ****, respectively). (D) Total Vessel Density (TVD): There was a significant difference in TVD between the MB group and the control group (P=0.003). At 6 hours, 12 hours, and 24 hours, the MB group displayed significantly higher TVD values than the control group (marked as **, *, ***, respectively).Inter-group P-values were derived from mixed linear models, and multiple comparisons at each time point were performed using Tukey’s method, with significance levels marked as follows: *p < 0.05; **p < 0.01; ***p < 0.001; ****p < 0.0001. |
Disease Severity and Clinical Outcomes
There were no statistically significant differences between the methylene blue (MB) group and the control group in Sequential Organ Failure Assessment (SOFA) scores (LSMD [95% CI]: 0.28 [−1.49, 2.06], P = 0.751) or Acute Physiology and Chronic Health Evaluation (APACHE) II scores (LSMD [95% CI]: 0.35 [−2.20, 2.89], P = 0.787) (Supplementary Figure 3A and B). Additionally, no significant differences were observed between the groups in the number of days free from organ support within 28 days (20.0 [1.0–22.0] vs 16.0 [1.3–22.0], P = 0.910) or in 28-day mortality rates (25.0% vs 41.7%, P = 0.200). Regarding hospital stay duration, neither ICU length of stay (P = 0.116) nor total hospital stay (21.0 [9.0–28.8] vs 13.0 [5.3–23.5], P = 0.520) showed significant differences between the groups (Table 2).
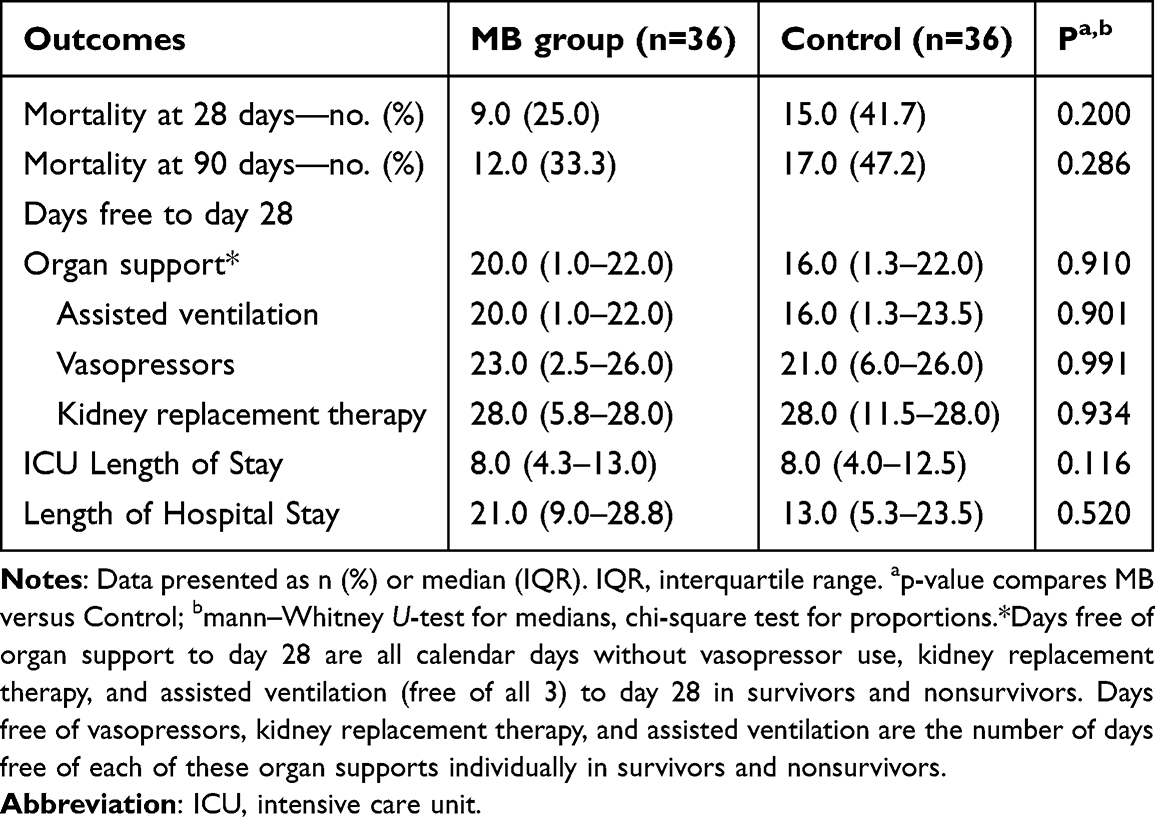 |
Table 2 Clinical Outcomes of Patients with Septic Shock After MB Treatment |
Subgroup Analysis
Subgroup analyses revealed that the study intervention did not significantly impact survival rates across different age groups (≥70 years: HR = 0.94, P = 0.925; <70 years: HR = 0.38, P = 0.106) or genders (female: HR = 0.72, P = 0.673; male: HR = 0.55, P = 0.232). When stratified by disease severity, no statistically significant differences in survival rates were observed between the intervention and control groups among patients with a Sequential Organ Failure Assessment (SOFA) score ≥8 (HR = 0.56, P = 0.366), an Acute Physiology and Chronic Health Evaluation (APACHE) II score ≥17 (HR = 0.21, P = 0.165), or a microvascular flow index (MFI) value ≥2.3 (HR = 0.34, P = 0.101). Even in patients requiring higher doses of vasopressors (norepinephrine ≥0.4 µg/kg/min), the intervention group did not demonstrate a significant survival advantage (P = 0.457) (Figure 3).
 |
Figure 3 Subgroup Analysis of Hazard Ratios (HRs) for Outcome Based on Various Clinical Variables. Overall: The overall HR is 0.59 (95% CI: 0.26 to 1.35), with a P-value of 0.209, indicating no significant difference in the outcome across all participants (n=72). Abbreviations: HR, hazard ratio; CI, confidence interval. |
Adverse Effects
The most frequently observed adverse reaction was the discoloration of urine to green or blue, which was noted in all 36 patients treated with methylene blue. Another monitored adverse event was the proportion of methemoglobin, which showed no statistically significant difference between the two groups following methylene blue infusion (LSMD [95% CI]: −0.02 [−0.01, 0.07], P = 0.718) (Supplementary Figure 5A). Other potential adverse effects, including changes in the PaO2/FiO2 ratio, serum creatinine, total bilirubin, and liver transaminase levels, also demonstrated no statistically significant differences between the groups post-intervention (Supplementary Figure 4A–G and Supplementary Figure 5B).
Discussion
This single-center randomized controlled trial evaluated the effects of methylene blue (MB) on microcirculation in patients with septic shock. The results demonstrated that a regimen consisting of a 2 mg/kg loading dose followed by a maintenance dose of 1 mg/kg (diluted in 500 mL of normal saline) administered every 12 hours rapidly (within 1 hour) and sustainably (up to 24 hours) optimized microcirculatory parameters, such as the microvascular flow index (MFI), and improved the decoupling between microcirculation and macrocirculatory hemodynamics, with no significant adverse effects observed. However, despite the marked improvement in microcirculation, MB did not significantly ameliorate organ dysfunction or 28-day mortality in these patients.
Microcirculatory dysfunction is one of the core pathological mechanisms underlying septic shock. Current guidelines primarily focus on fluid resuscitation and vasoactive agents to stabilize hemodynamics and improve tissue perfusion. However, microcirculatory failure can occur partially independent of macrocirculatory parameters.27 Furthermore, persistent deterioration of microcirculation is closely associated with organ failure and mortality in patients.5 Therefore, monitoring and targeted improvement of microcirculation are of critical importance. Animal studies have demonstrated that methylene blue significantly reduces leukocyte adhesion and increases functional capillary density,18 which aligns with the direct observation of improved sublingual microcirculation using handheld vital microscopes (HVMs) in this study. Additionally, research has shown that methylene blue protects the integrity of microvascular endothelial cells by mitigating the damaging effects of oxygen free radicals and inhibiting the release of inflammatory factors, thereby reducing inflammation-induced microcirculatory disruption.16 Thus, the core mechanisms by which methylene blue improves microcirculation include inhibiting leukocyte adhesion, maintaining capillary integrity, and attenuating inflammatory responses. These synergistic effects restore microvascular function and enhance tissue perfusion efficiency.
Although methylene blue significantly improved microcirculation in this study, its impact on clinical outcomes did not meet expectations, consistent with the findings of several previous studies.19,28–30 The failure of microcirculatory improvement to translate into clinical benefits may primarily be attributed to the complex pathophysiological mechanisms of septic shock, which involve multiple factors such as inflammatory responses, endothelial injury, and coagulation abnormalities.31 In this study, methylene blue was administered in conjunction with supportive therapies, including fluid resuscitation and vasoactive agents, primarily relying on its ability to reduce nitrogen compounds to enhance microcirculation and tissue perfusion. However, a single intervention may be insufficient to comprehensively reverse the course of septic shock.
Secondly, if intervention occurs after organ damage has entered an irreversible stage, such as apoptosis or necrosis,32 improvements in microcirculation may fail to translate into clinical benefits. This is particularly relevant in septic shock patients, where mitochondrial dysfunction leads to reduced oxygen utilization. Even if microcirculatory improvements enhance tissue oxygen delivery, cellular energy metabolism may remain compromised, thereby affecting organ function and survival outcomes.33 In this study, most patients received methylene blue treatment within 24 hours of septic shock diagnosis, aligning with the intervention timing in previous studies. For example, in a randomized controlled trial,29 patients diagnosed with septic shock within 24 hours were treated with methylene blue, yet no statistically significant difference in 28-day survival was observed between the treatment and control groups (P=0.650). Thus, the potential benefits of methylene blue on organ function may be influenced by multiple factors, including the complex pathophysiology of the disease, the therapeutic time window, and the limitations of monotherapy.
In this study, methylene blue did not significantly improve mean arterial pressure (MAP) or reduce the use of vasoactive agents, which may be attributed to the following reasons: First, the timing of intervention could influence its efficacy. The trial administered methylene blue within 24 hours of septic shock diagnosis, whereas studies suggest that its optimal effect is achieved when administered within 8 hours of onset, significantly improving vascular tone and hemodynamics.34 Second, the intensity of vasoactive agent use may impact the effectiveness of methylene blue. Multiple studies have shown that methylene blue exhibits significant efficacy when used in combination with multiple vasoactive agents.30,35 Third, the duration of methylene blue’s action may affect its therapeutic outcomes. For instance, in a case of refractory shock, a bolus of 1.5 mg/kg methylene blue administered over 15 minutes, followed by a continuous infusion of 0.25 mg/(kg·h) for 44 hours, successfully maintained hemodynamic stability without adverse effects.21 In the study by Weingartner et al,36 a 4 mg/kg injection of methylene blue significantly increased mixed venous oxygen saturation within 60 minutes and urine output within 20 minutes. Although the combined use of methylene blue may reduce the duration and dosage of vasoactive agents, it has not demonstrated significant benefits for patient prognosis. As a potential second-line treatment option, its role requires further validation through high-quality studies.37,38
Sublingual microcirculation monitoring has become a commonly used “bedside window” for assessing microcirculation in critically ill patients due to its convenience, non-invasiveness, and reproducibility. However, its “systemic representativeness” remains controversial. Studies have shown that sublingual microcirculation exhibits a quantitative correlation with intestinal mucosal microcirculation and can reflect the perfusion status of the intestinal mucosa.23 Nevertheless, patients with abdominal sepsis often demonstrate a “sublingual-intestinal microcirculatory dissociation” postoperatively, where sublingual microcirculation improves while intestinal microcirculation deteriorates. This dissociation is closely associated with intra-abdominal hypertension and preoperative ischemia, highlighting the limitations of this technique.39 Additionally, sublingual monitoring is susceptible to interference from oral secretions, probe pressure, and other local factors, necessitating comprehensive interpretation in conjunction with organ function markers such as lactate and creatinine. Current consensus suggests that sublingual monitoring can serve as a “bedside screening tool” for preliminary assessment of microcirculatory dysfunction but cannot replace organ-specific monitoring methods such as cerebral oxygen saturation and gastrointestinal pH. Multisite evaluation is required to enhance the accuracy of systemic microcirculatory assessment.26 Future research should explore the integration of sublingual monitoring with multimodal hemodynamic monitoring (eg, near-infrared spectroscopy, Doppler ultrasound) or combined therapeutic strategies to optimize microcirculatory status more comprehensively, thereby providing precise individualized treatment for critically ill patients such as those with septic shock.However, the study has certain limitations: First, the sample size was small and the design was single-center, limiting the diversity of the patient population. Second, the dosing regimen of methylene blue (2 mg/kg intravenous bolus followed by 1 mg/kg/12h maintenance) may require further optimization to enhance clinical efficacy, and the mechanism of action was not elucidated through the measurement of serum nitrate/nitrite levels. Additionally, while the cumulative fluid volume within 24 hours post-intervention was recorded, the impact of colloids such as albumin on microcirculation was not evaluated. Finally, although allocation concealment measures were implemented, the high incidence of urine discoloration caused by methylene blue may have exposed group assignments, potentially introducing bias in the adjustment of vasoactive agents by clinicians.
Conclusions
In summary, methylene blue has demonstrated significant efficacy in improving microcirculation in patients with septic shock and exhibits a high safety profile within appropriate dosing ranges, offering a new therapeutic option for clinical practice. Although its impact on short-term outcomes remains limited, these preliminary findings provide an important foundation for further exploration. Future research should focus on investigating the differential efficacy of methylene blue across various doses, timing of administration, and patient subgroups. Additionally, larger-scale, multicenter clinical trials are needed to further validate its potential clinical value, ultimately paving the way for more optimized treatment strategies for septic shock patients.
Abbreviations
APACHE, Acute physiology and chronic health evaluation; CRT, Capillary refill time; CI, Cardiac index; Dopa, Dopamine; ECMO, Extracorporeal membrane oxygenation; Epi, Epinephrine; ECPR, Extracorporeal cardiopulmonary resuscitation; GC, Guanylyl cyclase; HI, Heterogeneity index; HVMs, Handheld vital microscopes; ICU, Intensive care unit; iNOS, Inducible nitric oxide synthase; MAP, Mean arterial pressure; MB, Methylene blue; MFI, Microvascular flow index; NE, Norepinephrine; NO, Nitric oxide; PPV, Proportion of perfused vessels; PVD, Perfused vessel density; SSRIs, Selective serotonin reuptake inhibitors; SDF, Sidestream dark field; sGC, Soluble guanylate cyclase; SOFA, Sequential organ failure assessment; TVD, Total vessel density.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author (Yinghe Xu) on reasonable request.
Ethics Approval and Consent to Participate
The study was approved by the Ethics Committee of Taizhou Hospital, Zhejiang Province (Approval No.: K23230850) and conducted in accordance with the ethical standards of the 1964 Helsinki Declaration and its later revisions. Written informed consent was obtained from all participants involved in the study.
Acknowledgments
Grateful acknowledgment is extended to the nursing staff and medical professionals in the Intensive Care Unit (ICU) of Taizhou Hospital, Zhejiang Province, as well as the patients and their families for their invaluable contributions.
Funding
This work was supported by The Science and Technology Project of Taizhou (1801KY70、23ywa47), the Medicines Health Research Fund of Zhejiang, China (2024ky1784), the National Key Research and Development Program of Zhejiang Province (2023C03083), The Joint Fund of Zhejiang Provincial Natural Science Foundation of China under Grant No. LKLY25H200027.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Singer M, Deutschman CS, Seymour CW, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016;315(8):801–810. doi:10.1001/jama.2016.0287
2. Bauer M, Gerlach H, Vogelmann T, Preissing F, Stiefel J, Adam D. Mortality in sepsis and septic shock in Europe, North America and Australia between 2009 and 2019- results from a systematic review and meta-analysis. Crit Care. 2020;24(1):239. doi:10.1186/s13054-020-02950-2
3. Ince C. The microcirculation is the motor of sepsis. Crit Care. 2005;4(Suppl 4):S13–9. doi:10.1186/cc3753
4. Ince C, Mayeux PR, Nguyen T, et al. THE ENDOTHELIUM IN SEPSIS. Shock. 2016;45(3):259–270. doi:10.1097/SHK.0000000000000473
5. Sakr Y, Dubois MJ, De Backer D, Creteur J, Vincent JL. Persistent microcirculatory alterations are associated with organ failure and death in patients with septic shock. Crit Care Med. 2004;32(9):1825–1831. doi:10.1097/01.CCM.0000138558.16257.3F
6. Levy B, Collin S, Sennoun N, et al. Vascular hyporesponsiveness to vasopressors in septic shock: from bench to bedside. Intensive Care Med. 2010;36(12):2019–2029. doi:10.1007/s00134-010-2045-8
7. Evans L, Rhodes A, Alhazzani W, et al. Surviving Sepsis Campaign: international Guidelines for Management of Sepsis and Septic Shock 2021. Crit Care Med. 2021;49(11):e1063–e143. doi:10.1097/CCM.0000000000005337
8. Bentzer P, Griesdale DE, Boyd J, MacLean K, Sirounis D, Ayas NT. Will This Hemodynamically Unstable Patient Respond to a Bolus of Intravenous Fluids? JAMA. 2016;316(12):1298–1309. doi:10.1001/jama.2016.12310
9. Stolk RF, van der Pasch E, Naumann F, et al. Norepinephrine Dysregulates the Immune Response and Compromises Host Defense during Sepsis. Am J Respir Crit Care Med. 2020;202(6):830–842. doi:10.1164/rccm.202002-0339OC
10. Leone M, Einav S, Antonucci E, et al. Multimodal strategy to counteract vasodilation in septic shock. Anaesth Crit Care Pain Med. 2023;42(3):101193. doi:10.1016/j.accpm.2023.101193
11. Wieruszewski PM, Khanna AK. Early Multimodal Vasopressors-Are We Ready for It? Crit Care Med. 2022;50(4):705–708. doi:10.1097/CCM.0000000000005344
12. Porizka M, Kopecky P, Dvorakova H, et al. Methylene blue administration in patients with refractory distributive shock - a retrospective study. Sci Rep. 2020;10(1):1828. doi:10.1038/s41598-020-58828-4
13. Fernandes D, da Silva-Santos JE, Duma D, Villela CG, Barja-Fidalgo C, Assreuy J. Nitric oxide-dependent reduction in soluble guanylate cyclase functionality accounts for early lipopolysaccharide-induced changes in vascular reactivity. Mol Pharmacol. 2006;69(3):983–990. doi:10.1124/mol.105.015479
14. Evgenov OV, Sager G, Bjertnaes LJ. Methylene blue reduces lung fluid filtration during the early phase of endotoxemia in awake sheep. Crit Care Med. 2001;29(2):374–379. doi:10.1097/00003246-200102000-00028
15. Hosseinian L, Weiner M, Levin MA, Fischer GW. Methylene Blue: magic Bullet for Vasoplegia? Anesth Analg. 2016;122(1):194–201. doi:10.1213/ANE.0000000000001045
16. Tucker D, Lu Y, Zhang Q. From Mitochondrial Function to Neuroprotection-an Emerging Role for Methylene Blue. Mol Neurobiol. 2018;55(6):5137–5153. doi:10.1007/s12035-017-0712-2
17. Maurin C, Portran P, Schweizer R, et al. Effects of methylene blue on microcirculatory alterations following cardiac surgery: a prospective cohort study. Eur J Anaesthesiol. 2022;39(4):333–341. doi:10.1097/EJA.0000000000001611
18. Nantais J, Dumbarton TC, Farah N, et al. Impact of methylene blue in addition to norepinephrine on the intestinal microcirculation in experimental septic shock. Clin Hemorheol Microcirc. 2014;58(1):97–105. doi:10.3233/CH-141874
19. Ibarra-Estrada M, Kattan E, Aguilera-González P, et al. Early adjunctive methylene blue in patients with septic shock: a randomized controlled trial. Crit Care. 2023;27(1):110. doi:10.1186/s13054-023-04397-7
20. Jaiswal A, Kumar M, Silver E. Extended Continuous Infusion of Methylene Blue for Refractory Septic Shock. Indian J Crit Care Med. 2020;24(3):206–207. doi:10.5005/jp-journals-10071-23376
21. Brown G, Frankl D, Phang T. Continuous infusion of methylene blue for septic shock. Postgrad Med J. 1996;72(852):612–614. doi:10.1136/pgmj.72.852.612
22. Ocak I, Kara A, Ince C. Monitoring microcirculation. Best Pract Res Clin Anaesthesiol. 2016;30(4):407–418. doi:10.1016/j.bpa.2016.10.008
23. Verdant CL, De Backer D, Bruhn A, et al. Evaluation of sublingual and gut mucosal microcirculation in sepsis: a quantitative analysis. Crit Care Med. 2009;37(11):2875–2881. doi:10.1097/CCM.0b013e3181b029c1
24. Ibarra-Estrada M, Kattan E, Aguirre-Avalos G, Hernández G. Drug diluent and efficacy of methylene blue in septic shock: authors’ reply. Crit Care. 2023;27(1):345. doi:10.1186/s13054-023-04633-0
25. Massey MJ, Larochelle E, Najarro G, et al. The microcirculation image quality score: development and preliminary evaluation of a proposed approach to grading quality of image acquisition for bedside videomicroscopy. J Crit Care. 2013;28(6):913–917. doi:10.1016/j.jcrc.2013.06.015
26. Ince C, Boerma EC, Cecconi M, et al. Second consensus on the assessment of sublingual microcirculation in critically ill patients: results from a task force of the European Society of Intensive Care Medicine. Intensive Care Med. 2018;44(3):281–299. doi:10.1007/s00134-018-5070-7
27. Bakker J, Ince C. Monitoring coherence between the macro and microcirculation in septic shock. Curr Opin Crit Care. 2020;26(3):267–272. doi:10.1097/MCC.0000000000000729
28. Shaker EH, Soliman AM, Bedewy AAE, Elrawas MM. Comparative study between high and low dose methylene blue infusion in septic cancer patients: a randomized, blinded, controlled study. BMC Anesthesiol. 2025;25(1):15. doi:10.1186/s12871-024-02792-3
29. Kirov MY, Evgenov OV, Evgenov NV, et al. Infusion of methylene blue in human septic shock: a pilot, randomized, controlled study. Crit Care Med. 2001;29(10):1860–1867. doi:10.1097/00003246-200110000-00002
30. Park BK, Shim TS, Lim CM, et al. The effects of methylene blue on hemodynamic parameters and cytokine levels in refractory septic shock. Korean J Intern Med. 2005;20(2):123–128. doi:10.3904/kjim.2005.20.2.123
31. Angus DC, van der Poll T. Severe sepsis and septic shock. N Engl J Med. 2013;369(9):840–851. doi:10.1056/NEJMra1208623
32. Perl M, Chung CS, Ayala A. Apoptosis. Crit Care Med. 2005;33(12 Suppl):S526–9. doi:10.1097/01.CCM.0000185499.28006.4C
33. Singer M. The role of mitochondrial dysfunction in sepsis-induced multi-organ failure. Virulence. 2014;5(1):66–72. doi:10.4161/viru.26907
34. Puntillo F, Giglio M, Pasqualucci A, Brienza N, Paladini A, Varrassi G. Vasopressor-Sparing Action of Methylene Blue in Severe Sepsis and Shock: a Narrative Review. Adv Ther. 2020;37(9):3692–3706. doi:10.1007/s12325-020-01422-x
35. Andresen M, Dougnac A, Díaz O, et al. Use of methylene blue in patients with refractory septic shock: impact on hemodynamics and gas exchange. J Crit Care. 1998;13(4):164–168. doi:10.1016/S0883-9441(98)90001-6
36. Weingartner R, Oliveira E, Oliveira ES, et al. Blockade of the action of nitric oxide in human septic shock increases systemic vascular resistance and has detrimental effects on pulmonary function after a short infusion of methylene blue. Braz J Med Biol Res. 1999;32(12):1505–1513. doi:10.1590/S0100-879X1999001200009
37. Guinot PG, Martin A, Berthoud V, et al. Vasopressor-Sparing Strategies in Patients with Shock: a Scoping-Review and an Evidence-Based Strategy Proposition. J Clin Med. 2021;10(14):3164. doi:10.3390/jcm10143164
38. Jozwiak M. Alternatives to norepinephrine in septic shock: which agents and when? J Intensive Med. 2022;2(4):223–232. doi:10.1016/j.jointm.2022.05.001
39. Edul VS, Ince C, Navarro N, et al. Dissociation between sublingual and gut microcirculation in the response to a fluid challenge in postoperative patients with abdominal sepsis. Ann Intensive Care. 2014;4(1):39. doi:10.1186/s13613-014-0039-3
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.