Back to Journals » Clinical Epidemiology » Volume 9
The criterion validity of the web-based Major Depression Inventory when used on clinical suspicion of depression in primary care
Authors Nielsen MG, Ørnbøl E, Bech P, Vestergaard M, Christensen KS ![]()
Received 21 January 2017
Accepted for publication 16 March 2017
Published 6 July 2017 Volume 2017:9 Pages 355—365
DOI https://doi.org/10.2147/CLEP.S132913
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Irene Petersen
Marie Germund Nielsen,1 Eva Ørnbøl,2 Per Bech,3 Mogens Vestergaard,1,4 Kaj Sparle Christensen1
1Research Unit for General Practice, Department of Public Health, Aarhus University, 2Research Clinic for Functional Disorders and Psychosomatics, Aarhus University Hospital, Aarhus, 3Psychiatric Research Unit, Psychiatric Centre North Zealand, University Hospital of Copenhagen, Hillerød, 4Section for General Medical Practice, Department of Public Health, Aarhus University, Aarhus, Denmark
Background: The Major Depression Inventory (MDI) is widely used in Danish general practice as a screening tool to assess depression in symptomatic patients. Nevertheless, no validation studies of the MDI have been performed. The aim of this study was to validate the web-based version of the MDI against a fully structured telephone interview in a population selected on clinical suspicion of depression (ie, presence of two or three core symptoms of depression) in general practice.
Materials and methods: General practitioners (GPs) invited consecutive persons suspected of depression to complete the web-based MDI in a primary care setting. The validation was based on the Munich-Composite International Diagnostic Interview (M-CIDI) by phone. GPs in the 22 practices in our study included 132 persons suspected of depression. Depression was rated as yes/no according to the MDI and M-CIDI. Sensitivity, specificity, and positive predictive value of the International Classification of Diseases, Tenth Revision (ICD-10) algorithms of the MDI were examined.
Results: According to the M-CIDI interview, 87.9% of the included population was depressed and 64.4% was severely depressed. According to the MDI scale, 59.1% of the population was depressed and 31.8% was severely depressed. The sensitivity of the MDI for depression was 62.1% (95% confidence interval [95% CI]: 52.6–70.9) and the specificity was 62.5% (95% CI: 35.4–84.8). The sensitivity for severe depression was 42.2% (95% CI: 30.6–52.4) and the specificity was 85.1% (95% CI: 71.7–93.8). The receiver operating curve showed an area under the curve of 0.66 (95% CI: 0.52–0.81) for any depression and of 0.72 (95% CI: 0.63–0.81) for severe depression.
Conclusion: The MDI is a conservative instrument for diagnosing ICD-10 depression in a clinical setting compared to the M-CIDI interview. Only a few false-positive diagnoses were identified when the MDI was used on clinical suspicion of depression.
Keywords: Major Depression Inventory, depression, criterion validity, M-CIDI interview, diagnosing
Plain language summary
Why was the study done? Depression is a common mood disorder. The Major Depression Inventory (MDI) is widely used in Danish general practice to measure depression in symptomatic patients. Nevertheless, no studies assessing the validity of the MDI have been performed in this setting.
What did the researchers do? This study is the first to investigate the clinical validity of the MDI for diagnosing depression in a population selected on clinical suspicion of depression (ie, presence of two or three core symptoms of depression) in general practice and to validate it against a structural clinical interview.
What did the researchers find? Findings show that the MDI tends to underdiagnose depression according to the International Classification of Diseases, Tenth Revision (ICD-10) criteria compared to the Munich-Composite International Diagnostic Interview (M-CIDI) interview. Only few false-positive diagnoses of depression were recorded when the MDI was used on clinical suspicion of depression.
What do these results mean? The MDI is found to be a valid, although conservative, instrument for diagnosing depression on clinical suspicion in general practice. The results show that the use of MDI on clinical suspicion of depression can help to avoid overdiagnosis and overtreatment of depressive disorders.
Introduction
Mental disorders often remain unrecognized and misidentified worldwide.1 Approximately 9% of all contacts in general practice are related to mental disorders,2–4 and depression is the most frequently encountered mental health problem.5 Mitchell et al assessed an accurate diagnosis through a meta-analysis of 19 studies of routines and instruments of rule-in and rule-out of depression in general practice and found a weighted diagnostic sensitivity (SE) of 50.1% (95% confidence interval [95% CI]: 41.3–59.0%) in a primary care waiting-room population. This suggests that only half of the truly depressed are diagnosed. The positive predictive value (PPV) of 42% (95% CI: 39.6–44.3%) indicates that less than half of the diagnosed persons will actually have the true depression diagnosis.6
An accurate diagnosis is a prerequisite for appropriate treatment. Most diagnostic instruments used in primary care are validated against a waiting-room population. However, in daily clinical practice, case finding is based on the general practitioner’s (GP) suspicion of a psychiatric disorder.7 A systematic review by Thombs et al8 concluded that most studies of screening tools for depression are biased as they rarely exclude persons who already have a diagnosis of depression or receive treatment for depression or anxiety. In a cross-sectional study, Christensen et al found that only 5% more cases were identified through routine screening for depression compared with a broad case-finding strategy. In addition, the GPs’ diagnoses for depression were validated with the Major Depression Inventory (MDI), and the GPs almost make the same diagnosis as the MDI, and hence they trust the MDI.9 Therefore, case-finding instruments should be validated in a sample of consecutive persons suspected of depression by their GP to better reflect the population in which the instruments are used. Gilbody et al10 stated that the main downside of screening instruments is their low predictive value, especially when considering the relatively low prevalence of depression in primary care populations.
Danish clinical guidelines11 recommend using the MDI on clinical suspicion of depression (ie, presence of two or three core symptoms of depression according to the ICD-10) (Figure S1). The MDI was originally developed as part of a World Health Organization (WHO) project in the primary care setting12 and is compatible with both the ICD-10 and the Diagnostic and Statistical Manual of Mental Disorders, 4th ed (DSM-IV) classification systems. Application of psychometric instruments is increasing in Denmark (Figure S2), and GPs are reimbursed for using the tests.13,14
The psychometric properties of the MDI have been explored and discussed in several studies. Amris et al15 found that the MDI demonstrated insufficient psychometric properties when used to identify and assess the severity of depression in a clinical sample of females with chronic widespread pain, but no study has so far determined the efficiency of the MDI in a sample from a primary care setting. The MDI has been validated against the Present State Examination (PSE) in a sample of 43 subjects with a spectrum of depressive symptoms in a psychiatric department. The sensitivity of the MDI for moderate to severe depression was found to be 86%, whereas the specificity was found to be 86%.12 In a study by Cuijpers et al16 investigating the presence of major depressive disorder in a consecutive sample of 258 psychiatric outpatients, the sensitivity of the MDI was reported to be 66%, whereas the specificity was reported to be 65% when based on the paper version with 12 items compared to assessment by a psychiatrist. In a population-based study by Forsell17 investigating the association between the MDI and the Schedules for Clinical Assessment in Neuropsychiatry (SCAN) interview, a sensitivity of 0.51 and a specificity of 0.44 were found for all depressive disorders.
We aimed to validate a web-based version of the MDI in a sample selected on clinical suspicion of depression (ie, presence of two or three core symptoms of depression) by the GP compared to the structured clinical Munich-Composite International Diagnostic Interview (M-CIDI) by telephone.
Materials and methods
Development of online resource
We developed the webpage Sundhedsmappen.dk (in Danish) to collect web-based versions of the MDI from Danish general practices. The site is an online system intended to support diagnosis and monitoring of depression, anxiety, and blood pressure.14
Recruitment process
We included 22 general practices in the study. The GPs were recruited through invitations sent by mail to 700 practices, newsfeeds, network practices, and conference presentation. GPs showing interest in participating received a visit from the project leader, who gave detailed information about the study. GP reminders were sent by surface mail. The GPs were contacted by phone if they did not recruit any persons for the study.
On clinical suspicion of depression, the GP asked consecutive persons to complete the web-based version of the MDI at Sundhedsmappen.dk on a tablet PC or desktop computer in the practice. The data were then securely saved at our database. Due to the web-based data collection, completeness of the MDI tests was secured. The GP handed out an information brochure about the study to persons who had signed up. In total, 132 consecutive persons were recruited through GPs. Within two weeks after entering the study, the person was interviewed by phone by a certified (M-CIDI) interviewer.
The following inclusion criteria were applied: persons suspected of depression by the GP, aged 18 years or older, understanding written and spoken Danish, and giving oral informed consent at the start of the telephone interview.
The GPs received DKK 122.57 (≈EUR 16.50) per included person.
Depression measures
The study consisted of two depression measures; the MDI instrument and the psychiatric telephone interview M-CIDI, which is the reference standard in the study.
Major Depression Inventory
The MDI can be used in two ways: 1) as a diagnostic instrument and 2) as a severity scale of depression. The MDI applied as a diagnostic instrument is the primary focus of the analysis conducted in our study, whereas the MDI score is a secondary focus.
As a diagnostic instrument, the MDI covers both the DSM-IV and the ICD-10 coding system for depression. The ICD-10 algorithm is coded as mild depression (at least two core symptoms + two associated symptoms), moderate depression (at least two core symptoms + four associated symptoms), or severe depression (at least three core symptoms + five associated symptoms).12,18 The core items are indicated by items 1–3. The associated symptoms are indicated by items 4–10. A core symptom is present if the score for this symptom is at least 4, and an associated symptom is present if the score is at least 3.
The severity of depression is measured over the last 2 weeks in the form of a Likert scale at which the frequency of each symptom can be indicated from 0 (at no time) to 5 (all the time). The MDI has a severity rating score of 0–50. According to the MDI manual, the cut points for the total score of the MDI are no depression (≤19), mild depression (20–24), moderate depression (25–29), and severe depression (≥30).
The item concerning sleep problems, item 9, was split into two items in our study. These two items focus on the amount of sleep (too little or too much). The item with the highest response score is used in the total MDI score. Eating and at the same time sleeping too much are not typical signs of depression. Therefore, it is important to distinguish between too little and too much sleep. Studies suggest that up to 30% of the patients who are treated in primary care have atypical depression.19,20
Munich-Composite International Diagnostic Interview
The M-CIDI telephone interview was used as a reference standard to measure the prevalence of ICD-10 depression. The M-CIDI is a comprehensive, fully structured standardized diagnostic computer-assisted interview designed for trained certified lay interviewers for assessment of mental disorders according to the ICD-10 and DSM-IV criteria.21 The M-CIDI was developed by the WHO and is intended for both clinical and research purposes, which was the rationale for using this reference standard. Compared to the standard WHO-CIDI (version 1.2), the M-CIDI allows for an evaluation of additional DSM-IV diagnoses.22,23 We used a Norwegian version of the computerized M-CIDI.24
The interviewers in our study were M-CIDI certified and blinded to the individual’s MDI score. Five different interviewers performed the interviews; each interviewer conducted 64, 15, 35, 35, and 27 interviews, respectively. All interviewers were recertified and supervised by the project leader. Information about the M-CIDI results was not available for the participating GPs.
The anxiety diagnoses (n=8) from the M-CIDI were handled as “no depression” diagnoses.
For 17 persons, the M-CIDI generated the ICD-10 diagnosis F06.32, which is an organic depressive episode. These 17 persons were recoded according to their individual degree of core symptoms and accompanying symptoms by reviewing their responses to the M-CIDI interview. If a person had a depression diagnosis according to the ICD-10 algorithm, such person was categorized as having a present depression.
Statistical analysis and sample size
In our sample size calculation before performing our study using the GP’s clinical suspicion, we expected to find a prevalence of depression of 50%.9 We needed 60 depressed persons to complete the MDI scale to ensure that the total width of the 95% CI was no >0.20 around a sensitivity proportion of 0.80. By including 150 MDI-tested persons for interview, we expected to find around 75 depressed persons.
Prevalence, sensitivity, specificity, PPV, and negative predictive value (NPV) of the ICD-10 algorithms were examined for the MDI. Additionally, the criterion validation procedure included receiver operating curve (ROC) statistics for the MDI sum score.
Ethical approval
No written informed consent was required from participants for this study. Only oral information was necessary, and no ethical permission was required according to Danish law. Permission to conduct the study was granted by the Danish Committee of Multipractice Studies in General Practice and by the Danish Data Protection Agency, ID number: 2013-41-1756.
Results
Between 14 August 2013 and 19 February 2016, 22 Danish general practices recruited 246 persons assessed to be eligible for inclusion. In 2013, we had managed to recruit 28 patients; 146 in 2014, 63 in 2015, and 9 in 2016. To ensure an appropriate sample size, we decided to keep including until we reached a sufficient number of patients. The enrollment of patients in the study is shown as a flow chart in Figure 1. Even though the patients had agreed to participate at the consultation with their GP, 56 persons did not answer their phone when we called to perform the interview. Each person received a call for up to five times at different hours during daytime and evening; 31 persons declined to participate in the interview when asked on the phone.
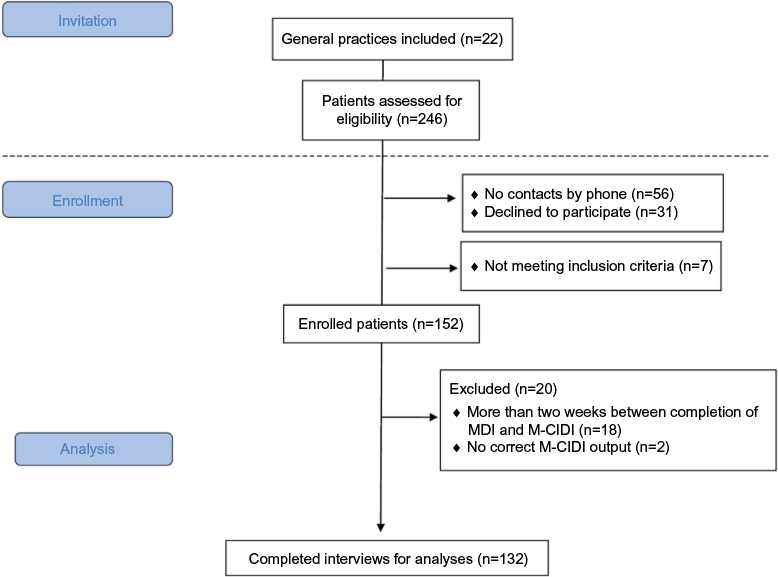 | Figure 1 Flow chart illustrating the inclusion of persons in the study. Abbreviations: M-CIDI, Munich-Composite International Diagnostic Interview; MDI, Major Depression Inventory. |
Table 1 compares the demographic and MDI-related characteristics of persons who completed both the MDI and the M-CIDI versus those who did not complete an M-CIDI. In total, 18 persons were excluded from the analysis due to the time-frame of a maximum of two weeks, between filling in the MDI and answering the M-CIDI interview. For these 18 patients the mean age (SD) was 39.3 (14.3), the mean MDI sum score (SD) was 27.7 (7.9) and the distribution of gender was 11 females (61.1%) and 7 males (38.9%).
 | Table 1 Response analysis Abbreviations: M-CIDI, Munich-Composite International Diagnostic Interview; SD, standard deviation; MDI, Major Depression Inventory. |
Person characteristics
Of the 132 interviewed persons, 116 (87.9%) were diagnosed with depression according to the M-CIDI interview; 16 (12.1%) had no depression, 8 (6%) had a mild depression, 23 (17.4%) had a moderate depression, and 85 (64.4%) had a severe depression.
According to the MDI ICD-10 algorithm, 54 (40.9%) had no depression, 14 (9.9%) had a mild depression, 22 (17.4%) had a moderate depression, and 42 (31.8%) had a severe depression. According to the MDI score, 20 (15%) had no depression (≤19), 18 (13.7%) had a mild depression (20–24), 24 (18.2%) had a moderate depression (25–29), and 70 (53%) had a severe depression (≥30).
A Venn diagram was used to illustrate the overlap between the depression diagnosis according to the M-CIDI, MDI ICD-10, and MDI sum scores for any depression and severe depression (Figures 2 and 3).
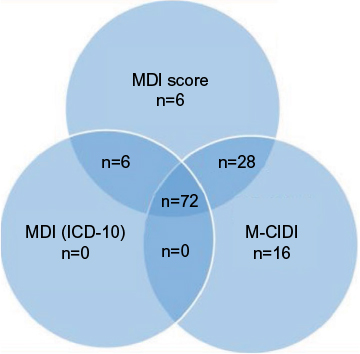 | Figure 2 Venn diagram for any depression according to the M-CIDI interview, MDI sum score, and the MDI ICD-10 algorithm. Note: Not identified, n=4. Abbreviations: M-CIDI, Munich-Composite International Diagnostic Interview; MDI, Major Depression Inventory; ICD-10, International Classification of Diseases, Tenth Revision. |
 | Figure 3 Venn diagram for severe depression according to the M-CIDI interview, MDI sum score, and the MDI ICD-10 algorithm. Note: Not identified, n=32. Abbreviations: M-CIDI, Munich-Composite International Diagnostic Interview; MDI, Major Depression Inventory; ICD-10, International Classification of Diseases, Tenth Revision. |
Table 2 presents the demographic and MDI-related characteristics of persons who completed the M-CIDI interview. As we initially expected the severity of depression determined the likelihood of holding a job; 60.9% of the moderately depressed were currently holding a job whereas only 48.2% of the severely depressed were currently holding a job.
 | Table 2 Person characteristics Abbreviations: M-CIDI, Munich-Composite International Diagnostic Interview; SD, standard deviation; MDI, Major Depression Inventory. |
Criterion validity
Table 3 shows the sensitivity, specificity, PPVs, and NPVs of the MDI. When we used the ICD-10 algorithm of the MDI to diagnose any depression, the sensitivity was 62.1% (95% CI: 52.6–70.9), the specificity was 62.5% (95% CI: 35.4–84.8), the PPV was 92.3% (95% CI: 84.0–97.1), and the NPV was 18.5% (95% CI: 9.3–31.4) (See Table S1, S2 and S3 for 2×2 tables for any, mild and moderate depression).
 | Table 3 Criterion validity and diagnostic criteria for MDI ICD-10 algorithm (N=132) Abbreviations: MDI, Major Depression Inventory; M-CIDI, Munich-Composite International Diagnostic Interview; CI, confidence interval; ICD-10, International Classification of Diseases, Tenth Revision. |
When we used the ICD-10 algorithm of the MDI to diagnose severe depression, the sensitivity was associated with the ICD-10 severe depression diagnosis after M-CIDI; the sensitivity was 41.2% (95% CI: 30.6–52.4), the specificity was 85.1% (95% CI: 71.7–93.8) , the PPV was 83.3% (95% CI: 68.6–93.0), and the NPV was 44.4% (95% CI: 34.0–55.3) (See Table S4 for 2×2 table for severe depression).
The sensitivity and specificity for the MDI sum scores were plotted along with the ROC (Figures 4 and 5). The area under the ROC curve for the MDI sum score is 0.66 (95% CI: 0.52–0.81) for any depression and 0.72 (95% CI: 0.63–0.81) for severe depression.
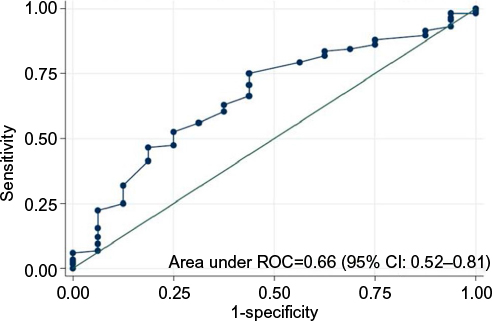 | Figure 4 The ROC for the MDI total score when associated with the M-CIDI diagnosis for any depression. Abbreviations: ROC, receiver operating curve; MDI, Major Depression Inventory; M-CIDI, Munich-Composite International Diagnostic Interview; CI, confidence interval. |
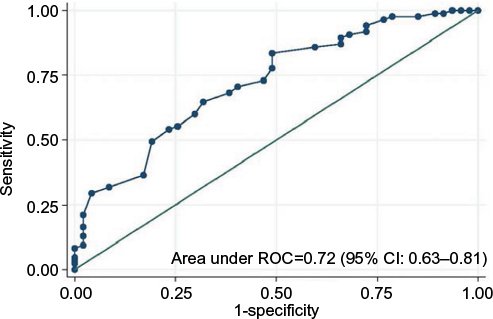 | Figure 5 The ROC for the MDI total score when associated with the M-CIDI diagnosis for severe depression. Abbreviations: ROC, receiver operating curve; MDI, Major Depression Inventory; M-CIDI, Munich-Composite International Diagnostic Interview; CI, confidence interval. |
In order to investigate the impact of recoding the 17 persons with F06.32 diagnoses, we performed a sensitivity analysis while excluding the 17 persons who were recoded in our study. These analyses showed no substantial changes in our results in Table 3 (results are not presented but are available from the author upon request).
Discussion
Statement of principal findings
We examined the web-based MDI depression scale administered on clinical suspicion of depression by the GP (ie, presence of two or three core symptoms of depression). To our knowledge, this study is the first to investigate the clinical validity of the MDI for diagnosing depression on clinical suspicion in a primary care setting.
The prevalence of depression is high in our study sample consisting of patients suspected of depression by their GP (ie, presence of two or three core symptoms of depression): 87.9% for any depression and 64.4% for severe depression. The MDI demonstrated a sensitivity of 62% for any depression, corresponding to a false-negative rate of 38%. The MDI demonstrated a low sensitivity of 41% for severe depression, corresponding to a false-negative rate of 59%. However, our findings of a low sensitivity in the MDI could be related to the M-CIDI interview being too sensitive.
The MDI demonstrated a modest specificity of 62% for any depression, corresponding to a false-positive rate of 38%. The specificity of the MDI test was relatively high (85%) for severe depression, corresponding to a false-positive rate of only 15%.
Strengths and limitations of the study
Our study was based on data from patients enrolled on clinical suspicion of depression (ie, presence of two or three core symptoms of depression). The MDI has now been tested in the GP’s daily practice in the clinic, which is a strength of our study. Furthermore, the M-CIDI worked well as a telephone interview with persons from the daily clinical practice after use of the MDI. It would have been a comprehensive logistic task if the participants in our study should have been interviewed face to face and not by telephone.
Another strength of our study was the relatively large sample size and the completeness of our data due to the web-based data collection (eg, no missing values for any items).
Our study reflects a fair presentation of the use of the MDI in daily clinical practice, even though the GPs might have oversampled persons with a known depression in our study. We expected a prevalence of depression of 50% in our study population, but the identified prevalence for any depression was 87.9%. Ideally, the included persons should be untreated for depression. However, we do not have any information regarding the respondents’ use of medication, which is a limitation of our study. There is a risk that GPs in our study might have used the MDI on patients already diagnosed with a depression, even though they were primed to use the MDI on clinical suspicion. In Denmark, GPs are recommended to retest the patient again after two weeks using the MDI before they start up any treatment.25 In our study, there is a time interval of about two weeks between the MDI test and the M-CIDI interview, which means that the patient probably has not started any treatment since the MDI test was performed.
Comparison with other studies
A previous study by Li et al26 found a higher prevalence of depression according to the PHQ-8 when using computer-assisted telephone interviewing compared to using computer-assisted personal interviewing.
Using a telephone interview for research focusing on depression has formerly been found a proper and valid method.27 The M-CIDI seems acceptable for the respondents and is efficient considering the required time and the ease of administration. Additionally, it seems to obtain at least as good agreement coefficients for symptoms and DSM-IV disorders as those obtained with the standard WHO-CIDI.23
In a study by Jordanova et al among primary care attendees, the CIDI was found to be a highly valid assessment of common mental disorders compared to the SCAN interview, although the CIDI tended to overdiagnose with a prevalence of 18.1% compared with 7.6% for the SCAN for any depressive episode or disorder.28 In a study by Brugha et al, the concordance between the SCAN interview and the CIDI interview ranged between “poor” and “fair” across almost all types of studied disorders and for comorbidity. Brugha et al22 stated that a consistent pattern of false positives was seen for all CIDI diagnoses when set against the SCAN calibration data.
A point for discussion in our study is that the M-CIDI interview might tend to be too sensitive when diagnosing depression, which could have affected our results demonstrating a false low sensitivity of the MDI because it identifies too few cases of depression according to the M-CIDI interview. In a study by Andrews et al,23 the interrater reliability of the CIDI was found to be perfect (overall intraclass kappa=1.0), whereas the SCAN obtained good overall reliability (intraclass kappa=0.67), which supports our choice of using the M-CIDI in our study. But in a study by Burgha et al,22 the kappa coefficient for any depression between CIDI and SCAN was 0.39.
Comparing our results with the findings reported in the meta-analysis by Mitchell et al, we learned that the use of the MDI tends to induce less false-positive depression diagnoses in general practice than if the GP would have to diagnose depression unassisted as in the study by Mitchell et al.6
The MDI has been validated against the PSE in a sample of 43 subjects with a spectrum of depressive symptoms in a psychiatric department; in the study by Bech et al,12 the sensitivity of the MDI algorithms for major depression varied between 86% and 92%, whereas the specificity varied between 82% and 86%. These findings differ from our results as they suggest a higher sensitivity of the MDI; this is possibly because their study was performed with a SCAN interview.
Our findings are in line with the findings by Cuijpers et al,16 who reported on the presence of major depressive disorder based on the MDI (with a sensitivity of 66% and a specificity of 65%) in consecutive persons in a psychiatric outpatient clinic.
In the literature, no studies have tested the MDI in a population in the primary care setting. In the study by Cuijpers et al, the population is similar as it is a highly prevalent population even though their study was based on a psychiatric outpatient population. The area under the curve (AUC) reported in the study by Cuijpers et al16 of 0.68 was similar to our study of 0.66. In the Danish media, an issue of great debate has been whether GPs in Denmark diagnose too many healthy people (nondepressed) with a depression diagnose as a consequence of the GPs use of the MDI. The discussion has focused on, whether transient stress or adjustment disorders are diagnosed as depression.29 As our results have shown that the MDI is a conservative instrument with a low false-positive rate, we find it important to elaborate on these findings in this high prevalence sample. Most tests have issues relating to categorization; healthy persons may be categorized as ill or ill persons may be categorized as healthy. Both scenarios are problematic, but the impact of these two different types of errors depends on many things. The consequences for healthy person receiving treatment and the consequences for ill person not receiving treatment are different and have different impact on, eg, society, but the prevalence is also of great importance.
Conclusion
The MDI is found to be a conservative instrument for diagnosing depression according to the ICD-10 criteria. Our findings are encouraging as the MDI depression scale appears to be a reasonable valid tool for diagnosing depression on clinical suspicion (ie, presence of two or three core symptoms of depression). This is an important finding as depression is a common disorder that significantly contributes to the morbidity in many persons seen in general practice. In contrary to general concerns, the MDI does not seem to overdiagnose depression in general practice. The Venn diagram for severe depression illustrates that the MDI does not overdiagnose severe depression. This is important because severe depression is often treated for long periods with antidepressant medication and because public discussions have often focused on the risk of overdiagnosing depression when using MDI in general practice. However, it is essential to be aware that GPs might risk underdiagnosing depression if they only rely on the MDI.
Further research is required to cross-validate our findings of the MDI and to further examine if the MDI is sensitive to change. Future studies also need to address the structural validity of the MDI.
Acknowledgments
We gratefully acknowledge the persons and general practitioners who took the time to participate in our study. This work was supported by unrestricted grants from the Lundbeck Foundation (grant number: R155-2012-11280) and the Primary Health Care Research Foundation of the Central Denmark Region.
Disclosure
The authors report no conflicts of interest in this work.
References
OECD. Making Mental Health Count: The Social and Economic Costs of Neglecting Mental Health Care. Paris: Organisation for Economic Co-Operation and Development Publishing; 2014. | ||
Alonso J, Angermeyer MC, Bernert S, et al. Use of mental health services in Europe: results from the European Study of the Epidemiology of Mental Disorders (ESEMeD) project. Acta Psychiatr Scand Suppl. 2004;420:47–54. | ||
Christensen AI, Ekholm O, Davidsen M, Jue K. Sundhed og sygelighed i Danmark 2010 & udviklingen siden 1987 [Health and Sickness in Denmark 2010 and Development Since 1987]. University of Southern Denmark, Copenhagen: The Danish National Institute of Public Health (NIPH); 2012. | ||
Timonen M, Liukkonen T. Management of depression in adults. BMJ. 2008;336(7641):435–439. | ||
Üstün T, Sartorius N. Mental Illness in General Health Care, An International Study. Chichester, New York, Brisbane, Toronto, Singapore: John Wiley & Sons; 1995. | ||
Mitchell AJ, Vaze A, Rao S. Clinical diagnosis of depression in primary care: a meta-analysis. Lancet. 2009;374(9690):609–619. | ||
Ostergaard SD, Foldager L, Allgulander C, et al. Psychiatric caseness is a marker of major depressive episode in general practice. Scand J Prim Health Care. 2010;28(4):211–215. | ||
Thombs BD, Arthurs E, El-Baalbaki G, Meijer A, Ziegelstein RC, Steele RJ. Risk of bias from inclusion of patients who already have diagnosis of or are undergoing treatment for depression in diagnostic accuracy studies of screening tools for depression: systematic review. BMJ. 2011;343:d4825. | ||
Christensen KS, Sokolowski I, Olesen F. Case-finding and risk-group screening for depression in primary care. Scand J Prim Health Care. 2011;29(2):80–84. | ||
Gilbody S, Richards D, Brealey S, Hewitt C. Screening for depression in medical settings with the Patient Health Questionnaire (PHQ): a diagnostic meta-analysis. J Gen Intern Med. 2007;22(11):1596–1602. | ||
The Danish College of General Practitioners. Unipolar depression-diagnostik og behandling [Unipolar depression-diagnostics and treatment]. 2010;2(1). | ||
Bech P, Rasmussen NA, Olsen LR, Noerholm V, Abildgaard W. The sensitivity and specificity of the Major Depression Inventory, using the Present State Examination as the index of diagnostic validity. J Affect Disord. 2001;66(2–3):159–164. | ||
Danish Medical Association [Lægeforeningen] [webpage on the Internet]. Psychometric Tests [Psykometriske tests]. Available from: http://www.laeger.dk/portal/page/portal/LAEGERDK/Laegerdk/P_L_O/Praksis/Oftest%20stillede%20sp%C3%B8rgsm%C3%A5l%20om%20almen%20praksis/Psykometriske%20tests. Accessed September 1, 2017. | ||
Christensen KS, Mortensen M, Beyer H, Vedsted P, Vestergaard M. Sundhedsmappen.dk: Gå online med psykometriske tests [Health folder.dk: go online with psychometric tests]. Practicus. 2013;215:18. | ||
Amris K, Omerovic E, Danneskiold-Samsoe B, Bliddal H, Waehrens EE. The validity of self-rating depression scales in patients with chronic widespread pain: a Rasch analysis of the Major Depression Inventory. Scand J Rheumatol. 2016;45(3):236–246. | ||
Cuijpers P, Dekker J, Noteboom A, Smits N, Peen J. Sensitivity and specificity of the Major Depression Inventory in outpatients. BMC Psychiatry. 2007;7:39. | ||
Forsell Y. The Major Depression Inventory versus Schedules for Clinical Assessment in Neuropsychiatry in a population sample. Soc Psychiatry Psychiatr Epidemiol. 2005;40(3):209–213. | ||
Olsen LR, Jensen DV, Noerholm V, Martiny K, Bech P. The internal and external validity of the Major Depression Inventory in measuring severity of depressive states. Psychol Med. 2003;33(2):351–356. | ||
Asnis GM, McGinn LK, Sanderson WC. Atypical depression: clinical aspects and noradrenergic function. Am J Psychiatry. 1995;152(1):31–36. | ||
Henkel V, Mergl R, Allgaier A, Kohnen R, Möller H, Hegerl U. Treatment of depression with atypical features: a meta-analytic approach. Psychiatry Res. 2006;141(1):89–101. | ||
Wittchen HU, Lachner G, Wunderlich U, Pfister H. Test-retest reliability of the computerized DSM-IV version of the Munich-Composite International Diagnostic Interview (M-CIDI). Soc Psychiatry Psychiatr Epidemiol. 1998;33(11):568–578. | ||
Brugha TS, Jenkins R, Taub N, Meltzer H, Bebbington PE. A general population comparison of the Composite International Diagnostic Interview (CIDI) and the Schedules for Clinical Assessment in Neuropsychiatry (SCAN). Psychol Med. 2001;31(6):1001–1013. | ||
Andrews G, Peters L, Guzman AM, Bird K. A comparison of two structured diagnostic interviews: CIDI and SCAN. Aust N Z J Psychiatry. 1995;29(1):124–132. | ||
Wittchen H, Pfister H. DIA-X-Interviews (M-CIDI): Manual für Screening-Verfahren und Interview; Interviewheft Längsschnittuntersuchung (DIA-X-Lifetime); Ergänzungsheft (DIA-XLifetime); Interviewheft Querschnittuntersuchung (DIA-X 12 Monate); Ergänzungsheft (DIA-X 12 Monate) [DIA-X Interviews (M-CIDI): Manual for Screening Procedures and Interview; Interviewheft Longitudinal Section Analysis (DIA-X-Lifetime); Supplementary Booklet (DIA-XLifetime); Interviewheft Cross-Section Study (DIA-X 12 Months); Supplementary Booklet (DIA-X 12 months)]. Frankfurt: Swets & Zeitlinger; 1997. | ||
Sundhedsstyrrelsen [Danish Health Authority]. Faglige retningslinjer for henvisning til psykolog. For patienter med let til moderat depression eller let til moderat angst [Professionel guidelines for referral to a psychologist. For patients with mild to moderate depression or mild to moderate anxiety]. 2012;(1). | ||
Li C, Ford ES, Zhao G, Tsai J, Balluz LS. A comparison of depression prevalence estimates measured by the Patient Health Questionnaire with two administration modes: computer-assisted telephone interviewing versus computer-assisted personal interviewing. Int J Public Health. 2012;57(1):225–233. | ||
Muskens EMH, Lucassen P, Groenleer W, van Weel C, Voshaar RO, Speckens A. Psychiatric diagnosis by telephone: is it an opportunity? Soc Psychiatry Psychiatr Epidemiol. 2014;49(10):1677–1689. | ||
Jordanova V, Wickramesinghe C, Gerada C, Prince M. Validation of two survey diagnostic interviews among primary care attendees: a comparison of CIS-R and CIDI with SCAN ICD-10 diagnostic categories. Psychol Med. 2004;34(6):1013–1024. | ||
Danmarks Radio [Danish Broadcasting Corporation]. DR1 Dokumentar: De raske syge [Danish Broadcasting Coporation Documentary: The healthy ill]. [TV Documentary]. Copenhagen: Danish Broadcasting Corporation; 2016. |
Supplementary materials
 | Figure S1 Major Depression Inventory, all 10 items used in our study. Note: Reproduced from Bech P. Clinical psychometrics. Oxford: John Wiley and Sons; 2012. Copyright © 2012, John Wiley & Sons, Ltd.1 |
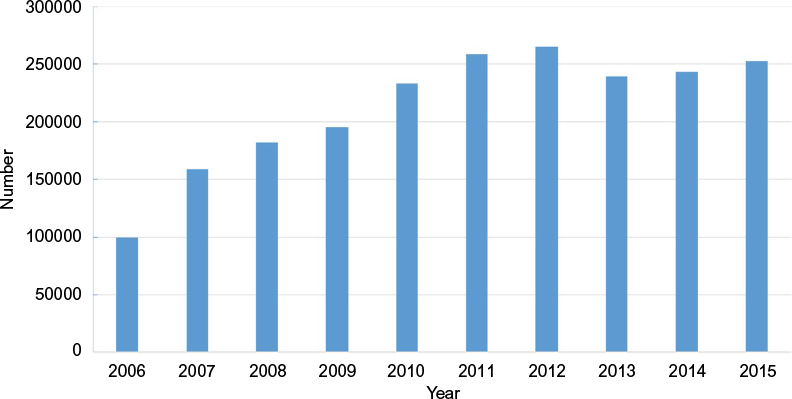 | Figure S2 GP use of psychometric tests in Denmark Abbreviation: GP, general practitioner. |
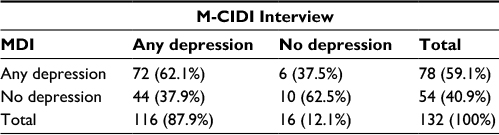 | Table S1 M-CIDI interviews and MDI ICD-10 diagnosis: any depression Abbreviation: ICD-10, International Classification of Diseases, Tenth Revision; M-CIDI, Munich-Composite International Diagnostic Interview; MDI, Major Depression Inventory. |
 | Table S2 M-CIDI interviews and MDI ICD-10 diagnosis: mild depression (moderate and severe depression were excluded) Abbreviation: ICD-10, International Classification of Diseases, Tenth Revision; M-CIDI, Munich-Composite International Diagnostic Interview; MDI, Major Depression Inventory. |
 | Table S3 M-CIDI interviews and MDI ICD-10 diagnosis: moderate depression (mild and severe depression were excluded) Abbreviation: ICD-10, International Classification of Diseases, Tenth Revision; M-CIDI, Munich-Composite International Diagnostic Interview; MDI, Major Depression Inventory. |
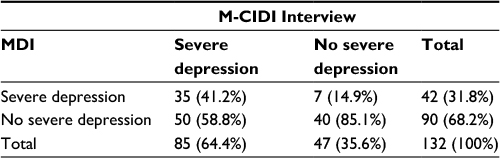 | Table S4 M-CIDI interviews and MDI ICD-10 diagnosis: severe depression (mild and moderate depression were included as no severe depression) Abbreviation: ICD-10, International Classification of Diseases, Tenth Revision; M-CIDI, Munich-Composite International Diagnostic Interview; MDI, Major Depression Inventory. |
References
Bech P. Clinical psychometrics. Oxford: John Wiley and Sons; 2012. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.