Back to Journals » Research and Reports in Urology » Volume 14
The “Cut-to-the-Light” Technique Laser Endoureterotomy for Complete Ureteral Obstruction Resurfaces! A New Application of an Old Technique
Authors Yarak N, Zouari S ![]() , Karray O, Sleiman W, Abdelwahab A, Bart S, Abdessater M
, Karray O, Sleiman W, Abdelwahab A, Bart S, Abdessater M ![]()
Received 22 April 2022
Accepted for publication 13 August 2022
Published 10 October 2022 Volume 2022:14 Pages 351—358
DOI https://doi.org/10.2147/RRU.S371856
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Panagiotis J Vlachostergios
Naim Yarak, Skander Zouari, Omar Karray, Walid Sleiman, Alaa Abdelwahab, Stéphane Bart, Maher Abdessater
Urology Department, Centre Hospitalier Régional René DUBOS, Pontoise, 95300, France
Correspondence: Maher Abdessater, Email [email protected]
Objective: To describe our new endoscopic approach in treating iatrogenic ureteral stenosis using the “cut-to-The-light” technique.
Methods: Case of a 54 year-old female patient who underwent a right percutaneous nephrolithotomy to treat a staghorn calculus with two subsequent complimentary ureteroscopies complicated by a severe proximal ureteral obstruction. An antegrade flexible uretereroscope and a retrograde rigid ureteroscope were used to locate the stenosis. With the aid of a 365-μm Ho: YAG laser fiber (settings 0.4 J, 12 Hz), we managed to successfully create a small incision in the stenotic lesion, the rigid ureterscopy light was clearly seen by the antegrade flexible ureteroscope and a through-and-through guidewire was then placed, securing the ureter. Ureteral dilatation was then performed followed by a full thickness incision of the ureteral stenosis. A single 8Fr, 28 cm double J ureteral stent was finally placed after stone fragmentation.
Results: The operating time was 200 mins. No blood loss. No fever or signs of UTI were seen shortly after the operation. The Foley catheter was successfully removed at day one post-op. The hospital stay was short of only 2 days.
Conclusion: The “cut-to-the-light” technique is a new application in the arsenal of ureteral stricture treatment that has been scarcely described in the literature before. The use of this method seems to offer excellent outcomes thus demonstrating the importance of this minimally invasive technique as an alternative to conventional invasive methods used. We believe that studies with larger samples and longer follow up are needed in order to fully determine the benefits of this method and to assess and reveal its suitable application and its drawbacks.
Keywords: ureteral stenosis, ureteroscopy, “cut-to-the-light” technique, laser endoureterotomy
Introduction
With the worldwide increase in urolithiasis prevalence (4–5%) we have noticed higher success rates and lower complications rates of ureteroscopy owing to radical URS improvements and stone-disintegration devices.1–4
A ureteral stricture is a late and serious complication of ureteroscopy. It is a luminal narrowing of the ureter leading to functional obstruction of the kidney that might be sometimes a silent process leading progressively to the loss of the ipsilateral renal function. Thus correct timing and convenient modalities of ureteral stricture treatment are crucial to preserve renal function.5 Management of the post-URS stricture exhibits conspicuous polemics with options ranging from open repair to include laparoscopic, robotic and interventional techniques.6
We herein report in this article a case of an iatrogenic complete ureteral obstruction caused by ureteroscopy (URS), in which a minimally invasive, endo-urological cut-to-the-light technique efficaciously repaired the ureteral stricture.
Methods
Clinical Presentation
A case of a 54 year-old female patient known to have cervical cancer treated by radio-chemotherapy in 2012, complicated by an intestinal obstruction due to radiation induced intestinal adhesions s/p right permanent ileostomy in 2014 and moderate renal failure related to cancer treatment.
The patient sought medical attention after laboratory workup for a flu-like illness revealed an acute kidney injury. Abdominopelvic ultrasound and CT scan confirmed the presence of a right staghorn calculus measuring 20 mm by 35 mm with a density of 470 HU compatible with a uric acid stone. After failure of medical treatment trial with urinary alkalinization, a right percutaneous nephrolithotomy was performed with two complementary flexible ureteroscopy sessions for residual calculi. Note that infrared spectroscopic studies revealed that the predominant composition of the calculus was uric acid (85%) and calcium-oxalate crystals (15%).
The patient had continuous unrelenting right flank pain with a subsequent abdominopelvic ultrasound and CT scan showing the evidence of a residual 17 mm by 26 mm staghorn calculus with an average density of 470 HU residing in the inferior calyceal system, associated with a proximal ureteral and calyceal dilatation (Figure 1), nevertheless without any evidence of ureteral stone or stenosis. Laboratory studies showed a slight increase in the creatinine level with a creatinine clearance of 39 µmol/L as compared to a baseline of 57 µmol/L.
 |
Figure 1 Portal phase of the computed tomography (CT) of the abdomen and pelvis with IV contrast injection showing a proximal ureteral and calyceal dilatation, a lower calyceal stone and a tapering of the right ureter (arrows). (A) Coronal view. (B) Axial view. |
The patient underwent another failed right flexible ureteroscopy confirming the presence of the lumbar ureteral stricture extending over 2 cm and 4 cm away from the ureterovesical junction with ensuing right permanent nephrostomy. Urinary alkalinization was not efficient because of absorption difficulties related to her ileostomy.
Three months after the last ureteroscopy, the patient sought medical attention at our department for the management of a complete right proximal ureteral stenosis. We endeavored to treat it endoscopically using a simultaneous retrograde and antegrade ureteroscopic approach with a Ho: YAG laser incision.
Laser Endoureterotomy Material
In this intervention, a two ureteroscopy approach was used: a retrograde rigid ureteroscope and an antegrade flexile ureteroscope. A 365-µm Ho: YAG laser fiber (settings 0.4 J, 12 Hz) was used to perform the endoureterotomy.
Surgical Technique
The surgical procedure was performed as follows. Under general anesthesia, the patient was put in the modified Valdivia position. Using an antegrade approach first, a contrast injection using a pre-existing nephrostomy tube showed a non-dilated right pelvicalyceal system, a filling defect corresponding to the already outlined uric acid stone as well as tapering of the contrast at the L3 level of the proximal ureter. A terumo guidewire was successfully placed in an antegrade fashion in the proximal ureter just above the stenosis. Using a 7 Fr ureteral catheter, a retrograde contrast injection was performed showing a blind end at the level of the lower border of L3. The length of the non-opacified zone and therefore of the stenosis was estimated to be of 2 cm (Figure 2). A Terumo guidewire was placed as well in the distal ureteral just before the stenosis. At this level, we inserted a 10/12 Fr 35-cm ureteral access sheath from the nephrostomy to the stenotic lesion under radiographic guidance. Using a disposable flexible ureteroscope for antegrade ureteroscopy, a pinhole lesion was observed and was considered as the stenotic lesion (Figure 3). With the aid of a 365-µm Ho: YAG laser (settings 0.4 J, 12 Hz), we managed to successfully create a small incision in the stenotic lesion (Figure 4). A Terumo guidewire was then passed through this incision down to the bladder and retrieved through the urethral orifice as a through-and-through guidewire as such securing the ureter (Figure 5A and B). A 6-Fr rigid ureteroscope was used in a retrograde manner and we progressed till the stenotic lesion which was tight and fibrous. When we flushed contrast reagent, it was observed by both the retrograde and antegrade ureteroscopes. At this time, the rigid ureterscopy light was clearly seen by the antegrade flexible ureteroscope (Figure 5C). In order to insert a retrograde 10/12 Fr ureteral access sheath, we dilated the ureter progressively with ureteral catheters of 7, 8 and 9 Fr and then we progressed with a full thickness incision beside the guidewire and under observation by the retrograde ureteroscope to ensure an efficient incision (Figure 6). A retrograde flexible ureterosocpe was then used to reach the pelvicalyceal system where a 2 cm renal pelvic stone was found evoking a uric acid calculi with a homogenous, slightly indented, yellow surface. A slow and progressive dusting of the stone was then performed using a 365-µm Ho: YAG laser. After confirming a stone-free kidney, we inserted an 8 Fr, 28 cm double J ureteral stent.
 |
Figure 2 X-ray fluoroscopique image (A) and schema (B) of the stenotic ureter. |
 |
Figure 3 The stenotic lesion as seen by the antegrade flexible ureteroscope. |
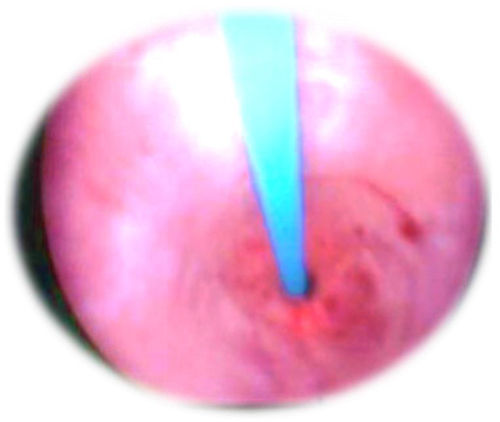 |
Figure 4 Ho: YAG laser incision of the stenotic lesion using the antegrade ureteroscope. |
 |
Figure 5 Guidewire was passed from antegrade ureteroscopy (A and B). Illumination of the obstruction by the retrograde approach (C). |
 |
Figure 6 Stenotic area post laser endoureterotomy and ureteral dilatation. |
Results
The whole operating time was 200 mins. No changes in the patient’s temperature were recorded during the intervention. No blood loss. No fever or signs of UTI were seen shortly after the operation. The post-operative lab tests were normal and the Foley catheter was successfully removed at day one post-op. The hospital stay was short of only 2 days.
The ureteric stent was removed 6 weeks later with no subsequent pain or complications. A follow up abdominopelvic CT scan was performed 4 weeks after the DJ stent removal revealing a stone free right kidney and ureter and showing an excellent contrast dye excretion and passage in the repaired ureteral zone with no evidence of ureteral narrowing.
Discussion
Ureteroscopic treatment of ureteric stones is now considered to be safe with high success rates owing to the enhancements in ureteroscopes along with improvements in intracorporeal lithotripsy devices.7 The rate of ureteroscopy complications have declined to <2% with postoperative ureteric stricture accounting for only <0.5% in recent series.8
Inflammation, collagen deposition and fibrosis are frequently seen on histological examination of tissue from a ureteral stricture, a finding that strongly corroborates with the predisposing factors for late stricture formation. Direct ureteric injury is paramount as it causes mucosal ischaemia from prolonged manipulation, resulting in fibrinous exudates formation on the traumatized wall. Another important risk factor is peri-ureteric fibrosis by dint of extravasation after perforation, especially in the setting of infection.9
The key element of an efficacious treatment is a timely diagnosis and early intervention to avoid obstructive complications. Owing to the tremendous improvement in endoscopy, the less-invasive endoureterotomy is considered nowadays as a crucial option in the urologists’ arsenal in the treatment of post-ureteroscopy ureteral strictures and is now swapping older invasive interventions. Several modalities can be used, ranging from cutting devices (including laser fiber, electrocautery or cold knif) under direct ureteroscopic vision to cutting balloon catheter using fluoroscopic guidance with favourable outcomes regardless of the method used.10 However, Holmium laser is considered to be the ideal choice inasmuch as it is compatible with the flexible endoscope, it has haemostatic effect and it is easily procurable.10 The endoureterotomy incision should be always full thickness, done from the ureteral lumen out to the periureteral fat and include 2–3 mm of normal tissue proximally and distally. In our case, we started with a small laser ureteral incision and then we proceeded with ureteral dilatation to finish with a full thickness incision as such to circumvent any damage to nearby structures. As a general rule, upper ureteral strictures are incised posterolaterally while distal ureteral strictures are incised along the anteromedial wall to avoid damage of nearby vessel injury.10
We decided to use the Ho:YAG laser fiber as it was shown that its use during endoureterotomy led to 53% to 88% success rate. Gnessin et al reported in a series of 35 patients with benign ureteral stricture who underwent laser endoureterotomy, that 82% of patients were symptom free and 79% had no radiological evidence of obstruction.11
Razdan et al described that non-ischaemic strictures and stricture lengths less than 1 cm have higher success rates and that a stricture length over 2 cm is considered as a significant predictor of treatment failure.12 Several series have recommended a combined approach for strictures less than 2 cm after demonstrating successful outcomes with using the combined technique for complete ureteral obstruction.13–15 Hence, contrast pyelography is useful for evaluating whether endoureterotomy can be performed.16 Under direct vision and using fluoroscopic guidance, the chief step is to pass a guidewire from one of the lumens, through and through to the other lumen. As we already stated in our surgical technique, the cutting is made at one end and guided towards the light source from the ureteroscope on the opposite end of the stricture.17 This is known as the “cut-to-the-light” technique that was first reported by Bagley in 1985 in a case of complete renal pelvis-ureteral junction obstruction after pyelolithotomy.18
We finished the procedure by placing a ureteral double J stent because we believe that ureteral stent placement after endoureterotomy is a routine practice, the goal of which is to mainly prevent extraureteral leakage of urine, thus facilitating ureteral healing, but also to prevent ureteral stricture recurrence. The cause of the latter is mainly an ischemic event of the ureter around the stent.16 However, there are still some controversies about the stent size and number. Comparing the efficacy and safety of double versus single ureteral stent placement after laser endoureterotomy, Hamdy et al found that, in the case of benign ureteral strictures of more than 1.5 cm, a higher success rate was achieved with double stent placement of the ureter after laser endoureterotomy in comparison to single stent placement.19 This finding corroborates with Isogai et al who also found a benefit with tandem stenting. Nevertheless, the mechanism is still poorly understood and further studies are needed to elucidate the usefulness of this technique.20
With a success rate averaging 55–85%, endoscopic treatments are often used as first-line interventions in patients with a short (<2 cm), complex stricture or obliterated ureter and with a renal function of >20%.21,22 To note that other invasive techniques are now being deployed according to stringent patient selection criteria with long, complex strictures previously radiated or operated on, among others the buccal mucosa graft ureteroplasty and robotic assisted corrections.23,24
Scarce information is provided in the literature regarding the long term monitoring of ureteral stricture treatment. We should note that most stricture recurrences are identified within the first year after surgery. Two to four weeks after stent removal, early follow-up imaging studies, including renal ultrasonography, IVP, or renal scintigraphy can be done. This can be delayed by up to 3 months if the patient is asymptomatic, and then imaging is repeated at 6-month intervals for the first 2 years.25
Finally, we believe that this case proves once again the efficacy of the “cut-to-the-light” technique in treating ureteral strictures and seems to offer excellent outcomes. However, this is only a case-report; therefore, studies with larger samples and longer follow ups are needed as well as comparative studies with other traditional techniques in order to fully determine the benefits of this method and to assess and reveal its suitable application and its drawbacks.
Ethics
Written informed consent has been provided by the patient to have the case details and any accompanying images published. Institutional approval was not required to publish the case details.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Darwish AE, Gadelmoula MM, Abdelkawi IF, Abdellatif AM, Abdel-Moneim AM, Hammouda HM. Ureteral stricture after ureteroscopy for stones: a prospective study for the incidence and risk factors. Urol Ann. 2019;11(3):276–281. doi:10.4103/UA.UA_110_18
2. Prezioso D, Illiano E, Piccinocchi G, et al. Urolithiasis in Italy: an epidemiological study. Arch Ital Urol Androl. 2014;86:99–102. doi:10.1016/j.eucr.2022.102036
3. Marchini GS, Vicentini FC, Mazzucchi E, Brito A, Ebaid G, Srougi M. Silent ureteral stones: impact on kidney function–can treatment of silent ureteral stones preserve kidney function? Urology. 2012;79(2):304–308. doi:10.1016/j.urology.2011.07.1436
4. Elashry OM, Elgamasy AK, Sabaa MA, et al. Ureteroscopic management of lower ureteric calculi: a 15-year single-centre experience. BJU Int. 2008;102:1010–1017. doi:10.1111/j.1464-410X.2008.07747.x
5. Wimpissinger F, Springer C, Kurtaran A, Stackl W, Türk C. Functional aspects of silent ureteral stones investigated with MAG-3 renal scintigraphy. BMC Urol. 2014;14:3. doi:10.1186/1471-2490-14-3
6. Vasudevan VP, Johnson EU, Wong K, et al. Contemporary management of ureteral strictures. J Clin Urol. 2019;12(1):20–31. doi:10.1177/2051415818772218
7. Chow GK, Patterson DE, Blute ML, Segura JW. Ureteroscopy: effect of technology and technique on clinical practice. J Urol. 2003;170(1):99–102. doi:10.1097/01.ju.0000070883.44091.24
8. Schuster TG, Hollenbeck BK, Faerber GJ, Wolf JS
9. El-Abd AS, Suliman MG, Abo Farha MO, et al. The development of ureteric strictures after ureteroscopic treatment for ureteric calculi: a long-term study at two academic centres. Arab J Urol. 2014;12(2):168–172. doi:10.1016/j.aju.2013.11.004
10. Singal RK, Denstedt JD, Razvi HA, Chun SS. Holmium:YAGlaser endoureterotomy for treatment of ureteral stricture. Urology. 1997;50(6):875–880. doi:10.1016/S0090-4295(97)00511-6
11. Gnessin E, Yossepowitch O, Holland R, PM Livne, Lifshitz DA. Holmium laser endoureterotomy for benign ureteral stricture: a single center experience. J Urol. 2009;182(6):2775–2779. doi:10.1016/j.juro.2009.08.051
12. Razdan S, Silberstein IK, Bagley DH. Ureteroscopic endoureterotomy. BJU Int. 2005;95(Suppl 2):94–101. doi:10.1111/j.1464-410X.2005.05207.x
13. Conlin MJ, Gomella LG, Bagley DH. Endoscopic ureteroureterostomy for obliterated ureteral segments. J Urol. 1996;156(4):1394–1399. doi:10.1016/S0022-5347(01)65598-8
14. Lingeman JE, Wong MY, Newmark JR. Endoscopic management of total ureteral occlusion and ureterovaginal fistula. J Endourol. 1995;9(5):391–396. doi:10.1089/end.1995.9.391
15. Macrì A, Magno C, Certo A, et al. Combined antegrade and retrograde ureteral stenting: the rendezvous technique. Clin Radiol. 2005;60(2):257–260. doi:10.1016/j.crad.2004.06.008
16. Shiozaki K, Izaki H, Fukuta K, Fukawa T, Takahashi M, Kanayama H. Laser endoureterotomy with cut-to-the-light technique for complete ureteral obstruction - A case report. Urol Case Rep. 2022;42:102036. doi:10.1016/j.eucr.2022.102036
17. Knowles DR, Staiman VR, Gupta M. Long-term results of the treatment of complete distal ureteral stenosis using a cutting balloon catheter device. J Urol. 2001;166:2087. doi:10.1016/S0022-5347(05)65511-5
18. Bagley DH, Huffman J, Lyon E, McNamara T. Endoscopic ureteropyelostomy: opening the obliterated ureteropelvic junction with nephroscopy and flexible ureteropyeloscopy. J Urol. 1985;133(3):462–464. doi:10.1016/s0022-5347(17)49026-4
19. Ibrahim HM, Mohyelden K, Abdel-Bary A, Al-Kandari AM. Single versus double ureteral stent placement after laser endoureterotomy for the management of benign ureteral strictures: a randomized clinical trial. J Endourol. 2015;29(10):1204–1209. doi:10.1089/end.2015.0445
20. Isogai M, Hamamoto S, Hasebe K, et al. Dual ureteral stent placement after redo laser endoureterotomy to manage persistent ureteral stricture. IJU Case Rep. 2020;3(3):93–95. doi:10.1002/iju5.12152
21. Meretyk S, Albala DM, Clayman RV, Denstedt JD, Kavoussi LR. Endoureterotomy for treatment of ureteral strictures. J Urol. 1992;147(6):1502–1506. doi:10.1016/s0022-5347(17)37608-5
22. Partin AW, Wein AJ, Kavoussi LR, et al. Campbell-Walsh Urology. Amsterdam, Netherlands: Elsevier Inc; 2016:1149–1154.
23. Gonzalez AN, Mishra K, Zhao LC. Buccal mucosal ureteroplasty for the management of ureteral strictures: patient selection and considerations. Res Rep Urol. 2022;14:135–140. doi:10.2147/RRU.S291950
24. Masieri L, Sforza S, Di Maida F, et al. Robotic correction of iatrogenic ureteral stricture: preliminary experience from a tertiary referral centre. Scand J Urol. 2019;53(5):356–360. doi:10.1080/21681805.2019.1651390
25. Lucas JW, Ghiraldi E, Ellis J, Friedlander JI. Endoscopic management of ureteral strictures: an update. Curr Urol Rep. 2018;19(4):24. doi:10.1007/s11934-018-0773-4
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.