Back to Journals » Clinical Ophthalmology » Volume 16
The DEPOT Study (Dry Eye Prescription Options for Therapy): Assessing the Efficacy and Safety of OTX-DED (Dexamethasone Ophthalmic Insert 0.3 mg) for Intracanalicular Use Compared with Loteprednol Suspension for the Treatment of Episodic Dry Eye
Authors Hovanesian JA ![]() , Keyser A
, Keyser A ![]() , Berdy G, Sorensen R
, Berdy G, Sorensen R
Received 30 August 2022
Accepted for publication 10 November 2022
Published 21 November 2022 Volume 2022:16 Pages 3841—3849
DOI https://doi.org/10.2147/OPTH.S387111
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
John A Hovanesian,1 Andrew Keyser,1 Gregg Berdy,2 Robert Sorensen3
1Harvard Eye Associates, Laguna Hills, CA, USA; 2Ophthalmology Associates, St. Louis, MO, USA; 3Inland Eye Specialists, Hemet, CA, USA
Correspondence: John A Hovanesian, Harvard Eye Associates, 23961 Calle Magdalena, Suite 300, Laguna Hills, CA, 92653, USA, Tel +1 949 951 2020, Email [email protected]
Purpose: To compare OTX-DED, an investigational dexamethasone intracanalicular insert, to loteprednol 0.5% suspension applied QID for 28 days as treatments for acute exacerbations of dry eye disease in terms of patient symptoms, corneal staining, tear breakup time (TBUT), and ocular redness.
Methods: Fifty patients with an acute exacerbation of dry eye with at least grade 1 corneal staining were randomized to receive treatment and were each evaluated in one eye at baseline, two weeks and four weeks with the standard patient evaluation of eye dryness (SPEED) questionnaire, the Oxford Scale for corneal stain, Schulze Scale for ocular redness, and intraocular pressure (IOP).
Results: Forty-four patients completed the study. Significant improvement was noted from baseline to both week 2 and 4 for each treatment in SPEED scores, corneal staining, and TBUT. Ocular redness improved significantly from baseline to week 2 for loteprednol and week 4 for both drugs. No significant difference was noted between treatments in any of these evaluations at any time point. Retention (visibility) of the OTX-DED insert was 95% at week 2 and 90% at week 4. IOP rose significantly from baseline to both week 2 and 4 for eyes receiving loteprednol but not for those receiving OTX-DED.
Conclusion: OTX-DED significantly improved on both signs and symptoms of eyes suffering from acute exacerbations of dry eye disease. This improvement was similar to that seen with loteprednol 0.5% suspension, a well-accepted treatment for this condition. IOP did not change significantly in patients with OTX-DED. These findings support the use of this unique intracanalicular insert for the treatment of acute dry eye once this product is approved and available for use.
Keywords: drug delivery, dry eye, steroid, OTX-DED, intracanalicular insert, Dextenza
Plain Language Summary
This study evaluated two anti-inflammatory steroid drugs to evaluate how well they worked in treating sudden exacerbations of dry eye disease. The first drug was dexamethasone, which is delivered to the eye not as a traditional eye drop but as a tiny insert placed in the tear drainage duct of the lower eyelid. This insert was compared to a widely accepted eye drop treatment, loteprednol. Fifty patients were evaluated over four weeks in terms of symptoms and common signs used by eye doctors to evaluate the severity of dry eye. These signs included corneal staining, stability of the tear film, and eye redness. Eye pressure was also evaluated because it commonly rises (sometimes causing glaucoma) in patients taking steroid medicines. In the study, both drugs performed very well and very similarly, showing statistically significant improvement in both signs and symptoms at both 2 and 4 weeks. Neither drug raised meaningful safety concerns. This study suggests that a new slow-delivery form of dexamethasone may be very useful in treating episodes of dry eye disease.
Introduction
Dry Eye Disease (DED) affects an estimated 5–15% of the American population1–3 and is characterized by altered homeostasis of the tear film, in which tear film instability and hyperosmolarity, ocular surface inflammation and damage, and neurosensory abnormalities play etiological roles.4 It is common for patients suffering from DED to experience episodic flares, which are typically associated with acute exacerbation of discomfort symptoms.5 Topical corticosteroid medication is routinely used to alleviate such acute signs and symptoms.6 In DED, eye drops are by far the most widely established method of topical medication delivery to the eye, with over 90% of ophthalmic formulations currently on the market being topical eye drops.7 Eye drops, however, are frequently associated with a lack of compliance, difficulty of use, and requirement of assistance from family members, with over 90% of patients demonstrating improper drop insertion technique.8,9 In addition, drops deliver medication to the eye at inconsistent frequencies, even when applied in accordance with proper usage, resulting in fluctuations in medication concentration.10 Novel drug delivery platforms present an alternative to eye drops, as they remove the difficulties associated with drop insertion from patients’ routines. Dextenza (dexamethasone ophthalmic insert 0.4 mg, Ocular Therapeutix, Bedford, MA) is an intracanalicular insert delivered to the lower lid lacrimal canaliculus by an eye surgeon after cataract surgery. Similar in shape to a dissolving collagen punctal plug, this insert made of hydrogel has a length of 3 mm and width of about 0.55 mm, and delivers a tapering dose of 0.4 mg of dexamethasone over several weeks, offering sufficient potency to control postoperative inflammation. In canine models, this insert delivered sustained levels of dexamethasone around 1000 ng/mL in tear fluid through 7 days, with complete release by 17 days.11 This steroid delivery mechanism has gained wide acceptance in cataract surgery and shows very infrequent incidence of intraocular pressure rise,12 a possible side effect of topical corticosteroid treatment.13 A similar product, OTX-DED, which delivers 0.3 mg of dexamethasone in an insert of about 2.2 length by 0.5 mm width, is being developed to alleviate dry eye symptoms and is still under investigation. OTX-DED can be implanted with the same techniques as Dextenza and has similar risks associated with the insertion process, as demonstrated in the video reference below.14 OTX-DED is the subject of this study.
The objective of this study was to evaluate the safety and efficacy of OTX-DED as a treatment for episodes of dry eye. This was done by measuring patient-reported efficacy, as well as impact on objective signs of inflammation and ocular surface damage, in comparison to a loteprednol 0.5% suspension (Lotemax, Bausch and Lomb, Bridgewater, NJ), an FDA-approved topical eye drop steroid suspension that is commonly used for episodic dry eye.
Materials and Methods
This was a multicenter, prospective, randomized controlled study with an open-label design examining the efficacy of relieving both signs and symptoms of DED in 50 patients with acute exacerbations of this disease. Enrolled patients were randomized to receive treatment with either OTX-DED, an investigational steroid insert, or loteprednol etabonate 0.5% suspension QID for 4 weeks. Patients receiving OTX-DED had this product inserted into the lower punctum by the investigator at the time of enrollment, and patients receiving loteprednol 0.5% were provided with a bottle of this medication at enrollment. Where clinically appropriate, both eyes of subjects were treated with the study drug, but only one eye of each patient was included in the study data collection. If both eyes met the inclusion/exclusion criteria, the eye with more severe DED based on signs as judged by the examiner at the screening/baseline visit was used for data collection. If both eyes met the criteria and had the same severity, the right eye was chosen as the study eye.
The primary outcome measure was the patient-reported score of the standard patient evaluation of eye dryness (SPEED) questionnaire 14 days after initiating therapy. The secondary outcome measures were SPEED score, corneal staining (Oxford Scale),15 tear breakup time, and ocular redness score (Schulze Scale)16 28 days after beginning therapy. The safety outcome measured at 14 and 28 days was intraocular pressure measured by Goldmann applanation.
At each follow-up study visit after enrollment, investigators examined the study eye for retention of OTX-DED using cobalt blue light to induce fluorescence of the fluorescein-conjugated insert. For patients taking loteprednol, investigators asked patients whether they were consistently using the eye drop.
Recruited patients were selected from patients seen in the office sequentially. Inclusion criteria for this study included age 18 years or greater, willingness to take an electronic survey about their tolerability of either study medication, a minimum of grade 1 corneal staining, and a recent, acute exacerbation of dry eye characterized by ocular surface discomfort. Either signs or symptoms of dry eye were used to determine dry eye exacerbation. Patients who were on a baseline regimen of artificial tears were asked to continue their baseline treatment, so that only one parameter (the initiation of the study drug) would be altered during the study.
Exclusion criteria included the following conditions in either eye within the 30 days prior to enrollment: clinically significant ocular trauma, active ocular herpes simplex or herpes zoster (eye or eyelid) infection, ocular inflammation (uveitis, iritis, scleritis, episcleritis, keratitis, and conjunctivitis), ocular infection (eg, viral, bacterial, mycobacterial, protozoan or fungal infection of the cornea, conjunctiva, lacrimal gland, lacrimal sac or eyelids including a hordeolum or stye). Other exclusion criteria included moderate to severe (grade 2–4) allergic, vernal or giant papillary conjunctivitis, eyelid abnormalities that significantly affect lid function (eg, entropion, ectropion, tumor, edema, blepharospasm, lagophthalmos, severe trichiasis, severe ptosis), ocular surface abnormality that may compromise corneal integrity (eg, prior chemical burn, recurrent corneal erosion, corneal epithelial defect, or map dot fingerprint dystrophy), participation in another ophthalmic clinical trial involving a therapeutic drug or device within 30 days prior to the distribution of the survey, participation in this trial in the same patient’s fellow eye, and patients who are pregnant or breastfeeding or who may become pregnant during participation in the study.
The study was registered on ClinicalTrials.gov as study NCT04911361 and conducted under a US FDA IND number 152083. The study was conducted under the approval of WCG IRB as protocol DEPOT 1911 OTX. None of the authors have any affiliation with WCG IRB. Ocular Therapeutix provided funding for this study. The study adhered to the principles of both the Declaration of Helsinki and good clinical practices as defined by the U.S. Food and Drug Administration. Reasonable requests for de-identified patient data relating to the study findings, including any outcome measures, will be available through the corresponding author for 5 years following the publication date. All patients provided informed consent prior to enrollment.
Results
Fifty patients were enrolled in the study, and 44 (88%) subjects completed all study visits at three study sites, all of which contributed approximately equal numbers of subjects (Table 1). Average age was 68± 9.3 (range 40–84) years. Thirty-six (80%) were females, and 27 (61%) were right eyes. Between the two treatment arms, there were no statistically significant differences in the distribution of age, gender, or eye enrolled (Table 2).
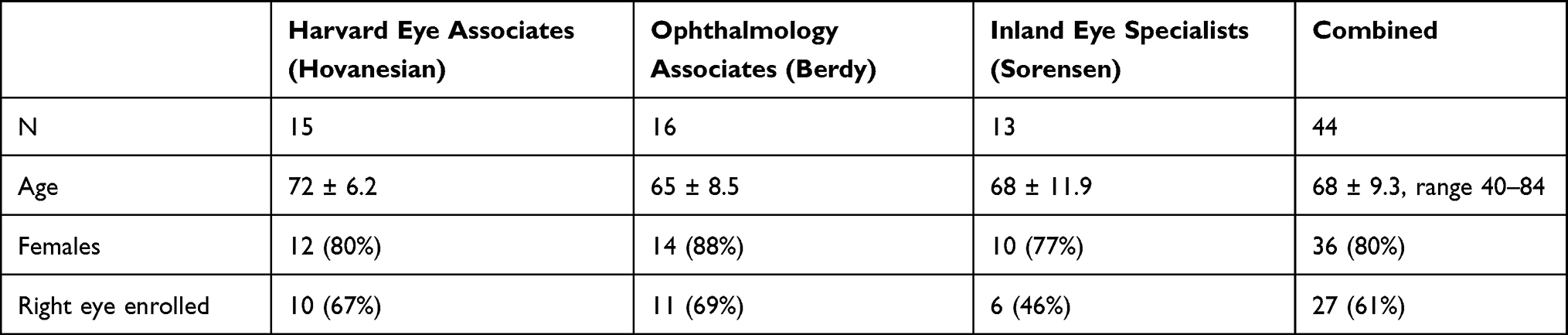 |
Table 1 Study Population at Each Site Was Similar |
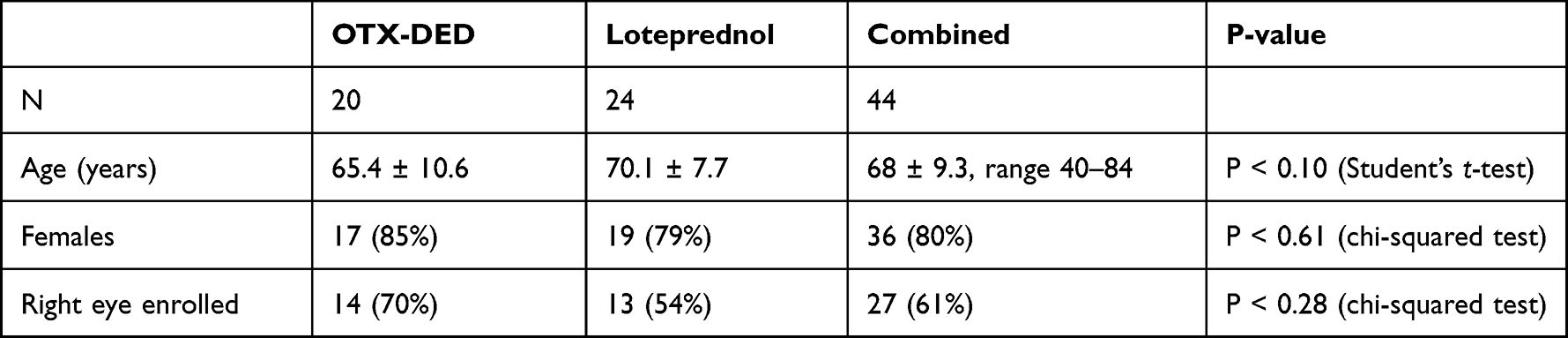 |
Table 2 Patients Randomized to the Two Treatment Groups Had Similar Characteristics |
Patients were included in the final data analysis only if they completed all study visits. There were six patients who did not complete all their study visits. Three subjects completed visit 1 and visit 3 but were unable to make their study visit within the Visit 2 window. One subject withdrew due to a family emergency. The last two subjects indicated they no longer wanted to continue participating in the study but did not give a specific reason as to why they decided not to proceed. No patient who withdrew described side effects or intolerability of either treatment as a reason for withdrawal. Of the 44 patients who underwent data analysis, 20 (45%) received OTX-DED and 24 (55%) received loteprednol.
Primary and First Secondary Outcome Measures
SPEED scores (Figure 1) significantly improved after treatment with both OTX-DED and loteprednol, with mean SPEED scores of 16.4 ±5.3 and 14.7 ± 6.0 at baseline, 11.6 ± 6.4 and 10.25 ± 5.9 at 2 weeks, and 10.6 ± 5.7 and 10.6 ± 5.8 and at 4 weeks, respectively (P < 0.0005 and P < 0.0001 for baseline vs 2 weeks and P < 0.0001 and P < 0.0002 for baseline vs 4 weeks, paired t-test).
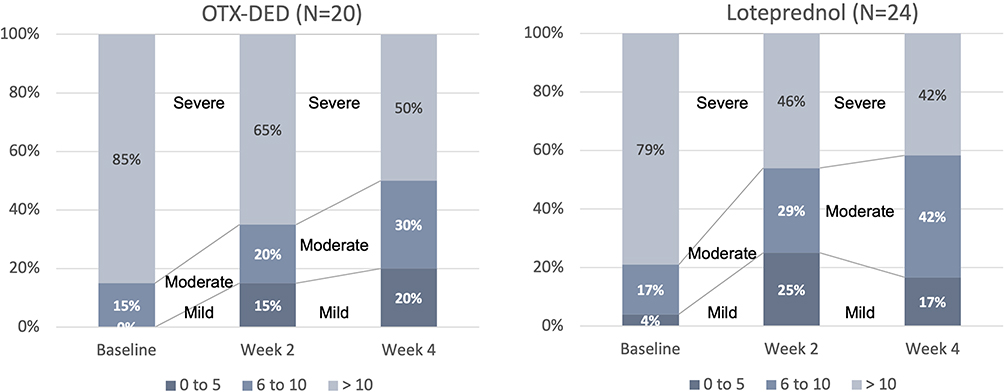 |
Figure 1 SPEED Scores Significantly Improved at 2 and 4 Weeks (P<0.00001, paired t-test). |
Among the OTX-DED and loteprednol treatment groups, respectively, SPEED scores of 5 or less were observed significantly more frequently in patients at 2 and 4 weeks than at baseline (Figure 1). These scores occurred in 0 and 1 (4%) patients before treatment, 3 (15%) and 6 (25%) after 2 weeks, and 5 (25%) and 4 (17%) after four weeks, respectively (P < 0.0008 and P < 0.003 for baseline vs 2 weeks and P < 0.005 and P < 0.0005 for baseline vs 4 weeks, respectively, McNemar’s Chi-squared test).
While both treatments significantly improved SPEED scores compared to baseline, between OTX-DED and loteprednol, no significant difference in SPEED score improvement was noted at any time point.
Other Secondary Outcome Measures
Corneal staining (Figure 2), measured by the Oxford scale, significantly improved among patients treated with OTX-DED from a mean grade of 2.3 ± 1.1 to 0.8 ± 0.7 and 0.8 ± 0.8 at baseline, week 2 and week 4, respectively (P < 0.0001 for baseline vs both 2 and 4 weeks, paired t-test). Among patients treated with loteprednol, similar improvement was seen from 2.3 ± 1.0 at baseline to 1.1 ± 0.9 after 2 weeks and 1.0 ± 0.9 after 4 weeks (P < 0.0001 for baseline vs both 2 and 4 weeks, paired t-test).
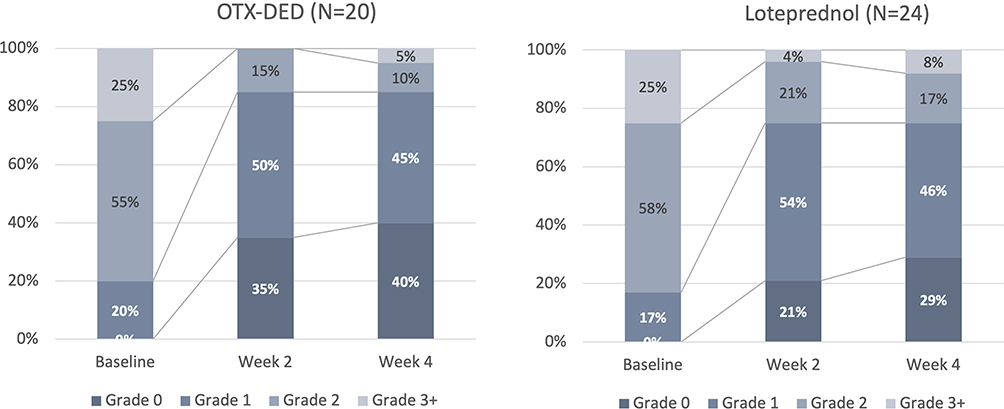 |
Figure 2 Corneal staining significantly improved with both OTX-DED and loteprednol (P< 0.0001 for baseline vs 2 and 4 weeks, paired t-test). With OTX-DED, corneal staining disappeared in 35% at 2 weeks and 40% at 4 weeks (Oxford Scale). |
All eyes had at least grade 1 staining before treatment, which was an inclusion criterion for the study. Of these, improvement to grade 0 was seen in 7 (35%) with OTX-DED and 5 (21%) with Loteprednol at 2 weeks and 8 (40%) with OTX-DED and 7 (29%) with Loteprednol at 4 weeks (Figure 2). This improvement was statistically significant for each drug (P < 0.0001, McNemar’s test for baseline vs both 2 and 4 weeks for both drugs), and the difference in staining improvement between OTX-DED and loteprednol was not statistically significant at any time point.
Mean TBUT improved significantly for patients treated with both OTX-DED and Loteprednol. These changes were statistically significant compared to baseline (McNemar’s chi-squared test for baseline vs 2 and 4 weeks; Table 3). No significant difference between OTX-DED and loteprednol was noted with regard to TBUT.
 |
Table 3 Change in Mean Tear Breakup Time (TBUT) |
Both OTX-DED and Loteprednol significantly increased the proportion of patients with a “normal” TBUT greater than 10 seconds (Figure 3, P < 0.00002 and < 0.00006 for OTX-DED for baseline vs 2- and 4-week visits and P < 0.00001 for Loteprednol baseline vs both 2- and 4-week visits).
 |
Figure 3 Both OTX-DED and Loteprednol significantly increased the proportion of patients with a “normal” TBUT greater than 10 seconds (P < 0.00002 and < 0.00006 for OTX-DED for baseline vs 2 and 4 week visits and P < 0.00001 for Loteprednol baseline vs both 2 and 4 week visits). |
Both drugs reduced redness (Schulze Scale, Figure 4), with significant improvement from baseline to Week 2 for Loteprednol (P < 0.02, paired t-test) and from baseline to Week 4 for both drugs (P < 0.001 for OTX-DED and P < 0.01 for Loteprednol, paired t-test). Again, no significant difference between drugs was noted.
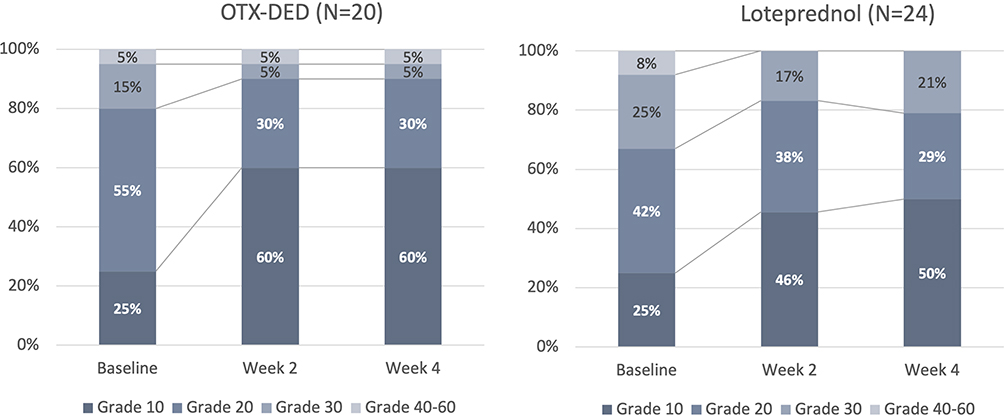 |
Figure 4 Both drugs reduced redness (Schulze Scale), with significant improvement from baseline to Week 2 for Loteprednol (P < 0.02, paired t-test) and from baseline to Week 4 for both drugs (P < 0.001 for OTX-DED and P < 0.01 for Loteprednol, paired t-test). |
Retention of OTX-DED Insert and Compliance with Loteprednol
At the 14-day follow-up visit, all 24 patients taking loteprednol suspension self-reported good compliance with the drug regimen. At 28 days, 10 (42%) reported they were not taking the medication as prescribed. Of the 20 patients with OTX-DED, the insert could not be observed in the nasal canaliculus in 2 (10%) at 14 days, though in one of these two patients the insert was later visualized at day 28, implying it was indeed present at day 14. At 28 days, the insert was not observed in 2 (10%) patients, of whom one had the insert visible at day 14. We concluded that the retention rate of OTX-DED was 95% at 14 days and 90% at 28 days.
Safety Outcome Measure
Mean IOP for each drug at each visit is shown in Figure 5. From baseline to both 2 and 4 weeks, IOP rose significantly among patients taking loteprednol (P < 0.02 and P < 0.009, paired t-test), though these differences were not clinically meaningful. No significant rise in IOP was observed among patients who received OTX-DED.
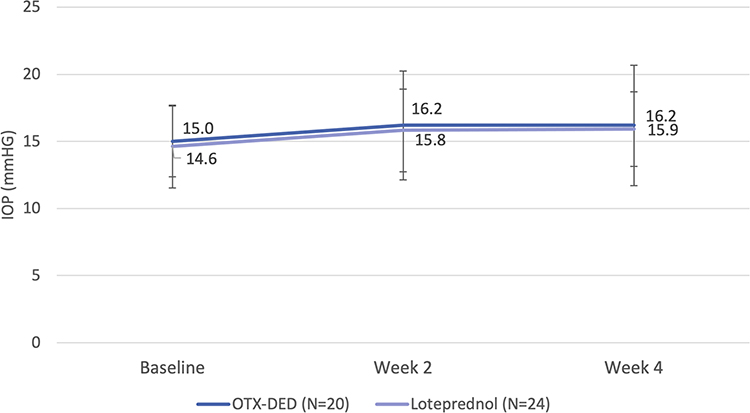 |
Figure 5 IOP rose significantly among patients taking Loteprednol (P < 0.02 and P < 0.009, paired t-test) but not among patients who received OTX-DED. |
Discussion
To our knowledge, this is the first study of OTX-DED for treatment of acute symptoms of dry eye. We compared this new drug to a long-established topical steroid, loteprednol, which is frequently selected off-label for its use in this condition and is known to have rapid efficacy and a tolerable side effect profile. This study showed both drugs significantly improved ocular surface health as measured by patient symptoms, corneal staining, tear breakup time, and conjunctival redness. Intraocular pressure rose slightly with both drugs, but not significantly with OTX-DED.
Of note, 80% of the enrolled patients in this study were female. This is not surprising, given the greater frequency of dry eye disease among females and the greater proportion of females in the living population over age 65. No significant difference in the proportion of females was seen between the two treatment groups. Therefore, we do not believe this influenced the findings of the study. However, it is unknown whether the findings of the study would be identical in a male-only population.
In this evaluation, we did not anticipate, nor did we find a major advantage of OTX-DED over loteprednol on the studied outcome measures. It is interesting to note that the small rise in IOP noted between baseline and weeks 2 and 4 was significant for loteprednol but not for OTX-DED. Though it is statistically significant, we do not believe this difference is clinically meaningful. Numerically, the two drugs had almost identical rises in IOP, and the loteprednol group was larger by four patients, which may explain why the IOP rise only for this drug was significant and only at the level of P < 0.02 and P < 0.009 using a paired t-test.
Despite the similarities in the performance and safety of these two drugs, a major difference exists in the way each is delivered. While loteprednol is a traditional eye drop suspension delivered QID, OTX-DED is an intracanalicular insert that slowly releases its active ingredient (dexamethasone) over several weeks. This has important theoretical advantages over an eye drop.
First, patient compliance becomes a non-issue with a sustained delivery vehicle like the dissolving hydrogel that the OTX-DED insert is composed of. In this study, 95% of patients had their insert retained at 14 days. (Although the inserts were only visualized in 18 of 20 (90%) of patients at 14 days, on the next follow-up visit, one of these patients’ missing inserts was confirmed to be present.) By 28 days, 90% of eyes retained their OTX-DED insert. By contrast, among patients taking drops, none reported compliance issues at 14 days, but 42% reported limited compliance by Day 28. This is not surprising since more than one study has shown a significant drop in patient compliance with dosing regimens more frequent than once daily and with prolonged use.17,18 In symptomatic dry eye, one might expect patients to be highly motivated and compliant; at least in this study, compliance issues with drops did not evidently interfere with the performance of loteprednol, though study patient compliance with medication is typically better than in a real-world scenario.
Second, a drug like loteprednol suspended in vehicle may not have the dose uniformity of a dissolved drug like dexamethasone. A study of prednisolone acetate suspension by Stringer showed a delivered dose of 500% of the declared concentration after a simulated 19 days of therapy, even when the bottle was shaken for 5 seconds before dispensing.19 In this study, we used the branded Lotemax suspension of loteprednol, but this same drug is available from several generic manufacturers. Though no study of these generic formulations has been performed to our knowledge, it is also reasonable to question the dosing uniformity of these varying suspensions and dispensing bottles.
Third, slow, sustained release of dexamethasone may cause a lower risk of side effects like an IOP rise. While dexamethasone, as a potent steroid, has traditionally been considered a high-risk medication for patients who are steroid responders, the sustained-release version of the drug compared very favorably with loteprednol—thought to be the safest steroid—at least in the limited population of this study. To be fair, this study did not include known steroid responders or patients with glaucoma, so care must be taken in interpreting these findings in that special population.
This study is not without its limitations. First, the sample size of 50 total patients randomized to two treatment groups is limited, with 44 patients completing all data at all visits. However, the remarkably similar performance of the two treatments, and the highly significant improvement both drugs showed from baseline to week 2 and 4, suggests this study was powered adequately to meet its objectives.
This was an open-label study. While this introduces the possibility of observer bias, the primary outcome measure was a patient-reported outcome, and all outcome measures were very similar between the two treatments. To fully mask the study, it would have been necessary to place a sham insert in patients treated with loteprednol and give inactive vehicle drops to patients treated with the OTX-DED intracanalicular insert. While these measures would have helped to mask the study, they certainly would have altered the outcomes; a sham insert would increase the tear lake, and an inactive vehicle would have some effect as a topical lubricant. In designing the study, the limitations of an open-label design were chosen over the introduction of confounding variables that would yield only a theoretical guard against observer bias.
We believe this study demonstrates that OTX-DED can be a useful agent for management of patients with episodic dry eye. Across the variables that both patients and clinicians care about—symptoms and ocular surface health—the drug showed rapid and safe performance, comparable to one of the most trusted, if off-label alternatives. As OTX-DED approaches FDA approval as a treatment indicated for dry eye disease, we hope this study will help guide clinicians in their expectations of this useful drug.
Data Sharing Statement
Reasonable requests for de-identified patient data relating to the study findings, including any outcome measures, will be available through the corresponding author, John A. Hovanesian, MD, for 5 years following the publication date.
Acknowledgments
This was funded by Research InSight, LLC under a grant from Ocular Therapeutix. Assistance in data collection and study management was provided by Leslie Lemieux, BS. Partial results of this paper were presented as a paper at the 2022 symposium of the American Society of Cataract and Refractive Surgery.
Disclosure
Dr John A Hovanesian reports grants from Ocular Therapeutix, during the conduct of the study; is a stockholder in Ocular Therapeutix, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Dana R, Bradley JL, Guerin A, et al. Estimated prevalence and incidence of dry eye disease based on coding analysis of a large, all-age United States Health Care System. Am J Ophthalmol. 2019;202:47–54. doi:10.1016/j.ajo.2019.01.026
2. Farrand KF, Fridman M, Stillman IÖ, Schaumberg DA. Prevalence of diagnosed dry eye disease in the United States among adults aged 18 years and older. Am J Ophthalmol. 2017;182:90–98. doi:10.1016/j.ajo.2017.06.033
3. Oliverd S, Beatriz M, Jamesm T, Karen B-R, Sheila W. Prevalence of dry eye among the elderly. Am J Ophthalmol. 1997;124(6):723–728. doi:10.1016/s0002-9394(14)71688-5
4. Craig JP, Nelson JD, Azar DT, et al. TFOS Dews II report executive summary. The Ocular Surface. 2017;15(4):802–812. doi:10.1016/j.jtos.2017.08.003.
5. Perez VL, Stern ME, Pflugfelder SC. Inflammatory basis for dry eye disease flares. Exp Eye Res. 2020;201:108294. doi:10.1016/j.exer.2020.108294
6. Pflugfelder SC, Geerling G, Kinoshita S, et al.Management and therapy of dry eye disease: Report of the management and therapy subcommittee of the International Dry Eye Workshop (2007). Ocul Surf. 2007;5(2):163–178. doi:10.1016/s1542-0124(12)70085-x.
7. Lang JC. Ocular drug delivery conventional ocular formulations. Adv Drug Deliv Rev. 1995;16(1):39–43. doi:10.1016/0169-409x(95)00012-v
8. Dietlein TS, Jordan JF, Lüke C, Schild A, Dinslage S, Krieglstein GK. Self-application of single-use eyedrop containers in an elderly population: comparisons with Standard Eyedrop Bottle and with younger patients. Acta Ophthalmol. 2008;86(8):856–859. doi:10.1111/j.1755-3768.2007.01155.x
9. An JA, Kasner O, Samek DA, Lévesque V. Evaluation of eyedrop administration by inexperienced patients after cataract surgery. J Cataract Refract Surg. 2014;40(11):1857–1861. doi:10.1016/j.jcrs.2014.02.037
10. Shell JW. Ophthalmic drug delivery systems. Drug Dev Res. 1985;6(3):245–261. doi:10.1002/ddr.430060307
11. Blizzard CD, Desai A, Driscoll A, Cheung M, Goldstein MH. Ocular pharmacokinetics of OTX-DED, a sustained-release intracanalicular insert delivering dexamethasone, in a canine model. Invest Ophthalmol Vis Sci. 2021;62(8):1323.
12. Ocular Therapeutix™ Announces Topline Results for Phase 2 Clinical Trial of OTX-DED for the Short-Term Treatment of Dry Eye Disease; December, 2011. Available from: https://www.businesswire.com/news/home/20211206005259/en/.
13. Pleyer U, Ursell PG, Rama P. Intraocular pressure effects of common topical steroids for post-cataract inflammation: are they all the same? Ophthalmol Ther. 2013;2(2):55–72. doi:10.1007/s40123-013-0020-5
14. Hovanesian JA Intracanalicular dexamethasone insert implantation. American Academy of Ophthalmology; June 6, 2019. Available from: https://www.aao.org/clinical-video/surgical-technique-intracanalicular-dexamethasone-.
15. Bron A, Evans VE, Smith JA. Grading of corneal and conjunctival staining in the context of other dry eye tests. Cornea. 2003;22(7):640–650. doi:10.1097/00003226-200310000-00008
16. Schulze MM, Jones DA, Simpson TL. The development of validated bulbar redness grading scales. Optom Vis Sci. 2007;84(10):976–983. doi:10.1097/OPX.0b013e318157ac9e
17. Stratton-Loeffler MJ, Lo JC, Hui RL, et al.Treatment of vitamin D deficiency within a large integrated health care delivery system. J Manag Care Spec Pharm. 2012;8(7):497–505.
18. Falagas ME, Karagiannis AK, Nakouti T, Tansarli GS. Compliance with once-daily versus twice or thrice-daily administration of antibiotic regimens: a meta-analysis of randomized controlled trials. PLoS One. 2015;10(1):e0116207. doi:10.1371/journal.pone.0116207
19. Stringer W, Bryant R. Dose uniformity of topical corticosteroid preparations: difluprednate ophthalmic emulsion 0.05% versus branded and generic prednisolone acetate ophthalmic suspension 1%. Clin Ophthalmol. 2010;4:1119–1124. doi:10.2147/OPTH.S12441
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.