Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 13
The Correlation of Semmes–Weinstein Monofilament Test with the Level of P-75 Neurotrophin as Marker of Nerve Damage in Leprosy
Authors Widasmara D, Panjarwanto DA, Sananta P
Received 26 February 2020
Accepted for publication 12 May 2020
Published 15 June 2020 Volume 2020:13 Pages 399—404
DOI https://doi.org/10.2147/CCID.S251356
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Dhelya Widasmara,1 Dwi Andhika Panjarwanto,2 Panji Sananta3
1Department of Dermatology and Venereology, Faculty of Medicine, Universitas Brawijaya, Saiful Anwar Regional General Hospital, Malang, Indonesia; 2Medical Study Program, Faculty of Medicine, Universitas Brawijaya, Malang, Indonesia; 3Orthopaedic and Traumatology Department, Faculty of Medicine, Universitas Brawijaya, Saiful Anwar Regional General Hospital, Malang, Indonesia
Correspondence: Dhelya Widasmara Email [email protected]
Introduction: Leprosy is a chronic infectious disease caused by Mycobacterium leprae that causes damage to the peripheral nerve, particularly Schwann cells. Treatment is useful only to kill bacteria but not to recover peripheral nerve damage. However, early detection of peripheral nerve damage is necessary. We examine P-75 neurotrophin (P75NTR) as an indicator of peripheral nerve damage in leprosy with the Semmes–Weinstein monofilament (SWM) test as the comparison.
Methods: This study uses a quantitative analytic observational study approach with cross-sectional design, conducted at Kediri Leprosy Hospital, Malang, East Java, Indonesia. All leprosy patients had a clinical examination and bacterial index to classify leprosy and then the SWM test to examine the presence of neuropathy in the palms and feet. P75NTR examination uses venous blood samples. An independent t-test was used to compare the SWM and P75NTR scores based on the type of leprosy, and then the Spearman correlation test was used to determine the correlation between SWM scores and P75NTR levels.
Results: In this study, SWM scores on the soles of the foot and palms and the P75NTR levels were higher in the PB group compared with MB (p< 0.05). Also, a significant positive correlation was found between P75NTR and the SWM scores on the palms of the hand (r=0.864; p=0.000) and the soles of the foot (r=0.864; p=0.000).
Conclusion: There is a strong positive correlation between P75NTR levels and SWM scores, so P75NTR levels are very likely to be a marker of neuropathy in leprosy, but further studies are still needed to examine the specific role of these biomarkers.
Keywords: leprosy, Semmes–Weinstein monofilament test, P-75 neurotrophin
Introduction
Leprosy is a chronic infection caused by Mycobacterium leprae bacteria that causes damage to the skin and peripheral nervous system (nerves outside the brain and spinal cord), skin, nasal mucous membranes, testicles, and eyes. This disease develops slowly (as early as 6 months and as late as 40 years) and can cause lesions on the skin and make secondary disability.1,2 According to the World Health Organization (WHO), leprosy is one of the 20th neglected tropical diseases that require special world attention.3 Leprosy is also known as “The Great Imitator Disease” because its manifestations are similar to many other skin diseases such as fungal skin infections so people rarely realise that they have leprosy.4
The prevalence of leprosy in the world is still quite high. The WHO noted that in 2014, 213,899 new cases of leprosy were detected worldwide, with the highest cases in the Southeast Asia region with a total of 154,834 cases.3 Indonesia is ranked as the third country of leprosy endemic after India and Brazil. East Java is one of the endemic areas of leprosy in Indonesia. Meanwhile, according to the Ministry of Health Survey in 2013, one-third of persons with leprosy in Indonesia were in East Java and equivalent to 5620 patients (14% were experienced by children with permanent disability). Also, until September 2014 there were 5622 new cases identified.6
M. leprae impairs the peripheral nerves of the human body. Depending on the damage to the peripheral nerves, peripheral nerve function disorders will occur such as sensory, motor, and autonomic. In general, if there is damage to nerve function that is not handled appropriately and precisely, defects will occur to a more severe level.7,8 Damage to sensory function results in numbness in the palms and feet, and injuries can occur easily. The cause of this neuropathy is because macrophages fail to phagocyte M. leprae in the body, which damages the nervous system so that the nerve cannot provide signals between the brain and other body parts.9,10
A simple method to assess sensory nerve function in leprosy is using the Semmes–Weinstein monofilament (SWM) test, which is an examination with a monofilament tool to assess sensations on the soles of the feet and palms, by applying gentle pressure using a monofilament placed in the soles of the feet and palms for 3 seconds until sensation is felt on the examination region. Every person without sensory nerve impairment should be able to feel the monofilament test. If the pressure is not felt in at least four of the ten predefined areas, then it can be assumed that neuropathy due to leprosy is present.11,12 The monofilament can be used as an early detection tool for nerve function disorders, which is an effort to prevent disability of people with leprosy. One of the earliest signs of impaired nerve function is loss of sensation in the palms and feet.
Recently, P-75 neurotrophin (P75NTR) has emerged as a potential target for the pharmacological control of neurodegenerative diseases. Based on previous research by Dechant et al, P75NTR plays a role in the regulation of neural plasticity, promotion of neurogenesis in adults, and increases expression in neurons, macrophages, microglia, astrocytes, and Schwann cells in response to lesions and neurodegenerative diseases.2
Also, at this time, assessing disability in leprosy still uses qualitative examinations such as the VMT (Voluntary Muscullari Test), SWM test, and WHO Disability Assessment, but because of the qualitative examination an inter-observer variation on interpretation will always be found.8 To date, there is no quantitative examination that can be used to assess disability in leprosy patients. Because of the potential of P75NTR in nerve cell regeneration and as a marker for damaged peripheral nerves, hereby the study aims to evaluate the correlation of the SWM test with P75NTR as a marker of peripheral nerve damage in leprosy patients.
Methods
Study Design
This study uses a cross-sectional survey design. The population of this study was patients with leprosy at Kediri Leprosy Hospital, East Java, Indonesia from July 2017 to August 2017. Data collection is done by examining the SWM test by a dermatologist expert in tropical skin disease. The monofilament is placed on the feet and palms using monofilament threads for 3 seconds; if the pressure is not felt, then it can be assumed that neuropathies due to leprosy are present. The inclusion criteria in this study were any type of leprosy patient multibacillary (MB) or paucibacillary (PB) that underwent therapy for less than 1 year. Exclusion criteria from this study were patients with leprosy reaction, psoriasis vulgaris-rosacea, steroid treatment for more than 7 days, atopic dermatitis, and other chronic medical diseases besides leprosy.
Tools and Laboratory Assessment
SWM test thread 0.2 g (white) was used to assess neuropathy on the palm and SWM test thread 2 g (blue) to assess neuropathy on the foot. Venous blood was taken as a sample for P75NTR assessment. The human P75NTR ELISA kit from Bioassay Technology Laboratory was used in this study. Monofilament examination is done at 10 points on each palm and foot (Figure 1), scored using binary numbers (0 means being able to feel the monofilament at the examination point; and score 1 means being unable to feel the monofilament at the examination point), a higher score indicating more severe neuropathy, and the average score for hand and sole of the foot was used for comparison. Scores will vary from 0 to 10 at each location examination, and a higher score indicates more severe neuropathy.
 |
Figure 1 Monofilament test points for examination. |
Statistical Analysis
Statistical analysis in this study uses SPSS version 22.0 for Windows (IBM Corporation, Armonk, NY, USA). A correlation test was used to evaluate correlation between the SWM score and the P75NTR level. Meanwhile, an independent t-test was used to compare the SWM score and P75NTR level based on leprosy type. All data are considered significant if p<0.05.
Results
The study involved 33 leprosy patients, 21 were MB type (63.6%) and 12 were PB patients (36.4%). We found there was a significant difference in SWM scores in PB-type leprosy compared with MB-type leprosy (5.5 vs 0.85; p=0.001). This shows that PB-type leprosy has a higher SWM score compared to the MB type, which means it has more severe neuropathy on the palms in the PB leprosy group (Figure 2).
 |
Figure 2 Average SWM score on leprosy patients’ palms between MB and PB types of leprosy. |
Similar findings were also found in the difference on the SWM foot region. PB-type leprosy has a higher SWM score compared to MB-type leprosy, indicating that neuropathy in the sole of the foot is more severe in PB-type leprosy compared to MB-type leprosy (Figure 3).
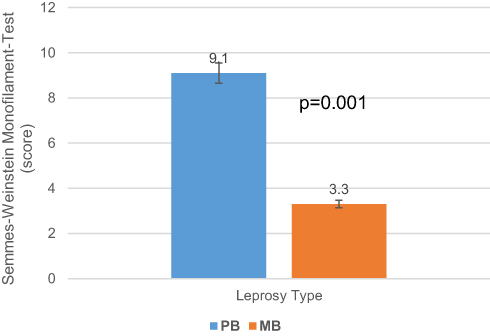 |
Figure 3 Average SWM score on leprosy patients’ feet between MB and PB types of leprosy. |
Comparison of P75NTR levels between MB and PB leprosy shows that PB leprosy has higher P75NTR levels compared to MB (40.09 ng/mL vs 32.65 ng/mL; p=0.001) (Figure 4). Also, we found a significant strong positive correlation between P75NTR levels on the score for theSWM test on the palm of the hand (r=0.864; p=0.000) and soles of the feet (r=0.864; p=0.000) (Figures 5 and 6). This shows that an increase in the P75NTR value will be followed with an increase in the SWM score. This can be interpreted as a description of the more severe neuropathy when higher P75NTR levels were found.
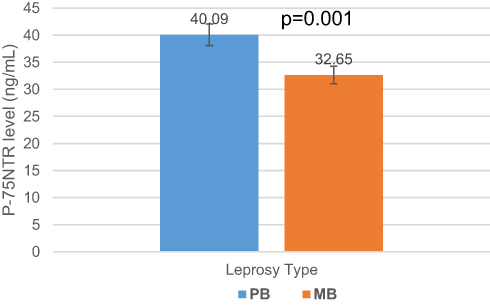 |
Figure 4 Comparison of P75NTR levels between MB and PB leprosy patients. |
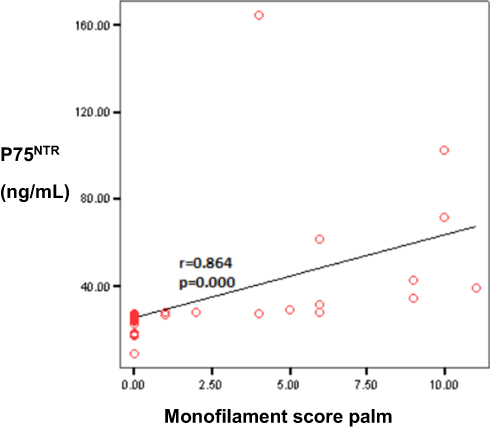 |
Figure 5 Correlation between P75NTR levels with SWM scores on the palms. |
 |
Figure 6 Correlation between P75NTR levels with SWM scores on the feet. |
Discussion
Peripheral nerve damage in leprosy patients is caused by infection with the bacterium M. leprae itself or the leprosy reaction. Sensory nerve damage occurs earlier than motor or autonomic nerve damage. Impaired touch sensation is one indicator to determine the level of disability of leprosy patients according to WHO criteria.13–15
M. leprae attacks macrophages, the cellular immune system, and the peripheral nervous system. The hypothesis of nerve damage mediated by the immune system is thought to be caused by the release of pro-inflammatory cytokines, including TNF-α, IL-6, and IL-1β by monocytes or macrophages. P75NTR can regulate monocyte/macrophage chemotaxis and induce nerve cell healing. The ability to interact with all Trk receptors, sortilin, and Nogo receptors allow P75NTR to control many signaling pathways. The roles of P75NTR that have been found in neurogenesis, growth regulation, synaptogenesis, and renewal of unwanted synapses make it the center of major signaling to promote nervous system healing.
In leprosy patients, the change in expression of some neurotrophins is related to the loss of nociceptive sensations in the initial phase. Association between nerve dysfunction in clinical tests and skin morphological changes in any type of leprosy has been well established. Based on previous studies, the lack of neurotrophins such as nerve growth factor (NGF) plays a role in the development of peripheral neuropathy, including in patients with MH and diabetes.4,18 In addition, a decrease in endogenous levels of NGF, NT3, and TrkA in skin lesions in leprosy has been reported.16,17 This indicates that the imbalance of neurotrophic factors plays a role in the disruption of peripheral nerve cell regeneration after nerve cells damage MH patients.19
In this study we found a strong positive correlation between P75NTR levels and SWM scores. Based on the WHO classification, leprosy is divided into two types, multibacillary and paucibacillary type. Pausibasiler (PB)-type leprosy occurs if the immune system is still able to fight M. leprae slightly; as a result, only a few bacteria multiplications were found.15,20 In the PB type of leprosy, macrophages try harder to phagocytose M. leprae, and induce higher pro-inflammatory cytokines such as TNF-α, IL-6, and IL-1β in the peripheral nerves, thereby inducing an increase in the amount of regulating P75NTR. Therefore, neural apoptosis in the PB type of leprosy is also more than in the MB type of leprosy.16,18 The occurrence of nerve apoptosis in large numbers will also be followed by a high SWM score due to more severe neuropathy. A better immunology response might be an explanation for the PB type of leprosy compared to the MB type of leprosy having higher SWM scores and P75NTR levels due to the higher amount of nerve apoptosis in PB-type leprosy.16,19
Thus, the number of nerve cells damaged or killed by M. leprae will automatically get a reaction to give signals to the body to activate pro-NGF activity. This activity will certainly activate P75NTR so that the blood circulating level of P75NTR will increase, so it can be used to detect nerve damage. Therefore, the amount of P75NTR that appears can be an indication that there is severe nerve damage due to M. leprae bacteria.20–22
High numbers of nerve cells damaged by M. leprae will automatically trigger signals to activate pro-neural growth factor activity. This activity will certainly activate P75NTR and increase its circulating level in blood and could be detected as a marker of nerve damage. Therefore, the amount of P75NTR that appears can be an indication that there is severe nerve damage due to M. leprae bacteria.5,17
Because this study is only a cross-sectional study, it is only able to provide a significant positive correlation between P75NTR on the SWM score, but has not been able to explain in detail the role of P75NTR on neuropathy in leprosy, so further research is needed to prove the causal relationship of P75NTR on the mechanism of leprosy neuropathy.
Ethical Consideration
All participants signed written informed consent prior to any data collection and all of the study consent process was acceptable and approved by the Ethical Committee Faculty of Medicine, Universitas Brawijaya with ethical clearance reference number: 001/EC/KEPK RSKK/06/2017. All procedures in the studies that involve human participants were in accordance with standards from the 1964 Declaration of Helsinki.
Funding
This study does not receive any specific grant from government or any private sectors.
Disclosure
The authors declare there is no conflict of interest regarding publication of current article.
References
1. Anand P. Neurotrophic factors and their receptors in human sensory neuropathies. Prog Brain Res. 2004;146:477–492.
2. Dechant G, Barde Y-A. The neurotrophin receptor p75NTR: novel functions and implications for diseases of the nervous system. Nat Neurosci. 2002;5(11):1131–1136. doi:10.1038/nn1102-1131
3. WHO. Neglected tropical disease. Geneve: WHO. Available from: https://www.who.int/neglected_diseases/diseases/en/.
4. Kusumaningrum N, Purnamawati S, Winarni DRA, Soebono H. Lepromatous leprosy mimicking systemic lupus erythematosus: a case report. Med J Indones. 2019;28(1):77–81. doi:10.13181/mji.v28i1.1793
5. Facer P, Mann D, Mathur R, et al. Do nerve growth factor-related mechanisms contribute to loss of cutaneous nociception in leprosy? Pain. 2000;85:231–238. doi:10.1016/S0304-3959(99)00273-0
6. Mia EP. Risk factors for leprosy in padang paramian regency. E J Andalas. 2016;1(2):1–7.
7. Facer P, Mathur R, Pandya SS, Ladiwala U, Singhal BS, Anand P. Correlation of quantitative tests of nerve and target organ dysfunction with skin immunohistology in leprosy. Brain. 1998;121:2239–2247. doi:10.1093/brain/121.12.2239
8. Friedman WJ. Neurotrophins induce death of hippocampal neurons via the p75 receptor. J Neurosci. 2000;20:6340–6346. doi:10.1523/JNEUROSCI.20-17-06340.2000
9. Fry EJ, Ho C, David S. A role for Nogo receptor in macrophage clearance from injured peripheral nerve. Neuron. 2007;53:649–662. doi:10.1016/j.neuron.2007.02.009
10. Hart AM, Terenghi G, Kellerth JO, Wiberg M. Sensory neuroprotection, mitochondrial preservation, and therapeutic potential of N-acetyl-cysteine after nerve injury. Neuroscience. 2004;125:91–101. doi:10.1016/j.neuroscience.2003.12.040
11. Hempstead BL, Martin-Zanca D, Kaplan DR, Parada LF, Chao MV. High-affinity NGF binding requires coexpression of the trk proto-oncogene and the low-affinity NGF receptor. Nature. 1991;350:678–683. doi:10.1038/350678a0
12. Hobbenaghi R, Tiraihi T. Neuroprotective effect of deprenyl in sensory neurons of axotomized dorsal root ganglion. Clin Neuropharmacol. 2003;26:263–269. doi:10.1097/00002826-200309000-00011
13. Kraemer BR, Yoon SO, Carter BD. The biological functions and signalling mechanisms of the p75 neurotrophin receptor. Handb Exp Pharmacol. 2014;220:121–164.
14. Longo FM, Massa SM. Small-molecule modulation of neurotrophin receptors: a strategy for the treatment of neurological disease. Nat Rev Drug Discov. 2014;12:507–525. doi:10.1038/nrd4024
15. Lastoria JC, Abreu MA. Leprosy: a review of laboratory and therapeutic aspects – part 2. An Bras Dermatol. 2014;89(3):389–401. doi:10.1590/abd1806-4841.20142460
16. Meeker RB, Williams KS. The p75 neurotrophin receptor: at the crossroad of neural repair and death. Neural Regen Res. 2015;10(5):721–725. doi:10.4103/1673-5374.156967
17. Michellin LB, Barreto JA, Marciano LH, et al. Leprosy patients: neurotrophic factors and axonal markers in skin lesions. Arq Neuro Psiquitar. 2012;70(4):281–286. doi:10.1590/S0004-282X2012000400012
18. Milanez MA, Abreu M. Leprosy: review of the epidemiological, clinical, and etiopathogenic aspects – part 1. An Bras Dermatol. 2014;89(2):205–218. doi:10.1590/abd1806-4841.20142450
19. Qiu J, Cafferty WB, McMahon SB, Thompson SW. Conditioning injury-induced spinal axon regeneration requires signal transducer and activator of transcription 3 activations. J Neurosci. 2002;25:1645–1653. doi:10.1523/JNEUROSCI.3269-04.2005
20. Raivich G, Hellweg R, Kreutzberg GW. NGF Receptormediated Reductionin Axonal NGF Uptake and Retrograde Transport Following Sciatic Nerve Injury and During Regeneration. Neuron. 1995;7:151–164. doi:10.1016/0896-6273(91)90083-C
21. Wilson AD, Hart A, Brannstrom T, Wiberg M, Terenghi G. Delayed acetyl-L-carnitine administration and its effect on sensory neuronal rescue after peripheral nerve injury. J Plast Reconstr Aesthet Surg. 2007;60:114–118. doi:10.1016/j.bjps.2006.04.017
22. Zhang CG, Welin D, Novikov L, Kellerth JO, Wiberg M, Hart AM. Motorneuron protection by N-acetyl-cysteine after ventral root avulsion and ventral rhizotomy. Br J Plast Surg. 2005;58:765–773. doi:10.1016/j.bjps.2005.04.012
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.