Back to Journals » Patient Preference and Adherence » Volume 20
The Developmental Trajectory of Learned Helplessness in Breast Cancer Chemotherapy Patients: A Longitudinal Study Based on Latent Growth Models
Authors Li X, Guo Z ![]() , Jiao Y, Lu Y, Ding S, Li X, Yang R, Chen C
, Jiao Y, Lu Y, Ding S, Li X, Yang R, Chen C ![]()
Received 28 October 2025
Accepted for publication 14 February 2026
Published 25 February 2026 Volume 2026:20 577150
DOI https://doi.org/10.2147/PPA.S577150
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Xiaoxiao Li,1,2,* Zhongqiang Guo,2,* Yanyan Jiao,3,* Yifan Lu,2 Shuming Ding,1 Xiaohuan Li,1 Rui Yang,1 Chaoran Chen2
1School of Medicine, Zhengzhou University of Industrial Technology, Zhengzhou, Henan, People’s Republic of China; 2School of Nursing and Health, Henan University, Kaifeng, Henan, People’s Republic of China; 3Department of Breast Surgery, the Third Affiliated Hospital of Zhengzhou University, Zhengzhou, Henan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhongqiang Guo, School of Nursing and Health, Henan University, The Northern Section of Jinming Avenue, Kaifeng, People’s Republic of China, Email [email protected] Chaoran Chen, School of Nursing and Health, Henan University, The Northern Section of Jinming Avenue, Kaifeng, People’s Republic of China, Email [email protected]
Objective: This study aimed to examine the trajectory of learned helplessness in breast cancer chemotherapy patients using latent growth curve models. It also analyzed how chemotherapy regimen, age, education, and social support influence changes in helplessness.
Methods: From October 2024 to June 2025, a total of 206 breast cancer patients undergoing chemotherapy at two tertiary hospitals in Henan Province, China, were enrolled as study participants using the convenience sampling method. Participants were assessed at four time points: prior to chemotherapy and after the 2nd, 4th, and 6th cycles, using the Learned Helplessness Scale and the Social Support Rating Scale. Latent growth models were employed for analysis.
Results: Learned helplessness increased linearly among patients, with individuals starting at lower levels showing faster growth. Significant individual differences were found in both baseline levels and rates of change. Patients receiving anthracycline-based chemotherapy showed a faster rate of helplessness increase compared to those on non-anthracycline regimens, although there was no significant difference in their initial levels. Younger patients had higher initial helplessness levels than older patients, but age did not affect the rate of change. Lower educational levels were associated with higher initial helplessness, but education did not influence the rate of change. Higher social support significantly reduced helplessness.
Conclusion: Learned helplessness in breast cancer chemotherapy patients increases linearly with notable individual differences. These findings suggest that healthcare providers should develop targeted interventions based on patients’ trajectories and influencing factors to reduce helplessness.
Keywords: breast cancer, learned helplessness, trajectory, latent growth model
Introduction
Breast cancer is the most common malignant tumor among women worldwide.1 Data released by the American Cancer Society in 2024 shows that the incidence rate of breast cancer continues to rise, increasing by approximately 1% annually between 2012 and 2021.2 Although the mortality rate of breast cancer has decreased with advancements in early detection and treatment, it remains the second most common cause of cancer-related death in women.3 In the comprehensive treatment regimen for breast cancer, chemotherapy is one of the most important treatment methods.4 Chemotherapy can significantly reduce the risk of breast cancer recurrence and prolong patients’ survival. However, chemotherapy-related adverse reactions (such as hair loss, nausea, vomiting, etc.) are likely to induce negative psychological responses including anxiety, depression, and fear of treatment.5 In recent years, the phenomenon of learned helplessness exhibited by breast cancer patients during chemotherapy has attracted increasing attention.
Learned helplessness refers to a psychological state or behavior characterized by a sense of powerlessness or abandonment that an individual develops when experiencing trauma, setbacks, or adversity.6 Learned helplessness alters mental and physical functions in humans and animals, including stress hormone activity, sleep, pleasure, preferences for sweet foods, eating habits and body weight, activity, immune function, and thinking and attention.7,8 Breast cancer patients cope with not only the physical pain of the disease and its treatment, but also the emotional pain associated with how they feel about their body and their role in society. As breast cancer patients feel more and more helplessness about the illness, they may be developing learned helplessness.9 This negative mental state and behavior can make patients less likely to follow treatment plans and raise their risk of depression. It greatly reduces their quality of life and well-being, and it is also an important risk factor for cancer coming back.10 So, besides improving medical treatment, it is very important to care for patients’ psychological health and improve their long-term quality of life.
Existing studies mainly focus on the current situation and influencing factors of learned helplessness in breast cancer patients,11 or examine how these factors work.12 Although these cross-sectional studies provide useful basic data, they cannot fully show how this psychological state changes during treatment. In particular, there are very few long-term studies on how different chemotherapy treatments affect the development of helplessness. As a result, we still know very little about how different treatment plans influence changes in helplessness.
The relationship between age and learned helplessness remains controversial in demographic studies.For example, Li et al11 found that younger patients felt more helpless, but Ju et al13 showed that patients near age 50 were more likely to have mental adjustment problems. The effect of education on helplessness is mixed. For example, Liu W. et al14 in their study on community-dwelling patients with multiple chronic conditions, found that the higher the educational level of the patients, the lower their level of learned helplessness. Liu Y. et al15 did not find the effect of education on helplessness after mouth cancer surgery patients.At present, there is insufficient research on how age and education level affect the development rate of learned helplessness.This limitation hinders the accurate identification of high-risk groups at different developmental stages.
Social support16 refers to the varieties of emotional and instrumental support received from social relationships. Previous studies17 found that social support enhances mental strength and reduces or prevents learned helplessness. S. Dai et al18 studies also found that although the social support of patients is generally stable, they change under the influence of factors such as individual traits, marital status, family role burden, and family income. The change in social support has a great impact on the learned helplessness of breast cancer patients during chemotherapy. However, most previous studies have adopted a cross-sectional design, making it difficult to reveal the mechanism by which social support influences the changes in learned helplessness. For this reason, our study will treat social support as a factor that changes over time, to see how it affects the development of learned helplessness in breast cancer patients receiving chemotherapy.
In summary, this study aims to systematically explore the following issues through four rounds of tracking during the chemotherapy period, using latent growth curve models: (1) the trajectory characteristics of learned helplessness in breast cancer chemotherapy patients; (2) the effects of different chemotherapy regimens, age, and education level on the starting level and rate of change of the trajectory; and (3) the dynamic role of social support in the development of helplessness. The findings aim to provide both theoretical and empirical support for the development of personalized psychological intervention systems for breast cancer patients.
Materials and Methods
Participants
A convenience sampling method was used to select 206 breast cancer chemotherapy patients from two tertiary hospitals in Henan Province between October 2024 and June 2025. The criteria for inclusion were: (1) Histopathologically diagnosed primary breast cancer; (2) receiving chemotherapy for the first time, with a total of six cycles planned; (3) being female and aged 18 years or older; (4) providing informed consent; (5) being fully alert and able to complete the questionnaire independently. The criteria for exclusion were: (1) having other serious illnesses or other types of cancer; (2) having a history of cognitive or mental health disorders. A basic sample size calculation was performed, which considered a 20% rate of invalid responses, leading to the final number of 206 participants. All participants provided and signed informed consent forms to take part in the study voluntarily. The study’s methods and plan were approved by the ethics committee (Ethics ID: HUSOM2024-594) and followed all relevant guidelines and regulations.
Research Tools
General Information Survey Questionnaire
The content of the General Information Questionnaire includes age, educational attainment, and chemotherapy regimen.
Learned Helplessness Scale (LHS)
The Learned Helplessness Scale, developed by Chinese scholars Wu et al19 was used to measure learned helplessness. This scale consists of two dimensions: helplessness and hopelessness, with a total of 18 items.The Cronbach’s a coefficient for the overall scale was 0.930, with a split-half-reliability of 0.901 and a test-retest reliability of 0.898. All items wererated using a 5-point Likert scale (1 to 5), with higher scores indicatingmore severe learned helplessness.
Social Support Rating Scale (SSRS)
The Social SupportRating Scale, developed by Chinese scholar Xiao,20 was used toassess social support. The scale consists of 10 items, covering threedimensions: subjective social support, objective social support, and social66support utilization, The Cronbach’s a coefficient for this scale was 0.896. Higher scores on this scale indicate higher levels of social support.
Data Collection Method
In obtaining consent we followed the ethical rules explained above. We explained the study to the patients who satisfied the criteria for participation in the study. Questionnaire was not handed to them until they agreed to participate in the study. Data collection was performed at four times: Before the first chemotherapy (T1), second cycle of chemotherapy (T2), fourth cycle of chemotherapy (T3) and sixth cycle of chemotherapy (T4). Each questionnaire was completed within one week after the end of the chemotherapy cycle. It was provided 15–20 minutes to fill the questionnaire. Answers were checked immediately for any omitted or erroneous responses; listwise deletion was applied to address missing data, ensuring data integrity. At the beginning, 222 patients were questioned. At T2, 213 valid questionnaire were returned; at T3, 208 valid questionnaire were returned and at T4, 206 valid questionnaire were returned. And 16 patients dropped out in the study because they did not want to continue.
The results of the chi-square and t-tests showed no significant differences between the drop-out and continuing participants in terms of chemotherapy regimen (χ2(1) = 1.875, p > 0.05), age (χ2(2) = 1.826, p > 0.05), education level (χ2(2) = 5.015, p > 0.05), learned helplessness (t(220) = 1.4, p > 0.05), and social support (t(220) = −0.379, p > 0.05). These findings indicate that there was no systematic attrition, so the data from drop-out participants were excluded.
Data Analysis
We summarized learned helplessness scores as means and standard deviations. We employed correlation analysis to examine the association of learned helplessness and social support at each time point. We used latent growth modeling (LGM) to examine the change of learned helplessness over time in breast cancer patients chemotherapy.We evaluated the goodness of fit of the model to the data using standard fit indices:21,22 CFI, TLI, RMSEA, and SRMR. A goodness-of-fit model was considered acceptable when the CFI and TLI were greater than 0.95, the RMSEA was less than 0.08, and the SRMR was less than 0.08. We extend the LGM by adding two kinds of covariates that do not change over time (ie, chemotherapy regimen, age, education), and that can change over time (ie, social support). We used SPSS 25.0 for the basic statistics and correlation analysis, and Mplus 8.3 for the latent growth modeling. Model estimation was conducted using the robust maximum likelihood method (MLR). The LGM included an intercept and a slope. The average intercept shows the typical starting score, and its variance shows how much patients differed at the beginning. The average slope shows the overall trend of change, and its variance shows how much the rate of change differed from person to person.
Results
Descriptive Statistics
The means, standard deviations, and correlation matrix of learned helplessness and social support at each stage are presented in Table 1. Learned helplessness in breast cancer patients undergoing 43 chemotherapy showed an increasing trend. There was a significant negative correlation between learned helplessness and social support at all time points.
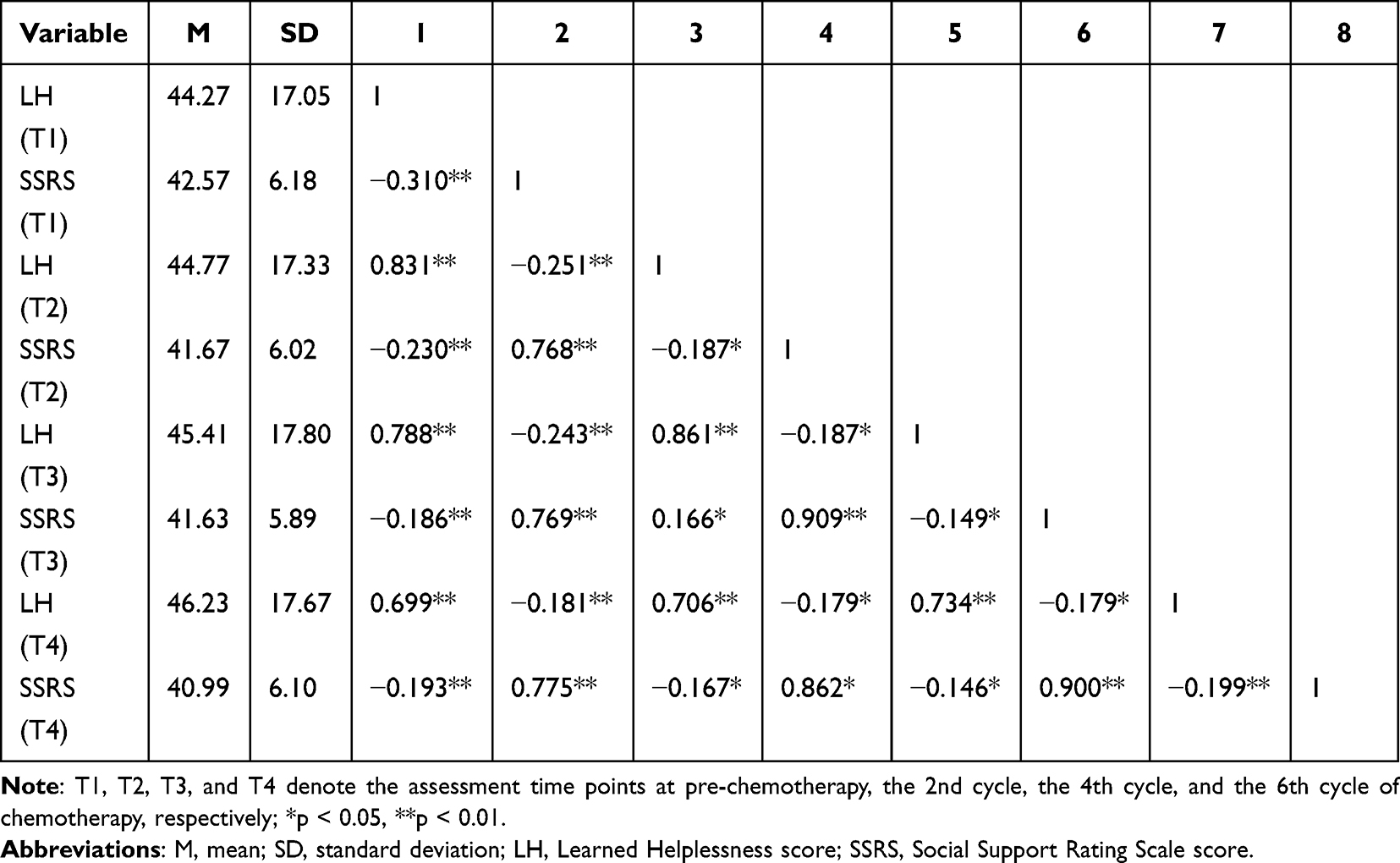 |
Table 1 Correlations, Means, and Standard Deviations Among Study Variables |
Trajectory of Learned Helplessness: Unconditional Model
To test whether the trajectory of learned helplessness in breast cancer chemotherapy patients is linear or nonlinear, we constructed both a linear unconditional model and a quadratic unconditional model, as shown in Table 2.The fit indices indicate that both models have non-significant χ2/df ratios, CFI and TLI values greater than 0.95, and RMSEA and SRMR values less than 0.08. We compared the AIC and BIC values and considered how clear and useful the model was for clinical research. We chose the linear unconditional model because it had smaller AIC and BIC values, is simpler, and easier to understand.
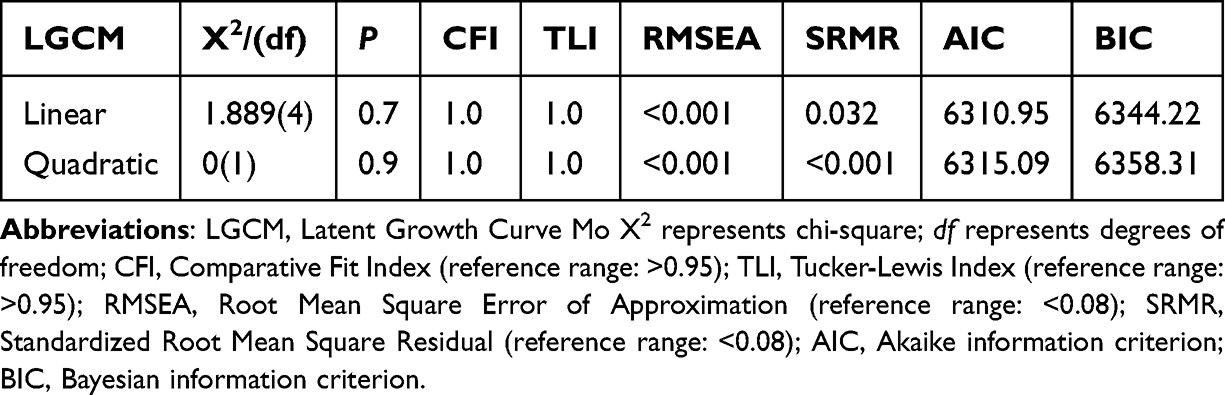 |
Table 2 Model Fit Indices for the Latent Growth Curve Models |
In this model, the average starting score for learned helplessness was 44.25 (P < 0.05), and the average rate of change per time point was 0.632 (P < 0.05). The relationship between the starting score and the rate of change was r = −0.398 (P < 0.05). This means that learned helplessness increased over time in a straight-line pattern (see Figure 1). Patients who started with lower helplessness scores showed a faster increase over time.
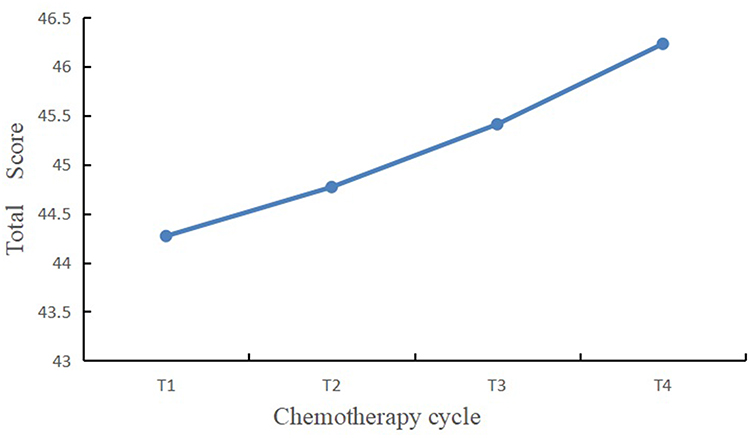 |
Figure 1 The Change Trajectory of Learned Helplessness in Breast Cancer Patients Undergoing Chemotherapy. Note: T1, T2, T3, and T4 represent the four time points respectively: before chemotherapy, and during the 2nd, 4th, and 6th chemotherapy courses. |
Also, both the variance of the starting score (σ2 = 267.36, P < 0.05) and the variance of the change rate (σ2 = 6.674, P < 0.05) were greater than zero. This shows that patients differed significantly from each other in both their initial level of learned helplessness and how quickly it changed over time.
Impact of Chemotherapy Regimen, Age, and Education Level on the Trajectory of Learned Helplessness
To examine the impact of chemotherapy regimen, age, and education level on the trajectory of learned helplessness, we added chemotherapy regimen (1 = anthracycline-based drugs, 2 = non-anthracycline-based drugs), age (1 = 18–45 years, 2 = 46–60 years, 3 = >60 years), and education level (1 = middle school or below, 2 = high school, 3 = college or above) as covariates in the linear unconditional model, creating a conditional model (see Figure 2).The results show that the conditional model fit the data well, with χ2(10) = 8.761, p = 0.55, CFI = 1.00, RMSEA = 0.00, and SRMR = 0.026. There was no major difference in learned helplessness at the start between patients on different chemotherapy types (γα1 = −2.957, p > 0.05). However, their helplessness increased at different speeds (γβ1 = 2.419, p < 0.01). Specifically, patients who received anthracycline-based chemotherapy saw their helplessness rise faster than those on other types of chemotherapy. There was a significant difference in the initial levels of learned helplessness between patients of different ages (γα2 = −5.324, p < 0.01), with younger patients showing higher initial levels of helplessness compared to older patients. However, there was no significant age-related difference in the rate of change (γβ2 = 0.112, p > 0.05). There was a significant difference in the initial levels of learned helplessness between patients with different education levels (γα3 = −4.729, p < 0.01), with patients of lower educational levels showing higher initial levels of helplessness. However, there was no significant difference in the rate of change based on education level (γβ3 = 0.125, p > 0.05).
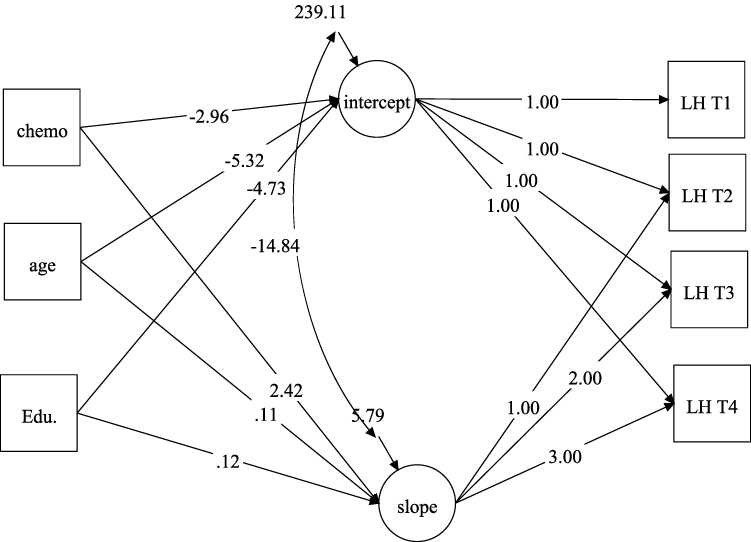 |
Figure 2 Influences of Chemotherapy Regimen, Age, and Education on Learned Helplessness Trajectories. Note: “Chemo” represents the chemotherapy method, “age” represents age, “Edu.” represents the level of education, “LH” represents the level of Learned Helplessness, and T1, T2, T3, and T4 represent four time points respectively: before chemotherapy, during the 2nd chemotherapy course, during the 4th chemotherapy course, and during the 6th chemotherapy course. |
Impact of Social Support on the Trajectory of Learned Helplessness
To examine the impact of social support on the trajectory of learned helplessness in breast cancer chemotherapy patients, we included social support as a time-varying covariate, and chemotherapy regimen, age, and education level as time-invariant covariates in the conditional model (see Figure 3). The results indicate that the conditional model provided an acceptable fit to the data, with χ2(22) = 42.09, p = 0.006, CFI = 0.972, RMSEA = 0.067, and SRMR = 0.054. At each time point, higher social support levels were associated with lower levels of learned helplessness: prior to chemotherapy (β = −0.390, t = −3.450, p < 0.001), after the second chemotherapy cycle (β = −0.354, t = −3.650, p < 0.001), after the fourth cycle (β = −0.311, t = −2.976, p < 0.01), and after the sixth cycle (β = −0.273, t = −2.023, p < 0.05). This shows that social support helps reduce learned helplessness. However, the explained variance for the intercept (R2 = 0.110, p < 0.05) and the slope (R2 = 0.195, p > 0.05) suggest that social support accounts for only a limited amount of the variation.
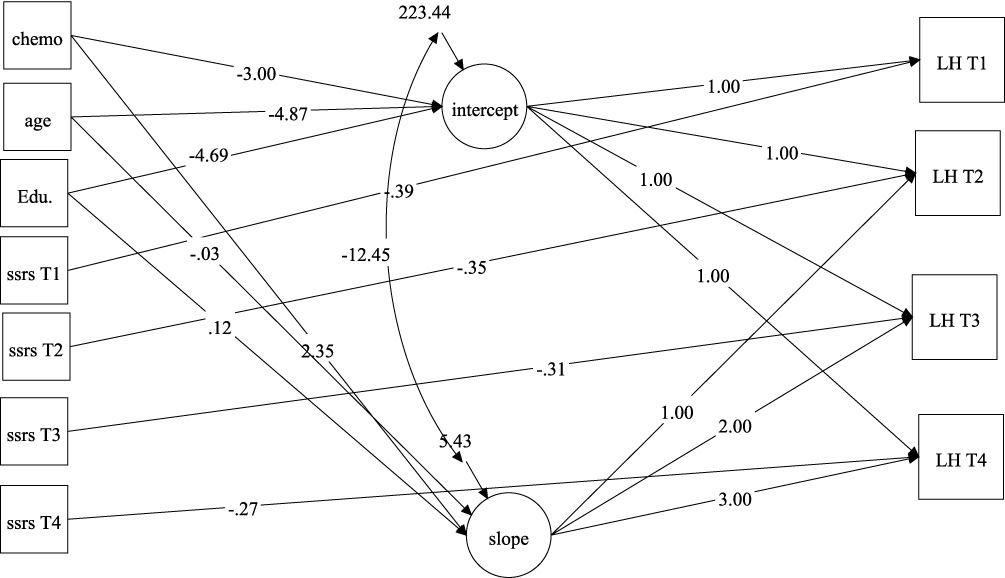 |
Figure 3 The Influence of Social Support on the Trajectory of Learned Helplessness. Note: “Chemo” represents the chemotherapy method, “age” represents age, “Edu.” represents the level of education, “LH” represents the level of Learned Helplessness, “SSRS” represents the level of Social Support Rating Scale, and T1, T2, T3, and T4 represent the four time points respectively: before chemotherapy, and during the 2nd, 4th, and 6th chemotherapy courses. |
Discussion
Trajectory of Learned Helplessness in Breast Cancer Chemotherapy Patients
This study used latent growth models to examine how learned helplessness changes over time in breast cancer patients receiving chemotherapy. The results indicated that the rate of increase of learned helplessness was straight line. Patients with learned helplessness scores at baseline of lower values showed a faster rate of increase. There were significant differences between patients in both the initial score and rate of increase. This study also found that the overall level of learned helplessness in breast cancer patients was lower than that in lung cancer patients23 and neuroendocrine tumors.24 This was the same as our previous report. These differences may be related to the following: the degree of development of the disease, survival rate, and degree of illness in the body. With the recent development in medical technology and early cancer screening, the 5-year survival rate of breast cancer patients is now 80–85%, which is much higher than that of lung cancer and neuroendocrine tumors.25 This may be one reason why patients with the latter two diseases have higher helplessness. Previous studies26 have shown that learned helplessness in treatment is not fixed, but changes with time. This finding is consistent with Bonanno’s theory of psychological adjustment27 and Seligman’s learned helplessness theory.28 Breast cancer patients, although reporting learned helplessness generally at lower levels, showed a steady increase during chemotherapy. Those with learned helplessness scores of initial values of lower levels showed a faster rate of increase. This may be associated with the following: the accumulation of side effects of chemotherapy, such as nausea and fatigue,29 changes in body appearance, such as hair loss or removal of the breast, which causes social anxiety,30 and the increasing personal burden as treatment progresses. These may be related and lead to the steady increase in helplessness. Therefore, when chemotherapy begins, medical staff should identify high-risk patients early and provide targeted psychological assistance to help prevent the rapid increase in learned helplessness.
Differences in the Trajectory of Learned Helplessness in Breast Cancer Chemotherapy Patients Based on Chemotherapy Regimen
From the results of the conditional model, there was no significant difference in the level of learned helplessness between patients receiving anthracycline-based chemotherapy and those receiving non-anthracycline-based chemotherapy at the initial stage of treatment. However, as the chemotherapy process progresses, compared with patients receiving non-anthracycline-based regimens, patients in the anthracycline-based group show a faster increasing trend in learned helplessness. This small difference early may be due to the fact that a patient’s initial psychological impact is due to the stress of the cancer diagnosis, not the type of chemotherapy.31 Later in treatment, the faster rise in helplessness in anthracycline chemotherapy, it is due to its stronger side effects. Anthracycline drugs inhibit the growth of cancer cells, but they also cause more noticeable side effects. It is reported that up to 80%–100% of patients using anthracycline drugs lose their hair.32 In addition, the most common side effects of these drugs include nausea, vomiting, low blood cell counts, and heart damage that accumulates gradually.33 After each course of anthracycline treatment, patients have to experience these unpleasant symptoms again. This “treatment followed by pain” repeated cycle may let patients feel that they cannot control their own situation, which would accelerate the feeling of helplessness. Therefore, it is suggested that clear and structured psychological education should be offered to breast cancer patients with anthracycline chemotherapy early, so that breast cancer patients can know what side effects will occur and how to cope with them. In addition, using both drug-based and non-drug-based support can help reduce the physical and mental burden of side effects and slow down the increase in learned helplessness.
Age Differences in the Development Trajectory of Learned Helplessness in Breast Cancer Chemotherapy Patients
The results from the conditional model showed that younger breast cancer patients had much higher levels of learned helplessness at the beginning of chemotherapy than older patients. However, as treatment continued, the speed at which helplessness changed was similar for both age groups.Younger breast cancer patients are often at an important time in their lives. They may be studying, building a career, or raising a family. During this period, it is very important for them to keep their appearance and continue their social roles. They also often carry heavy financial and family responsibilities. As compared to the older patients, younger patients experienced more stress from the higher expected return of cancer back, family responsibilities, and money problems.34 This result is in agreement with Soqia et al.35 Currently, there is still little studies on how learned helplessness could change over time in patients of different ages during chemotherapy. Most of the current studies focused on the impact of age on survival, ability to cope with treatment, and quality of life.36 Some studies did find that younger and older patients differ in how they process information, use social support, and cope psychologically.37 However, structured psychological support has been found to help patients of all ages cope better with their disease.Therefore, medical staff should consider younger patients as a high-risk group for emotional distress, especially during early treatment. It is recommended that we do comprehensive psychological assessments when patients are diagnosed and before they start chemotherapy. Support during early stages should focus on issues of particular importance to younger women, such as fertility, work, and family role. This form of targeted assistance will help reduce early feelings of helplessness. In addition, all breast cancer patients should receive ongoing psychological support during their treatment to help them develop healthy coping skills. This will not only help patients complete treatment more successfully, but also help them in the long term.
Differences in the Trajectory of Learned Helplessness Among Breast Cancer Patients Undergoing Chemotherapy by Educational Level
The results revealed that patients with less education had much higher levels of learned helplessness at the onset of chemotherapy compared to those with more education. However, the speed at which helplessness changed over time was similar between the two groups. Essentially, the level of learned helplessness is a comprehensive reflection of an individual’s cognition, emotions, behaviors, and ability to perceive the external environment after repeatedly facing uncontrollable negative events.38 Previous research39 has found that people with less education often feel less confident and less able to manage their illness.40 In contrast, individuals with more education can often read books, search the internet, and find other ways to better understand and cope with their condition. They are also more likely to teach themselves, which can help them feel more confident during the recovery process and lessen any unnecessary worry.41 Unlike the initial level of helplessness, the rate of change reflects how patients adapt to their role and use medical resources to better cope with their condition over time. Currently, most research has focused on how learned helplessness changes over time in patients with similar levels of helplessness at the start, while not much has been studied regarding how learned helplessness changes over time in patients with similar rates of change. Most existing studies focus on how education affects survival,42 treatment compliance, and recovery after surgery.43 Some research44 has found that patients with less education often have less access to medical information, which impacts their understanding of their treatment, their ability to communicate with doctors, and their confidence in managing their own health.45 Still, with proper support, patients’ ability to cope can improve greatly.46 Therefore, medical staff should pay more attention to how education level affects patients’ psychological adjustment. When it comes to patients with less education, it’s helpful to provide video and picture health information instead of only written information. When communicating with patients, medical staff should speak in simple language and avoid using medical jargon. This can help patients better understand their condition and treatment, make realistic expectations, and gradually enhance their own sense of control and confidence in managing their disease.
The Impact of Social Support on the Development Trajectory of Learned Helplessness in Breast Cancer Chemotherapy Patients
As shown in previous studies,47 from the time of diagnosis of breast cancer to the time of start of chemotherapy, the attention of patients to support and understanding they obtain in social relationships increases greatly. Based on this, the level of objective social support may play an important role in the emergence of learned helplessness.48 Most of the previous studies based on cross-sectional design have found that social support is negatively correlated with learned helplessness. This study further adopted the latent growth model and considered social support as a time-varying covariate. Based on the latent growth model, we explored the role of social support in the dynamic evolution of learned helplessness from the results of this study, from which we can find that the social support level of breast cancer patients receiving chemotherapy is relatively stable This stability of social support may be related to patients’ relatively stable personal characteristics, such as personality traits49 and coping styles.16 However, in addition to these stable factors, patients’ social support is also influenced by a number of unstable factors, such as sudden unexpected events, career changes, family adversity, and the deterioration of peers’ illness conditions. Therefore, the social support of breast cancer patients receiving chemotherapy has a certain degree of fluctuation. This fluctuation is easily accepted by patients and affects their level of learned helplessness at this time. Huang Jinhui et al50 demonstrated that social support, a key external resource for psychological adaptation, can buffer against or reduce patients’ sense of learned helplessness. From the results of this study, from the beginning of chemotherapy to the end of chemotherapy, the level of social support can explain part of the variation of learned helplessness, which to some extent, supports the contextual protective effect of social support. However, in terms of the proportion of explained variation, the proportion of variation explained by social support is limited. This result shows that in addition to social support, learned helplessness is also affected by many other factors such as self-efficacy.51 Based on the above results, it is suggested that a multi-level social support system should be constructed in clinical practice: encourage family members to accept systematic care training to participate in care and improve the quality and continuity of emotional companionship; strengthen the relationship of trust between doctors and patients through regular follow-ups and open communication; organize group discussions and peer support activities.
Limitations
This study can provide us the useful data for understanding the process how learned helplessness occurs in breast cancer patients undergoing chemotherapy. However, there are some limitations in this study. First, convenience sampling was adopted in this study, which may lead to a certain degree of selection bias. Future research could conduct large-sample multicenter studies. Second, this study only followed patients from before chemotherapy until the sixth treatment cycle. Longer follow-up in future research would help understand how helplessness changes over a longer time. Third, the reliance on self-reported measures may be subject to response bias. Additionally, there may be other important factors affecting helplessness that were not considered in this study. Future work should look into these factors and study changes in learned helplessness more closely, while also controlling for conditions that could influence the results.
Conclusion
Learned helplessness increases over time in breast cancer patients during chemotherapy. Patients taking anthracycline-based chemotherapy do not start with higher helplessness, but their helplessness grows faster than those on other types of chemotherapy. Younger patients begin with higher helplessness than older patients, but their rate of increase is similar. Similarly, less educated patients show higher helplessness at the start, though their helplessness does not grow faster over time. Finally, more social support is consistently linked to lower levels of learned helplessness throughout treatment.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author, Zhongqiang Guo, upon reasonable request.
Ethical Approval and Consent to Participate
This study was approved by the Ethics Committee of Henan University (Ethical Review No. HUSOM2024 - 594), and permission was obtained from the nursing departments and hospital administrations of the participating institutions. This study was conducted in accordance with the principles of the Declaration of Helsinki. It strictly adhered to the principles of informed consent, voluntary participation, and data anonymity to ensure compliance with ethical standards and safeguard participant privacy.
Acknowledgments
The authors sincerely thank everyone in the research team and breast cancer survivors who participated in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There was no funding support.
Disclosure
The authors declare that they have no competing interests.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–11. doi:10.3322/caac.21660
2. Giaquinto AN, Sung H, Newman LA, et al. Breast cancer statistics 2024. CA Cancer J Clin. 2024;74(6):477–495. doi:10.3322/caac.21863
3. Giaquinto AN, Sung H, Miller KD, et al. Breast cancer statistics, 2022. CA Cancer J Clin. 2022;72(6):524–541. doi:10.3322/caac.21754
4. Wang X, Feng Z, Huang Y, et al. A nomogram to predict the overall survival of breast cancer patients and guide the postoperative adjuvant chemotherapy in China. Cancer Manag Res. 2019;11:10029–10039. doi:10.2147/CMAR.S215000
5. Wan X, Zhang Y, Peng Q, et al. A study of the relationship and mediating effects of perceived stress and post-traumatic growth in patients undergoing postoperative chemotherapy for breast cancer. Eur J Oncol Nurs. 2024;71:102659. doi:10.1016/j.ejon.2024.102659
6. Scherer KR. Learned helplessness revisited: biased evaluation of goals and action potential are major risk factors for emotional disturbance. Cognition Emotion. 2022;36(6):1021–1026. doi:10.1080/02699931.2022.2141002
7. Song X, Vilares I, Manelis A. Assessing the relationship between the human learned helplessness depression model and anhedonia. PLoS One. 2021;16(3):e0249056. doi:10.1371/journal.pone.0249056
8. Yang Z, Liu L. Research progress of learned helplessness. Prog Biochem Biophys. 2018;45(9):961–965. doi:10.16476/j.pibb.2018.0198
9. Greer S. Mind-body research in psychooncology. Adv Mind Body Med. 1999;15(4):236–244. doi:10.1054/ambm.1999.0096
10. Wang X, Wang N, Zhong L, et al. Prognostic value of depression and anxiety on breast cancer recurrence and mortality: a systematic review and meta-analysis of 282,203 patients. Mol Psychiatry. 2020;25(12):3186–3197. doi:10.1038/s41380-020-00865-6
11. Li S, Lu H, Wu M, Li H, Gao J, Wang M. Analysis of learned helplessness status and influencing factors in breast cancer patients. Chin J Nurs Educ. 2024;21(1):68–73.
12. Zhang Y. A study on the current status and influencing factors of learned helplessness in postoperative breast cancer chemotherapy patients [master’s thesis]. Henan University; 2024. doi:10.27114/d.cnki.ghnau.2024.000869.
13. Ju S, Jung YJ, Lee S, et al. Effects of chemotherapy (anthracyclin, cyclophosphamide following docetaxel regimen) on sleep, anxiety, depression, and quality of life in patients with breast cancer. Oncology. 2025:1–11. doi:10.1159/000543730
14. Liu W, Jiang N, Li Y, Cheng S. Status and influencing factors of learned helplessness in patients with multiple chronic conditions in the community. J Nurs Sci. 2025;40(7):12–15,19.
15. Liu Y, Weidong L, Pei Q, Zhang L, Fan J, Wang Q. Analysis of the current status and influencing factors of learned helplessness in pos-toperative patients with oral cancer. J Nurs Sci. 2025;40(5):16–19.
16. Dai P, Yi G, Qian D, Wu Z, Fu M, Peng H. Social support mediates the relationship between coping styles and the mental health of medical students. Psychol Res Behav Manag. 2023;16:1299–1313. doi:10.2147/PRBM.S405580
17. Shastri U, Prakasan N, Satheesan L, Kumar K, Kalaiah MK. Parental stress, learned helplessness, and perceived social support in mothers of children with hearing loss and mothers of typically developing children. Audiol Res. 2024;15(1):1. doi:10.3390/audiolres15010001
18. Dai S, Shi Y, Zhang Y, et al. Influencing factors of two-way social support for the old adults in China: a cross-sectional study. Geriatric Nursing. 2023;54:192–198. doi:10.1016/j.gerinurse.2023.09.007
19. Wu X, Zeng H, Ma S. Development of learned helplessness scale and its relationship with personality. J Sun Yat-Sen Univ Sci. 2008;30(3):357–361.
20. Xiao S. Theoretical basis and research applications of the social support rating scale. J Clin Psychiatry. 1994;(2):98–100.
21. Steiger JH. Structural model evaluation and modification: an interval estimation approach. Multivar Behav Res. 1990;25(2):173–180. doi:10.1207/s15327906mbr2502_4
22. Bentler PM. Comparative fit indexes in structural models. Psychol Bull. 1990;107(2):238–246. doi:10.1037/0033-2909.107.2.238
23. Huang F, Shi Y, Ding L, Huang J, Zhang Z. Learned helplessness and associated factors among patients with lung cancer. Patient Prefer Adherence. 2024;18:467–474. doi:10.2147/PPA.S446523
24. Zhu Z, Zhu L, Han Q, et al. Study on the core influencing factors of the postoperative trajectory of learned helplessness in patients with neuroendocrine tumor. J Nurs Adm. 2025;25(5):392–396,403.
25. Mattiuzzi C, Lippi G. Current cancer epidemiology. J Epidemiol Glob Health. 2019;9(4):217–222. doi:10.2991/jegh.k.191008.001
26. Xie C, Li L, Li Y. Trajectories of learned helplessness in maintenance haemodialysis patients and their predictive effects on self-management: a latent growth mixture modeling approach. Psychol Res Behav Manag. 2023;16:351–361. doi:10.2147/PRBM.S401380
27. Bonanno GA, SMY H, Chan JCK, et al. Psychological resilience and dysfunction among hospitalized survivors of the SARS epidemic in Hong Kong: a latent class approach. Health Psychol off J Div Health Psychol Am Psychol Assoc. 2008;27(5):659–667. doi:10.1037/0278-6133.27.5.659
28. Seligman MEP, Weiss J, Weinraub M, Schulman A. Part I: introduction. Behav Res Ther. 1980;18(5):459–512. doi:10.1016/0005-7967(80)90011-x
29. Lv D, Lan B, Zhang L, Sun X, Yang M, Ma F. Association between depression and anxiety status of breast cancer patients before adjuvant chemotherapy and chemotherapy-induced adverse events. Cancer Med. 2023;12(4):4794–4800. doi:10.1002/cam4.5283
30. Paterson C, Kozlovskaia M, Turner M, et al. Identifying the supportive care needs of men and women affected by chemotherapy-induced alopecia? A systematic review. J Cancer Surviv Res Pract. 2021;15(1):14–28. doi:10.1007/s11764-020-00907-6
31. Grassi L. Psychiatric and psychosocial implications in cancer care: the agenda of psycho-oncology. Epidemiol Psychiatr Sci. 2020;29e89. doi:10.1017/S2045796019000829
32. Freites-Martinez A, Shapiro J, Goldfarb S, et al. Hair disorders in patients with cancer. J Am Acad Dermatol. 2019;80(5):1179–1196. doi:10.1016/j.jaad.2018.03.055
33. Volkova M, Russell R. Anthracycline cardiotoxicity: prevalence, pathogenesis and treatment. Curr Cardiol Rev. 2012;7(4):214–220. doi:10.2174/157340311799960645
34. Yang T, Zhu Z, Shi J, et al. Association among financial toxicity, depression and fear of cancer recurrence in young breast cancer patient-family caregiver dyads: an actor-partner interdependence mediation model. BMC Psychiatry. 2025;25(1):97. doi:10.1186/s12888-025-06546-4
35. Soqia J, Al-Shafie M, Agha LY, et al. Depression, anxiety and related factors among syrian breast cancer patients: a cross-sectional study. BMC Psychiatry. 2022;22(1):796. doi:10.1186/s12888-022-04469-y
36. Thong MSY, Koch-Gallenkamp L, Jansen L, et al. Age-specific health-related quality of life in long-term and very long-term colorectal cancer survivors versus population controls – a population-based study. Acta Oncol Stockh Swed. 2019;58(5):801–810. doi:10.1080/0284186X.2018.1557340
37. Fitch MI, Nicoll I, Lockwood G, Chan RJ, Grundy P. Adolescent and young adult perspectives on challenges and improvements to cancer survivorship care: how are we doing? J Adolesc Young Adult Oncol. 2021;10(4):432–442. doi:10.1089/jayao.2020.0097
38. Abramson LY, Seligman ME, Teasdale JD. Learned helplessness in humans: critique and reformulation. J Abnorm Psychol. 1978;87(1):49–74. doi:10.1037/0021-843X.87.1.49
39. Sullivan DR, Liu X, Corwin DS, et al. Learned helplessness among families and surrogate decision-makers of patients admitted to medical, surgical, and trauma ICUs. Chest. 2012;142(6):1440–1446. doi:10.1378/chest.12-0112
40. Chui W-Y-Y, Chan SW-C. Stress and coping of Hong Kong Chinese family members during a critical illness. J Clin Nurs. 2007;16(2):372–381. doi:10.1111/j.1365-2702.2005.01461.x
41. Jia L, Xu H. Learned helplessness and its influencing factors among stroke patients with dysphagia. J Nurs Sci. 2022;37(23):39–42.
42. Xu J, Du S, Dong X. Associations of education level with survival outcomes and treatment receipt in patients with gastric adenocarcinoma. Front Public Health. 2022;10:868416. doi:10.3389/fpubh.2022.868416
43. Agarwal N, Chan AK, Bisson EF, et al. Impact of educational background on preoperative disease severity and postoperative outcomes among patients with lumbar spondylolisthesis: a quality outcomes database study. J Neurosurg Spine. 2024;41(3):341–352. doi:10.3171/2024.3.SPINE231024
44. Li Y, Lv X, Liang J, Dong H, Chen C. The development and progress of health literacy in China. Front Public Health. 2022;10:1034907. doi:10.3389/fpubh.2022.1034907
45. Sadeghian R, Hamedani MA, Salehipour S, Sarabandi A, Kiani F, Babamohamadi H. The health literacy level and its related factors in iranian women with breast cancer undergoing chemotherapy. Front Public Health. 2023;11:1150148. doi:10.3389/fpubh.2023.1150148
46. Coulter A, Entwistle VA, Eccles A, Ryan S, Shepperd S, Perera R. Personalised care planning for adults with chronic or long-term health conditions. Cochrane Database Syst Rev. 2015;2015(3):CD010523. doi:10.1002/14651858.CD010523.pub2
47. Campbell B, Mackenzie L, Lewis J. Beyond breast cancer: an exploration of the experiences of middle-aged female breast cancer survivors in Australia. Maturitas. 2024;188:108089. doi:10.1016/j.maturitas.2024.108089
48. Smallheer BA, Dietrich MS. Social support, self-efficacy, and helplessness following myocardial infarctions. Critical Care Nurs Quarter. 2019;42(3):246–255. doi:10.1097/CNQ.0000000000000265
49. Khosravi S, Jalali A, Jalali R, Salari N, Alikhani M. Personality traits, psychological needs, and social support among suicide attempters. Omega. 2022;84(3):899–913. doi:10.1177/0030222820921017
50. Huang J, Shi Y, Chen Y, Tang L, Zhang Z. How social support influences learned helplessness in lung cancer patients: the chain mediation role of individual resilience and self-efficacy. Front Psychol. 2024;15:1436495. doi:10.3389/fpsyg.2024.1436495
51. Jiang C, Liu T, Lv J, Ding L, Huang J, Zhang Z. A structural equation model analysis of the relationship between social support and depression in lung cancer patients: the mediating role of learned helplessness and self-efficacy. Curr Psychol. 2024;43(41):31830–31839. doi:10.1007/s12144-024-06725-8
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.